PERTH & KINROSS CHP COMMITTEE
185
Please note any items relating to Committee business are embargoed and should not be made public until after the meeting PERTH & KINROSS CHP COMMITTEE The Final Meeting of the Perth & Kinross CHP Committee will be held on Tuesday 11 August 2015 in the James Murray Suite, Murray Royal Hospital at 9.00am to 11.30am. Apologies/enquiries to: Mrs Val Aitken, Perth and Kinross CHP. Tel: 01738 459524. AGENDA LEAD REPORT OFFICER NO 1. APOLOGIES Linda Dunion 1.1 DECLARATION OF INTERESTS – AGENDA ITEMS Linda Dunion (verbal) The Chairperson will invite members of the committee to declare any interests in agenda item. The Chairperson will also remind members of the committee to update any changes to the register of interests as recorded on their declaration form. 2. PRESENTATIONS 2.1 Framework for a Person Centred Approach to Support People in Communities Sandra Gourlay/Jane Dernie/Lesley Sinclair 32/2015 (attached) (the Committee is asked to note the progress made towards development of the framework and support integrated care approach) 2.2 Reshaping Care for Older People: Enhanced Community Support Update Report Morag Martindale/Leeann Wright 33/2015 (attached) (the Committee is asked to note the work of the Enhanced Community Support Model and support the continuation of the workstream as a key priority area for the Partnership.) 3. MINUTES OF PREVIOUS MEETING Linda Dunion 3.1 Minute of Perth & Kinross CHP Committee meeting 9 June 2015 (attached) 3.2 Action Point Update (attached) 4. MINUTES OF MEETINGS OF SUB-GROUPS ARE SUBMITTED FOR THE INFORMATION OF THE COMMITTEE, AND THE CONSIDERATION OF ANY RECOMMENDATIONS 4.1 Safety, Clinical Governance & Risk Group Meeting 2 June 2015 Morag Martindale (attached) The aim of Perth and Kinross CHP is to improve the health and wellbeing of our communities in P&K as part of the NHS by working with a range of partners. This agenda is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
Transcript of PERTH & KINROSS CHP COMMITTEE
Please note any items relating to Committee business are embargoed and should not be made public until after the meeting PERTH & KINROSS CHP COMMITTEE The Final Meeting of the Perth & Kinross CHP Committee will be held on Tuesday 11 August 2015 in the James Murray Suite, Murray Royal Hospital at 9.00am to 11.30am. Apologies/enquiries to: Mrs Val Aitken, Perth and Kinross CHP. Tel: 01738 459524. AGENDA LEAD REPORT OFFICER NO 1. APOLOGIES Linda Dunion
1.1 DECLARATION OF INTERESTS – AGENDA ITEMS
Linda Dunion (verbal) The Chairperson will invite members of the committee to declare any interests in agenda item. The Chairperson will also remind members of the committee to update any changes to the register of interests as recorded on their declaration form.
2. PRESENTATIONS 2.1 Framework for a Person Centred Approach to Support People in Communities Sandra Gourlay/Jane Dernie/Lesley Sinclair 32/2015 (attached) (the Committee is asked to note the progress made towards development of the framework and support
integrated care approach)
2.2 Reshaping Care for Older People: Enhanced Community Support Update Report Morag Martindale/Leeann Wright 33/2015 (attached)
(the Committee is asked to note the work of the Enhanced Community Support Model and support the continuation of the workstream as a key priority area for the Partnership.)
3. MINUTES OF PREVIOUS MEETING Linda Dunion 3.1 Minute of Perth & Kinross CHP Committee meeting 9 June 2015 (attached) 3.2 Action Point Update (attached) 4. MINUTES OF MEETINGS OF SUB-GROUPS ARE SUBMITTED FOR THE INFORMATION OF
THE COMMITTEE, AND THE CONSIDERATION OF ANY RECOMMENDATIONS
4.1 Safety, Clinical Governance & Risk Group Meeting 2 June 2015 Morag Martindale (attached) The aim of Perth and Kinross CHP is to improve the health and wellbeing of our communities in P&K as part of the NHS by working with a range of partners. This agenda is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP

5. SERVICE DELIVERY & REDESIGN/HEALTH IMPROVEMENT/PATIENT CENTRED/HEALTH INEQUALITIES 5.1 Primary Care Update Angela Cunningham 34/2015 (attached) (the Committee is asked to note the updates and to support the continued work to achieve what has been
proposed) 5.2 Update Alcohol Drug Partnership (ADP) Strategy Ian Smillie 35/2015 (attached)
(the Committee is asked to note the activity undertaken to date in the development of the Perth & Kinross ADP Strategy and the planned next steps for the further development of the Strategy.)
5.4 Local Delivery Plan Lorraine Marshall 36/2015 (attached) (the Committee is asked to note the report) 6 HEALTH & SOCIAL CARE INTEGRATION 6.1 Health & Social Care Integration Update Bill Nicol (verbal)
6.2 Perth & Kinross Integrated Care Fund Julieann Flynn 37/2015 (attached) (the Committee is asked to support
• the aims and objectives of the Integrated Care Fund • the management and assurance arrangements • the direction and scope of the programme)
7. GOVERNANCE & ASSURANCE
7.1 Perth & Kinross CHP Performance & Risk Report Alison Wood 38/2015 (attached)
(the Committee is asked to note report)
7.2 Annual Report of Perth & Kinross Safety, Clinical Governance & Risk Group 2014/15 Morag Martindale 39/2015 (attached)
(the Committee is asked to note the report)
7.3 Perth & Kinross CHP – Financial Position to June 2015 Sandy Berry 40/2015(attached)
(the Committee is asked to note • the information contained in this report, • progress made in absorbing savings targets during the year • the ongoing remit of the CHP’s Budgetary Review Group in terms of ensuring the delivery of a
balanced recurring budget • and support the ongoing work underway in the CHP to improve the recurring financial position.)
The aim of Perth and Kinross CHP is to improve the health and wellbeing of our communities in P&K as part of the NHS by working with a range of partners. This agenda is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP

7.4 Final Perth & Kinross CHP Committee Report April – August 2015/16 Alison Wood 41/2015 (attached)
(the Committee is asked to note the report)
7.5 Dissolution of Perth & Kinross CHP – 11 August 2015: Interim Arrangements to 31 March 2016. Alison Wood 42/2015 (attached)
(the Committee is asked to • agree the transitional governance arrangements following the dissolution of CHPs and prior to the
transfer of functions and responsibilities to the Integration Joint Boards • agree that the Interim Lead Officer will direct PKCHP Committee workplan business in line with NHS
Tayside’s governance and management processes • note the timetable of business which will be scheduled to SMT and for onward direction to
management and governance forums as required)
8. INFORMATION Update Papers for information: 8.1 Record of attendance 2015-16 Linda Dunion (attached) Mrs Evelyn Devine Interim Lead Officer Perth and Kinross CHP 11 August 2015 Distribution Members Mr Arthur Andrews, Public Partnership Group Member, Perth & Kinross CHP
The aim of Perth and Kinross CHP is to improve the health and wellbeing of our communities in P&K as part of the NHS by working with a range of partners. This agenda is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP

Mrs Gillian Costello, Associate Nurse Director Dr Morag Curnow, Clinical Dental Director, Perth & Kinross CHP Mrs Jane Dernie, Lead AHP, Perth & Kinross CHP Mrs Evelyn Devine, Interim Lead Officer, Perth & Kinross CHP Councillor Dave Doogan, Local Authority Member Mr Ian Duncan, Community Pharmacist, Perth & Kinross CHP Mrs Linda Dunion, Chairperson, Perth & Kinross CHP Mr Bob Gillespie, Voluntary Services Member Mrs Sandra Gourlay, Lead Nurse, Perth & Kinross CHP Dr John Harper, Consultant Physician, Perth & Kinross CHP Councillor Kate Howie, Local Authority Member Dr Neil McLeod, General Practitioner Mr Raymond Marshall, Area Partnership Forum Representative Dr Morag Martindale, Clinical Director, Perth & Kinross CHP Mrs Maureen Summers, Carers Representative Mrs Sheila Tunstall-James, Vice Chairperson, Perth & Kinross CHP Mr John Walker, Interim Chief Officer, Perth & Kinross Health and Social Care Integration Advisors Mr Sandy Berry, Finance Manager, Perth & Kinross CHP Mr Christopher Smith, Head of Human Resources, Perth & Kinross CHP Attendees Mrs Valerie Aitken, Corporate Services/Business Support Manager, Perth & Kinross CHP Miss Alison Wood, Head of Corporate Services, Perth & Kinross CHP Dave Davidson, Scottish Health Council Tayside, Ashludie Hospital, Victoria Street, Monifieth, Angus DD5 4HQ Those who receive papers Ms Jane Duncan, Head of Corporate Communications, NHS Tayside Lesley McLay, Chief Executive, NHS Tayside Mr Bill Nicoll, Director of Community Services, NHS Tayside
The aim of Perth and Kinross CHP is to improve the health and wellbeing of our communities in P&K as part of the NHS by working with a range of partners. This agenda is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
Please note any items relating to Committee business are embargoed and should not be made public until after the meeting
Item Number 2.1
Report Number 07/2015
Perth and Kinross CHP Committee 11 August 2015
Framework for a Person Centred Approach to Support People in Communities 1. SITUATION AND BACKGROUND
This report is to inform and update Perth and Kinross CHP Committee around the production of a Framework for a Person Centred Approach to support people in communities
The Framework has been developed jointly between Health and Social Care Colleagues and is seen as a key tool to help teams developed a shared approach for joint working. The development of this Framework was instigated by the Joint Integrated Leadership Team. Personalisation and Person Centred Care was a shared theme of the group and a topic that was prioritised to be worked on together in preparation for increased joint working. Leadership from both Health and Social Care was identified and a working group was initiated on the 27th October 2014. Initially the working group explored each organisations understanding and journey around the personalisation agenda. Staff involved with delivery of care feed in to the group and this exercise demonstrated the need for a shared document that pulled together the approach teams should adopt when they work together to ensure a person centred intervention. The working group looked to examples of good practice and based a lot of its work on the GIREC approach. (Getting it right for every child)
2. ASSESSMENT
The draft Framework (Appendix 1) has been shared at various events to get feedback and input to its content. Consultation with GP’s at GP group, workshop at New Perspectives Event, Older Peoples Standards setting group in NHS Tayside and various staff forums have been undertaken. The working group ran a desktop exercise in February and inputted changes as a result of that and the next step is to test Framework and tool using a Simulated Patient format. This will be run in conjunction with Dundee University and will provide valuable information on what will be required to roll this approach out. See note of PDSA for test. (Appendix 2)
1 This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held

Once tested and refined the working group would recommend its adoption across locality teams in Perth and Kinross. Support to spread and lead staff in its adoption may be vital to its success.
3. RECOMMENDATION Committee is asked to note the progress made towards development of the framework to support integrated care approach. Support the next steps. 4. REPORT SIGN OFF Evelyn Devine, Interim Lead Officer, Perth & Kinross CHP
Jane Dernie AHP Lead 10 July 2015
2 This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held
Appendix 1
May 2015
Framework for a Person Centred Approach to Support People in Communities
Creating a shared understanding of personal outcomes which enable a person centred approach to be taken with individuals in their communities
3 This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held

Contents Vision ..................................................................................................................................... 5
What Getting it Right for every Adult means ............................................................................... 5
For Practitioners .................................................................................................................. 5
For Managers across Health and Social Care services ............................................................... 5
GIRFEA Principles ..................................................................................................................... 6
Measuring Outcomes ............................................................................................................... 7
Indicators of Wellbeing ......................................................................................................... 7
Key components required within Integrated Care Teams ............................................................. 8
Objectives of the Partnership ................................................................................................ 8
Partnership Values ............................................................................................................... 8
Primary Contact and Lead Professional ...................................................................................... 9
Definition of Primary Contact ................................................................................................ 9
Definition of Lead Professional ............................................................................................ 10
Appendix 1 Wellbeing Web Tool .............................................................................................. 11
4 This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held

Vision “I can plan my support with people who work together to understand me and my carer(s), allow me control, and bring together services to achieve the outcomes important to me.” What Getting it Right for every Adult means: They will feel confident about the help they are getting They understand what is happening and why They have been listened to carefully and their wishes have been heard and understood They are appropriately involved in discussions and decisions that affect them They can rely on appropriate help being available as soon as possible They will have experienced a more streamlined and co-ordinated response from practitioners For Practitioners: Putting the person at the centre and developing a shared understanding within and across
agencies Using common tools, language and processes, considering the individual person as a whole,
and promoting closer working where necessary with other practitioners For Managers across Health and Social Care services: Providing leadership and strategic support to implement the changes in culture, systems and
practice required within and across agencies to implement Getting it Right for Every Adult Planning for the transition as staff in agencies move from the current working processes to
the new person-centred processes
5 This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held

GIRFEA Principles Where carers are mentioned, this includes any significant other individual within the person’s life. 1. Promoting the wellbeing of individual adults & older people
This is based on understanding how adults & older people function within their own families and communities, and addressing their needs at the earliest possible time.
2. Keeping adults & older people safe Emotional and physical safety is fundamental and is wider than adult protection
3. Putting the individual at the centre Individuals should have their views listened to and they should be involved in decisions that affect them
4. Taking a whole person approach Recognising that what is going on in one part of an individual’s life can affect many other areas of his or her life
5. Building on strengths and promoting resilience Using an individual’s existing networks and support where possible
6. Promoting opportunities and valuing diversity Everyone should feel valued in all circumstances and practitioners should create opportunities to celebrate diversity
7. Providing additional help that is appropriate, proportionate and timely Providing help as early as possible and considering short and long-term needs
8. Supporting informed choice Facilitating individuals and their families to be able to choose how they live their life, where they live and what they do. People should have control of their support by determining and executing the who, what, when and how of that provision
9. Working in partnership with families/ carers Facilitating, wherever possible, those who know the adult or older person well to achieve their outcomes
10. Respecting confidentiality and sharing information Sharing information that is relevant and proportionate while safeguarding the individual’s right to confidentiality
11. Promoting the same values across all working relationships Recognising respect, patience, honesty, reliability, resilience and integrity are qualities valued by individuals, their families and colleagues
12. Making the most of bringing together each worker’s expertise Respecting the contribution of others and co-operating with them, recognising that sharing responsibility does not mean acting beyond a worker’s competence or responsibilities
13. Co-ordinating help Recognising that adults, older people and their families benefit from practitioners working together, where appropriate, to provide the best possible help
14. Building a competent workforce to promote an individual’s wellbeing Committed to continuing individual learning and development and improvement of inter-professional practice.
6 This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held

Measuring Outcomes
Indicators of Wellbeing I am healthy • staying well • spending time outside • getting help when ill • exercising to keep healthy • healthy diet • understanding and managing long term conditions I feel supported • by carers • living in a home that is clean and warm • my carers are supported • having social contact • getting help to stay in my home • having choice in the support provided • having someone to trust • with my financial affairs I am active • doing things that are enjoyable • taking part in leisure activities • exercising to keep healthy • trying new things • getting out and about • am responsible • responsible for making decisions • responsible for my own actions • responsible for valuing and respecting other people I feel respected • being listened to • involved in making decisions • helped to communicate • my carers are included • relationships with family and friends maintained • my cultural, ethnic, religious and sexual needs are valued • my routines are maintained I feel safe • protected from harm • not scared to go out • managing my money • managing my medication • controlling who comes into my home • having a safe place to go • involved in managing risks and dangers • adult protection risks are identified, recognised, responded to and reduced
7 This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held

I am achieving • achieving full potential • having hobbies and interests • living as independently as I can • knowing where to get help • spending time with friends and family • learning new things/having a job I feel included • maintaining positive friendships and relationships • participating in community activities • feeling cared for by family and friends • having opportunities to meet new people • valued as part of the community • involved in making decisions I am responsible • responsible for making decisions • responsible for my own actions • responsible for valuing and respecting other people
Key components required within Integrated Care Approach
Objectives of the Partnership The aim of the (ICA) is to enhance the partnership work between Agencies/Organisations to achieve positive outcomes for individuals with complexity of needs in order they can live healthier and safer lives in their community.
Partnership Values The ICA relationship will be based on:- • Equality; • Mutual respect and trust; • Open, honest and transparent communication; • Co-operation and consultation; • A commitment to achieving positive outcomes for service users; • A willingness to work in partnership and promote inter-agency learning; • A shared commitment to providing excellent services to the community; and • A desire to make the best use of resources • Promote a recovery orientated system. And will ensure that: • Team members to be supported by training in person centred approaches • Team members to understand and respect the unique roles of team members. • Team structures identified with referral routes and roles and responsibilities identified. • Teams to identify communication routes and structures. • Lead professional model recommended.
8 This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held
The SHANARRI outcome measurement tool adapted from the Angus model will be used as the core tool within Integrated Care Approach (ICA). However there will be a number of additional outcome measurement tools that will be appropriate for use depending on the individual’s health & wellbeing status, for example, the use of Richter in Drugs & Alcohol Services, the Goal Attainment Score in Occupational Therapy and the Palliative Performance Indicator (PPI) in Specialist Palliative Care
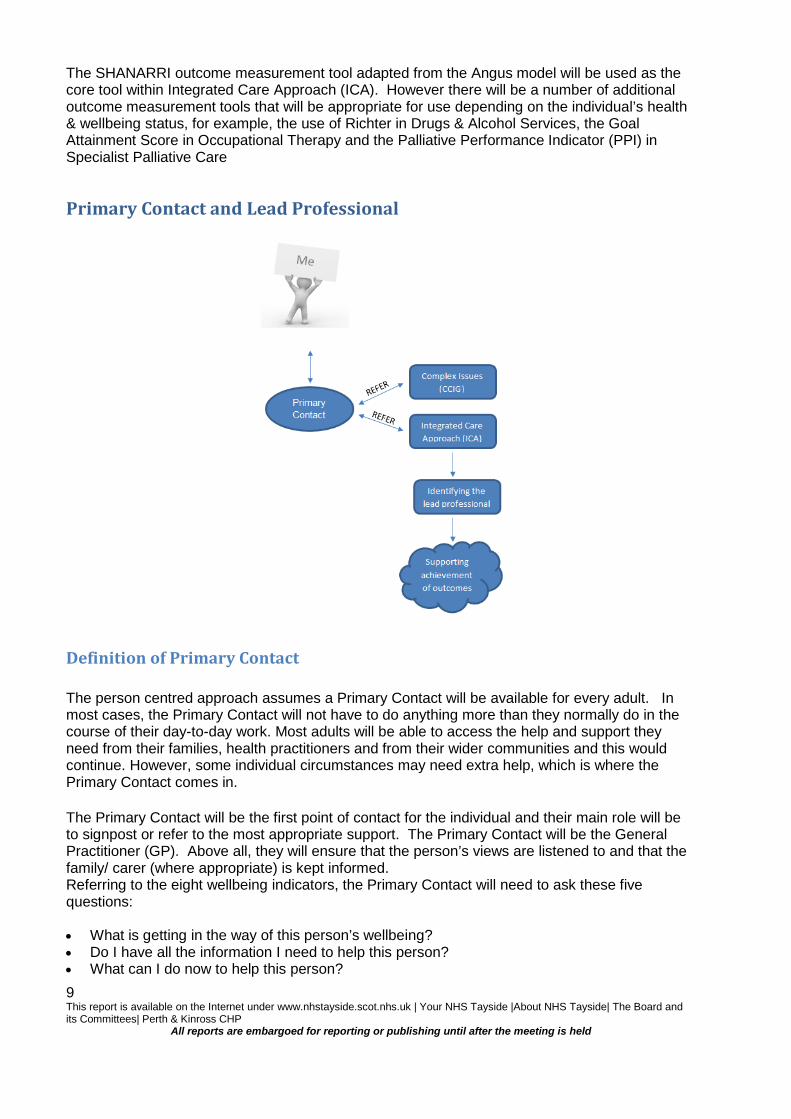
Primary Contact and Lead Professional
Definition of Primary Contact
The person centred approach assumes a Primary Contact will be available for every adult. In most cases, the Primary Contact will not have to do anything more than they normally do in the course of their day-to-day work. Most adults will be able to access the help and support they need from their families, health practitioners and from their wider communities and this would continue. However, some individual circumstances may need extra help, which is where the Primary Contact comes in.
The Primary Contact will be the first point of contact for the individual and their main role will be to signpost or refer to the most appropriate support. The Primary Contact will be the General Practitioner (GP). Above all, they will ensure that the person’s views are listened to and that the family/ carer (where appropriate) is kept informed. Referring to the eight wellbeing indicators, the Primary Contact will need to ask these five questions: • What is getting in the way of this person’s wellbeing? • Do I have all the information I need to help this person? • What can I do now to help this person? 9 This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held
• What can my agency do to help this person? • What additional help may be needed from others?
Definition of Lead Professional When two or more agencies work together to help an adult or older person and their family/ carer who have complex care needs, there will be a Lead Professional to co-ordinate that help. The Lead Professional will: • make sure that the person and their family/ carer fully understand what is happening at each
point so that they can be involved in the decisions that affect them • act as the main point of contact for the individual, practitioners and their family / carer, • promote teamwork between agencies and with individual and their family/ carer • ensure the person’s support plan is implemented and reviewed, accurate and up to date • be familiar with the working practices of other agencies • support other staff who have specific roles or who are carrying out direct work or specialist
assessments • ensure the person is supported through key transition points, particularly any transfer to a
new Lead Professional
10 This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held

Appendix 1 Wellbeing Web Tool
Service User
Date of completion Name of worker
1
2
3
Scaling Key 1 = Not at all true of me 10 = Very true of me
11 This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held
Act Plan
Study Do
Act Plan
Study Do
Appendix 2
MODEL FOR IMPROVEMENT
Objective for this PDSA Cycle: Test of practical application of the “Framework for a person centred approach to support people in communities”
What question(s) do we want to answer on this PDSA cycle? Did it enable the key wellbeing indicators to be defined from the individuals perspective? Did it lead to identification of a lead professional as agreed by the individual? Did it lead to the achievement of a baseline indicator of wellbeing? Predictions: Challenging to identify lead professional Need for training for professionals in this approach/ framework/ outcome focus (rather than output) Framework will be appropriate for practical use in integrated care approach and should be further tested within locality teams
Plan: Undertake sessions using simulated patients with both social and healthcare needs to test the framework, with a Social Worker, District Nurse and OT/Physiotherapist, by the end of June 2015. The session will take place at the ‘Smart House’ in Perth.
Plan for collection of data: The session will be recorded by HCC Communication team. Feedback will be taken from the simulated patient and the professionals involved to evaluate the framework and their experience Did it enable the key wellbeing indicators to be defined from the individuals perspective? Did it lead to identification of a lead professional as agreed by the individual? Did it lead to the achievement of a baseline indicator of wellbeing?
12 This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held
Do: Carry out the change or test; Collect data and begin analysis. Study: Complete analysis of data Act: Are we ready to make a change? Plan for the next cycle
13 This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held
Please note any items relating to Committee business are embargoed and should not be made public until after the meeting
Item Number 2.2
Report Number 33/2015 Perth & Kinross CHP Committee
11 August 2015 Reshaping Care for Older People: Enhanced Community Support Update Report 1. SITUATION AND BACKGROUND
The Enhanced Community Support model (ECS) has been developed to support more complex patients in
their own homes. These patients receive care coordination at a practice level by the primary care team.
Healthcare professionals provide prompt identification and appropriate, timely responses to adult and older
people's health care needs, thus helping to avoid crisis interventions and unnecessary or prolonged
hospital or care home admission.
Delivery of the right amount of care, delivered by the right service, at the right time are essential to provide
person-centred support to patients by a multidisciplinary healthcare team.
Enhanced community support promotes:-
• Proactive identification of at risk/ frail people who are at risk of admission/readmission.
• A practice based MDT approach to supporting complex patients in their own homes.
• Care coordination at a practice level by the primary care team.
• An improvement in professionals capacity to be more proactive and less reactive.
• Improved involvement of patient and carers in the care planning process.
• Improved multidisciplinary working between relevant care services.
• A shift in the Balance of Care from Hospital to Community based services.
• Improved public perception of services and experience of care.
The scope of the project is to:
• To develop and test Enhanced Community Support for adults and older people.
• To work with three practices in two localities to test the model: North - Ardblair Surgery and Perth
City- Glover Street, Victoria Practice and Drumhar, Yellow practice. To scope resource
requirements, referral pathways, processes and procedures, organisational development and
training requirements in order to identify the improvement actions required to develop and test a
robust model .
1 This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held
• To undertake a comprehensive evaluation of project findings taking into consideration all risks,
financial constraints and core services impact.
2. ASSESSMENT ECS model has now been developed and is being refined, based on learning from the pilot sites. Ardblair
Practice has been ‘live’ since 20th January 2015. Glover Street, Victoria practice has been ‘live’ since 20th
April 2015. Yellow Practice Drumhar has been live since 29th June 2015. The model is now well established
in both Ardblair and Glover Street and very positive feedback being received from the staff involved.
A Business case for potential staffing for ongoing rollout of ECS to more practices is being prepared to
ascertain financial commitment.
An initial three month evaluation of the project at Ardblair is attached to this report. The findings are
encouraging with 30 patients receiving a service up to April 2015, 22 of whom have been identified as
receiving care at home as an alternative to hospital admission. A three month evaluation report on Glover
Street activity is due at the end of July 2015. A six month Ardblair evaluation report is due at the end of
August 2015. All involved in the projects are extremely positive about this way of working in relation to both
patient and staff experience. There is clear evidence of integrated working and better outcomes for
patients. 3. RECOMMENDATIONS That Committee note the work of the Enhanced Community Support Model and support the continuation of the work stream as a key priority area for the Partnership.
4. REPORT SIGN OFF Evelyn Devine, Interim Lead Officer, Perth & Kinross CHP
Iona Lancaster Quality and Effectiveness Lead
30 June 2015
2

PERTH & KINROSS ENHANCED COMMUNITY SUPPORT
PROJECT
3
April 2015
Table of Contents 1. Introduction ............................................................................................................................3 2. Background ............................................................................................................................3 3. Project Outcomes and Objectives.........................................................................................4 4. Methods of Evaluation............................................................................................................5 5. Case for Change – Baseline Case Study..............................................................................6 6. Three Month Evaluation Findings.........................................................................................7
6.1 MDT Feedback………………………………………………………………………………………….....7
6.2 Referrals for Crisis prevention and Crisis Management……………………………………………....8
6.3 Length of Stay on Enhanced Community Support………………………………………………….....9
6.4 Early Assessment and Intervention Timescales……………………………………………………... .9
6.5 Main Reason for Admission…………………………………………………………………………….. 10
6.6 Enhanced Community Support Outcome at Point of Discharge……………………………………. 10
6.7 Unplanned Admission, Emergency Bed Days and Admission Reason for Ardblair GP Practice…11
6.8 Change in Risk Level Following Enhanced community support Intervention……………………….11
6.9 Anticipatory Care Plans / Key Information Summary………………………………………………….11
6.10 Medication Reviews……………………………………………………………………………………..12
6.11 Person Centred Goal Achievement post Enhanced Community Support………………………....12
6.12 Team Attendance at Board Rounds and Multidisciplinary Meetings……………………………….12
6.13 Key Worker……………………………………………………………………………………………….12
6.14 Overall Professional Input……………………………………………………………………………….13
6.15 Referral source…………………………………………………………………………………………...13
6.16 Documented Evidence of Multidisciplinary Action Planning…………………………………………14
6.17 Ongoing support………………………………………………………………………………………….14
6.18 Onward Referrals………………………………………………………………………………………...14
6.19 Team survey; Baseline Feedback……………………………………………………………………...15
7. Summary of Findings……………………………………………………………………………. 15
8. Recommendations………………………………………………………………………………….15 Appendix 1 : Enhanced Community Support Evaluation : Data Collection Plan……………………..…16
Appendix 2 : Enhanced community Support Risk Stratification Tool………………………………….…18
4

1. Introduction The aim of Perth & Kinross’s Enhanced Community Support project is to ensure healthcare professionals are in a position to provide prompt identification and appropriate, timely responses to adult and older people's health care needs, thus helping to avoid crisis management and unnecessary or prolonged hospital or care home admissions. Delivery of the right amount of care, delivered by the right service, at the right point in the continuum of care, especially at the interfaces of illness, recovery and independence will be essential to facilitate appropriate multidisciplinary healthcare planning. This in turn will allow us to enable people to maintain their health, independence and well being, for as long as possible. The project’s outcomes are aligned with several of the Scottish Governments draft Health and Social Care Outcomes.
2. Background An Older Peoples Board (OPB) has been set up in NHS Tayside to define the strategic direction and set the quality standards of healthcare for older people in Tayside. They will establish a core data set to measure the quality of whole system performance of care in line with national standards and government targets for older people including those with dementia. As standards are defined by the OPB they will be implemented and embedded by existing Community Health Partnerships and future Health and Social Care Integration Partnerships and Directorate structures across NHS Tayside. The Government’s 20:20 Vision sets out a strategic vision that by 2020 everyone is able to live longer and have healthier lives at home, or in a homely setting. It promotes a focus on prevention, anticipation and supported self-management and supports the ethos that whatever the setting, care should be provided to the highest standards of quality and safety, with the person at the centre of all decisions (A Route Map to the 20:20 Vision for Health and Social Care, Scottish Government 2011). The Quality Strategy sets out an approach that supports the 20:20 vision through the assurance that care will be delivered in a person centred, safe, effective, efficient, equitable and timely manner putting the patient at the heart of our NHS. (The Healthcare Quality Strategy, NHS Scotland, 2010). The direction given by NHS Tayside's Older Peoples Board is that people will be able to live a fulfilled life as part of the community of their choice with support to assist them to achieve this. The Board endorses the progression of new and flexible models of community support to enable this. Therefore Perth & Kinross will work with adults and older people in localities to support positive change by promoting Enhanced Community Support and its central function of proactive care where people are identified to be at risk.
5
3. Project Outcomes and Objectives Outcomes The projects outcomes are aligned with several of the Scottish Governments Health and Social Care
Outcomes:
• Healthier living Individuals and communities are able and motivated to look after and improve their health and wellbeing, resulting in more people living in good health for longer, with reduced health inequalities.
• Independent living People with disabilities, long term conditions or who become frail are able to live as safely and independently as possible in the community, and have control over their care and support.
• Positive experiences and outcomes People have positive experiences of health, social care and support services, which help to maintain or improve their quality of life.
• Carers are supported People who provide unpaid care to others are supported and able to maintain their own health and wellbeing.
• Services are safe People using health, social care and support services are safe- guarded from harm and have their dignity and human rights respected.
• Engaged workforce People who work in health and social care services are positive about their role and supported to improve the care and treatment they provide.
• Effective resource use The most effective use is made of resources across health and social care services, avoiding waste and unnecessary variation
Objectives The following project objectives have been developed from these National outcomes
• To develop ‘Level 2’ of the following tiered, Locality Model structure in line with the NHS Tayside’s Older Peoples Board’s draft strategy for locality models.
6

• Proactive identification of at risk/ frail people who are at risk of admission/readmission and who
meet Enhanced Community Support criteria.
• To support complex patients in their own homes.
• Care coordination at a practice level by the primary care team.
• That the delivery of Enhanced Community Support will make a positive difference in people’s
perception of services and their experience of care.
• Improved involvement of patient and carers in the care planning process.
• Professionals are supported with appropriate training and development opportunities to enable them
to offer enhanced community support to their patients.
• An improvement in professionals’ capacity to be more proactive and less reactive.
• Improved multidisciplinary working between relevant care services.
• A shift in the Balance of Care from Hospital to Community based services.
• To assess the sustainability of further roll out of Enhanced Community Support across P&K
4. Methods of evaluation The multi-perspective and multi-factorial nature of both Enhanced Community Support and the problems it addresses demands a correspondingly comprehensive approach to evaluation. The Matters Framework, represents such an approach. The Matters Framework applies the concepts of person-centredness and continuous improvement to simultaneously harmonise strategy and practice while improving people’s experience, engagement and ownership of services, programs, and interventions. At the heart of the framework is an enhanced understanding of what matters from the “matters perspectives” of: people; the workforce; core experts; service partners; and business decision-makers.
Hospital at Home
Integrated Care (Locality Integrated Care teams)
Enhanced Community Support (Practice based MDT approach)
Universal Care
Level 4
Level 2
Level 3
Level 1
7

Using this whole systems approach a performance framework and evaluation plan were developed to be used for this project. (Please see Appendix 1 for a copy of the evaluation plan).
5. The Case for Change: Baseline case study The following is an example of one of the case studies gathered by staff before the start of the project, to highlight the need for different ways of working. Future reports will include actual project case studies. Case Study
Situation
Elderly lady with a diagnosis of Vascular type dementia who lives at home with her elderly husband as her main carer. Her husband was concerned that she had suddenly become more confused, forgetful and vague. It was also noted that her mobility had deteriorated. The GP commenced antibiotic medication as this lady had, had previous urinary infections.
Action
Antibiotics commenced on Friday afternoon. Home carers visited Saturday morning and were concerned about the patients condition contacted NHS24. Patient was admitted to PRI. Following review in hospital the lady was discharged home on Monday - GP and CPN informed of discharge.
Results Following discharge home and compliance with antibiotics, this patient returned to her previous level of function.
What could have been done differently?
Community mental health team assessment at home in order to provide appropriate advice and support to patient, carer and home carers. To reduce the concern over the weekend period and potentially alleviating need for hospital admission. GP/NHS 24 asked DN (who was also familiar with this lady) to visit over the weekend to assess and support her condition /efficacy of antibiotics during this acute period. Had an anticipatory Care Plan and Key Information Summary been in place then they would have given all the important information about this lady to NHS 24 which would have allowed them to potentially avoid this hospital admission. Had a self management plan for urinary infection been in place in this lady’s home then family and carers would have been aware of the steps to take to manage this condition and who to contact for advice and support.
8
6. Three-Month Evaluation Findings
6.1 MDT Feedback
This feedback provides a sample of professionals’ comments during the initial 3 month period. They clearly demonstrate improvements in patient care, team working, and increased engagement and recognition of the benefits of this new way of working. Early Feedback (first month) “Staff are concerned about looking at the more proactive or amber patients as this could have a huge impact on existing workloads” “There has been increased communication and coordination (of care) for our patients, so the patient journey is slicker” “There has been a reduction in paperwork and time taken for referrals” “There is a big difference to what patients say in hospital and the reality when they get home” (re: Medication Management on discharge) “Some of the GPs are not seeing the benefits of the new way of working yet” Recent Feedback (3 months) “It is so good to be able to address patients’ needs as soon as they arise and have immediate access to the whole MDT” “Team working is improving and all the GPs are now engaging well with this new way of working” “The Medicine for the Elderly Consultant has proved a very useful resource and link with acute services” “We are keeping patients at home who would previously have been admitted and we are working more proactively now”
9

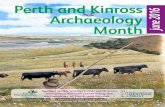
6.2 Referrals for Crisis Prevention and Crisis Management Crisis Prevention and Crisis Management are defined through the use of the P&K Risk Stratification Tool (See Appendix 2). People in the ‘red’ category are considered to be crisis management, and people in the ‘amber’ category are for crisis prevention. Examples of people referred for crisis management (red risk) would be people at risk of hospital admission or readmission with 7 days; and people referred for crisis prevention (amber category) are people at risk of hospital admission within 1 month. This risk tool supports the multidisciplinary teams assessment at the point of referral with a list of criteria for each category and suggested strategies for reducing the risk level and promoting health and wellbeing for the person (See Appendix 2 for full Risk Stratification Tool). Table 1: Referrals for Enhanced Community Support - 12 January 2015 to 15 April 2015. MMM-YY Total Referrals Jan-15 10 Feb-15 8 Mar-15 8 Apr-15* 4 *Part month To date, referral rates are variable on a week to week basis. The team are still learning to proactively identify patients at times when referrals are low. Chart 1: Referrals for Crisis Prevention and Crisis Management - 12 January 2015 to 15 April 2015
10

This chart indicates that 66% of the patients seen to date by the team have been for crisis prevention (amber category). The remaining 33% of people were seen for management of an actual crisis (red category). With time and experience, as the team become more practised in proactive identification of cases for crisis prevention, it is expected that Enhanced Community Support will reduce the need for crisis management (red category) of complex patients. All of the above people were deemed to be at risk of hospital admission. 6.3 Length of Stay on Enhanced Community Support Table 2: Length of Stay on Enhanced Community Support (discharged patients only) - 12 January 2015 to 15 April 2015 Length of Stay
Total (%)
Up to 1 week 10 (40%) Up to 2 weeks 4 (16%) Over 2 weeks 5 (20%) Missing Data* 3 (12%) Total 25 * No date for discharge was recorded; all missing data will be followed up for the 6 month report.
• Overall average length of stay on Enhanced Community Support: 11 days • Overall median length of stay on Enhanced Community Support: 7 days
4
6
5
3
6
2
3
1
0
1
2
3
4
5
6
7
Jan-15 Feb-15 Mar-15 Apr-15
Crisis Prevention Crisis Management
11
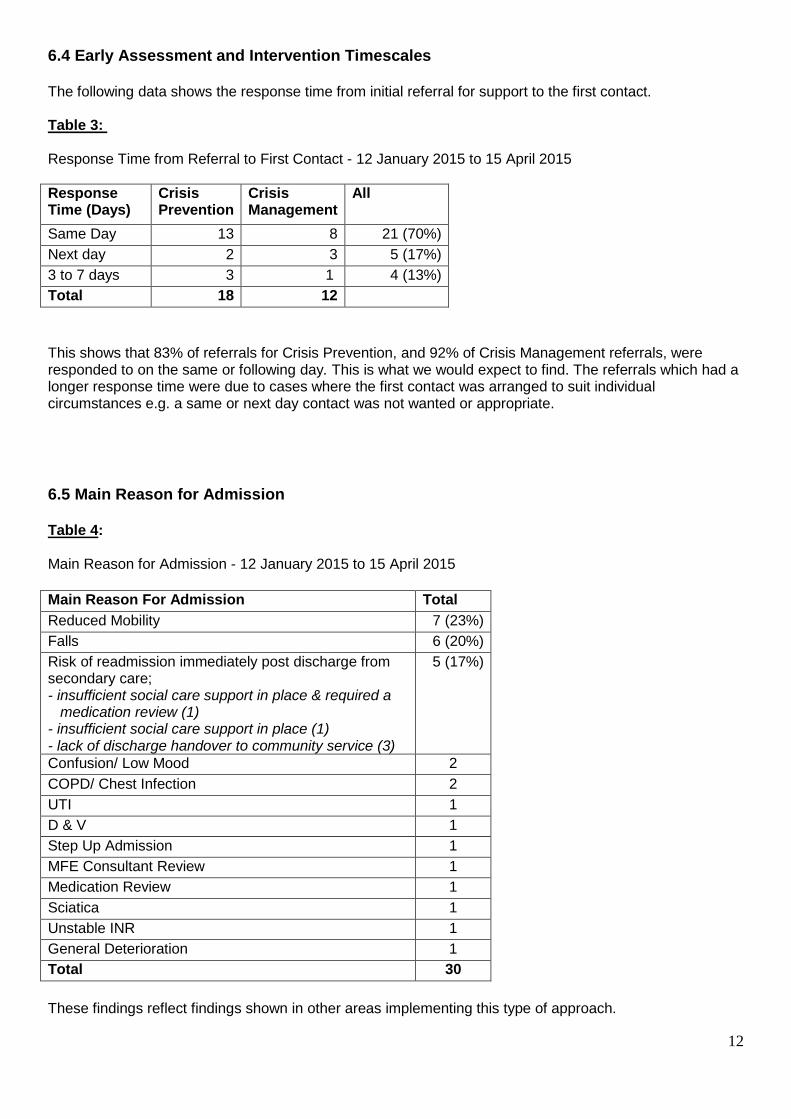
6.4 Early Assessment and Intervention Timescales The following data shows the response time from initial referral for support to the first contact. Table 3: Response Time from Referral to First Contact - 12 January 2015 to 15 April 2015 Response Time (Days)
Crisis Prevention
Crisis Management
All
Same Day 13 8 21 (70%) Next day 2 3 5 (17%) 3 to 7 days 3 1 4 (13%) Total 18 12 This shows that 83% of referrals for Crisis Prevention, and 92% of Crisis Management referrals, were responded to on the same or following day. This is what we would expect to find. The referrals which had a longer response time were due to cases where the first contact was arranged to suit individual circumstances e.g. a same or next day contact was not wanted or appropriate. 6.5 Main Reason for Admission Table 4: Main Reason for Admission - 12 January 2015 to 15 April 2015 Main Reason For Admission Total Reduced Mobility 7 (23%) Falls 6 (20%) Risk of readmission immediately post discharge from secondary care; - insufficient social care support in place & required a medication review (1) - insufficient social care support in place (1) - lack of discharge handover to community service (3)
5 (17%)
Confusion/ Low Mood 2 COPD/ Chest Infection 2 UTI 1 D & V 1 Step Up Admission 1 MFE Consultant Review 1 Medication Review 1 Sciatica 1 Unstable INR 1 General Deterioration 1 Total 30 These findings reflect findings shown in other areas implementing this type of approach.
12
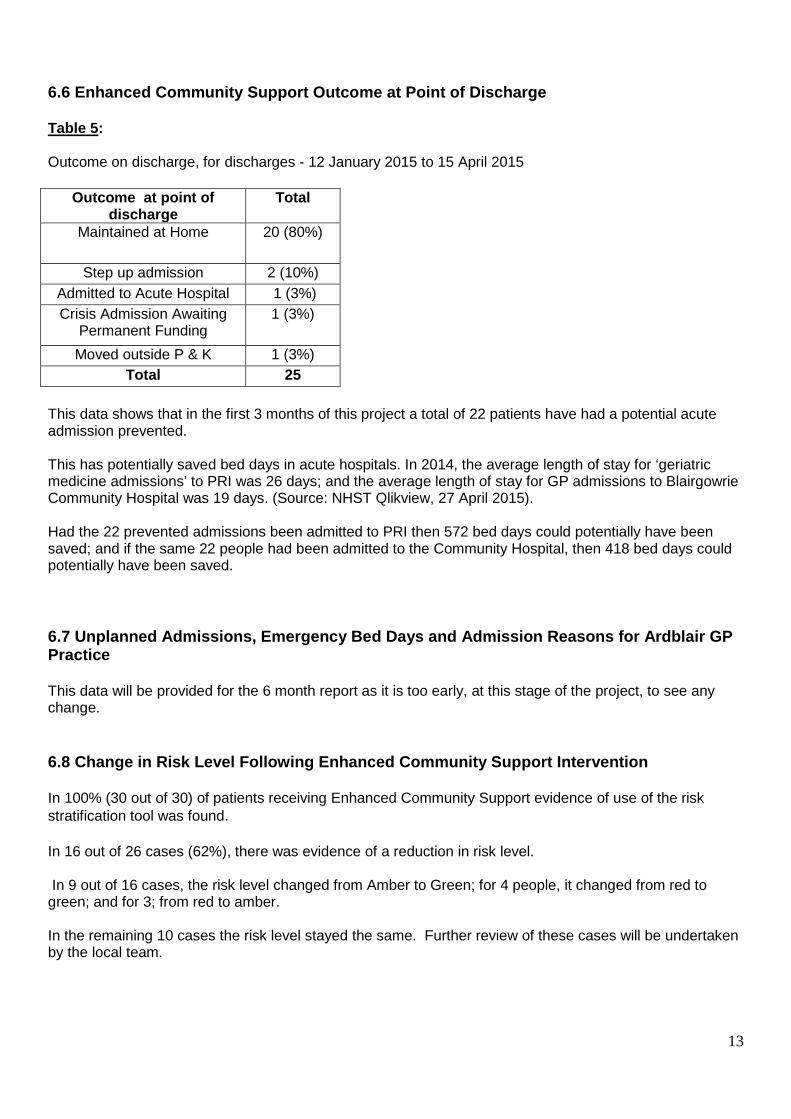
6.6 Enhanced Community Support Outcome at Point of Discharge Table 5: Outcome on discharge, for discharges - 12 January 2015 to 15 April 2015
Outcome at point of discharge
Total
Maintained at Home 20 (80%)
Step up admission 2 (10%) Admitted to Acute Hospital 1 (3%) Crisis Admission Awaiting
Permanent Funding 1 (3%)
Moved outside P & K 1 (3%) Total 25
This data shows that in the first 3 months of this project a total of 22 patients have had a potential acute admission prevented. This has potentially saved bed days in acute hospitals. In 2014, the average length of stay for ‘geriatric medicine admissions’ to PRI was 26 days; and the average length of stay for GP admissions to Blairgowrie Community Hospital was 19 days. (Source: NHST Qlikview, 27 April 2015). Had the 22 prevented admissions been admitted to PRI then 572 bed days could potentially have been saved; and if the same 22 people had been admitted to the Community Hospital, then 418 bed days could potentially have been saved. 6.7 Unplanned Admissions, Emergency Bed Days and Admission Reasons for Ardblair GP Practice This data will be provided for the 6 month report as it is too early, at this stage of the project, to see any change. 6.8 Change in Risk Level Following Enhanced Community Support Intervention In 100% (30 out of 30) of patients receiving Enhanced Community Support evidence of use of the risk stratification tool was found. In 16 out of 26 cases (62%), there was evidence of a reduction in risk level. In 9 out of 16 cases, the risk level changed from Amber to Green; for 4 people, it changed from red to green; and for 3; from red to amber. In the remaining 10 cases the risk level stayed the same. Further review of these cases will be undertaken by the local team.
13
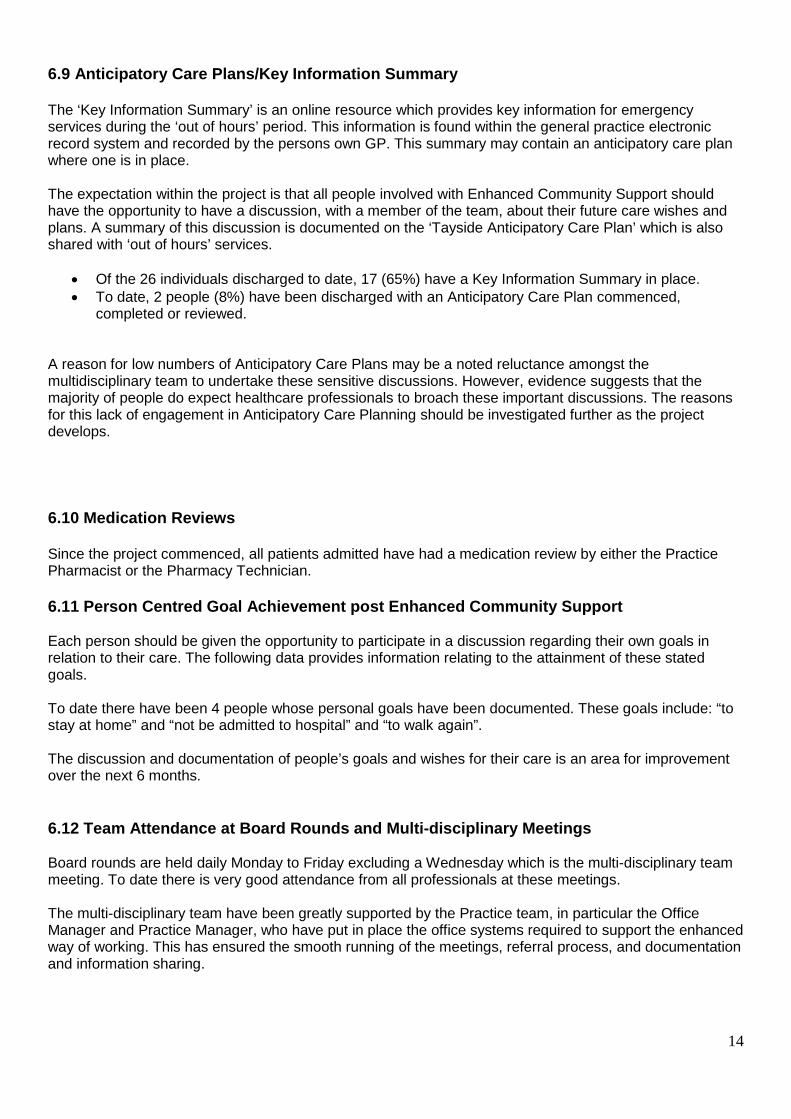
6.9 Anticipatory Care Plans/Key Information Summary The ‘Key Information Summary’ is an online resource which provides key information for emergency services during the ‘out of hours’ period. This information is found within the general practice electronic record system and recorded by the persons own GP. This summary may contain an anticipatory care plan where one is in place. The expectation within the project is that all people involved with Enhanced Community Support should have the opportunity to have a discussion, with a member of the team, about their future care wishes and plans. A summary of this discussion is documented on the ‘Tayside Anticipatory Care Plan’ which is also shared with ‘out of hours’ services.
• Of the 26 individuals discharged to date, 17 (65%) have a Key Information Summary in place. • To date, 2 people (8%) have been discharged with an Anticipatory Care Plan commenced,
completed or reviewed.
A reason for low numbers of Anticipatory Care Plans may be a noted reluctance amongst the multidisciplinary team to undertake these sensitive discussions. However, evidence suggests that the majority of people do expect healthcare professionals to broach these important discussions. The reasons for this lack of engagement in Anticipatory Care Planning should be investigated further as the project develops. 6.10 Medication Reviews Since the project commenced, all patients admitted have had a medication review by either the Practice Pharmacist or the Pharmacy Technician. 6.11 Person Centred Goal Achievement post Enhanced Community Support Each person should be given the opportunity to participate in a discussion regarding their own goals in relation to their care. The following data provides information relating to the attainment of these stated goals. To date there have been 4 people whose personal goals have been documented. These goals include: “to stay at home” and “not be admitted to hospital” and “to walk again”. The discussion and documentation of people’s goals and wishes for their care is an area for improvement over the next 6 months. 6.12 Team Attendance at Board Rounds and Multi-disciplinary Meetings Board rounds are held daily Monday to Friday excluding a Wednesday which is the multi-disciplinary team meeting. To date there is very good attendance from all professionals at these meetings. The multi-disciplinary team have been greatly supported by the Practice team, in particular the Office Manager and Practice Manager, who have put in place the office systems required to support the enhanced way of working. This has ensured the smooth running of the meetings, referral process, and documentation and information sharing.
14

6.13. Key Worker The following data provides information regarding which professionals take the lead on care coordination. This is normally the person with the most input to the patient. Table 6: Key worker for people supported by Team - 12 January 2015 to 15 April 2015 Key Worker Total District Nurse 11 (37%) GP 9 (30%) MFE Consultant 3 (10%) Pharmacy 2 (7%) Physio 2 (7%) OT 2 (7%) Community Mental Health Nurse 1 (2%) Total 30 6.14 Overall Professional Input The following data provides information regarding the input of different professionals to each case. It does not provide a measure of the frequency of contacts, complexity of cases or level of input, but an indication of how many referrals each professional has supported. It therefore cannot be used as a definite measure of resource requirements at the 3-month stage. A more detailed analysis of time and contacts and case complexity for each professional involved per case, will be carried out as part of the 6 month review. It should also be noted that documentation has not always been fully completed. While every effort has been made to fill any gaps for this report, some underreporting may occur in respect of professional input to cases. Table 7: Professional Input to people supported - 12 January 2015 and 15 April 2015 ECS Professional Total GP 19 (63%) District Nurse 17 (56%) OT 17 (56%) Physio 12 (40%) Community MH Nurse
7 (23%)
MFE Consultant 8 (27%) Pharmacy 12 (40%) Practice Nurse 5 (17%)
15

6.15 Referral Source Table 8: Referral Source for people supported by Team - 12 January 2015 and 15 April 2015 Referral Source Total GP 13 (43%) District Nurse 10 (33%) Social Work 3 (10%) Pharmacy 2 (7%) Secondary Care 1 (3%) Older Peoples Mental Health Nurse
1 (3%)
Total 30 6.16 Documented Evidence of Multidisciplinary Action Planning Key to care coordination is evidence that regular professional action planning supports patient centred goals.
• In all appropriate cases (28 out of 30 cases) documented evidence of multi-disciplinary action planning was found. The remaining 2 cases only required the input of one professional and therefore multi-disciplinary action planning was not required. This was evidenced through an audit of the joint documentation.
Planning joint visits, professional assessments or investigations are examples of the types of actions which were documented. 6.17 Ongoing support This is the input required to support the patient after discharge from Enhanced Community Support.
• 12 out of 26 discharged people (46%) required ongoing support with combinations of care package; District Nursing; Community Mental Health Nursing; Medicine for the Elderly Consultant review and Physiotherapy review.
• 6 people remained at home without the need for statutory services. These people self-managed or
had support from informal care. 6.18 Onward referrals These are the referrals made to other services or organisations whilst on Enhanced Community Support and provide information regarding potential interface/s with other services/organisations. However it should be noted that where 3rd Sector services/informal support is used this is not always well documented. A very wide range of referrals have been made at this stage. They include:
16

• Social Work for new care package, increased care package, carers assessment or rapid response • CT Scanning • Speech and Language Therapy • Macmillan Nurses • Symptom Control Clinic • Befriending Service • Urology • Blood Transfusion in Community Hospital • INR Clinic in Community Hospital • Dietician
6.19 The Team Survey: Baseline Feedback This is a questionnaire which has been used to determine a baseline of how well the team is working together. The questionnaire is based on ‘The Team Survey: a tool for health care team development’ (Millward & Jeffries, 2001) and considers collaborative care, communication and team effectiveness. This survey was completed by the multi-disciplinary team during the early stages of the project and will be repeated at nine months when a comparison can be made. Ideally this survey should be completed prior to any project scoping and this will be the case for future project teams. The results indicated that this team believe they are already an effective team in the 3 key survey aspects of collaboration, communication and their perception of their ability to achieve objectives and work with other teams and partners in health and social care. The areas which may be improved over the next 6 months are:
• Team members supporting each other through help and advice when needed or proactively i.e. without being asked;
• The Team’s confidence in solving any problems they encounter • Knowing where to get information
7. Summary of Findings These initial 3 month findings appear to show that the outcomes and objectives of the project are being achieved. People are being supported at home by the right people in a timely manner and multidisciplinary working and communication is much improved. The daily meetings appear to be key to proactive identification of people requiring support. The benefit of the newly established link with a named social worker and their attendance at the weekly Multidisciplinary Team Meeting is also clear. The evidence also suggests the majority of patients supported by the team have a reduced risk of admission to hospital, are appropriately supported in the community environment and that many have returned to their previous or an improved level of independence. There also appears to be evidence of improved multidisciplinary working and communication and staff feedback also shows support for this new way of working.
17
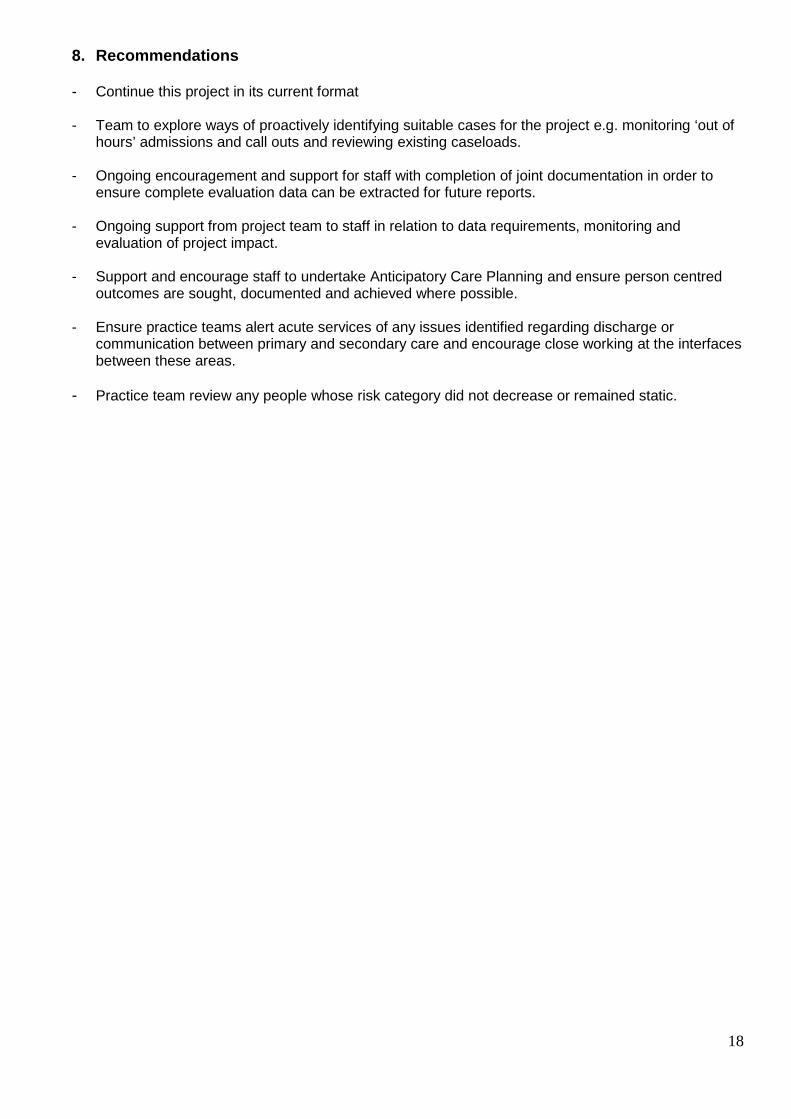
8. Recommendations - Continue this project in its current format - Team to explore ways of proactively identifying suitable cases for the project e.g. monitoring ‘out of
hours’ admissions and call outs and reviewing existing caseloads. - Ongoing encouragement and support for staff with completion of joint documentation in order to
ensure complete evaluation data can be extracted for future reports. - Ongoing support from project team to staff in relation to data requirements, monitoring and
evaluation of project impact. - Support and encourage staff to undertake Anticipatory Care Planning and ensure person centred
outcomes are sought, documented and achieved where possible. - Ensure practice teams alert acute services of any issues identified regarding discharge or
communication between primary and secondary care and encourage close working at the interfaces between these areas.
- Practice team review any people whose risk category did not decrease or remained static.
18

Appendix 1 ECS EVALUATION: Data Collection Plan
Perspective Theme Tool/ Method Sample/ Participants Owner
Phase Periodic (P) Beginning (B) Mid (M) End (E)
Due Date
Person
Patient-held self-management/prevention plans
Proportion of crises where self-management/ prevention plan was used/was not used to avoid crisis. Case audit to identify unsuccessful uses of prevention plan or where use did not prevent crisis (Patient records)
Patients who have had a crisis
KG M, E June 2015 September 2015
Service access appropriateness
Patient interviews to gather evidence of people knowing what to do and who to contact to prevent crisis Semi-structured interviews with suggested themes: Planning for feeling unwell; Relationships with health professionals; Tools for staying well (Patient interviews)
Sample of practice patients
KG B, E
Jan to March 2015 September 2015
Self-management of predicted crisis
Support for self-management for predicted crisis patients- i) Patient activation measure (PAMs) and - individual and aggregated scores ii) Organisational support for self-management (survey questionnaire)
Sample of ECS crisis prevention support patients
KG P Throughout project
Expert
ECS team synergy Core ECS team attendance at MDT/Board round (ECS board round/MDT activity log); ECS team vitality (Team Survey Questionnaire)
ECS team KG
ECS Team attendance- P ECS Team Health- B and E
Throughout project Team Survey: Jan to March 2015 September 2015
Crisis prediction tool effectiveness
Case review of crises where prediction tools did not identify risk of crisis (Patient records)
Patients having had crisis
Core Team with support
M, E June 2015 September 2015
ECS effectiveness Case review of predicted crises- self assessment by core ECS Team; Case review of appropriateness of MDT community crisis prevention (Patient records)
Sample of ECS crisis prevention support patients
Core Team with support
M, E June 2015 September 2015
Clinical effectiveness ECS crisis prevention discharges with achieved clinical goals as a proportion of all discharges (ECS database)
ECS discharges from predicted crisis referrals
KG M, E June 2015 September 2015
Personal -centred goal achievement
Case review of individual goals & actions for crisis prevention (Patient records)
ECS discharges from predicted crisis referrals
Core Team with support
M, E June 2015 September 2015
Partners
Identifying partner crises prediction opportunities
Case review of unpredicted crises (Patient records) Unpredicted crises
Core Team with support
M, E June 2015 September 2015
ECS partnership synergy
Partnership analysis for partners in the crisis prediction & prevention network (PAT)
Collaborating partners KG B, M, E
Jan to March 2015 June 2015 September
19
Perspective Theme Tool/ Method Sample/ Participants Owner
Phase Periodic (P) Beginning (B) Mid (M) End (E)
Due Date
2015
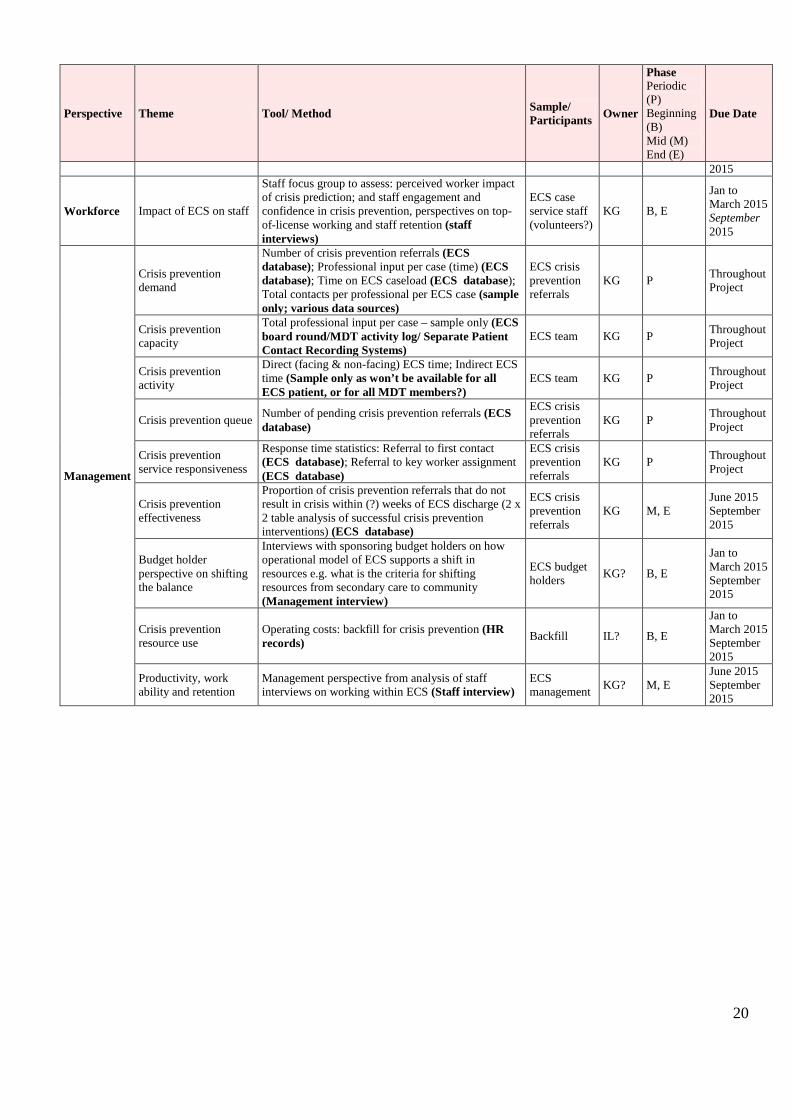
Workforce Impact of ECS on staff
Staff focus group to assess: perceived worker impact of crisis prediction; and staff engagement and confidence in crisis prevention, perspectives on top-of-license working and staff retention (staff interviews)
ECS case service staff (volunteers?)
KG B, E
Jan to March 2015 September 2015
Management
Crisis prevention demand
Number of crisis prevention referrals (ECS database); Professional input per case (time) (ECS database); Time on ECS caseload (ECS database); Total contacts per professional per ECS case (sample only; various data sources)
ECS crisis prevention referrals
KG P Throughout Project
Crisis prevention capacity
Total professional input per case – sample only (ECS board round/MDT activity log/ Separate Patient Contact Recording Systems)
ECS team KG P Throughout Project
Crisis prevention activity
Direct (facing & non-facing) ECS time; Indirect ECS time (Sample only as won’t be available for all ECS patient, or for all MDT members?)
ECS team KG P Throughout Project
Crisis prevention queue Number of pending crisis prevention referrals (ECS database)
ECS crisis prevention referrals
KG P Throughout Project
Crisis prevention service responsiveness
Response time statistics: Referral to first contact (ECS database); Referral to key worker assignment (ECS database)
ECS crisis prevention referrals
KG P Throughout Project
Crisis prevention effectiveness
Proportion of crisis prevention referrals that do not result in crisis within (?) weeks of ECS discharge (2 x 2 table analysis of successful crisis prevention interventions) (ECS database)
ECS crisis prevention referrals
KG M, E June 2015 September 2015
Budget holder perspective on shifting the balance
Interviews with sponsoring budget holders on how operational model of ECS supports a shift in resources e.g. what is the criteria for shifting resources from secondary care to community (Management interview)
ECS budget holders KG? B, E
Jan to March 2015 September 2015
Crisis prevention resource use
Operating costs: backfill for crisis prevention (HR records) Backfill IL? B, E
Jan to March 2015 September 2015
Productivity, work ability and retention
Management perspective from analysis of staff interviews on working within ECS (Staff interview)
ECS management KG? M, E
June 2015 September 2015
20

Appendix 2 RISK STRATIFICATION - Enhanced Community Support Purpose of tool: 1. To identify people at risk of hospital admission
2. To prioritise focus/ actions for the MDTM 3. To assist in monitoring the progress of individuals and outcomes for the MDT
RISK CATEGORY CRITERIA SUGGESTED STRATEGIES
RED Crisis
Management
• At risk of hospital admission/ readmission within 7 days • Acute change/exacerbation in conditions from baseline
status • Change in functional status/decline in condition since last
visit • Timeous discharge from hospital • Carer crisis • Evidence of rapid deterioration in cognitive status • Unexplained falls • Adult at risk of harm • Acute infection
A
sses
s …
…. R
evie
w .…
... E
valu
ate
• Urgent cases discussed/ resolved appropriately out with daily meeting • Assessment / Reassessment • High intensity contact with patient and face to face visit • Consideration of Rapid Access Clinic for the Elderly (RACE) attendance. • Urgent medication review • Initiate referral to appropriate services / liaise with specialist services • Alert OOH services and complete KIS or Adastra • Initiation of diagnostic tests as appropriate, in accordance with SIGN and local
guidelines. • Increased GP collaboration – telephone and/or joint visits • Hospital discharges - Liaison with Front Door Service/Ward • Review and monitor any changes in plan of care with MDT at Board rounds
and weekly MDT meetings Move to AMBER when condition is stabilising
AMBER Crisis
Prevention
• Potential risk of hospital admission/ readmission within 1 month
• Explained falls • Chronic infections • Weight loss/unexplained and/or continued • Evidence of change of condition from baseline • Decline in cognitive status • Breakdown in interagency care continuum • Carer stress/ change in family circumstances • Any patient admitted to a step up bed
• Regular review and monitoring of condition. • Plan care according to patient choices, discuss with appropriate parties. • Patient education – medication, disease process, treatment options, lifestyle
choices • Anticipatory approaches • Self management strategies • Multi-agency review as appropriate Move to GREEN when condition is stable
GREEN
• Stable long term conditions • Ongoing medical & social support of patient and carer • Hospital admission
• Discharge back to mainstream services and if appropriate to the locality Integrated Care Team.
• Routine monitoring and reassessment every 4-6weeks • Multi-agency review as needed • Regular review of self management strategies • Support self management strategies and management plan
Adapted from Lothian COMPASS Team’s Risk Stratification 21

Please note any items relating to Committee business are embargoed and should not be made public until after the meeting Minute NHS Tayside PERTH & KINROSS COMMUNITY HEALTH PARTNERSHIP COMMITTEE Minute of the above meeting held at 9.00am on Tuesday 9 June 2015 in the James Murray Suite, Murray Royal Hospital, Perth. Present Dr Morag Curnow, Clinical Dental Director, Perth & Kinross CHP Mrs Jane Dernie, Lead AHP, Perth & Kinross CHP Mr Ian Duncan, Community Pharmacist, Perth & Kinross CHP Mrs Linda Dunion, Chairperson, Perth & Kinross CHP Mr Jim Foulis, Interim Associate Nurse Director Mrs Sandra Gourlay, Lead Nurse, Perth & Kinross CHP Dr Neil Mcleod, GP Representative, Perth & Kinross CHP Dr Morag Martindale, Clinical Director, Perth & Kinross CHP Mrs Maureen Summers, Carers Representative Mrs Sheila Tunstall-James, Vice Chair, Perth & Kinross CHP Mr Sandy Berry, Finance Manager, NHS Tayside Mr Christopher Smith, Head of Human Resources Apologies Mr Arthur Andrews, Public Partnership Group Member, Perth & Kinross Mrs Evelyn Devine, Interim Lead Officer, Perth & Kinross CHP Councillor Dave Doogan, Local Authority Member , Perth & Kinross Council Mr Bob Gillespie, Voluntary Services Member Dr John Harper, Consultant Physician, Medicine for the Elderly, Perth Royal Infirmary Councillor Kate Howie, Local Authority Member, Perth & Kinross CHP Mr Raymond Marshall, Area Partnership Forum Representative Mr Bill Nicoll, Director of Primary & Community Services, NHS Tayside Mr John Walker, Executive Director of Housing & Community Care, Perth & Kinross Council In Attendance Mrs Valerie Aitken, Corporate Services/Business Support Manager, Perth & Kinross CHP Mrs Julieann Flynn, Head of Children, Young People and Families Services. Mr Chris Lamont, Head of Nursing for Health Improvement & Health Inequalities, Perth & Kinross CHP Ms Karen Melville, Pharmacy Team Leader, Perth & Kinross CHP Miss Lauraine Miller, HR Business Lead, Perth & Kinross CHP Mrs Lindsey Miller, Service Manager Integrated Community Services Ms Sue Muir, Interim Head of Older Peoples Services Mr Rob Packham, Associate AHP Director, NHS Tayside. Mrs Maggie Rapley, Service Manager Psychiatry of Old Age Miss Alison Wood, Head of Corporate Services and Business Support, Perth & Kinross CHP Ms Hong Zhang, Voluntary Services Representative Mrs Linda Dunion in the Chair ACTION 1. WELCOME AND APOLOGIES
The aim of Perth and Kinross CHP is to improve the health and wellbeing of our communities in P&K as part of the NHS by working with a range of partners. This minute is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP 10

Please note any items relating to Committee business are embargoed and should not be made public until after the meeting Minute NHS Tayside 1.1 Declaration of Interests
Mrs Dunion invited the Committee to declare any interests in the items of business on the agenda or any changes to the original Declaration they had submitted so these could be noted by the Board Secretary, Tayside NHS Board, from the minutes. There were no interests to declare.
2. PRESENTATION
2.1
CLINICAL, CARE AND PROFESSIONAL GOVERNANCE FRAMEWORK Rob Packham – Report 20/2015
Rob Packham, Associate AHP Director for NHS Tayside gave a
presentation titled ‘Getting it Right for Everyone’ the Joint Clinical, Care
and Professional Governance Framework for Health & Social Care
Integration (HSCI) in Tayside.
The Joint Framework will underpin best practice through shared standards
and a performance framework across health and social care, primary and
secondary care and to minimise harm associated with unhelpful variations
and drive continous improvements. The framework has been recognised
across the UK as a model for others to follow.
Linda Dunion on behalf of the committee thanked Rob for his informative
presentation. Christopher Smith raised the issue regarding one challenge
around Staff Governance and how do we get one standard to fit across all
workforces. Christopher Smith is interested in being involved in further
discussions around the Staff Governance standards. Due to Maggie
Rapley’s previous involvement in Care Governance Rob stated he would
welcome Maggie’s input. Michelle Watt is currently looking into how the
independent contractors can be included in the shared standards.
The aim of Perth and Kinross CHP is to improve the health and wellbeing of our communities in P&K as part of the NHS by working with a range of partners. This minute is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP 11

Please note any items relating to Committee business are embargoed and should not be made public until after the meeting Minute NHS Tayside
The committee noted the achievements of the working group and supported the formal conclusion of the group. Also noted the proposal for a revised title and the plan to inaugurate and formally constitute the Tayside Joint Professional Forum (R1). The Committee also agreed to provide support to ratify and officially adopt the updated and Sealed Joint Framework for Clinical, Care and Professional Governance across the four partner organisations and to transfer accountability for the progress to the R1 group in the future.
3. MINUTES OF PREVIOUS MEETING
3.1 Minute of Perth & Kinross CHP Committee Meeting 14 April 2015
The Committee requested amendment to Item 2.2, last sentence, contained
in the minutes of the meeting of 14 April 2015. Item should have read
‘ The question around Health checks for carers was also raised however
Paul Henderson informed the committee that the uptake for the service was
minimal, however carers are provided support and signposting to access
Health Checks across the localities’.
Proposed by Sheila Tunstall-James Seconded by Evelyn Devine
3.2 ACTION POINT UPDATE The Committee noted the Action Point Update.
4. MINUTES OF MEETINGS OF SUB-GROUPS ARE SUBMITTED FOR THE INFORMATION OF THE COMMITTEE, AND THE CONSIDERATION OF ANY RECOMMENDATIONS
4.1 Safety, Clinical Governance & Risk Group Meeting – 7 April 2015. Dr M Martindale commended the Prisoner Healthcare Staff with regards the
excellent and accurate note keeping which recently helped when dealing
with a SPSO complaint.
The aim of Perth and Kinross CHP is to improve the health and wellbeing of our communities in P&K as part of the NHS by working with a range of partners. This minute is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP 12
Please note any items relating to Committee business are embargoed and should not be made public until after the meeting Minute NHS Tayside
The Committee noted the minute of the meeting.
5. SERVICE DELIVERY & REDESIGN/HEALTH IMPROVEMENT/PATIENT CENTRED/HEALTH EQUALITIES.
5.1. Perth Royal Infirmary Stroke Update Sue Muir – Report No 21/2015 Sue Muir Interim Head of Older Peoples Services provided an update on
Stroke Services within Perth Royal Infirmary. The committee were
informed how stroke care at PRI has been enhanced by a dedicated stroke
unit, improved patient pathways, more focused specialist treatment,
rehabilitation goal setting, daily patient reviews and proactive discharge
planning. These improvements impact on outcomes for patients, overall
bed usage and patient length of stay.
The committee discussed Perth & Kinross performance against the stroke
care ‘bundle’ target and noted that steps are being taken by NHS Tayside
and partners to manage the delivery of unscheduled and scheduled care.
The Committee endorsed the following recommendations:
• That where possible, capacity is retained in the Stroke Unit at Perth Royal Infirmary to accommodate Stroke patients on day 1 of admission.
• That P&K CHP continues to support partners to find early solutions to enable safe and effective discharge from hospital for patients in the stroke unit and reduce delays in discharge.
• That all efforts to accommodate increased inpatient demand is supported where capacity in the unit allows.
The aim of Perth and Kinross CHP is to improve the health and wellbeing of our communities in P&K as part of the NHS by working with a range of partners. This minute is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP 13
Please note any items relating to Committee business are embargoed and should not be made public until after the meeting Minute NHS Tayside
5.2
Perth & Kinross Psychiatry of Old Age (POA) Services – Post Diagnostic Support Maggie Rapley – Report No. 22/2015 Maggie Rapley, Service Manager for Psychiatry of Old Age provided an
update on the POA Services in Perth & Kinross. NHS Tayside has
successfully adopted and implemented the Alzheimer Scotland 5 Pillar
Model of Post Diagnostic Support (PDS) which was included within
Scotland’s National Dementia Strategy 2013 – 2016.
A Heat Target was introduced in April 2013 – ‘To deliver expected rates of
dementia diagnosis and by 2015/16, all people newly diagnosed with
Dementia will have a miniumum of a year’s worth of post diagnostic support
co-ordinated by a Linkworker, including the building of a person-centred
support plan’. The introduction of Alzheimer Scotland Link Worker
(ASLWs), which are funded through P & K Change Fund monies, has
allowed Perth and Kinross to ensure capacity is found to the meet the
demands of PDS. The Link workers support people living with dementia,
their carers and families. This is promoting self management and person
centred care planning which is better enabling people with dementia to live
independently and positively with dementia in the community. Year three
evaluation is currently being finalised however year one and two
evaluations indicates that this social model is meeting the needs of those
with an early diagnosis of dementia, and has received positive feedback
from service users.
Challenges remain around the methods of recording PDS data across
Tayside, however this is being explored. There is a lot of work ongoing
within GP Practices and there is a need to ensure this data is captured.
The aim of Perth and Kinross CHP is to improve the health and wellbeing of our communities in P&K as part of the NHS by working with a range of partners. This minute is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP 14

Please note any items relating to Committee business are embargoed and should not be made public until after the meeting Minute NHS Tayside
The Committee noted the progress to date on PDS within Perth & Kinross and the ongoing social model supported by ASLW and supported that the evaluation of year three of the ASLW model in support of PDS be presented at the Pathfinder Board/IJB at a future date. The committee also acknowledged that investing in the social aspects of the PDS model delays contact with care specialist services thus promoting self management.
5.3
Central Healthcare/Keepwell Update Chris Lamont – Report 23/2015
Chris Lamont, Head of Nursing for Health Improvement and Health
Inequalities for Perth & Kinross informed committee of the proposed
changes to the Central Healthcare and Keep Well Service delivery. The
Nurse led service has previously delivered health input to specifically those
who are deemed as homeless and/or vulnerable housed across Perth &
Kinross. This is in tandem with the Keep Well Services who deliver health
checks to those in identified post code areas in order to detect high risk
group clients who may develop Cardio Vascular Disease.
In April 2015, a funding bid to the Integrated Care Fund (ICF) was
successful which will help deliver heatlh improvement and early
interventions to those deemed as difficult to engage with and suffering from
health inequalities. Work has already commenced to deliver the planned
Health Improvement Model across Perth & Kinross. Committee members
commented on the need to intervene at an early stage and the need to
develop further links including working with familes and liase with
independent contractors which is in line with HSCI. This is a real
opportunity to target inequalities and develop different ways of working
similar to Enhanced Care Services. Chris agreed to come back at a future
forum with an update on the new model.
The aim of Perth and Kinross CHP is to improve the health and wellbeing of our communities in P&K as part of the NHS by working with a range of partners. This minute is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP 15
Please note any items relating to Committee business are embargoed and should not be made public until after the meeting Minute NHS Tayside
The Committee noted the identified changes which have been introduced and planned. The Commiteee also agreed that further updates and progress reports be submitted to Pathfinder Board/IJB.
6. HEALTH & SOCIAL CARE INTEGRATION 6.1
Health & Social Care Integration (HSCI) Update – Verbal Report Committee members were informed of the progress of Health & Social Care
Integration in Perth & Kinross.
Applications for the Chief Officer post for HSCI in Perth & Kinross has now
closed. The integration scheme, which sets out the arrangements for
integration, is awaiting final approval from the Scottish Government
following the summer recess. The development of the Strategic Plan is
ongoing. The Pathfinder Board is currently analysing data and looking at where
services are to sit within the HSCI. The committee were assured that there
is a great deal of work ongoing behind the scenes to ensure everything is in
place by April 2016.
Committee members who recently attended the ‘New Perspective – New
Opportunities’ HSCI Event informed the meeting that the event was
excellent. The event brought together Health, Social Care and third sector
colleagues and was great to see everyone working together and was very
reassuring for the future Health & Social Care in Perth & Kinross.
6.2
Perth & Kinross Integrated Locality Working Lindsey Miller – Report No 24/15 Lindsey Miller, Service Manager MFTE, Community Hospitals and
Specialist Palliative Care provided update on Integrated Locality Working in
line with the 2020 vision.
The aim of Perth and Kinross CHP is to improve the health and wellbeing of our communities in P&K as part of the NHS by working with a range of partners. This minute is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP 16

Please note any items relating to Committee business are embargoed and should not be made public until after the meeting Minute NHS Tayside
In Perth & Kinross we are focusing on ensuring that people get back into
their home or community environment as soon as appropriate with minimal
risk or readmission. We are putting the person at the centre of everything
we do and ensuring support for our carers.
The aims and objectives of the Perth & Kinross Integrated Care Approach
Groups are to restore and improve quality of life for individuals within our
local communities and will focus on adults over the age of 18 years of age,
but will predominately concentrate on older people presenting with multiple
co-morbidities, and complexity due to frailty and or social support issues.
Sandra Gourlay informed meeting that she has been working on the Person
Centred Framework and is to provide presentation at GP Group this week,
this framework supports the Integrated Care Approach. Lindsey Miller
provided presentation at recent GP Protected Learning Time (PLT) event to
share information on developments with regards to the Integrated Care
Approach.
The Community agreed to support the ongoing development of an Integrated Care Approach which will work to meet the needs of our more complex population in our communities and localities and support the Scottish Governments 2020 Vision.
6.3 Update on OT Integration Jane Dernie – Report No 25/2015
Jane Dernie, Lead AHP, presented update on OT Integration.
A project team in now in place and are overseeing the delivery of the
project plan. The integration project is being led by the Occupational
Therapy Integration Implementation Manager with the support of a Project
The aim of Perth and Kinross CHP is to improve the health and wellbeing of our communities in P&K as part of the NHS by working with a range of partners. This minute is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP 17

Please note any items relating to Committee business are embargoed and should not be made public until after the meeting Minute NHS Tayside
Manager from PKC Business Improvement Team.
Five workstreams have been commissed that have representation from
both Health & Council OT staff. The workstreams are as follows:
A – Clinical and Operational Model
B – Workforce Development and Documentation
C – Information Technology
D – Performance Management
E – Communication and Engagement.
The project team report that there has been good progress in working
towards project and work stream delivery and demonstrated excellent OT
staff, stakeholder and community engagement. A questionnaire was sent
out and the results were overwhelmingly positive. A number of comments
mainly around communication issues have been taken on board.
The project will co exist with a key piece of work looking at Professional
Leadership for OT across NHS Tayside. The P & K Older People’s
Strategy Group will monitor the progress.
The Committee noted the report.
7. GOVERNANCE & ASSURANCE
7.1 Perth & Kinross CHP Committee Work Plan 2015-16 Alison Wood – Report No. 26/2015
Alison Wood presented the CHP Committee Work Plan for 2015-16.
Committee were asked to note that the last meeting of Perth & Kinross
CHP Committee will take place on 11 August 2015 and that the P & K
Health & Social Care Integration Pathfinder Board will be the forum to
enable the transition to the IJB. Relevent items of business will be
submitted to the Pathfinder Board post August 2015 and other items which
The aim of Perth and Kinross CHP is to improve the health and wellbeing of our communities in P&K as part of the NHS by working with a range of partners. This minute is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP 18

Please note any items relating to Committee business are embargoed and should not be made public until after the meeting Minute NHS Tayside
will be submitted to ‘other forums’ unspecified at present.
Community requested assurance at final meeting which ‘other forums’
business is to transferred to if it is not the Pathfinder Board.
The Committee noted the current position and that a further update will be given at the next meeting.
7.2 Perth & Kinross CHP Performance & Risk Report Miss Alison Wood –Report No 27/2015
Alison Wood presented the Performance and Risk Report. Key points
noted were around Delayed Discharge and Supplementary Staffing.
Further resources are to be assigned to Enhanced Care and
Physiotherapy/OT as part of the Scottish Government funding which has
been allocated to improve delayed discharges.
The committee acknowledged the current National problem which is
currently in place with regards to recruitment and retention of nursing and
medical staff. A lot of work is currently on going looking at hotspot areas
and improvements to recruit.
Sickness Absence statistics revealed a slight increase in long term sickness
but a decrease in short term sickness in March compared with February
2015.
The Committee noted the report.
7.3 Clinical Director Report Morag Martindale – Report No 28/2015
The aim of Perth and Kinross CHP is to improve the health and wellbeing of our communities in P&K as part of the NHS by working with a range of partners. This minute is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP 19

Please note any items relating to Committee business are embargoed and should not be made public until after the meeting Minute NHS Tayside Clinical Director, Morag Martindale provided an update on Enhanced Care
Service (ECS) which was launched in January 2015 in Ardblair Medical
Practice, Blairgowire. Victoria Practice Glover Street commenced the
project in April and Yellow Practice Drumhar Health Centre is schedule to
begin in July 2015. The interim evaluation has shown evidence that at this
stage 27 patients had benefited from this service and for the majority of
these patients avoided hospital admission. . This service was highlighted at
the Patient Safety Network Meeting as an example of good practice. The
committee heard examples of the great work which is being developed and
provided to ensure person centred care is being delivered
Since the commencement of daily team meetings this has provided team
members within Ardblair to share information and to appoint the most
appropriate keyworker able to provide for the needs of the patient. This
meeting saves a considerable amount of time previously spent on the
phone. There is also a weekly meeting whereby the MFTE Consultant is
present.
Dr Martindale has also been involved reviewing the improvement plan for
Prisoner Healthcare and facilitating and implementating recommendations
for medical staff.
Other current work includes:
• Peer review meetings in General Practice.
• Clinical representation on the Health Records Management Committee.
• Provides a link between Consultants and GP regarding new pathways
of care and changes to service.
• Chair of Perth & Kinross SCGR Committee.
• Consultant job planning for MFTE and POA.
The Committee noted the report
The aim of Perth and Kinross CHP is to improve the health and wellbeing of our communities in P&K as part of the NHS by working with a range of partners. This minute is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP 20

Please note any items relating to Committee business are embargoed and should not be made public until after the meeting Minute NHS Tayside
7.4 Perth & Kinross CHP Financial Report – Financial Position to March 2015 Mr Alexander Berry – Report No 29/2015
Finance manager Sandy Berry provided the committee with an update on
the CHP’s financial performance to the end of March 2015. The Budget
Review Group will continue as a management group that will transition to
appropriate forum within HSCI once this has been agreed.
The Committee noted the report, the progress made in absorbing savings targets during the year and suspported the ongoing work underway in the CHP to improve the recurring financial position. The committee also noted the ongoing remit of the CHP’s Budgetary Review Group in terms of ensuring the delivery of a balanced recurring budget.
7.5 Perth & Kinross CHP Staff Governance Report June 2015 Lauraine Miller – Report No 30/2015
HR Business Lead, Lauraine Miller provided a Staff Governance Report
which provided an update on the ongoing progress and plans to meet the 5
elements of the NHS Scotland Staff Governance Standards.
Regular newsletters continue to be sent to staff updating on progress and
changes across Perth & Kinross CHP. Updates on HSCI have been given
through the Partnership Forum and Consultation Events.
The Committee noted the report and that future staff governance issues will be submitted as appropriate to the Perth & Kinross Pathfinder Board/IJB.
The aim of Perth and Kinross CHP is to improve the health and wellbeing of our communities in P&K as part of the NHS by working with a range of partners. This minute is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP 21

Please note any items relating to Committee business are embargoed and should not be made public until after the meeting Minute NHS Tayside
7.6 Steps to Better Healthcare Programme – Medicines Leadership
Karen Melville – Report No 31/2015 The Committee noted the update report.
8. INFORMATION
8.1 Record of attendance 2014-15 The Committee noted this report.
The final meeting of the Committee will be held on Tuesday 11 August
2015 at 9am in the James Murray Suite, Murray Royal Hospital.
Subject to any amendments recorded in the Minute of the subsequent meeting of the Committee, the foregoing Minute is a correct record of the business proceedings of the meeting of the Perth & Kinross CHP Committee held on Tuesday 9 June 2015 and was approved by the Committee at its meeting held on Tuesday 11 August 2015.
CHAIR DATE 11 August 2015
The aim of Perth and Kinross CHP is to improve the health and wellbeing of our communities in P&K as part of the NHS by working with a range of partners. This minute is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP 22

ACTION POINTS UPDATE NHS Tayside Item 3.2
Perth & Kinross Community Health Partnership Committee 11 August 2015
Meeting Minute Reference Heading Action Point Responsibility Status
3 14 April 2015 6.1 Health & Social Care Integration
Update report required Director Community & Primary Care Services
11 August 2015 Agenda
Please note any items relating to Committee business are embargoed and should not be made public until after the meeting
1 This action note is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held

Please note any items relating to Committee business are embargoed and should not be made public until after the meeting Perth & Kinross CHP
Safety, Clinical Governance and Risk Group Minute of the above meeting held at 1.30pm on 2 June 2015 in the Meeting Room, 2 12, Pullar House Present Dr Morag Martindale, P&K CHP Clinical Director (Chairperson) Alison Wood, Head of Corporate Services and Business Support, P&K CHP Grace Gilling, Interim Service Manager, P&K CHP Jane Dernie, Allied Health Professions Lead for P&K CHP Julie Flynn, Head of Adult & Children, Young People & Families Services (Interim), P&K CHP Karen Buckley, Infection Control Adviser, NHS Tayside Lindsey Miller, Service Manager for Integrated Community Services, P&K CHP Maggie Rapley, Service Manager, Psychiatry of Old Age, P&K CHP Mark Dickson, Safety, Clinical Governance and Risk Management Coordinator, P&K CHP Sandra Gourlay, Lead Nurse, P&K CHP Apologies Evelyn Devine, Interim Lead Officer, P&K CHP Graeme Lamont, Locality Pharmacist, P&K CHP Jillian Galloway, Prisoner Healthcare Service Manager, P&K CHP Sue Muir, Head of Older Peoples Services, P&K CHP In Attendance Beth McDowell, Care Assurance Officer, NHS Tayside Dawn Wigley, Head of Nursing, Prisoner Healthcare Kerry Greig, SCGR Support Officer, P&K CHP Robert Packham, Associate AHP Director, NHS Tayside Dr Morag Martindale in the Chair ACTION 1. APOLOGIES
Dr Morag Martindale opened the meeting and welcomed all in attendance. Introductions were made around the table. Apologies were noted as above.
2. 3.
PATIENT STORY Dr Martindale shared the story of a patient, and described actions that had been taken to address his concerns. The Group noted the improvements that had been made for this patient. PREVIOUS MEETING 7TH APRIL 2015 The group approved the minute from the previous meeting on 7th
April 2015.
1 The aim of Perth and Kinross CHP is to improve the health and wellbeing of our communities in P&K as part of the NHS by working with a range of partners. This minute is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
Please note any items relating to Committee business are embargoed and should not be made public until after the meeting 4.
MATTERS ARISING FROM THE MINUTE There were no matters arising from the minute of the meeting on 7 April 2015.
5. ACTION POINTS UPDATE 6.
7.
The action point update was discussed. Grace Gilling confirmed Mental Health and Learning Disabilities should report into the P&K SCGR Group at present. Maggie Rapley provided the group with a progress report regarding 2 complaints received by POA:
1. A local incident review, which was escalated to a complaint, was not upheld by the Ombudsman.
2. Following a conciliation meeting, held with a patient’s family, the family have decided not to take further action.
Lindsey Miller confirmed action 8.2.3 from 7 April 2015 has been completed. Data regarding Antimicrobial Prescribing will be reported up through Community Hospital’s exception reports. Mark Dickson informed the group that feedback has been received, from all services, confirming that a training plan is in place or being progressed for 2015/2016. Some services were unsure what was meant by a “Risk Assessed” training plan; this refers to the rationale and justification as to what training is required by different members of staff in order to minimise risk. ANNUAL REPORT 2014/2015 Mark Dickson provided the group with a summary of the draft Annual Report for 2014/2015. The group noted and agreed the contents of the report. GROUP WORK PLAN 2015/2016 The group approved the work plan and noted an update on progress would be provided at a future meeting. The work plan has been designed around the Clinical Care and Professional Governance Joint Framework for Integration, and the six domains of Governance.
2 The aim of Perth and Kinross CHP is to improve the health and wellbeing of our communities in P&K as part of the NHS by working with a range of partners. This minute is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP

Please note any items relating to Committee business are embargoed and should not be made public until after the meeting 8.
SAFETY 8.1 Record Keeping and Documentation Audit This item will be carried forward to the next SCGR Group meeting on 4 August 2015. 8.2 Clinical Care and Professional Governance Joint Framework for Integration Robert Packham provided the group with a presentation on the Clinical Care and Professional Governance Joint Framework for Integration. Key points from the presentation include:
• Information Governance – ‘the duties related to the protection of information, information sharing, records management Information Technology management, data reporting and documentation standards.’
• Professional Regulation Workforce Development – ‘the need
for our organisations to have assurance that we have a workforce fit for purpose and sustainable into the future.’
• Patient/Service User/Carer and Staff Safety – ‘our duty is to create a safe working environment for staff along with our duty of care to patients, service users and carers.’
• Patient/Service User/Carer and Staff Experience – ‘the importance of involving service users and carers in the design and delivery of health and social care supports and services. It also reflects the importance of staff at the front line having the opportunity to shape services in line with specialist and best practice knowledge alongside their awareness of the needs of specific care groups and local communities.’
• Regulation, Quality and Effectiveness of Care – ‘the drive towards evidence based practice to improve outcomes and achieve Best Value in the design, organisation and delivery of services. Good governance in this domain should deliver on the Christie Commission requirements and the 20:20 vision of person centred, high quality services for the people of Tayside.’
• Promotion of Equality and Social Justice – ‘The national
health and wellbeing outcomes, together with the integration planning and delivery principles, are grounded in a human rights based and social justice approach.’
3 The aim of Perth and Kinross CHP is to improve the health and wellbeing of our communities in P&K as part of the NHS by working with a range of partners. This minute is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP

Please note any items relating to Committee business are embargoed and should not be made public until after the meeting
• Accountability for Clinical, Care and Professional Governance – ‘NHST Board and the three Local Authorities have existing mechanisms to demonstrate accountability to the Scottish Government and the public. Joint boards will integrate new and existing methods of professional performance management and governance within each of the three Integration Authorities. These will include arrangements for the protection of people of all ages, as well as strategic planning and community planning across Tayside.’
Working within the Joint Framework provides the opportunity to make small incremental improvements in quality of service, over a period of time. Beth McDowell presented a paper on AHP Core Standards and Quality Indicators to the group. This paper was compiled to assist AHPs to monitor and report on essential core clinical and non-clinical standards. Results indicated that there is diversity of governance practice amongst the 12 AHPs. Work has been carried out across each of the AHPs; asking a number of questions in order to gauge standards in each domain. Data has been collated and presented in a table, which clearly illustrates each of the AHPs score differently against each of the core clinical and non-clinical standards. The table also identifies where any gaps in knowledge are and provides us with an opportunity to imbed research, educate and engage people. In conclusion Robert suggested that a co-ordinated leadership around each of the topics would be advantageous. Each service should select 2 top priorities, from each domain, to work on every year. This will ensure an incremental improvement is made. He reminded the Group that every clinician is responsible for every part of the clinical and care governance dimensions. 8.3 Service Exception Reports Prisoner Healthcare Update A report was submitted by Prisoner Healthcare and made available to the group. Dawn Wigley informed the group that the report from Her Majesty’s Inspectorate of Prisons (HMIP) on HMP Perth, is due to be issued on 11 June 2015. HMIP visited HMP Perth during December 2014 to perform their inspection. Within the past two months there have been two episodes of staff taking the role of first responders to serious incidents. A meeting has been set up to review the level of training and skills required for
4 The aim of Perth and Kinross CHP is to improve the health and wellbeing of our communities in P&K as part of the NHS by working with a range of partners. This minute is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
Please note any items relating to Committee business are embargoed and should not be made public until after the meeting
this group of staff. A further update will be provided at the next SCGR meeting on 4 August 2015. Psychiatry of Old Age A report was submitted by POA and made available to the group. The group acknowledged this report. Pharmacy & Anticoagulant Service A report was submitted by Pharmacy and made available to the group. The group acknowledged this report. Integrated Community Services A report was submitted by Integrated Community Services and made available to the group. Lindsey Miller provided the group with the following update:
• Community Hospitals
The Care Governance Meeting for Community Hospitals had taken place on 27 May 2015.
• Medicine for the Elderly
A complaint has been received. Lindsey will carry out a piece of work regarding the complaint and will provide a further update to the group at the next meeting on 4 August 2015. An ongoing service review is taking place in Tay Ward at present. Retention of staff and recruitment is the largest challenge faced by MFE at present.
• Specialist Palliative Care Service
The Ombudsman is currently reviewing a complaint received regarding Specialist Palliative Care Services. Lindsey will update the group once a response has been received and will share any learning.
Children, Young People and Families A report was submitted by CYPF and made available to the group. Julie Flynn informed the group that training within CYPF is a
Jillian Galloway / Dawn Wigley
Lindsey Miller
Lindsey Miller
5 The aim of Perth and Kinross CHP is to improve the health and wellbeing of our communities in P&K as part of the NHS by working with a range of partners. This minute is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
Please note any items relating to Committee business are embargoed and should not be made public until after the meeting 9.
challenge. Investigation has revealed that staff turnover and the complexity of training required for new staff in this area are contributing factors. District Nursing A report for District Nursing was not available for this meeting, but a report will be submitted for the next SCGR meeting on 4 August 2015. Sandra informed the group that the first District Nursing and Intermediate Care Governance meeting took place on 19 May 2015. Terms of Reference have been agreed, and membership has been agreed for this group. Adult Mental Health Services A report was submitted by Adult Mental Health Services and made available to the group. Grace Gilling highlighted the challenge AMHS is facing with regards to staff recruitment and retention. This is a national challenge and not one that is specific to P&K. Allied Health Professions A report was submitted by AHP and made available to the group. Jane Dernie informed the group that recruitment is the biggest challenge faced by AHP at present. The hydro pool has been opened in the Rehabilitation Unit and is functioning well under the new governed regime. 8.4 Sharing Learning
SCEAs’ SIGN OFF
Morag Martindale informed the group that she had not been notified of any SCEAs requiring final sign off.
PATIENT EXPERIENCE 9.1 Complaints
9.1.1 P&K Complaints Summary Alison Wood provided the group with a summary of the complaints report provided for April 2015. The group noted the high level of compliance with the 20 day response times.
6 The aim of Perth and Kinross CHP is to improve the health and wellbeing of our communities in P&K as part of the NHS by working with a range of partners. This minute is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP

Please note any items relating to Committee business are embargoed and should not be made public until after the meeting 10.
Morag Martindale informed the group that there is currently a focus on engaging GPs, in GP related complaints received within Prisoner Healthcare. This should be an effective learning exercise. A complaint which was sent to the Ombudsman, regarding Prisoner Healthcare, was not upheld. 9.1.2 Lessons Learned from Complaints (November 2014-
April 2015)
Alison Wood shared a 6 month overview of the learning from complaints within the CHP, for the period of November 2014 to April 2015. This information will be captured in the reports submitted to this meeting in future. Maggie Rapley highlighted the importance of quality record keeping in order to investigate complaints robustly.
9.2 Unannounced Visits since last meeting
• Pitlochry Community Hospital GP Unit
Alison Wood provided the group with a verbal report on the unannounced visit to Pitlochry Community Hospital on 22 April 2015. A number of issues relating to Estates have been taken forward. A recommendation that the HON or SCN carries out regular spot checks of documentation audits has been made.
OPERATIONAL & CLINICAL EFFECTIVENESS 10.1 Clinical Governance Self Assessment Reporting
Timetable Mark Dickson shared a reporting timetable with the group. The timetable will provide all services with an opportunity to revisit the Clinical Governance Self Assessment and review progress on priority actions and demonstrate improvement. Lindsey Miller informed the group that work has begun on the Clinical Governance Self Assessment report for Community Hospitals, and also for Tay and Stroke wards. Further work is required before Lindsey can share the results with the group. A further update will be provided after 2 months. The group discussed various suggestions regarding Self
7 The aim of Perth and Kinross CHP is to improve the health and wellbeing of our communities in P&K as part of the NHS by working with a range of partners. This minute is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
Please note any items relating to Committee business are embargoed and should not be made public until after the meeting
Assessment reporting in order to monitor progress with the services’ action plans arising from the top priorities. These suggestions will be discussed at the Clinical Governance leads group. Dr Morag Martindale will provide the group with an update at the next SCGR meeting on 4 August 2014.
10.2 Infection Control
10.2.1 CHP Infection Control Update Karen Buckley provided the group with an Infection Control update. Continuing work around Catheter Associated Urinary Tract Infections (CAUTI) is working well. Pitlochry Community Hospital will be the last of the community hospitals to adopt the new working practices. They will be able to collect data by the end of June 2015. Karen will meet with Morag MacRae to discuss how to report this data into the SCGR group. A great deal of education has been given on the topic of catheter care. Karen will provide a further update at the next SCGR meeting on 4 August 2015. The removal of the bath from the store room in Pitlochry will be paid for by Infection Control. Beko dishwashers have been leaking in Pitlochry and Crieff Community Hospitals. Karen has asked the Procurement team to arrange for Beko engineers to visit these sites to view and provide advice on the problem. Maggie Rapley informed the group that fridges in both Leven and Kinclaven wards have been condemned. As Infection Control procurement lead for NHST, Karen will provide feedback to the procurement group. A new HEI self assessment document has been issued for comments. Karen will meet with Alison Wood and Mark Dickson to review the document. Karen would like to introduce a number of additional questions into the HEI Unannounced Visit document.
10.3 Measures for Safety Clinical Governance and Risk Mark Dickson summarised the most recent score card, which was discussed at the CHP Directorate’s Performance Review meeting on 5 May 2015. The group noted this report.
Morag Martindale
Karen Buckley
8 The aim of Perth and Kinross CHP is to improve the health and wellbeing of our communities in P&K as part of the NHS by working with a range of partners. This minute is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP

Please note any items relating to Committee business are embargoed and should not be made public until after the meeting 11.
12.
10.4 Clinical Quality Forum Update - 18 May 2015 Mark Dickson highlighted the key discussion points, from the Clinical Quality Forum which he attended on 18 May 2015, to the group. These included:
• A presentation from Diane Campbell around PVCs. • A high level presentation from Robert Packham on the
Clinical Care and Professional Governance Joint Framework for Integration.
• Caroline McQuillian gave a report on the Comments, Concerns, Feedback and Complaints report for NHST
• Eileen McKenna provided an update on the DATIX risk regarding nursing workforce.
Sandra Gourlay will ask Eileen McKenna to attend the SMT to discuss her role in recruitment and the challenges currently faced. The group would like to take a proactive role in minimising risk in this area. LEADERSHIP & GOVERNANCE 11.1 Ombudsman Report April 2015 The Ombudsman Report for April 2015 was provided to the group. The group noted the contents of this report. Dr Morag Martindale will issue a summary of the Ombudsman Report to the group. 11.2 Getting it Right Safety, Clinical Governance & Risk Issue
4 (April 2015) The group noted this report. WORKFORCE 12.1 DATIX Risks Mark Dickson informed the group that there are currently 15 DATIX service risks within the CHP, and 7 of these relate to workforce challenges. As previously mentioned, Sandra Gourlay will invite Eileen McKenna to attend the next Executive Group meeting and SCGR Group meeting to discuss workforce.
Sandra Gourlay
Morag Martindale
9 The aim of Perth and Kinross CHP is to improve the health and wellbeing of our communities in P&K as part of the NHS by working with a range of partners. This minute is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
Please note any items relating to Committee business are embargoed and should not be made public until after the meeting
13.
Date of next meeting The next meeting of the Safety, Clinical Governance and Risk Group will be held on Tuesday 4th August 2015 at 1:30 pm in Meeting Room 12, 2nd Floor, Pullar House.
2015 Safety, Clinical Governance and Risk Group meeting dates:
• Tuesday 6th October 2015 at 1.30 pm in Room 12, 2nd Floor, Pullar House
• Tuesday 1st December 2015 at 1.30 pm in Room 12, 2nd Floor, Pullar House
10 The aim of Perth and Kinross CHP is to improve the health and wellbeing of our communities in P&K as part of the NHS by working with a range of partners. This minute is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP

Please note any items relating to Committee business are embargoed and should not be made public until after the meeting
Safety Clinical Governance & Risk Group Meetings Glossary of Abbreviations
AHP Allied Health Professions AMHS Adult Mental Health Services BCP Business Continuity Plan BSL British Sign Language CAUTI Catheter Associated Urinary Tract Infection CDI or C.Diff Clostridium Difficile CHP Community Health Partnership CQI Clinical Quality Indicator CYPF Children Young People & Families DBT Dialectical Behaviour Therapy DNA Did not attend ECT Electroconvulsive Therapy ECT Enhanced Care Team GAP General Adult Psychiatry GDET Generic Data Entry Tool H&S Health & Safety HAI Healthcare Associated Infection HEI Healthcare Environment Inspectorate HMIP Her Majesty’s Inspectorate of Prisons ICT Infection Control Team IPCU Intensive Psychiatric Care Unit IHI Institute for Healthcare Improvement MFTE Medicine for the Elderly MiDIS Multi-Disciplinary Information System MIIU Minor Injuries and Illness Unit MRH Murray Royal Hospital NHSS NHS Scotland NHST NHS Tayside OPAC Older People in Acute Care P&K Perth & Kinross PHC Prisoner Health Care POA Psychiatry of Old Age PVC Peripheral Vascular Catheter SAB Staphylococcus Aureus Bacteraemia SCN Senior Charge Nurse SEAN Scottish Electroconvulsive Therapy Accreditation Network SIDCAAR Self-Inflicted Death in Custody Audit, Analysis and Review SBAR Situation, Background, Assessment, Recommendation SEWS Scottish Early Warning Score SCEA Significant Clinical Event Analysis SCGR Safety, Clinical Governance & Risk SIGN Scottish Intercollegiate Guidelines Network SMT Senior Management Team SOP Standard Operating Procedure SPS Scottish Prison Service TPAR Tayside Prescription & Administration Record
11 The aim of Perth and Kinross CHP is to improve the health and wellbeing of our communities in P&K as part of the NHS by working with a range of partners. This minute is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
Please note any items relating to Committee business are embargoed and should not be made public until after the meeting
Item Number 5.1
Report Number 34/2015 Perth & Kinross CHP Committee
11 August 2015 PRIMARY CARE UPDATE 1. SITUATION AND BACKGROUND
A report, Towards 2020 – Setting a Strategic Vision for Tayside, was submitted to Perth & Kinross CHP Committee in April 2014, by Dr Michelle Watts, Associate Medical Director, setting out the key strategic areas and high level plans for Primary Care Services in Tayside. The Committee were asked to endorse the “design principles” detailed in the report and support the development of a work plan and the testing of new models of care. The Committee asked that an update paper be submitted the following year.
2. ASSESSMENT
A number of papers, strategies and plans have been written since this original paper, including the Primary Care Premises Strategic Plan for Tayside, the NHS Tayside Local Delivery Plan and the NHS Tayside Clinical Services Strategy as well as more local papers and initiatives. The paper focused on 5 key strategic areas – Service Planning; Interfaces; Infrastructure; Workforce; Leadership. The following sections provide an update for the key areas highlighted in each of the strategic areas.
Service Planning Proposals included -
• The development of patient focused end to end pathways of care o There have been some developments in designing whole patient pathways in
partnership with primary and secondary care. Some examples include coeliac disease, community optometric management , medication review, pain management, and long term conditions including diabetes and COPD.
o Further development of pathways is also included in NHS Tayside Local Delivery Plan.
o The inclusion of Anticipatory Care Planning and the Key Information Summary in the GMS Contract is encouraging the sharing of information between in and out of hours services, including the ambulance service and A&E, thus removing some of the seams and enhancing the patient journey. To date, several thousand have been completed, enabling timely and appropriate sharing of information.
1 This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held
Please note any items relating to Committee business are embargoed and should not be made public until after the meeting
• The development of Primary Care datasets and a Tayside dataset o All practice clusters in Perth & Kinross have been presented with Integrated
Resource Framework (IRF) data relating to their individual practices. This data includes patients who are high consumers of health and social care.
o Proposals for datasets to demonstrate performance in primary care are under discussion at the NHS Tayside Quality and Outcomes Framework (QOF) planning group. This will link in to the emerging governance frameworks within the new Integrated Joint Boards.
o Inclusion of Primary Care data reports on NHS Tayside’s Qlikview system is underway
• Engagement with practices and consideration of new and innovative models of care o Cluster meetings are being facilitated by each of the CHPs. o Perth & Kinross CHP have developed a programme for the Cluster meetings to
ensure that all practices are receiving the same information and are given equal opportunity to participate.
o Enhanced Community Support model of care is being tested in Perth & Kinross with 3 practices, one in Blairgowrie and two in Perth City, with a view to identifying what works within this model and rolling it out to all practices in Perth & Kinross
o The Integrated Care Model is underway in Perth City with plans to test out this way of working in the Strathearn locality.
Interfaces Proposals included – • Support primary care engagement re Health & Social Care Integration through clear job
plans, support for leadership and development and a clear accountability o Dundee CHP have Cluster Lead GPs in place currently. Perth & Kinross are exploring
with the Cluster meeting GPs whether they would prefer one cluster lead or whether all representatives on the Group should rotate this role. Once all GPs have responded, Cluster Lead GPs will be appointed
• Minding the gap o GPs are encouraged, through the Quality and Productivity section of QOF, to complete
a number of Anticipatory Care Plans and ensure that these are recorded on the patient’s electronic Key Information Summary (eKIS). This is available to a range of professionals both in and out of hours. It is recognised that a single patient record that would ensure timely professional to professional communication is the preferred option but, until the complexities around this are resolved, the use of the eKIS, electronic referral and discharge systems can start to bridge the gaps in communication.
• Sharing of Learning from significant events o As part of the GMS contract, practices are required to carry out a minimum number of
Significant Event Analyses (SEA) each year. The purpose of the SEA process is to analyse and learn from events, either to consolidate the systems and processes in place or to make the necessary improvements to prevent the event from recurring. A number of practices in Tayside have been testing the NHS Tayside wide Datix system to record incidents regarding discharge from hospital and drug errors. This enables the sharing of incidents and the associated learning which may identify system wide deficiencies or help other practices with similar issues. All practices have access to the Datix system currently but there is a roll out programme regarding the training of Practice Managers as verifiers to enable them all to utilise the system to its full potential. There is a planned roll out of the datix system across all 4 independent contractor streams.
2 This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held
Please note any items relating to Committee business are embargoed and should not be made public until after the meeting
Infrastructure Proposals included – • Support of a Strategic capital plan from primary care by NHS Tayside Board
o Due to the complexity regarding the accommodation of GP practices in Tayside, with some practices occupying Board owned premises, others occupying premises leased from a third party developer and others in owner occupied premises; a draft Premises Strategic Plan has been developed by the Associate Medical Director for Primary Care. This recommends that a single primary care strategy is developed, fully costed, risk assessed and agreed with each Integrated Shadow Board.
Workforce Proposals included – • Rethink of the 10 minute consultation model
o Scottish Government have been advised on the need to increase the length of appointments and encourage different ways of working in the new Scottish GMS Contract which will be in place from 2017
• Support and test new ways of working
o The Associate Medical Director for Primary Care has written a proposal for “Developing a Sustainable GP Workforce in Tayside”. The proposed models include a career start scheme, support for collaborative working through integration and the creation of multi-disciplinary teams.
o It is important to acknowledge the implications of the reducing GP workforce. There is a significant reduction in the number of doctors training as GPs and very little availability of locum GPs to fill the rising number of vacancies in practices. This presents significant challenges to the current model of delivery for general practice and has created an appetite to start to look at different ways of working.
Leadership Proposals included – • Ensure a clear career structure with nationally agreed training and payscales
appropriate to the roles they are undertaking, and at parity with consultant colleagues o This will require addressing at a Scottish Government level
However, in order to start to build on clinical leadership in Perth & Kinross -
o In partnership with Scottish Government, a local Joint Clinical Leadership event took place in May 2015 with representatives from primary and secondary care where the lead professionals benefitted from the networking opportunity with colleagues from health and social care and opportunities to improve communication between professionals were explored.
The NHS Tayside draft Clinical Services Strategy, Reshaping clinical services for the future, has been developed, from which there are a number of recommendations. It is proposed that a Primary Care Clinical Services Strategy be developed, pulling together all aspects of primary care as noted above. Such a strategy will ensure that primary care in its entirety is examined and plans to cover all areas of the service are written. The Primary Care Services work plan is currently being updated. A new Scottish GP Contract will come into force in 2017, with the focus moving away from GPs concentrating on QOF, rather they will be providing medical expertise and advice to practice teams. In the intervening period, to allow the planning and negotiations to take place to deliver a contract to address 3 This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held
Please note any items relating to Committee business are embargoed and should not be made public until after the meeting GP recruitment challenges as well as the increasing elderly, frail population, there will be no major changes to the current QOF. 3. RECOMMENDATIONS
The CHP Committee is asked to o Note the updates as requested o Support the continued work to achieve what has been proposed above
4. REPORT SIGN OFF
Evelyn Devine, Interim Lead Officer, Perth & Kinross CHP
Angela Cunningham Primary Care Manager Perth & Kinross CHP
13 July 2015
4 This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held

Please note any items relating to Committee business are embargoed and should not be made public until after the meeting
Item Number 5.2
Report Number 35/2015 Perth & Kinross CHP Committee
11 August 2015
REPORT: UPDATE ALCOHOL DRUG PARNERSHIP (ADP) STRATEGY 1. SITUATION AND BACKGROUND
In April 2012 the Scottish Government confirmed the formal process of how ADPs will report to the Scottish Government. This reporting framework letter “SUPPORTING ALCOHOL AND DRUG PARTNERSHIPS (ADPS) TO DELIVER IMPROVED OUTCOMES FOR ALCOHOL AND DRUGS: FUNDING ALLOCATIONS AND PLANNING & REPORTING ARRANGEMENTS 2012 - 15 – NHS TAYSIDE” (April 2012). This letter set out the requirements of ADPs to provide three year plans to Scottish Government. As part of this process the ADP developed a three year rolling strategy. The ADP will no longer submit annual delivery plans in March and subsequent update reports in June. It will now only submit one annual report in September regarding progress and the milestones/objectives for 2014. This annual report was submitted in September 2014 to the Scottish Government and was noted by Housing & Health Committee in October 2014.
1.2 The ADP Recovery Strategy aims are:
1) Celebrate the positive impact of recovery on individuals and communities; 2) Support communities to support themselves; 3) Target specific groups affected by drugs and alcohol and support frontline services to
review and refocus their work to these individuals and areas; 4) Ensure appropriate support and services for children and young people affected by
parental misuse; 5) Ensure we address cross-cutting issues (complex needs) affecting many individuals –
mental health, criminal justice, homelessness, unemployment; 6) Create capacity in professional services to support community engagement to promote a
preventive agenda; and 7) Ensure that there is a clear focus on addressing the whole population approach to alcohol
and cultural change.
1 This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held

Please note any items relating to Committee business are embargoed and should not be made public until after the meeting 2. ASSESSMENT
This Report is to inform committee of the progress of the Alcohol Drug Partnership (ADP) Strategy. The ADP strategy is a “sea change” on how services will be provided in the future and the role of clients in this process. This has meant a change from a treatment approach to a recovery focused where clients are no longer passive recepitants but are active players in their recovery. In the past recovery was seen as a potential episode in treatment. The environment the ADP strategy has started to develop is the complete opposite, now treatment may be seen as an episode in recovery. The ADP has taken this forward by developing service user and carers groups. These groups are now proactively engaged in various areas within the ADP structure. The development of mutual aid is starting to consolidate this process. This is the start of a process of change which will take time to embed and other partners to embrace completely. This is the beginning of a journey and the ADP actively seeks the committees support in this journey, to make recovery a reality within Perth and Kinross It is proposed that CHP Committee note the ADP Annual Report Priorities to Scottish Government for 2014. These are set out below with progress updates:
Priorities 1 The ADP will complete its Joint Commissioning Strategy by December 2013
that will incorporate a Logic Model and Integrated Resources Framework to set out clearly the resource and service inputs, activities and outputs to deliver the desired outcomes to the target populations in line with our themed priorities. Available resources to be redirected to support a recovery oriented system of care.
1a PROGRESS The ADP has recently completed its Commissioning Delivery Plan this is being taken forward by the ADP Finance and Commissioning Group. The ADP has already moved resources from Adult Treatment Services to Children and Young People Services to support the prevention agenda. The ADP is in the process of developing its Recovery Orientated System of Care (ROSC) pilot in Perth City. This pilot will incorporate new service level agreements with partners and related outcome frameworks.
2 The ADP to ensure that there is a clear strategy to take forward the issues identified in “Evidence for Success” in relation young people, parents and alcohol.
2a PROGRESS The ADP is taking forward a review of alcohol and drugs education provision within the Curriculum of Excellence. This will be taken forward by the ADP Children, Young People & Families group. This has been further supported by a joint Alcohol Scoping Exercise between the ADP and PKC Licensing Board.
2 This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held

Please note any items relating to Committee business are embargoed and should not be made public until after the meeting
3 The ADP will ensure an organisational development process is developed to redefine working practices to provide coherent and supportive framework to enable recovery.
3a PROGRESS The ADP has taken forward development days with its delivery groups and has worked with STRADA to develop its strategic approach. The ADP is in the process of developing its Recovery Orientated System of Care (ROSC) pilot in Perth City. This pilot will incorporate new service level agreements with partners and related outcome frameworks.
4 The ADP will develop a phased approach to roll out SMART Recovery (SRUK) meetings within prison and across local services within Perth and Kinross.
4a PROGRESS The ADP purchased a block licence from SRUK which has allowed a network of meetings to be developed. There are now meetings in the Community, Prison and Murray Royal Hospital. The ADP has also supported the development of the SRUK Families and Friends pilot locally in partnership with Cair Scotland.
5 The ADP will develop ADP quality assurance by piloting self-evaluation process and case file audits within ADP services as per Child Protection Committee (CPC) framework.
5a PROGRESS The ADP has reviewed its Self-Evaluation Calendar and is the process of supporting local services to develop recovery planning returns. These returns will part of the quality assurance process. The ADP has also commissioned Quality Principles training for peer stakeholders. These peers will review local services using Quality Principles and provide reports to the ADP. These reports will be used as part of the quality assurance process. However, due to changing priorities within the CPC this year (2015) there will be no direct drug and alcohol case file audit.
6 Focus on developing its Recovery Orientated System of Care (ROSC) and workforce development and mitigating the adverse impact of substance misuse on children and young people.
6a
PROGRESS The ADP is in the process of developing its Recovery Orientated System of Care (ROSC) pilot in Perth City. This pilot will incorporate new service level agreements with partners and related outcome frameworks. The ADP is currently working with STRADA to develop workforce planning. The ADP Children, Young People & Families Group has being reviewing its membership and priorities and will focus on a “Whole Family Approach “with ADP partners.
3 This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held

Please note any items relating to Committee business are embargoed and should not be made public until after the meeting We now need to build on these achievements by continuing to promote recovery and integration between peer workers, mutual aid and services. This will require understanding of recovery and new ways of working and different skills sets for services. This is currently being further developed by the ADP in its new strategy for 2015 – 2020. This strategy will build on the 2012 strategy and develop future recovery approaches and connect these to the nine National Health and Well Being Outcomes. The process will also have to be supported by community planning partners if this approach is to be successful. It is recommended that CHP agree the continuation of further developments within ADP Strategy to build on the work already achieved as outlined in this report.
3. RECOMMENDATIONS
It is recommended that the CHP Committee:
I. Note the activity undertaken to date in the development of the Perth and Kinross ADP Strategy;
II. Note the planned next steps for the further development of the ADP Strategy. 4. REPORT SIGN OFF Evelyn Devine, Interim Lead Officer, Perth & Kinross CHP. Bill Atkinson Chair Perth & Kinross ADP
July 2015
4 This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held

Please note any items relating to Committee business are embargoed and should not be made public until after the meeting
Item Number 5.4
Report Number 36/2015 Perth & Kinross CHP Committee
11 August 2015 NHS TAYSIDE LOCAL DELIVERY PLAN 2015-16 1. SITUATION AND BACKGROUND
The draft Local Delivery Plan (LDP) 2015-16 was presented to NHS Tayside Board at its meeting on 12 March 2015 for comment and approval. The NHS Tayside Board approved the draft LDP, subject to three minor amendments, for submission as a final version to the Scottish Government Health Performance Directorate on 20 March 2015. The final LDP has now been distributed to NHS Tayside Board members. 2. .ASSESSMENT
Formal sign off of NHS Tayside’s Local Delivery Plan for 2015-16 was provided by John Connaghan, NHSScotland Chief Operating Officer, Performance and Delivery, in his letter of 31 March 2015 to the NHS Tayside Board Chief Executive. The letter outlined certain points for the NHS Tayside Board to note in taking the LDP forward during 2015/16. Progress against the LDP will be conducted at national level through the NHS Tayside Board’s Annual and Mid Year Reviews to be held during 2015/16. Quarterly reporting on progress with the LDP will be made to NHS Tayside Board. The first report was presented to NHS Tayside Board in June. The LDP is now available on the NHS Tayside website. 3. RECOMMENDATIONS
The Committee is asked to note the information for taking forward the LDP during 2015/16. 4. REPORT SIGN OFF Evelyn Devine, Interim Lead Officer, Perth & Kinross CHP 11 August 2015


2
IInnttrroodduuccttiioonn 33 SSttrraatteeggyy DDeevveellooppmmeenntt iinn 22001155//1166 55 RReessppoonnssee TToo NNHHSSSSccoottllaanndd IImmpprroovveemmeenntt PPrriioorriittiieess FFoorr 22001155//1166
SSTTRRAATTEEGGIICC PPRRIIOORRIITTYY AARREEAASS:: HHeeaalltthh IInneeqquuaalliittiieess aanndd PPrreevveennttiioonn 88 AAnntteennaattaall aanndd EEaarrllyy YYeeaarrss 1199 PPeerrssoonn CCeennttrreedd CCaarree 2211 SSaaffee CCaarree 2244 PPrriimmaarryy CCaarree 2277 IInntteeggrraattiioonn 3344
IImmpplleemmeennttaattiioonn PPllaannss ffoorr 22001155//1166 ttoo SSuuppppoorrtt DDeelliivveerryy 3388 ooff EEvveerryyoonnee MMaatttteerrss
NNHHSS BBooaarrdd’’ss CCoonnttrriibbuuttiioonn ttoo CCoommmmuunniittyy PPllaannnniinngg PPaarrttnneerrsshhiippss 4433 AAppppeennddiixx 11 :: LLDDPP SSttaannddaarrddss 4455 AAppppeennddiixx 22 :: MMaappppiinngg ooff KKeeyy PPllaannss 4477

3
The Local Delivery Plan (LDP) is the delivery contract held between the Scottish Government and NHS Boards in Scotland. The LDP focuses upon the priorities for NHS Scotland and supports delivery of the Scottish Government’s national performance framework, the 2020 Vision for health and social care, and the health and social care outcomes that are being developed. The LDP will be considered alongside the new strategic commissioning planning arrangements for Integrated Joint Boards. Each year, the LDP evolves to support the delivery of the national priorities, for example last year saw an increased focus on delivering outcomes for the people of Scotland. The LDP for 2015/16 builds upon last year and requires NHS Boards to develop plans focused on new actions planned in a small number of strategic priority areas. The LDP 2015/16 begins by stating that NHS Tayside is reviewing its approach to strategy. This will concentrate upon the pace and reach – as opposed to the direction - of change. The new Integrated Strategy that will be produced over the course of 2015 will have an important impact on the LDP 2016/17, although the responses to the NHSScotland Improvement Priorities 2015/16 have already begun to map out the actions for next year as part of the ongoing process of improvement and movement towards the 2020 Vision.
SSttrruuccttuurree ooff tthhee LLDDPP 22001155//1166 Three elements – underpinned by finance and workforce planning – form the structure of the LDP for this year - Response to NHSScotland Improvement Priorities for 2015/16 Implementation Plans for 2015/16 to support delivery of ‘Everyone Matters’:
2020 Workforce Vision NHS Board’s Contribution to Community Planning Partnerships Response to NHSScotland Improvement Priorities for 2015/16 sets out the improvement actions being taken forward in the following strategic priority areas: Health Inequalities and Prevention Safe Care Antenatal and Early Years Primary Care Person Centred Care Integration Implementation Plans for 2015/16 to Support Delivery of Everyone Matters outlines local implementation plans for 2015-16 to deliver the five priorities contained within Everyone Matters: 2020 Vision Implementation Plan – Healthy Organisational Culture; Sustainable Workforce; Capable Workforce; Integrated Workforce; and Effective Leadership and Management.

4
NHS Board’s Contribution to Community Planning Partnerships sets out how Boards will continue to strengthen their approach to community planning during 2015/16.
LLDDPP SSttaannddaarrddss 22001155//1166 There will be no HEAT targets contained within the 2015/16 LDP due to the delivery of the existing HEAT targets in March 2015. The LDP will now contain nineteen Standards. Performance trajectories will not be required for these Standards, with the exception of the 12 weeks outpatient waiting times standard. The LDP Standards for 2015/16 are outlined within Appendix 1. The Scottish Government will continue to review the LDP Standards to ensure that their definitions are consistent with changes in service delivery through the 2020 Vision.
5
STRATEGY DEVELOPMENT IN 2015 This LDP for 2015/16 comes at a time when NHS Tayside is reviewing its future approach to strategy. The NHS Tayside Strategic Health Plan 2012 – 2015 was approved by NHS Tayside Board in March 2012. Consideration has already been given about how best to replace that strategy in a new and changing environment. In the context of the 2020 Vision and the parallel vision for health promotion and public health, the strategic direction is largely fixed but there is a need to consider further the pace and reach of strategic change and how best to make it sustainable. NHS Tayside has already made considerable progress in the direction of the 2020 Vision and continues to deliver against the HEAT Targets/Standards, but the Board increasingly recognises that to realise fully the ambitions of the 2020 Vision for care and those for promoting better health and reducing health inequalities, it is necessary to take much more of an integrated, ‘whole systems’ approach to strategy. This means considering together the various services in Tayside for health, care and support that, through different ways of being organised and connected, can make significant improvements to people’s health and well-being. The intention is to have a high-level Integrated Health Strategy for Tayside that will run in the first instance to 2020. Many of the components of the strategy have already been developed, but further work is required to pull these elements together into a single, integrated package, develop the workstreams further, and to communicate and affirm the strategy internally and externally. There will be six themes underpinning the new strategy: 1. Prevention. Concentrating increasingly on services that help both staff and public to
identify and respond rapidly to emerging risks and signs of deterioration. 2. Engagement. Offering people more opportunities to engage in managing their own
care and support and in tackling risks to their health. 3. Responsiveness. Providing everyone with services that are not just effective, but
which respond to their wider personal needs and preferences. 4. Community-Focused. Encouraging and supporting local communities to build up
and mobilise their resources to create accessible opportunities for people to improve their health and well-being.
5. Collaborative. Working with a range of local statutory, third sector and commercial
organisations to maximise the improvements possible to people’s health and well-being.
6. Strengths. Building and developing the strengths of NHS Tayside, including its role as
a tertiary centre and its links to Dundee University, to maximise the contribution the organisation can make to Tayside and Scotland in terms of its employment, economic and social impact alongside benefits for health and care.
These six themes reflect what is needed to make faster and wider progress towards the 2020 Vision and towards national priorities regarding health inequalities and health improvement. Underpinning the six themes will be the requirement to maintain the quality – effectiveness, safety and value for money – of current services. The themes emphasise

6
that many of the most significant improvements to the quality of services will come in the future from building a wider set of connections outside NHS Tayside. However good the services provided by NHS Tayside are on their own terms, it is increasingly accepted that the overall outcomes and benefits that can be achieved are dependent upon what the recipient of NHS services, other local services and organisations, and communities also choose to do. Reinforcing the best of what is already done along with building new ways of working with others is to be an essential platform for effective changes to health, care and support, and to changes that people locally can support. This platform will offer an opportunity to remodel and redesign services in a way that is driven by improving quality in ways that those using services will recognise, and more importantly to which they have contributed. The changes from remodelling services that will be most important in the future are those that create: 1. Increased engagement of people in communities – especially the poorest ones – to
address more effectively the risks associated with poor health – economic, environmental and behavioural risks.
2. A locality focus along with other agencies on the provision of services that can be
continuous, responsive and joined up around the overlapping and reinforcing problems faced by individuals and families with the greatest needs.
3. Less dependence upon hospital – especially inpatient – care for those with complex,
ongoing needs through more prevention and more effective community interventions.
4. Improved opportunities for people with ongoing conditions to manage their own
conditions effectively through improved monitoring systems and better access to information and support.
5. Greater flexibility about how, where and when services are delivered to match
better the needs and wishes of service users. 6. Reduced reliance on spend on property and buildings to release more money for
direct patient services. 7. Improved research & development, education and innovation capacity, which
builds upon the work of the Academic Health Science Partnership, to enable NHS Tayside along with its partners to give the people of Tayside access to the latest types of care and to contribute to the wider economy and society.
The kind of redesign and remodelling of services outlined above which will lie at the heart of this Integrated Health Strategy for Tayside are put forward on the basis of achieving significant improvements to health, care and support for people in Tayside. Taking forward the changes that will produce these benefits will not be without challenges: 1. These changes have to be introduced while continuing to provide current services
24/7 and transitions will not always be easy especially those staff roles which will develop and transform to provide care and support in different ways.
2. New models of service provision – especially the community based emphasis – will
have implications for the organisation of existing – especially hospital – services that will have to be addressed.

7
3. A shift to community engagement and locality planning requires different approaches to the planning and delivery of services compared to those with which staff and public are familiar.
4. The funding pressures faced by NHS Tayside and other partner organisations make it
difficult to focus on - and to identify resources for - significant change even where there are significant benefits.
In the light of the above, before moving to develop the Integrated Health Strategy for Tayside, the following actions will be undertaken: 1. Engagement within NHS Tayside regarding how far the six themes represent the
principal areas for change over the next five years. 2. A review of the financial, workforce and property contexts within which the
Integrated Health Strategy for Tayside will be launched and how specific issues might be anticipated and addressed proactively.
3. (Following internal and external consultation) determining the most appropriate
‘strategic workstreams’ through which the Integrated Health Strategy will be undertaken. 1
4. Engagement with Integrated Joint Boards and partner organisations on how best to
develop further both a strategically integrated and a locality focused approach to care and health.
5. Establishment of a Multi Partner Advisory Group to support partnership contributions
to the Strategy and its development and implementation. 6. Confirmation of the validity of existing arrangements for patient/public engagement
in decision making. These actions are to be complete by June 2015 with a view to having the first iteration of the Integrated Health Strategy for Tayside produced by the end of 2015.
1. At this stage, it is proposed that there are 6‐8 workstreams covering the five year period. The workstreams
would be based on ‘areas of challenge’ (e.g. extending self‐management of care). These would represent the 6‐8 big things NHS Tayside need to do. There would still be planning of individual services.
8
The LDP should set out local priorities for addressing health inequalities and improving prevention work based on the needs of the local population, with a focus upon those communities where deprivation is greatest. Outlining Improvement aims, levels of activity and demonstration of how activity is embedded in to routine practice, along with information on prioritisation of action and progress monitoring.
OVERVIEW Tackling health inequalities is central to the public health agenda. Four years ago, on behalf of NHS Tayside and its partners, we published The Health Equity Strategy - Communities in Control - whose objective was to eliminate health inequalities in Tayside within a generation. An audit/stock-take of where we had got to in Tayside in moving towards health equity shows numerous examples of encouraging progress; however, progress was greater and more rapid in some areas than in others. In the areas where progress has not been so substantial, the organisational culture around targeting of services and programmes towards those most in need has not been as receptive as it needs to be to deliver on what is a very radical Strategy.
Our job in the NHS (and with other colleagues, Integrated Joint Boards and across the local Partnerships), is to re-energise our equity-focused work so that it becomes a core part of how all public sector organisations, including hospitals, work on a day-to-day basis. Underlining that approach, CEL 01 (2012), Health Promoting Health Service (HPHS) promotes that ‘every healthcare contact is a health improvement opportunity’. Given the proportionately greater use of acute services by patients from deprived communities, health improvement in acute settings offers an opportunity to reduce health inequalities. A revised CEL to be issued in 2015 will reflect the health improvement topics highlighted for the 2015/16 Local Delivery Plan: smoking, alcohol, food and health, breastfeeding, staff health (Healthy Working Lives), physical activity and active travel. There is an underpinning health behaviour change training programme to support frontline staff. SMOKING The Scottish policy on tobacco, Creating a Tobacco-Free Generation: A Tobacco Control Strategy for Scotland sets out plans to make Scotland a smoke-free nation. The Scottish Government has previously recognised the importance of a comprehensive approach to tobacco control and has published a series of strategies and policies to support increased legislative control and investment in smoking prevention and cessation programmes. PRIORITY ACTIONS Delivering on the prevalence targets set out in Creating a Tobacco-Free Generation: A Tobacco Control Strategy for Scotland requires that we decrease the numbers of new smokers taking up smoking. A change in investment has therefore been delivered that diverts substantial amounts of resource away from smoking cessation and into evidence-based interventions that decrease the numbers of young people who take up smoking. These interventions are focussed on communities classified as SIMD quintile 1 and 2. This change in direction is much more likely to deliver on the policy objective of a smoke-free nation than the previous approach.

9
Strengthen the Delivery of the Smoking Prevention Work Streams In 2015/16, the Early Years and Young People Team will continue to deliver their current smoking prevention programme to primary and secondary schools and young people across Tayside. In addition, NHS Tayside has successfully bid to become one of the Scottish Government’s pilot sites for the ASSIST intervention, which is to be offered to the 27 local authority managed secondary schools across Tayside. The planning of this work has been taken forward in partnership with local authority partners. ASSIST is a licensed intervention and requires a prescribed series of quality assurance mechanisms for the training of staff and delivery to schools. Implementation of the programme began in January 2015 and the pilot will run until June 2017. The team will also work with cessation colleagues and multi-agency partners to design and implement an intervention that protects looked after-children and young offenders from exposure to tobacco and second hand smoke. Engaging with all schools across the three localities presents the main challenge to the delivery of the smoking prevention work. Measure to demonstrate improvement The smoking prevalence estimates published by SALSUS give an indication of the relative progress made in preventing children from taking up smoking tobacco at 13 and 15 years old. Implement Smoke-Free Premises and Grounds In 2015/16 work will be taken forward on competent implementation of the revised smoking policy and effective communication to staff, patients and visitors. Work will be undertaken to review the revised nursing documentation and make a judgement around whether all the measures required to support patients and staff in achieving a smoke-free hospital stay are in place. Communication with our communities is a key part in this process and we will set out our vision for partnership with local people, so that we can harness the assets of local people in making Tayside a healthier place. Through local Tobacco Alliances we will work to engage with local authorities and partners to enable them to use their remits to further this agenda so for example, we see the first smoke-free play parks and public areas. The revised Tobacco Control Policy requires to be in place by March 2015. However, consolidation and effective implementation including working to communicate with the public, is likely to be an ongoing process. The major challenge presented in this area is in encouraging a change in behaviour from smokers and to enlist the support of the majority of the public who are non-smokers. Measures to demonstrate improvement CEL (1) 2012 Annual Report Submission. Monitoring progress in implementation can be achieved through point prevalence surveys. New e-pharmacy system to record activity. Maximise the Effectiveness of the Community Pharmacy Smoking Cessation Scheme The implementation of the new specification has taken several months to bed in and this has been complicated by issues with the new e-pharmacy service that has been implemented simultaneously. During 2015/16 we will continue to work with community pharmacists to support them in starting to perform under the new system. Nationally, work is ongoing to adapt the e-pharmacy system to get around the glitches in the current IT. We will continue to publicise the smoking cessation service and promote the help that is available for patients wishing to stop smoking. The timescale for these actions are ongoing. A larger challenge is likely to be around how smoking cessation services are redesigned to effectively compete with more widespread use

10
of e-cigarettes. A programme of work will be described and undertaken in 2015/2016 to understand how smoker’s requirements for support has changed and how we can support the group of e-cigarette users who are still addicted to nicotine and wish to move their lives on. Measure to demonstrate improvement The LDP standard challenges smoking cessation services to consolidate activity and maximise the number of 3 month quits achieved. FOCUS FOR 2015/16 Successful implementation of the ASSIST programme with community linkage.
Effective communication that describes a different narrative of our expectations for patients, visitors and staff to be partners in making Tayside a healthier place. A tangible element of this refreshed approach will be the revised Smoking Policy; we will work with local authorities and other partners to investigate how the approach taken by this policy can be spread.
Consolidation of the community pharmacy smoking cessation service and re-positioning of the service to compete with e-cigarettes: a programme of work will be undertaken to provide evidence for us to redesign and re-position services to make them more relevant to the needs of patients.
KEY DELIVERABLES BEYOND 2015/2016 Creating a Tobacco-Free Generation creates an aspiration for Scotland to become a
healthier place where almost nobody smokes. There are smoking prevalence trajectories to meet to ensure that this ambition for the population of Tayside can be met. We are conscious of the 46 priorities within the strategy and the wide range of actions that will be undertaken with partners to deliver this ambitious plan.
SUBSTANCE MISUSE Substance misuse disproportionately affects the most vulnerable and socio-economically deprived in our community. Changing Scotland’s Relationship with Alcohol: Framework for Action focuses upon reducing alcohol consumption. The Road to Recovery: A New Approach to Tackling Scotland’s Drug Problem highlights the importance of a recovery focused approach. There is strong research evidence that reducing alcohol consumption reduces alcohol-related health and social harm. Alcohol consumption can be reduced by restricting affordability, availability and accessibility. Restriction on density of outlets through licensing is a way of reducing harm from alcohol. Other evidence-based measures include minimum unit price and drink driving measures. Alcohol brief interventions are key to reducing harm from alcohol too. PRIORITY ACTIONS NHS Tayside will have a direct involvement in the redesign of substance misuse services to create a greater focus on “whole families” and support for recovery in the Angus local communities and to address new ways of working to deliver the ‘Support and Connect’ Project - a recovery directed system - within the Dundee communities. Work has already been initiated across agencies in Perth & Kinross to support the development of a recovery focussed model of care. NHS Tayside will actively support the future development of mutual aid groups within this locality.
11
Alcohol Licensing NHS Tayside will continue to work with ADPs to make available and accessible the information on health and social harms from alcohol intake with a view to influencing licensing decisions to restrict availability of alcohol. NHS Tayside is a statutory consultee for licensing applications and as such has the opportunity to influence licensing applications. In all three localities, work is progressing: In the Angus locality, early work to describe the extent of alcohol provision and alcohol related social harm is being built on by the collaboration of an NHS Tayside Information Analyst with ADP colleagues so that data from Local Authority, Police and Health can be used to scope out the extent of alcohol related harm to health and to society. The information within the scoping paper can then be used to inform decisions on licensing of premises for sale of alcohol. In the Dundee locality, NHS Tayside in collaboration with community planning partners, completed a comprehensive assessment of alcohol related harm in the city and a statement on licensing overprovision. The locality Licensing Board has since made a statement to the effect that the city is overprovided for in terms of licensed premises and so there is an onus on applicants to show that the granting of a new licence would not contribute to over provision. In the Perth & Kinross locality, NHS Tayside has participated in the ADP initiated and chaired Alcohol Scoping Meetings over recent months and has, with the input of community planning partners, completed a report outlining the health and social harms and describing the alcohol provision within that locality. Overall, it is encouraging that community planning partners in each of the three local authority areas are keen to address the issues of health and social harms related to alcohol. NHS Tayside remains committed to working with the Licensing Forum within each area and building on the work already ongoing. Alcohol Brief Interventions (ABIs) Continue work in community pharmacies to deliver ABIs to those people who are less likely to attend their GP e.g. young men from deprived areas. There is an enhanced service contract with community pharmacies for the delivery of screening and brief interventions. Funding to continue this is in the plan for 2015/16. Analysis of the data recorded at community pharmacies will be undertaken to ensure ABI delivery best fits need, especially in communities less likely to engage with Primary Care, by February 2016. Measure to demonstrate improvement Ongoing measurement of LDP Standard to embed ABIs in the three priority settings and broaden delivery in wider settings. Access to Services Extra clinic time (which was established in January 2013) will continue. NHS Tayside is meeting the LDP access standard and we will continue to work towards maintaining this. Measure to demonstrate improvement Ongoing measurement of the LDP Standard to ensure that no clients wait more than 3 weeks to appropriate drug or alcohol treatment.
12
FOCUS FOR 2015/16 Continue delivery of ABIs in the priority areas of Primary Care, Accident & Emergency and
Antenatal Services and embed training to deliver ABIs.
Apply learning from community pharmacy delivery of ABIs so that provision for people in deprived areas is tailored to need and effectiveness of delivery.
Work with each Licensing Forum to provide relevant data to assist Licensing Boards in recognising the health and social harms from alcohol in their locality.
Contribute to the Alcohol and Drug Partnership implementation of the recommendations from recent needs assessment, firstly around children affected by parental substance misuse and secondly on new psychoactive substance use.
KEY DELIVERABLES BEYOND 2015/2016 To focus on a recovery approach, looking ahead to a life that is no longer defined by
substance misuse and in which change initiated and driven by the individual is supported by family and community.
The risk of death from drugs is increased when people use combinations of drugs, both
prescribed and illicit. There are a number of actions planned to reduce polypharmacy, including a pilot in a deprived area. Actions from an audit of drugs prescribed to people who misuse substance are being and will be taken forward.
Alcohol and Drug Partnerships have incorporated the learning from two needs
assessments, 1) around the needs of children affected by parental substance misuse and 2) around new psychoactive substances into their workplans for the upcoming year.
The Drug Death Review Group continues as an expert group to share learning from review
of drug deaths which ADP partners apply within their locality to reduce risk of death from substance misuse.
PREVENTION OF OBESITY AND PROMOTING HEALTHY EATING The Scottish Government policy (Preventing Overweight and Obesity in Scotland: A Route Map Towards Healthy Weight) sets out four preventative actions - control exposure to, demand for and consumption of excessive amounts of highly calorific foods and drinks; increase opportunities for physical activity in daily lives and minimising sedentary behaviour; establish life-long habits for positive health behaviour; and increase the responsibility of organisations for the health and wellbeing of employees. National policy also calls for assurance that cost effective and appropriate weight management services are provided. PRIORITY ACTIONS Multi-agency partnership working is necessary to make ‘sustainable changes to our living environment in order to shift from one that promotes weight gain to one that supports healthy choices and healthy weight for all’. NHS Tayside is working with local authorities and external partners such as local employers and voluntary agencies to integrate support and, provide sustainable preventative and treatment services. Health improvement programmes for obesity prevention and treatment are in place (Maternal and Infant Nutrition, Child Healthy Weight, Adult Weight Management and Workforce):

13
Maternal & Infant Nutrition (MIN)
The MIN programme is improving the capability and capacity of those working with nutritionally vulnerable women of childbearing age and infants, by increasing access to training opportunities that are based on the principles of health behaviour change, asset based approaches and early intervention. It is also improving and increasing the workforce contribution to: obesity management in pre-pregnant, ante-natal (optiMum) and post-natal women (Weight Watchers); promotion of Healthy Start (including retailers) and; in supporting women with infant feeding choices and their experience of infant feeding.
Measures to demonstrate improvement
Number of courses delivered and attendance; pre and post knowledge and skills evaluation; post course application assessment (planned).
Number of obese women receiving optiMum; number of women attending postnatal weight management (Weight Watchers) and % achieving ≥5% reduction in body weight.
Uptake of Healthy Start scheme and vitamin supplements; feedback from families. Achievement of UNICEF UK Baby Friendly accreditation. Breastfeeding rates.
Child Healthy Weight (CHW)
The CHW programme continues to deliver a high quality healthy weight service to children, young people and their families. This includes developing and implementing a childhood weight management pathway which includes referral in to and out of the Paediatric Overweight Service Tayside (POST) (clinical service). It is also improving the Fun Fit Tayside (FFT) programme (child healthy weight whole class approach) with the three local authority education departments. POST continues to deliver a comprehensive training programme for healthcare professionals and others, and collects and analyses outcome and patient experience and performance data to support continuous quality improvement and service redesign.
Measures to demonstrate improvement
Clinical service - change in BMI SD; qualitative feedback. Prevention – number of teachers trained to deliver FFT; number of schools and classes
undertaking FFT; qualitative feedback.
Adult Weight Management (AWM)
The AWM programme continues to develop and implement an evidence-based, high quality and best value weight management pathway for overweight/obese adults. Work is focusing on the surgical patient pathway (Tier 4) and the non surgical specialist weight management pathway (Tier 3), but Tier 2 also requires attention. There are inequalities in the level of services provided at Tier 2 across each of the three CHPs. The population needs assessment also identified that within the current financial envelope the service can only support <2% of the obese population in Tayside. A lack of integrated weight management data collection results in the inability to target improvement in services and look at clinical outcomes. In response to this, the AWM Service was re-designed and an improvement plan is being implemented to reduce the inequalities in all tiers of the pathway. A shift in resource from Orlistat spend to help bridge some of the funding gap is proposed and an integrated weight management data collection system is being developed.
Measures to demonstrate improvement
Numbers of patients achieving ≥5% weight loss in Tier 2. Demographics and number of patients commencing and completing Tier 2. Numbers of patients achieving ≥5% weight loss in Tier 3.

14
Demographics and number of patients commencing and completing Tier 3. Reduce spend on Orlistat by at ≥50% Number and percentage of patients undergoing bariatric surgery who meet agreed criteria
for Tier 4. Numbers of hits on Tayside Nutrition MCN (weight management) internet site.
Workforce
Improving access to healthier food and drink options on NHS sites and beyond and, increasing the knowledge, skills, confidence and attitudes of NHS staff and others towards healthier eating and obesity prevention is a priority. This includes attainment of Healthy Working Lives awards for all acute and community hospitals, achievement of the Healthyliving Award plus on NHS sites, removal all soft drinks with added sugar content greater than 0.5g per 100ml from vending machines in hospitals and, including health promoting health service criteria in the specification for the combined vending contract for drinks, confectionery and snacks. Measures to demonstrate improvement
Number of NHS sites registered with Healthy Working Lives. Number of ‘Winning Weigh’ programmes in workplaces. Number of NHS Tayside dining areas (serving to staff and the public) holding the national
Healthyliving Award plus. FOCUS FOR 2015/16 Target healthy weight interventions at women of child bearing age from low income
families.
Achieve UK Baby Friendly accreditation as a minimum standard by NHS Tayside and Children’s Centres.
Implement the child healthy weight pathway and undertake a robust analysis of the necessary steps for healthy eating and physical activity for children, young people and families that address obesity prevention.
Continue to assist vulnerable families to develop fundamental food skills and access affordable healthy food.
Enable NHS Tayside’s Nutrition & Dietetic services to support partners in activities that prevent and control obesity.
Increase capacity and capability of the adult weight management service and address the specific needs of priority groups.
Undertake a system wide risk assessment of NHS Tayside’s seating provision for severely obese individuals.
Develop and implement obesity prevention and control strategies in the workplace. Devise a standardised framework supporting high-quality, consistent evaluation of obesity
prevention and treatment. Apply the principles of co-production and asset based approaches to the design and
delivery of all obesity prevention and treatment approaches.

15
KEY DELIVERABLES BEYOND 2015/2016 To help achieve the Scottish Government aims of having a higher proportion of people in a normal weight range, NHS Tayside will work to make the region an environment where healthy life choices become easier. Beyond 2015/16, the priority will be to take forward implementation of weight management pathways for children, young people and adults in target populations and a comprehensive multi-agency prevention programme. PHYSICAL ACTIVITY Physical Activity is driven by a number of Scottish Government policies formulated to get Scotland active: CEL 01 (2012) Health Promoting Health Service; The Physical Activity Implementation Plan- a More Active Scotland – Building a Legacy from the Common Wealth Games 2014; Active and Healthy Ageing - An Action Plan for Scotland 2014. PRIORITY ACTIONS Promotion of the benefits of physical activity for staff is taken forward through the Healthy Working Lives (HWL) programme. There has been information provided on the benefits of physical activity on NHS Tayside Staffnet and though notice board displays. There have been opportunities provided for staff to be active during the working day including promotion of walking outdoors at break times, use of stairs for health benefits as well as annual pedometer or stair climbing challenges. Active travel has also been promoted through a variety of routes including HWL and corporate routes. Information highlighting the benefits of physical activity and active travel has also been targeted at patients and visitors through notice board displays in patient waiting areas and the NHS Tayside internet pages. The national physical activity pathway has been implemented with associated training in the pre-assessment service across Tayside. There has also been a pilot of the use of improvement tools to evaluate progress in one area. Engagement has been held with various agencies in order to progress actions around physical activity and active travel e.g. TACTRAN, local authorities and NHS Tayside staff from various Directorates. Measures to demonstrate improvement Progress is continually measured by achieving/maintaining HWL Awards and providing satisfactory evidence of meeting the requirements of CEL 01. FOCUS FOR 2015/16 Through the HWL award programme there will be promotion of the benefits of physical
activity and active travel for staff as well as physical activity /active travel initiatives.
Carry out a travel survey of staff in conjunction with TACTRAN and Operations Directorate to inform the development of an overarching NHS Tayside Travel Plan.
Provide an NHS Tayside annual physical activity challenge, information and opportunities for staff to be physically active at work / commuting to work.
CEL 01 reporting requirements will direct the focus on the promotion of physical activity for
patients, visitors and staff. This information is not yet available for the 2015/16 reporting period.

16
KEY DELIVERABLES BEYOND 2015/2016 Develop key deliverables to demonstrate improvement, measurement and reporting on the
national targets set out within ‘Lets Make Scotland More Active’ for recommended physical activity levels and future CEL 01 reporting requirements.
LEARNING DISABILITIES The Keys to Life ten-year strategy document sets out the stark health inequalities faced by people with learning disabilities (LD) – significantly shorter life expectancy, increased risk of accompanying sensory and physical impairments, poorer physical and mental health than the general population. For example, the average
number of health co-morbidities in the population of people with LD at aged 20 is the same as for the general population at age 50.
The health inequalities faced by people with LD make a significant contribution to overall health inequalities. In order to address the health inequalities, there is a need to identify people who have LD and ensure that their additional needs are met. However, people with LD remain “invisible” on routine administrative health care data sets. The Scottish Government has issued guidance to redress this. PRIORITY ACTIONS NHS Tayside has acted on the Scottish Government guidance relating to the establishment of a database which would allow the ascertainment of health inequalities at locality level and the development of a SMART action plan to reduce health inequalities for people with LD. The overall purpose of the work is to improve wellbeing and to reduce health inequalities in order to promote health equity for people with LD and to protect their human rights. In keeping with Scottish Government guidance, a named public health lead has been identified, collaborative work between Public Health, Primary Care and Specialist Learning Disability Services is ongoing. NHS Tayside recognises that there is a need to strengthen the improvement in care of people with Learning Disability when they are accessing general hospital based services for physical healthcare reasons. Working with colleagues in partner agencies, for example social care, education, housing and third sector is essential within the Health and Social Care Integration agenda. A high level risk is around the difficulties in identifying people on routine data since data sources tend to underestimate the number of people who have a Learning Disability and who may need services. It is essential to record the additional needs of people with LD so that reasonable adjustments are made so that they can equitably access care. Several strands of work are underway and will be developed further to address this risk: Firstly, using the Read codes issued by Scottish Government in October 2014, a pilot identification of people with LD has successfully been undertaken in one practice. Discussions have begun around the roll-out of this to all practices so that when the national database, SPIRE is established, the data extracted from each individual practice will be as complete as possible. By February 2016, we will measure progress by the number of GP practices in which this Read code search has been undertaken in preparation for SPIRE.
17
Secondly, a locality based pilot, in Dundee, has evidenced the feasibility of describing needs of people with LD through recording the additional needs of people being seen in the community by the community LD teams on a database. The aim is to replicate this in other localities. Thirdly, NHS Tayside will explore, within appropriate information sharing governance arrangements, how recent data extracts may contribute to identifying those people who have LD and ensuring that health services are ready to meet their needs. A system which can “flag” the additional health care needs of people with LD, for example on eKIS, is required and fits with the wider work within the Improving Interpretation and Translation Strategy that NHS Tayside is undertaking to fulfil Equality Act responsibilities. A further high level risk is around the redistribution of resources that would enable the Specialist Learning Disability Services to support other services, including primary and secondary care to deliver high quality care where reasonable adjustments are made for LD service users, as described in keys to Life recommendations. By applying the “Triple Aim Framework” (Institute of Healthcare Improvement), NHS Tayside will be able to simultaneously pursue: 1. The health of the population who have LD. 2. The good health care experience of people in the LD population. 3. The cost per capita for providing care of this population so that health is maximised for a given
expenditure. FOCUS FOR 2015/16 Making people with LD visible on routine health data by completing the Primary Care Read
code search, developing and extending the locality LD database and exploring how best to use data extracts in order to meet individual health and population health needs, especially ensuring that additional needs are recorded and reasonable adjustments to healthcare provision made.
Committing to a dedicated primary care liaison resource to support General Practice and Primary Care, especially support for delivery of annual health checks (recommendation 21 from Keys to Life).
Working in partnership to ensure that people with learning disabilities receive the appropriate level of support in general hospitals, including appropriately funded support from familiar carers as well as from specialist learning disability acute care liaison nurses (recommendation 24 from Keys to Life).
Working with partner agencies within The Tayside Public Health Information Network (TAYPHIN) to identify the information required to support delivery of care within health and social care integration.
Completing a focused needs assessment for people with Learning Disability in Tayside, including discussions with people from the LD community, family and carers, analysing factors that contribute to person centred care and development of a Health Improvement and Co-production plan.
Ensuring that people with a particularly high level of need e.g. older people, those with
autism and young people transitioning into adult systems have their needs identified and met.
Assess patient pathways and redesign where necessary to support timely interventions and provide opportunities to improve quality of life and health across acute care, community based care, rehabilitation and enablement and to encourage social inclusion.
18
KEY DELIVERABLES BEYOND 2015/2016 Identification of the majority of people with LD in Tayside; the ability to describe their
health needs and how to meet them.
Availability of accessible data to measure a proportion of the health inequality indicators specified by Scottish Government.
Development of a SMART Action Plan to reduce health inequalities for people who have a learning disability.
19
The LDP should set out the local actions to be taken to ensure that the relevant parts of the workforce will have the capacity, training and relevant protocols to carry out the duties under the Children and Young People (Scotland) Act 2014: action – named person service for every child up to aged five and a single statutory Child’s Plan for every child aged under five who requires one – by August 2016.
The Scottish Government’s vision is for Scotland to be the best place in the world to grow up. GIRFEC (Getting It Right For Every Child) is the national approach for improving outcomes and life chances for children and young people. Parts 4 and 5 of the Children and Young People (Scotland) Act 2014 address two key elements of the GIRFEC approach, namely the Named Person Service and the Child’s Plan. The Act places a duty on Health Boards to provide a Named Person Service for every child from birth until they commence school. The Children and Young People (Scotland) Act 2014 has a phased implementation, with the parts addressing GIRFEC being introduced in August 2016. PRIORITY ACTIONS The framework to ensure NHS Tayside is prepared for implementation by August 2016 consists of a number of multi-agency and single agency groups as follows: The Tayside GIRFEC Group is a multi-agency group with representation from senior
officers from the three Tayside Local Authorities (Perth & Kinross, Angus and Dundee), NHS Tayside, Police Scotland, the third sector and the Scottish Government. The Group is currently chaired by the Chief Executive of Dundee City Council and NHS Tayside is represented by the Child Health Commissioner.
Each of the three Tayside Local Authorities has a multi-agency GIRFEC Implementation Group with representation from the relevant CHP Children’s Services.
The NHS Tayside GIRFEC Group is a single agency group chaired by the Child Health Commissioner, who is also the CEL 29 Change Manager.
The NHS Tayside GIRFEC Group has created and oversees the Implementation Plan which addresses eight key areas as follows: 1. Vision, values and principles 2. Consent and Information Sharing 3. Role of the Named Person 4. Lead Professional 5. Electronic Sharing of Information 6. GIRFEC Assessment 7. Child’s Plan 8. Self Evaluation In addition to the GIRFEC Implementation Plan, work is also being undertaken to cross reference the plan against the recently created “Touchpoint Programme” document circulated by the National Implementation Support Group. Inextricably linked to the issue of ensuring staff capacity and training is the work being taken forward under the Transforming Health Visiting and School Nursing Service. In NHS Tayside, this agenda is being taken forward by the Chief Nurse for Children and Families and an Implementation Plan exists for this work too. With regard to the Family Nurse Partnership, this

20
has reached small scale permanence throughout Tayside with all eligible young mums being offered the programme. The challenge arises from NHS Tayside, as one health system, working with three separate local authorities, each of whom has their own pace of progress, priorities and ideas. To mitigate this challenge, the overarching Tayside GIRFEC Group supports, where possible, undertaking work on a Tayside-wide bases. Examples of this are the production of a basic GIRFEC e-learning module and Lead Professional Training tool which are available for all agencies. In addition, several short-life multi-agency working groups with membership from across Tayside are meeting to agree a consistent Tayside-wide approach to aspects of the Child’s Plan, sharing information and assessment. Future discussion will also focus on delivering a consistent, multi-agency, pan Tayside message to the public, particularly parents and carers. To address the area of IT capability and compatibility in respect to information sharing, the Tayside Data Sharing Group, in considering the information sharing requirements of the Public Bodies (Joint Working) (Scotland) Act 2014, will ensure a framework which can also address the requirements of the Children and Young People (Scotland) Act 2014. The close working relationship between the Child Health Commissioner, Chief Nurse, Children & Families, and Local Authority colleagues, will ensure that the GIRFEC Implementation Plan and Transforming Health Visiting and School Nursing Implementation Plan complement each other effectively and efficiently. FOCUS FOR 2015/16 The NHS Tayside GIRFEC Implementation Plan sets out the actions required to ensure readiness on the part of NHS Tayside, and all these actions require to be completed. These actions underpin delivery on the eight key areas which were outlined on the previous page. As mentioned, this Plan will be augmented with reference to the Touchpoint Document and will also focus on ensuring communication with the public is robustly addressed. The Plan will also sit alongside the Transforming Health Visiting and School Nursing Implementation Plan. In addition, however, there are other areas which will require focus in 2015/16 and these include: Other elements of the Children and Young People (Scotland) Act 2014 (Children’s Planning;
Children’s Rights; Corporate Parenting).
The Early Years Collaborative - ensuring continued commitment and progress with the three Tayside EYCs.
The work of the Chief Nursing Office focussing on transforming the School Nursing Service.
KEY DELIVERABLES BEYOND 2015/2016 Progress beyond 2015/16 will be measured against the developed suite of primary and
supporting measures focussed on Early Years. These consist of the three high level stretch aims of the Early Years Collaborative focussing on stillbirth, infant death and developmental concerns at 27 – 30 months.
21
The LDP should set out how services will support a positive care experience delivered in accordance with the “five must do’s with me”. Outlining the key local action being taken to transform the culture to support staff and the public to be open and confident in giving and receiving feedback; widely publicise the information people need to give feedback and make complaints, and the support available for them to do so; and with a focus on learning from feedback, implementing the changes; and telling people what improvements were made as a result of their feedback. The plan will include information on how progress will be measured locally.
There are a range of national drivers in relation to person centred care including:
The Patients Rights (Scotland) Act 2011. The Healthcare Quality Strategy (2010). 2020 Vision. Listening and Learning Report: how feedback, comments, concerns and complaints can
improve NHS services in Scotland. Scottish Health Council (2014). PRIORITY ACTIONS Within NHS Tayside, person centred care is a key strategic priority with a broad definition that includes family, carers and staff. The ambition of NHS Tayside’s Clinical Governance Strategy is that “every day every one of us delivers, sees and experiences standards of care that we would want for our own loved ones. This can only happen by putting the patient at the centre of everything we do, working as a team and making sure we have the information and data we need to deliver excellent treatment”. Creating the right conditions for staff to provide safe, effective person-centred care is vital, therefore NHS Tayside has developed in partnership with staff, patients, carers and the public the Vision, Aim, Values and Behaviours to express what they believe to be the best environment to deliver person-centred, safe and effective clinical care. Underpinning the Clinical Governance Strategy is NHS Tayside’s Care Governance Measurement & Monitoring Framework which details eight specific ambitions and key actions to improve quality. One ambition focuses on improving patient experience ‘Patients, carers and members of the public will increasingly feel like they are being treated as vital and equal partners in the design and assessment of their local NHS. They should also be confident that their feedback is being listened to and see how this is impacting on their own care and the care of others.’ In order to achieve this, the following programmes of activity have been progressed: Feedback We understand that feedback about the experiences of our patients is an important gauge of the service we provide. Feedback can be used as a measure of the quality of our service and allows patients to be more involved in their own care and contribute to improving care. NHS Tayside has identified three key priority areas for progression during 2015/16 in relation to feedback, these priorities are as follows:

22
1. Identification and implementation of accessible feedback mechanisms. 2. Undertake and act on whole systems review of the complaints procedure, ensuring the
implementation of quality assurance mechanisms and objectivity of investigations, and the implementation of all key elements of ‘Can I Help You?
3. Building capability (through strong leadership, role modelling and professional supervision) in frontline staff to optimise patient and carers’ experiences and to act appropriately when individuals raise dissatisfaction or make suggestions.
FOCUS FOR 2015/16 Raising public awareness of how to provide feedback.
Ensuring feedback mechanisms are accessible to our diverse population.
Implementing the use of validated tools for gathering feedback through the use of volunteers.
Developing our systems to support timely provision of information to both the public and staff on actions or improvements made in response to feedback received.
Improving and gaining assurance regarding the quality of our complaints handling.
Agreeing and implementing standards for complaint handling that ensure objectivity and transparency of the process and outcome.
Development of a culture that values all forms of feedback, including the empowerment of all staff to resolve things early – with apologies given freely and action taken where things go wrong – and a strong leadership focus on complaints handling and governance arrangements.
Improving Care Experience NHS Tayside has engaged with the Person-Centred Health and Care Collaborative since its inception and has made progress with implementing aspects of person centred care principally through its improving care experience programme which incorporates four existing improvement programmes - Releasing Time to Care plus (RTC plus); Caring Behaviours Assurance System (CBAS), Leading Better Care (LBC) development programme and Dementia and Delirium care. Progress with actions that support the ‘five must do’s with me’ includes:
implementing person-centred visiting and person centred handovers; investing in values based reflective practice facilitator training; routine use of patient feedback in quality improvement activity; public involvement in service evaluation and design; introducing “teach back”; testing the use of volunteers to conduct telephone patient experience surveys and patient
interviews; training and protocol implementation to support early detection and treatment of delirium
in all settings; improving the reliability of the use “All About Me” for all patients with cognitive
impairment, learning disability or specific communication needs; implantation of SAGE and THYME® communication training to support all staff in health
and social care to effectively support people who are in emotional distress; training of staff in the use of health behaviour change techniques, evidence based
interventions that support person centred care and enhance patient experience, and anticipatory care plans;
customer care training; development and use of Team Vitality & Care Questionnaire, supporting individual clinical
teams to use results to improve team working and person centred approach to care.

23
NHS Tayside recognises the value of volunteers and volunteering particularly the contribution volunteers make to health across all sectors. NHS Tayside’s plan for volunteering in 2015/16 mirrors the three national outcomes - 1. Volunteering contributes to Scotland’s Health.
2. The infrastructure that supports volunteering is developed, is sustainable and inclusive.
3. Volunteering, and the positive contribution it makes, is widely recognised, with a culture which demonstrates its value across partners involved.
There are currently 754 active, formally recruited volunteers providing services to enhance patient care across NHS Tayside. FOCUS FOR 2015/16 Volunteering will continue to be provided as a single Volunteering Service across Tayside.
Review the Volunteering Policy to incorporate changes associated with Health & Social
Care Integration.
In order to recognise the contribution volunteering makes to health, a celebration of volunteering is planned as part of the National Volunteer Week and long service awards will be presented to volunteers by NHS Tayside Board members.
The objective for NHS Tayside in 2015/16 is to build on the work detailed above which focussed on developing capacity and capability within the workforce to drive changes in practice that are aligned to the person centred programme particularly to support the implementation of the ‘5 must do’ elements. KEY DELIVERABLES BEYOND 2015/2016 The aim within NHS Tayside is to test a model that brings together a multidimensional
approach to improving care and care experience by supporting the Nursing/Midwifery, Medical and AHP leads within individual teams to use a range of quality improvement methodologies including values based reflective practice, improvement methodology and critical companionship to deliver sustainable improvements in person centred care.
Outcomes will be routinely reported through existing governance arrangements within the
Board, the metrics will be reassessed every 6 months alongside routine, real time data which will be used to support teams and facilitators to refine their improvement efforts.

24
The LDP should set out the priority actions the NHS Board is taking across the Scottish Patient Safety programmes of work, the plans for spread and sustainability and the impact they are having on patient care, including examples from each programme of how safety of care has improved in the last 12 months. This should include plans to ensure that governance and leadership across managerial and clinical staff is in place for each programme and that robust data collection methods are in place to demonstrate improvement. Boards will work towards implementing the recommendations set out in the Vale of Leven Inquiry Report.
The overarching aim of the Scottish Patient Safety Programme (SPSP) is to reduce avoidable harm to patients by improving the safety of patient care at all points of care delivery with a goal to reduce HSMR by 20% by December 2015. PRIORITY ACTIONS The multiple and increasing programmes attached to SPSP has led NHS Tayside to focus on a more systematic approach to improving patient safety where it is seen as more than a national programme, with improvements that address local safety priorities identified by frontline clinicians and the voice of patients and carers. Following consultation with frontline clinical teams and data from patient feedback, mortality reviews, and Significant Clinical Events Analysis, the following three areas have been identified as NHS Tayside priorities for patient safety; multidisciplinary team working, deteriorating patients and medicines safety. In August 2014, NHS Tayside launched a new Patient Safety Network to support the patient safety agenda for the next two years and will collectively support the individual aims of each national patient safety programme, more details of which can be found at; http://www.scottishpatientsafetyprogramme.scot.nhs.uk/programmes The Patient Safety Network will bring together and support multidisciplinary team members from across organisational and professional boundaries to improve the safety of care across the whole patient pathway. It will create the conditions for improvement by providing a forum to; develop staff, create knowledge, exchange information and spread good practice. It will also provide the opportunity for staff to develop their Quality Improvement Skills and to move forward Patient Safety activities within their service with a curriculum of topics delivered to support this. NHS Tayside has delivered considerable improvements in patient safety across all the programmes. Examples of this include: A sustained reduction in cardiac arrests within Ninewells Hospital, with the most recent 15
data points below the centreline. Our Intensive Care Unit in Ninewells Hospital has had a 0% central venous infection rate since June 2013.
Intensive Care Unit in Perth Royal Infirmary has gone 11 months without a ventilator acquired pneumonia.

25
Within the primary care setting, 100% of our GP practices have undertaken the Safety Climate Survey and 96% of practices have completed two trigger tools (structured case note reviews), both of which aim to improve patient safety.
Our maternity unit continues to demonstrate improvement with each of the elements of the sepsis six bundle. The median time to first antibiotic is currently 35 minutes (recommendation within 60 minutes).
Within the mental health setting there is a sustained reduction in patients experiencing restraint.
FOCUS FOR 2015/16 A robust and clearly defined measurement framework (ROI) has been developed, aligned
to the measurement plans which already exist through the national programmes. This framework will support the three workstreams and will be used to coordinate and monitor progress across the organisation. Reporting against this framework will be embedded within the existing clinical governance reporting structures.
Locally defined patient safety priorities, CEL 19 published in August 2013, sets out a set of
ten patient safety essentials to be implemented everywhere in NHS Scotland. Work is now being led by the Patient Safety Team, the Nursing and Midwifery Directorate and the Infection Control Team to develop local mechanisms and tools to support directorates and teams to provide assurance that the ten essentials of patient safety have been reliably implemented and comprehensively spread in all relevant clinical areas.
Early testing of a ‘patient safety toolkit’ to self assess or peer review reliable
implementation of the ten essentials is underway to provide assurance including; direct observations, soft intelligence, conversations with patients and staff and dashboards. They will also support directorates and teams to ensure that any recording or monitoring of these measures is proportionate and does not detract from the provision of high quality, compassionate patient care by generating an excessive data burden as a step down approach to process measurement will be incorporated.
KEY DELIVERABLES BEYOND 2015/2016
Continue to develop and deliver the Scottish Patient Safety Programmes, striving to reduce
mortality, harm and avoidable injury in a variety of care settings including Acute Adult Care, Maternity, Neonatal, Paediatrics, Mental Health and Primary Care settings including:
The development of the Patient Safety Network aimed at ensuring sufficient Board
level capacity and capability to deliver, report and learn from the safety programmes within the context of a broader whole system approach to quality improvement capacity and capability.
Supporting effective implementation of the Scottish Patient Safety Indicator (SPSI). NHS Tayside is working in partnership with Health Improvement Scotland and
NHS Borders to develop and test the Health Foundation prototype work focused on the measuring and monitoring of safety www.health.org.uk/publications/the-measurement-and-monitoring-of-safety

26
Vale of Leven Inquiry Report A mapping exercise against the recommendations from the Vale of Leven Inquiry Report was undertaken by NHS Tayside. This focused upon the position of NHS Tayside against the recommendations and identification of key themes which required further work to address any adverse findings and shortcomings. As a result of the mapping exercise, an overarching NHS Tayside Improvement Action Plan was developed. To drive continuous improvement and demonstrate clinical and professional leadership, the Improvement Action Plan will be delivered by establishing a small number of multidisciplinary workstreams under the auspices of a Core Steering Group chaired by the Board Nurse & Midfwife Director and Medical Director. The local reporting structure for the overarching NHS Tayside Improvement Action Plan will be conducted through NHS Tayside Improvement and Quality Committee. NHS Tayside will work with the national Implementation Group and Reference Group to take forward the recommendations from the Inquiry Report. A linkage both nationally and locally to demonstrate the monitoring and implementation of the recommendations is forming part of the work of both national Groups.

27
The LDP should set out the prioritised local actions that are being pursued to increase capacity in primary care and the resources identified to achieve this. The plan should also identify where national actions would help local delivery.
The key strategic areas and high level plans for Primary Care services in Tayside take into account the available national, international and professional body of literature and evidence. These plans are being set out with a view to developing over the next five years towards 2020. Although there is a heavy emphasis on general practice within this section, these issues apply equally to the other contractor bodies within pharmacy, dentistry and optometry and the wider primary care team. The objectives set out within the five areas of service planning, interfaces, infrastructure, workforce and leadership have been benchmarked against the national Route Map to the 2020 Vision for Health and Social Care and connect closely with the work ongoing across the whole Tayside system, including Transforming Outpatients, Shaping Surgical Services, the Older People’s Board, Integrated Partnerships and the Health Equity Strategy. Our Strategic Work Plan (summarised in the driver diagram below) also takes cognisance of the need to consider emerging agendas within areas such as pharmacy (Prescription for Excellence), optometry and community dentistry. In addition to this, our strategic narrative has been set against the emerging health and social care integration agenda.
PRIORITY ACTIONS
The following strategic areas must be considered as a “whole” in order to effect the transformational change in culture and practice which will be required to meet our challenges: Throughout this all runs our “golden thread” of” Prepared Patient - Prepared Process - Prepared Professional.” Leadership and Workforce “The Prepared Professional” The importance of clinical leadership is now recognised at all levels, and is well supported in Tayside. As the importance of primary care involvement in service planning and development becomes increasingly recognised and valued, so has the involvement of primary care leaders in diverse forums from locality to national level. The Associate Director of Primary care role (7 sessions per week) is supported by primary care clinical leads in dentistry, optometry, pharmacy and each of the three Community Health Partnerships as well as out of hours services and Managed Clinical Networks. A Leadership Framework has been developed, and there is active and ongoing participation within a number of leadership activities at national regional and local level. Tayside is a pilot Board for paired learning, and is exploring how this can be done at both a primary/secondary care level, and between health and social care. FOCUS FOR 2015/16 Work with Primary Care providers and our partners in Public Health and Local Authorities
to consider existing patterns of demand and workload and to aspire to improving quality in primary care in reviewing models of consultation.
28
We will look to explore different kinds of consultation with practices and patients, using the best evidence and improvement methodology to support tests of change. This will include use of IT including e-consultation (NHS Tayside has offered to be a pilot Board for the work being developed with NHS 24), patient access to records, and learning from access surveys. Our optometrists and dentists already have close links with acute services with shared learning across a number of areas. Our locality pharmacist model is well placed to fit the strategic priorities within Prescription for Excellence. We are working with our Local Medical Committee to undertake a local workforce survey review to feed in to the Board’s Workforce Plan.
Continue to support and test new ways of working, building on successes to date including
health inequalities and rural fellows, working with NHS Education for Scotland supporting research and personal development for newly qualified GPs, helping to retain skills and support succession planning. New proposals include integrated primary care roles, working across areas of interface such as medicine for the elderly, unscheduled care and paediatrics as well as supporting practices. We have successfully tested this approach as part of our unscheduled care / winter planning work, bringing a salaried GP and locality pharmacist into an integrated team working across a locality and helping to enable patients to stay at home and reduce length of stay and admissions. Our optometrists and dentists already have close links with acute services with shared learning across a number of areas. Our locality pharmacist model is well placed to fit the strategic priorities within Prescription for Excellence.
Ensure a clear career structure and leadership development opportunities, with nationally
agreed training and pay scales appropriate to the role. We will look to develop this further, working in collaboration with national and local partners to test models. Examples of this include the leadership and development structure we are implementing around out of hours care, with a substantive Clinical Director post supported by Locality Leads to help shape the future development of a whole system 7-day working across both primary and secondary care.
We are building good links with the newly established Tayside Academic Health Sciences Network, with shared learning opportunities around leadership developments for both undergraduate and postgraduate students in partnership with the Deanery.
National Action That Would Support Local Delivery Clear strategic direction around national workforce planning for GPs, based around risk
stratified population per whole time equivalent GP. National funding to support leadership development and expansion of programmes to
further include more of the primary care team. Career development pathways for clinical managers. Explicit support for organised Protected Learning Time with cover provided via NHS 24.
Resource (finance and expertise) to support leadership development. Endorsement for the leadership development proposals developed by the Royal College of
General Practitioners. Explore contractual opportunities to allow more accurate workforce assessment. Develop shared outcome measures across priorities such as Prescription for Excellence and
the new GMS Contract. Networking support for developments such as optometric prescribing and dental
inspections. Resource Shift Identified Allocation of a proportion of winter plan monies enabled the successful enhanced care at
home pilot, supporting MDTs to proactively manage patients in their own home, and

29
promote earlier discharge. Change Fund and Integration Fund monies continue to support the application of the model at scale.
Leadership development and funding support has been identified from Board allocations, as well as Integration Fund monies this financial year.
Support from our Organisational Development Team is provided in Primary Care across a number of different levels.
Planning and Interfaces “Prepared Process” “Prepared Patient” As healthcare policy and delivery adapt to meet the changing and growing demand for services, so too must the traditional interfaces. The ability to move seamlessly across interfaces at all levels is an essential requirement if we are to deliver safe and effective care. We need to have a reliable and consistent “Prepared Process”. The advent of a more “Scottish” GP contract in 2013 has resulted in some changes designed to reflect national planning priorities, most notable this year being patient safety and the introduction of anticipatory care planning within a contractual context. It is anticipated that this contract will not change significantly over the next year or two, and its complexities and history mean that, at best, it will be a useful piece in what will require to be a much bigger toolkit. The GMS contract, as yet does not formally align with the integration agenda, other than in broad terms, most notably the use of Anticipatory Care Plans. Growing demand and complexity continues to drive increasing referral rates and unscheduled care, and any attempts to tackle waiting times and national “targets” must start at the beginning of the patient’s journey in the community, and service planning needs to be considered in this context, starting with the “Prepared Patient”. FOCUS FOR 2015/16 Work to develop patient focussed, evidence based end to end pathways of care needs to
be strengthened and will be an NHS Tayside priority. Initial pathways will focus on areas such as frail elderly, dementia, assess to admit and complex care. The role and input of all parts of the primary care system, including social care, must be considered as part of any pathway proposal, and should be done as part of a single system approach. These pathway developments will take account of the national strategic drivers such as Prescription for Excellence, Review of Nursing in the Community and the New Role for Health Visitors.
Existing mechanisms, such as the GP Contract will be used to support the embedding of
pathways – examples to date include colorectal referrals, use of digital photography on dermatology referrals, falls, and DVT. This will be further developed and new options investigated.
New ways of sharing data and information will be explored. We will look to produce
primary care data reports utilising individual clinician data and agreed data sets. We will facilitate practices sharing and learning from data (including from Local Authorities) in local clusters which will help inform the local population needs and service requirements. We are developing a primary care data set encompassing care governance and quality standards across all four independent contractors, and reported to NHS Tayside Board (and in due course, to the Integrated Joint Boards). These will be developed to take account of the proposed integration measures.

30
Seek to engage with practices willing to consider new and innovative models of care, with a focus on reducing unscheduled care, outpatient attendances, and more integrated working. A number of opportunities are beginning to emerge around tests of change – most notably in Dundee with Whitfield and Menzieshill / Maxweltown Local Care Centre models, the work around Enhanced Community Support in Broughty Ferry, Monifieth and Carnoustie, using the Integrated Resource Framework to drive service delivery discussions in Perth & Kinross, and options for new kinds of service delivery across practices in Tayside, which include exploring the “Nuka” model and implementing the “year of care“ model across the most deprived practices in Dundee to improve pathways of care for diabetic patients, and in rural areas such as Letham, Angus.
Primary care will be a key component of the developing NHS Tayside Clinical Services Strategy, with development having the active engagement of the Local Medical Committee.
Support the establishment of Health and Social Care Partnerships in Tayside to create the
conditions for the meaningful engagement of primary care in this important agenda. This should be conducted by clear job planning, support for leadership and development, and accountability. BMA research has shown that the most important enablers to supporting integration are a collaborative culture, good professional relationships and effective leadership. Work requires to be taken forward with new partnerships to agree what this needs to look like in each area.
In promoting the primary/secondary care interface, we will continue to develop the
positive culture of collaborative working through building on the work of Joint Clinical Boards, Older People’s Board, local interface groups, clinical pathways, sharing of significant events, electronic communication and messaging systems. As demand continues to grow, both in primary and secondary care, we will create opportunities for joint working for integrated pathways of care, service planning and shared learning.
National Action That Would Support Local Delivery Consideration of national pathways and national purchase of systems such as “Map of
Medicine” would allow implementation of local pathways of care at a national scale. More “joined up thinking” at national level to consider how national strategy could be more
aligned to support pathways of care which both begin and end in primary care. Resource Shift Identified By working in collaboration with local partners, Tayside’s property strategy developments
are now starting to provide community infrastructure to support multidisciplinary models of care in buildings that are both fit for purpose and value for money. Site rationalisation allows a percentage of funding to be reinvested in service development. Continued dialogue will be held between primary and secondary care around the resource shift required to deliver increased activity.
Technology and Data FOCUS FOR 2015/16 Support joint working to ensure that the information that is shared is timely, complete and
accurate to support patient journeys. We will further develop the single electronic patient record, the Key Information Summary (KIS) and electronic referral and discharge documentation to enhance sharing of information across patient pathways. This will also be considered as part of NHS Tayside’s refreshed eHealth Strategy.

31
Continue to test the sharing of learning from significant events through incident recording using the DATIX system and extend this to all practices during 2015, allowing electronic sharing of incidents, complaints and events. This will be further rolled out to the remaining three independent contractor streams. We will seek to implement full roll out of electronic referral between primary and secondary care optometry, and facilitate access to NHS Net and the Clinical Portal for all independent contractors.
National Action That Would Support Local Delivery Agreed target dates for developments such as e-pharmacy, optometry referral. A national eHealth Strategy which enables delivery at Board level. Support to enable patient access to records, booking, e-consultation and decision support
and sign posting. An agreed primary care IT provider to allow for the development of a system which can
interface with other existing systems. Contracts and Resources Within Tayside the majority (63/65) of general practices have a 17C Contract. There is currently no appetite to consider other contractual models such as 17J. However, locality models are now well established across all three Integrated Joint Boards, and through leadership development, support groups of contractors are now starting to consider the total community resource available and what service delivery models may need to be in place for the future. There is a growing awareness of the need to consider how all four independent contractor models can work better together, and how these models can support the integration agenda. If post 2017, the new GP Contract is predicated on the role of the “expert generalist” providing co-ordination and management of complex care in the community then there will be a significant need for other resources in the community to consider taking on roles traditionally undertaken in practice. These could include large elements of prescribing, public health (including immunisations) and mental health. Supporting people to self direct their own care with direct access to specialties such as physiotherapy, occupational therapy, social care and employability will free up more GP time and resource. Direct access to other community specialists such as optometrists, dentists, midwives has already demonstrated a successful shift in how people access services. FOCUS FOR 2015/16 Support investment in primary care estate and infrastructure, which recognises the wider
context of what we are trying to deliver in the future, using new and innovative models of commissioning. Some good examples include working with communities to identify land and fundraising (Edzell), and the collaboration with Dundee City Council which saw the new Whitfield Local Care Centre open in April 2014, followed by plans for Menzieshill and Maxwelltown in 2015/16 (which includes the potential to explore new service models for primary care, taking on management and delivery of services currently being delivered in secondary care such as family planning, dermatology/leg ulcers, continence services).
Prioritise investment in services and facilities in places which match the growing
demographic changes, and which should be planned and designed in partnership wherever possible. The Carse of Gowrie should be considered in this context.
32
Utilise the roles and contractual frameworks of other independent contractors alongside general practice. For example, the new Pharmacy Contract and the “Prescription for Excellence” agenda will be explored, ensuring the patient accesses the right professional at the right time and in the right place. Direct referral between primary and secondary care optometry and dentistry is well established, and the advent of improved IT systems will help to further strengthen this.
Further strengthen the roles and skills of community nursing including district nursing,
health visiting, school nursing, public health, mental health and minor injury and illness nursing teams. We will look to develop locality “hubs” enabling provision of a wide range of services including minor illness and injury, phlebotomy, long term condition monitoring, pre-op assessment, wound management and community clinics.
Work with patients and local communities to understand together the difficulties and
challenges they face accessing care ensuring that feedback, stories, learning from significant events, formal engagement and self management support are all embedded within the primary care culture. We will however consider more radical reviews around access and demand across the system, patient held records, the use of telehealth and fully utilising the opportunities offered by new infrastructure. NHS Tayside will look towards our partners in the third and independent sectors to play a much bigger role and above all we will develop the principles of the “Prepared Patient” in partnership utilising the principles of co-production.
National Action That Would Support Local Delivery National dialogue around how people can self direct and access health care advice. Helping to disseminate and facilitate learning. Support acute targets which match primary care priorities. Consider the public health agenda alongside contracts and national targets. Commission research to support evidence based outcome measures. KEY DELIVERABLES BEYOND 2015/2016
The narrative above sets out the key strategic priority areas which will be taken forward to achieve our Vision for Primary Care services in 2020. The “golden thread” of the Prepared Patient – Patient Process – Prepared Professional will continue to run through all our work, and help bind us to the work of others at individual, local, regional national (and international) level. The driver diagram below sets out the main high level strategic objectives which we will look to develop over 2015/16 as part of NHS Tayside’s Clinical Services Strategy and which will support our developing integration agenda. This will be articulated within the NHS Tayside Clinical Services Strategy with measurable outcomes and timeframes set within a Strategic Work Plan and Financial Framework reporting to Health and Social Care Integrated Boards.
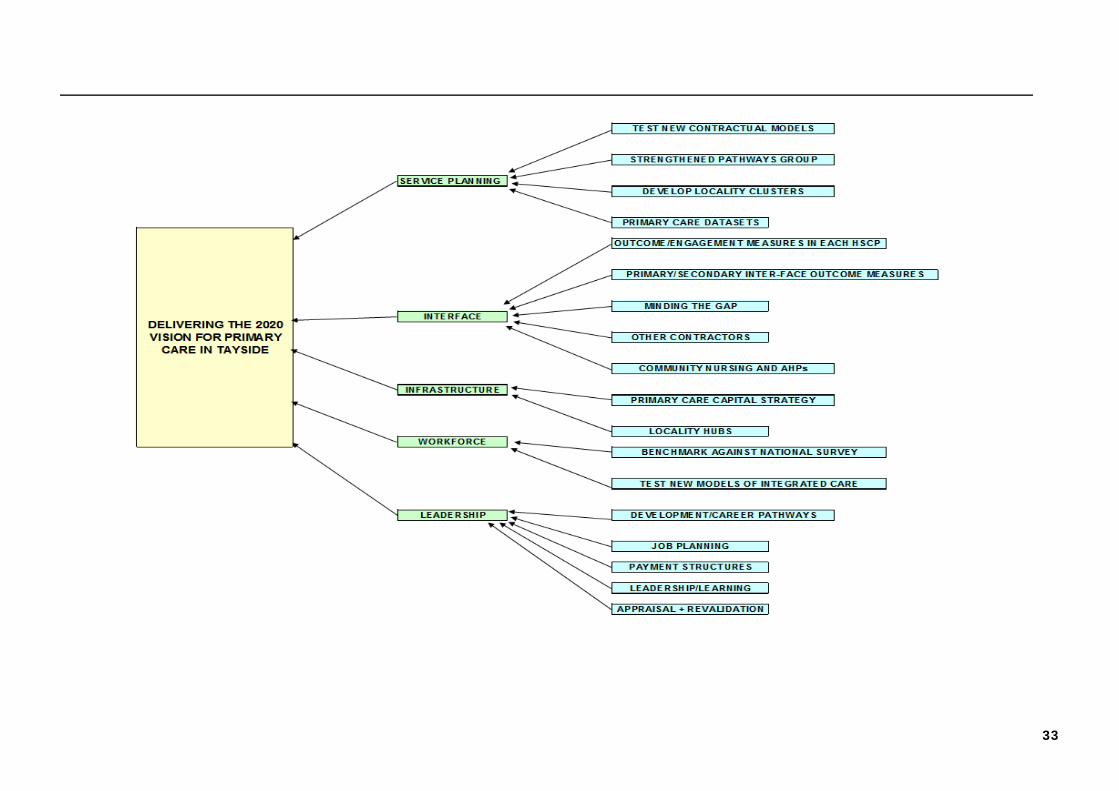
33
34
Integrated partnerships will be required to establish a Strategic Planning Group to prepare the Strategic Plan – this group will include representation of the key stakeholders. The LDP should set out the key local actions that are being pursued to ensure effective involvement of clinical and care professionals in the Strategic Planning Group. The plan should also set out the redesign priorities emerging for the integrated care pathways delivered in the community.
NHS Tayside is working with the three constituent local authorities, Angus, Dundee City and Perth & Kinross to establish health and social care partnerships in accordance with the Public Bodies (Joint Working) (Scotland) Act 2014 and associated Statutory Guidance and Regulations. The partners in each area are building models of care consistent with the Government’s 2020 Vision for Health and Social Care. The focus of the partnerships will initially be on adults and older people and the intention is to establish the partnerships in accordance with the “body corporate” model and the partners have prepared Draft Integration Schemes for the creation of Integration Joint Boards (IJBs) in each area in accordance with the regulations. Work has also commenced on the preparation of Joint Strategic Commissioning Plans so that once the Ministerial approval of the schemes is secured, the plans can be agreed, enabling the formal establishment of the IJBs and the transfer of functions and responsibilities before or on 1 April 2016. This work will reflect the strategic direction set out in the NHS Tayside ‘Rich Picture Vision’ and the development of the NHS Tayside Clinical Services Strategy and will connect with the Community Plans and Single Outcome Agreements for each partnership area. PRIORITY ACTIONS
There are in place regular steering groups to progress integration at a Tayside wide level in each area, we have worked with our local authority partners to put in place shadow board arrangements and the appointment of Interim Chief Officers, progressing to establish the IJBs and appoint the Chief Officers on a designate basis. It is anticipated that the draft schemes will have been submitted prior to 31 March 2015 and that these will be approved within the scheduled 12 week period set out by Scottish Government for the Ministerial Approval and Order. The planned schedule is for the Joint Strategic Commissioning Plans to be completed and agreed by September 2015, enabling the formal establishment of the IJBs in autumn 2015. The transfer of functions and responsibilities to the IJBs is anticipated on or before 1 April 2016. The partners are also agreeing a range of governance frameworks to strengthen the assurance in support of the move towards integration, including:
Clinical, Care and Professional Governance Framework (including feedback) Financial and Audit Governance Framework Workforce and Staff Governance Framework Joint Risk Management Strategy / Framework
There is also in development integrated workforce planning, information sharing and data handling, corporate and support services and participation and engagement arrangements.
35
We will agree the range of services that are within scope that will be directly managed or hosted and those that will be included within the “Large Hospitals” definition and will detail the functions, services and responsibilities that will devolve and the associated budgets and set aside amounts. These will be the subject of scrutiny through the due diligence process to ensure that there is openness and transparency around the proper transfer of the functions and responsibilities to the IJBs. Although the specific proposals are focussed on health and social care integration involving principally NHS Tayside and the local authorities, it is the clear intention in each partnership to develop a fully inclusive partnership to include the third and independent sectors as well as patients, service users, carers, communities and individuals. The partners have agreed and submitted plans and proposals for the Integrated Care Fund to support the implementation of new models of care. Importantly, at the heart of the integration work will be the development of integrated locality service delivery (on a multi-disciplinary team basis) and locality planning. This will involve considerable workforce development and workforce planning and organisational development. We have already agreed planning and delivery localities within each partnership area, built around natural communities, neighbourhoods and clusters of GP practice populations, on which to focus the locality development work. We acknowledge the challenge of engaging clinicians, professional and practitioners within localities and will work to build on the existing strengths of joint working at the very local level, particularly around the best practice from our work on reshaping care for older people supported through the Change Fund. A particular challenge will be the engagement of primary care practitioners, particularly General Practitioners in the localities, clusters and MDTs. We will identify GP practice leads, GP Locality / Cluster Leads and will build and strengthen locality team working as well as connecting acute and primary care integrated working through a clinical engagement and development process. The aim will be to ensure that the vision of supporting people to keep well at home and within the community with planned and scheduled care, reducing crisis admission to care and to hospital through unscheduled care will be a key aim, and this will be based around making community the right place. The development of the support networks in localities will be supported by work with acute care and large hospitals with the aim of these becoming more community facing and the development of an Integrated Care Collaborative that will ensure cohesion between the Strategic Hospital Plan (to be developed in partnership) and the Joint Strategic Commissioning Plans for each area, ensuring a joint investment strategy for the “set aside” amounts for the unscheduled care pathways. While NHS Tayside will continue to meet the challenging targets for unscheduled care, particularly through Accident and Emergency, we are increasingly challenged to meet targets for reducing hospital admissions for over 75 year olds and to manage capacity and flow through acute care due to unscheduled care admissions and increasing complexity and frailty. This is impacting upon the ability to manage care through hospital, to maintain emergency and elective pathways of care and to ensure safe, effective and timely discharge home or to an appropriate care setting. While we have worked in partnership to consistently meet the target for discharge of patient within 28 days during 2014/2015, this is proving increasingly challenging and we will develop improvement plans in each area to meet the new target for the discharge of patients within 14 days of being medically fit. A particular concern has been the increasing trend in the overall numbers of people whose discharge from hospital has been delayed, particularly those patients delayed in acute hospitals.

36
We will work within each partnership to use the additional delayed discharge funding allocation over the next three years to create capacity to reduce demand pressures, reducing unscheduled care admissions, further improving discharge planning and moving towards immediate discharge or transfer of patients from acute care. We will build on the success of the Enhanced Community Support model in moving from the positively evaluated pilots to scaling this up and testing within whole localities, starting within the South Locality in Angus and rolling out to other areas. We will also build on the effectiveness of our work on the development of community based teams for dementia care across Perthshire and test similar models within Angus and Dundee. This will strengthen our capability to further deliver on the targets for identification of people with dementia and provision of post diagnostic care and support. As part of the Clinical Services Strategy, we will seek to release capacity and resources to strengthen our community teams through more efficient use of our property and estate and through operating from fewer sites. This will include the re-provision of community hospital care and a re-focus towards planned and step-up care. We will seek to re-provide care from Royal Victoria Hospital, Dundee and to develop a new sub-acute care facility for the city. FOCUS FOR 2015/16 We will continue to build the health and social care partnerships in conjunction with partners by: Securing Ministerial approval for the Integration Schemes.
Supporting the implementation of the plans and proposals within the Integrated Care Fund Plans.
Completing and agreeing the Joint Strategic Commissioning Plans for each partnership area.
Establishing the Integration Joint Boards and appointing Chief Officers.
Completing all governance and supporting frameworks to underpin the partnership arrangements.
Transferring functions, responsibilities and budgets to the Integration Joint Boards on or before 1 April 2015.
We will also;
Develop and complete an Integrated Workforce Plan.
Develop an integrated clinical and professional engagement programme to support integration.
Establish an Integrated Care Collaborative for the planning and coordination of Unscheduled Care Pathways, development of a Strategic Hospital Plan and agree the direction of set aside resources.
Agree with partners a Delayed Discharge Improvement Plan for Tayside and for each partnership area, including deployment of national delayed discharge funding to deliver the 14 day target and to move towards 72 hour discharge from an acute hospital setting.
Scale up the Enhanced Community Support Model within one locality area and seek to progressively roll out across Tayside.

37
Spread the delivery of a community based dementia model of care to additional localities and scale up to locality.
Implement new models of care to replace facilities-based care with integrated community team working.
Develop sub-acute care within retained community hospitals and commence development of a new sub-acute centre for Dundee.
KEY DELIVERABLES BEYOND 2015/2016
In future years we will support the Integrated Joint Boards to: Enhance the Joint Strategic Commissioning Plans and develop Locality Plans.
Implement the Integrated Workforce Plan to create integrated locality teams across all areas.
Fully roll out the Enhanced Community Support Model.
Deliver improvement across the national outcomes and indicators.
Continue the implementation of the Delayed Discharge Improvement Plans.
Complete the integration of Occupational Therapies.


38
In the context of delivery of the highest quality of safe, effective and person-centred care, our workforce is the critical enabler. It is the commitment and skill of workforce that provides our services, builds our capacity, maintains our efficiency, and delivers our quality agenda. That is why in 2014 our Board published its 'People Matter' Strategy, which set out its commitment to the delivery of the "Everyone Matters - 2020 Workforce Vision", and the actions it would progress in 2014/15 to do so. Against the key areas required under CEL 20 (2014) to deliver "Everyone Matters", in 2015-16 the following priorities will therefore be actioned in NHS Tayside: HEALTHY ORGANISATIONAL CULTURE 2015/16 Commitment: We will promote and recognise the behaviours of individuals and teams at all levels which reflect our values. Values and Behaviours - Since the Board launch of the NHS Tayside core value set in December 2013, which mirror the NHS Scotland value set, staff across NHS Tayside have been part of line-led discussions on these values, their meaning, and individual responsibilities. This has been supported by information packs and toolkits distributed to all line managers to support this exercise. Implementation is subject to regular audit, with reporting to the Board's Staff Governance Committee. The most recent audit report (February 2015) demonstrates that 74% of staff who completed the audit felt that their team were aware of the NHS Tayside values. This correlates with the results of the 2014 National Staff Survey, in which 76% of staff reported that they were aware of the NHS Tayside values. Importantly, recognition by staff of our prioritisation of the care of patients and those who use our services increased to 70%. In 2015/16, work building on that platform will be implemented, including the use of values and behaviours across staff appraisals and objectives; further development sessions on values and behaviours; a reintroduction of visible leadership walk-rounds to reinforce the Board's vision and core values; and line manager feedback to individuals on behaviours that are not consistent with the values. Staff Experience - National Staff Survey and iMatter - The 2014 National Staff Survey results, published in December 2014, saw NHS Tayside achieve the highest percentage increase in overall response rates, and the Board aims to maintain this momentum across 2015/16. Having been a pilot Board for the staff experience programme, NHS Tayside has been an early implementer of the national iMatter programme, with a comprehensive 3 year roll out plan agreed by the Board. For 2015/16, oversight of implementation of the iMatter toolkit has been delegated to our Local Directorate Partnership Foras, with formal quarterly progress reporting to the Board's Staff Governance Committee. Engaging and Involving Staff - The 2014 National Staff Survey saw 84% of NHS Tayside staff stating they are clear on their duties and responsibilities, with some 76% confirming they understand how their work fits into the overall aims of NHS Tayside, and perceptions of NHS Tayside as a positive place to work continued to grow, with 61% of recommending us as an employer of choice. Against this positive backcloth, NHS Tayside has embarked on a redesign of our partnership arrangements to ensure staff involvement in all decision making, and that staff remain active participants in our agenda. To strengthen the Area Partnership Forum's (APF) strategic role, recent changes to our APF work plan ensure all clinical and financial strategic matters are considered at this table alongside the
39
existing Staff Governance issues, and Management attendees of the APF revised to include all Board Directors. The priority for 2015/16 is the embedding of a revised Local Partnership Fora structure. This structure, developed with and agreed by Staff Partners, ensures the consideration by key decision makers and staff partners across all local services of their clinical strategy, financial plans, and co-production of workforce plans. Progress reviews of this work programme are regularly reported to the APF, and will continue throughout the year. SUSTAINABLE WORKFORCE 2015/16 Commitment: We will use high quality workforce data and contextual information to inform local workforce plans 2015/16 Commitment: We will ensure that recommendations from the Working Longer Review around occupational health, safety and wellbeing are fully implemented and that flexible approaches are taken. Strengthening Workforce Planning - Against a Scottish Government priority of boosting the economy and job creation, NHS Tayside has taken a tactical position of maintaining and growing our workforce. Across the last two financial years to date (March 2012 to January 2015) we have grown staffing numbers by 400 WTE. Vacancy Areas - The skills challenge that faces the wider health community also impacts in Tayside across medical, nursing and some other specialist staff, with vacancy management issues arising across a range of disciplines including:
Medical: Anaesthetics, Addiction Psychiatry, Clinical Oncology, Dermatology, Emergency Medicine, ENT, General Adult Psychiatry, Immunology, Medicine for the Elderly, Neurosurgery, Paediatrics, Neurophysiology, Neonatology, Child & Adolescent Psychiatry, Old Age Psychiatry, Oral Max Surgery, Orthodontics, Obstetrics & Gynaecology, Ophthalmology, Histo and Cyto Pathology, Palliative Medicine, Radiology, and Trauma & Orthopaedics. Nursing: Particularly Community Nursing, Health Visiting, Public Health, Theatres. Other Staff groups:- Physiotherapy, Radiology, eHealth, and Healthcare Science.
With the Scottish economy requiring further inward migration to help address some of these challenges, opportunity to engage alongside colleagues in Scottish Government around UK migration policy needs therefore to be viewed by as a critical tactical enabler. Despite these challenges, NHS Tayside continues to be successful in positioning itself as an employer of choice, securing, for example, recruitment of an additional 32 medical and dental staff over the last 12 months. Nursing Workload Tools - As an early adopter Board, we have already begun the comprehensive roll out of the national Nursing Workload Tools, which are informing an ongoing recruitment programme for nursing staff across all specialties. In line with emerging requirements, in November 2014 alone, we recruited 180 new graduate nurses from universities throughout Scotland. Modern Apprenticeships - At the same time, and in support of Scottish Government commitment to tackling inequalities and youth employment, we have invested heavily in the development of skills across the Tayside population. Alongside our established Health and Social Care Academy model, supporting individuals from across our community to be work-ready, we
40
have moved to significantly expand our Modern Apprenticeship Programme, which will see an additional recurring 25 places (34 in total) across a range of specialities. Board Workforce Plan - The scale of workforce growth described above brings with it challenges however, and 2015/16 sees a commitment around reshaping our workforce. Led by our Clinical Services Strategy, this will see us taking a robust position on some staff working in different roles, delivering services in different ways, and in different places. This in turn offers opportunities for staff retraining and career development. This agenda will be reflected in our Workforce Plan to be submitted to Scottish Government in June 2015, built in partnership, and which will support our Clinical and Financial Strategies, securing the principle of the right people in the right place to ensure the safety and quality of care. Workforce Optimisation - Enabling effective staff deployment is a key 2015/16 Board strategic priority. Alongside challenges of reducing protection costs, the Board has prioritised the use of eRostering to ensure the best use of staff and skills across shifts. Following successful piloting, procurement of a full eRostering system was completed in 2014, and NHS Tayside is now leading NHS Scotland in the implementation of eRostering. Initially focussing on nursing rosters across 2015/16, this tool will be rolled out throughout the period 2015-17 across Junior Medical, AHP, and some other non-clinical services. The use of eRostering tools compliments existing work implementing other systems which support data-driven management. This targeting of effective staff deployment to meet clinical need underpins the Board's target of significant reduction of supplementary staff expenditure throughout 2015/16. CAPABLE WORKFORCE 2015/16 Commitment: We will ensure that everyone has a meaningful conversation about their performance, their development and career aspirations 2015/16 Commitment: We will develop the skills and behaviours required for working collaboratively and flexibly across primary and secondary care, and across health and social care. Appraisal - In the context of NHS Tayside's work on values and behaviours, incorporation of behaviour as the primary focus of appraisal has already been agreed with the Board's Remuneration Committee for use within the Executive / Senior Manager cohort as a pilot group in 2015. This is based around the piloting of the nationally-recognised "VOICES" reflective tool developed by Cohort 8 of 'Delivering for the Future' national Strategic Clinical Leadership Development Programme 2014, to capture the contribution of leadership behaviours within the behavioural element of each objective. In support of our appraisal programme, in-house development will continue to be delivered by the Learning & Development and Organisational Development Teams to ensure both the ongoing development of appraisal skills, and, following piloting and evaluation, supporting the embedding of behavioural factors in appraisal for all staff groups. eKSF - Alongside this, while continuing to promote the effective use of eKSF for all Agenda for Change staff, work is being led by the Employee Director, Director of HR and Nurse and Midwife Director throughout 2015 supporting the senior Operations management team in improving their use of appraisal and promoting access to development for Support Services staff. This focus in ensuring effective appraisal is a key enabler to ensuring all staff have equitable access to personal development opportunities, as monitored by our Area Partnership Forum and Staff Governance Committee.
41
INTEGRATED WORKFORCE 2015/16 Commitment: We will work with partners toward the Health and Wellbeing Outcomes [4] developing a shared culture, values and ways of working through effective teams and local partnerships 2015/16 Commitment: We will provide leadership to continue to support the integration of primary and secondary care, recognising the role of GPs, dentists, pharmacists and others as part of the workforce. Supporting Integration - The system-wide impact of the Health and Social Care Integration (HSCI) agenda will continue to be a primary focus at all levels of the organisation. A Chief Officer has already been appointed for the Angus partnership, while both Dundee and Perth & Kinross partnerships begin to move toward similar early appointments. NHS Tayside established an NHS HSCI Partnership Board in 2014/15 to help support delivery of a positive staff experience moving in to the new integrated arrangements and this will continue to be met across 2015/16. A network of functional joint forums have also been established, including Human Resources and Finance, to promote early joint planning, across the range of Council geographies. Meetings will continue throughout 2015/16 with the new HSCI Chief Officers and staff partners from all partner organisations to ensure a focus on effective staff working and maximising the positive impact of integration through shared understanding and shared values. Supporting Primary and Secondary Care - NHS Tayside recognises that Primary Care and Community Services provide both the first and ongoing point of contact between an individual and healthcare professionals in the majority of cases, and therefore the importance of Primary and Community Services care as the gateway to secondary care. The appointment by NHS Tayside in early 2015 of a Director of Community Services and Primary Care, working alongside a Director of Acute Services, will help ensure our services work more closely together, and with GPs, Dentists and other partners to develop a sustainable workforce model. In the context of HSCI, 2015/16 will see the emergence of early sharing and integration of workforce information, and through that, development of more effective integrated workforce plans which better reflect the needs of our local population. EFFECTIVE LEADERSHIP AND MANAGEMENT 2015/16 Commitment: We will build leadership skills to lead/drive Quality Improvement 2015/16 Commitment: We will ensure leaders at all levels and in all professions have the skills to support the workforce through change. Building Capability - 2014/15 saw Learning and Development and Organisational Development expert teams refresh NHS Tayside's Leadership Strategy and introduce initiatives which support the skills, behaviours and capabilities required by those we see leading delivery of our clinical, financial and people strategies in the coming years. This work will continue across 2015/16, including extending expert development programmes on improvement techniques to underpin our values around quality of care. This includes in 2015/16, delivery of a comprehensive suite of development interventions that focus on people management and change management skills. This will ensure leaders at all levels are enabled to demonstrate the values and behaviours promoted by NHS Tayside and NHS Scotland, while supporting service changes that may emerge from local and national clinical strategies. At the same time, this work will begin to build the platform for the enhanced line management requirements around performance, policy, engagement, and equality likely to arise from the move to a national HR shared services model.
42
LDP SICKNESS ABSENCE STANDARD NHS Tayside has made significant strides in relation to reducing sickness absence. Our performance at December (most recent available) across the rolling year, offers a local NHS Tayside average of 4.83% against a national position of 4.97%. While we have consistently remained below the Scottish average across 2014/15, and achieved one of the largest sustained reduction in overall rates, we clearly still have more to do to achieve the 4% standard. That is why we have adopted a focus around staff well being, and ensuring effective staff support; this includes the recent high profile Board launch of the "Live Positive" training and support materials, designed in partnership to help staff cope with stress and anxiety, and build awareness and self reliance, and progress in this area will remain the central tenant of our approach across 2015/16.

43
NHS Tayside is a key member of the ANGUS Community Planning Partnership (CPP) which works towards improving the area's economy, improving community learning, making Angus a healthier and safer community in which to live, and protecting and enhancing the quality of the Angus environment. NHS Tayside is represented by the Chairman of NHS Tayside and the Director of Primary & Community Services on the CPP Board. Additionally the CHP Interim Lead Officer, Director of Public Health, and other local officers are members of the full Partnership. The CHP has been fully engaged in its strategic development and actively supports and promotes the set of core values of CPP planning for place: through actively engaging with its communities, promoting sustainable growth, promoting fairness and equality, and providing excellent public services that are value for money. Work is currently taking place to reinvigorate the Partnership and plans are well advanced to replace the current system of Thematic Partnerships reporting into the Community Planning Partnership. The CPP has the responsibility for overseeing the delivery of the Single Outcome Agreement. The full Community Planning Partnership meets four times per year and agenda items for future discussions during 2015/16 will include: Locality Approach & Community Empowerment; Sustainable Economy & Employment; Poverty & Disadvantage; and Shifting the Balance of Care. These cross cutting issues will also inform the new Single Outcome Agreement from 2016 onwards. A formal full year and mid year report are provided to the Partnership which highlights progress in the performance of the Angus Community Plan and Single Outcome Agreement 2013/16. The new strategic emphasis will see planning for place at a locality level on a holistic basis. In order to take this forward an event will be held in each of the four localities during 2015 for communities to determine their 3-5 priorities. It is envisaged these will be held thereafter on an annual basis. All partners will contribute to the leadership and commit to actions determined within the localities. The importance of the third sector to the work of the Partnership and the locality approach has been underlined by the development of a Third Sector Compact which has set out the broad principles which will govern the relationship between the Angus Community Planning Partnership and the local third sector in future years. NHS Tayside is a key member of the DUNDEE Community Planning Partnership, and is represented on the Partnership Management Group and Co-ordinating Group. NHS Tayside leads Healthy Dundee (the Health and Care Partnership) and is a fully engaged partner in the ongoing implementation of the Single Outcome Agreement for 2013-2017 and the associated Delivery Plan, with its emphasis on reducing inequalities, and on implementing prevention and early intervention approaches. Healthy Dundee has been responsible for overseeing the implementation of the Dundee Action Plan for the Health Equity Strategy and driving forward the top priority Physical and Mental Wellbeing outcomes and deliverables first agreed in the 2012 SOA i.e.
Reducing harm from substance misuse Introducing city-wide social prescribing, and Rolling out Equally Well approach to mental wellbeing.

44
A Health Inequalities Sub Group of Healthy Dundee has been established and is working across the Partnership to ensure that our core health inequalities work is targeted at the most deprived communities in Dundee in an efficient and effective evidence based way. Health Inequalities has been included within the Dundee bid for Integrated Care Funding for 2015/16 and we aim to use this resource to:
i. Review and consolidate existing health inequalities work by merging existing health inequalities programmes to provide multi disciplinary locality teams.
ii. Build the capacity of public and voluntary organisations to adopt health inequalities sensitive practice.
In Dundee, we have had a particular focus on employability and mitigating the impact of welfare reform. NHS Tayside is represented on the Dundee Partnership Employability Group and Dundee CHP hosts the newly established NHS Tayside Employability and Welfare Reform Forum on behalf of the Director of Public Health. This Forum has overseen the development and implementation of NHS Tayside’s Outcomes Focussed Plan and has included a number of key pieces of work such as the development of a Welfare Reform “App”, the development of an online repository of information for NHS Staff and the development of an on-line training resource. NHS Tayside is a key member of the PERTH & KINROSS Community Planning Partnership. It is an active contributor on the Community Planning Partnership Board, Community Planning Partnership Executive Officer Group (CPPEOG), the four Outcome Delivery Groups and Community Empowerment Working Group Following the agreement of the Single Outcome Agreement in June 2014, four Outcome Delivery Groups were established from existing thematic groups:
1. Health and Social Care integration Pathfinder Board 2. Children and Young People 3. Community Safety and Environment 4. Economy and Lifelong Learning
These Groups lead and are responsible for actions which support the delivery of the Community Plan and Single Outcome Agreement across Perth and Kinross. They plan, oversee and are accountable for delivery by Community Planning Partners of key actions which support the relevant Community Plan objectives. The Health and Social Care Integration Pathfinder Board is the Outcome Delivery Group committed to providing the support structures that allow people to lead health, independent and active lives. Linked to these aims are tackling inequalities and prevention. The Vice Chair of this Group is a Tayside NHS Non Executive Board member. During 2015, its chief focus is on ensuring the effective implementation of the Public Bodies (Joint Working) (Scotland) Act and the creation of the Integration Joint Board for Perth & Kinross, and as a result embedding new locality based ways of working. NHS Tayside representatives are active in the Community Empowerment Working Group, which the Non Executive Board member chairs. This group advises the Community Planning Partnership on involving and engaging with communities, aims to share best practice as to "what works" in community development, as well as advising on the effective use of community research and intelligence. During 2015, the Group will take forward its recommendations relating to community empowerment and participation into a comprehensive plan for action.
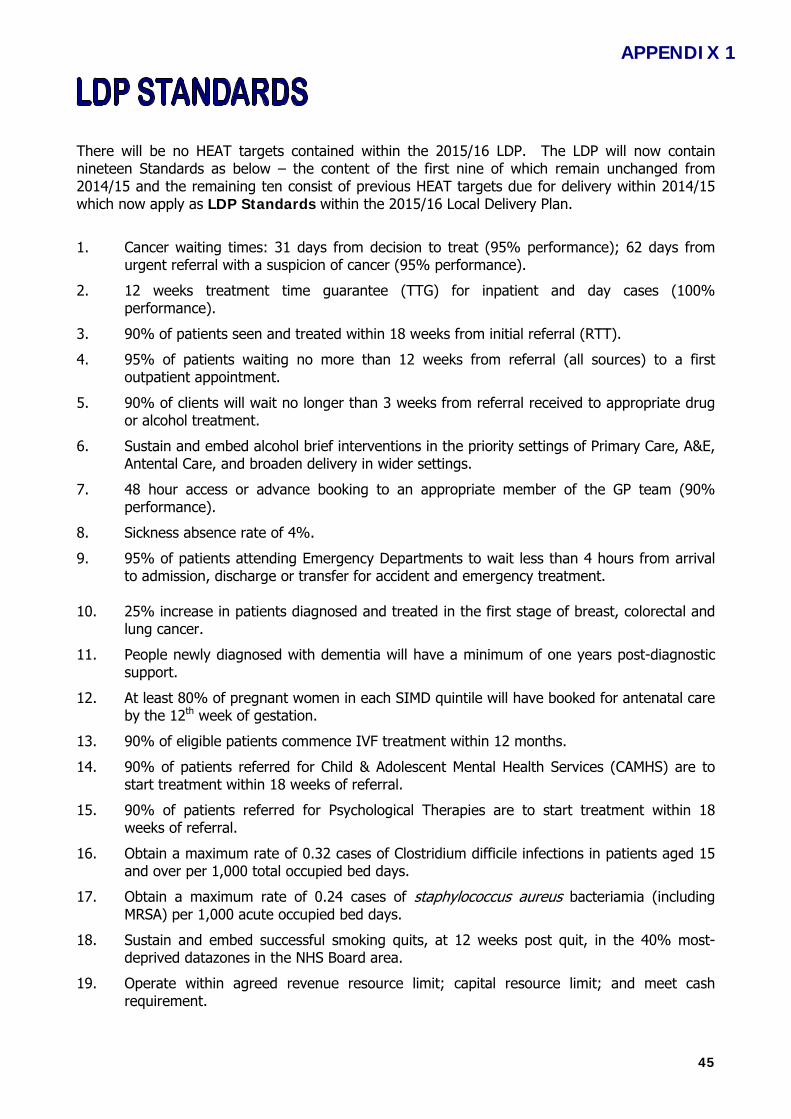
45
There will be no HEAT targets contained within the 2015/16 LDP. The LDP will now contain nineteen Standards as below – the content of the first nine of which remain unchanged from 2014/15 and the remaining ten consist of previous HEAT targets due for delivery within 2014/15 which now apply as LDP Standards within the 2015/16 Local Delivery Plan.
1. Cancer waiting times: 31 days from decision to treat (95% performance); 62 days from urgent referral with a suspicion of cancer (95% performance).
2. 12 weeks treatment time guarantee (TTG) for inpatient and day cases (100% performance).
3. 90% of patients seen and treated within 18 weeks from initial referral (RTT).
4. 95% of patients waiting no more than 12 weeks from referral (all sources) to a first outpatient appointment.
5. 90% of clients will wait no longer than 3 weeks from referral received to appropriate drug or alcohol treatment.
6. Sustain and embed alcohol brief interventions in the priority settings of Primary Care, A&E, Antental Care, and broaden delivery in wider settings.
7. 48 hour access or advance booking to an appropriate member of the GP team (90% performance).
8. Sickness absence rate of 4%.
9. 95% of patients attending Emergency Departments to wait less than 4 hours from arrival to admission, discharge or transfer for accident and emergency treatment.
10. 25% increase in patients diagnosed and treated in the first stage of breast, colorectal and
lung cancer.
11. People newly diagnosed with dementia will have a minimum of one years post-diagnostic support.
12. At least 80% of pregnant women in each SIMD quintile will have booked for antenatal care by the 12th week of gestation.
13. 90% of eligible patients commence IVF treatment within 12 months.
14. 90% of patients referred for Child & Adolescent Mental Health Services (CAMHS) are to start treatment within 18 weeks of referral.
15. 90% of patients referred for Psychological Therapies are to start treatment within 18 weeks of referral.
16. Obtain a maximum rate of 0.32 cases of Clostridium difficile infections in patients aged 15 and over per 1,000 total occupied bed days.
17. Obtain a maximum rate of 0.24 cases of staphylococcus aureus bacteriamia (including MRSA) per 1,000 acute occupied bed days.
18. Sustain and embed successful smoking quits, at 12 weeks post quit, in the 40% most-deprived datazones in the NHS Board area.
19. Operate within agreed revenue resource limit; capital resource limit; and meet cash requirement.
APPENDIX 1

46
The nineteen standards will be formally performance and risk managed through monthly update at the NHS Tayside Senior Leadership Team, and quarterly reporting to NHS Tayside Board on progress with the Local Delivery Plan standards. If necessary, the Board will also receive exception reports. The performance report provides a validated data position against each standard, with supplementary information where standards have or are at risk of not meeting expected performance, detailing issues affecting performance and the actions being taken to address these. Board Meetings are held in public and reports are available via NHS Tayside Internet. The Local Delivery Plan Corporate Risk is also presented to the Board on an annual basis and the Strategic Risk Management Group on a quarterly basis. Executive Leads responsible for overseeing the delivery of each LDP standard are responsible for making sure that the appropriate mechanisms are in place to review and manage performance, and to implement the necessary actions through the respective service improvement/action plans.
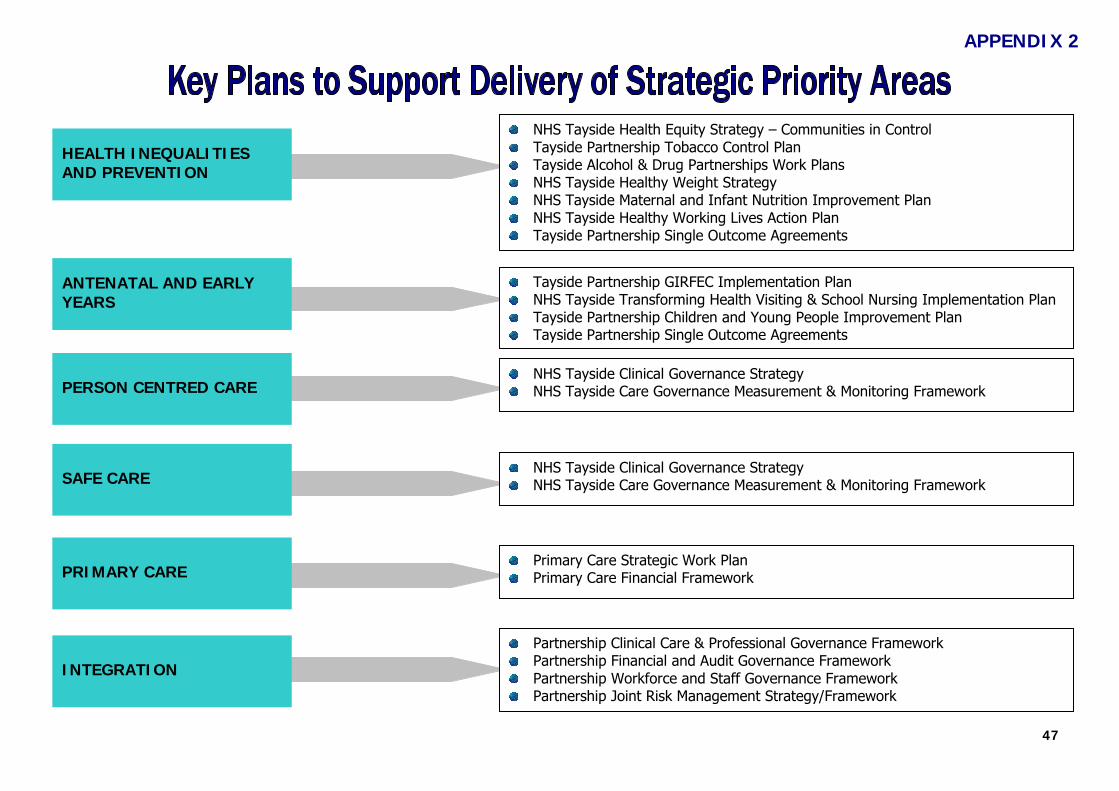
47
HEALTH INEQUALITIES AND PREVENTION
ANTENATAL AND EARLY YEARS
PERSON CENTRED CARE
SAFE CARE
PRIMARY CARE
INTEGRATION
NHS Tayside Health Equity Strategy – Communities in Control Tayside Partnership Tobacco Control Plan Tayside Alcohol & Drug Partnerships Work Plans NHS Tayside Healthy Weight Strategy NHS Tayside Maternal and Infant Nutrition Improvement Plan NHS Tayside Healthy Working Lives Action Plan Tayside Partnership Single Outcome Agreements
Tayside Partnership GIRFEC Implementation Plan NHS Tayside Transforming Health Visiting & School Nursing Implementation Plan Tayside Partnership Children and Young People Improvement Plan Tayside Partnership Single Outcome Agreements
NHS Tayside Clinical Governance Strategy NHS Tayside Care Governance Measurement & Monitoring Framework
NHS Tayside Clinical Governance Strategy NHS Tayside Care Governance Measurement & Monitoring Framework
Primary Care Strategic Work Plan Primary Care Financial Framework
Partnership Clinical Care & Professional Governance Framework Partnership Financial and Audit Governance Framework Partnership Workforce and Staff Governance Framework Partnership Joint Risk Management Strategy/Framework
APPENDIX 2
Please note any items relating to Committee business are embargoed and should not be made public until after the meeting
Item Number 6.2
Report Number 37/2015 Perth & Kinross CHP Committee
11 August 2015
PERTH & KINROSS INTEGRATED CARE FUND
1. PURPOSE OF THE REPORT
The purpose of the report is to seek support from Perth & Kinross CHP Committee in the
development and implementation of the Integrated Care Fund Agenda.
2. RECOMMENDATIONS
Perth & Kinross CHP Committee are asked to support: • The aims and objectives of the Integrated Care Fund • The management and assurance arrangements • The direction and scope of the programme.
3. EXECUTIVE SUMMARY
In spring 2014 the Scottish Government announced the availability of an additional £100m for
health and social care partnerships in 2015-16 to help deliver improved outcomes from health and social care integration, shift towards prevention and continue to tackle inequalities. The Perth and Kinross Partnership’s share of this fund is £2.63m. Perth & Kinross Partnership have approved 37 projects, the majority from the Third Sector (attached appendix 1).
4. REPORT DETAIL
In April 2015, Health & Social Care Partnerships across Scotland were allocated additional resources to support the delivery of improved outcomes from health and social integration, help drive shift towards prevention and further strengthen approaches to tackling inequalities. Perth & Kinross’s allocation is £2.6 m. The funding allocated is to support partnerships to focus on prevention, early intervention and care and support for people with complex and multiple conditions, particularly in those areas where multi morbidity is common in adults under 65, as well as in older people. The Integrated Care Fund is to be used to test and drive a wider set of innovative and preventative approaches in order to reduce future demand, support adults with multi morbidity and address issues around the inverse care law, where people who most need care are least likely to receive it.
1 This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held
Please note any items relating to Committee business are embargoed and should not be made public until after the meeting
Central to these approaches must be the shift to support the assets of individuals and communities so that they have greater control over their own lives and capacity for self management, particularly of multiple conditions. Therefore the Third Sector has a particularly crucial role to play in supporting such an approach. There are 6 principles that should underpin the use of the fund: Co Production - the use of the Fund must be developed in partnership, primarily between health, social care, housing, third sector, independent sector, people who use support and services and unpaid carers. It should take an inclusive and collaborative local approach that seeks out and fully supports the participation of the full range of stakeholders, particularly the third sector, in the assessment of priorities and delivery of innovative ways to deliver better outcomes Sustainability – the Fund needs to lead to change that can be evidenced as making a difference that is sustainable and can be embedded through mainstream integrated funding sources in the future. Locality – the locality aspects must include input from professionals, staff, users and carers and the public. Partnerships should develop plans with the people who best know the needs and wishes of the local population. Such a bottom-up approach should maximise the contribution of local assets including the third sector, volunteers and existing community networks. Partners will be expected to weight the use of their funding to areas of greatest need. Leverage – the funding represents around 1% of the total spend on adult health and social care so must be able to support, unlock and improve the use of the total resource envelope. Our approach to strategic commissioning will be key to this so it is important that plans for the use of this resource are embedded in the strategic commissioning process. Involvement – Partnerships should take a co-production, co-operative, participatory approach, ensuring the rights of people who use support and services and unpaid carers are central to the design and delivery of new ways of working – delivering support and services based on an equal and reciprocal person centred relationship between providers, users, families and communities. These relationships should be evidenced within each partnership’s plans. Outcomes – partnerships will be expected to link the use of the funds to the delivery of integrated health and wellbeing outcomes for adult health and social care which will be the responsibility of the new Integration Joint Boards or lead agencies following enactment of the legislation for integration. Perth & Kinross Health & Social Care Partnership submitted their Integrated Care Fund Plan to the Scottish Government January 2015 describing how the Partnership intends to drive service innovation, development and improvement and to communicate priorities. The Partners are expected to submit and publish locally, two progress reports at six monthly intervals to the Ministerial Strategic Group on Health and Community Care. In November 2014, all agencies were invited to submit proposals for funding using the 6 principles and national integrated health and wellbeing outcomes as criteria to score the proposals. The Integrated Care Fund Board tasked representatives from all agencies to review and approve the proposals based on the criteria. Thirty Seven projects have now been successful in receiving funding from the Integrated Care Fund.
2 This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held

Please note any items relating to Committee business are embargoed and should not be made public until after the meeting
An Assurance Structure and process has been implemented to provide confidence to the Board that all projects funded through the Integrated Care Fund meet the objectives and outcomes within the timescales agreed (1 year funding). Projects have been aligned to six workstreams. The workstreams have joint leads who are responsible for providing direction, support and monitoring of the projects. The workstreams developed and to be progressed as part of the bid are as follows:
• Workstream 1: Carers Strategy Group • Workstream 2: Co Morbidities / Mental Health • Workstream 3: Deprived communities • Workstream 4: H&SCI Consultation & Engagement • Workstream 5: Older People’s Development Group • Workstream 6: Enablers
5. CONTRIBUTION TO NHS TAYSIDE’S STRATEGIC AIMS
The Integrated Care Fund should be used to test and deliver a matrix of supports and interventions to improve health and wellbeing outcomes through, for example: deepening our focus on improving personal outcomes, supporting health literacy and adopting a co-production approach; using technology to enable greater choice and control; and adopting an assets-based societal model to improve population health and wellbeing. Plans should build on learning from Reshaping Care for Older People and extend the reach of successful approaches to the priority actions for partnerships set out in the National Action Plan for Multi-morbidity. It should include strands that will lead to reduced demand for emergency hospital activity and emergency admissions. Investment in existing institutional bed capacity such as long stay beds, should not form part of the plans for the use of the Integrated Care Fund. Plans should adopt and support delivery of the aim for 2020 that all adults with multiple conditions are supported to live well and experience seamless care from the right person when they need it and, where possible, where they want it
6. MEASURES FOR IMPROVEMENT
The activities support the delivery of integrated health and wellbeing outcomes and contribute
to wider work designed to tackle health inequalities.
• People are able to look after and improve their own health and wellbeing and live in good health for longer.
• People including those with disabilities, long term conditions, or who are frail, are able to live, as far as reasonably practicable, independently and at home or in a homely setting in their community.
• People who use health and social care services have positive experiences of those services, and have their dignity respected.
• Health and social care services contribute to reducing health inequalities. • People who provide unpaid care are supported to reduce the potential impact of their
caring role on their own health and well-being. • People who use health and social care services are safe from harm.
3 This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held

Please note any items relating to Committee business are embargoed and should not be made public until after the meeting
• People who work in health and social care services are supported to continuously improve the information, support, care and treatment they provide and feel engaged with the work they do.
• Resources are used effectively in the provision of health and social care services, without waste.
7. IMPACT ASSESSMENT & INFORMING, ENGAGING & CONSULTING
The official launch of the Integrated Care Fund Programme in Perth and Kinross took place on
Thursday 4 June 2015, the main criteria for the ICF event supported to:
• Provide an overview on the Integration of health and social care and development of the strategic plan
• Provide the opportunity for networking across the agencies • Provide an overview of the proposed themes, outcomes, reporting and evaluation
requirements • Identify the support requirements from projects to ensure successful management
delivery of the individual projects
8. PATIENT EXPERIENCE
It is envisaged that the patient experience will provide improved quality of life linking with co-morbidities and targeted towards deprived communities.
9. RESOURCE IMPLICATIONS
Perth and Kinross received £2.6m from the national share of £100m for 2015 / 2016. 37 projects were funded (Appendix A attached). Currently, projects are funded for a period of one year. All projects funded must evidence long term sustainability of the investment.
10. RISK ASSESSMENT
The ICF Board will develop a shared risk management strategy for the Programme that sets out key risks and an agreed risk monitoring framework. This strategy will ensure the ICF Board have a process in place to identify, assess and prioritise risks related to the delivery of the Programme and have a regular update on risks at each meeting to provide assurance.
11. LEGAL IMPLICATION
There are no known legal implications
12. INFORMATION TECHNOLOGY IMPLICATIONS
There are no known information technology implications.
13. HEALTH & SAFETY IMPLICATIONS
There are no health and safety implications.
4 This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held
Please note any items relating to Committee business are embargoed and should not be made public until after the meeting
14. HEALTHCARE ASSOCIATED INFECTION (HAI)
There are no Healthcare Associated Infections implications
15. DELEGATION LEVEL
Bill Nicoll, Director Community Services
16.
TIMETABLE FOR IMPLEMENTATION
17.
March 2016 REPORT SIGN OFF
Evelyn Devine, Perth & Kinross CHP
18. SUPPORTING DOCUMENTS
• Appendix 1 – Approved Integrated Care Fund Projects 2015
5 This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held
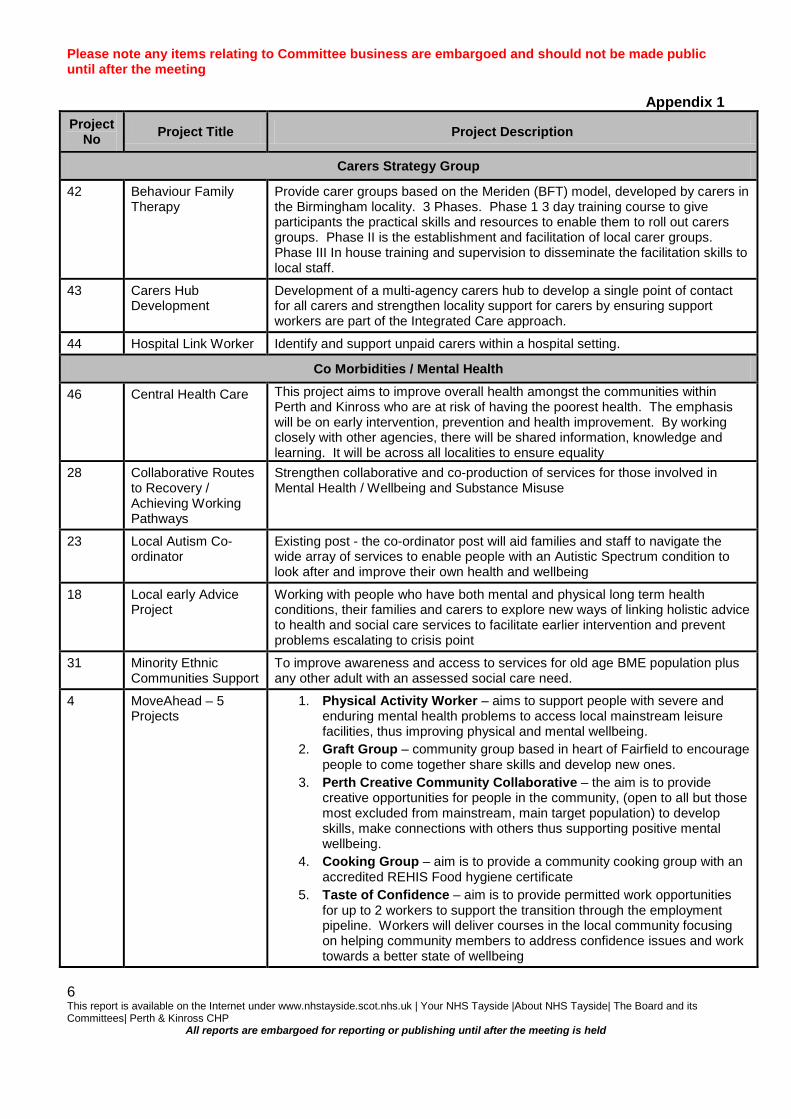
Please note any items relating to Committee business are embargoed and should not be made public until after the meeting
Appendix 1
Project No Project Title Project Description
Carers Strategy Group
42 Behaviour Family Therapy
Provide carer groups based on the Meriden (BFT) model, developed by carers in the Birmingham locality. 3 Phases. Phase 1 3 day training course to give participants the practical skills and resources to enable them to roll out carers groups. Phase II is the establishment and facilitation of local carer groups. Phase III In house training and supervision to disseminate the facilitation skills to local staff.
43 Carers Hub Development
Development of a multi-agency carers hub to develop a single point of contact for all carers and strengthen locality support for carers by ensuring support workers are part of the Integrated Care approach.
44 Hospital Link Worker Identify and support unpaid carers within a hospital setting.
Co Morbidities / Mental Health
46 Central Health Care This project aims to improve overall health amongst the communities within Perth and Kinross who are at risk of having the poorest health. The emphasis will be on early intervention, prevention and health improvement. By working closely with other agencies, there will be shared information, knowledge and learning. It will be across all localities to ensure equality
28 Collaborative Routes to Recovery / Achieving Working Pathways
Strengthen collaborative and co-production of services for those involved in Mental Health / Wellbeing and Substance Misuse
23 Local Autism Co-ordinator
Existing post - the co-ordinator post will aid families and staff to navigate the wide array of services to enable people with an Autistic Spectrum condition to look after and improve their own health and wellbeing
18 Local early Advice Project
Working with people who have both mental and physical long term health conditions, their families and carers to explore new ways of linking holistic advice to health and social care services to facilitate earlier intervention and prevent problems escalating to crisis point
31 Minority Ethnic Communities Support
To improve awareness and access to services for old age BME population plus any other adult with an assessed social care need.
4 MoveAhead – 5 Projects
1. Physical Activity Worker – aims to support people with severe and enduring mental health problems to access local mainstream leisure facilities, thus improving physical and mental wellbeing.
2. Graft Group – community group based in heart of Fairfield to encourage people to come together share skills and develop new ones.
3. Perth Creative Community Collaborative – the aim is to provide creative opportunities for people in the community, (open to all but those most excluded from mainstream, main target population) to develop skills, make connections with others thus supporting positive mental wellbeing.
4. Cooking Group – aim is to provide a community cooking group with an accredited REHIS Food hygiene certificate
5. Taste of Confidence – aim is to provide permitted work opportunities for up to 2 workers to support the transition through the employment pipeline. Workers will deliver courses in the local community focusing on helping community members to address confidence issues and work towards a better state of wellbeing
6 This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held
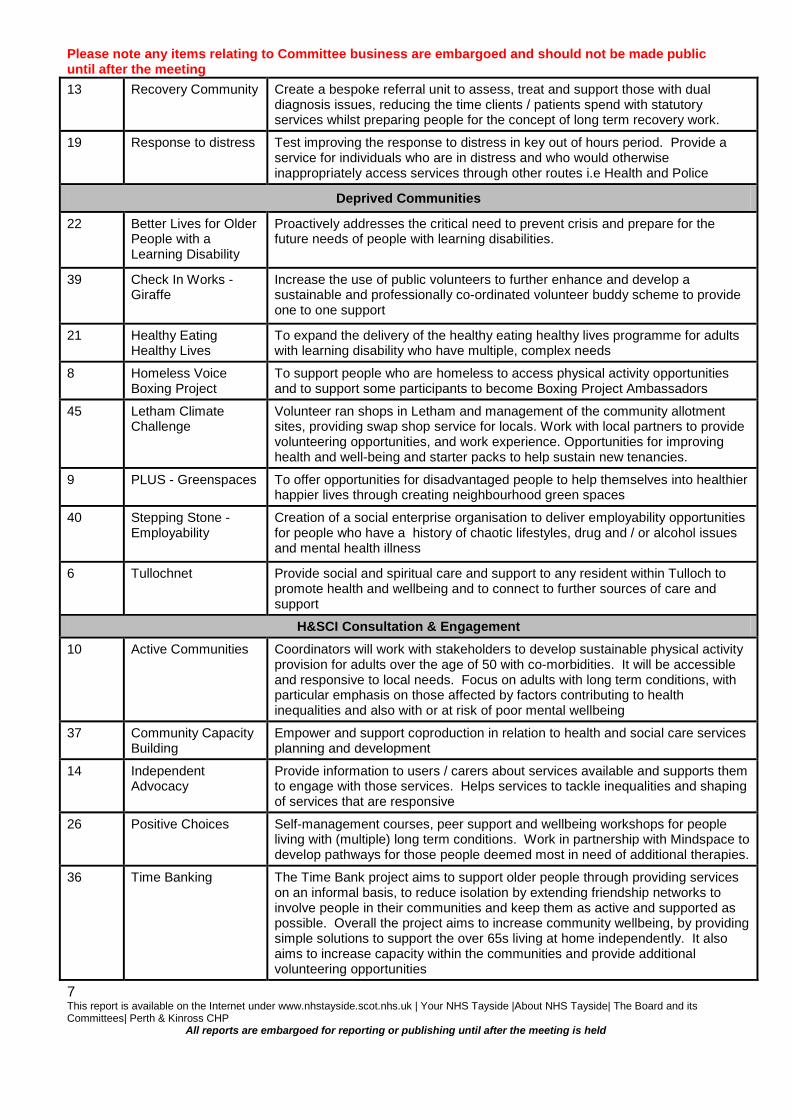
Please note any items relating to Committee business are embargoed and should not be made public until after the meeting 13 Recovery Community Create a bespoke referral unit to assess, treat and support those with dual
diagnosis issues, reducing the time clients / patients spend with statutory services whilst preparing people for the concept of long term recovery work.
19 Response to distress Test improving the response to distress in key out of hours period. Provide a service for individuals who are in distress and who would otherwise inappropriately access services through other routes i.e Health and Police
Deprived Communities
22 Better Lives for Older People with a Learning Disability
Proactively addresses the critical need to prevent crisis and prepare for the future needs of people with learning disabilities.
39 Check In Works - Giraffe
Increase the use of public volunteers to further enhance and develop a sustainable and professionally co-ordinated volunteer buddy scheme to provide one to one support
21 Healthy Eating Healthy Lives
To expand the delivery of the healthy eating healthy lives programme for adults with learning disability who have multiple, complex needs
8 Homeless Voice Boxing Project
To support people who are homeless to access physical activity opportunities and to support some participants to become Boxing Project Ambassadors
45 Letham Climate Challenge
Volunteer ran shops in Letham and management of the community allotment sites, providing swap shop service for locals. Work with local partners to provide volunteering opportunities, and work experience. Opportunities for improving health and well-being and starter packs to help sustain new tenancies.
9 PLUS - Greenspaces To offer opportunities for disadvantaged people to help themselves into healthier happier lives through creating neighbourhood green spaces
40 Stepping Stone - Employability
Creation of a social enterprise organisation to deliver employability opportunities for people who have a history of chaotic lifestyles, drug and / or alcohol issues and mental health illness
6 Tullochnet Provide social and spiritual care and support to any resident within Tulloch to promote health and wellbeing and to connect to further sources of care and support
H&SCI Consultation & Engagement 10 Active Communities Coordinators will work with stakeholders to develop sustainable physical activity
provision for adults over the age of 50 with co-morbidities. It will be accessible and responsive to local needs. Focus on adults with long term conditions, with particular emphasis on those affected by factors contributing to health inequalities and also with or at risk of poor mental wellbeing
37 Community Capacity Building
Empower and support coproduction in relation to health and social care services planning and development
14 Independent Advocacy
Provide information to users / carers about services available and supports them to engage with those services. Helps services to tackle inequalities and shaping of services that are responsive
26 Positive Choices Self-management courses, peer support and wellbeing workshops for people living with (multiple) long term conditions. Work in partnership with Mindspace to develop pathways for those people deemed most in need of additional therapies.
36 Time Banking The Time Bank project aims to support older people through providing services on an informal basis, to reduce isolation by extending friendship networks to involve people in their communities and keep them as active and supported as possible. Overall the project aims to increase community wellbeing, by providing simple solutions to support the over 65s living at home independently. It also aims to increase capacity within the communities and provide additional volunteering opportunities
7 This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held
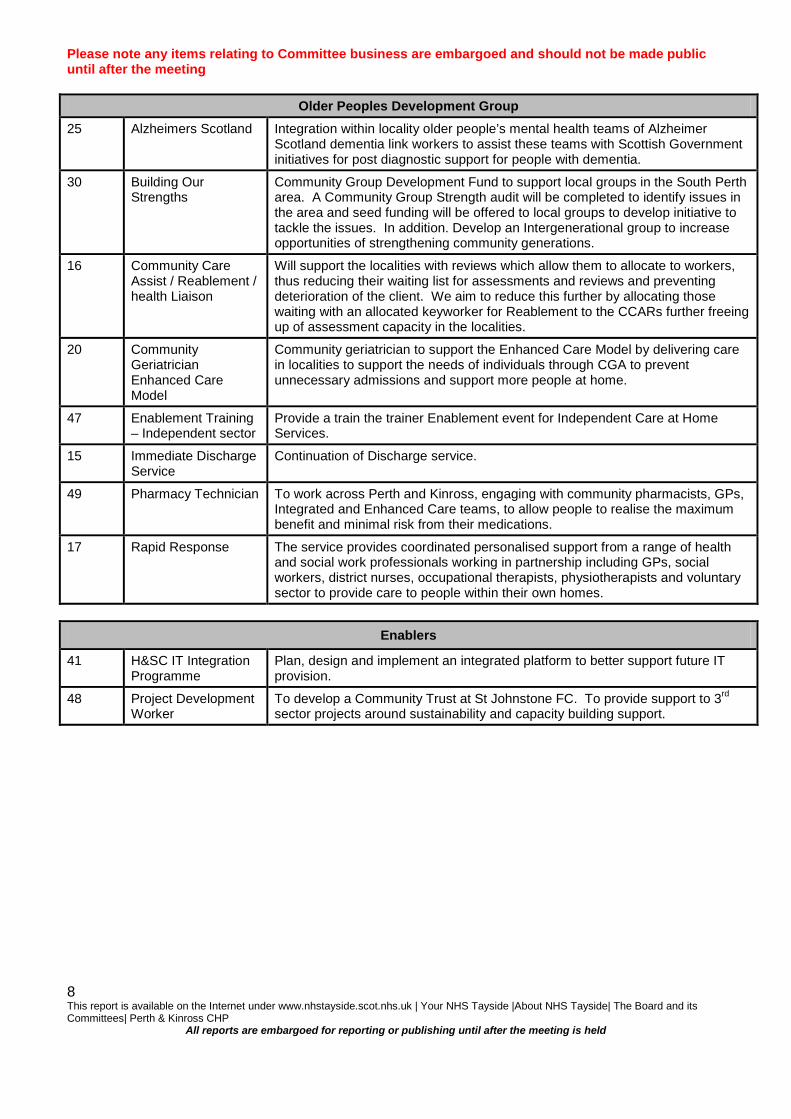
Please note any items relating to Committee business are embargoed and should not be made public until after the meeting
Older Peoples Development Group
25 Alzheimers Scotland Integration within locality older people’s mental health teams of Alzheimer Scotland dementia link workers to assist these teams with Scottish Government initiatives for post diagnostic support for people with dementia.
30 Building Our Strengths
Community Group Development Fund to support local groups in the South Perth area. A Community Group Strength audit will be completed to identify issues in the area and seed funding will be offered to local groups to develop initiative to tackle the issues. In addition. Develop an Intergenerational group to increase opportunities of strengthening community generations.
16 Community Care Assist / Reablement / health Liaison
Will support the localities with reviews which allow them to allocate to workers, thus reducing their waiting list for assessments and reviews and preventing deterioration of the client. We aim to reduce this further by allocating those waiting with an allocated keyworker for Reablement to the CCARs further freeing up of assessment capacity in the localities.
20 Community Geriatrician Enhanced Care Model
Community geriatrician to support the Enhanced Care Model by delivering care in localities to support the needs of individuals through CGA to prevent unnecessary admissions and support more people at home.
47 Enablement Training – Independent sector
Provide a train the trainer Enablement event for Independent Care at Home Services.
15 Immediate Discharge Service
Continuation of Discharge service.
49 Pharmacy Technician To work across Perth and Kinross, engaging with community pharmacists, GPs, Integrated and Enhanced Care teams, to allow people to realise the maximum benefit and minimal risk from their medications.
17 Rapid Response The service provides coordinated personalised support from a range of health and social work professionals working in partnership including GPs, social workers, district nurses, occupational therapists, physiotherapists and voluntary sector to provide care to people within their own homes.
Enablers
41 H&SC IT Integration Programme
Plan, design and implement an integrated platform to better support future IT provision.
48 Project Development Worker
To develop a Community Trust at St Johnstone FC. To provide support to 3rd sector projects around sustainability and capacity building support.
8 This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held

Please note any items relating to Committee business are embargoed and should not be made public until after the meeting
Item Number 7.1
Report Number 38/2015 Perth & Kinross CHP Committee
11 August 2015
PERTH & KINROSS CHP PERFORMANCE AND RISK REPORT 1. SITUATION AND BACKGROUND
Attached is the Performance and Risk Report for Perth and Kinross CHP. The Performance Report (Appendix 1) draws from latest available data which relate to the key performance topics.
The Risk Report (Appendix 2) provides a summary of the current “Operational” risks which are recorded on the DATIX system for P&K CHP.
2. ASSESSMENT
Detailed performance analysis is given for each section in the Report. Key points for noting are:
• Delayed Discharges
The run chart shows ongoing variability in bed days lost from January 2012 to June 2015. There has been a decrease in the number of bed days lost since the last report 2 months ago. This continues to be addressed through a range of activities.
• Supplementary Staffing
Expenditure on supplementary staffing continues to be monitored closely. There has been an increase in supplementary staffing costs compared to the previous year and this is partly due to the difficulty in accessing bank staff, and having to obtain agency staffing instead.
• Sickness rates
During June 2015 overall, sickness increased by 0.75% to 5.4%. Areas within the CHP experiencing the highest levels of sickness absence have been identified and further information on challenges and mitigating actions requested.
This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held 1

3. RECOMMENDATIONS Perth and Kinross CHP Committee is asked to note the report. Future reports will be submitted to the SMT and the Communities and Primary Care Directorate Performance Review forum (Item 7.5 refers).
4. REPORT SIGN OFF
Evelyn Devine, Interim Lead Officer, Perth and Kinross CHP.
Alison Wood Head of Corporate Services and Business Support Perth and Kinross CHP 3rd August 2015
This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held 2

Performance Report Perth and Kinross CHP Committee 11 August 2015 Appendix 1
TOPIC: Delayed Discharges Productivity and Efficiency Reshaping care
Clinical Governance Patient Safety
Key Performance chart Lost bed days to delayed discharge (days)
Notes Source: Qlikview, extracted 3rd August 2015 Patient CHP: Perth & Kinross, Non-Complex
Aim Perth & Kinross Council and Perth & Kinross CHP will work collaboratively with acute care services to reduce the number of bed days lost through delayed discharges relating to people over 65 years Key activities for improvement Discharge pathway training rolled out across all ward areas in P&K. A yearly review is undertaken across P&K ward areas and changes to the pathway made as necessary. Further resources will be assigned to enhanced care and physiotherapy/OT as part of the Scottish Government funding which has been allocated to improve delayed discharges, as well as to care at home options. Performance analysis The run chart shows ongoing variability bed days lost from January 2012 to June 2015.
Key performance status Note: Data contained in this report is for management purposes only and should not be considered to represent definitive levels of performance. Data may be invalidated, preliminary, incomplete or defined in a different way to published statistics. However, the data is considered to be sufficiently robust to provide reliable, if broad, indications of relative performance.
3
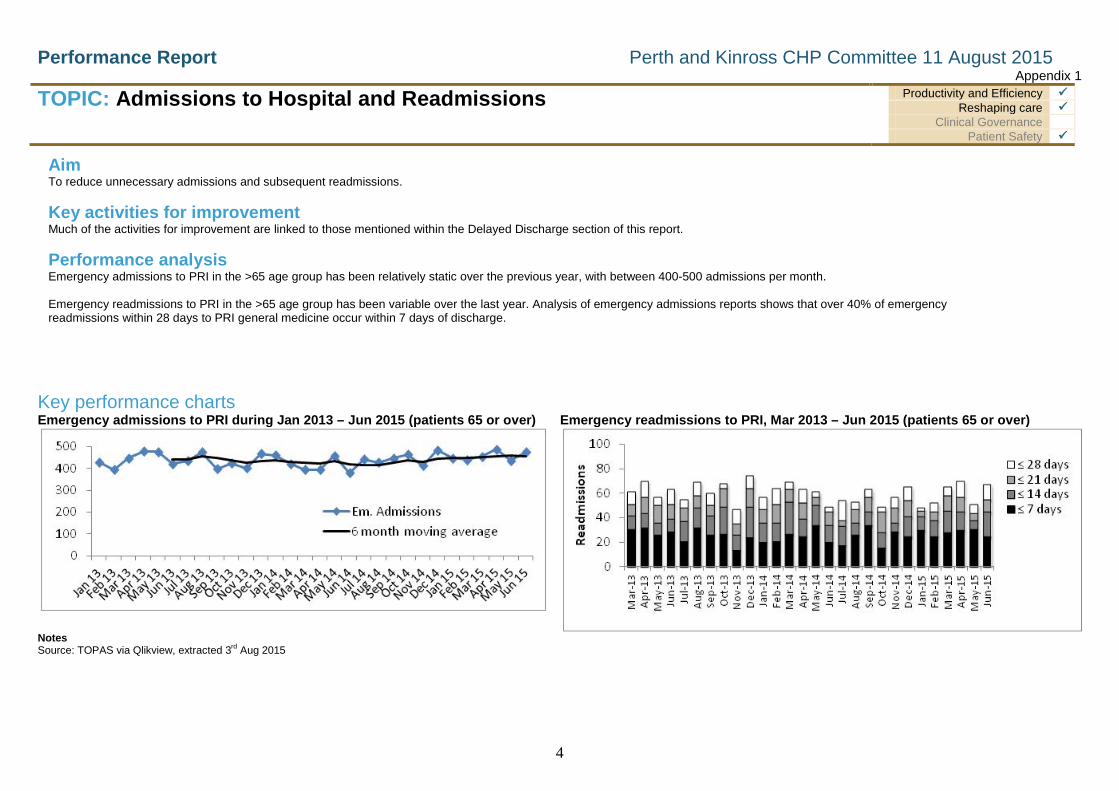
Performance Report Perth and Kinross CHP Committee 11 August 2015 Appendix 1
TOPIC: Admissions to Hospital and Readmissions
Productivity and Efficiency Reshaping care
Clinical Governance Patient Safety
Key Key performance charts Emergency admissions to PRI during Jan 2013 – Jun 2015 (patients 65 or over) Emergency readmissions to PRI, Mar 2013 – Jun 2015 (patients 65 or over)
Notes Source: TOPAS via Qlikview, extracted 3rd Aug 2015
Aim To reduce unnecessary admissions and subsequent readmissions. Key activities for improvement Much of the activities for improvement are linked to those mentioned within the Delayed Discharge section of this report. Performance analysis Emergency admissions to PRI in the >65 age group has been relatively static over the previous year, with between 400-500 admissions per month. Emergency readmissions to PRI in the >65 age group has been variable over the last year. Analysis of emergency admissions reports shows that over 40% of emergency readmissions within 28 days to PRI general medicine occur within 7 days of discharge.
4

Performance Report Perth and Kinross CHP Committee 11 August 2015
TOPIC: Clinical Quality Indicators Productivity and Efficiency Reshaping care
Clinical Governance Patient Safety
Aim That all hospital areas within Perth and Kinross CHP will achieve 95% compliance or over for
• Prevention of pressure ulcers • Falls prevention • Assessment and ongoing management of patient Food, Fluid and Nutrition
Performance analysis This information is now available via Qlikview, and shows the overall compliance percentage across all appropriate CHP areas. Over the last two months: • Overall performance with pressure ulcer care remains high, although data
for June 2015 shows a drop in overall compliance to 89%. • Overall performance with falls prevention remains at a high level, with an
overall compliance of 93% in May and 96% in June 2015. • Overall performance with nutritional care remains at a high level, with an
overall compliance of 99% in May and 96% in June 2015 • Work continues through the CHP Lead Nurse and Safety, Clinical
Governance & Risk Team to engage with clinical areas not meeting the compliance target, establish any challenges, and provide support where appropriate.
Notes Source:– GDET via Qlikview. The data represents P&K Community Hospitals, Garry, Tummel and Leven ward at MRH, Tay Ward and the Stroke Unit at PRI, and Cornhill Inpatient Unit.
Pressure Ulcer Prevention
Falls Prevention
Nutritional Care
5

Performance Report Perth and Kinross CHP Committee 11 August 2015
TOPIC: Supplementary Staffing Productivity and Efficiency Reshaping care
Clinical Governance Patient Safety
Aim To reduce the year on year spend on Bank, Overtime and Agency
Key performance status
Key activities for improvement • Review consistency of shift patterns to maximise flexibility of staffing resource • Review availability of bank staff, particularly in rural areas • Monitoring of all bank, agency and overtime requests
Apr ‘14- June ‘15 Apr ’15 – June ‘16
Increase/ (decrease)
Agency £86,977 £122,692 £35,715 Overtime £19,473 £37,967 £18,494 Bank £100,572 £132,783 £32,211 Extra Hours £119,366 £109,788 (£9578) Total £326,388 £403,230 £76,842
Activity update • Continued close monitoring of use of supplementary staffing to contain as far as
possible use of Agency and Bank • Due to the high level of demand across Tayside for bank nursing staff, PKCHP
has been required to pay for the more expensive option of agency staffing. • This information will be used in combination with sickness absence information to
explore areas for further improvement.
6

Performance Report Perth and Kinross CHP Committee 11 August 2015
TOPIC: Sickness Absence Productivity and Efficiency Reshaping care
Clinical Governance Patient Safety
Aim To reduce the levels of sickness absence to 4% or less
Key performance status
Key activities for improvement • Although the target for reducing sickness absence has been
achieved, the focus continues to encourage accurate and timely recording of sickness absence on SSTS to ensure quality absence data.
Activity update • HR team continue to meet with managers on regular basis to review
sickness absence and agree actions plans for long term absences cases.
• HR team supporting managers in better use of absence data to identify priority areas/cases
• Ongoing work with hotspot areas to assess training needs for staff in implementing the Promoting Attendance at Work Policy
• Where initial reasons for absence is “unknown” all managers have been asked to undertake retrospective checking of reasons for absence as soon possible.
Performance analysis • During June 2015 overall, sickness increased by 0.75% to 5.4%,
long term sickness increased by 0.35%, and short term sickness increased by 0.4% compared to the last month.
7

Performance Report Perth and Kinross CHP Committee 11 August 2015
TOPIC: Stroke Care Productivity and Efficiency Reshaping care
Clinical Governance Patient Safety
Aim Perth & Kinross CHP will work collaboratively with Acute Care Services to comply with the Quality Improvement Scotland Stroke Standards and the NHST Local Delivery Plan Stroke Care Bundle Target of 75% of patients achieving adherence to the bundle. Stroke care evidence suggests that improved patient outcomes are achieved for stroke patients who receive a specific ‘bundle’ of care. The ‘bundle’ consists of a patient:
• reaching the stroke unit by day 1 • receiving swallow screening by day 1 • receiving brain imaging within 24 hours of admission • receiving aspirin by day 1(unless contraindicated).
Nationally a decision has been made that the stroke bundle should be included as part of the Health Board’s Local Delivery Plan.
Key performance status
Key activities for improvement • Monthly multidisciplinary PRI Quality Improvement Group meetings with
representation from CHP and Acute Care Services. • Interrogation and exception reporting on all patients as they are admitted
to the stroke unit to establish anyone who has failed any standard to ensure reason/s established and followed up if required.
• Ongoing reminders/education of staff re standards. • Monthly reporting to staff of PRI’s status in regard to meeting standards. • Short life working group set up to look specifically at improving standard
related to accessing the stroke unit. Group has now reported findings.
Performance analysis • In P&K we track our performance in relation to the stroke bundle on an
ongoing basis. Improvement work in bundle performance continues with the aim of achieving reliability. Access to the stroke unit for all stroke patients, because of issues with capacity in PRI and delayed discharges, continues to prove to be a challenge. Further work is underway to assist with increasing capacity potential and lengths of stay.
0.0%
20.0%
40.0%
60.0%
80.0%
100.0%
Jun-14 Jul-14 Aug-14 Sep-14 Oct-14 Nov-14 Dec-14 Jan-15 Feb-15 Mar-15
Perc
enta
ge o
f pat
ient
s
Month
Percentage of initial stroke patients receiving appropriate bundle of care
Percentage of initial stroke patients receiving appropriate bundle of care Target (75%)
Note: Data contained in this report is for management purposes only and should not be considered to represent definitive levels of performance. Data may be invalidated, preliminary, and incomplete or defined in a different way to published statistics. However, the data is considered to be sufficiently robust to provide reliable, if broad, indications of relative performance
8
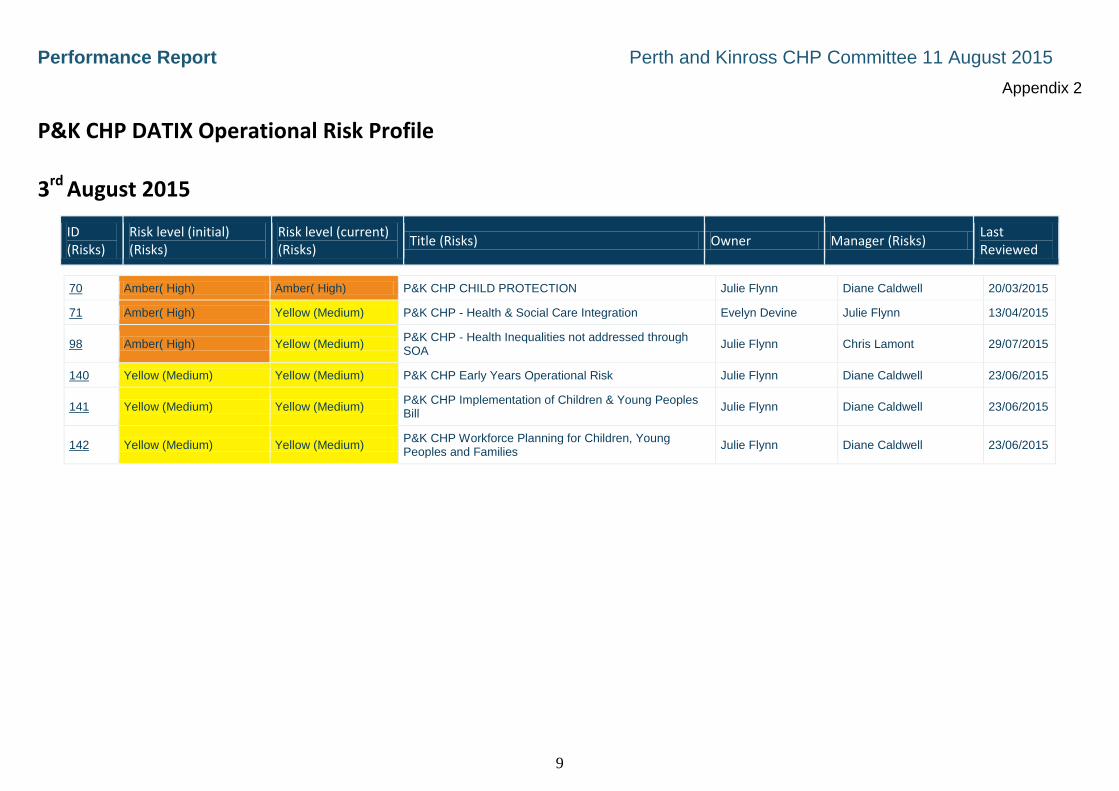
Performance Report Perth and Kinross CHP Committee 11 August 2015
Appendix 2
P&K CHP DATIX Operational Risk Profile 3rd August 2015
ID (Risks)
Risk level (initial) (Risks)
Risk level (current) (Risks)
Title (Risks) Owner Manager (Risks)
Last Reviewed
70 Amber( High) Amber( High) P&K CHP CHILD PROTECTION Julie Flynn Diane Caldwell 20/03/2015
71 Amber( High) Yellow (Medium) P&K CHP - Health & Social Care Integration Evelyn Devine Julie Flynn 13/04/2015
98 Amber( High) Yellow (Medium) P&K CHP - Health Inequalities not addressed through SOA
Julie Flynn Chris Lamont 29/07/2015
140 Yellow (Medium) Yellow (Medium) P&K CHP Early Years Operational Risk Julie Flynn Diane Caldwell 23/06/2015
141 Yellow (Medium) Yellow (Medium) P&K CHP Implementation of Children & Young Peoples Bill
Julie Flynn Diane Caldwell 23/06/2015
142 Yellow (Medium) Yellow (Medium) P&K CHP Workforce Planning for Children, Young Peoples and Families
Julie Flynn Diane Caldwell 23/06/2015
9
Please note any items relating to Committee business are embargoed and should not be made public until after the meeting
Item Number 7.2
Report Number 39/2015 Perth & Kinross CHP Committee
11 August 2015 ANNUAL REPORT OF PERTH & KINROSS SAFETY, CLINICAL GOVERNANCE & RISK GROUP 2014/15 1. PURPOSE
In order to assist the Community Health Partnership (CHP) in conducting a regular review of the activity and effectiveness of the Safety, Clinical Governance & Risk (SCGR) Group, the group submits an annual report to the P&K CHP Committee.
2. PERTH & KINROSS SAFETY, CLINICAL GOVERNANCE AND RISK GROUP
2.1 Composition During the financial year ended 31 March 2015, membership of the Perth & Kinross Safety, Clinical Governance and Risk Group comprised:
Dr Morag Martindale Clinical Director (Chairperson) Alison Wood Head of Corporate Services (Executive Lead) Angela Cunningham Primary Care Manager / Service Improvement Manager (from February 2015) Caroline Patterson Clinical Governance Manager Diane Caldwell Head of Children, Young People & Families (until June 2014) Evelyn Devine Head of Older Peoples Services Grace Gilling Interim Service Manager, Integrated Mental Health Services
Graeme Lamont Principal Pharmacist Jane Dernie Head of Allied Health Professions
Jim McGuinness Healthcare Manager, HMP Perth Prison (until February 2015) Julie Flynn Head of Children, Young People and Families Services (from
June 2014) Karen Buckley Infection Control Advisor Lindsey Miller Service Manager for Integrated Community Services Mark Dickson Safety, Clinical Governance & Risk Coordinator Sandra Gourla y Interim Lead Nurse
Attendance as Required
Arlene Napier Head of Clinical Governance & Risk Ian Jenkins Fire Safety Advisor
Rev Geoff Williams Head of Spiritual Care Val Fyall OHSAS Health & Safety Advisor
1 This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held

Please note any items relating to Committee business are embargoed and should not be made public until after the meeting
Support to the Group was provided by Yvonne Wimbury and Kerry Greig - Safety, Clinical Governance & Risk Support Officers.
2.2 Meetings
The Forum has met on six occasions during the period from 1 April 2014 to 31 March 2015 on the undernoted dates:
♦ 1st April 2014 ♦ 3rd June 2014 ♦ 5th August 2014 ♦ 14th October 2014 ♦ 2nd December 2014 ♦ 3rd February 2015
The attendance schedule is attached at Appendix 1.
2.3 Business
The group monitors and supports the delivery of Safety, Clinical Governance & Risk Management throughout all services within the CHP, as well as acting as a mechanism to share information and learning in all aspects of SCGR. This includes monitoring and sharing learning from adverse events and any findings from Local Incident Reviews or Significant Clinical Event Analysis (SCEAs). There is a focus on making improvements and monitoring performance to identify where attention is required or good practice can be shared. The Group also provides assurance to the P&K CHP Committee, P&K CHP Senior Management Team and the Tayside Clinical Quality Forum that effective and robust SCGR activity is ongoing within the CHP.
All meetings include reporting from services on Safety, Risk Management, Clinical Effectiveness, Person Centeredness and any learning. The group also shares learning and any actions required regarding complaints, adverse events, Local Incident Reviews and SCEAs.
Details of the business items considered are attached at Appendix 2. Minutes of the meetings of the P&K Safety, Clinical Governance and Risk Group are submitted to the P&K CHP Committee.
3. OUTCOMES
The group receives reports from all services within the CHP at each meeting, and these reports contain a summary of their ongoing SCGR activity. The format of the report includes sections on Safety, Clinical Governance, Risk and Learning, and the group scrutinises the activity that is reported, in order to be assured of robust systems for SCGR at service level.
2 This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held

Please note any items relating to Committee business are embargoed and should not be made public until after the meeting
The group also scrutinises key SCGR data at the group, and updates are provided on 20 key measures, which are discussed to establish any challenges or learning within services. The group have discussed the content of each Scottish Public Services Ombudsman report at the meetings, and any learning which is pertinent to CHP services. Ensuring learning from local adverse events or complaints continues to be strengthened at the group, and a process is in place which ensures learning is shared and all appropriate actions are completed in order to close the loop. The group receives a summary of activity with regards to SCEAs within P&K CHP, and SCEAs which require sign-off are discussed at the group to ensure that all outstanding actions are complete. Services feed back as part of their service report a summary of any SCEAs and the key learning to share with the group. The group is provided with a summary of any unannounced walkrounds which have taken place since the previous meeting, and there is an opportunity to discuss any areas where there was scope for improvement or particular good practice. Specific business which the group has supported during the year include: • Assurances sought that all areas are adhering to the Clinical Informed Consent
Policy. • The group was provided with an overview of the work carried out by the Spiritual
Care's community team across Tayside. • Completion of the Clinical Governance Self-assessment for P&K CHP, and
supporting services to complete the assessment individually. • Presentation and review of all P&K CHP DATIX incidents relating to medication for
the period January 2014 – March 2014. • Learning from the “Child U” Serious Case Review • Presentation on Interpretation and Translation and the responsibilities on services
and staff • Potential falls hazards identified within ward areas at MRH • The NHST Strategic direction for obtaining feedback, and considerations for P&K
CHP • The Vale of Leven enquiry findings, and the creation of a position statement for
P&K CHP based on the recommendations.
4. CONCLUSION
As chair of the P&K Safety, Clinical Governance and Risk Group during financial year 2014/15, I am satisfied that the integrated approach, the frequency of meetings, the breadth of the business undertaken, and the range of attendees at meetings of the Committee has allowed us to fulfil our remit. As a result of the work undertaken during the year I can confirm that adequate and effective Safety, Clinical Governance & Risk arrangements were in place throughout Perth & Kinross CHP during the year.
3 This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held

Please note any items relating to Committee business are embargoed and should not be made public until after the meeting
I would like to thank all members of the Group for their contributions and continued support for the past year, members of staff who have prepared reports presented at the Group, and the Safety, Clinical Governance and Risk Team for their ongoing support. I would also like to thank Kerry Greig for her excellent ongoing support with the Group.
(signed)………………….………………………………. Dr Morag Martindale On behalf of the P&K CHP Safety, Clinical Governance and Risk Group
4 This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held

Please note any items relating to Committee business are embargoed and should not be made public until after the meeting Appendix 1 PERTH AND KINROSS SAFETY, CLINICAL GOVERNANCE AND RISK GROUP – 2014/15
Name
Designation
Organisation
01 04 14
03 06 14
05 08 14 14 10 14
02 12 14
03 02 15
Members Alison Wood Head of Corporate Services P&K CHP √ (By
Teleconference) √ √ √ √ √
Caroline Paterson Clinical Governance & Risk Management Team Lead
NHS Tayside Apologies Apologies √ Apologies Apologies Apologies
Diane Caldwell (until June then Julie Flynn)
Head of Children, Young People & Families
P&K CHP √ Apologies
Dr Morag Martindale Clinical Director P&K CHP √ √ √ √ Apologies Apologies Evelyn Devine Lead Officer P&K CHP Apologies Apologies Apologies Apologies Apologies √ Grace Gilling Interim Service Manager GAP P&K CHP Apologies √ √ Apologies √ Apologies Graeme Lamont Principal Pharmacist P&K CHP √ Apologies √ √ √ √ Jane Dernie Head of Allied Health Professions P&K CHP Apologies √ √ Apologies √ √ Jim McGuinness Prisoner Healthcare Service
Manager P&K CHP Apologies Apologies Apologies √ Apologies
Julie Flynn Head of Children, Young People & Families
P&K CHP Apologies Apologies √ √ √
Karen Buckley Infection Control Advisor NHS Tayside √ Apologies √ (Part) √ Apologies Apologies Lindsey Miller (June first meeting)
Service Manager for Integrated Community Services
P&K CHP √ √ Apologies Apologies Apologies
Mark Dickson Safety, Clinical Governance & Risk Co-ordinator
P&K CHP Apologies √ √ √ √ √
Sandra Gourlay Interim Lead Nurse P&K CHP √ √ √ Apologies √ √ Attendance as Required
Arlene Napier Head of CGR NHS Tayside Ian Jenkins Fire Safety Advisor NHS Tayside Rev Geoff Williams Spiritual Care NHS Tayside √ Val Fyall OHSAS H&S Advisor NHS Tayside In Attendance Angela Cunningham Primary Care Manager / Service
Improvement Manager P&K CHP √ √ √
Chris Lamont Head of Nursing Prisoner Healthcare
√ √
Gill MacFarlane Infection Control Nurse P&K CHP √ √

Please note any items relating to Committee business are embargoed and should not be made public until after the meeting Jo McEwen Advanced Nurse Practitioner -
Antimicrobial Stewardship
NHST
Kate Wright Head of Nursing (POA) Kerry Greig SCGR Support Officer P&K CHP √ Apologies Apologies Lee Sievewright Podiatry Service Manager, NHS
Tayside √
Lesley Booth Professional and Practice Development Nurse
P&K CHP √
Maggie Rapley Service Manager POA √ √ √ √ Pammy Chima Project Manager Integration
Translation Services √
Pauline McOmish Professional and Practice Development Nurse Children, Young People & Families
P&K CHP √ Apologies
Sarah Kelly Community Nurse Team Leader √ Tia Dixon Acting Service Manager
Occupational Therapy √
Tracey Passway Clinical Governance Risk Management Team Leader
√ √
Yvonne Wimbury SCGR Support Officer P&K CHP √ √ √
Not required to attend.

Please note any items relating to Committee business are embargoed and should not be made public until after the meeting
Appendix 2 PERTH & KINROSS SAFETY, CLINICAL GOVERNANCE AND RISK GROUP
SCHEDULE OF BUSINESS CONSIDERED APRIL 2014 – FEBRUARY 2015 1st APRIL 2014
• Action Points Update
o NHST Action Plan regarding report on ‘Manchester Child U’
• Annual Report for SCGR Group 2013/2014
o The group approved the contents of the report for 2013/2014.
• Group Role and Remit for 2014/2015
o Presentation and discussion on revised role and remit for 2014/2015.
• Group Work Plan for 2013/2014 and 2014/2015
o Presentation and revision of the group work plan for 2014/2015. o Agreement of additional priorities for incorporation into the 2014/2015 group work plan.
• Service Level Information
o Service exception reports (Services reporting on any key improvements or risks in relation to Safety, Clinical
Governance and Risk)
o Adverse Events/Complaints (Services to share any learning and improvements made after a significant
incident) (Services to share any learning and improvements made as a result of
complaints)
• Sharing Learning
o Vital Signs 575 –Treating Patients With Communication Barriers o Under the Influence of an Unauthorised Substance (Prisoner Healthcare) o Serious Case Review – Child U o Healthcare Support Worker Supported Improvement Plan o SCEA’s Sign Off (Services to share progress with actions, any learning and improvements made as a
result)
Please note any items relating to Committee business are embargoed and should not be made public until after the meeting
• Performance
o Complaints P&K Complaints report for the period March 2013 to February 2014.
o Unannounced visits o Infection Control o Report to CQF & CHP Measures for Safety, Governance & Risk
• NHST Information
o Clinical Quality Forum Update (17th March 2014) o Ombudsman Reports January 2014 and February 2014 o ‘Getting it Right’ Safety, Clinical Governance & Risk
Newsletter issues 2 and 3 (February and March 2014)
• Risk
o CHP Risks Inclusion of Children & Young People Bill Workforce (within Children & Young Peoples Services) Early Years
o Business Continuity Management
3rd JUNE 2014
• Safety
o Service exception reports (Services reporting on any key improvements or risks in relation to Safety, Clinical
Governance and Risk)
• Sharing Learning
o Spiritual Care Service Presentation on the work of Chaplains.
o Serious Case Review ‘Child U’ o SCEA’s Sign Off
(Services to share progress with actions, any learning and improvements made as a result)
o DATIX Presentation and review of all P&K CHP DATIX incidents relating to medication for
the period January 2014 – March 2014.
• Patient Experience
o Complaints Presentation of P&K Complaints Report for the period May 2013 - April 2014. (Services to share any learning and improvements made as a result of
complaints)
o Unannounced Visits Pitlochry Community Hospital, GP Ward
Please note any items relating to Committee business are embargoed and should not be made public until after the meeting
• Operational and Clinical Effectiveness
o Infection Control o Report to CQF & CHP Measures for Safety, Governance and Risk o Clinical Quality Forum Update (19th May 2014) o CHP Risks
• Leadership & Governance
o Ombudsman Reports March 2014 and April 2014 o ‘Getting it Right’ Clinical Governance & Risk Newsletter Issue 4 April 2014
• Workforce
o Discussion relating to workforce issues, recruitment and training.
5th AUGUST 2014
• Safety
o Service exception reports (Services reporting on any key improvements or risks in relation to Safety, Clinical
Governance and Risk)
• Sharing Learning
o Serious Case Review ‘Child U’ o SCEA’s Sign Off
(Services to share progress with actions, any learning and improvements made as a result)
o DATIX o Clinical Informed Consent Policy
Assurances sought that all areas are adhering to the Clinical Informed Consent Policy.
o Anticoagulation Service Redesign Presentation following the Anticoagulant Service Rapid Improvement Event held in
October 2013. o Enhanced Care Service
Discussion regarding how best to share the new structure of the Enhanced Care Service with the group.
• Patient Experience
o Complaints Presentation of P&K Complaints Report for the period July 2013 – June 2014. (Services to share any learning and improvements made as a result of
complaints)
Please note any items relating to Committee business are embargoed and should not be made public until after the meeting
o Unannounced Visits
Kinclaven Ward, Murray Royal Hospital
• Operational and Clinical Effectiveness
o Infection Control o Report to CQF & CHP Measures for Safety, Governance and Risk o Clinical Quality Forum Update (21st July 2014) o P&K CHP Performance Review Meeting Update o CHP Risks
• Leadership & Governance
o Ombudsman Reports May 2014 and June 2014 o ‘Getting it Right’ Clinical Governance & Risk Newsletter Issue 6 June 2014 and Special
Edition: Person Centeredness o Update on SCGR Improvement and Reporting System
• Workforce
o No items discussed.
14th OCTOBER 2014
• Patient Story (The telling of a patient story to share a patient’s experience and learning with the group.)
• Safety, Clinical Governance & Risk Group Work Plan 2014/2015 (Review of Group Work Plan for 2014/2015 and progress made to date.)
• Safety
o Clinical Governance Self Assessment Overview of process for completion of Clinical Governance Self Assessment
Questionnaire. Community Nursing and Palliative Care Self Assessment Findings.
o Service exception reports
(Services reporting on any key improvements or risks in relation to Safety, Clinical Governance and Risk)
• Sharing Learning
o Tayside Podiatry Staff/Patient Engagement - CARE Measure o SCEA’s Sign Off
(Services to share progress with actions, any learning and improvements made as a result)
o Learning from NHST SCEA o Patient Safety Network Launch
Please note any items relating to Committee business are embargoed and should not be made public until after the meeting
• Patient Experience
o Complaints Presentation of new P&K Complaints Report format for the period 1 January 2014
– 30 September 2014. (Services to share any learning and improvements made as a result of
complaints)
o Unannounced Visits Amulree Ward, Murray Royal Hospital
o National Patient Experience
• Operational and Clinical Effectiveness
o HIS Older People’s Inspection to PRI. (Findings from the HIS unannounced inspection of PRI, on 7th-9th July 2014, shared with the group.)
o Infection Control o CHP Measures for Safety, Governance and Risk o CHP Risks
• Leadership & Governance
o Clinical Quality Forum Update (15 September 2014) o Ombudsman Reports July 2014 and August 2014 o ‘Getting it Right’ Clinical Governance & Risk Newsletter Issues 8 August 2014 and 9
September 2014.
• Workforce o Discussion relating to workforce issues, recruitment and training.
2nd DECEMBER 2014
• Patient Story
(The telling of a patient story to share a patient’s experience and learning with the group.)
• Safety
o Service exception reports (Services reporting on any key improvements or risks in relation to Safety, Clinical
Governance and Risk)
• Sharing Learning
o Serious Case Review ‘ Child U’ o SCEA’s Sign Off
(Services to share progress with actions, any learning and improvements made as a result)

Please note any items relating to Committee business are embargoed and should not be made public until after the meeting
• Patient Experience
o Interpretation and Translation
Presentation regarding the revised Interpretation and Translation Policy. Accessing British Sign Language Interpreters. Discussion within the group.
o Complaints
Presentation of new P&K Complaints Report format for the period 1 January 2014 – 30 November 2014.
(Services to share any learning and improvements made as a result of complaints)
o Unannounced Visits
Crieff Community Hospital, Ward 2.
• Operational and Clinical Effectiveness
o Clinical Governance Self Assessment o Infection Control o Report to CQF & CHP Measures for Safety, Governance and Risk o Clinical Quality Forum Update (17 November 2014) o CHP Risks o New Standard Operating Procedure
(Group briefed on Administration of Controlled and Non Controlled drugs by Healthcare Support Workers.)
• Leadership & Governance
o Ombudsman Reports September 2014 and October 2014 o ‘Getting it Right’ Clinical Governance & Risk Newsletters September 2014 and October
2014. o NHST Guidance – Nutritional Standards
Inclusion of Nutritional Standards within Service Exception Reports.
• Workforce
o Discussion relating to workforce issues, recruitment and training included in Service Exception Reports.
3rd FEBRUARY 2015
• Patient Story (The telling of a patient story to share a patient’s experience and learning with the group.)

Please note any items relating to Committee business are embargoed and should not be made public until after the meeting
• Safety
o Service exception reports (Services reporting on any key improvements or risks in relation to Safety, Clinical
Governance and Risk) o SBAR Report: Potential Falls Hazards – Mental Health Services for Older People within
Murray Royal Hospital o Sharing Learning
SCEA’s sign off
• Patient Experience o Strategic Direction for Obtaining Feedback
(Presentation on the strategic direction for obtaining patient feedback within NHST) o Complaints
Presentation of new P&K Complaints Report format for the period 1 January 2014 – 23 January 2014.
(Services to share any learning and improvements made as a result of complaints)
• Operational and Clinical Effectiveness
o Clinical Governance Self Assessment o Infection Control o Measures for Safety, Clinical Governance and Risk o Clinical Quality Forum Update (12 January 2015)
No update available. o CHP Risks
• Leadership & Governance
o Vale of Leven Position Statements. o Ombudsman Reports November 2014 and December 2014 o ‘Getting it Right’ Clinical Governance & Risk Newsletter Issues December 2014 and
January 2015.
• Workforce
o Discussion relating to workforce issues, recruitment and training included in Service Exception Reports.

Please note any items relating to Committee business are embargoed and should not be made public until after the meeting
Item Number 7.3
Report Number 40/2015 Perth & Kinross CHP Committee
11 August 2015
PERTH & KINROSS COMMUNITY HEALTH PARTNERSHIP – FINANCIAL POSITION TO JUNE 2015 1. PURPOSE OF THE REPORT The purpose of this report is to inform the Committee of the financial position of Perth & Kinross
Community Health Partnership (Perth & Kinross CHP) at 30 June 2015.
2. RECOMMENDATIONS The CHP Committee is asked to note the information contained in this report, note the progress
made in absorbing savings targets during the year and to support the ongoing work underway in the CHP to improve the recurring financial position. The Committee is asked to note the ongoing remit of the CHP’s Budgetary Review Group in terms of ensuring the delivery of a balanced recurring budget.
3. EXECUTIVE SUMMARY The financial position at 30 June 2015 for Perth & Kinross CHP’s Hospital and Community
Health Services (HCHS), GP prescribing and share of other budgets is set out in the table 1 at section 4. At June the CHP is reporting a June month end overspend of £437k. The Director of Communities, CHP Interim Lead Officer and CHP Executive Team continue discussions to improve the CHPs in year and recurring financial position.
4. FINANCIAL POSITION A summary of the CHP’s financial position at 30 June 2015 is reported in table 1 below. Budget figures are quoted after allowing for £2.434m (4.1% of accessible budgets) of devolved recurring savings as per NHS Tayside’s budget setting process for 2015/16. The savings target of £2.434m has been attributed to HCHS Services (£1.314m) and Prescribing (£1.120m). Budgets for Family Health Services (including General Medical Services, General Pharmaceutical Services, General Dental Services, General Ophthalmic Services, etc.) are managed on a Tayside-wide basis but are apportioned to Community Health Partnerships on a pro-rata basis. The funding shown in table 1 is consistent with the CHP’s amended scheme of establishment. TABLE 1 - SUMMARY OF POSITION TO 30 JUNE 2015
Annual Budget
(£k) Budget to Date (£k)
Expenditure to Date (£k)
Over/Under (-) Spend
(£k) Hospital & Community Health Services 39,061 10,320 10,635 315 GP Prescribing 25,025 6,337 6,424 87 General Medical Services 21,409 5,684 5,719 35 Other Family Health Services 13,586 3,372 3,372 0 Total 99,081 25,713 26,150 437
1 This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held
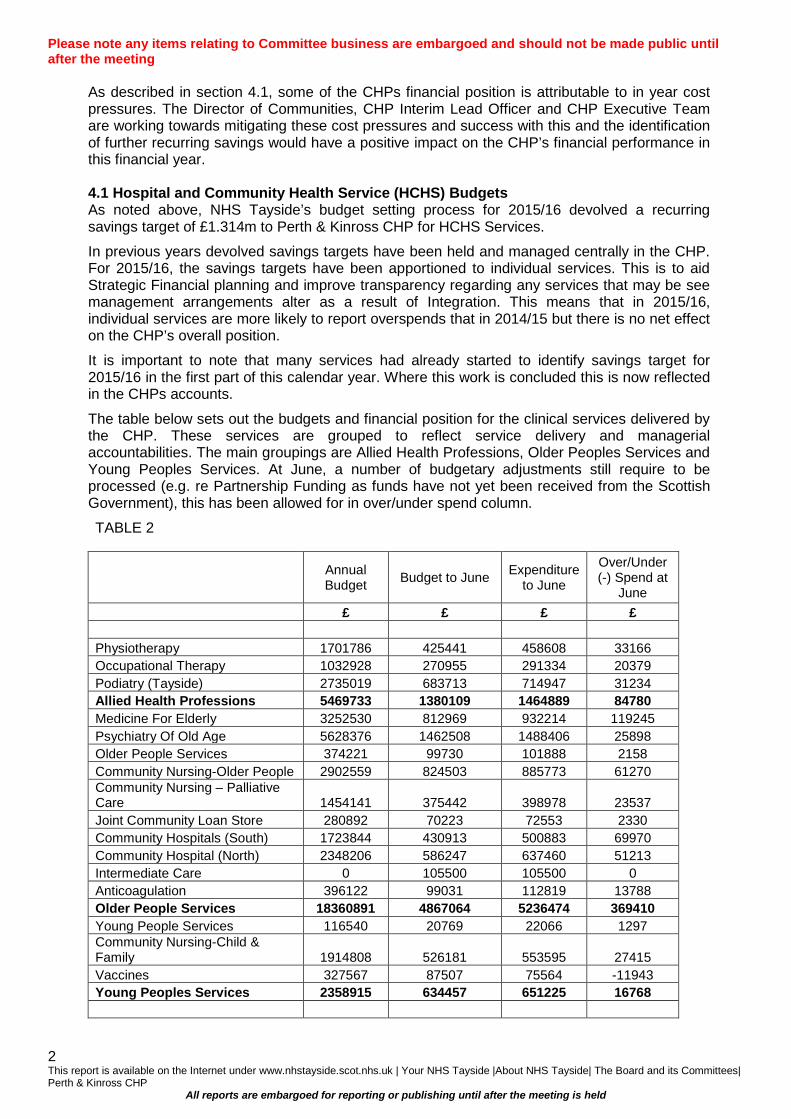
Please note any items relating to Committee business are embargoed and should not be made public until after the meeting
As described in section 4.1, some of the CHPs financial position is attributable to in year cost pressures. The Director of Communities, CHP Interim Lead Officer and CHP Executive Team are working towards mitigating these cost pressures and success with this and the identification of further recurring savings would have a positive impact on the CHP’s financial performance in this financial year.
4.1 Hospital and Community Health Service (HCHS) Budgets As noted above, NHS Tayside’s budget setting process for 2015/16 devolved a recurring savings target of £1.314m to Perth & Kinross CHP for HCHS Services.
In previous years devolved savings targets have been held and managed centrally in the CHP. For 2015/16, the savings targets have been apportioned to individual services. This is to aid Strategic Financial planning and improve transparency regarding any services that may be see management arrangements alter as a result of Integration. This means that in 2015/16, individual services are more likely to report overspends that in 2014/15 but there is no net effect on the CHP’s overall position.
It is important to note that many services had already started to identify savings target for 2015/16 in the first part of this calendar year. Where this work is concluded this is now reflected in the CHPs accounts.
The table below sets out the budgets and financial position for the clinical services delivered by the CHP. These services are grouped to reflect service delivery and managerial accountabilities. The main groupings are Allied Health Professions, Older Peoples Services and Young Peoples Services. At June, a number of budgetary adjustments still require to be processed (e.g. re Partnership Funding as funds have not yet been received from the Scottish Government), this has been allowed for in over/under spend column.
TABLE 2
Annual
Budget Budget to June Expenditure to June
Over/Under (-) Spend at
June £ £ £ £ Physiotherapy 1701786 425441 458608 33166 Occupational Therapy 1032928 270955 291334 20379 Podiatry (Tayside) 2735019 683713 714947 31234 Allied Health Professions 5469733 1380109 1464889 84780 Medicine For Elderly 3252530 812969 932214 119245 Psychiatry Of Old Age 5628376 1462508 1488406 25898 Older People Services 374221 99730 101888 2158 Community Nursing-Older People 2902559 824503 885773 61270 Community Nursing – Palliative Care 1454141 375442 398978 23537 Joint Community Loan Store 280892 70223 72553 2330 Community Hospitals (South) 1723844 430913 500883 69970 Community Hospital (North) 2348206 586247 637460 51213 Intermediate Care 0 105500 105500 0 Anticoagulation 396122 99031 112819 13788 Older People Services 18360891 4867064 5236474 369410 Young People Services 116540 20769 22066 1297 Community Nursing-Child & Family 1914808 526181 553595 27415 Vaccines 327567 87507 75564 -11943 Young Peoples Services 2358915 634457 651225 16768
2 This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held

Please note any items relating to Committee business are embargoed and should not be made public until after the meeting
Annual Budget Budget to June Expenditure
to June
Over/Under (-) Spend at
June Primary Care 422530 103133 97273 -5860 Med Training-Non Psychiatry 599182 149796 134184 -15612 Prisoner Health Services 2541129 772946 850830 77884 C.H.P. Management 299986 74996 66743 -8253 Lead Community Nursing 346811 82651 71902 -10749 Adults MH And Wellbeing 324546 75234 87028 11794 PCHP Admin & Clerical 1705619 426394 423619 -2775 Resource Transfer 6273000 1568250 1568250 0 Carers Strategy 124009 0 0 0 Partnership Funding 100000 0 45 45 Grants Voluntary Bodies 39000 -250 -2000 -1750 Other Perth & Kinross Services 12775812 3253149 3297874 44725 Centrally Managed Budget 95815 185279 -15831 -201110 TOTAL HCHS 39061166 10320059 10634631 314572
The main issues reflected in the June accounts, together with actions being taken to address these issues are summarised in table 3 below:-
TABLE 3
Issue Action/Detail Timescale
Medicine for the Elderly – In year overspends
Some of these services are operating with relatively high sickness absence levels (e.g. Tay Ward at 11.7% to June). This, exacerbated by maternity and recruitment issues, is necessitating the use of supplementary staffing – much of which is premium cost agency staffing.
Medicine for the Elderly overspends are also partly attributable to provision of additional bed capacity. This has a direct effect on staffing levels, costs and overspends. Work continues to move the service back towards agreed bed capacity levels.
Ongoing
Palliative Care – In year overspends
In Patients services are running with relatively high levels of sickness absence. This, coupled with instances of maternity leave and relatively high occupancy levels, are triggering overspends.
Ongoing
Community Hospitals – In year overspends
Some of these services are operating with relatively high sickness absence levels (e.g. Pitlochry 15.9%, Aberfeldy 9.7%, Crieff 8.9%, and St. Margarets 8.5% - all for period April to June 2015). This is exacerbated by managing vacancies in staffing. This has necessitated the use of supplementary staffing – much of which is premium cost agency staffing. The service is actively recruiting and reviewing staffing on a weekly basis.
Ongoing
Anti-coagulation Mainly historic activity pressures – under review via CHP Management team.
End of September
Child & Family Services
The service has had to adapt to recent funding changes and is doing so against a background of staff sickness, hard to fill posts and limited opportunities for further skill mix without compromising the professional agenda.
Ongoing
3 This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held

Please note any items relating to Committee business are embargoed and should not be made public until after the meeting
Issue Action/Detail Timescale
Prisoner Healthcare This service is showing increased cost pressures partly related to medical cover and requirement to use agency nursing to cover vacancies. The new Prisoner Healthcare Management Team is actively managing this situation to ensure long term service delivery is clinically and financially optimal.
Ongoing
Adult Mental Health & Well Being
There are a number of funding streams under review. Completion of the review may resolve reported pressures.
End of August
Protection Costs The CHP continues to incur c£6k per month of pay protection costs. Service Managers, in conjunction with Human Resources at a local and NHS Tayside level, continue to review this cost and seek pragmatic resolutions to addressing this.
Limited progress to date, but work ongoing.
4.2 Prescribing The reported Prescribing position reflects actual prescribing costs for April and estimates for May and June and is after budgets have absorbed devolved savings targets of £1.120m. The heavy reliance on estimates indicates some caution needs to be attached to these figures. Preliminary feedback suggests the month end overspend reflects a combination of progress regarding savings targets, growth in number of prescribed items being higher than anticipated and unit prices being above the budgeted level.
4.3 General Medical Services (GMS) There remain a number of pressures within GMS budgets. The month-end position reflects increasing Premises costs (often due to issues out-with NHS Tayside’s control), the volume of services being delivered through Enhanced Services and demand led pressures on Health Board funds including maternity cover. The management of these budgets continues to be overseen by the Associate Medical Director for Primary Care. A submission was made to NHS Tayside Prioritisation Process regarding funding for this service and further updates will be provided in future Finance reports.
4.4 Year End Out-turn
While the CHP is reporting a June overspend of c£437k. There is a corporate financial planning assumption that the ongoing effort to improve the CHP’s financial position will have a benefit in future months and that there will be an element of improvement over the coming months compared to the first 3 months of the financial year. Perth & Kinross CHP finances are managed within the overall level of financial resources available to NHS Tayside. Reports to NHS Tayside Finance and Resources Committee in late 2014/15 noted there were a number of risks to NHS Tayside delivering the requisite level of recurring savings. Partly based on NHS Tayside’s recent difficulties in identifying recurring savings during 2014/15, it can be assumed that there will be challenges to NHS Tayside delivering a balanced budget in 2015/16. Progress towards breakeven for NHS Tayside and Perth CHP will be dependent on both identifying efficiency saving opportunities and implementing those opportunities and mitigating cost pressures. NHS Tayside has created 5 corporate work streams have are intended to assist the whole organisation work towards identifying and delivery savings during 2015/16. Perth CHP will contribute to these work streams which are led by NHS Tayside Executives and are titled:-
• Workforce and Care Assurance • Optimising Demand Management • Optimising our Environments of Care • Cost Effective procurement • Repatriating Services.
4 This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held
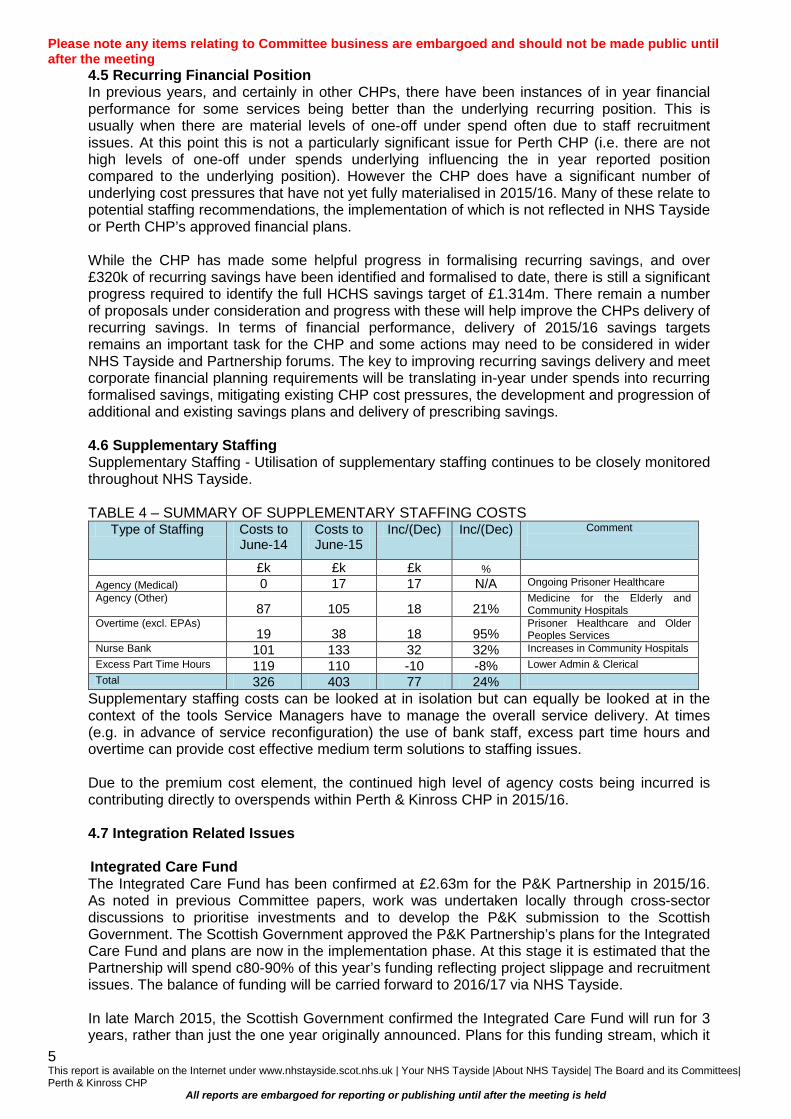
Please note any items relating to Committee business are embargoed and should not be made public until after the meeting
4.5 Recurring Financial Position In previous years, and certainly in other CHPs, there have been instances of in year financial performance for some services being better than the underlying recurring position. This is usually when there are material levels of one-off under spend often due to staff recruitment issues. At this point this is not a particularly significant issue for Perth CHP (i.e. there are not high levels of one-off under spends underlying influencing the in year reported position compared to the underlying position). However the CHP does have a significant number of underlying cost pressures that have not yet fully materialised in 2015/16. Many of these relate to potential staffing recommendations, the implementation of which is not reflected in NHS Tayside or Perth CHP’s approved financial plans. While the CHP has made some helpful progress in formalising recurring savings, and over £320k of recurring savings have been identified and formalised to date, there is still a significant progress required to identify the full HCHS savings target of £1.314m. There remain a number of proposals under consideration and progress with these will help improve the CHPs delivery of recurring savings. In terms of financial performance, delivery of 2015/16 savings targets remains an important task for the CHP and some actions may need to be considered in wider NHS Tayside and Partnership forums. The key to improving recurring savings delivery and meet corporate financial planning requirements will be translating in-year under spends into recurring formalised savings, mitigating existing CHP cost pressures, the development and progression of additional and existing savings plans and delivery of prescribing savings.
4.6 Supplementary Staffing
Supplementary Staffing - Utilisation of supplementary staffing continues to be closely monitored throughout NHS Tayside. TABLE 4 – SUMMARY OF SUPPLEMENTARY STAFFING COSTS
Type of Staffing Costs to June-14
Costs to June-15
Inc/(Dec) Inc/(Dec) Comment
£k £k £k %
Agency (Medical) 0 17 17 N/A Ongoing Prisoner Healthcare Agency (Other)
87 105 18 21% Medicine for the Elderly and Community Hospitals
Overtime (excl. EPAs) 19 38 18 95%
Prisoner Healthcare and Older Peoples Services
Nurse Bank 101 133 32 32% Increases in Community Hospitals Excess Part Time Hours 119 110 -10 -8% Lower Admin & Clerical Total 326 403 77 24%
Supplementary staffing costs can be looked at in isolation but can equally be looked at in the context of the tools Service Managers have to manage the overall service delivery. At times (e.g. in advance of service reconfiguration) the use of bank staff, excess part time hours and overtime can provide cost effective medium term solutions to staffing issues. Due to the premium cost element, the continued high level of agency costs being incurred is contributing directly to overspends within Perth & Kinross CHP in 2015/16.
4.7 Integration Related Issues Integrated Care Fund The Integrated Care Fund has been confirmed at £2.63m for the P&K Partnership in 2015/16. As noted in previous Committee papers, work was undertaken locally through cross-sector discussions to prioritise investments and to develop the P&K submission to the Scottish Government. The Scottish Government approved the P&K Partnership’s plans for the Integrated Care Fund and plans are now in the implementation phase. At this stage it is estimated that the Partnership will spend c80-90% of this year’s funding reflecting project slippage and recruitment issues. The balance of funding will be carried forward to 2016/17 via NHS Tayside. In late March 2015, the Scottish Government confirmed the Integrated Care Fund will run for 3 years, rather than just the one year originally announced. Plans for this funding stream, which it
5 This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held
Please note any items relating to Committee business are embargoed and should not be made public until after the meeting
is assumed will be c£2.63m per annum, have still to be determined. The funding for 2016/17 and 2018/19 will be consider alongside the carry forward from 2015/16. Delayed Discharge Funding Recently the Scottish Government has confirmed that funding to support work addressing Delayed Discharges will be available for a 3 year period (2015/16 – 2017/18). This fund will be c£800k in 2015/16, increasing to c£900k in 2016/17 and 2017/18. Full local plans for this funding stream have still to be fully developed and approved. Change Fund – Reshaping Care for Older People The Committee will be aware that the Scottish Government previously allocated funding to the Reshaping Care for Older People programme (Change Fund) for a 4 year period from 2011/12 and concluding in March 2015. A proportion of the cumulative funding to March 2015 has been carried forward into 2015/16 and will be utilised in a manner consistent with local plans and other Scottish Government Funding streams (e.g. those set out above). The overall plans are reviewed regularly via the Older Peoples Strategy Group. While the Partnership continues to develop it planning regarding services that have been, and are, effected by the above funding streams it is important to note that there are medium term risks associated with sustaining services developed through the Change Fund unless recurring funding can be identified. Integration Arrangements NHS Tayside and PKC Finance continue to work constructively, alongside other Local Authorities, to develop the financial frameworks regarding the Integration agenda. Work areas include financial reporting arrangements, scoping of budgets, budget and financial planning, financial governance frameworks including the Integration Scheme and Due Diligence processes. The main focus is currently on the Due Diligence process with an impending need to apply more resource to the strategic financial planning required to support the creation of the local Strategic Plan. Resource Transfer These budgets are reported at £6.079m. Proposals regarding uplifts to these budgets for 2015/16 have now been agreed.
5. CONTRIBUTION TO NHS TAYSIDE’S STRATEGIC AIMS Perth & Kinross CHP’s budgetary framework for 2015/16 reflects the Operational Plan under
which the CHP is delivering its services in this financial year.
6. MEASURES FOR IMPROVEMENT Efficiency improvements are reported in section 4.4 & 4.5 of this report. Other measures are
noted in the risk assessment.
7. IMPACT ASSESSMENT & INFORMING, ENGAGING & CONSULTING This paper has been prepared by the CHP Finance Manager in conjunction with the Interim
Lead Officer.
8. PATIENT EXPERIENCE None other than those specified in the paper.
9. RESOURCE IMPLICATIONS
Financial
Resource implications are detailed throughout this paper. Workforce None other than those specified in the paper.
6 This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held
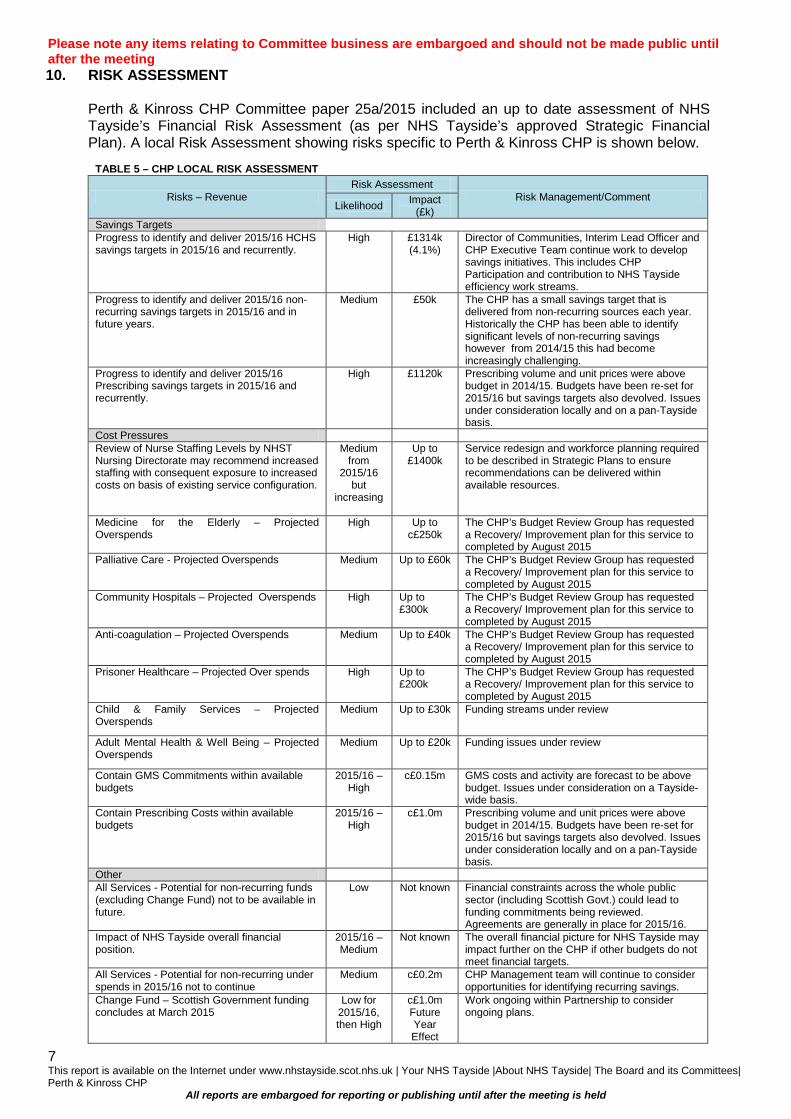
Please note any items relating to Committee business are embargoed and should not be made public until after the meeting 10. RISK ASSESSMENT
Perth & Kinross CHP Committee paper 25a/2015 included an up to date assessment of NHS Tayside’s Financial Risk Assessment (as per NHS Tayside’s approved Strategic Financial Plan). A local Risk Assessment showing risks specific to Perth & Kinross CHP is shown below.
TABLE 5 – CHP LOCAL RISK ASSESSMENT
Risks – Revenue Risk Assessment
Risk Management/Comment Likelihood Impact
(£k) Savings Targets Progress to identify and deliver 2015/16 HCHS savings targets in 2015/16 and recurrently.
High £1314k (4.1%)
Director of Communities, Interim Lead Officer and CHP Executive Team continue work to develop savings initiatives. This includes CHP Participation and contribution to NHS Tayside efficiency work streams.
Progress to identify and deliver 2015/16 non-recurring savings targets in 2015/16 and in future years.
Medium £50k The CHP has a small savings target that is delivered from non-recurring sources each year. Historically the CHP has been able to identify significant levels of non-recurring savings however from 2014/15 this had become increasingly challenging.
Progress to identify and deliver 2015/16 Prescribing savings targets in 2015/16 and recurrently.
High £1120k Prescribing volume and unit prices were above budget in 2014/15. Budgets have been re-set for 2015/16 but savings targets also devolved. Issues under consideration locally and on a pan-Tayside basis.
Cost Pressures Review of Nurse Staffing Levels by NHST Nursing Directorate may recommend increased staffing with consequent exposure to increased costs on basis of existing service configuration.
Medium from
2015/16 but
increasing
Up to £1400k
Service redesign and workforce planning required to be described in Strategic Plans to ensure recommendations can be delivered within available resources.
Medicine for the Elderly – Projected Overspends
High Up to c£250k
The CHP’s Budget Review Group has requested a Recovery/ Improvement plan for this service to completed by August 2015
Palliative Care - Projected Overspends Medium Up to £60k The CHP’s Budget Review Group has requested a Recovery/ Improvement plan for this service to completed by August 2015
Community Hospitals – Projected Overspends High Up to £300k
The CHP’s Budget Review Group has requested a Recovery/ Improvement plan for this service to completed by August 2015
Anti-coagulation – Projected Overspends Medium Up to £40k The CHP’s Budget Review Group has requested a Recovery/ Improvement plan for this service to completed by August 2015
Prisoner Healthcare – Projected Over spends High Up to £200k
The CHP’s Budget Review Group has requested a Recovery/ Improvement plan for this service to completed by August 2015
Child & Family Services – Projected Overspends
Medium Up to £30k Funding streams under review
Adult Mental Health & Well Being – Projected Overspends
Medium Up to £20k Funding issues under review
Contain GMS Commitments within available budgets
2015/16 – High
c£0.15m GMS costs and activity are forecast to be above budget. Issues under consideration on a Tayside-wide basis.
Contain Prescribing Costs within available budgets
2015/16 – High
c£1.0m Prescribing volume and unit prices were above budget in 2014/15. Budgets have been re-set for 2015/16 but savings targets also devolved. Issues under consideration locally and on a pan-Tayside basis.
Other All Services - Potential for non-recurring funds (excluding Change Fund) not to be available in future.
Low Not known Financial constraints across the whole public sector (including Scottish Govt.) could lead to funding commitments being reviewed. Agreements are generally in place for 2015/16.
Impact of NHS Tayside overall financial position.
2015/16 – Medium
Not known The overall financial picture for NHS Tayside may impact further on the CHP if other budgets do not meet financial targets.
All Services - Potential for non-recurring under spends in 2015/16 not to continue
Medium c£0.2m CHP Management team will continue to consider opportunities for identifying recurring savings.
Change Fund – Scottish Government funding concludes at March 2015
Low for 2015/16, then High
c£1.0m Future Year Effect
Work ongoing within Partnership to consider ongoing plans.
7 This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held

Please note any items relating to Committee business are embargoed and should not be made public until after the meeting 11.
LEGAL IMPLICATION
There are no legal implications directly resulting from this paper.
12. INFORMATION TECHNOLOGY IMPLICATIONS There are no Information Technology implications directly resulting from this paper.
13. HEALTH & SAFETY IMPLICATIONS There are no Health and Safety implications directly resulting from this paper.
14. HEALTHCARE ASSOCIATED INFECTION (HAI) There are no HAI implications directly resulting from this paper.
15. DELEGATION LEVEL 16.
There are no delegation issues directly resulting from this paper. REPORT SIGN OFF Evelyn Devine, Interim Lead Officer, Perth & Kinross CHP
Alexander Berry Finance Manager NHS Tayside 11 August 2015
8 This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held

Please note any items relating to Committee business are embargoed and should not be made public until after the meeting
Item Number 7.4 Report Number 41/2015
Perth & Kinross CHP Committee 11 August 2015
TAYSIDE NHS BOARD FINAL REPORT OF PERTH & KINROSS CHP COMMITTEE APRIL – AUGUST 2015 1. PURPOSE
In order to assist the Board in conducting a regular review of the effectiveness of the systems of internal control, the Code of Corporate Governance requires that this Standing Committee submits an annual report to the Audit Committee. This report is submitted in fulfilment of this requirement. It covers the period April to August 2015 which is the length of time that the Committee met prior to its disestablishment, in preparation for the Integration Joint Board of Perth and Kinross Health and Social Care Partnership.
2. PERTH & KINROSS CHP COMMITTEE 2.1 Composition
During the current year up to August 2015 membership of Perth and Kinross CHP Committee comprised:
Mrs Linda Dunion, Chairperson Mr Arthur Andrews, PPG Group Member Dr Morag Curnow, Clinical Dental Director Mrs Jane Dernie, Head of AHPs Mrs Evelyn Devine, Interim Lead Officer Councillor Dave Doogan, Perth & Kinross Council Mr Ian Duncan, Community Pharmacist Mr Bob Gillespie, Voluntary Services Member Mrs Sandra Gourlay, Lead Nurse Dr John Harper, Consultant Physician, MfTE, PRI Councillor Kate Howie, Local Authority Member, Perth & Kinross Council Dr Neil McLeod, General Practitioner Representative Mr Raymond Marshall, Area Partnership Forum Representative Dr Morag Martindale, Clinical Director Mr Bill Nicoll, Director of Community Services & Primary Care Mrs Maureen Summers, Carers Representative Mrs Sheila Tunstall-James, Vice Chairperson Mr John Walker, Depute Director Housing & Community Care
This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held
1

Please note any items relating to Committee business are embargoed and should not be made public until after the meeting
Support to the Committee is provided by Mrs Valerie Aitken, Corporate Services/Business Support Manager.
2.2 Meetings
The Committee has met on three occasions during the period from 1 April 2015 to 11 August 2015 on the undernoted dates: 14 April 2015 09 June 2015 11 August 2015 Record of Attendance is attached at Appendix 1.
2.3 Business Minutes of the meetings of the Committee have been timeously submitted to the Tayside NHS Board for its information. Details of the business items considered are attached at Appendix 2. Service Delivery & Redesign/Health Improvement/Patient Centred/Health Inequalities Adult Support & Protection Violence against Women Telehealth Carer Strategy HMP Perth Recovery College Workforce Plan Central Healthcare/Keepwell Stroke Services Post Diagnostic Support Clinical & Care Governance Framework Drug & Alcohol Local Delivery Plan Review of Primary Care Enhanced Care Services Person Centred Care Health & Social Care Integration Health & Social Care Integration Action Plan & Status Integrated Locality Working OT Integrated Services Joint Clinical & Care Commissioning Integrated Care Fund Workstreams
This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held
2

Please note any items relating to Committee business are embargoed and should not be made public until after the meeting
Governance & Assurance • Performed financial stewardship and agreed proposals for seeking
recurring balance by monitoring the financial position through the submission of reports
• Scrutinised regular performance reports providing assurance to Perth and Kinross CHP Committee
• Scrutinised minutes from the Safety, Clinical Governance and Risk (SCGR) Group.
• Considered regular reports from Steps to Better Healthcare Programme regarding Medicines Leadership
• Scrutinised Workforce Governance and Partnership update reports • Considered reports from the Clinical Director of the CHP which reported
on clinical input to the business of the CHP.
3. OUTCOMES
The committee has, through its scrutiny and monitoring, been able to assure NHS Tayside Board of its:
• Financial Management (Best Value) by giving continuing emphasis to monitoring efforts to SEEK financial balance and savings targets during 2015. It received updates at each meeting of the processes to assure it of the financial governance measures undertaken by the Interim Lead Officer and her budget holders to ensure efficient, effective and prudent financial management.
• Performance monitoring through identifying the principal targets and standards the CHP has responsibility for and demonstrating progress against these through compilation and monitoring of trend charts at each meeting.
• Improvements to quality, value and patient satisfaction by maintaining a calendar of service reports from each of the major patient pathways; these are scrutinised on, at least, an annual basis. Plans for strategic service changes or improvements are subject to reports on an ad hoc basis
• Contributions to NHS Tayside programmes such as Health & Social Care Integration, Mental Health Services for Older People including Post Diagnostic Support, Steps to Better Health Care and Health Inequalities. The committee has been well briefed and supports the continuing progress of improving care and support for adults and families, enhanced care and alternatives to admission, as well improvements to pharmacy and the various workstreams under the Change Fund and Integrated Care Fund programme.
• Partnership Working (Best Value) was demonstrated through reports from joint or integrated services and bi-annual staff governance reports.
The Committee has completed 50% of its workplan for 2015/16 by August 2015 and the remaining 50% of business not completed will be remitted to the Interim Lead Officer, Perth and Kinross CHP, to drive and direct the CHP Committee workplan business to bi-monthly Senior Management Team meetings in line with the timetabled programme, and onwards to the Integrated Leadership Group of the
This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held
3
Please note any items relating to Committee business are embargoed and should not be made public until after the meeting
Community and Primary Care Directorate and/or committee structures as detailed in Item 7.5 – Dissolution of Perth & Kinross CHP Report which was submitted at the final Perth & Kinross CHP Committee meeting held on 11 August 2015.
All business was conducted in open session.
4. BEST VALUE
The Board is required to provide overt assurance on Best Value. An updated Best Value Framework was approved by the Board on 24 June 2014. The Committee has considered the elements relevant to it and this evidence is provided at Appendix 3.
5. RISK REPORTING Perth & Kinross CHP Committee received reports on the following Corporate Risks during 2015: Adult Support and Protection Violence Against Women Clinical Governance Health & Social Care Integration Human Resources Healthcare Associated Infection
6. CONCLUSION As Chair of the Perth & Kinross Community Health Partnership Committee from April to August 2015, I am satisfied that the integrated approach, the frequency of meetings, the breadth of the business undertaken, and the range of attendees at meetings of the Committee has allowed us to fulfil our remit as detailed in the Code of Corporate Governance. As a result of the work undertaken during the year I can confirm that adequate and effective arrangements were in place throughout NHS Tayside during the year. I would again pay tribute to the dedication and commitment of fellow members of the Committee and to all attendees. I would thank all those members of staff who have prepared reports and attended meetings of the Committee, and last, but certainly not least, express my sincere thanks to Val Aitken for her support of the Committee. (signed)……………………………………….. MRS LINDA DUNION CHAIRPERSON 2015/16 On behalf of PERTH & KINROSS CHP COMMITTEE
This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held
4
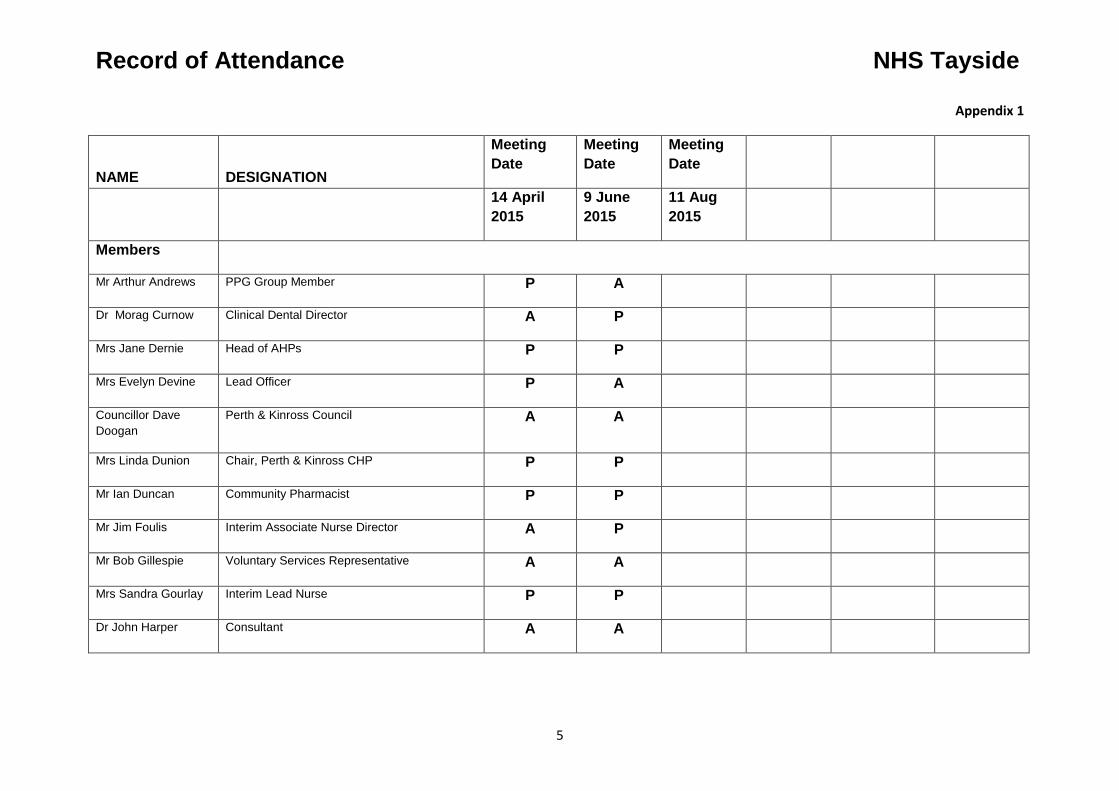
Record of Attendance NHS Tayside
Appendix 1
NAME DESIGNATION
Meeting Date
Meeting Date
Meeting Date
14 April 2015
9 June 2015
11 Aug 2015
Members
Mr Arthur Andrews PPG Group Member P A
Dr Morag Curnow Clinical Dental Director A P
Mrs Jane Dernie Head of AHPs P P
Mrs Evelyn Devine Lead Officer P A
Councillor Dave Doogan
Perth & Kinross Council A A
Mrs Linda Dunion Chair, Perth & Kinross CHP P P
Mr Ian Duncan Community Pharmacist P P
Mr Jim Foulis Interim Associate Nurse Director A P
Mr Bob Gillespie Voluntary Services Representative A A
Mrs Sandra Gourlay Interim Lead Nurse P P
Dr John Harper Consultant A A
5

Record of Attendance NHS Tayside
NAME DESIGNATION
Meeting Date
Meeting Date
Meeting Date
14 April 2015
9 June 2015
11 Aug 2015
Councillor Kate Howie
Perth & Kinross Council P A
Dr Neil McLeod General Practitioner P P A
Mr Raymond Marshall
Partnership Forum Representative A A
Dr Morag Martindale Clinical Director P P
Mr Bill Nicoll Director of Community & Primary Care Services
P A
Mrs Maureen Summers
Carers Representative P P
Mrs Sheila Tunstall-James
Vice Chairperson P P
Mr John Walker Executive Director (Housing and Community Care)
A A
Advisors
Mr Sandy Berry Accountant, NHS Tayside P P
Mr Christopher Smith Head of HR, Perth & Kinross CHP A P A
6

Record of Attendance NHS Tayside
NAME DESIGNATION
Meeting Date
Meeting Date
Meeting Date
14 April 2015
9 June 2015
11 Aug 2015
Attendees
Mrs Karen Melville Pharmacy Team Leader A P
Miss Alison Wood Head of Corporate Services P P
Mrs Valerie Aitken Corporate Services/Business Support Manager P P
Mr Paul Henderson Perth & Kinross Council P
Mrs Grace Gilling Service Manager, Perth & Kinross Adult Mental Health Services
P
Aileen Tarditio Unified Communications Manager, eHealth Directorate
P
Miss Lauraine Miller HR Business Lead, NHS Tayside P
Mr John Gilruth Depute Director Housing & Community Care, Perth & Kinross Council
P
Rob Packham Associate AHP Director P
Chris Lamont Head of Nursing, Community Nursing P
7

Record of Attendance NHS Tayside
NAME DESIGNATION
Meeting Date
Meeting Date
Meeting Date
14 April 2015
9 June 2015
11 Aug 2015
Julieann Flynn Head of Children, Young People and Famlies Service
P
Lauraine Miller HR Business Lead P
Maggie Rapley Service Manager Psychiatry of Old Age P
Hong Zhang Voluntary Services P
Iain Smillie
Angela Cunningham
Lindsey Miller
Lorraine Marshall
8
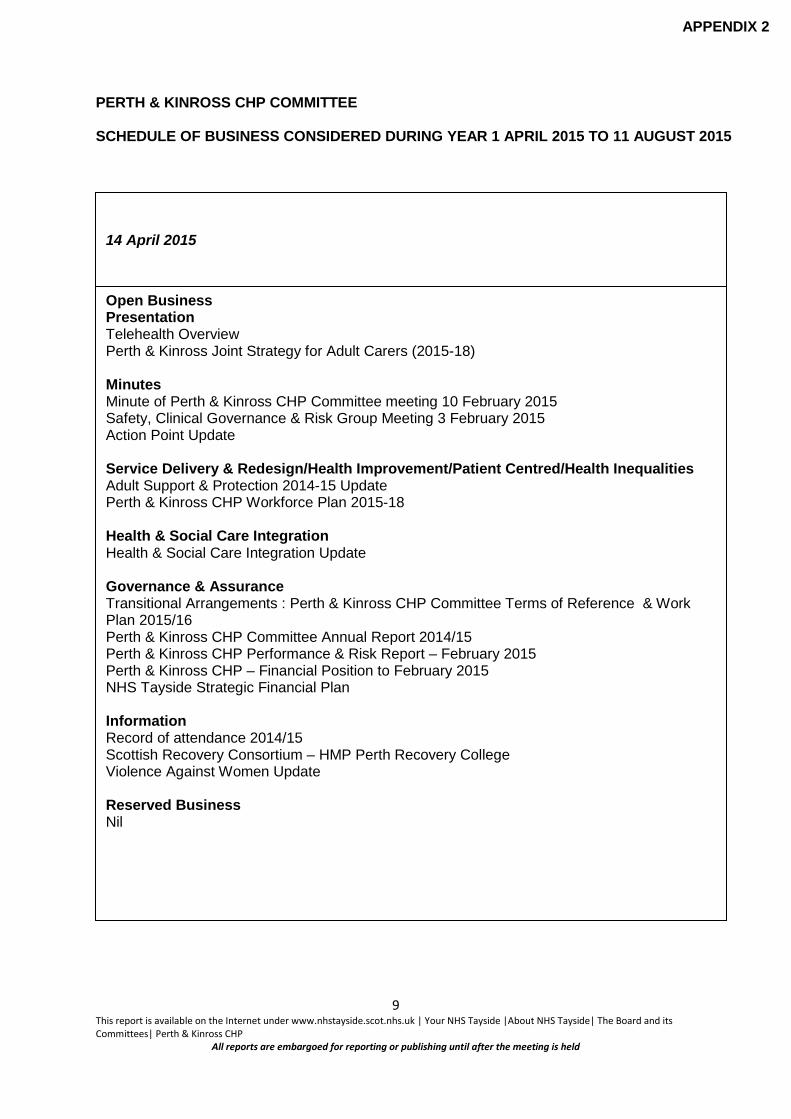
PERTH & KINROSS CHP COMMITTEE SCHEDULE OF BUSINESS CONSIDERED DURING YEAR 1 APRIL 2015 TO 11 AUGUST 2015
APPENDIX 2
14 April 2015
Open Business Presentation Telehealth Overview Perth & Kinross Joint Strategy for Adult Carers (2015-18) Minutes Minute of Perth & Kinross CHP Committee meeting 10 February 2015 Safety, Clinical Governance & Risk Group Meeting 3 February 2015 Action Point Update Service Delivery & Redesign/Health Improvement/Patient Centred/Health Inequalities Adult Support & Protection 2014-15 Update Perth & Kinross CHP Workforce Plan 2015-18 Health & Social Care Integration Health & Social Care Integration Update Governance & Assurance Transitional Arrangements : Perth & Kinross CHP Committee Terms of Reference & Work Plan 2015/16 Perth & Kinross CHP Committee Annual Report 2014/15 Perth & Kinross CHP Performance & Risk Report – February 2015 Perth & Kinross CHP – Financial Position to February 2015 NHS Tayside Strategic Financial Plan Information Record of attendance 2014/15 Scottish Recovery Consortium – HMP Perth Recovery College Violence Against Women Update Reserved Business Nil
9 This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held

10 June 2014
Open Business Presentation Clinical, Care and Professional Governance Framework Minutes Minute of Perth & Kinross CHP Committee meeting 14 April 2015 Safety, Clinical Governance & Risk Group Meeting 7 April 2015 Action Point Update Service Delivery & Redesign/Health Improvement/Patient Centred/Health Inequalities Perth Royal Infirmary Stroke Update Perth & Kinross Psychiatry of Old Age (POA) Services – Post Diagnostic Support Central Healthcare/Keepwell Update Health & Social Care Integration Health & Social Care Integration Update Perth & Kinross Integrated Locality Working Update on OT Integration Governance & Assurance Perth & Kinross CHP Committee Work Plan 2015/16 Perth & Kinross CHP Performance & Risk Report Clinical Director Update Report Perth & Kinross CHP – Financial Position to March 2015 Perth & Kinross CHP Staff Governance Report June 2015 Steps to Better Healthcare Programme – Medicines Leadership Information Record of attendance 2014/15 Reserved Business Nil
09 June 2015
10 This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held

11 August 2015
Open Business Presentation Person Centred Care Reshaping Care for Older People: Enhanced Community Support Update Minutes Perth & Kinross CHP Committee Meeting 9 June 2015 Safety, Clinical Governance & Risk Group Minutes 2 June 2015 Action Point Update Service Delivery & Redesign/Health Improvement/Patient Centred/Health Inequalities Primary Care Update Update Alcohol & Drug Partnership (ADP) Strategy Local Delivery Plan Health & Social Care Integration Health & Social Care Integration Update Perth & Kinross Integrated Care Fund Governance & Assurance Perth & Kinross CHP Performance & Risk Report Annual Report Perth & Kinross Safety, Clinical Governance & Risk Group 2014/2015 Perth & Kinross CHP – Financial Position to June 2015 Perth & Kinross CHP Committee Report April – August 2015 Dissolution of Perth & Kinross CHP – 11 August 2015: Interim Arrangements to 31 March 2016. Information Record of attendance 2015/16 Reserved Business Nil
11 This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held

PERTH & KINROSS CHP COMMITTEE
CHARACTERISTIC 1 – GOVERNANCE AND ACCOUNTABILITY REQUIREMENT MEASURE /EXPECTED
OUTCOME RESPONSIBILITY TIMESCALE EVIDENCE RECEIVED
Board and Committee decision-making processes are open and transparent.
Board and Committee meetings are held in open session and minutes are publically available.
Perth & Kinross CHP Committee
On going This occurs at every meeting and minutes and papers are published to NHS Tayside Internet site.
APPENDIX 3
12 This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held

Board and Committee decision-making processes are based on evidence that can show clear links between activities and outcomes
Reports for decision to be considered by Board and Committees should clearly describe the evidence underpinning the proposed decision.
Perth & Kinross CHP Committee
As required All reports submitted to the Committee for a decision can evidence the underpinning information required to support the recommendations required of the committee.
Report 1/2015 Report 4/2015 Report 10/2015 Report 12/2015 Report 13/2015 Report 20/2015 Report 21/2015 Report 22/2015 Report 23/2015 Report 24/2015 Report 31/2015 Report 33/2015 Report 34/2015 Report 35/2015
13 This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held

CHARACTERISTIC 2 – PERFORMANCE MANAGEMENT
Performance is systematically measured across all key areas of activity.
The Board delegates to Committees the performance reporting for key areas of activity
Board receives regular performance reports
Perth & Kinross CHP Committee
As required
Every meeting
The Board scrutinises the Performance of P & K CHP Committee through its detailed minutes which are submitted to the board after each meeting.
The Board and its Committees approve the format and content of the performance reports they receive which should include –
Assess its performing against the following criteria:
Performance reporting provides an understanding of whether the organisation is on track to achieve its short and long-term strategic, operational and quality objectives
The Board/Committees reviews the performance reporting under its remit and agrees the measures
Perth & Kinross CHP Committee
Every meeting The Committee scrutinises its performance in relation to Financial Management, Risk Management and key Business Performance measures including clinical and staff governance indicators.
14 This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held
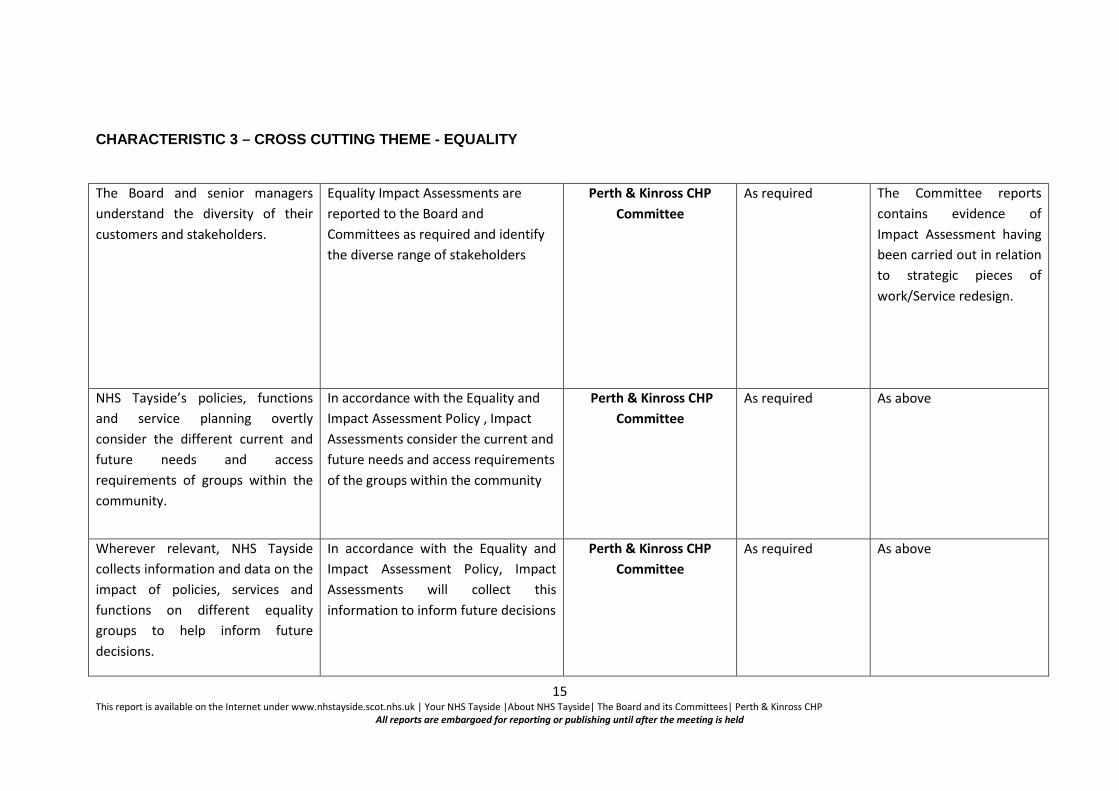
CHARACTERISTIC 3 – CROSS CUTTING THEME - EQUALITY The Board and senior managers understand the diversity of their customers and stakeholders.
Equality Impact Assessments are reported to the Board and Committees as required and identify the diverse range of stakeholders
Perth & Kinross CHP Committee
As required The Committee reports contains evidence of Impact Assessment having been carried out in relation to strategic pieces of work/Service redesign.
NHS Tayside’s policies, functions and service planning overtly consider the different current and future needs and access requirements of groups within the community.
In accordance with the Equality and Impact Assessment Policy , Impact Assessments consider the current and future needs and access requirements of the groups within the community
Perth & Kinross CHP Committee
As required As above
Wherever relevant, NHS Tayside collects information and data on the impact of policies, services and functions on different equality groups to help inform future decisions.
In accordance with the Equality and Impact Assessment Policy, Impact Assessments will collect this information to inform future decisions
Perth & Kinross CHP Committee
As required As above
15 This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held
NHS Tayside engages with and involves equality groups to improve and inform the development of relevant policy and practice.
In accordance with the Equality and Impact Assessment Policy, Impact Assessments will involve equality groups and inform the development of relevant policy and practice
Perth & Kinross CHP Committee
As required
16 This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held

Please note any items relating to Committee business are embargoed and should not be made public until after the meeting
Item Number 7.5
Report Number 42/2015
Perth and Kinross CHP Committee 11 August 2015
DISSOLUTION OF PERTH AND KINROSS CHP 11 AUGUST 2015: INTERIM ARRANGEMENTS TO 31 MARCH 2016 1. SITUATION AND BACKGROUND NHS Board agreed to conclude CHP Committees on or before 31st August 2015, to clear the way for the emergent Integration Joint Boards. This was promulgated on the advised timetable for approval of the draft Integration Schemes which now will be extended until October 2015. This means that the transfer of functions and services is unlikely to occur in advance of 1 April 2016, as the IJBs will have to meet formally after the scheme approvals, approve the Joint Strategic Commissioning Plans, consult on the plans and agree a transfer date that will enable a smooth transition of functions and services. Therefore, it seems likely that the delegated services will need to continue to be managed under alternative governance and accountability arrangements for an extended period after the CHP Committees have concluded. At its meeting on 25 June 2015, NHS Tayside Board agreed to maintain strong accountability and governance during this period through the following measures:
• CHPs to report on completion of existing workplans and to complete final reports to 31 August 2015.
• Alternative arrangements agreed for the decision making responsibilities relating to functions currently governed through the CHP Committees.
• CHP and Primary and Community Directorate senior management arrangements consolidated to provide oversight of operational management responsibilities.
• Detailed report to August NHS Board to set out proposed interim and future arrangements for governance, accountability and management arrangements for current and retained NHS functions.
2. ASSESSMENT
2.1 Arrangements following the dissolution of CHPs The Director of Community and Primary Care Services will present a report at Tayside NHS Board’s meeting on 27 August 2015 which sets out the proposals for dealing with the business of the CHP Committees during the period from 1 September 2015 to 31 March 2016.
1 This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held

Please note any items relating to Committee business are embargoed and should not be made public until after the meeting
At that meeting, it will be proposed to Tayside NHS Board that the roles and responsibilities of the CHP Committees will be discharged through a combination of officer level delegation, management decision making structures and other decision making and governance structures and committees within NHS Tayside in accordance with a revised Scheme of Delegation. An overview of these arrangements are as follows:
1. The NHS Tayside Scheme of Delegation will be revised to take account of the dissolution of the CHP Committees.
2. Finance and Budgeting Reporting will be through the Finance and Resources Committee and NHS Board.
3. Clinical, Professional and Care Governance Reporting will be through the Improvement and Quality Committee (now named the Clinical and Care Governance Committee).
4. Performance Management The overall Clinical and Care Governance, including patient safety, incidents, complaints, infection control and clinical quality indicators will be reported through the Performance Review process to the Clinical and Care Governance Committee as above. Health and safety and risk will be governed at local level and will be reported through the Strategic Risk Management Group and through the Board Assurance Framework to the NHS Board. Operational and Business performance will also be reported through the Performance Review process and will be included in the performance reporting to NHS Board.
5. Staff, Workforce and Partnership Working The staff, workforce and partnership aspects will be dealt with through local management arrangements and escalated though the management structure and to the Staff Governance Committee. These issues may also be channelled through the partnership structure from the local partnership forum to the Directorate Partnership Forum and through the Workforce and Governance Group and Area Partnership Forum.
6. Operational Management These aspects will be dealt with at Perth and Kinross CHP Senior Management Team level and escalated through the Directorate Management Team, (Corporate) Senior Management Team, Chief Executives and Directors and through to Standing Committees or NHS Board as appropriate.
2.2 CHP Committee Workplan Business The schematic at Appendix 1 illustrates the reporting arrangements during the interim period September 2015 to March 2016. It will be remitted to the Interim Lead Officer, Perth and Kinross CHP, to drive and direct the CHP Committee workplan business to bi-monthly Senior Management Team meetings in line with the timetabled programme, and onwards to the Integrated Leadership Group of the Community and Primary Care Directorate and/or committee structures described in paragraphs 1 – 6 above.
2 This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held
Please note any items relating to Committee business are embargoed and should not be made public until after the meeting
2.3 A look back over the work of Perth and Kinross CHP Committee
Perth and Kinross CHP Committee can look back over the last ten years to a series of achievements. It has progressed pathways which have supported shifting the balance of care as well as developing and modernising services. It has overseen improvements to equity of access to services, across a range of settings. It has also been able to significantly progress the integration agenda through partnership working. In addition, the Committee successfully fulfilled its corporate governance responsibilities to provide assurance to Tayside NHS Board that the functions delegated to it have met performance standards within resources. The Director of Community and Primary Care Services, NHS Tayside, has stated, ‘It is important to acknowledge that the CHP Committees have operated successfully over a ten year period during which the members of each CHP Committee have made a significant, sustained contribution towards improvement of health and care in Tayside. The success of the CHPs in Tayside has provided a strong foundation for the transition towards the next stage of the journey through health and social care and so the CHP Committees will make way for the formal establishment of the Integration Joint Boards as the vehicles for integration.’
4. RECOMMENDATIONS
Perth and Kinross CHP Committee is asked to
• Agree the transitional governance arrangements following the dissolution of CHPs and
prior to the transfer of functions and responsibilities to the Integration Joint Boards • Agree that the Interim Lead Officer will direct PKCHP Committee workplan business in
line with NHS Tayside’s governance and management processes as detailed in the Appendix 1 schematic
• Note the timetable of business which will be scheduled to SMT and for onward direction to management and governance forums as required (Appendix 2)
5. REPORT SIGN OFF Evelyn Devine, Interim Lead Officer, Perth & Kinross CHP Alison Wood Head of Corporate Services and Business Support Perth and Kinross CHP 6 August 2015
3 This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held
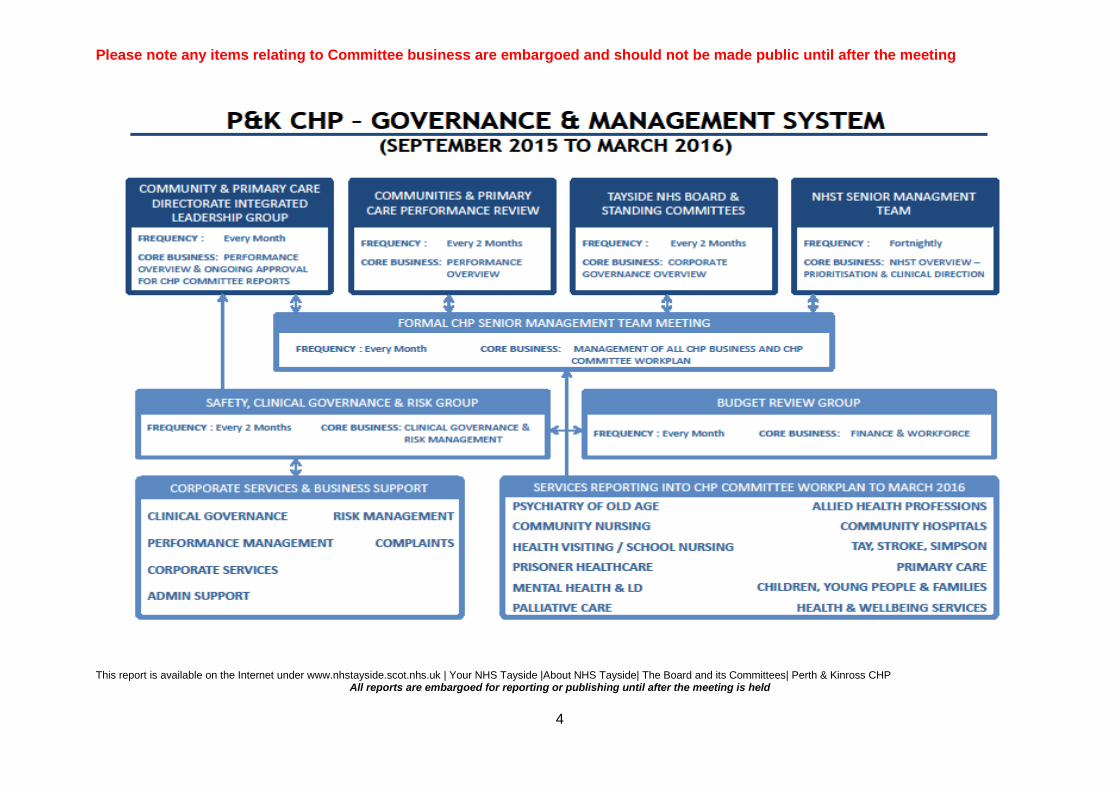
Please note any items relating to Committee business are embargoed and should not be made public until after the meeting
This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP All reports are embargoed for reporting or publishing until after the meeting is held
4

Please note any items relating to Committee business are embargoed and should not be made public until after the meeting
Appendix 2 The Perth and Kinross CHP Committee work plan has been developed to reflect the leadership role of the CHP to work in partnership with people and organisations to shape, design and deliver services. The CHP is also a key partner in contributing to improving people’s health and well being to ensure a high quality of life within all Perth and Kinross communities.
Perth and Kinross CHP Committee Work Plan 2015-16 Business item Lead Officer 14 April 2015 09 June
2015 11 August 2015
SMT 29 October 2015
SMT 17 December 2015
SMT Feb 2016 (DATE TO BE CONFIRMED)
Service Delivery & Redesign/Health Improvement/Patient Centred/Health Inequalities
Child Protection Julieann Flynn X Adult Support & Protection Grace Gilling X Violence against Women Julieann Flynn X Drug & Alcohol Ian Smillie X Suicide & Self Harm – Children & Young People
Julieann Flynn X
Suicide & Self Harm – Adults Grace Gilling X Weight Management – Children & Young People & Adults
Dr Laura Stewart X
Equally Well Julieann Flynn X Local Delivery Plan Bill Nicoll/Lorraine
Marshall X
Central Healthcare/Keepwell Chris Lamont X Stroke Services Sue Muir X Telehealth Aileen Tardito/Jane
Dernie X X
Respiratory Services Jane Dernie X Podiatry
Lee Sievewright X
Mental Health Services for Older People
Maggie Rapley X
This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP All reports are embargoed for reporting or publishing until after the meeting is held
5

Please note any items relating to Committee business are embargoed and should not be made public until after the meeting
Business item Lead Officer 14 April 2015 09 June 2015
11 August 2015
SMT 29 October 2015
SMT 17 December 2015
SMT Feb 2016 (DATE TO BE CONFIRMED)
Development of Community Hospitals/SLA
Sue Muir X
Review of Primary Care Angela Cunningham X Adult Mental Health Services Improvement Plan
Grace Gilling X
Steps to Better Healthcare/Palliative Care
Lindsey Miller X
Carer Strategy Lindsey Miller X Prisoner Healthcare Jillian Galloway X Learning Disability Strategy Angie McManus Clinical Strategy Andrew Russell/Ann
Eriksen X
Children, Young People & Family Services
Julieann Flynn X
Post Diagnosis Support Maggie Rapley X Community Care Services Lindsey Miller X Welfare Reform Aileen Tait X Unschedule Care/LUCAP Sue Muir X HMP Perth Recovery College Delphine Easson X Clinical and Care Governance Framework
Rob Packham/Jane Dernie
X X
Winter Planning Amanda Clements X Review of MIIUs Lindsey Miller X Delayed Discharges Sue Muir X Enhanced Care Services Lindsey Miller X Person Centred Care Jane Dernie/
Sandra Gourlay X
Workforce Plan Alison Wood X This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held
6
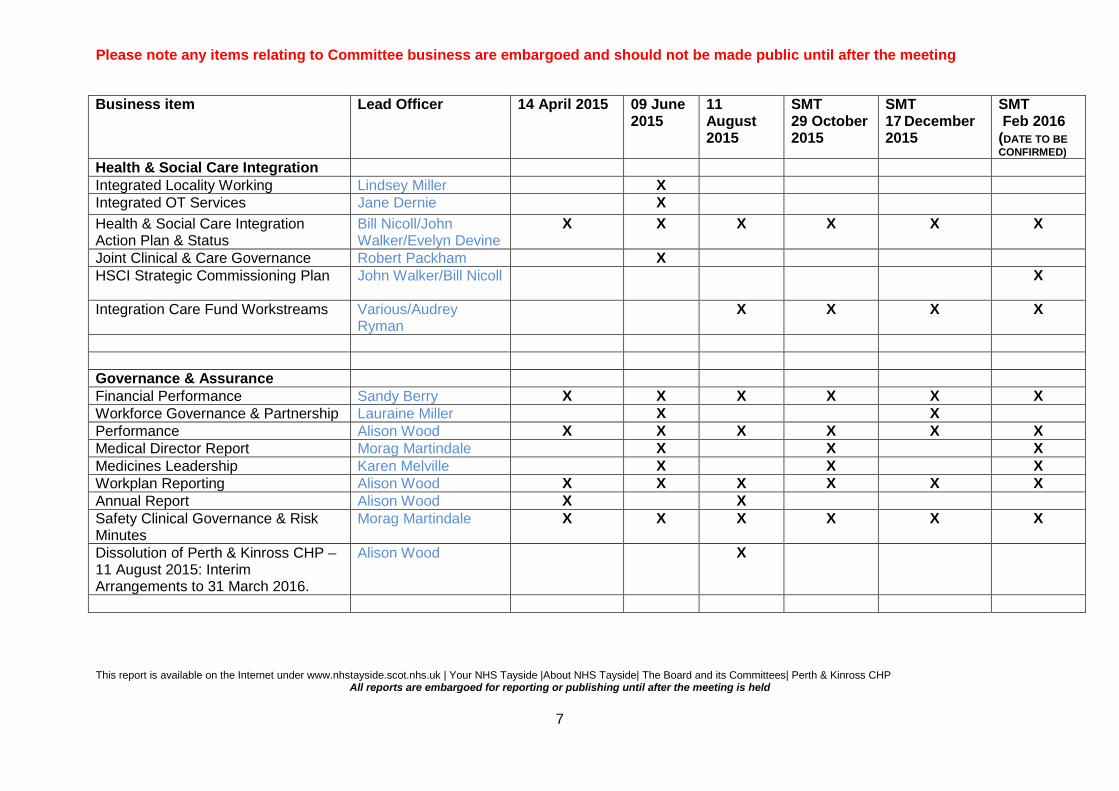
Please note any items relating to Committee business are embargoed and should not be made public until after the meeting
Business item Lead Officer 14 April 2015 09 June 2015
11 August 2015
SMT 29 October 2015
SMT 17 December 2015
SMT Feb 2016 (DATE TO BE CONFIRMED)
Health & Social Care Integration Integrated Locality Working Lindsey Miller X Integrated OT Services Jane Dernie X Health & Social Care Integration Action Plan & Status
Bill Nicoll/John Walker/Evelyn Devine
X X X X X X
Joint Clinical & Care Governance Robert Packham X HSCI Strategic Commissioning Plan John Walker/Bill Nicoll X
Integration Care Fund Workstreams Various/Audrey Ryman
X X X X
Governance & Assurance Financial Performance Sandy Berry X X X X X X Workforce Governance & Partnership Lauraine Miller X X Performance Alison Wood X X X X X X Medical Director Report Morag Martindale X X X Medicines Leadership Karen Melville X X X Workplan Reporting Alison Wood X X X X X X Annual Report Alison Wood X X Safety Clinical Governance & Risk Minutes
Morag Martindale X X X X X X
Dissolution of Perth & Kinross CHP – 11 August 2015: Interim Arrangements to 31 March 2016.
Alison Wood X
This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP All reports are embargoed for reporting or publishing until after the meeting is held
7

Please note any items relating to Committee business are embargoed and should not be made public until after the meeting
Record of Attendance Perth & Kinross CHP Committee 2015/16 NHS Tayside Item 8.1 11 August 2015
NAME DESIGNATION Meeting Date
Meeting Date
Meeting Date
14 April 2015
9 June 2015
11 August 2015
Members Mr Arthur Andrews PPG Group Member P A Dr Morag Curnow Clinical Dental Director A P Mrs Jane Dernie Head of AHPs P P Mrs Evelyn Devine Lead Officer P A Councillor Dave Doogan
Perth & Kinross Council A A
Mrs Linda Dunion Chair, Perth & Kinross CHP P P Mr Ian Duncan Community Pharmacist P P Mr Jim Foulis Interim Associate Nurse Director A P Mr Bob Gillespie Voluntary Services Representative A A Mrs Sandra Gourlay Interim Lead Nurse P P Dr John Harper Consultant A A Councillor Kate Howie
Perth & Kinross Council P A
Dr Neil McLeod General Practitioner P P A Mr Raymond Marshall
Partnership Forum Representative A A
Dr Morag Martindale Clinical Director P P Mr Bill Nicoll Director of Community & Primary Care
Services P A
Mrs Maureen Summers
Carers Representative P P
Mrs Sheila Tunstall-James
Vice Chairperson P P
Mr John Walker Executive Director (Housing and Community Care)
A A
1 This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held

Please note any items relating to Committee business are embargoed and should not be made public until after the meeting
Record of Attendance Perth & Kinross CHP Committee 2015/16 NHS Tayside Item 8.1 11 August 2015
NAME DESIGNATION Meeting Date
Meeting Date
Meeting Date
14 April 2015
9 June 2015
11 August 2015
Advisors Mr Sandy Berry Accountant, NHS Tayside P P Mr Christopher Smith Head of HR, Perth & Kinross CHP A P A Attendees Mrs Karen Melville Pharmacy Team Leader A P Miss Alison Wood Head of Corporate Services P P Mrs Valerie Aitken Corporate Services/Business Support Manager P P Mr Paul Henderson Perth & Kinross Council P Mrs Grace Gilling Service Manager, Perth & Kinross Adult Mental
Health Services P
Aileen Tarditio Unified Communications Manager, eHealth Directorate
P
Miss Lauraine Miller HR Business Lead, NHS Tayside P Mr John Gilruth Depute Director Housing & Community Care,
Perth & Kinross Council P
Rob Packham Associate AHP Director P Chris Lamont Head of Nursing, Community Nursing P Julieann Flynn Head of Children, Young People and Famlies
Service P
Lauraine Miller HR Business Lead P Maggie Rapley Service Manager Psychiatry of Old Age P Hong Zhang Voluntary Services P Iain Smillie Angela Cunningham Lindsey Miller Lorraine Marshall 2 This report is available on the Internet under www.nhstayside.scot.nhs.uk | Your NHS Tayside |About NHS Tayside| The Board and its Committees| Perth & Kinross CHP
All reports are embargoed for reporting or publishing until after the meeting is held