Pharma Mrp 1
90
- 1 - A MANAGEMENT RESEARCH PROJECT ON PHARMACEUTICAL INDUSTRY
Transcript of Pharma Mrp 1
- 1 -
A
MANAGEMENT RESEARCH PROJECT
ON
PHARMACEUTICAL
INDUSTRY
- 2 -
CHAPTER-1
INTRODUCTION OF PHARMACEUTICAL INDUSTRY
1.1 About Pharmaceutical Industry. 1.2 Bulk Drugs and Formulation.
1.3 Research & Development.
- 3 -
ABOUT PHARMACEUTICALS:
Pharmaceuticals are medicinally effective chemicals, which are converted to dosage forms suitable for patients to imbibe. In its basic chemical form, pharmaceuticals are called bulk drugs and the final dosage forms are known as formulations. Bulk drugs are derived from 4 types of intermediates (raw materials), namely
• Plant derivatives (herbal products) • Animal derivatives e.g. Insulin extracted from bovine pancreas • Synthetic chemicals • Biogenetic (human) derivatives e.g. Human insulin
They are substance known as medicine, used in preventing and curing illness and disease. Usage of pharmaceutical is governed by underlying science of illness and disease. The branches of medical science are shown in figure 1.1.
Figure 1.1 Branches of medical science

- 4 -
1) Allopathy: It is known as the modern medicine and world over the pharmaceutical industry is focused upon it.
2) Ayurveda: It is an ancient Indian medical science and mainly uses herbal remedies. It is gaining importance in pharmaceutical market particularly in United States.
3) Unani: It has its origin in China and is prevalent in South East Asia.
4)Homeopathy: It was founded by a German physician and was fairly popular in 19th century. It is still prevalent in third world countries.
- 5 -
BULK DRUGS AND FORMULATION: In basic form, pharmaceutical are called bulk drugs. They are derived from intermediate raw material, namely
1) Plant derivatives
2) Animal derivatives
3) Synthetic chemicals
Formulation:
Bulk drugs in their raw form cannot be used as medicine and they have to be converted in to form in which human can use them as medicine. This type of final dosage form is known as formulations. Formulations can be classified into two types namely,
1) Ethical products These types of formulations are available only under medical prescription to prevent
misuse. Doctors, to cure a disease in the patient primarily prescribe ethical formulations. Generally, for ethical products direct advertisements to users is prohibited.
2) Over the Counter products: These types of formulation known as OTC can be purchased by users directly, for example pain balms, health tonics etc. For over the counter product direct advertisements to user can be used to promote product under certain conditions.
Formulations can be categorized as per the route of administration to patients, namely, 1) Oral: They are taken internally by patients, for example tablets, syrup, capsules, powders etc. 2) Topical: They are applied on skin, for example creams, ointments, liquids, aerosol etc. 3) Parenterals: They are injected in an intravenous and intramuscularly fashion. 4) Others: It includes eye drops, surgical dressings etc.

- 6 -
Research and Development Four types of research are conducted in the pharmaceutical industry:
1. Fundamental or Basic Research: This involves discovering new molecules from scratch. No Indian company does basic research, simply because it is far too expensive. Indian drug companies don’t make the kind of profits required for automation. In the West, compounds are screened by robots or hi-tech equipments and the equipment can cost up to 2 billion pounds (Rs 13,800 crores).
2. Process Research or Reverse Engineering: Here, a company copies a molecule
(Indian patent law covers process patents, not product patents). Reverse engineering by Indian companies has been very cost effective and efficient. However, Western companies regard this as a violation of intellectual property rights (IPR). A new patent law will, obviously, not permit reverse engineering.
3. Analogue or Discovery Research: Companies modify an existing molecule (or a
new one that hasn’t yet been commercialized), after accessing international patent databases, to arrive at a new molecule. Some of the bigger Indian companies (Ranbaxy, Dr Reddy’s, Torrent, Sun pharma) are either conducting discovery research or plan to do so.
4. Genetic Research: It aims at establishing the link between genes and diseases and
could one day determine the best drugs for individuals based on their genetic makeup. No Indian company does this kind of research, but several government or academic institutions (National Institute of Immunology and Jawaharlal Nehru University in New Delhi, Center for Microbiology in Hyderabad) have begun work in this area.
Few doubt that India has the potential to emerge as a global research and development base in sectors like pharmaceuticals and software. But that does not necessarily mean that it will. The key lies in the country’s ability to scale up its research and development expenditure. At last count, India’s research and development expenditure stood at 0.86 per cent of the GDP, which is much lower than that 0of developed countries such as the US (2.79 per cent), Japan (2.83 per cent) and Germany (2.33 per cent). Similarly, if India has to realize its potential of becoming a leading supplier of generic drugs, the pharma sector will need to increase its R&D spend almost five-fold in the next five years- from Rs 320 to 1,500 crores.
- 7 -
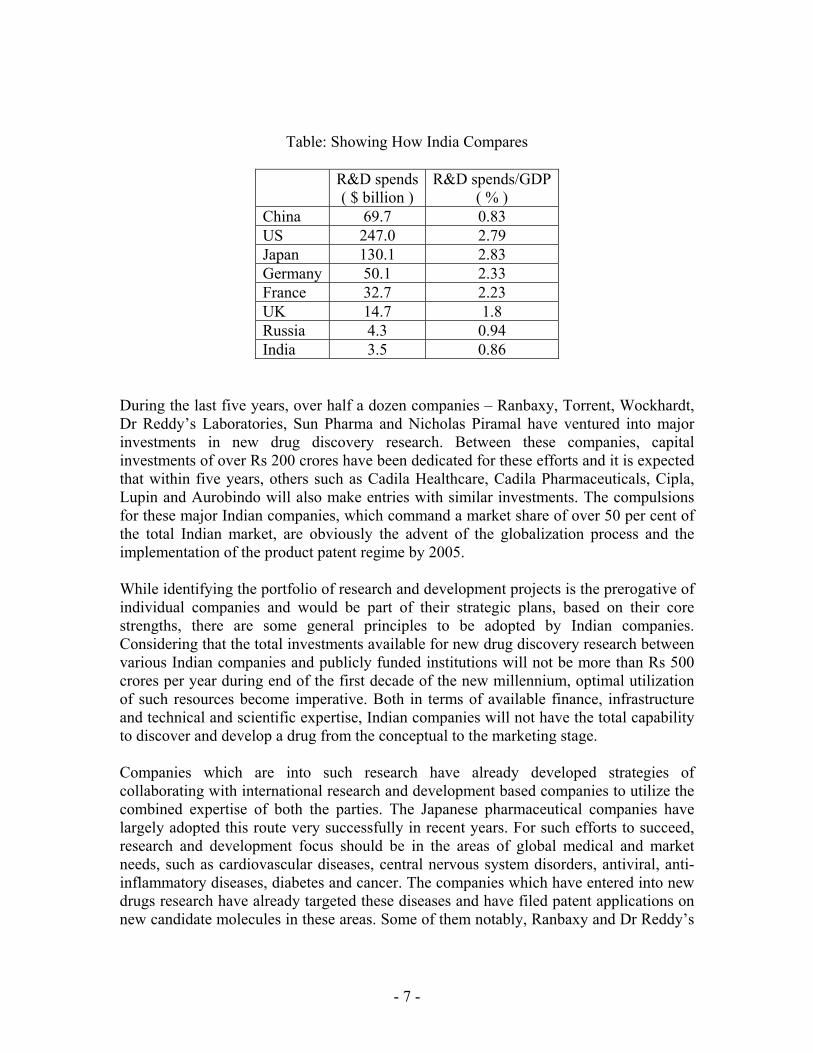
Table: Showing How India Compares
R&D spends( $ billion )
R&D spends/GDP( % )
China 69.7 0.83 US 247.0 2.79 Japan 130.1 2.83 Germany 50.1 2.33 France 32.7 2.23 UK 14.7 1.8 Russia 4.3 0.94 India 3.5 0.86
During the last five years, over half a dozen companies – Ranbaxy, Torrent, Wockhardt, Dr Reddy’s Laboratories, Sun Pharma and Nicholas Piramal have ventured into major investments in new drug discovery research. Between these companies, capital investments of over Rs 200 crores have been dedicated for these efforts and it is expected that within five years, others such as Cadila Healthcare, Cadila Pharmaceuticals, Cipla, Lupin and Aurobindo will also make entries with similar investments. The compulsions for these major Indian companies, which command a market share of over 50 per cent of the total Indian market, are obviously the advent of the globalization process and the implementation of the product patent regime by 2005. While identifying the portfolio of research and development projects is the prerogative of individual companies and would be part of their strategic plans, based on their core strengths, there are some general principles to be adopted by Indian companies. Considering that the total investments available for new drug discovery research between various Indian companies and publicly funded institutions will not be more than Rs 500 crores per year during end of the first decade of the new millennium, optimal utilization of such resources become imperative. Both in terms of available finance, infrastructure and technical and scientific expertise, Indian companies will not have the total capability to discover and develop a drug from the conceptual to the marketing stage. Companies which are into such research have already developed strategies of collaborating with international research and development based companies to utilize the combined expertise of both the parties. The Japanese pharmaceutical companies have largely adopted this route very successfully in recent years. For such efforts to succeed, research and development focus should be in the areas of global medical and market needs, such as cardiovascular diseases, central nervous system disorders, antiviral, anti-inflammatory diseases, diabetes and cancer. The companies which have entered into new drugs research have already targeted these diseases and have filed patent applications on new candidate molecules in these areas. Some of them notably, Ranbaxy and Dr Reddy’s
- 8 -
Laboratories have already entered into licensing arrangements with international companies. Besides these areas, it is also imperative that Indian companies involve themselves in research and development for the discovery of new drugs for diseases which are largely endemic to the developing countries. Many of these diseases have not been properly addressed by the multinational corporations in view of the small market and the low buying power of the patients. In such cases, since they largely belong to the orphan drug category, with potentially very low commercial returns, government and international agencies should subsidies the companies by providing funds for carrying out research in those areas. While fixing targets for outcomes from research and development inputs is risky, it is fair to assume that with annual investments reaching Rs. 500 crores per year by 2010, form all sources, Indian industry should be able to discover and develop at least three new molecular entities per year for various disease conditions. It is also expected that around 50 new patents will be issued or applied for, based on Indian research efforts. A part form the above investments by Indian companies, multinational companies will also invest in basic research in India, including clinical research, both on their own and through contract research organizations. Considering the variety and quantum of intellectual capital available and low overhead costs, it is fair to assume that international companies will do well to establish research and development centers here. Other areas which have the potential to be major targets for attention in India are research and development efforts in innovative and patentable new drug delivery systems for established drugs, a relook at racemic molecules with reference to the potential for developing new chiral drugs, biotechnology products and development of new clinical indications for drugs in current use. Most importantly, an area of great relevance to India is the area of drugs based on the Indian traditional system of medicine. General Insurance Company (GIC) is the sole medical insurance provider in the country, covering only 4 per cent of the population. There could be significant opportunities for pharma companies when the health insurance sector opens up to private sector. By forming exclusive alliances with insurance companies, pharma companies could potentially increase penetration of their products within the insurer’s customer base. Based on patient’s medical records from insurance companies, they could undertake customized marketing and distribution programs to increase sales and build loyalty.

- 9 -
Recognizing the importance and strengths of the Indian pharmaceutical industry, the Government of India has made conscious efforts to assist its overall development to meet the challenges of the post 2005 era. The two committees which have been constituted for this purpose have come out with very positive recommendations to create an ambience conducive to the development of a strong research and development based drug industry supported by appropriate fiscal measures. At this stage, the Indian industry needs this support and its success will depend only on the concerted efforts of all parties concerned with healthcare in this country.

- 10 -
CHAPTER -2 INRODUCTION OF INDIAN PHARMACEUTICAL
INDUSTRY 2.1 – Overview 2.2- History and Development 2.3- Major Therapeutic Segments 2.4- Growth drivers of the Indian
Pharmaceutical Industry.

- 11 -
2.1 OVERVIEW:
• The pharmaceutical industry is a lifeline industry which plays a very crucial role in building a strong human capital of a country and is very essential for economic growth and development.
• Today, it is at the top end of India's science-based industries with wide ranging capabilities in the complex field of drug manufacture and technology. The contribution of the pharmaceutical industry towards a nation’s growth cannot be undermined.
• The Pharmaceutical industry in India is one of the largest and most advanced among the developing countries.
• Today it is in the front rank of India’s science-based industries with wide ranging capabilities in the complex field of drug manufacturing and technology.
• The Indian pharmaceutical industry is highly fragmented, but has grown rapidly due to the friendly patent regime and low cost manufacturing structure.
• Globally, the output of Indian pharmaceutical industry ranks 4th in terms of volume and 13th in terms of value.
• Intense competition, high volumes and low prices characterize the Indian domestic market. Exports have been rising at around 30% CAGR over last five years.
• In India, medicines account for 2.5% in hospitalization and 0.5% in domiciliary treatment cost.
• There could be sharp dip in the growth rate in the population in India, which is already down to about 1.7% year and is projected to go down further to about 1.5% by the turn of the century and to roughly 1% by2010.
• Indian’s per capita expenditure for healthcare remains Rs.115.5 compared to the US (Rs.6876.00) and Japan (Rs.14, 832).
• In India the values for pharmaceutical production of bulk drugs and formulations in 2001-02 were Rs.5439 Crores and Rs. 21104 corers respectively.
• The Indian Pharmaceutical market ranks about 20th in the world and accounts for less than 1% of world market. It is expected by 2003; the market could be worth of $ 7-9 billion (Rs.280 billion to Rs.360 billion).
• India accounts for 6% of all bulk drugs export. There are about 250 large/medium units and about 8000 small-scale units in operations, which form the core of the industry. There are about 350 bulk drugs i.e. active pharmaceutical molecules having therapeutic values and used for production of pharmaceuticals, which accounts for, majority of formulations produced in the country.
• During the year ending March 1998, pharmaceutical companies for various bulk drugs, formulations and intermediates filed 265 IEMs. These IEMs are expected to generate employment for about 19000 people and there would be an investment of approximately Rs.4.1 billion on these projects. During the same period foreign investment proposal worth approx. Rs.1.6 billion were approved.
• Between August 1991 and March 1998, Gujarat received 5174 proposals for the projects and topped the list in terms of value of investment, which was estimated

- 12 -
to be Rs.1379 billion during that period. Next to Gujarat was Maharashtra and other States receiving more than 5% of the investment proposal are Tamil Nadu, Andhra Pradesh, Karnataka, Uttar Pradesh, Punjab and Madhya Pradesh.
• The top 12 companies in India together will have a turnover of around 50 billion in the domestic market by 2005, or approximately 25% of industry turnover. About half a dozen companies with a turnover of Rs.35 billion by 2005 will be able to spend about 8% of their turnover on research.
• The Drug Pricing Control Order (DPCO) has severely restricted profitability and hence innovation. However, the government has been relaxing controls in a slow but progressive manner. The span of control of DPCO has come down from 90% in 1980s to 50% in 1995 and is likely to be further reduced as per the latest proposed changes.
• In the domestic market, old and mature categories like anti- infectives, vitamins, analgesics are degrading or stagnating while new lifestyle categories like cardiovascular, CNS, anti diabetic are growing at double-digit rates. The growth of a company in the domestic market is thus critically dependent on its therapeutic presence.
• The growth in the Indian pharmaceuticals:
Industry at around 15% p.a. compares well with the industry’s growth of 14% per annum in North American Region. India is ranked 5th in the World, and accounts for 8% of the worlds production of drugs and pharmaceuticals by volume.
• Globally, the output of Indian pharmaceutical industry ranks 4th in terms of volume and 13th in terms of value.
• In FY02, the domestic Indian pharma market was valued at $4.5bn, representing 1.6% of the global market, and is growing at an annual rate of 8 to 9%.
• The industry produces about 60,000 finished medicines and roughly 400 bulk drugs, which are used in formulations.
• At the end of FY01, the Indian pharmaceutical industry had over 23,000 units, although this number cannot be authenticated. Around 260 players constituted the organized sector while 6,000-8,000 players existed in the small scale sector.
• The industry is highly fragmented, with the largest formulation players having a market share of less than 6%.
• The top ten players account for 36% of the formulation market in contrast with the global scenario where the top ten players account for 49% of the Pharmaceutical market.
• In FY01, the total output of the Indian pharmaceutical industry was Rs 229 bn, which grew by 16% yoy. In FY02, it was above Rs. 260 bn, of which bulk drugs accounted for Rs. 54 bn (21%) and formulations Rs 210 bn (79%).
• The demand for the industry is mainly from urban areas (74%).

- 13 -
• Urban areas witnessed a 15% increase in sales in FY02 as against 13% in FY01. • The industry grew at 2.6% yoy during Oct 2002 and 9% during Jan to Oct 2002. • In FY03, the industry would have grown by 10-15% increase in sales, production
and exports, despite adverse global conditions. • The odd 400 bulk drugs make up 20% of total drug production. During FY91-
FY01, the production of bulk drugs increased at a compounded annual growth rate (CAGR) of 20%.
• On the other hand, formulations, which are the end product of the medicine manufacturing process, had a CAGR of 17% during FY91-FY01. Most of the domestic demand for formulations is met by the domestic industry.
- 14 -
2.2 HISTORY AND DEVLOPMENT:
History of pharmaceutical industry in India:
• India’s traditions in the science of health and healing go back to the halcyon days of Susruta, Vaghatta and Charska. Our systems of medicine like Ayurveda were well established and schools and hospitals with treatises and instructions manual were in wide use.
• The establishment of a modern pharmaceutical industry in India may be and to have commenced with the setting up of Bengal Chemicals by Acharya P.C. Ray in Calcutta and of Alembic Chemicals in Baroda, by B.D. Amin. Significant who helped the indigenous drug industry were the establishment of the Haffkine Institute in Bombay, the King Institute in Madras in 1904 and the Pasteur Institute in Coonoor in 1907.
The Early Years
• The industry received a fillip during World War I as the local demand for allopathic medicines increased steeply and imports were almost completely cut off. The outbreak of World War II proved to be a shot in the arm for the industry. A number of products in the category of phyto-chemicals, based on indigenous raw materials and several synthetic drugs and biological were manufactured during the war period. The immediate post-war years (1945-1947) experienced a continued shortage of drug and pharmaceuticals throughout the world. The industry in India had, therefore, no difficulty in maintaining its tempo of growth.
Post Independence Development
• In the post-independence years, several international pharmaceutical companies have set up manufacturing facilities in the country. Public sector units like HAL and IDPL were also set up. The diversified character of the industry's growth is reflected in the range and variety of products manufactured. These cover a wide therapeutic spectrum ranging from antibiotics to vitamins. The following table gives us a picture of the progress of drug industry in India.
In Financial year 2002:
• Several out licensing deal have been entered into pharma majors in the last few months and many more are ripe. This is a strong pointer to the fact that the country is gearing up for the patent regime (post 2005). Dr. Reddy’s anti-diabetic molecule out licensed to Novo-Nordisk entered the last stage of clinical trials before it enters commercial.
• The domestic industry recorded a 9% growth rate, falling short of historic double-digit growth rates. The primary reason for the same is due to the fact that domestic market continues to remain price sensitive and premium pricing of product is extremely difficult to maintain.

- 15 -
• MNC’s continued to under perform their domestic peers for the second consecutive year in succession. While the top 5 domestic companies recorded a revenue growth of more than 20% last year, consolidated MNC pharma growth was less than 3% with margins at half the average of domestic majors. However, MNC’s have been quick in responding to this trend with most companies intensively restructuring their operations in a bid to bounce back. Post restructuring, MNC pharma majors are expected to record healthy growth rates though growth rates are still expected to be lower than the domestic majors.
• The pharma industry is expected to have grown by 8-9% in FY01. While top 5 domestic companies have grown at 14% in FY01, top 5 MNC’s have grown at a slower rate of 7.2%. The slow growth in sales of MNC’s is because of their relatively older product portfolio. As in the past MNC’s continued to shy away from launching new products in the domestic markets.
• Growth in traditional therapeutic segments such as antibiotics is stagnating and competition is increasingly getting stiffer. The price war is so intense that companies have in-fact started promoting unbranded versions of formulations (alternatively called as “generic generics”) against their own branded formulations, to generate growth. However, life style segments such as cardiovascular, anti-diabetes, anti-ulcer and anti-depressants are lucrative and fast growing. Growth in domestic sales in the future will depend on the ability of companies to launch/shift products in relatively fast-growing therapeutic segments. These are likely to be the key earnings drivers. Volumes may, however, continue to come from traditional segments such as anti-invectives, vitamins, tonics and mineral supplements.
• A committee, formed to recommend measures for legitimizing the OTC business in India, has suggested that some 67 brands be sold through OTC. This will help in expanding the size of the market, as companies will be permitted to advertise via mass media and increase availability of these products.
• A new concept that is gaining momentum in the pharma industry is contract research apart from contract manufacturing. Given the low cost high quality advantage Indian companies are poised to benefit from contract research business on behalf of multinationals. As for contract manufacturing, large global pharmaceutical companies are finding it profitable to outsource production. To cash on these opportunities many large production houses in the country are becoming US FDA compliant.
• The expiry of patents going off patent in the next few years is opening up big opportunity for domestic companies to capture the consequent generic market in the US and the Europe. The US generic market is projected to be US $ 15 bn by 2004. Though generic is low margin business, Indian company’s skills in reverse engineering and cost effective production enables them to yield better realisations. Indian Pharma companies like Sun Pharma, Dr. Reddy, Ranbaxy are aggressively trying to cash in on this opportunity.
• The government has recently allowed 100% Foreign Direct Investment Pharma FDI in drugs and pharmaceutical companies. This is expected to open floodgates of contract research work in the country. However, technology transfer by MNC’s even to 100% subsidiaries seems quite unlikely before 2005 deadline.

- 16 -
• The penetration of health insurance is abysmally low in the country. The entry of private players would not only bring in quantum leap in the health insurance business but also increase capital inflows into this sector. It would also bring in the concept of managed healthcare in the country. These would finally lead to overall increase in per capita usage of drugs.

- 17 -
2.3 MAJOR THERAPEUTIC SEGMENTS:
This section gives an overview of the major therapeutic segments in the Indian pharmaceuticals sector. These segments account for nearly 85% of the domestic formulation market
Indian TherapeuticSegments
Market Share (%)
Growth
Systemic Antibiotics 15.7 5.9 Cardiovascular 6.9 17.4 CNS 6.5 11.5 Vitamins 6.1 8.7 Anti-Inflammatory 6 12.9 Cough and Cold Preparations 5.3 1.7 Antacid and anti-Ulcerants 4.3 15 Anti-TB 2.5 -3.1 Anti-anemic 2.8 10.7 Anti-diabetic 2.7 34.1 Analgesic 3.10 15 General nutrients 1.80 -1. Anti parasitic & antifungal 3.9 19

- 18 -
1. Analgesics & anti-pyretics:
• They are used for relief in pain/ fever. In this segment, most of the popular drugs like Aspirin, Analgin and Paracetamol are off patent.
• Yet, DPCO coverage is high hence, margins are low. In case of formulations, including OTC brands and anti-spasmodic combinations, the market size is around Rs. 3.1 bn and is growing 15% yoy.
• But, a large number of local players result in keen competition, while volumes drive sales.
• Major players in formulations are Burroughs Wellcome, SmithKline Beecham, Hoechst and Wockhardt. Paracetamol and Analgin formulations also have large export markets.
2. Antacids and anti-ulcerants
• This segment has large number of new under-patent molecules, due to ongoing R&D on developing more effective ways to combat acidity/ ulcers.
• DPCO coverage is high as it encompasses the major drug Ranitidine. But, as this globally popular anti-ulcer drug has gone off patent in Jul ’97, there are good export opportunities.
• The domestic formulations market for antacids is estimated to be Rs 4.3 bn, growing 15% yoy.
• Major players are Knoll and Parke Davis. For anti-ulcer formulations, market size is Rs2.3bn growing at 17-18% yoy, with major growth in Omeprazole based formulations.
• Major players are Glaxo, Cadila, Ranbaxy, and Dr Reddy’s Labs etc.
3. Antibiotics:
• They are a vast range of drugs. The earlier generation drug groups such as Penicillins (e.g. Amoxycillin) and Macrolides (e.g. Erythromycin) have mostly gone off patent. Newer generation groups like Quinolones (e.g. Ciprofloxacin) and Cephalosporins (e.g. Ceftriaxone) are still largely under patent.
• DPCO mostly encompasses the latest generation drugs. Penicillin-G, itself an antibiotic drug, is a common intermediate for many other antibiotics.
• Total domestic formulations market is estimated to be Rs 15.7 bn and is growing at 5.9% yoy. Of this, 27% is accounted by semi-synthetic Penicillins. The fastest growing major subgroup is Cephalosporins at 23.9% yoy.
• Major players are Glaxo, Ranbaxy, Cipla, Hoechst, Alembic, Burroughs Wellcome, and Ambalal Sarabhai etc.
• Antibiotics also have a large export market, especially off-patent drugs like Amoxycillin, Ampicillin, Sulphamethoxazole and Cephalexin. Cephalosporins, which will be going off patent in near future, have a high export potential.
- 19 -
4. Anti-tuberculosis:
• These products find greater application in developing nations due to tropical concentration of the disease incidence. All popularly used drugs are off patent
• DPCO continues to cover the main drug Rifampicin. • The dominant player in both bulk drugs and formulations is Lupin. The domestic
formulations market is estimated to be Rs 2.5 bn, losing 3.1% yoy. • Other major players are Hind. Ciba and Cadila. MNCs like Glaxo and Hoechst are
increasing their presence in this segment. Export opportunities may grow manifold if the spread of AIDS leads to large-scale resurgence of TB in developed nations.
5. Cardiac therapy:
• It is the world’s top therapeutic segment and new drugs are continually introduced by MNCs abroad.
• However, most of the drugs popularly used in India are off patent. DPCO coverage is also low.
• Domestic formulations market size, estimated to be Rs 6.9 bn is growing 17-18% pa.
• The leading players are mostly local companies like Sun Pharma, Torrent, Cadila, ICI etc. Share of MNCs is relatively low. With increasing level of urbanization in India, heart trouble is on the rise. Also, cardiac care is a long-term therapy, providing a good market for the players.
6. Anti-rheumatics:
• These products relieve inflammation/ joint pain and also have analgesic/ anti-pyretic properties.
• All major drugs used in India are off patent yet DPCO coverage is high especially due to inclusion of major drug Ibuprofen under price control. However, DPCO ’95 excluded another major drug Diclofenac Sodium. The domestic formulations market is estimated to be Rs 6 bn, growing at 12.9 %yoy. The growth is again hampered by DPCO coverage, while volumes largely drive sales.
• Major players are MNCs like Knoll, Roussel, Hind Ciba, and Pfizer etc. Local players have higher presence in topical formulations. A large global market for anti-rheumatics makes Ibuprofen the top pharmaceutical product exported from India. But, even here multiple players has kept margins low.
- 20 -
7. Respiratory system:
• Ailments like cough and are common occurrences, especially among children. Asthma is often chronic, providing assured long-term demand for medication. Patent coverage is very low.
• Also, as DPCO has excluded most popular anti-cough drugs, there have been price hikes and high sales growth.
• The domestic cough & cold formulations market is estimated to be Rs 5.3 bn, growing 1.7% yoy.
• Of this 75% are anti-cough preparations, wherein major players are MNCs like Pfizer, Parke Davis, Rhone Poulenc. In anti-cold formulations, key players are Burroughs, Alembic etc. The anti-asthmatics market is Rs2bn, growing 15.5% yoy. The dominant leader here is Cipla.
8. General Nutrients:
• They are taken mostly in case of deficiencies in India. Globally, the trend is towards imbibing them as a tonic.
• So, if such a fad catches on, the Rs 1.8 bn domestic market losing 1% yoy, would notch good growth in future.
• All drugs are off patent but DPCO coverage is very high. • Leading players are MNCs like E-Merck, Pfizer, Glaxo, Abbott etc. Local players
have very poor presence in the segment, probably deterred by the high DPCO coverage which limits margins.
9. Other therapeutic segments:
• This covers segments like Anti-anemic, Anti-diabetes, Anti-emetic, Anti-histamine, Anti-malarial, CNS & Psychiatric therapy, Gynecological, Nutrients & Mineral Supplements.
• The major group is a Psychiatric product, which has Rs 6.5 bn market, growing 11.5% yoy. All other groups range between Rs 1-2 bn in size.
• The antidiabetic market is growing at the rate of 34% in present environment.
- 21 -
2.4 GROWTH DRIVERS OF THE INDIAN PHARMACEUTICAL INDUSTRY:
Indian pharmaceutical industry, which is highly fragmented due to various therapeutic segments and specialty of individual firm in each segment, drive it due to following growth drivers in the present era.
• Industry’s entrepreneurship and its scientific and technological skills:- Unique blend of this two key elements with innovative marketing strategies gave cutting edge to the Indian companies in the market.
• Low manufacturing cost base: The cost of manufacturing is lower in India due to low labor costs and lower equipments cost.
• High process development skills: Specialization of the companies by reverse engineering enables them to develop cost effective and non-infringing processed for product going generic. India has a history of developing such processes due to the prevalence of process patents.
• Business Environment: The government has recently allowed 100% Foreign Direct Investment Pharma FDI in drugs and pharmaceutical companies. This is expected to open floodgates of contract research work in the country.
• Innovative Scientific manpower & competent workforce: India has a pool of personnel with high managerial and technical competence as also skilled workforce. It has an educated work force and English is commonly used. Professional services are easily available.
• Friendly Patent regime: The current Patent law in India relating to Pharmaceuticals provides for only process patent which encourage various small scale companies to go for reverse engineering and make the profit.
- 22 -
Chapter 3
Emergence of Indian Pharma MNCs
3.1 Global MNCs
3.2 R&D in MNCs
3.3 Emerging Indian Pharmaceutical Industry
3.4 Emerging global generic market

- 23 -
Global MNCs: Global leaders of the pharma industry which dominate all components of business and industrial activity in drugs, including R & D, production and marketing are the MNCs located primarily in the US, Western Europe and Japan. MNCs are defined as ‘Large Business Companies which operate in many countries’. These highly visible corporations which are generally regarded as products of the capitalists and free trade societies of the Western world, gained their dominance during the second half of the last century. Today they control the markets as well as the economies of not only the countries where they are based, but also of many other countries in the developed and developing world. In the pharmaceutical industry the top twenty companies of the western world command over 60% of the global markets and due to various compulsions, these companies are getting to be more and more dominant through arrangements between them. The global MNCs have some special characteristics, even though, even within them, there are wide disparities. For example, the US MNCs have over 60% of their global sales coming from their domestic market, while the MNCs of the smaller European countries such as Switzerland, Sweden, Denmark etc. sell over 90% of their global production abroad. The third category of MNCs is illustrated by the case of Japan, which has over the last half a century adopted a policy of licensing their products to western MNCs for development and marketing in territories outside Japan. R&D in MNCs: Over 90% of the drugs available today have been discovered and developed by the R & D based MNCs, the majority of them from the USA. These US companies together had a turn-over of around $178 billion ($130 billion in USA and $48 billion abroad) in 2001. as a percent of sales, their average R & D spend within the US in 2001 was around 13.8% and abroad around 3.5%. Over 60% of their total R & D expenditure is currently in areas of cancer (18.5%), infections (12.7%), and cardiovascular system disease (11%). Outside the US, R & D activities of US MNCs are largely in Western Europe (52%), Japan (12%), Canada (5.3%) and Central & Eastern Europe (5.2%). It is significant that R & D spending by MNCs of Us origin in the Asia-Pacific region is as low as 0.9% of their total investment in R & D. Global MNCs in most cases market their products in over 100 countries of the world, directly or through their fully or partly owned subsidiaries. Yet another characteristic of their operations is that they, as a rule, set up manufacturing and R & D bases in locations which provide maximum benefits to them in terms of costs of production. Critics of MNCs feel that these companies have no allegiance to the countries where they operate

- 24 -
and have little regard for the economic or societal problems of the countries where they are domiciled. The three major trade blocks, the European Community (EC), the North American Free Trade Agreement (NAFTA) and the Asian-Pacific Economic Conference (APEC), as well as the General Agreement for Tariffs and Trade (GATT), have further provided the impetus for MNCs to freely roam the world at their pleasure and sweet will. The MNCs have also mastered the science of transfer pricing as a valuable tool to maximize profits form global business, across countries. Emerging Indian Pharmaceutical MNCs: Indian pharma companies need to satisfy the following conditions if they are to graduate to the status of multinational corporations (MNCs):
• A product range of relevance to major markets abroad.
• Access to these markets with generic (patent expired or non patented) products.
• Costs and price advantages.
• Production as per the regulatory requirements, such as adherence to Good Laboratory, Good Manufacturing and Good Clinical Practices.
• R & D capability for discovery and total or partial development of drugs relevant
to other markets.
• Marketing facilities through subsidiaries or through tie-ups with local companies.
• Ability to get Abbreviated New Drug Application (ANDA) approvals to enable early marketing of generic versions of patented drugs.
Indian Companies with Potential to be Drug MNCs: It is significant that in the US and Western Europe, the largest MNCs are those which are research based companies, each one of them investing over $1 billion annually in R & D mostly on new drugs research. While the US companies spend bulk of the R & D budget within the US, they increasingly carry out or outsource R & D from companies abroad. For example, while the growth in domestic R & D by these companies was 11.8% in 2001 over 2000, the corresponding figure for R & D abroad was 33.8%. The companies in India which have invested in New Drugs Discovery Research include Ranbaxy, Dr Reddy’s Laboratories, Torrent, Wockhardt, Zydus Cadila, Cadila Pharma, Lupin, Sun Pharma, Cipla, Nicholas Piramal, US Vitamins, Orchid, Aurobindo, Glenmark, Kopran and Unichem.
- 25 -
Like the US association of PhRMA, 12 of these companies have formed a new association, termed the Indian Pharma Alliance, whose members account for 90% of the total expenditure on new drug research in India. Their total sales top $1 billion, constituting 30% of the exports from India. Within the short period of 5-8 years over half a dozen Investigational New Drug Application (INDA) of these companies have been approved by the Indian drug control authorities in areas as diverse as Benign Prostatic Hyperplasia (BPH), diabetes, microbial and fungal infections, asthma cardiovascular diseases and cancer. Some of these products under development have been licensed out to MNCs such as Novo Nordisk, Novartis, Bayer etc. other Indian companies which also have candidate drugs for development are Dabur, Glenmark and Kopran. The strategy adopted by all these companies has been to initiate discovery programme in chosen therapeutic areas, identity candidate molecules, file international patents and license them to global pharma companies for development and marketing on terms which will include milestone and royalty payments. Examples of success in new drug research in India include the discovery of eight candidate molecules by Dr Reddy’s Laboratories, three for type II diabetes, three for cancer, one each for inflammation and elevated cholesterol and seven from Ranbaxy, of which three are for BPH, two for additions to several new drug delivery systems, including the once daily formulation of Ciprofloxacin licensed to Bayer. While Wockhardt has three biogenetic molecules and two anti-infective in the pipeline, Cipla has been active in developing improved therapy for asthma, cardiac care and oncology, Torrent has in their pipeline, products for hypertension and diabetes, while Glenmark has candidate molecules for respiratory diseases, Kopran for gastro-intestinal disorders and Sun Pharma has a number of drug delivery systems and one product in human trials. Overall, considering the relatively low investments made by India companies, their track record should indeed be considered impressive. Entering Global Generic Markets: The 1970 Indian Patents Act enabled the Indian Companies to master the process technologies for the production of most of the bulk drugs used in formulations. Exports of these products however have been restricted to only countries where there are no valid patents for the products. The new strategies which Indian companies can adopt, include the manufacture and exports of generic drugs, which are outside patents for the global markets. Between 2002 and 2005, drugs currently valued at $40 billion are going off patents, in USA alone. For example, patents on several block-busters such as Prilosec for ulcers ($4bn), Claritine for allergy ($3.4bn) and Neurotin for epilepsy ($1.4bn) are expiring in
- 26 -
2002, Depakote for CNS disorders ($800mn), Accupril for hypertension ($600mn), and Ortho Cyclene for Contraception ($650mn), in 2003, Glucovance for diabetes ($2bn), Flovent for asthma ($1.6bn), Procrit for anemia ($1.5bn) and Diflucan for vaginal candidiasis ($1 bn) in 2004 and in 2005 , Provacid for Ulcer ( $ 3.75 bn ), Zoloft for depression ($3bn) & pravachol for hyper cholesterolemia ($1.7bn). India has the capacity to produce all of these bulk drugs and offer them at competitive for the global generic market. Already the leading companies have made considerable process in this direction, which calls for early approval, of Abbreviated New Drug Applications (ANDAs) to enable companies market the generic products immediately after the product expires, for example, Ranbaxy has over no ANDAs and over 30 drug master files (DMFs) filed in USA $ Europe, Dr. Reddy’s 7&35, Cipla over 40 DMFs, Wockhardt 5 ANDAs & 18 DMFs and Sun pharma 6ANDAs. Marketing strategies have involve direct selling and through subsidiaries as well as through major generic companies, such as Andrx, Ivax, Teva, Par, Warrick etc. the companies have been expediting their ANDAs so that benefit form the exclusivity for 180 days provided for , under the Hatch-Waxman Act is available to them ahead of other major products which have been target several blockbusters such as Fluoxetine, omeprazok, ciprofloxacin amlodipine, setraline, albendazole, metformin, and some of the biotechnology products such as erythropoietin, human insulin and hepatitis is vaccine . Conclusion It is obvious that top ten Indian pharma companies have the potential to become MNCs in the global context, even though in size and available resources, they will be mini MNCs. These companies will have annual sales ranging form $ 400 mn to $1.5 bn by 2010 and will spend 10% of their sales turn over on R&D, bulk of it, on new drug discovery These companies will be to 100 countries & belt them will be able to discover and develop 3 to5 new technology entities per year, out of which two will be relevant to the developing world, they will follow a collaborative mode including licensing co-development and/or marketing of their product with global MNCs. India thus will be the fourth largest pharma force in the world, next only to USA, western Europe and Japan , with around a dozed companies opening in all the major markets of the world.
- 27 -
CHAPTER-4
WTO & ITS IMPACT ON INDIAN PHARMACEUTICAL INDUSTRY
3.1 Impact of Global Regulation on Indian Pharmaceutical Industry
3.2 WTO & Indian Pharmaceutical Industry

- 28 -
Impact of Global Regulation on Indian Pharmaceutical Industry.
Globalization is a process which involves economic inter-dependence of countries world-wide removing all barriers for economic integration as if the whole world is a single village. Obviously, in this process, the rich nations with their superior financial power, control the scenario and the poor and the developing nations are forced to integrate surrendering their economic independence knowing fully well what they are forced to accept is really prejudicial to their own interest. In this process the world financial institutions like the World Bank, IMF and now the WTO advance the interest of the rich countries alone. The draconian policies of the World Bank and the IMF under the structural adjustment programme resulted in the net transfer of $178 billion between 1984 and 1990 from the poor countries to the commercial banks of rich nations. (UNDP Human Development Report, 1994). The Transnational Corporations (TNCs) of the rich nations are practically controlling the world finances. Today, the whole world is colonized by global finance and the TNCs supported by the neo-colonial structure including the World Bank, IMF and WTO are controlling the financial situation world-wide. The governments of third world countries are powerless against global finance and are unable to control its movement within their own national boundaries.
The situation of the world drug industry is no different. 'Operating at the behest of the Pharmaceutical Research and Manufacturers' Association (PhRMA) for a decade and a half, the U.S.Government has waged a ruthless crusade to force third world countries to adopt strait jacketing intellectual property rules at the expense of protecting public health', says the editorial comment in the June 1998 issue of Multinational Monitor, a journal published from Washington.
The structural adjustment programme introduced by the government of India at the behest of the IMF, World Bank and WTO created a serious impact on India's drug industry, health care system, on the workers engaged in the industry and ultimately on the people of the country. These reform policies are mainly the reduced role of the Government, cut in subsidy in the social sector, increase in administered prices, liberalization of trade by increasing tariff rates providing incentives for foreign investment, privatization of the public sector, equating foreign companies with Indian companies, de-regulating the labour market etc. This is aimed at the withdrawal of the state initiative from the social and welfare sectors like health, education, public distribution etc.
In this article I shall try to show how the workers of the drug industry and the people of our country are affected by the impact of globalization.
Drug industry situation prior to the Indian Patent Act, 1970
At the time of independence, the total drug production in our country was around Rs. 10 crores. At that time the MNCs taking the help of the colonial Patent and Designs Act, 1911 exploited the drug market of our country. They were engaged mainly in the import
- 29 -
of drugs from their country of origin. Between 1947-57, 99% of the 1704 drugs and pharmaceutical patents in India were held by foreign MNCs. During that time the MNCs who were controlling 80% of the market did not come forward with financial investment and technological help to establish drug production centers in India. Drug prices in India were amongst the highest in the world. In 1954, the first public sector drug company Hindustan Antibiotic Ltd. (HAL) was established with the help of WHO and UNICEF. The Indian Drugs and Pharmaceutical Limited (IDPL) was established in 1961 with help from the Soviet Union. The establishment of these two public sector units and the coming into force of the Drug Policy of 1978 had been mainly responsible for the availability of drugs and medicines at relatively lower prices in India. The country became almost self-sufficient in the production of drugs.
Indian Patent Act 1970
The Patent Bill was first introduced in Parliament in 1967, but the Patent Act, 1970 came into force only in 1972. The Indian Patent Act 1970 which is in operation in our country does not allow product patents on medicines, agricultural products and atomic energy. This is the most suitable patent act for the developing world. Here, process patents are allowed for 5-7 years. Mainly with the help of the Indian Patent Act 1970 India is today self-sufficient in the production of basic drugs covering various groups of drugs. Indian scientists developed new processes for 107 drugs. Indian companies are now among the world leaders in the production of bulk drugs from basic stages. At present, the prices of drugs in India are comparatively cheaper than many other countries. As per UNIDO, India is identified to produce its own drug needs with its own technology and manpower indigenously. After 1970, many new drug firms were established by Indian businessmen. At present, around 23 thousand small, big, and medium factories are producing drugs in India.
Attempts to change the Indian Patent Act 1970 are a part of this globalization programme. The imposition of an unequal trade treaty like the World Trade Organization (WTO) is a step towards globalization in favour of the MNCs of rich nations. With its help, the market of the developing nations is forced open for the developed countries. Most of the developing countries were forced to sign the WTO agreement without realizing its implication: as a result, the developed countries are the gainers. Already, at the dictates of the IMF, World Bank and WTO, the Government of India is slackening all checks and controls to invite the MNCs in all industries including the pharmaceutical industry. FERA and MRTP Acts have been amended. Customs duties and corporate taxes have been lowered. Relief, concessions and facilities have been extended to the MNCs as to Indian companies. All these, already, had an adverse impact on the indigenous drug industry. As per the requirement of WTO guidelines for the product patent regime, the availability of new drugs in our country may be delayed depending on the desire of the patent holders. As per the guidelines, a product patent is granted for 20 years and a process patent for another 20 years. At present, newer drugs are made available in our country within a 4-6 years period. Prices of drugs will go up by 5 to 10 times as it is evident from the prices of drugs in India and other countries like Pakistan, U.K. and U.S.A. where product patents are in force. Ranitidine is sold by Glaxo in India at Rs.

- 30 -
7.20. The same product is sold by the same company in Pakistan at Rs. 65 and in the U.S.A. at Rs. 545. Similarly, the anti-viral drug Aciclovir costs Rs. 33.75 in India while the same drug is sold in Pakistan at Rs. 363. There are many such examples. The drug prices in the U.S.A., U.K. and other developed countries have gone up so high that the health care expenditure in those countries is predominantly funded by insurance companies at a very high premium. In those countries people cannot think of treatment without insurance coverage. Product patent regime will definitely hamper India's drugs exports as countries will be forced to purchase from patent holders only.
Dilution of Drug Policy and Drug Price Increase
Unlike consumer goods, drugs are not purchased by the preference of a person, but on a doctors' prescription. Consumers have no choice of their own on this matter.
Prices of drugs are increasing by leaps and bounds along with the prices of other commodities in recent times. The drug manufacturers are flouting the Drug Price Control Order (DPCO). The DPCO was first introduced in 1970. In 1970 most of the drugs were under price control. In 1987 this was diluted and the number of drugs which were restricted declined to 347, in 1987 it was brought down to 163 drugs and in 1994 only 73 drugs were under DPCO. Even then industry is not happy; they want the control to be abolished totally. They have already demanded decontrol of 17 bulk drugs and further recommended full decontrol within 3 years time (Economic Times, 28th September, 1998). Many developed countries of Europe control drug prices directly. In the U.K., the government determines the profit level of drugs supplied by individual companies. A company has to reimburse excess profits to the Department of Health.
A recent study shows that the prices of many life-saving bulk drugs have gone up steeply. Drugs policies in our country are decided not by the need of our people, the pattern of diseases or by the purchasing capacity of the people, but by the profit motive of the industry and the Central Government are playing the role of a silent onlooker.
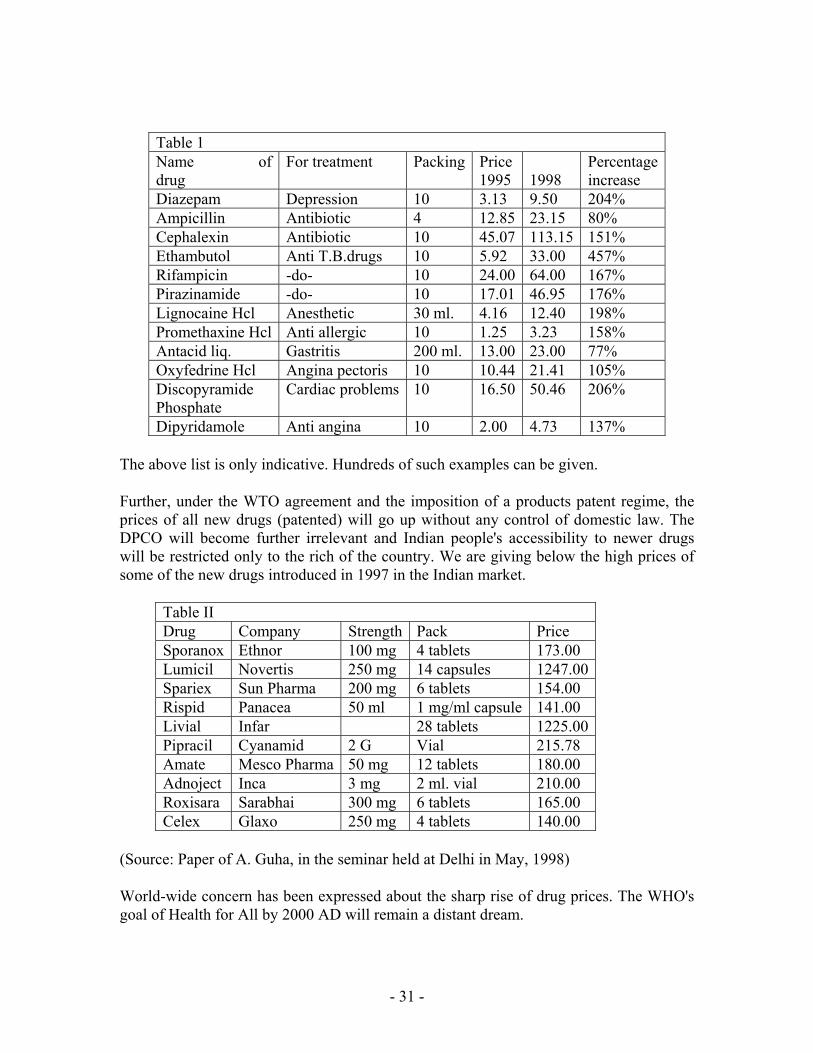
We are giving below the prices of twelve essential drugs before the liberal decontrol of DPCO in 1995 and today.
- 31 -
Table 1 Name of drug
For treatment Packing Price1995
1998
Percentageincrease
Diazepam Depression 10 3.13 9.50 204% Ampicillin Antibiotic 4 12.85 23.15 80% Cephalexin Antibiotic 10 45.07 113.15 151% Ethambutol Anti T.B.drugs 10 5.92 33.00 457% Rifampicin -do- 10 24.00 64.00 167% Pirazinamide -do- 10 17.01 46.95 176% Lignocaine Hcl Anesthetic 30 ml. 4.16 12.40 198% Promethaxine Hcl Anti allergic 10 1.25 3.23 158% Antacid liq. Gastritis 200 ml. 13.00 23.00 77% Oxyfedrine Hcl Angina pectoris 10 10.44 21.41 105% Discopyramide Phosphate
Cardiac problems 10 16.50 50.46 206%
Dipyridamole Anti angina 10 2.00 4.73 137%
The above list is only indicative. Hundreds of such examples can be given.
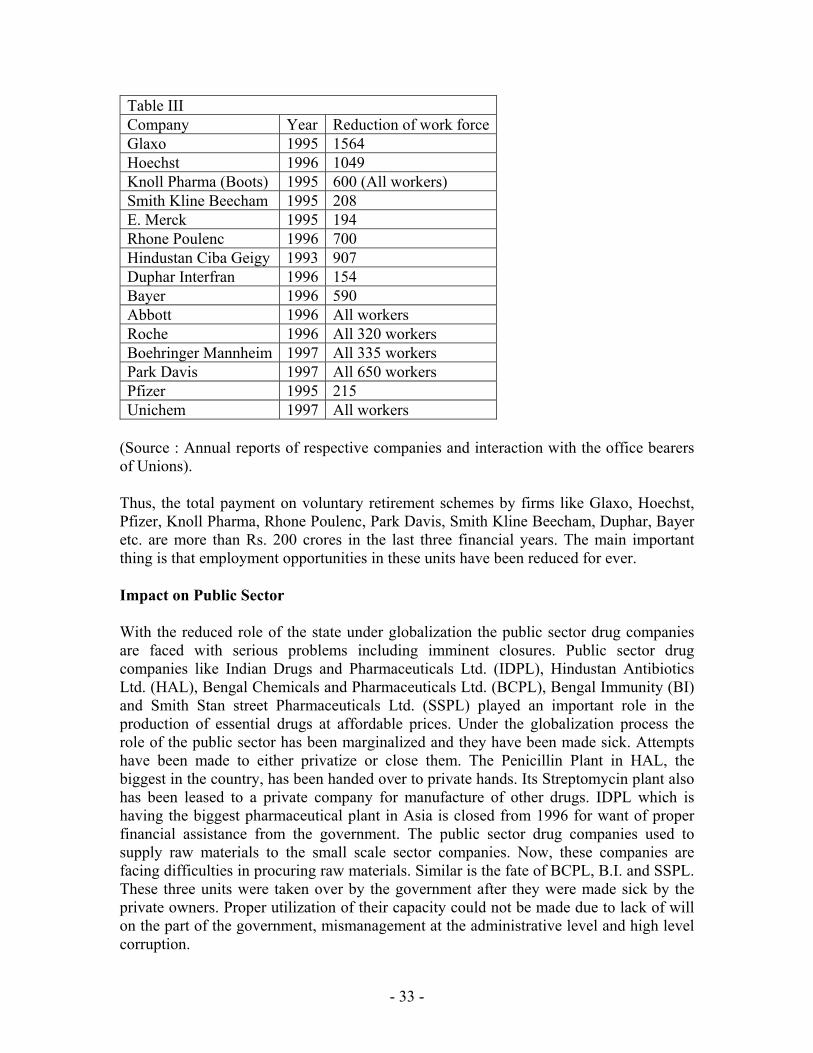
Further, under the WTO agreement and the imposition of a products patent regime, the prices of all new drugs (patented) will go up without any control of domestic law. The DPCO will become further irrelevant and Indian people's accessibility to newer drugs will be restricted only to the rich of the country. We are giving below the high prices of some of the new drugs introduced in 1997 in the Indian market.
Table II Drug Company Strength Pack Price Sporanox Ethnor 100 mg 4 tablets 173.00 Lumicil Novertis 250 mg 14 capsules 1247.00 Spariex Sun Pharma 200 mg 6 tablets 154.00 Rispid Panacea 50 ml 1 mg/ml capsule 141.00 Livial Infar 28 tablets 1225.00 Pipracil Cyanamid 2 G Vial 215.78 Amate Mesco Pharma 50 mg 12 tablets 180.00 Adnoject Inca 3 mg 2 ml. vial 210.00 Roxisara Sarabhai 300 mg 6 tablets 165.00 Celex Glaxo 250 mg 4 tablets 140.00
(Source: Paper of A. Guha, in the seminar held at Delhi in May, 1998)
World-wide concern has been expressed about the sharp rise of drug prices. The WHO's goal of Health for All by 2000 AD will remain a distant dream.

- 32 -
Moreover, with the rapid development in technology, a greater number of new drugs are being introduced. Experts say that very few of them are having therapeutic advantages over the existing drugs. 'Out of 348 new drugs introduced by 25 big US companies during 1981 to 1988 only 3 per cent made important potential contribution while 84 percent made little or no potential contribution' said the US federal authority. Hence the introduction of new costly drugs should be properly monitored by the central government.
Mass Ending of Jobs
With the reduction of the customs duties on foreign imports many drugs manufactured in India have become unviable compared to the foreign goods in the Indian market. As a result, the owner of these factories are closing down their units and throwing the workers out of employment. Messrs. Boehringer Mannheim, and Parks Davis who were the lone producers of Chloramphenicol in India stopped their production as its prices in the international market were cheaper than the cost of production in India. M/s. Sarabhai Chemicals closed their Vitamin 'C' plant for a similar reason. Like Chloramphenicol and vitamin 'C' many other drugs like Paracetamol, Metronidazole, Ampicillin, Amoxycillin etc. are available at a cheaper price in our country from abroad because of the lowering of the customs duties so that Indian factories have closed and workers are on the streets. For the above drugs our country has became dependent on foreign supply.
In their attempt to shift the production to the third party manufacturing already, Hindustan Ciba Geigy, Roche, Abbot, Boehringer Mannheim, Boots, Park Davis, Unichem etc. have closed their factories and offered a voluntary retiring scheme to workers and they have sold the land of their factory premises at a premium price. Apart from these closures, Pfizer, Rhone Poulenc, Hoechst, Glaxo etc. have reduced their work force. Crores of rupees have been spent to give VRS. These companies are manufacturing their products with the help of loan licensees. Some of the companies have opened new smaller factories in new places and appointed workers with lower wages and more workload. More casual workers are being appointed. In the last two years in the Mumbai Thane region of Maharashtra around 30,000 workers have lost their jobs in the pharmaceutical industry.
Apart from the factory workers the distribution workers are gradually being replaced by Cost & Freight agency system. In this system, the original company does not have any responsibility for the workers. They are employed by agents with more workload and lower wages. In the last decade around 15 thousand distribution workers have lost their jobs in the pharmaceutical industry. Moreover, through the agency system the Government is deprived of sales tax.
In marketing also the field workers or the sales promotion employees are facing tremendous attacks in the name of franchise, co-marketing, appointment of communicators etc. many permanent sales promotion employees are losing their jobs. Many others are appointed in the name of so-called executives to remove them from the fold of the union. More casual and contractual workers are being recruited.
- 33 -
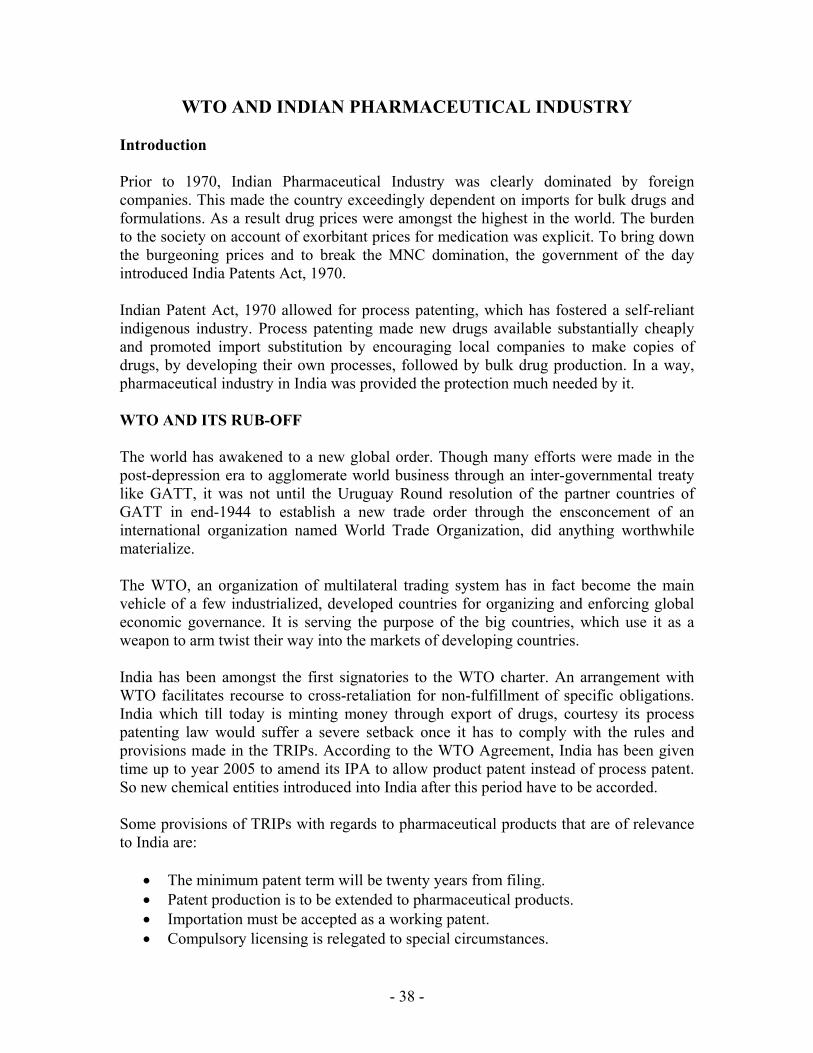
Table III Company Year Reduction of work forceGlaxo 1995 1564 Hoechst 1996 1049 Knoll Pharma (Boots) 1995 600 (All workers) Smith Kline Beecham 1995 208 E. Merck 1995 194 Rhone Poulenc 1996 700 Hindustan Ciba Geigy 1993 907 Duphar Interfran 1996 154 Bayer 1996 590 Abbott 1996 All workers Roche 1996 All 320 workers Boehringer Mannheim 1997 All 335 workers Park Davis 1997 All 650 workers Pfizer 1995 215 Unichem 1997 All workers
(Source : Annual reports of respective companies and interaction with the office bearers of Unions).
Thus, the total payment on voluntary retirement schemes by firms like Glaxo, Hoechst, Pfizer, Knoll Pharma, Rhone Poulenc, Park Davis, Smith Kline Beecham, Duphar, Bayer etc. are more than Rs. 200 crores in the last three financial years. The main important thing is that employment opportunities in these units have been reduced for ever.
Impact on Public Sector
With the reduced role of the state under globalization the public sector drug companies are faced with serious problems including imminent closures. Public sector drug companies like Indian Drugs and Pharmaceuticals Ltd. (IDPL), Hindustan Antibiotics Ltd. (HAL), Bengal Chemicals and Pharmaceuticals Ltd. (BCPL), Bengal Immunity (BI) and Smith Stan street Pharmaceuticals Ltd. (SSPL) played an important role in the production of essential drugs at affordable prices. Under the globalization process the role of the public sector has been marginalized and they have been made sick. Attempts have been made to either privatize or close them. The Penicillin Plant in HAL, the biggest in the country, has been handed over to private hands. Its Streptomycin plant also has been leased to a private company for manufacture of other drugs. IDPL which is having the biggest pharmaceutical plant in Asia is closed from 1996 for want of proper financial assistance from the government. The public sector drug companies used to supply raw materials to the small scale sector companies. Now, these companies are facing difficulties in procuring raw materials. Similar is the fate of BCPL, B.I. and SSPL. These three units were taken over by the government after they were made sick by the private owners. Proper utilization of their capacity could not be made due to lack of will on the part of the government, mismanagement at the administrative level and high level corruption.

- 34 -
It is not because of any inherent weakness but due to the lack of political will, deliberate efforts to destroy them, corruption and mismanagement that these public sector units have been rendered commercially unviable.
Moreover, the number of workers engaged in these units have been reduced drastically. When IDPL was established it had a strength of more than 15,000 workers. Today, it has been reduced to less than 7,000.
With the pharmaceutical industry taking a leap towards biotechnology development world-wide, only the public sector drug companies, with the backing of the Central Government, could have faced the challenge effectively from the MNCs in the new situation.

- 35 -
Mergers and Acquisitions
International and national level mergers, acquisitions and takeovers have now become a common phenomenon in the pharmaceutical industry. Internationally American Home Product merged with Cyanamid, SKB with Sterling, Rhone Poulenc took over Fashions, BSF with Boots, Glaxo with Burroughs Welcome, Ciba Geigy with Sandoz, Warner Hindustan with Parke Davis, Hoechst with Rhone Poulenc etc. are some of the examples of big take over. By mergers and acquisitions these companies became even larger with more financial power at their disposal over their competitors. (See Table IV for the top pharmaceuticals of the world).
In coming days, with the help of international financial companies the MNCs will capture and take control of Indian companies to control the Indian market.
To match the situation created by international mergers and takeovers, Indian companies are adopting the same path. For example Wockhardt took over Merind and Tata Pharma, Ranbaxy took over Croslands, Nicholas Piramal took over Roche, Boehringer, Sumitra Pharma. The inevitable results are job loss of workers. Because of overlapping of jobs large numbers of workers are declared surplus. After merger Glaxo-Welcome and Ciba-Sandoz announced a reduction of 15 thousand and 10 thousand of their work force respectively world-wide. Upjohn and Pharmacia decided to close 24 of their 57 plants in different countries after their merger.
Some countries are adopting the 'buy and grow' method. They are taking over some popular brands and increasing their business. SKB took over Crocin from Duphar, Ranbaxy took over 7 leading brands from Gufic, Dr. Reddy's Lab purchased 6 products of Dolphin and two each from Pfimex and SOL Pharma. Sun pharma purchased all leading brands of NATCO, after selling the popular brands the companies are becoming sick and closing their shutters throwing the workers on the street.
The governments permission to the MNCs to come to India with 100% equity have threatened the existing companies with the same origin and their workers.
Through the process of mergers, acquisitions and takeovers MNCs will gradually perpetuate their grip on the Indian industry by the creation of a limited number of mega companies having monopoly control and domination world wide. In the absence of competition people will have to pay any price as it happens in the sellers market.

- 36 -
CONCLUSION
The present government at the centre is bringing a bill in the winter session of Parliament to change the Indian Patent Act 1970. The change in the Act is not in the interest of the people of the country. Now patents have become an object of business instead of development. Considering the wide gap of industrial and technological development between developed and developing countries monopoly rights through the patent system should not be allowed to the rich nations. Today 85% of the patents are being controlled by the TNCs of the rich nations. 'Globalization is hurting poor people, not just the poor countries. In this process poor countries and poor people will become increasingly marginalized', says the 1997 world development report of UNDP.
The question is why this pressure and hurry? The main aim is to impose the conditionalities of WTO and to change the Indian Patent Act as MNCs need more markets and are eyeing Asia which is the largest continent of the world where 60% of the world population lives but contributes only 20% of the world pharmaceuticals business. With a high rate of population growth it is expected that the need of drugs will tremendously increase in the third world countries including India in the next millennium. India contributes 16.1% of the world population, but it produces only 1.2% of world drug production (See Table V). Hence the MNCs are trying to have more control over the pharmaceutical markets of the developing nations.
Developed countries are backing their own big companies to capture markets in other countries even at the cost of the interest of the people there. The United States has successfully battled for the inclusion of strict intellectual property rules in international trade agreements such as NAFTA and GATT. Often the U.S. position has literally been drafted by PhRMA. These trade agreements disregard public health considerations and have forced dramatic changes in the intellectual property rules the world over. Still PhRMA is not satisfied. And when PhRMA is not happy the office of U.S. Trade Representative (USTR) is not happy, says the editorial comment of Multinational Monitor.
The above comments clearly indicate the intention of the USA and other rich nations. Unfortunately, the Government of India is dancing to their tune. Against this, it is necessary to develop and launch broad-based movements everywhere with the active support of people hailing from all walks of life to force the government to change their stand.

- 37 -
TableIV Some top pharma company mergers in the world Company Merger Year of
merger Value of merged company
Dow Chemicals Marion Labs 1986 $ 6.21 bn. Bristol Myers Squibb Corp 1989 12.09 bn. Beecham group SmithKline & French 1989 7.9 bn. American Home Products American Cynamide 1994 9.7 bn. Hoffman La Roche Syntex Lab. 1994 5.3 bn. Eli Lyly PCS Health System 1994 4 bn. Sandoz Gerber 1994 3.7 bn. Smith Kline Beecham Sterling 1994 2.9 bn. Glaxo Burroughs Wellcome 1995 14.2 bn. Hoechst MMD Roussel 1995 7.2 bn. Pharmacia Upjohn 1995 7 bn. Rhone-Poulenc Rorers Fison 1995 2.7 bn. BASF Boots 1995 1.3 bn. Ciba Geigy Sandoz 1996 30.1 bn. Hoffman la Roche Comage Ltd. 1997 11 bn. Hoechst A.G. Rhone Poulenc 1998 Astra Zeneca 1998 67 bn.
(Source: Compilation from reports published in various news papers at different times)
Table:5 Percentage of drug production and world population in some countries Country % of world
drug production % of world population
USA 28.2% 4.7% Germany 7.7% 1.5% France 7.1% 1.1% U.K. 3.4% 1.1% Brazil 1.7% 2.8% India 1.2% 16.1%
(Source : Business Standard, February 19, 1997)
- 38 -
WTO AND INDIAN PHARMACEUTICAL INDUSTRY
Introduction Prior to 1970, Indian Pharmaceutical Industry was clearly dominated by foreign companies. This made the country exceedingly dependent on imports for bulk drugs and formulations. As a result drug prices were amongst the highest in the world. The burden to the society on account of exorbitant prices for medication was explicit. To bring down the burgeoning prices and to break the MNC domination, the government of the day introduced India Patents Act, 1970. Indian Patent Act, 1970 allowed for process patenting, which has fostered a self-reliant indigenous industry. Process patenting made new drugs available substantially cheaply and promoted import substitution by encouraging local companies to make copies of drugs, by developing their own processes, followed by bulk drug production. In a way, pharmaceutical industry in India was provided the protection much needed by it. WTO AND ITS RUB-OFF The world has awakened to a new global order. Though many efforts were made in the post-depression era to agglomerate world business through an inter-governmental treaty like GATT, it was not until the Uruguay Round resolution of the partner countries of GATT in end-1944 to establish a new trade order through the ensconcement of an international organization named World Trade Organization, did anything worthwhile materialize. The WTO, an organization of multilateral trading system has in fact become the main vehicle of a few industrialized, developed countries for organizing and enforcing global economic governance. It is serving the purpose of the big countries, which use it as a weapon to arm twist their way into the markets of developing countries. India has been amongst the first signatories to the WTO charter. An arrangement with WTO facilitates recourse to cross-retaliation for non-fulfillment of specific obligations. India which till today is minting money through export of drugs, courtesy its process patenting law would suffer a severe setback once it has to comply with the rules and provisions made in the TRIPs. According to the WTO Agreement, India has been given time up to year 2005 to amend its IPA to allow product patent instead of process patent. So new chemical entities introduced into India after this period have to be accorded. Some provisions of TRIPs with regards to pharmaceutical products that are of relevance to India are:
• The minimum patent term will be twenty years from filing. • Patent production is to be extended to pharmaceutical products. • Importation must be accepted as a working patent. • Compulsory licensing is relegated to special circumstances.

- 39 -
• In infringement suits over process patents, the ‘burden of proof’ is reversed. • Provide transitional arrangements – deferment of the acceptance of
pharmaceutical product patents by developing countries for ten years. • Limited exclusively is granted to developing countries for pharmaceutical
products whose patent applications are filed after the enforcement of the TRIPs agreement.
EMR ROUTE The EMR route is a backdoor method of granting monopoly rights. To ensure a smooth transition from process patent regime to a product patent one, WTO has granted India a grace period of ten years. During this period, all patent applications received by her would be put in a ‘black box’ for further future consideration. However, in the interim, pharmaceutical companies can apply for exclusive marketing rights (EMRs) for their products for a period of five years, even before India’s transition is fully phased. Any company that has been registered for a patent and has received marketing rights in any of the WTO member countries can avail the EMR route in India. EMR’S IMPLICATION A mere grant of a patent and exclusive marketing rights by any member country would automatically qualify a company to avail EMR in India for that product, for a minimum period of five years. This clause has a very serious implication. The company in question can happily experiment with the lives of poor Indians. If their experiment fails, the drug can be withdrawn and in the process endangering the lives of millions of Indians. However, if the drug proves successful, given the provision of the validity of a patent for twenty years, the company can take in enormous monopoly profits. THE CURRENT SCENARIO There are as many as 23,000 pharmaceutical firms in India, engaged in the production of 16,000 formulation and 700 bulk drugs. With over 28.60 lakhs of manpower employed in the sector, it is growing drastically. The year India became a member signatory of WTO, in 1995 its investment in pharmaceutical industry was Rs. 1380 crores in 1999-2000. These two indicators are proof enough to exhibit the panic in the industry. The industry is growing by leaps and bounds to ensure that post 2005 it takes on its TNC competitors head on. Individual companies like Ranbaxy, Dr. Reddy’s Laboratories, Cipla, Dabur, Aurobindo Pharma, Orchid Chemicals and others are setting the pace and defining industry standard. Ranbaxy with its presence in 40 countries, with operations in 24 and manufacturing facilities in 6 countries, with 7000 people across the globe is the harbinger of the coming of the age of the Indian industry. Incidentally it spends double the industry standards on its R & D efforts.
- 40 -
Capital expenditure of the tune of millions is being incurred by the industry to modernize plants and machinery. Global marketing alliance, mergers and acquisitions have taken the industry by storm. Some companies like Cipla are examining their future role in path-breaking areas of research such as genetics, hoping to open up unexplored venues of global alliance for the introduction of new therapeutic agents. DRL and Ranbaxy are doing collaborative work with companies such as Novo-Novordis and Bayer. Path-breaking work on agronomy and scientific development of traditional medicines is on. Companies are focusing on securing international patents for new processes, for novel drug delivery systems and innovative drug formulations. Indian pharmaceutical industry is growing at the rate of 12-15% per year as against the global industry growth rate of 8%. This can be attributed to healthcare cost-containment pressures, keeping pharmaceutical prices low, while export opportunities and low domestic per capita consumption have provided higher growth potential. Exports were 192% higher than imports in the year 1999-2000. annual drug per capita expenditure is only $3 as compared to Japan’s $412, Germany’s $222, United States’ 191, Canada’s $124 and United Kingdom’s $97. The pharmaceutical sector has undergone several policy changes in the past two years. It has largely benefited from the budget proposals made by the government. Some of the positive steps taken by the government apropos of, the industry are :
• Pharmaceutical industry has been recognized as a knowledge-based industry. • The government has plans to step up the R&D expenditure. Ironically, only 4.3%
of the projected Rs 1400 crores proposed investment in R&D as in the ninth five year plan has been made. Given a year’s time from now for the 5 year plan to give way to the tenth five year plan, this plan seems quite overdue.
• Rationalization of excise duty and reduction in interest rates in export financing. • Additional deductions under income tax laws for R&D expense. • Foreign direct investment permit up to 74% through automatic rout under powers
delegated to the RBI of by the government as the case may be. Automatic route for FDI and /of for technology collaboration would not be available to those who have had any previous joint venture of technology transfer / trademark agreement in the same of allied field in India.
PRE 2005 The phase of transition has taken over. Established national pharmaceutical majors are gobbling up smaller companies through consolidations, acquisitions and mergers. The very notion of the entry of TNCs into India post WTO has propped up Indian firms to follow the dictum: United we stand, Divided we fall. Consolidations have become a buzzword in the industry. Smaller players unable to bear the brunt of heavy competition are giving up to larger ones. With only three odd years in hand, Indian pharmaceutical firms are losing no time in extensive copying to reap full advantage of the laxity in the current policy, copying
- 41 -
though a cheap practice, yet given the policy of price control, Pharma firms are left with no option to invest in research and development . Price control is a non incentive for innovation. Lower drug prices might also imply increasing healthcare expenditure. On the one hand where global giants like Novartis and Hoechst have already set up 100% Indian subsidiaries, some are increasing their stakes in existing ventures and some restructuring their operations. Quite contrary to these optimists are some pessimists who still linger with the rear that their top of the line products would find no ready market in India given the amount of piracy and low product prices. Companies are increasingly investing in riskier, cutting edge technologies. SmithKline Beecham is one of the first such companies to leap into new technologies. Glaxo is also contemplating to develop broader portfolio of drugs. Indian pharmaceutical companies are in the process of building a strong distribution network and manufacturing facilities so that they can be in a better position to attract foreign partners post WTO. Also the would leverage their bargaining power. POST 2005 Indian pharmaceutical industry would be have to confront the reality of the implementations of TRIPs Agreement from the year 2005. The year would be a turning point, a defining one in India’s pharmaceutical trade. Post-2005 period would be characterized by many hectic business changes. Most transnational companies are likely to introduce there new-patented drug once the product patent becomes fully operational. Indian pharmaceutical would try to haggle with them and government might introduce compulsory licensing. This would lead to an increase in the bargaining power of the patent holder. Also it is likely that TNCs might not set up base in India but consider it as an assembly point of some drugs manufactured by them. However, new launches in the post –WTO period is a guaranteed fact. These new launches would primarily be high margin, low volume products. Competition is likely to increase in the domestic market due to due to the entry of transnational companies. This would whittle down many manufacturers and small and medium enterprises would slowly decimate. They would lose the benefits enjoyed so far and forced to compete with the foreign firms. Not only would they lose their significance, and their existence would be jeopardized with the implementation of the TRIPs agreement. The product sales of foreign transnational companies would increase at the expense of the local layers. Local players would increase their research and development expenditures and try to expand their business overseas to enter the generic market due to their cost efficiency. Imitation is cheaper then innovation. Post-2005, drug discovery would be a costlier affair that Indian pharma companies cannot afford. Joint ventures would become the order of the day. Prizes of drugs would shoot high. IPR rules would enable TCNs to jack up prizes of their products far beyond cost and earn monopoly rents and profits. Higher prices would mean higher cost on medicament. This would lead to

- 42 -
social chaos. People of a developing country like India can ill- afford to buy drugs, which are far beyond their reach. Social healthcare system would collapse. Only a pro-active intervention by the government can save the life of millions. Masses would keep on going for the older, cheaper versions of the products, provided they are available, leaving the higher priced newer products. This is what I would term as ‘patient’s paradox’. The patient can neither afford highly effective, high priced products nor do the cheaper drugs help him in faster recovery. Though money spent on cheaper drug would be more, yet the patient is not burden, for his payment is made in phases quite convenient to him. More expensive drug may faster recovery, possibly eliminating future hospitalization and hence on the whole it may prove cost effective too. Merger and joint venture would to less in jobs. Downsizing would be a card game to the pharma majors. Downsizing has its own implications. Society will have to bear the cost of unemployment. Effective demand would come down as result of survivors would be beset with problems like depression, fear of change, loss of loyalty minimum job requirements. Fear of bearing sacked would haunt their beleaguered minds and as a result their personal lives would be jeopardizes. Due to stringency in laws, counterfeit markets would evolve, product diversion practices would prosper and also there would be a splurge in counterfeit labeling practices. On the brighter side, in the next 8 years an estimated 60 major pharma products in excess of $ 40 billion will lose patent protection, This will foster a robust growth in the generic bulk drugs and formulation industry. India has the advantage of lower manufacturing and manpower costs. Moreover, reverse engineered drugs even while under even while under patent would help Indian pharmaceutical manufacturers to target the first wave of generic competition to hit the market in developed nations when the drug goes off patent. WHAT SHOULD THE GOVERNMENT DO? Since India has been a signatory to WTO it cannot come out of it as and when it wishes, It is bound by the rules and regulations of the multilateral trading body, Non fulfillment of the objectives set out by WTO in TRIPs agreement would invite cross retaliation in trade, Hence, it is advisable that apropos of , post WTO scenario, the government should adopt a proactive approach, taking full advantage of the leniency set out in a few articles of the TRIPs agreement. Article 8 and Article 30 are such ones, which would provide the policy makers with recuperative pills to their earlier follies. Article 8 of the TRIPs Agreement states the right of the parties to “ adopt measures necessary to protect public health and nutrition and to promote public interest in sectors of vital importance to their socio- economic and technological development provided that such measures are consistent with the provisions of the agreement” Taking advantage of the provision in this article the government can go for compulsory licensing on the grounds of competition, health and pubic interest. Compulsory licensing
- 43 -
would also allow certain scope for bargaining and pressure. Argentina and Brazil have already adopted this measure without any protest from the WTO. Also India has the discretion of non- granting of patents to a drug if it poses concern to public health. Article 30 provides for some exceptions to the rights conferred, Following are the exceptions, which may be deemed legitimate.
Importation of protected product that has been legitimately put on the market elsewhere. Acts carried out privately on a non- commercial scale or for a non- commercial
purpose. Use of an invention for research and experimentation and for reaching purposes. Preparation of medicines for individual cases according to a prescription. Compulsory licensing. Use of the invention by a third party who started or tool serious precautionary
action, before the application for the patent long before its publication.
The exceptions provided are self explanatory and the government must take maximum advantage of them while framing the pharmaceutical policy. To maintain an effective control the government must verify the international import price of all new drugs before fixing the selling price and promote the use of generic drugs at all levels. Also on all essential drugs, which list is had of by the government, a rigid price control is to be maintained keeping in view the poor affordability by Indian patients of overcharged drugs. A more novel practice would be if the government would purchase all the drugs and them distribute them through its own machinery. Government by dint of its authority and standing can be a good haggler and can procure the drugs at cheaper rates. This would solve the problem of individual affordability. But to do so is no mean task and it would require healthy coffers and a strong political will coupled with business acumen and immaculate diplomacy. OPTIONS OPEN TO BUSINESS In –house and individual research should be done away with. They simply add to the financial burden of the pharma company. Moreover, adept that we are in copying. New drug discovery would take so long a time which companies can ill afford to spend given the dynamic world of open competition. Instead, the scientific resources that we have should be coupled with foreign collaboration to ensure that the speed in the discovery of new drug as well as humanitarian touch is even poised. However, one can in no way discount the abilities of Indian scientists. It is exposure that matters. India should get ready for contract researching. It can take up contracts from contract research organizations that would provide with no-holds barred independent product development base.
- 44 -
Transition from innovation of new process to innovation off new products is a cumbersome task. Pharma companies should step up their R&D expenditure if they are to prove that they are no minnows. Leading firms Ranbaxy, Standard Organics Limited are building capacities to produce generic drugs. All pharma companies should imitate them if they are to grow. The world generic drug market id expected to grow to 40$ billion by 2005 and thereafter its growth is predicted in leaps and bounds. Hence, all off patents drugs are to be produced with equal zest. Since global pharmaceuticals companies do not have much stake in India at present, all efforts should be made to procure licenses from them for production of their patented drugs. This would also help in restricting global majors from entering in to India on a large-scale post-WTO. Companies with large subsidiaries in India like Glaxo, Pfizer are likely to introduce licensed drugs through their subsidiaries only. More focus should be laid on the preventive aspect of disease control while developing new drugs. This would enhance the image of the company in the society. India should take position in developing, producing and exploring tropical drugs, given its traditional medicinal plant base. In this polarized world it would be in the better interests of Indian pharmaceutical industry if it develops South-South cooperation. Finally, the customers on their part should try to cut on the drug pill; rationalize their health spending by using the most cost-effective methods of treatment and try self-medication to avoid paying exorbitant prices.

- 45 -
WTO PATENT LAWS AND THEIR IMPLICATION The world is divided into three categories based on economics and quality of life parameters, the developed, the developing and the least developed countries. The disparities between them are not only in terms of their national products, or per capita incomes, but also on their health and nutritional status. Unfavorable population growth, low literacy levels, poor living conditions and several other factors are often quoted as reasons for the current state of inequalities within the world community. Global issues of environmental degradation, exploitation of limited natural resources, urban migration and alienation of youth are yet other areas of concern to the developed and the developing countries. Their effects on the latter are, however, much more disastrous. In terms of socio-economic and health indicators, India too has shown substantial progress during the last twenty years. Life expectancy for males has moved down from 129 to 72 per 1,000 live births, and population growth from 2.1 to 1.9 per cent. Such progress is far too insignificant and much too slow considering the enormity of the problems that the country faces. Role of the pharmaceutical industry in healthcare was a little over Rs 10 crores, which during the fifty years grew 1,000 fold to Rs 10,000 crores. The industry also evolved through the growth phases, primarily from the status of importing drugs, moving rapidly to re-packing of bulk imports of formulations, to their production, and then to manufacturing of bulk drugs from penultimate intermediates, through relatively simple chemical processes. India is a signatory to the General Agreement on Trader and Tariffs (GATT) agreement which includes Trade Related Intellectual Property Rights (TRIPS). Intellectual Property Rights (IPR) are the rights of the originator of an innovative idea or product which can be registered as trademark, copyright or patent for different categories. The developing countries have been given a ten-year transition period within which they would have to modify their existing laws. The Patent Act, 1970 allows only process patents in the areas of food, pharmaceutical and chemicals. This act was introduced to emphasize self sufficiency in drug production and to save foreign exchange. Three years after a patent was granted anybody is allowed to use the process and pay royalties to the patent holder. A strategy that companies followed was to take a new product that has been patented outside the country, reverse engineer the product and come out with a new production process which would be patented in the country. The company could now sell the product within the country and other countries that have similar patent laws under the new production process for which it owned the process patent. By this method it could avoid paying royalty fees to the company that owned the original product patent.
- 46 -
Under the TRIPS, the Indian pharmaceutical industry would be affected on the following aspects:
1. Implementation of product patents by January 5, 2005. 2. A patent term of 20 years (against the existing term of 7 years in India)
implemented from January 5, 2001.
3. Exclusive marketing rights (EMRs) for a period of 5 years are granted to companies for products that are patented after 1995 and are patented in any other country already.
4. The burden of proof has been shifted from the plaintiff to the defendant during
these years in the case of disputes. This is the reverse of the prevailing mechanism under current Indian patent law.
Around 92 per cent of the existing products are off-patent and any company can compete in this segment. A lot of off-patent equivalents are available to the consumer which will keep the prices of patented drugs down. Many drugs that are currently under patent are expected to go off patent in the next five years. This would provide an opportunity for Indian companies to follow their reverse engineering strategy. However, in the long term, the extension of the patent period would affect the pharma industry adversely as there will not be sufficient products to reverse engineer. Therefore, the company would either have to go for process innovations that would substantially bring down the cost of the patented product so that even after the royalty of the product is paid the product still remains price competitive, or Indian companies will have to increase their focus on research and development of new products. EMRs are granted when the following four criteria are satisfied:
1. Patent application has been filed in India.
2. Patent obtained in another WTO country.
3. Marketing approval obtained in another WTO country.
4. Marketing approval obtained in India. There is no denying the fact that the Patents Act, 1970 was a major watershed in the development of the Indian Pharmaceutical Industry. It is not correct, of course, to say that, the Indian law was unique in this matter. In fact, even prior to the Indian Act, many countries, Brazil, Argentina, Mexico, Turkey, Israel and even Italy and to a lesser extent Spain, Portugal and Canada, not to speak of iron-curtain countries and China, had considerably watered down patent systems for pharmaceutical products. Many of them did not provide any protection at all, whereas India had saved the system by allowing process protection, although for a virtually insignificant period.
- 47 -
The point to note is that even though over 20 countries in the developing and developed belts had poor patent protection for pharmaceuticals, none of them exploited the opportunity to the level that Italy and India did. Therefore, to say that weak patent protection alone was responsible for India’s dramatic growth in this sector in the seventies and eighties is incorrect. Credit should go to the breed of technology support systems provided by leading Indian academic institutions. Thus, the 1970 Patents Act enabled the self-reliant growth of the Indian industry, and the consumers benefited due to market forces and price controls. There also were signals that the approach adopted by the government and industry in the seventies and eighties had major drawbacks. For one, the numbers of companies were in the organized sector whose activities were controlled and monitored by the Central Government. The balance was in the small scale sector under the control of state governments. Even though the Drug Control Agency was responsible for the quality products marketed by all sectors, it was impossible to continuously police over 60,000 packs form 24,000 companies, spread all over the country. Fierce competition ensued and price wars were common, much to the detriment of companies who wanted to invest in expansion, research and development, quality control and national and international marketing efforts. The economic reforms announced in 1991 have often been heralded as an opening of a new chapter for the Indian industry. While in theory, this may indeed be the case, in practice, the impact is still to be seen in any major way, even after a decade. Two major issues connected with the Indian pharmaceutical industry, which coincidentally came up for major changes were reviews on Drug Price Control Order (DPCO), and India becoming a signatory of GATT and a founder member of WTO. India also joined the Paris Convention and signed the Patent Co-operation Treaty (PCT). Reducing the number of drugs under price control enabled many companies to improve their bottom line which had plummeted to as low as four per cent on turnover. For the first time, after many years, the primary and secondary markets for pharmaceutical sector turned bullish, opening up new investment opportunities.

- 48 -
IMPACT OF GATT AND WTO India is committed to implementing a full-fledged patent system by January 1, 2005. product patent applications have been accepted from January 1, 1995 and Exclusive Marketing Rights (EMR) are to be granted if the conditions are satisfied. Considering the time frames required for satisfying the conditions, it is unlikely that any drug would qualify for protection under the EMR route. The Indian industry is free to exploit any patents existing or applied for before January 1, 1995 and as such the consumer will not be effected by the exclusive provisions granted under patents for such products. Products for which patent applications have been filed after 1995 and issued on the basis of processing after 2005 will enjoy full protection and those products can be manufactured, marketed or imported only by the patentee, his assignee or licensee. Such exclusivity also gives them the right to price their products as high as market can bear. Prices of patented products would be higher than what would have been, if there was no patent system operative in a country. Prices, however, will not be uniform throughout the world, even for patented products, since companies take into account the buying power of the patients which varies from country to country. They will still be higher than for generic products, since companies rely on the higher margins that patented products can command for funding their research and development for discovery of new drugs. In that situation, what are the options available for developing countries where patients cannot afford the high prices of life-saving drugs, especially, when there are no viable alternatives available. Government subsidies, insurance schemes and in extreme cases, where national interests are at stake, invoking the provisions under administrative controls on prices or even granting of compulsory licenses are some of the options available to developing countries. From a protected economy, a sellers market and political and bureaucratic patronage for conducting business, India during the new millennium will be moving into an era of international competition, lowered tariffs on imports, borderless trade and free markets and global standards for manufacturing and quality of its products. Such a transition would require Indian companies to achieve global scales of operations according to General Medical Practitioner (GMP) standards, competitive levels of technological competence, strong research and development, not only for process development, but also for new drug discovery, global distribution and marketing networks and international collaborations and alliance including joint ventures. The present structure and organization of the Indian pharmaceutical industry was born out of several compulsions in the past. The industry needs to restructure itself to reduce the number of companies through mergers, acquisitions and strategic alliances to ensure minimum economically viable sizes. The small and medium scale operations will be more and more marginalized and will either shut down or merge with the larger players. The role of the remaining units will be as ancillaries for large companies rather than supplying finished products to the market place.
- 49 -
In bulk drug production, wherever logistics and cost considerations favour production in the small scale, they will continue as supply partners. These changes are painful, but imperative in the changed scenario of globalization and international competition that Indian industry faces. It was estimated that Indian domestic market will be around Rs 12,000 crores in 2000 AD, growing annually at the rate of 12-15 per cent at constant prices, which works out to a per capita annual consumption of Rs 120. with higher penetration into the rural market, largely untapped till date and an annual additional population of almost 20 million, it is realistic that by 2005, the turnover at current prices of drugs will be close to Rs 25,000 crores. With an average price increase of atleast 20 per cent during this period, the market will grow to around Rs 30,000 crores. Even with that increase, the prices of drugs in India will be only one-fifth of the international prices. Therefore, in terms of volumes, Indian production will be 10 per cent of the world’s production, placing it in the fifth position after USA, Western Europe, Japan and China. India will thus be one of the major forces in the world, even without taking into account its potential to produce and export generic drugs, drug intermediates and fine chemicals worth an additional Rs 20,000 crores. All in all, an impressive 15 per cent of world’s production for drugs and drug intermediaries could be form India. Four essential ingredients for success in achieving the above objectives are investments to the tune of around Rs 5,000 crores to set up production bases by domestic and international companies would be required; technologies used for production should be state-of-the-art, cost-effective and environment friendly; since one third of the Indian production of bulk drugs and intermediates is estimated for international markets, credible standards of quality need to be established and strong marketing strategies to capture global market shares should be developed. Realizing these objectives should be the prime concern of the Indian pharmaceutical industry in the coming years.
- 50 -
CHAPTER-5
OPPORTUNITIES AND NEW TRENDS IN INDIAN PHARMACEUTICAL INDUSTRY
5.1 Biotechnology.
5.2 Bio-Informatics.
5.3 Phyto biotechnology.
5.4 CRO drivers and challenges.

- 51 -
BIOTECHNOLOGY
According to the economics times of the 10th of October 02, India’s star rising in biotech. Pharmaceutical firma and research look forward to cost effective and high quality research, development and manufacturing of drugs with speed and cost efficiency. Biotechnology revenue is expected to grown five fold to reach $750 million by 2005, rising to 41.5 billion by 2007, with 60% coming form export to the global market. The global bioscience market is poised for significant growth over the next five years, with particular development noted bin the Asia/pacific region. Also the government science provides a great deal of the necessary backbone to develop and deliver innovative technologies, build fast growing and lucrative enterprise, attract international investment and create high additional opportunity for employment. Biotechnological research has a long gestation period. The product development pipeline consist of innovation in basic research resulting in the research leads; evolution of research result; product and process result; involvement of industrial partners or enhanced public investment to take product to the market. Falling in the line with requirements of the product pipeline in the Indian biotechnological enterprise is being systematically develop at the following rate,
Opportunity exists in all this are of biotechnology sector in India. Developing the biotechnology industry in the private sector has seen the rise of the bioenterpreneur in India just as in the rest of the world, but biotechnology has unlike other industries has problem it’s own. It is different form away from other industry because of the following.
• Cost of start up • Other people’s cost • Basic early research based • Time of market • Regulation • Patents • Regulation • Education and emotion
This industry is highly capital intensive industry and the tie to realization is very long. Developing a product and taking it to the market takes a minimum of seven years and depending upon the sector it is addressing. The regulation on biotechnology whether it is research, commercialization and patent protection are still evolving. This are the reasons why as investor in India shies away from biotechnology.

- 52 -
According to recombinant capital if you examine the biotech sectors financing history science 1987, you are all see that three years out of the 15 years have signified the high points:1991, 1996and 2000. However the actual financing windows don’t feet nearly feet in to the December based calendar years: the 1991 window actually spanned about five quarters, from the first quarter of the 1991 through the end of the sector 1992. The 1996 window started in the 1995, and continued through the 1996. And the 2000 windows end to all windows started in the 1999 and continued through the fourth quarter of 2000. Given those statistics, it appears that valleys last 12-13 quarters spread the peaks. If this pattern holds true, we won’t get another window for six more quarters- the beginning of 2004. In fact, deposit the current down cycle – during which the stock price continue to plummet and public offering are the rare occurrence- biotech companies still have to raise an impressive amount of cash. In 2001, that amount to $14.7 billion a steep drop from 2000’s recording –smashing $31.4 billion, but still the second best years in the history. And, in the first six months of 2002, biotech hauled nearly $7.8 billion, slightly more then they did in the first half year of 2001. Even the biotech IPO window is far from open 2002, they contributed 5.4 billion in the new financing to young firms in the US and elsewhere, almost companies around the globe raised slightly less, about $1.7 billion. Although the revenue do not look as brilliant as they did in 2000b they are definitely not bad. Within biotechnology, the first companies return to the health will be those to the products nearest to commercialization. In the meantime, the industry’s fundamentals remain solid: a dance pipeline of late-stage drug candidates, availability of the financial resources to carry those products to the commercialization, strong market and continuing government support. In spite of this dismal scenario the biotechnology sector in India is faring pretty well. According to the CII
• There are 150 BT companies India • 75% of these companies have been established in the last 5 years • The 2002 revenue forecast for BT cos. is $150million. • The export revenues are forecast at $ 60 m. • VC funding has been modest at $20 m. • Total investment to date by biotech companies is $100m. • Employment strength of scientific personal in the BT sector stand at – 15,000
Despite all this there is no denying that it is hard to get fund for a biotech companies and this true not only for India is the scene worldwide. A very fitting remark- by the largely pro-biotech Nuffield report.
- 53 -
As GM crop research is organized at present, the following worst case scenario is all too likely; slow progress in those GM crops that enable poor countries to be self sufficient in food; advances directed at crop quality or management rather than drought tolerance or yield enhancement; emphasis on innovations that save labor cost (for example, herbicide tolerance), rather than those which create productive employment, major yield-enhancing process in developed countries to produce or to substitute for GM crops now imported in conventional (non-GM) form from poor countries. A very general (and necessarily simplified) overview of some of the key characteristics of biotech science is offered here: Methods – Data mining (genomics/bioinformatics), lab and green house trial and error (transgenic). Time-lines – Transgenic work from initial to product, minimum 6 to 8 years (or longer depending on whether working on difficult trial or recalcitrant crop, and regulatory delays). Hardware – Expensive lab equipment and reagents, powerful computers. Personnel/skills – High – MSc, PhD, Post-doc (molecular biology, biophysics, bio-computer modeling etc.) Disciplinary interaction – Computing (bioinformatics/genomics), cloning, transformation, field testing etc. Networks – Across labs, between companies, local-international (particular for proprietary technologies – e.g., gene constructs) Public-private – Most R & D in private sector, or public bodies in US/Europe. But increasing importance of private sector, particularly via MNCs. Funding – External funding essential (DBT, but also international collaboration, often with private sectors/ university partnerships). Intellectual property – Patents (for genes/sequences and processes), plant variety protections (for background material). Regulations – Bio safety issues (import/export, labs/greenhouse, field trials etc) – national and international requirements. According to economical and political Weekly of India figures for R & D expenditure are difficult to come by, but recent estimates of public research effort in ‘modern biology’ in India are in the order of 700 research groups across the countries. Most funding for this comes through the department of science and technology, the department of

- 54 -
biotechnology (DBT) and CSIR. Other funding is channeled by the ministry of agriculture and the ministry of health through various institutes. Estimates of R and D in the private sector are almost impossible to ascertain. Of the big multinational science and biotech companies, based in India have several R and D operations in the country. Monsanto, the major US base biotech company, for example has a R and D sector based on the IISc campus in Bangalore with around 70 scientist active there, and a recent announcement has indicated the prospect of other such centre in Hyderabad. Of the other agricultural focused in India none have such extensive research facilities but all have some degree of local contract research being done in the other biotech are such as pharmaceuticals, big players like Astra Zeneca have long has a presence in India, with a research base in Bangalore. What is important to realized in respect of MNCs is that there R and D research are global in scale, with work being done in the Europe, US, India and else where are a part of internationalized projects. Of the Indian private sector, as well be in the more detail below, there are a verity of agreements, many in tie up alliances agreement with the MNCs with the developed R and D capacities outsides the country. In India addition to the growing area of biotech related contract research being offered by the India companies, some are developing their own R and D capacity. The leading drugs manufacturer in India had biotech R and D capabilities some time, wile investment in biotech by the reliance have caught many peoples attention. But in addition many smaller companies are adding biotech research to their existing portfolio of activities. But we have to remember that generalizations are misleading. There are different types of lab trying to do different types of things with different networks and with different impacts. Disaggregating biotech is therefore an important starting point in any analysis which is attempting to look at patterns and prospects in the biotech sector. In looking at the biotech science in Bangalore, the labs can be classified into broadly four different types: as with all typologies there are problems of overlaps and non-exclusivity, as in many senses the important thing about biotech are the connections made between these groupings – from the public to private, from MNCs to contracts research outfit, from small, local alliance partner to big major, and so on. It is this hybrid nature and network based organization of biotech science and industry that makes it distinct. Table A identifies the case studies which the following reflections are based on.
Type Case studies University/public science Indian institute if science (IIS), National
centres for biological science (NCBS), university of agricultural science (USA).
Start up company Avesthagen, Strand Genomics, Metahelix Establish local company Biocon/Syngene, Rallis Multinational Monsanto, Nunhems-Proagro

- 55 -
By differentiating biotech activities in this way, as shown in table B it is clear how each grouping has different constraints. The degree to which each of this different groupings can deliver biotech products and services which will benefit economy is thus depends on different factors, ranging from public support of research to clarification or regulatory procedures to intellectual property protection to market share dynamics. Just as there is no one biotech science or industry, as a consequence there is no one position in respect of an wild range of public positions. While one can be skeptical of the claims, and question the rather broad definition of bio technology used in this estimates, even if this projections are only partly true, and projections of the international private sector expenditure is factored in, the total investment by commercial sector is likely to exceed that invested by government by several fold even if the DBT, DST and other are successful in that negotiation for public fund in the coming years, they can not hope to garner the resources available in the private sector. This pattern is likely to continue into the future and fundamentally shaped emergence of the biotech sector in India, and its contribution to development. Table B offers a basic typology, which identifies some of the differentiating characteristics of each of these four types.
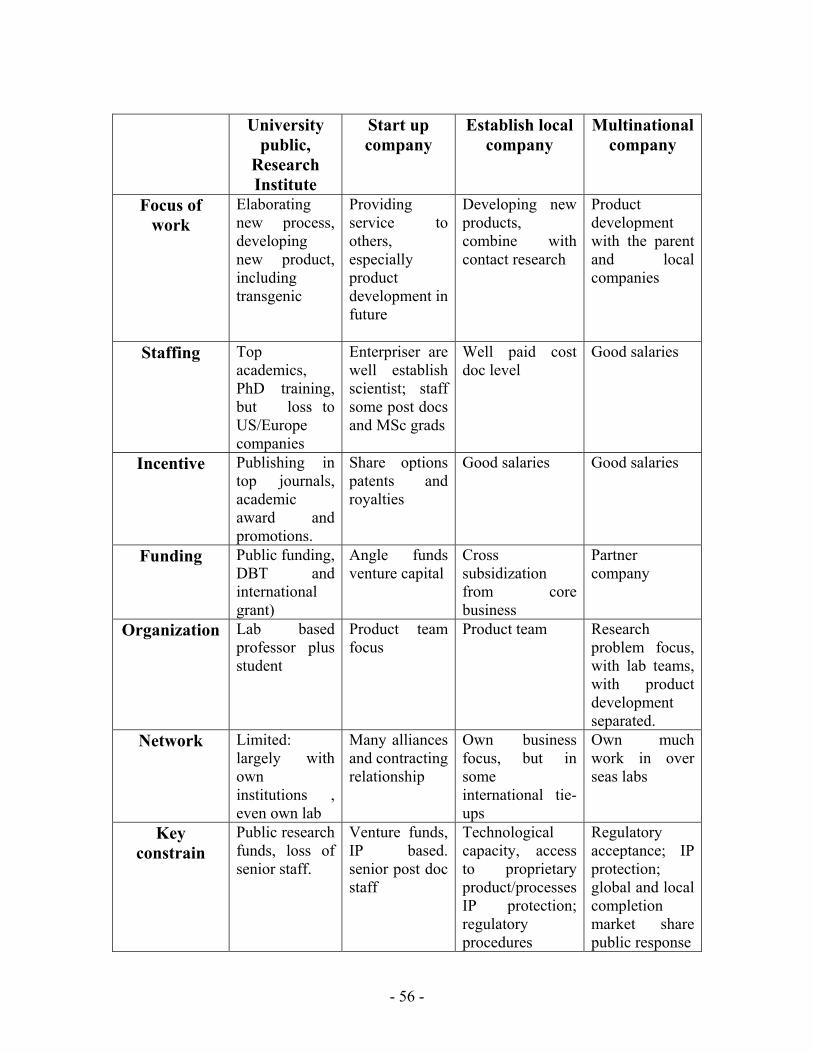
- 56 -
University
public, Research Institute
Start up company
Establish local company
Multinational company
Focus of work
Elaborating new process, developing new product, including transgenic
Providing service to others, especially product development in future
Developing new products, combine with contact research
Product development with the parent and local companies
Staffing Top academics, PhD training, but loss to US/Europe companies
Enterpriser are well establish scientist; staff some post docs and MSc grads
Well paid cost doc level
Good salaries
Incentive Publishing in top journals, academic award and promotions.
Share options patents and royalties
Good salaries Good salaries
Funding Public funding, DBT and international grant)
Angle funds venture capital
Cross subsidization from core business
Partner company
Organization Lab based professor plus student
Product team focus
Product team Research problem focus, with lab teams, with product development separated.
Network Limited: largely with own institutions , even own lab
Many alliances and contracting relationship
Own business focus, but in some international tie-ups
Own much work in over seas labs
Key constrain
Public research funds, loss of senior staff.
Venture funds, IP based. senior post doc staff
Technological capacity, access to proprietary product/processes IP protection; regulatory procedures
Regulatory acceptance; IP protection; global and local completion market share public response

- 57 -
BIOINFORMATICS Bioinformatics: The cutting edge of modern biology Growth of biotechnology has accelerated particularly during the last decade due to accumulation of vast sequence and structure information as a result of sequencing of genomes and solving of crystal structures. This coupled with advances in information technology has made biotechnology increasingly dependent on computationally intensive approaches. This has led to the emergence of a super specialty discipline called bioinformatics. Bioinformatics has become a frontline applied science and is of vital importance to the study of new biology which is widely recognized as the defining scientific endeavor of the twenty-first century. The genomic revolution has underscored the central role of bioinformatics in understanding the very basics of life processes. Advanced beyond the genome project With the completion of sequencing of human genome and a number of other genomes from a variety of organism, the main challenge before the bioinformatician is to analyze and interpret the information. In this regard the following issues are of particular importance:- High Throughput Genome Assembly Annotation Comparative Modeling and assignment of Protein Folds Prediction of Structure, Dynamics and Thermodynamics Advances biotechnological applications e.g. drug design, gene therapy etc System modeling
Applications of Bioinformatics Present day application of Bioinformatics is diverse. It ranges from studies of evolution of life on Earth to generation of designer drugs. Sequence analysis focus upon the finding of new genes analyze structure of the gene to determine its function and correlate how an altered structure of a gene can be linked with diseases. Molecular modeling studies attempts to understand how the three dimensional topography of a protein to its function. Other complex applications include modeling of cell signaling and metabolic pathways, studding protein-protein interaction, understand mechanism how protein families evolve and map the expression pattern of a plethora of genes in different cells and tissues. The Genome databases In the international vista bioinformatics is progressing at an astonishing rate. The major thrust areas seem to be the acquisition of sequence data, incorporating them in form of

- 58 -
classified databases, integrating sequence information with structure data, developing tools for effective data-mining and developing a common platform for resource sharing and integration. In this last area the outcome had been the international Nucleotide Sequence Database Collaboration [INSDC] involving the three major genome databases of the world. GenBank, EMBL and DDBJ. 1. The INSDC comprise of. 2. The taxonomy project – for using a uniform taxonomy for all databases. 3. The feature table-giving shared rules to allow the database to be exchanged among the three organizations. 4. Db_xref qualifier-explicit referencing of specific sequence within the database. 5. Country qualifier-country of origin of the sequence. In order to achieve the multitude of objectives on the global scale, growth of public domain databases have been particularly instrumental. Today we can retrieve an unimaginable amount of information on virtually any aspect of cellular biology from the internet whether it is bibliographic or genomic or structural or even functional. This information acts as the seed data for valuable downstream research. The public domain apart from providing the basic information, also fortunately provides the utilities required for analyzing and interpreting such data. It ranges from multiple sequence alignment to virtual gene expression studies, electronic PCR and so on. The Many Faces of Genome Analysis The availability of genome information provides the bioinformatician with a new set of challenges. This is to analyze the seemingly fragmentary body of knowledge. Currently the predominant areas of bioinformatics data analysis include: Sequence Alignment Studies Prediction of Protein Structure
The two areas have within them the commonalties and differences that one might expect. Sequence Analysis Studies:- Sequence analysis studies are of two major types namely pair wise alignment e.g. one that is experienced through BLAST searches and multiple alignment studies e.g. one experienced with programmes like Clustal. In all cases the idea is to find the similarity or difference between a set of sequences and attempt to infer how they arose and how they are changing. Sequence analysis is an extraordinary tool for studying evolutionary relationships among genomes gene duplication splicing and so on.
- 59 -
Protein Structure Prediction:- Predicting the structure of a protein from the sequence information is one of the most exciting areas of Bioinformatics. The crux of the process lies in the assignment of folds and domains in the primary structure thereby developing an acceptable model of tertiary and quarter nary level structures. Lately, several methods are available e.g. comparative modeling, threading methods, abinitio methods and use of genetic algorithms. Mining From the Genome- In Trail of the Treasure A well-equipped Bioinformatics laboratory in place, the fortunes to follow are stupendous. Euphemistically called genome data mining, the method uses traditional methods like sequence similarity studies, multiple alignment, etc. coupled with more complex developments such as Serial Analysis for Gene Expression (SAGE), electronic PCR, micro array informatics and so on. Some of the areas of application include:
Gene identification Drug Discovery Phylogenomics Detection of genomic markers and polymorphism Understanding gene expression profiles Exploring new metabolic and regulatory pathways Assigning function to unknown ESTs Understanding protein-protein interactions
High Performance Computing-Adding Tooth to a Blunted Knife With the exponential growth of genome information and the need to accomplish quick analysis, the once extraordinary power of serial computation is beginning to falter. Given the present sizes of the known genomes, an operation such as whole genome comparison is likely to take unacceptably long times. This constraint has resulted in the evolution of the concept of parallel computation. Parallelization efficiently scales up the process by cutting down computation time. The Indian side of Bioinformatics India embarked upon major national for Bioinformatics studies. Leading the bandwagon is the Department of Biotechnology’s Biotechnology information Systems of India. Spread –out as a distributed resource across the country with about 61 centers the network is expected to bolster the Indian attempt to harness the deluge of biological information. Other programmes include the High performance Computing Initiatives at the Center for Development of Advanced Computing, Pune where parallel computing is used to address problem of evolutionary biology, large-scale genome comparison and biological system modeling. Super computing facility has been established at IIT Delhi for promotion of in-silico drug development.

- 60 -
The Biotechnology information System Network Structure: The network comprises of 10 Distributed Information Centers (DICs) and 50 Distributed Information Sub-Centers (DISCs). The entire system is headed and coordinated by an Apex Biotechnology Information center at the DBNT Headquarters in New Delhi. Activities: The major activities of Bioinformatics Centers are
To provide a national bioinformation network to cover the diverse areas of the multidisciplinary areas of biotechnology. To develop information resources develop databases information handling tools
and techniques. To establish information linkages with the international organization. To evolve programmes of education and implement human resource development
in Bioinformatics To undertake research and development activities in the field of Bioinformatics.
State-of the Art: Aided by a highly sophisticated communication backbone and six Interactive Graphics Facilities for Molecular modeling, the network has been instrumental in the development of important databases and software. Four long term Advanced Diploma Courses in Bioinformatics at the post M.Sc level is currently operational at Mdurai,Pune,Calcutta and New Delhi for increasing the production of trained personnel in the area. The network also maintains an array of mirror sites of some of the major public domain databases for the benefit of practicing scientists. M.Sc, M-Tech and Ph.D programmes in Bioinformatics have also been introduced recently.
- 61 -
PHYTO BIOTECHNOLOGY Depletion of soil fertility along with modern intensive farming has disturbed the ecological balance leading to economic loss of crop yields and increased pest virulence. Man’s intent to short term gains forced him to chose to synthesize most of the naturally occurring molecules and in the bargain he forgot to look into the long term objective “ Nurturing eco friendly Natural resources” The need of the hour is to protect the environment, humans, animals and crops seem to be only through biotechnology. Biotechnology can provide safer environment, eco friendly and degradable products. Technological break through have paved way for scientific innovations particularly to protect the environment, humans, animals and crops. Biotechnology can double the vigour of crops, increase the valour of animals and modify the fertility status of human beings through gene transformation and clonal modifications. The eco balance of environment acts like a check valve which checks and balances through co-existence of flora and fauna. Unfortunately scientific innovations have disrupted the creative nature. The results out of misuse/abuse of eco balances are un imaginable. Constant usage of synthetic colours, flavors and other taste giving chemical ingredients is producing carcinogenic effect. Break through in biotechnology capabilities could produce, nutraceuticals or other natural molecules. These does not cause alterations in eco system or release any hazardous chemo pollutants. The introduction of natural molecules will form part of the nature and they become eco acceptors or eco rejuvenators. This will enable the eco chain to continue with out a break. The only way to avoid man made calamities is to follow the philosophy of universal eco system and maintenance of good earth. Biotechnology will provide better health and nutrition to the world . The tools of biotechnology will play a major role in increasing crop yield and preserve environment through reduction of chemical use. BIOTECHNOLOGY IN 21ST CENTURY
I) Challenges & opportunities for biotechnology in 21st century: It has been mentioned that the 21st century is the century of biology or of the life sciences. During this century, human life would be expected to change with developments in the biological sciences, which will be made possible by the use of integration of both chemistry& physics with biology. With the fore seeable depletion of fossil fuels and the impending problems o the global environment, the human race has to look into new ways of managing the environment and creating economic wealth in a more sustainable manner.

- 62 -
The many opportunities existing in biotechnology are not devoid of challengers & risks, they are both technological as well as socio economic in nature. The third world countries have rich source of biological material and scientific human resource. But it lacks contemporary, state of the art R&D facilities and financial resources which can only tackle the risks & challenges for 21st century technologies. Hence it is imperative that both developing and developed countries should come together in sharing their strengths so that the out come will be a Win – Win situation.
II) RELEVANCE OF BIO TECHNOLOGY IN INDUSTRY IN 21ST CENTURY:
The dawn of civilization has brought in its wake variety of gifts from mother nature catering to the needs of mankind for food, clothing, shelter, medicine, colours, taste, flavor, decoration etc. Man gainfully exploited many of these products. However, very little was done to maintain & nurture their core value. Green revolution focusing on food production brought in the use of chemical fertilizers & pesticides to boost t production. Whilst boosting the yield & production these inorganic inputs also left behind their residues having harmful effects on animal & environmental health. Health & hygiene have become major concerns world over. Adverse residual impacts of inorganic chemicals have prompted the people to shift to Natural / organic products not only in foods & health care product but also in industrial products such as color, dyes, paints, flavour, perfume, toiletries, packaging, pollution control environment management etc. Eco friendly has almost become an essential prefix in many products of day to day usage in the western world and markets for such products are growing phenomenally. In this environment biotechnology becomes the driver to cater to the changing product needs of day to day utilities of people in the global market place and also find potential solutions for emerging problems concerned with plant / animal & environmental health & hygiene. Biotechnological applications include not only in now famous genetic engineering crops / varieties to suite specific environmental conditions, pest resistance/ tolerance but also in Phyto pharmaceutical, vaccines/ anti bodies, tissue culture. Global bioscience market is also poised for significant growth over the next 5 years. With particular development in Asia pacific region with respective governments focusing on this industry. Countries like India can leverage their knowledge base in biosciences to build globally competitive. India has great potential to develop & market products with low cost high quality research, development & manufacturing. Biotechnology revenue in India is expected to grow 5 folds to reach us$ 750 million by 2005 and us$ 1.5 billion by 2007 with 60% growth coming form exports. IT spending in biosciences is expected to cress $ 138 M in India predominantly in the areas of system cluster, storage, Application software & services. Govt, focus on life sciences would not only provide essential base to develop & deliver innovative products

- 63 -
& technologies but also build fast growing & lucrative enterprises, attract investments and create high value job opportunities. Products enabling market entry, establishment & forward movement to build confidence amongst people concerned ( viz. investors, financiers, employees & business associates of growth) and propel returns ( for reinvestment & business expansion ) aren’t in sight getting marketable products on hand is the need of the hour. Innovation, infrastructure & investments are key drivers for biotech business to prosper. CRITICAL DRIVERS FOR BIOTECH STARTS UPS: Beyond science and money the other drivers encourage development of a biotechnology industry is “a risk taking culture certainly is KEY” The majority of biotech companies lose huge sums of money, and may not achieve profitability for years after incorporation. The loss making impact on the biotech balance sheets and the huge appetite for cap9ital , required the presence of another unique driver to move from start up to the public capital markets where the initial investors are rewarded for their risks and companies have grater opportunities for funding in the us, that driver is NASDAQ, which has made it possible for companies without a track record of net earnings to trade publicly, From the above it is clear that the critical drivers for development of biotechnology are
I) Access to investment capital II) A risk taking culture III) Aggressive technology transfer programmes IV) R&D collaboration between small & medium biotech companies & big
corporate organizations. Biotechnology will always be volatile because the business model requires huge upfront expenses and all or none results. Individual companies may become more stable as they move form single products to portfolios of products. If you analyze the successful biotechnology companies anywhere they share one major similarity i.e. they did not run out of money before they provide their product. Similarly a biotech firm will fail if it cannot continually introduce new and innovative products to the market. UNIQUE TECHNOLOGIES REQUIRED FOR COMMERCIAL ISOLATION OF BIO ACTIVANTS Agri based raw materials are heterogeneous in nature with reference to their physical nature and chemical constituents due to varying agro climatic conditions and the package of Agricultural practices adopted by the cultivators. For e.g. the nicotine content in tobacco leaf varies depending on the nitrogen fertilizer, quantities applied to the crop. Similarly the moisture content and drying on the nitrogen fertilizer, quantities applied to eh crop. Similarly, the moisture content and drying of red chilies in sum will render the produce devoid of the pigment, where as shade drying will retain the pigment. Like wise storage of neem seed with high content of fruit will degrade the neem seed due to heat generation with respect to azadirachtin content.
- 64 -
As any processor has to buy raw materials on whose quality he has no control, it is the technology that adopted plays a major role in over coming these obstacles to produce homogeneous product with consistent quality and cost effectiveness. By Understanding this challenge one has to develop technology for material specific and product specific requirement viz: The primary process, i.e. cleaning, storage. Secondary processing i.e. expelling, grinding, seaving and final processing i.e. extraction, isolation and purification and formulation in a way to over come the challenges of producing homogeneous end products from heterogeneous raw materials ( the steps in processing charges as per the primary product quality and the bio activant we are looking for). Though one may say, that all the final products produced by different processors are the same, in terms of quality, one tends to over look the process technology, the quantity of raw material consumed the yield of the active ingredient with respect to the original concentration available in raw material, the stability of the final product etc. Scientists have significant results through constant R&D effort to over come the above mentioned factors for cost effectiveness. For Example:
1. The storage condition of neem seed are optimized for moisture percentage, fruit content, packaging, aeration, stacking to render a shelf life of 2 year, which other wise is 6 months with respect to the percentage of Azadirachtin.
2. The condition for expelling of neem kernel to get cold pressed neem oil are optimized in such a way, so as to have a stability of one year, which conventional processing is not more than 2 months with respect to lemonoids content in the oil.
3. With reference to various natural products extracts – neem, curcumine, piprine and capsaicin – for isolating bio activants one has to develop a single process common to all these products. This process should require in few inventories of raw materials as against using multiple solvent for each product. This process also enables the use of the single production infrastructure for multiple product production, which save in capital cost as against having multiple plants for multiple product extraction due to process variations.
4. All these process have to be environment friendly, i.e. minimum solvent usage , nil solvent residues, no effluent i.e. no contaminated water requiring treatment is produced, all by products are usable, as feed, fodder or fertilizer etc.
BIOTECH BUSINESS- AN ANALYSIS VIEW OF STATUS & STRATEGIES TO BE ADOPTED FOR SUCCESS Biotechnology / bio informatics – have become industry buzzwords after IT. Many business units have already come up with investments from established companies & entrepreneurs. Business seene: very few ventures have taken off on business front & many are struggling. Finance is the major ingredient for the investment venture was available. However, key success factors & pre requisites of this speciality business viz. marketable

- 65 -
products, technology& competent people to mange the business ventures was questionable. As such, entrepreneurs should quickly take stock of the situation, analyze their business approaches. Identify the grey areas and see how the critical factors for business success could be proactively tackled. Analysis of business Approaches A critical analysis of the industrial units/ companies indicates that in most cases the business was started as a concept with scores of proposals & tons of ideas, which could seldom take a business shape. It is observed that basically there are 3 models of business approaches- to start/ diversify in biotech business for sustained growth viz, (A) project route (B) Product / technology route and(C) investment in existing Biotech R&D companies The pros & cons of each of these models is discussed below:
A) Project Route: It is like the “concept” model. Big business houses/ multinational companies& corporate organizations normally adopt this route to get into this “SUNRISE” industry, consultants & star performers in house, are engaged to prepare a project report with renowned scientist to advice. Remarks: This route is not only time consuming but also calls for appreciable disposition of funds. Lot of time & money goes sown the drain in deciding on technology to be developed/ bought from indigenous / foreign sources which may be “Reinventing the wheel” in reality. Further, no body carries responsibility for the Technology as a mother to child and it may suffer with ‘surrogate mother’ attitude (which may be too wild or soft) As a consequence desired/ targeted results may not come through and the product may be lost in this competitive world. This route is good for “Brick & Mortar” products, but not for knowledge based products organizations to backup.
B) Products/ Technology Route: When “science” becomes industrial reality it’s “Technology”. When concept becomes marketable it’s a “product”. The medium sized companies in a hurry to take full advantage of the market situation may buy the “Product” (for marketing) and “Technology” ( for manufacturing) and gain entry into the new business/ market to cutting short the time lag for entry and establishment success rate of this route is higher than the former, However, gains are of short term as detailed below.

- 66 -
Remarks: Technology vendor charges heavily for his product/ technology and the buyer has to depend on him on a continued basis i.e. either for change in raw material/ ingredient / application etc. Further, the firm could produce only a specific product (from the technology bought) , which may last in the market only until the market interest lasts. Independently, such an enterprise may not be able either to develop new products (with the same technology) or develop new technologies to meet the upcoming challenges I market place. Thus, such units won’t be able to compete with technocrat based biotech companies, which may always have portfolio of precuts in pipeline.
C) Involvement through investment in an existing biotech R&D company route: There are quite a few small scale biotech units who have successfully developed marketable products/ Technologies with limited material resources but highly knowledgeable technocrats of brainpower essential for sustained development & growth of this knowledge business “the biotechnology” What they may require is the financial support either to market the products developed or to double/ triple or quadruple- the success story for other product in pipeline or to strengthen the production base ( with economies of scale ) to mobilize supplies to cater to market demand with cost competitiveness. The investors will be benefit not only with marketable products to start with but also people and portfolio of products in pipeline, for sustained growth. Entrepreneurs who have already invested enough money with people time & effort on their own as in approach a or b would be greatly benefited as the latter would compliment their business mission to tale shape with essential drivers for market entry& establishment but also to scale up their operation 7 propel growth. Thus, it’s the best route for company (be it a multinational/ corporate or private enterprise) with investment interest in biotech R&D business. What it means to the Small scale enterprise Technocrats in Biotech companies slog for long years and toil in product development including a) identification B) isolation C) extraction D) stabilization E) standardization ( of product & process) before coming out with biotech product. Appreciable time, Men & Material are spent along with hard work, sustained efforts and brain power of people concerned in giving birth to “Proven technology ”. Some of them would have even exhausted all their resources in developing a product, identifying markets/ customers christening& establishing a brand.
- 67 -
This is the stage when just returns are likely to be realized for the hard work of biotechnologists and profits have to flow in. If a strong venture capital company/ financial institution or potential multinational/ corporate investors could supports them for spreading the market, diversifying eh product portfolio or customers these enterprises and grow to higher levels of business scaling up their operations. Individuals concerned carry appreciable attachment & pride with their enterprise & products and would be happy to associate with companies who would help them to realize their dreams. However, camel & the Arab tent policy does not work, The investing company instead of becoming the driver with financial muscle power, should become a partner in realizing the dreams of entrepreneurs harnessing their knowledge base & brain power. Complementing the small & medium scale biotech company by a financially capable corporate organization will yield enormous trust and profits for either party. This is the win win formula for diversification or developing biotech business by a financially capable organization.
- 68 -
CROs DRIVERS AND CHALLENGES In the last 12 months more than half of the top 10 leading contract research organization (CROs) have invested large quantities of time and capital in evaluating India as key strategic location for conducting international clinical trials on the face of it, given the countries notorious reputation in protecting intellectual property especially in the life science industry juxtaposed to its burgeoning regulatory system that governs clinical research. Why would global research house suddenly focus their attention in India? The answer lies in the fact that while the afore said perception warrants some concerns, there is a lot of myth concerning the mechanic of conducting clinical research in India. In reality, the environment for conducting clinical trials in the country is very different from what it was even three years ago. Arguably the country offers a set of advantages that are so unique and strong vis a vis other regions of the world that no major drug research company can afford to ignore India in their medium to long term strategy. The highest advantage that India offers in conducting clinical research is the ability to conduct a trial faster than most of the major locations in the world in most of the significant therapeutic segments. This is one industry where time is a greater driver than money. In a detailed study conducted by international consultancy company emst and young in this area. It was concluded that in most cases there is a 20 to 30 % time advantage of carrying. Out a phase III study in India when compared to undertaking it in North America of Western Europe. Increasingly it was also observed that the number of patients involved in a trials , the greater our time advantage, from the cost perspective ,carrying out a study in India in strict accordance with global guidelines results in accost saving of about 25 to 40% when compared to the regions mentioned above. Like with many topics that are relatively new and complex, the aspect of conducting clinical trials in India has attracted a fair amount of skepticism and criticism. The most common place accusation is that of multinational drug companies using naïve Indian patients as guinea pigs for conducting novel research. The unfortunate part of the story is that critics of clinical research have little knowledge about what a clinical trial entail and even less knowledge about the kind of research that is permitted by the Indian regulatory authority the drug controller genera of India (DCGI). Under the current domestic guidelines, no chemical entity that has not been created / discovered in India can undergo a first in man or phase I study . Further more, a phase II or a phase III study can only be conducted if a simultaneous study for the same molecule is being conducted in another location after assessing key safety and ethical considerations. While there have been mishaps under the guise of clinical research, it is usually due to the clandestine operations of investigators that fails to adhere to the prescribed regulatory and ethical process for conducting clinical research in this country. To a grate extent the

- 69 -
benefits that clinical trials can provide to our population and to our medical infrastructure far out weight its potential drawbacks.
Key factors in a clinical trials US INDIA No of patients across urban life style disease. High Very high No of patients across tropical diseases. Low Very high Speed for recruiting patient for a trial. Low to Medium Very high Speed of conducting a trial. Medium Very high Return rate of patients. Medium Very high Pool of qualified doctors and clinicians. Very high Medium to high Heterogeneous population mix. High High Adherence to quality guidelines. High High Availability of technology to streamline trials Very high Medium to high
Cost of conducting a clinical trial US INDIA Phase study I $ 30 million < 50% Phase study II $50 million < 50% Phase study III $180million < 50%
First phase III clinical studies (the most common phase of clinical research conducted in India) offer patients, who suffer from terminals disease and complex medical condition. A chance to try out the latest research for their respective aliment on an average, these drugs are 3to 5 years ahead of the best solutions that are currently available in the market domestically and internationally. Second clinical research drugs allows patients to be treated free of cost with the latest medication that would other wise be cost prohibitive for the majority of the ailing population in this country. Third the majority of clinical research currently being conducted in India is being sponsored by international organization. Subsequently adherence to international community of harmonization (ICH) guidelines is steadily becoming the norm rather than the exception. Whilst this has several ramifications, a key out come of conducting a trial under the aforceasid guideline is the training of medical personnel in the area of good clinical practice. This deals with the systematic conduct, monitoring recording and reporting of clinical trial. Based on emst and young interaction with doctors who had undergone training in good clinical practice it was evident that in several case good clinical practice had altered the fundamental mindset in which these professional treated and maintained the records of their regular patients. Till date, we estimate close to 70 medical sites in the country , where teams of doctors have undergone good clinical practice training. even if a minor percentage of the country’s vast pool of doctors undergoes the afore said training it will

- 70 -
have a slow but fundamental impact on the quality of healthcare across public and private institutions . Fourth in most cases where a clinical trial is conducted at a medical institute , the sponsors of the trial pay a research fee that goes directly to the corpus of that institute. However a recent trend that is being observed is that sponsors are contributing directly to the infrastructure of the specific therapeutic department that is involved in conducting the trials. Discovery process is tough Period : up to 6 years Cost : Roughly $ 60 million Odds of drug reaching market: 1: 10,000 Identifying and validating targets: This involves developing the concept of how a new drug and treat a disease. Compounds that should be pursued further are short listed. Screening: Compounds that have desirable potencies and that react encouragingly are pulled out. These are the hits converting hits into leads calls for further refinement in the compound. During which solubility, toxicity, adsorption, metabolism etc are tested, even as the potency and activity are maintained. Stages of drug development Period: up to 12 years Cost: up to $ 200-250 million Odds of drug reaching market: 1:200 Pre clinical trials: toxicity and pharma co kinetic (ADME) are observed via tests in labs and in animals. IND Filing: company files an application for an investigational new drug (IND) with the FDA. This filling includes results of pre clinical trials and the plan for human clinical trials. Phase I trials: conducted on 20-100 healthy volunteers to prove safety. Once molecule enters clinical trials odds of success drop to 1:5. Phase II trials: 100-300 people suffering from the disease are treated. Considered by many companies as the stage to opt for licensing agreement. Phase III trials: involves between 1000 to 5000 patients in a bid to verify previous trials. New drug approval filling: FDA receives information and if satisfied gives its approval if it feels molecules is not yet ready for market may call for phase IV trials. Post marketing surveys: Companies have to conduct continuous surveillance once drug hits market, all through the life of the drug, serious reactions can result in drug withdrawal. Sale and marketing costs can take the entire cost of exercise right from drug discovery to development to as much as $ 400 million.

- 71 -
CHAPTER-6
INDIAN PHARMA INDUSTRY BEYOND 2005
- 72 -
The Indian Pharmaceutical Industry Beyond 2005: The Silver Lining The pharmaceutical industry is a lifeline industry that plays a very crucial role in building a strong human capital of a country and is very essential for economic growth and development. Today, it is at the top end of India’s science-based industries with wide ranging capabilities in the complex field of drug manufacture and technology. The contribution of the pharmaceutical industry towards a nation’s growth cannot be destabilized. The Indian pharmaceutical industry supplies essential drugs to consumers at much lower prices than any of its counterparts in the world. For e.g., prices of cardio-vascular drugs in India such as Atenolol and Enalapril are 25-30 times less than the US prices. This fact is particularly significant in a country where availability of inexpensive medicines is crucial to the healthcare for the masses. The pharmaceutical industry in India being highly fragmented has a wide range of over 100,000 drugs, (which includes vitamins, antibiotics, antibacterials, cardio-vascular drugs etc). Nearly 80 percent of the manufacturers have sales less than Rs 100 crores. The top ten companies in the industry control around 31 percent of the market. Now, let us take into consideration the primary aspects having impact on the pharmaceutical industry post-2005 policy regime. TECHNOLOGY – THE VITAL COMPONENT The manufacturing technology forms the backbone of not only the primary process involving the production of various bulk drugs form the raw materials and the intermediates , but also the secondary process involving the conversion of bulk drug into formulations. Formulations with a new delivery system or a highly specialized system like the multi-cell-multilayer micro dialysis cell technology or timed release etc are highly technology intensive. In the years to come, this technological component is certainly going to be the driving force in the pharmaceutical industry. In the post 2005 era also technological component is expected to play a vital role in terms of delivering the drugs at the exact site in the human body, thus potentiating their action with the least of the adverse effects. Technology has always played a significant role in improving the patient’s compliance. it is certainly expected to do so in future. R&D- THE SURVIVAL KIT With the introduction of new, strict patent laws in 2005, the Indian pharmaceutical industry will no longer take the advantage of the reverse engineering that has been its strength. In spite of this, India should be able to meet its January 1, 2005 commitment for product patents. Exclusive marketing rights (EMR) mechanism is being implemented and
- 73 -
should make some significant intellectual property (IP) protection available even sooner. Both houses of parliament have considered the proposed IP legislation. DISCOVERY RESEARCH With just few years to go before product patent bill implementation in India, Only two discovery research projects of Indian origin have moved to phase I/II, and even they are an improvement on existing targets. While this is no different than the path Japan traveled in the 1975-90 period, Indian companies will need to do much more, and faster, to gain a fighting chance for a position on global pharma arena. Not surprisingly, only five Indian companies have undertaken serous R&D investments, and even they are necessarily meager, given the limited profitability and the low value of the rupee. Much of the “research” efforts are still focused on analogue research, as that is not only financially affordable, but also what the current skill level would allow. While Indian is very strong in process chemistry, biology and applied biochemistry will require government academia private sector initiatives as will as enormous investments but the start in the short five years of so has been quite encouraging, and the outlook is very bright indeed, given the very talented and highly educated workforce and increasingly global resource base of the selected companies. D-FACTOR OF R&D Clinical research complements R&D initiation: R&D requires two distinct sets of skills. Research or discovery skills call for an established infrastructure and a tripartite collaboration between the private sector, academia and the government . this will clearly take some time for India to full y establish; though the new science of biotechnology should eliminate many wheels that it should not have to reinvent. Clinical development: The D of R&D, offers more near term opportunities, due to the availability of large patient populations for many major diseases plus well run hospitals in major cities that can adopt GCP standards that meet the US FDA requirements. Leading western clinical research organizations (CROs) are setting up shop in India. In brief, CRO activity is ideally suited for India. Especially for the more costly phase II and phase III trials. In addition many large selling drugs are going off patent through 2005, opening up window for ANDA filing as well.
- 74 -
DOMESTIC PHARMA PLAYERS The domestic players came into prominence only after the government‘s intervention in1970 in the form of recognizing process patents. The market, as viewed by the players in this segment, has three broad segments. Namely the patented segment, the generic segment and the branded formulations segment. The patented segment covers drugs that are under patents in regulated markets and yet has a market in areas where process patents are recognized. The generic segment includes drugs that are off patent and can gain entry into regulated markets in the same form as it is manufactured in India. The brand3ed formulations are products, which are form in house R&D facilities, received through a new drug discovery system. The R&D function among the Indian pharma companies is still at a very nascent stage. Even well entrenched players allocate as low as 2.5 % of their total turnover towards research and development expenses. This poorly with national pharma companies whose R&D accounts for as large as 15 to 20 % of their total turnover. With India having signed the WTO agreement, the road is all set for the recognition of product patents. The domestic pharma players have initiated investments on research facilities to counter the new regime. The key players in in-house research are Cipla, Dr Reddy’s and Ranbaxy. Though R&D, as a percentage of turnover of these companies have not crossed the five per cent mark, efforts have been taken to achieve this landmark figure in the next couple of years. The future course of action in the domestic segment is either a take over by a MNC/powerful Indian pharma player or act as in licensing partners. In licensing is either purchase of rights to market a product that another company has discovered and developed or undertaking the development and marketing of a product that another company discovered. Western generic market entry to drive near term growth: At least two Indian companies are now ready to file ANDAs the moment a major product goes off patent. Over the next three years many Indian companies are going to play an active role in a large number of such opportunities. Indian pharmaceutical company managements are now experienced and bold enough to accept the inevitable patent battles with innovator companies. Companies have acquired manufacturing facilities in developed countries, and have prominent presence in many smaller countries to sell branded generics. This is a major shift from earlier emphasis on Russia, Africa and such less developed markets. The resulting rapid cash flow growth should accelerate Indian pharmaceutical companies’ global expansion as well as the necessary investments in R&D.

- 75 -
KEY NEGATIVES Generic: while many negatives plague the Indian pharmaceutical industry, the recent penetration of the rock bottom low priced “generic generics” have caused the prices and margins to erode for many companies. It is now common to have a dozen brands of large molecule in about six months of its introduction in the western markets. Cut throat competition now faces more damaging competition as “generic” is sold to the end consumer at the same price as branded generics. But the expense of the manufacturer, while wholesalers continue to earn their usual40 % margin. This is likely to be a transitory consolidation process, where the strong will eventually emerge stronger. THE ADVANTAGE POST 2005 Indian pharma companies have a unique cost advantage that facilitates in the production of drugs at 1/20th of the cost incurred in other developed economies. The key ingredient the cost of manpower is unthinkably low, enabling in the low cost manufacture of drugs. This could be extended to research function, which is again, manpower intensive .Scientists for R&D in India could be hired at 15-20 % of the cost prevailing in US. Even accounting for higher levels of uncertainties among Indian companies to bring about blockbuster drugs, the low costs in conducting research makes them at par with the pharma companies in developed economies. There the uncertainly is relatively low but the cost of overall research is astronomically high due to bloated costs of research inputs. Going by these trends, the signals are very clear in the industry. Companies in India could either be research outfits for MNCs or would become powerful players in niche segments with unmatchable price competitiveness. Contract research is already in vogue in India. The sector is poised with a mammoth challenge of providing health care to the second most populous country of the world. Pharma companies, be they domestically bred of form international parentage, have increasingly realized the significance of challenge lying ahead. Time is ripe to bring out hidden potential for both survival and also sustenance. The industry is poised to see more consolidations and mergers in the years to come. Such activities would give way to the industry’s maturity.
Pharmaceuticals are one of the most happening sector in the next decade, globally in general and in India in particular, with advent of these trends.

- 76 -
CHAPTER -7
MAJOR TRENDS OBSERVED AND FINDINGS 7.1 – Consolidation 7.2- Export 7.3- Mergers and acquisitions 7.4- Pharma Outsourcing 7.5- New Launches after Year 2005 by the MNC’s in
India. 7.6- Generics 7.7- Co-marketing 7.8- Organized health management 7.9- Creating the health – new concept
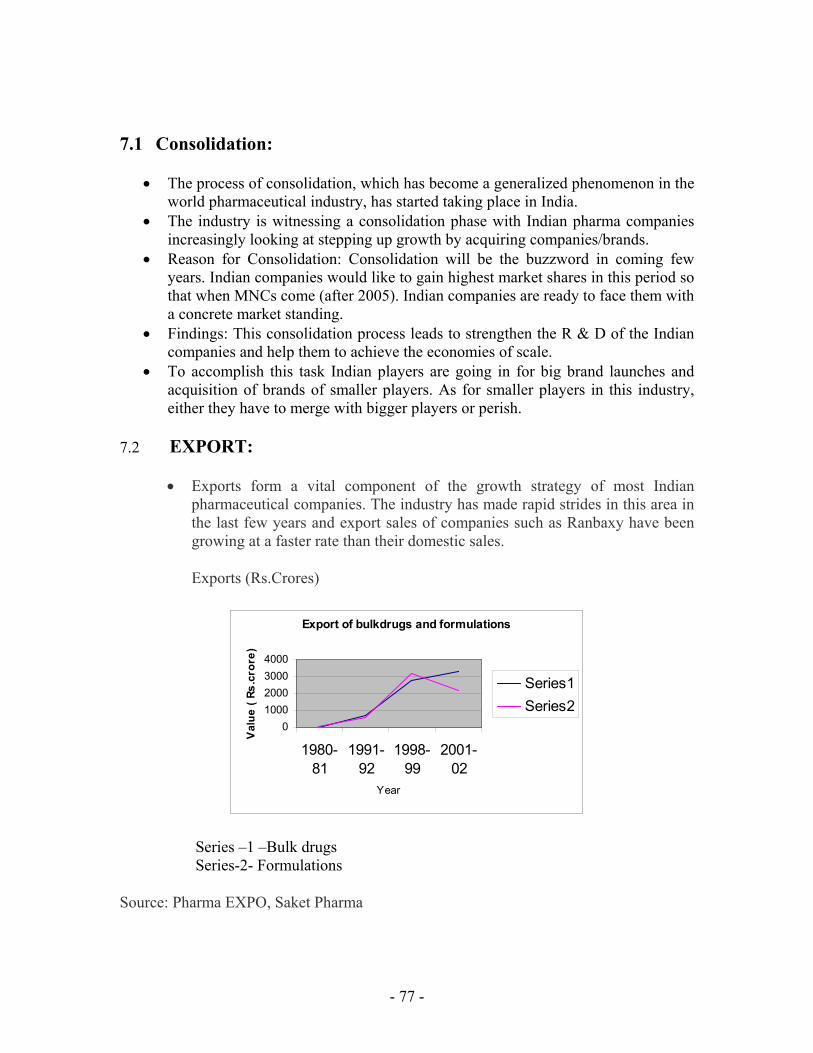
- 77 -
7.1 Consolidation:
• The process of consolidation, which has become a generalized phenomenon in the world pharmaceutical industry, has started taking place in India.
• The industry is witnessing a consolidation phase with Indian pharma companies increasingly looking at stepping up growth by acquiring companies/brands.
• Reason for Consolidation: Consolidation will be the buzzword in coming few years. Indian companies would like to gain highest market shares in this period so that when MNCs come (after 2005). Indian companies are ready to face them with a concrete market standing.
• Findings: This consolidation process leads to strengthen the R & D of the Indian companies and help them to achieve the economies of scale.
• To accomplish this task Indian players are going in for big brand launches and acquisition of brands of smaller players. As for smaller players in this industry, either they have to merge with bigger players or perish.
7.2 EXPORT:
• Exports form a vital component of the growth strategy of most Indian pharmaceutical companies. The industry has made rapid strides in this area in the last few years and export sales of companies such as Ranbaxy have been growing at a faster rate than their domestic sales.
Exports (Rs.Crores)
Export of bulkdrugs and formulations
01000200030004000
1980-81
1991-92
1998-99
2001-02
Year
Val
ue (
Rs.c
rore
)
Series1Series2
Series –1 –Bulk drugs Series-2- Formulations
Source: Pharma EXPO, Saket Pharma
- 78 -
• Reasons for increase in Export: This is due to the liberalization policy adopted by the government and decrease in Tariff barriers.
• The Government’s stipulation that formulations manufacture must be covered back by the manufacture of bulk drugs to the extent of at least 10% and;
• The easy access to funding through the equity route following the opening up of the Indian capital markets which has resulted in a large number of units being set up to manufacture bulk drugs.
• The positive fall-out of this has been that along with the growth witnessed by the companies, their skill levels have increased leading to a broad-basing of the industry.
• Findings: The next five years will witness a spate of patent expire of blockbuster drugs that will accord opportunities to supply bulk drugs and formulations to advanced markets.
- 79 -
7.3 Mergers and Acquisitions:
• In coming days, with the help of international financial companies the MNCs will capture and take control of Indian companies to control the Indian market.
• Have threatened the existing companies with the same origin and their workers. • Reasons for Merger and Acquisition: This is observed as the effect of
globalization on Indian pharmaceutical industry and the government’s permission to the MNCs to come to India with 100% equity.
• Findings: Through the process of mergers, acquisitions and takeovers MNCs will gradually perpetuate their grip on the Indian industry by the creation of a limited number of mega companies having monopoly control and domination world wide. In the absence of competition people will have to pay any price as it happens in the sellers market.
7.4 Pharma Outsourcing:
• What is the first thing that comes to your mind when you hear the word ‘Outsourcing’? Majority of us will say Information Technology. IT has been the key growth driver for the Indian economy.
• This was possible primarily on account of their strategy of successfully acting as an outsourcing base for their client Pharma could be the next outsourcing success story providing further strength to the Indian economy. In this report.
• Avenues available for Indian companies: • Indian companies have an opportunity in outsourcing in the form of contract
manufacturing and contract research. The following chart gives a brief overview of the various avenues available for Indian pharma companies.
• Contract manufacturing: • Contract manufacturing takes place when an Indian company utilizes its
manufacturing facilities to produce drugs on behalf of an MNC. • Depending upon the terms of the agreement, the Indian company either receives a
fixed commission for the drugs manufactured, which are subsequently sold by the other company and/or a right to sell the drug in the domestic market.
• The contract manufacturing agreements are not only for the manufacture of bulk drugs but also for the production of formulations. Moreover, the formulations manufactured need not only be generics.
• With product patents being introduced in India from 2005, Indian contract manufacturing companies are also likely to get contracts for the production of patented drugs.

- 80 -
• Reason for outsourcing by MNC pharmaceutical companies:
• After an NCE receives patent, it has to undergo clinical trials and various regulatory procedures. Only after successfully completing these requirements is it allowed to enter the market and generate revenues.
• These clinical trials and regulations take on an average 8 – 10 years. Thus, out of the 20 years of patented life of the drug, almost half is lost.
• Consequently, the company is required to make the most of the remaining patented life of the drug and generate adequate revenues to not only recover the huge R&D investments but also generate profits.
• Further, globally companies have realized that pharma R&D and marketing of drugs are going to be the key drivers for growth going forward.
• Hence, such MNC companies would want to concentrate on these two crucial growth drivers and let some other company do the manufacturing activity.
• Another very important benefit accruing to these MNC companies is that they are able to isolate themselves from the various problems involved with owning a manufacturing facility like labour disputes etc.
• Apart from the above factors, another key reason for MNCs inclination towards outsourcing is the fact that the manufacturing can be done in developing countries at an extremely low cost.
• Reason for selecting India as outsourcing destination: • Low cost skilled labour is the greatest advantage that India has. Indian companies
have been successfully reverse engineering patented drugs since the seventies and have developed excellent skills in drug manufacturing.
• For drugs to be sold in the US market (the largest drug market), the plant in which it is manufactured should be US FDA approved. In view of this, an increasing number of domestic pharma companies are getting their plants approved by the US FDA. This is another factor in favor of Indian companies.
• Another factor working in India’s favour (though not something we should be proud of) is that the environmental norms in India are not as stringent as international ones and are also not strictly enforced.
• This has also prompted many MNCs to choose India for manufacturing drugs for which it would have been extremely difficult to get environmental clearance in their country. With India now allowing 100% FDI investment in the pharma sector, many MNCs might also consider establishing a base in India for carrying out their manufacturing activities.
• Contract research is an agreement entered into by an Indian research company with an MNC pharma company wherein the Indian company carries out drug research and testing on behalf of the MNC.
• Thus, the Indian company will undertake the various stages of clinical trials on the MNC drug. This would include selecting patients on whom the tests will be carried out and also evaluating the results for the same.

- 81 -
• Apart from the above, the MNC pharma company could also enter into a contract with the Indian company for the development of a New Chemical Entity (NCE). It takes roughly US$ 350 m to US$ 500 m (source: Pfizer Journal) for an NCE to go through the various stages of clinical trails and enter the market. The MNCs hence sell the drugs at a premium to recover this high expenditure.
• Reasons of doing contract research by MNC’s pharma. • However, off late there has been increased pressure from the US government on
MNC pharma companies to bring down the drug prices. US government now passing regulations enabling a smooth entry of generics there is a higher threat of competition.
• Hence, there is a need to bring down the R&D expenditure. This is the key reason for the MNC pharma companies opting for outsourcing their research activities.
• Reasons for using India as a outsourcing Hub: • Like in contract manufacturing, in contract research also India has a cost
advantage. • There are two key reasons for India being a low cost contract research hub.
Firstly, the availability of low cost and highly skilled scientists and research personnel and secondly, the availability of large number of patients with ethnic diversity at a much lower cost.
• Moreover, the Indian scientists have excellent molecule synthesis skills, which give them a distinct edge over their international counterparts.
• With pharma research becoming more and more IT oriented, India again stands to gain as it will be in a position to leverage on its strong IT base and get more contracts.
• And finally, the Indian companies now follow the Good Clinical Practice (GCP) guideline, the compliance of which is prescribed by the US FDA.
• The above factors make India an obvious first choice when MNC pharma companies consider contracting their research activities.
• Findings: Pharma outsourcing is a phenomenon waiting to happen which could yield high returns for the domestic pharma companies. And very rightly, most Indian companies (big and small) have identified the same and are taking steps to project themselves as the best option for outsourcing. However, the Indian companies need to understand that although lucrative, in the long run only the research based companies will survive. Thus, ideally they should utilize the funds generated by these activities to develop a good research and development infrastructure.

- 82 -
7.5 New launches after Year 2005 by the MNCs in India.
• Come year 2005, India will witness a plethora of new launches. International companies will come in the country with top of the line products. These products will be priced on the higher side so as to enable the respective companies to recover their investment in R&D. Masses will keep on going for the older cheaper versions of the products, leaving newer products a high price, low volume proposition.
• As for local players they will keep on manufacturing popular off patent products. They will also go in for franchise manufacturing and acquiring marketing rights for overseas MNCs. Indian companies could also get into research tie-ups with international players, mainly for clinical research. Companies like Dr, Reddy’s Lab are already doing so.
• Reason for launching new products beyond 2005: • The multinationals seem quite content in postponing the launch of their
blockbuster products in India till the product patent becomes a reality. • Findings: By launching the products beyond 2005 MNC compromise revenues
from Indian operations than to allow their products getting copied. • Another interesting trend, which is slowly but steadily catching up with MNC
pharma companies is the marketing alliance they are logging with domestic majors. It makes perfect sense for them to leverage on their strong marketing strength to take innovative products from domestic majors to market. For example, Glaxo currently markets Cipro-D molecule, a key product from Ranbaxy’s pipeline. Prior to that Pfizer teamed up Shanta Biotech to market its Hepatitis B vaccine.

- 83 -
7.6 Generic business:
• Let us understand what are generic drugs in the first place. Generic drugs are the chemical and therapeutic equivalents of brand-name drugs, typically sold under their generic chemical names at prices below those of their brand-name equivalents.
• These drugs are required to meet similar governmental standards as their brand-name equivalents and must receive regulatory approval prior to their sale in any given country. Generic drugs may be manufactured and marketed only if relevant patents on their brand-name equivalents (and any additional government-mandated market exclusivity periods) have expired, been challenged and invalidated, or otherwise validly circumvented.
• Reasons for Increasing the Business of Generic Market: • By 2005, 15 of the leading 35 blockbuster molecules in the world are expected to
go off patent, which makes the opportunity highly lucrative for generic companies. Besides this, rising healthcare costs and an ageing US population that requires larger medical attention is intensifying pressure on the government and legislators to reduce healthcare related expenses.
• Findings: Thus there is pressure on the government to enable a faster generic entry to put a cap on the healthcare cost. This could be justified by the fact that means approval time for a generic drug has come down to around 18 months from an average of more than 26 months in 1995.
• While on one hand, these players devise their game plan to ensure fastest entry of their generic drug to the market; brand name manufacturers on the other hand devise numerous strategies to delay competition from lower cost generic versions of their products.

- 84 -
7.7 Co-marketing: One of the major plus points of the Indian pharmaceutical industry is its’ well established marketing and distribution network
• For a commission, Indian companies can capitalize on their existing distribution network and enter into marketing agreements with other companies that have a product but do not have the sales force required to market the same.
• Wockhardt has entered into a marketing agreement with Bayer AG for the marketing of the anti-diabetic drug Acarbose.
• Reason for co-marketing: To reduce the marketing and distribution expense by various pharmaceuticals. And also helpful for the company which has a good product but no sales force.
• Findings: Useful in achieving the economies of scale by both the company and helpful in this competitive dynamic world.
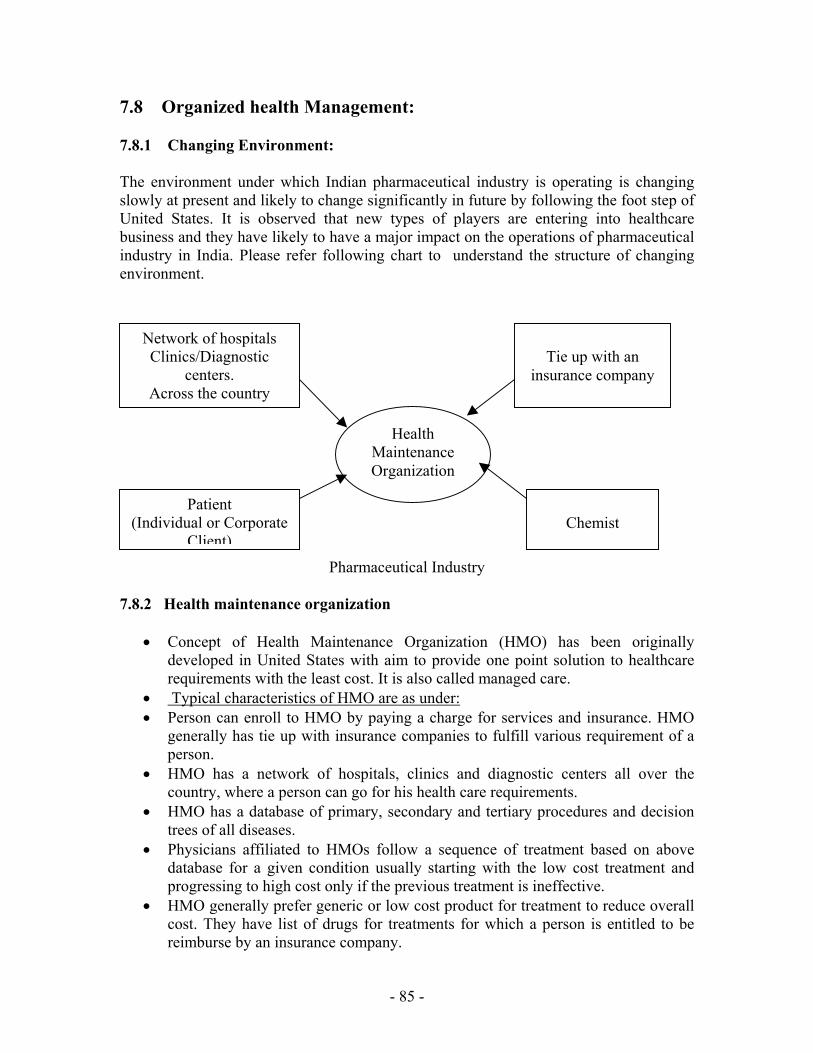
- 85 -
7.8 Organized health Management:
7.8.1 Changing Environment: The environment under which Indian pharmaceutical industry is operating is changing slowly at present and likely to change significantly in future by following the foot step of United States. It is observed that new types of players are entering into healthcare business and they have likely to have a major impact on the operations of pharmaceutical industry in India. Please refer following chart to understand the structure of changing environment.
Pharmaceutical Industry 7.8.2 Health maintenance organization
• Concept of Health Maintenance Organization (HMO) has been originally developed in United States with aim to provide one point solution to healthcare requirements with the least cost. It is also called managed care.
• Typical characteristics of HMO are as under: • Person can enroll to HMO by paying a charge for services and insurance. HMO
generally has tie up with insurance companies to fulfill various requirement of a person.
• HMO has a network of hospitals, clinics and diagnostic centers all over the country, where a person can go for his health care requirements.
• HMO has a database of primary, secondary and tertiary procedures and decision trees of all diseases.
• Physicians affiliated to HMOs follow a sequence of treatment based on above database for a given condition usually starting with the low cost treatment and progressing to high cost only if the previous treatment is ineffective.
• HMO generally prefer generic or low cost product for treatment to reduce overall cost. They have list of drugs for treatments for which a person is entitled to be reimburse by an insurance company.
Health Maintenance Organization
Network of hospitals Clinics/Diagnostic
centers. Across the country
Tie up with an
insurance company
Patient (Individual or Corporate
Client)
Chemist

- 86 -
• In India a full-fledged HMO has not yet started by any one but smaller version of HMO is operating in present environment as discussed below.
Third party administrator The one-stop shop for managing the health of employees across the companies has already started by Mumbai based entrepreneur Mr. Nimesh Parekh with joint venture with United Kingdom based company (M/s Sedgwick Parekh Health Management). They called it a third party administrator (TPA). Company has tied up with hospitals (some 101 in 26 cities) and diagnostic centers where employees from his enrolled firms can go for their medical needs. It also provides a 12-hour help desk that guides people through hospital procedures, provides names of blood banks, ambulances, and processes insurance claims. Other TPAs: Paramount in Mumbai and Heritage in Calc Preferred provider organization In Mumbai, Ms. Swati Piramal, PhD from Harvard University in health maintenance organization, runs Preferred Provider Organization (PPO). She is mining huge amounts of data on sections and subsections of cultures across a large geographical segment of the country. Combined with this will be disease protocols that will yield at click of mouse, a decision-tree analysis on the treatment of primary, secondary and tertiary diseases.
- 87 -
7.8.3 Impact of changing environment on Indian pharmaceutical industry
• It is very clear from figure that in future structure like HMO will be having considerable influence on Indian Pharmaceutical Industry at distant future and some of the influences are described below.
o Pharmaceutical companies introducing new products not only have to provide better therapeutic advantages but also have to keep prices low to get users associated with HMOs or related organization.
o Competitions will intensify with introduction of generic products o Market will expand due to reduced cost of treatment. o Corporate restructuring and strategic tie up between various players will
increase.
• Finding: Role of insurance companies was limited in nature due to government control on the insurance sector in past. The only player in healthcare insurance market was government owned General Insurance Corporation offering single product “Mediclaim”. Now, after opening of insurance sector, it is likely that private companies having some foreign stake will enter into the healthcare insurance market, which might result into increased spending on healthcare business and thus provide boost to pharmaceutical industry. Role of insurance companies as a payer in decision-making will also increase in future.

- 88 -
7.9 CREATING HEALTH: A NEW CONCEPT
• It means wealth is necessary to purchase the goods and services that contributes to health. But now we are moving into a period that turns the equation to wealth follows health.
• Consider this example. Suppose some one have got a new innovative medicine whose clinical efficiency is beyond doubt and which is cost effective. It means treatment is less expensive for a payer and he can direct his money to other productive way. At the same time medicine reduces the incidence of illness and death among its target population. Now these people can contribute to society’s productivity thus driving economy. This is called moving from treating disease to creating health.
• A variety of factors are driving towards this new approach. Among the most important are: 1) Advances of science and, 2) More informed, self reliant and motivated customer.
• Advances of science:
In area of medical science, a series of revolution are under way. Some of them are:
1) Biological knowledge, including the genetic bases for disease 2) Technology including electronics, robotics, and communication 3) Information including globally accessible and analyzable databases Combination of above is creating a new science called “Genomic” which breaks the pharmaceutical R&D into three steps namely, 1) Target Selection
• In this approach, researchers collect detailed medical histories and genetic information from larger groups of people.
• Using the technology, the clinical and genetic information – genotypic profiles are prepared. Powerful databases are built to identify disease genes, which are common to most patient populations.
2) Drug Candidate Selection
• After candidate’s genotypic profile has been identified next stage is to find most effective drug suitable for given genotypic profile.
• Due to availability of automated technology, latest computer technology and molecular biology, it is now possible to see effect of given molecule on genotypic profile in very effective and efficient manner.
3) Product Development
• If one get a molecule that acts on a target, next question in pre clinical is that how to metabolized it.

- 89 -
• Advances in technologies like mass spectrometry will allow preparing metabolic profile very quickly, thus it will decrease the time required to develop new drug.
Finding of the concept:
• Informed customer
• People have always been interested in their health, obviously, but recently lifestyles and technology have not provided the means for them to access health information.
• But in future due to advent of Internet technology customer will have health information on their desktop whenever required.
• Pharmaceutical companies, physician or even chemist will be ready to share information regarding health for customers.
• Even in each case, they will go beyond the idea of helping people to get well to answer to customer demand for information for a healthier life.
• As customer will have easy access to information, critical success factor will be scientific innovation and proving value. Each company will not only have to innovate its product but also have to prove its value to the customer.
Role of Internet:
• The Internet can link up patients, doctors, chemist shops, and laboratories thus streamlining of paperwork and saving administrative costs.
• Another step would be online disease management, especially for chronic ailments. As in most industries, the push towards web in health care too will be driven by consumers and change in social attitude.
• Desire for better health will increase the demand for better information and services and that where Internet can play an important role.

- 90 -
BIBLIOGRAPHY Federation of Indian Chamber of Commerce and Industry (FICCI), Indian HealthCare Industry WTO and Its Competitiveness Field articles from the library of Ahmadabad Management Association (AMA), Ahmadabad. Search Engines: www.google.com www.indiainfoline.com www.yahoosearch.com