PET Imaging for Solid Tumors Post CMS Final Decision (CAG-00181R4)
Upload
cynthia-andersonCategory
view
218download
1
Int. J. Radiation Oncology Biol. Phys., Vol. 69, No. 1, pp. 155–162, 2007Copyright � 2007 Elsevier Inc.
Printed in the USA. All rights reserved0360-3016/07/$–see front matter
doi:10.1016/j.ijrobp.2007.02.055
CLINICAL INVESTIGATION Rectum
PET-CT FUSION IN RADIATION MANAGEMENT OF PATIENTS WITHANORECTAL TUMORS
CYNTHIA ANDERSON, M.D.,* MARY KOSHY, M.D.,* CHARLES STALEY, M.D.,y NATIA ESIASHVILI, M.D.,*
SHARAM GHAVIDEL, M.S.,* ZACH FOWLER, M.D.,* TIM FOX, PH.D.,* FABIO ESTEVES, M.D.,z
JEROME LANDRY, M.D.,* AND KAREN GODETTE, M.D.*
Departments of *Radiation Oncology and ySurgery and zDivision of Nuclear Medicine, Department of Radiology,Emory University School of Medicine, Atlanta, GA
Purpose: To compare computed tomography (CT) with positron emission tomography–CT (PET-CT) scans withrespect to anorectal tumor volumes, correlation in overlap, and influence on radiation treatment fields and patientcare.Patients and Methods: From March to November 2003, 20 patients with rectal cancer and 3 patients with anal can-cer were treated with preoperative or definitive chemoradiation, respectively. Computed tomography simulationdata generated a CT gross tumor volume (CT-GTV) and CT planning target volume (CT-PTV) and 18F-fluoro-2-deoxy-glucose PET (FDG-PET) created a PET-GTV and PET-PTV. The PET-CT and CT images were fusedusing manual coregistration. Patients were treated with three-dimensional conformal therapy to traditional doses.The PET, CT, and overlap volumes (OVs) were measured in cubic centimeters.Results: Mean PET-GTV was smaller than the mean CT-GTV (91.7 vs. 99.6 cm3). The mean OV was 46.7%. Astumor volume increased, PET and CT OV correlated significantly ( p < 0.001). In 17% of patients PET-CT alteredthe PTV, and in 26% it changed the radiation treatment plan. For 25% of patients with rectal cancer, PET detecteddistant metastases and changed overall management. Ten rectal cancer patients underwent surgery. When thepretreatment PET standardized uptake value was >10 and the posttreatment PET standardized uptake valuewas <6, 100% achieved pathologic downstaging ( p = 0.047).Conclusions: Variation in volume was significant, with 17% and 26% of patients requiring a change in treatmentfields and patient management, respectively. Positron emission tomography can change the management foranorectal tumors by early detection of metastatic disease or disease outside standard radiation fields. � 2007Elsevier Inc.
Anorectal cancer, PET-CT, Radiotherapy.
INTRODUCTION
Positron emission tomography–computed tomography
(PET-CT) fusion is gaining acceptance for use in radiation
management of patients with primary tumors at several sites,
including head and neck, lung, and lymphoid neoplasms
(1–6). For patients with carcinoma of the rectum, PET-CT
is frequently used to diagnose and stage tumors, evaluate
for treatment response, and assess for tumor recurrence.
The utility of PET-CT over PET alone includes better ana-
tomic correlation of areas that show high avidity for 18F-flu-
oro-2-deoxy-glucose (FDG). Cohade et al. (7) determined in
a retrospective study of 45 patients with colorectal cancer that
PET-CT improved the staging and restaging accuracy from
78% to 89% compared with PET alone. In another study,
155
PET-CT was found to alter the staging in 20% of patients
and locate findings not seen in 17% of patients when evalu-
ated by PET alone (8).
Two recent articles have described the benefits of PET-CT
in the treatment of anal carcinoma. In the first, PET detected
nodal metastases in 24% of patients who were considered
node negative on CT scan (9). Cotter et al. (10) reported
the ability of PET imaging to detect correctly 91% of primary
lesions, compared with 59% by CT scan. Twenty-three
patients with clinically negative lymph nodes and 17% of
patients with normal CT scan results were considered node
positive on PET scan.
Although several studies have demonstrated the utility of
PET scans for the detection of colorectal primary tumors,
data on its impact on radiation treatment fields for rectal and
Reprint requests to: Jerome Landry, M.D., Department of Radia-tion Oncology, Emory University Hospital, 1365 Clifton Road NE,Atlanta, GA 30322. Tel: (404) 778-3473; Fax: (404) 778-4139;E-mail: [email protected]
Presented orally at the Annual Meeting of the Radiological Societyof North America, November 28–December 3, 2004, Chicago, IL.
Conflict of interest: none.Received May 11, 2006, and in revised form Feb 9, 2007.
Accepted for publication Feb 14, 2007.

156 I. J. Radiation Oncology d Biology d Physics Volume 69, Number 1, 2007
anal tumors continue to emerge. Ciernik et al. (11) evaluated
the value of PET-CT on radiation planning for patients with
tumors at several sites, including carcinoma of the rectum
(6 patients) and carcinoma of the anus (7 patients). In more
than half of all patients (56%), the gross tumor volume
(GTV) delineation was significantly altered. Gross tumor vol-
ume increases were seen in 3 of 6 patients with rectal prima-
ries, with a mean GTV increase of 50% and a planning target
volume (PTV) increase of 20%. In patients with tumors of the
anal canal, PET-CT influenced the boost volumes but did not
alter the initial standard fields. The mean change of GTV was
34%, with 3 patients experiencing an increase and 1 patient
a decrease in volumes. The mean change to PTV was 18%.
In a study by Thomas et al. (12), PET imaging changed the
overall management of 51% of patients with advanced and
metastatic colorectal cancer. Positron emission tomography
provided additional tumor information in 70% of patients, up-
staging disease in 66% of patients, and downstaging disease in
30%.
We analyzed the clinical impact of PET-CT fusion on ra-
diotherapy planning and management of patients with rectal
and anal primaries. Specifically, we compared the size of tu-
mor volumes on CT with those on PET scans, the correlation
in overlap between both sets of images, and the influence of
PET-CT on the radiation treatment fields and overall man-
agement of patient care.
PATIENTS AND METHODS
The Human Investigations Committee (HIC) at our institution ap-
proved a protocol in 2001 that allowed for prospective and retro-
spective review of all gastrointestinal malignancies in which
radiation was used as part of the overall management. The cohort
of patients in this study was covered as part of the HIC approval.
In addition, all patients provided consent for treatment with chemo-
therapy, radiotherapy, and surgery.
We collected data on all patients with biopsy-proven, intact pri-
mary anorectal tumors treated at a county and private hospital
from March to November 2003. Twenty-three patients underwent
PET-CT fusion scans as part of treatment planning. Twenty patients
(87%) were diagnosed with rectal cancer and were treated with pre-
operative chemoradiotherapy, whereas 3 patients (13%) received
definitive chemoradiation for tumors of the anus.
PET-CT scan and CT simulation proceduresPatients abstained from caloric intake for a minimum of 4 h before
administration of FDG and were required to have a serum glucose
level <200 mg/dL. Ten to fifteen millicuries (370–555 MBq) of
FDG were injected i.v. with 45–60 min allowed for the uptake
phase. Patients with rectal cancer were scanned and treated in the
prone position on a belly board to allow for anterior displacement
of small bowel from the treatment field. Patients with anal cancer
were scanned and treated supine.
Imaging and data acquisition were performed on either an inte-
grated big-bore PET-CT system (Discovery LS; GE Medical Sys-
tems, GE Healthcare, Chalfont St. Giles, United Kingdom) at the
county hospital or a separate PET-CT (DST; GE Medical Systems)
and CT simulation system (Discovery LS; GE Medical Systems)
at the private hospital. On the integrated system, patients were in
the treatment position for simulation on the dedicated integrated
PET-CT system, with automatic fusion of the PET-CT images.
Thirty minutes before scanning, patients with rectal cancer drank
450 mL of barium sulfate suspension (Readi-Cat2; E-Z-EM, West-
bury, NY) for small bowel opacification. Rectal contrast was not used
because of its ability to cause image artifact during interpretation
of the PET-CT images. Computed tomography data were acquired
first during shallow breathing, whereas PET data were acquired
during free breathing and over multiple breathing cycles. Computed
tomography scans were performed without contrast, and parameters
included tube rotation time of 0.5 s per revolution, 140 kV, 180 mA,
with a reconstructed slice thickness of 5 mm. Scanning length was
867 mm, and acquisition time was less than 1 min for the entire axial
field of view.
After CT data acquisition, the table top—with the patient in the
same position—was advanced into the PET scanner, and acquisition
of PET data began at the head. Data were acquired from four to five
table positions for 5 min each. For attenuation correction of the PET
images, CT sections were reduced to PET resolution by smoothing
with a Gaussian filter (8-mm full width, half maximum), and atten-
uation correction slices were reconstructed using an iterative recon-
struction. Images were viewed on a Xeleris workstation (GE
Medical Systems). The PET and CT data sets were then transferred
to a viewing station using Digital Imaging and Communications in
Medicine software.
At the private hospital, all patients received a planning CT simu-
lation scan followed by a PET-CT scan in the same position used dur-
ing the CT simulation. Patients with rectal cancer drank 450 mL of
barium sulfate suspension 20–30 min before both PET-CT scan
and CT simulation. Rectal contrast was not used for CT simulation
to mimic the conditions of the PET-CT scan. The PET-CT was fused
to CT simulation scan images by manual coregistration. A minimum
of three matched anatomic landmarks were selected, with an average
acceptable error of 2 mm. The final data set was sent to an ECLIPSE
treatment-planning system for radiation planning.
PET scan interpretationThe standardized uptake value (SUV) was used as a semiquantita-
tive tool to supplement visual interpretation. Standardized uptake
values were determined by manually drawing a region of interest
over the suspected lesion in the transaxial plane. The SUV in each
pixel was calculated according to the following formula: SUV =
activity concentration/(injected dose/body weight). The maximum
SUV within a region of interest was used to minimize finite resolu-
tion effects. Any suspected lesion with a maximum SUV $2.5
was considered malignant. Histograms of FDG uptake intensity
were not generated.
Radiation and chemotherapy treatment and impact ofPET-CT on management
All patients were treated with concurrent chemotherapy and ra-
diotherapy using three-dimensional conformal therapy. All grossly
visible tumors were contoured prospectively as the gross tumor vol-
ume (GTV). Results of initial diagnostic scans and colonoscopy
were used at the time of contouring. The CT-GTV included the en-
tire circumference of the rectum at the level of the visible abnormal-
ity. The PET-GTV was contoured initially using the coregistered
PET-CT images and was not visible when the CT-GTV was con-
toured so as to minimize bias. The PET-GTV was defined on the
basis of the visual interpretation of the radiation oncologist, and
all contours were analyzed by one radiation oncologist (J.L.).
The PET-GTV and CT-GTV were measured in cubic centimeters.
The overlap volume (OV) was contoured as a separate volume and

PET-CT fusion for anorectal tumors d C. ANDERSON et al. 157
similarly measured. Percentage of overlap was calculated by divid-
ing the OV by the CT-GTV. The CT volume was chosen to deter-
mine the overlap percentage because it is ultimately the data set
that is used for all radiation treatment planning. The clinical target
volume (CTV) was created to account for microscopic disease and
typically was defined as the GTV plus a 2-cm margin. No additional
margin was added to generate the planning target volume.
Initial radiation fields for patients with rectal cancer were de-
signed for a four-field box technique with adjustments made to field
size when necessary according to PET data. On the anterior and pos-
terior fields, the superior border was L5/S1, the inferior border was
the bottom of the obturator foramen with a minimum of a 2-cm mar-
gin on the most distal aspect of the CTV, and the lateral borders were
placed 2 cm distal to the pelvic inlet. For the lateral fields, the ante-
rior margin was placed posterior to the pubic symphysis for patients
with T3 disease and anterior to the symphysis for T4 disease. The
initial field was treated to 45 Gy with a reduced field boost that en-
compassed the CTV alone to a mean total dose of 50.4 Gy (range,
50.4–59.4 Gy). Chemotherapy was delivered concurrently and con-
sisted of continuous infusion 5-fluorouracil at 225 mg/m2 during
radiation. One month after surgery the patients received adjuvant
5-fluorouracil and leucovorin for 6 cycles. Patients were scheduled
for follow-up PET-CT scanning to assess tumor response within
2 weeks of completing chemoradiation. Surgery was planned for
1 to 2 weeks thereafter.
Patients with cancer of the anal canal were treated in an anterior–
posterior fashion, with the initial field being wider anteriorly than
posteriorly. The initial superior border was placed at the junction
of L5/S1, and the inferior border was 3 cm below the anal tumor.
Lateral borders covered the lateral inguinal lymph nodes anteriorly
and the pelvic inlet posteriorly. Adjustments to the borders were
made according to PET data. At 30.6 Gy, the superior border
was lowered to the bottom of the sacroiliac joints for both fields,
and the reduced field received a boost dose of 14.4 Gy. Finally,
the GTV plus a 2-cm margin received a 5.4–14.4-Gy boost to
give a total dose of 50.4–59.4 Gy according to the stage of disease.
The medial and lateral inguinal nodes were boosted with electron
fields to deliver 45 Gy in clinically N0 patients and 55.8–59.4
Gy to patients with involved lymph nodes. Patients received 5-fluo-
rouracil at 1000 mg/m2 � 96 h along with mitomycin-C at 10 mg/
m2 � 1 during the first and fourth week of radiation. Follow-up
scans were obtained between 1 and 3 months after completion of
treatment.
Data analysisMean GTV and OVs from the CT and PET were calculated. The
impact of PET on formation of GTV and PTV and its ability to
correspond to OV were analyzed. Additional analyses included
changes in treatment strategy based on PET data and correlation
of posttreatment PET imaging with pathologic response when
appropriate.
Data were analyzed with JMP Statistical Discovery Software
5.0.1a (SAS Institute, Cary, NC). Results were calculated by analy-
sis of variance and root mean square methods.
RESULTS
Patient demographicsTwenty patients (87%) were diagnosed with rectal cancer,
and 3 patients (13%) were treated for tumors of the anus.
Table 1 shows demographic information on all patients.
Thirteen patients (56.5%) were male, and mean age was 58
years (range, 30–81 years). Patients were staged clinically ac-
cording to the American Joint Committee on Cancer Staging
Manual, 6th edition, on the basis of physical examination, co-
lonoscopy report, pathologic reports from the biopsy speci-
men, and pretreatment imaging, including CT scan of the
chest, abdomen, and pelvis, PET-CT scan, rectal ultrasound,
and chest X-ray. Staging CT scans and serum carcinoem-
bryonic antigen levels were measured before PET-CT imag-
ing. Lymph nodes were considered positive if they were
palpable on clinical examination, measured greater than 1.5
cm on CT scan, were enlarged on transrectal ultrasound, or
had an SUV >2.5 on PET-CT.
Of the patients with rectal primaries, 12 (60%) were staged
T3N0 (IIA); 2 (10%) were T4N0 (IIB); 3 (15%) were
T3NxM1 (IV), and T3N1 (IIIB), T2N2 (IIIC), and TxNxM1
(IV) were each represented with 1 patient (5% each). The 4
patients with metastatic disease had suspicious lesions de-
tected on PET-CT in the liver, lung, para-aortic lymph nodes,
and descending colon, respectively. Each patient subse-
quently underwent a dedicated spiral high-resolution CT
scan of the abdomen or lung to further evaluate the abnormal
areas. Radiographically suspicious lesions were presumed to
represent metastases and were not biopsied. Two patients
(67%) with cancer of the anus were staged as T3N0 (II),
and the third (33%) was staged T3N2 (IIIB). Seventeen pa-
tients (74%) were treated at a county hospital and 6 (26%)
at a private institution.
Observed volumesPositron emission tomography volumes, on average, were
smaller than CT volumes (Table 2). The mean PET-GTV was
91.7 cm3 (median, 37.1 cm3; range, 2.9–859 cm3), and the
mean CT-GTV was 99.6 cm3 (median, 66 cm3; range,
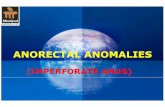
>17–570 cm3). The mean OV was 46.7% and ranged from
11% to 99% (Fig. 1).
Table 1. Patient demographics
GenderMale 13 (56.5)Female 10 (43.5)
Age (y)Range 30–81Mean (y) 58
Tumor locationRectum 20 (87)Anus 3 (13)
Stage by locationRectum
T3N0 (IIA) 12 (60)T4N0 (IIB) 2 (10)T3N1 (IIIB) 1 (5)T2N2 (IIIC) 1 (5)T3NxM1 (IV) 3 (15)TxNxM1 (IV) 1 (5)
AnusT3N0 (II) 2 (67)T3N2 (III) 1 (13)
Values are number (percentage) unless otherwise noted.

158 I. J. Radiation Oncology d Biology d Physics Volume 69, Number 1, 2007
Table 2. PET volume, CT volume, overlap volume, and overlap percentage
Patient no. Site Stage CT volume (cm3) PET volume (cm3) Overlap volume (cm3) Overlap (% of CT volume)
1 Rectum TxNxM1 62 48 36 582 Rectum T3NxM1 105.8 31.2 25.7 243 Rectum T3N0Mx 29.6 18.3 10 344 Rectum T3N0Mx 82 23 16 205 Rectum T3N0M1 47 50 26 556 Rectum T3N0Mx 62 49 32 527 Rectum T3N0Mx 121 141 84 698 Rectum T3N0Mx 22.4 2.9 15.1 679 Rectum T3N0Mx 56.9 37.1 21.9 38
10 Rectum T3N0Mx 24 25 3 1311 Rectum T3N0Mx 119 139 84 7112 Rectum T3N0Mx 117 77 60 5113 Rectum T3N1Mx 32 4 4 1114 Rectum T2N2Mx 68 27 23 3415 Rectum T3N0Mx 66 34.7 27.6 4216 Rectum T3N0Mx 170 169 49 2917 Rectum T4NxMx 156 119 70 4518 Rectum T3N0Mx 37 32 21 5719 Rectum T4N0Mx 197.1 127.7 92 4720 Rectum T3N0M1 50 26 23 4621 Anal canal T3N0Mx 570 859 562 9922 Anal canal T3N0Mx 17 16 10 5923 Anal canal T3N2Mx 79 52 43 55
Abbreviations: PET = positron emission tomography; CT = computed tomography.
Correlation between CT and PET volumes andoverlap volumes
The majority of patients had PET or CT volumes between
0 and 200 cm3, but initial analysis revealed the presence of
a single patient with rectal cancer whose PET volume was
859 cm3 and CT volume was 570 cm3. To account for the in-
fluence of this patient on the results, statistical analyses were
performed both including and excluding his data.
As tumor volume increased on CT or PET imaging, so too
did OV in a statistically significant fashion ( p < 0.001). This
result was observed and remained significant if the outlier pa-
tient was excluded ( p < 0.001). In addition, as the size of the
tumor increased, there was a significant correlation between
the PET and CT volumes (R2 = 0.94, p < 0.0001) that was still
present without the outlier (R2 = 0.75, p < 0.0001).
The overlap percentage was calculated as a percentage of
OV to CT tumor volume and was intended to determine
how much of the OV corresponded to the PET vs. CT volume
(Fig. 1). As both PET and CT volumes increased, there was
Overlap Percentage of CT Volume
0%
20%
40%
60%
80%
100%
120%
1 3 5 7 9 11 13 15 17 19 21 23Patient
% O
verla
p
Fig. 1. Overlap percentage of computed tomography volume.
a statistically significant correlation between the PET volume
and overlap percentage or CT volume and overlap percentage.
However, the statistical significance of these findings was not
maintained once the outlier patient was removed from analy-
sis. This suggests that when tumor volumes are small on either
imaging modality (between 0 and 200 cm3), there may be
wide variation between the locations of the primary tumor
on PET as compared with CT, but as volumes become larger,
the degree of correlation becomes more pronounced.
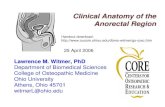
Figure 2 illustrates the radiation portals of a patient with
T3N0 adenocarcinoma of the rectum whose planning fields
underwent significant change as a result of PET data.
Colonoscopy revealed a mass that originated 4 cm from
the anal verge; the colonoscope could only be advanced
to 7 cm, thus the superior aspect was not visualized. The
initial PET scan demonstrated an SUV uptake of 16 within
the lesion. The posttreatment PET-CT scan showed a small
focus in the inferior rectum with an SUV of 3.3. Unfortu-
nately, the patient did not present for surgery to allow for
pathologic correlation, but the dramatic change in SUV
supports tumor instead of inflammation in the area of
FDG avidity.
Impact on radiation treatment planningIn 4 of 23 patients (17%; one anal canal tumor and three
rectal tumors), integration of the PET volume with the plan-
ning volumes resulted in a change in the PTV. Twenty-six
percent of patients (6 of 23) experienced a change in the
radiation treatment-planning process. Changes included
increasing field sizes because traditional fields would have
cut through a contoured PET tumor volume or changing

PET-CT fusion for anorectal tumors d C. ANDERSON et al. 159
Fig. 2. Radiation field change as a result of positron emission tomography (PET) data for a patient with T3N0 adenocar-cinoma of the rectum. Colonoscopy described a mass 4 cm from the anal verge. Note the location of the anterior border ofthe lateral field on the image on the right based on computed tomography gross tumor volume (CT GTV) (blue) comparedwith PET GTV.
a treatment course from definitive to palliative because of the
detection of distant metastases.
Impact on overall managementFor the 20 patients with rectal cancer, PET imaging
resulted in a change in overall management of 5 patients
(25%), predominantly by avoiding unnecessary surgery and
early detection of distant metastases. Positron emission
tomography findings did not impact the overall treatment
for any of the patients with anal carcinoma.
Postradiation preoperative PET-CT and pathologicfindings in patients with rectal primaries
Fourteen of 20 patients (70%) with rectal primaries
received a PET-CT scan 2 weeks after the completion of ra-
diotherapy to assess tumor response. In all patients, the SUV
decreased in the location of the tumor from a range of 10–25
to 5–7, representing a mean change of 66%.
Of the 15 patients who remained candidates for surgery,
10 underwent surgical resection. Subset analysis was
performed to determine whether the change in degree of
PET avidity from pretreatment to posttreatment imaging
could be predictive of pathologic downstaging and, thus,
save some patients from an unnecessary surgery (Table
3). Results indicated that 100% of patients (5 of 5) who
had a pretreatment PET SUV >10 and a posttreatment
PET SUV <6 achieved pathologic downstaging after neoad-
juvant therapy with negative lymph nodes and #T3 tumors
( p = 0.047, Fisher’s exact test). The mean SUV change in
these patients was 68%, which is not sufficiently different
from the overall mean change to assist in clinical decision
making.
When pathologic reports of patients who underwent sur-
gery were compared with the results of posttreatment PET-
CT scans, discrepancies were noted in 3 of 9 patients
(33%) with regard to nodal staging. All 3 patients’ posttreat-
ment scans indicated there had been metabolic improvement
of the rectal primary mass and no hypermetabolic regional
adenopathy. However, pathologic specimens in each case
demonstrated positive regional lymph nodes and residual vi-
able tumor. Although this represents discordance in the nodal
disease in one third of the patients, the small number of

160 I. J. Radiation Oncology d Biology d Physics Volume 69, Number 1, 2007
Table 3. PET changes after chemoradiation for rectal cancer and pathologic findings
Patient no. Pretreatment SUV Posttreatment SUV % SUV changePretreatment SUV >10 and
posttreatment SUV <6 Pathologic stage
2 14.7 7.4 50 No T3N13 10 5.8 42 Yes T3N04 29.2 17.8 39 No T3N06 15.9 5.5 65 Yes T1micN08 23 7 70 No T3N19 6 0 100 No T3N1
12 10.6 5 53 Yes T3N015 14.9 0 100 Yes T1micN016 16 3.3 79 Yes T0N019 19.1 8 58 No T4N0
Abbreviation: PET = positron emission tomography; SUV = standardized uptake value.
patients in this subset analysis precludes calculation of sensi-
tivity and specificity.
All 4 patients who demonstrated distant metastatic disease
at the time of diagnosis received follow-up imaging. The 2 pa-
tients with presumed lung or para-aortic metastases showed
resolution at the primary site but eventual progression of dis-
ease in the suspected areas. The patient with an additional
colon lesion and the patient with liver lesions demonstrated
worsening disease at these locations at first follow-up.
Postradiation PET-CT findings in patients with analprimaries
For the 2 patients with Stage II anal carcinoma, PET-CT
imaging showed improved metabolic uptake within the pri-
mary lesion at the time of first follow-up scan. Persistent
thickening was noted on a follow-up CT scan for the patient
with Stage IIIB disease.
DISCUSSION
Combined-modality PET-CT is increasingly being applied
in oncology to assist with initial staging of tumors as well as
monitoring response to therapy in several disease sites. This
has translated into increased incorporation of combined-mo-
dality PET-CT into radiation oncology for treatment planning
(13). There are several benefits for using a combined PET-CT
over a PET or CT scan alone. Most notably, a combined scan
provides a noninvasive way to assess a tumor’s biologic activ-
ity and incorporates spatial localization to help improve stag-
ing accuracy. For colorectal cancer, PET-CT has an accuracy
between 83% and 93% for initial staging, a 96% sensitivity
and 97% specificity for local recurrence, and a 95% sensitivity
and 98% specificity for detecting distant metastases (14, 15).
For cancer of the anal canal, the sensitivity and specificity of
PET have not been fully determined.
There are few studies on the impact of PET-CT data on the
radiation management of these lesions. The primary endpoint
of this investigation was to assess the impact of PET-CT fu-
sion on both the radiotherapy planning and overall manage-
ment of patients with anorectal tumors. Specifically, we
compared the overlap between tumor volumes contoured on
the PET and CT images and then calculated the frequency
with which the contours led to a change in radiation field
design.
Mean PET and CT volumes were quite similar, but the
ranges and median volumes differed more dramatically. The
CT-GTVs tended to be larger than what was contoured on
PET. There are several potential explanations for this observa-
tion. If it is difficult to distinguish between malignant and re-
active tissues on CT imaging, an over-definition of the true
GTV can occur. In contrast, areas that display high avidity
for FDG on PET imaging often have sharper borders that
can help in GTV contouring. Conversely, the inability of
a portion of tumor to uptake FDG secondary to hypoxia or
necrosis can falsely underestimate an area at risk. This is par-
ticularly troublesome if the rim of residual tumor cells is less
than 1 cm thick because of the resolution limitations of the
PET scanner.
The distinction between inflammation, physiologic bowel
activity, and tumor can be difficult to interpret on PET-CT as
well. In our study, SUV was used as the method to determine
whether an area represented malignancy when the PET-CT
scans were initially interpreted. During the contouring, we
relied on a visual assessment of the tumor to generate the
PET-GTV. Recently, the National Cancer Institute issued
consensus recommendations for the use of PET imaging to
determine response to therapy for patients with cancer (16).
The investigators discussed the advantages and disadvan-
tages of the different methods for assessing FDG uptake,
including the SUV and visual methods. Visual interpretation
was considered the easiest method but can also be subjected to
reader interpretation. In contrast, SUV assessment provides
a semiquantitative method for analysis but can be defined
numerous ways and requires attenuation correction. No con-
sensus guidelines were set to recommend one method over
another, and both remain acceptable. All of our patients with
rectal primaries who received a posttreatment PET-CT scan
showed a decrease in FDG avidity in their tumors, with a mean
reduction of 66%. This supports the idea that these areas rep-
resented viable tumor instead of inflammation or normal
bowel activity; however, future studies are needed to deter-
mine a more reliable way to make this distinction.

PET-CT fusion for anorectal tumors d C. ANDERSON et al. 161
When the outlier patient was both included and excluded
from analysis, the observation that increases in tumor volume
on either CT or PET lead to increases in the overlap volume
remained statistically significant. The clinical implication of
this finding is that larger tumors are more likely to have over-
lapping CT and PET volumes and are less likely to have in-
adequate tumor volume coverage during radiation treatment
planning. It is also possible that tighter tumor margins can
be used to define the PTV when both the PET and CT tumor
volumes are large. However, the same significance was not
maintained when we correlated overlap percentage to either
CT or PET volumes.
Without inclusion of the outlier patient, the observation
that increases in PET or CT volumes correlated with overlap
percentage no longer retained significance. Again, several
potential explanations can be found. As primary lesions of
the rectum or anus increase in size, their adherence to adja-
cent structures can limit the variability of tumor location
between imaging modalities as a function of peristalsis or
respiration. Furthermore, larger tumors may be more easily
visible for correct contouring on either CT or PET. Thus,
when tumor volumes are small (between 0 and 200 cm3 in
our series), there may be wide variation between the locations
of the primary lesion on PET as compared with CT, but as the
volumes become larger, the degree of correlation becomes
more pronounced.
The lack of a strong correspondence between PET and CT
in patients with smaller primaries can also be due to the pit-
falls of manual coregistration. Meltzer et al. (6) indicated that
this technique can be fraught with limitations when used to
delineate treatment volumes in small areas with dense anat-
omy, such as the head and neck. Although shortcomings of
manual coregistration remain in the management of anorectal
tumors, it may not have the same clinical significance as in
the head and neck.
The potential pitfalls of manual coregistration are avoided
when the CT portion of a PET-CT study is used for radiation
treatment planning, as is the case at our county institution. At
our private facility, the treatment-planning CT is obtained
separately. However, we attempt to minimize the potential
for error by pursuing a PET-to-CT fusion with a 2-mm mar-
gin of error, as is calculated by our fusion software.
It is difficult to assess the impact of not using rectal con-
trast at the time of CT simulation. Because rectal contrast
can cause artifact interference on PET-CT images, we abstain
from using it during the planning CT so that both studies are
performed under nearly identical circumstances. Rectal con-
trast can provide improve delineation of the gross tumor, but
it may not be as helpful in targeting the extraluminal extent of
disease, which is where some field modifications occurred.
The inability to use rectal contrast in both studies, though,
may be a potential limitation of incorporating PET-CT in
treatment planning.
The goal of the overlap percentage was to ascertain
whether the overlap volume tended to correspond more
commonly with the PET or CT volume. The CT volume was
used in the denominator to calculate the overlap percentage
because it is ultimately the CT data set that is used for all
radiation treatment planning. Although including or not
including the outlier patient in this analysis led to mixed sta-
tistical significance, the trend of an increasing overlap per-
centage with increased PET and CT volume was consistent
when all patients were included.
The ultimate clinical significance of this study was to de-
termine the frequency with which the use of PET-CT fusion
altered radiation treatment, overall management, and surgical
outcomes in patients. In our series, 26% of patients experi-
enced a change in the radiation treatment-planning process
either by increasing traditional radiation treatment field sizes
that would have cut through a PET tumor volume or changing
a patient’s overall treatment course from definitive to pallia-
tive. Furthermore, the integration of PET data altered the
PTV in 17% of patients. We believe that this dramatic change
in field design justifies routine use of PET-CT fusion in radio-
therapy planning.
It is important to consider the impact of PET-CT fusion on
the care of patients with rectal and anal primaries separately.
For the 20 patients with rectal carcinoma, the results of PET
imaging altered the management of 25% of patients by de-
tecting distant metastases and avoiding surgery. This sup-
ports the use of PET-CT imaging as part of the routine
initial workup of patients with rectal cancer.
The majority of patients received a posttreatment scan at
2 weeks, and all patients showed a dramatic response to neo-
adjuvant chemoradiation with a decrease in SUV by at least
half in the primary lesions. We sought to determine whether
the degree of response to preoperative therapy noted on
PET-CT imaging could be predictive of pathologic down-
staging. On subset analysis, all patients with advanced tu-
mors whose pretreatment SUV was >10 and posttreatment
SUV was <6 achieved pathologic downstaging (all pathol-
ogy specimens were #T3N0) at the time of surgery. How-
ever, the number of patients in our subset is small, and the
percentage change in SUV between those who experienced
pathologic downstaging and those who did not is not dra-
matic. Thus, we cannot suggest that a certain percent change
exists that may safely eliminate surgery or predict patho-
logic downstaging in patients. Additional investigation in
a prospective fashion with a larger number of patients is
needed.
For patients with rectal primaries who underwent surgical
resection, we compared the results of pathologic reports with
preoperative PET-CT scans. Our results demonstrated the
limitations of PET imaging to define accurately the extent
of involved regional adenopathy. Of 20 patients who under-
went surgery, 3 were thought to have no hypermetabolic
adenopathy after chemoradiation on imaging, but their
pathologic specimens demonstrated positive lymph nodes.
Although our numbers are too small to calculate sensitivity,
specificity, or predictive values, other studies note the limita-
tion of FDG-PET in analyzing lymph nodes, with a sensitivity
of 29% (17). This limitation of PET is understandable be-
cause involved lymph nodes may be too small after treatment
to be adequately characterized by PET. Alternatively, the

162 I. J. Radiation Oncology d Biology d Physics Volume 69, Number 1, 2007
contained tumor cells may have become metabolically less
active and are therefore less FDG avid.
Results for patients with anal primaries were less dramatic;
the number of patients in our series is small. However, few
studies have investigated the utility of PET-CT for manage-
ment of carcinoma of the anus. Of the three patients in our se-
ries, PET-CT fusion altered the radiation treatment planning
in 1 patient during the creation of the initial PTV. This result
is similar to that reported by Ciernik et al. (11), who noted
that incorporation of PET-CT data impacted the size of the
fields designed to treat the primary lesion during the final
boost but did not increase the size of the initial large radiation
fields. Although PET-CT may not commonly change initial
fields, its improved ability to detect nodal disease over CT
alone is significant because this may lead to additional radi-
ation dose to the involved groins.
LimitationsIt is important to note the limitations of our study. Our in-
vestigation involved a small series of patients, the majority of
whom had carcinoma of the rectum, which makes conclu-
sions about the role of PET-CT fusion in the management
of anal primaries less generalizable. At our private institution,
manual coregistration of the PET-CT to the simulation CT
REFER
differed from the practice at our county institution, in which
the CT data set obtained at the time of PET-CT was used for
radiation treatment planning. This certainly can lead to differ-
ences in contours of the GTV and overlap but may represent
what occurs in some clinical practice applications. The clin-
ical significance of the outlier patient could be more clearly
defined if there were more patients with large, locally ad-
vanced tumors. However, because both imaging modalities
provide useful data on the extent of tumor in patients with
anorectal primaries, we advocate incorporating data from
both modalities in radiation treatment planning.
CONCLUSION
We recommend routine use of PET-CT in the initial stag-
ing and workup for patients with cancer of the rectum or anus.
Data gathered from this imaging modality can lead to invalu-
able data on the true extent of the primary lesion and meta-
static spread and can lead to changes in radiation treatment
planning that may alter clinical outcomes. Future studies in-
clude comparison and long-term follow-up to determine the
ultimate clinical impact of PET-CT fusion on management
of patients with anorectal tumors.
ENCES
1. Paulino AC, Koshy M, Howell R, et al. Comparison of CT- andFDG-PET defined gross tumor volume in intensity modulatedradiotherapy for head-and-neck cancer. Int J Radiat OncolBiol Phys 2005;61:1385–1392.
2. Bradley J, Thorstad WL, Mutic S, et al. Impact of FDG-PET onradiation therapy volume delineation in non-small cell lungcancer. Int J Radiat Oncol Biol Phys 2004;59:78–86.
3. Erdi YE, Rosenweig K, Erdi AK, et al. Radiotherapy treatmentplanning for patients with non-small cell lung cancer using pos-itron emission tomography (PET). Radiother Oncol 2002;62:51–60.
4. Zinzani PL, Magagnoli M, Chierchetti F, et al. The role of pos-itron emission tomography (PET) in the management of lym-phoma patients. Ann Oncol 1999;10:1181–1184.
5. Isasi CR, Lu P, Blaufox MD. A meta-analysis of 18F-fluoro-2-deoxy-glucose positron emission tomography in the staging andrestaging of patients with lymphoma. Cancer 2005;104:1066–1074.
6. Metzer CC, Bransetter BF. Review of role of PET-CT fusion inhead and neck cancer. Oncology 2005;19:250–253.
7. Cohade C, Osman M, Leal J, et al. Direct comparison of 18F-FDG-PET and PET-CT in patients with colorectal carcinoma.J Nucl Med 2003;44:1797–1803.
8. Rosen RS, Patel PV, Wahl RL, et al. The role of FDG-PET inthe initial staging of newly diagnosed and untreated colorectalcancer [abstract 1069]. Presented at the 51st Annual Meetingof the Society of Nuclear Medicine; June 19–23, 2004; Philadel-phia, PA.
9. Trautmann TG, Zuger JH. Positron Emission Tomography forpretreatment staging and posttreatment evaluation in cancer ofthe anal canal. Mol Imaging Biol 2005;7:309–313.
10. Cotter SE, Grigsby PW, Siegel BA, et al. FDG-PET/CT in theevaluation of anal carcinoma. Int J Radiat Oncol Biol Phys2006;65:720–725.
11. Ciernik IF, Dizendorf E, Baumert BG, et al. Radiation treatmentplanning with an integrated positron emission and computer to-mography (PET/CT): A feasibility study. Int J Radiat Oncol BioPhys 2003;57:853–863.
12. Thomas C, Kassam Z, Wong W, et al. The influence of positronemission tomography (PET) in changing treatment options inlocally advanced metastatic colorectal cancer [abstract 206].Presented at the 2005 Gastrointestinal Cancers Symposium;January 27–29, 2005; Hollywood, FL.
13. Paulino AC, Johnstone PAS. FDG-PET in radiotherapy treat-ment planning: Pandora’s box? Int J Radiat Oncol Biol Phys2004;59:4–5.
14. Sachelaire I, Kerr K, Ghesani M, et al. Integrated PET-CT:Evidence-based review of oncology indications. Oncology2005;19:481–490.
15. Delbeke D, Martin WH. PET and PET-CT for evaluation ofcolorectal carcinoma. Semin Nucl Med 2004;34:209–223.
16. Shankar LK, Hoffman JM, Bacharach S, et al. Consensus rec-ommendations for the use of 18F-FDG PET as an indicator oftherapeutic response in patients in National Cancer Institute Tri-als. Consensus recommendations for the use of 18F-FDG PETas an indicator of therapeutic response in patients in NationalCancer Institute Trials. J Nucl Med 2006;47:1059–1066.
17. Kantorova I, Lipska L, Belohlavek O, et al. Routine (18)F-FDGPET preoperative staging of colorectal cancer: Comparison withconventional staging and its impact on treatment decisionmaking. J Nucl Med 2003;44:1784–1788.