Perspectives on Modern Orthopaedics Locking... · 2018. 3. 4. · using conventional implants...
8
Innovations in Locking Plate Technology George J. Haidukewych, MD Abstract The philosophy and techniques of open reduction and internal fixation of frac- tures have evolved during the past sev- eral decades. 1-3 To achieve functional rehabilitation of the limb, anatomic re- duction, rigid internal fixation, and early joint motion historically were stressed. 1-3 Although constructs were quite stable biomechanically, healing often was delayed because of the ex- tent of soft-tissue dissection and bony devascularization required. Indirect reduction was introduced in the 1980s by Mast et al 4 and others 5,6 in an at- tempt to decrease surgical dissection by relying on ligamentotaxis, blind re- positioning of fragments, reduction aids such as the femoral distractor, and other methods to maintain soft-tissue integ- rity and preserve bony perfusion. Ad- ditionally, plates were redesigned to limit contact with the underlying bone and further preserve bony vascular- ity. 2 In the 1990s, Krettek et al 7 pop- ularized minimally invasive percuta- neous plate osteosynthesis techniques using conventional implants placed through small incisions and submus- cular tunnels. Cadaveric studies dem- onstrated better preservation of pe- riosteal vasculature with these minimally invasive methods than with standard open exposures for internal fixation. 8 As part of the continued de- velopment of biologically friendly plat- ing, and to facilitate minimally inva- sive plating techniques, the use of plates that allow screws to lock into the plate to create a fixed-angle construct is gain- ing popularity. Understanding the bio- mechanics of these devices is neces- sary to appreciate fully the current indications, clinical results, and com- plications of locking plate technology. Historical Perspective Certain periarticular fractures, such as the comminuted distal femoral frac- ture, historically have been difficult to treat. The distal fragment is short, and options for fixation often are lim- ited because of the concurrent pres- ence of lag screws or coronal fracture planes. Any internal fixation device must provide coronal plane stability to maintain correct alignment during healing. Several 95° fixed-angle devic- es, such as the blade plate or dynam- ic condylar screw, have been used suc- cessfully to manage such injuries; however, these devices cannot be used in all situations. This shortcoming ne- cessitated the development of other methods to achieve fixed-angle or “locked” internal fixation constructs. Early attempts to gain angular sta- bility of conventional screws placed through commercially available plates led to the development of the Schuhli nut (Synthes, Paoli, PA). 9 This device, essentially a threaded wash- er, served two purposes: it allowed screws to lock to the plate, therefore preventing screw toggle, and it lim- ited the contact of the plate with the underlying bone in an attempt to pre- serve periosteal perfusion. The results of biomechanical studies and clinical series have documented the im- proved stability and clinical utility of Dr. Haidukewych is an Orthopaedic Traumatol- ogist, Tampa General Hospital and Florida Or- thopedic Institute, Tampa, FL. Dr. Haidukewych or the department with which he is affiliated serves as a consultant to or is an employee of DePuy, a Johnson & Johnson Com- pany. Reprint requests: Dr. Haidukewych, Florida Orthopedic Institute, 13020 Telecom Parkway, Temple Terrace, FL 33637. Copyright 2004 by the American Academy of Orthopaedic Surgeons. Plating techniques remain the mainstay for managing most periarticular and se- lected long bone fractures. However, movement toward more biologically appropri- ate plating techniques is occurring in an attempt to minimize soft-tissue stripping, decrease the need for bone grafting, and improve union rates. Internal fixation with locking plates creates a toggle-free, fixed-angle construct. Early data on the biome- chanical and clinical performance of these implants are encouraging. Current in- dications for locked plating include periarticular fractures, typically those with me- taphyseal comminution. Although impressive union rates have been reported, malunion remains a concern, especially when percutaneous techniques are used. Fur- ther clinical and biomechanical research on locking plate technology is needed to define its place fully alongside existing technology in orthopaedic trauma. J Am Acad Orthop Surg 2004;12:205-212 Perspectives on Modern Orthopaedics Vol 12, No 4, July/August 2004 205
Transcript of Perspectives on Modern Orthopaedics Locking... · 2018. 3. 4. · using conventional implants...

Innovations in Locking Plate Technology
George J. Haidukewych, MD
Abstract
The philosophy and techniques of openreduction and internal fixation of frac-tures have evolved during the past sev-eral decades.1-3 To achieve functionalrehabilitation of the limb, anatomic re-duction, rigid internal fixation, andearly joint motion historically werestressed.1-3 Although constructs werequite stable biomechanically, healingoften was delayed because of the ex-tent of soft-tissue dissection and bonydevascularization required. Indirectreduction was introduced in the 1980sby Mast et al4 and others5,6 in an at-tempt to decrease surgical dissectionby relying on ligamentotaxis, blind re-positioningof fragments, reductionaidssuch as the femoral distractor, and othermethods to maintain soft-tissue integ-rity and preserve bony perfusion. Ad-ditionally, plates were redesigned tolimit contact with the underlying boneand further preserve bony vascular-ity.2 In the 1990s, Krettek et al7 pop-ularized minimally invasive percuta-neous plate osteosynthesis techniquesusing conventional implants placedthrough small incisions and submus-
cular tunnels. Cadaveric studies dem-onstrated better preservation of pe-riosteal vasculature with theseminimally invasive methods than withstandard open exposures for internalfixation.8 As part of the continued de-velopment of biologically friendly plat-ing, and to facilitate minimally inva-sive plating techniques, the use of platesthat allow screws to lock into the plateto create a fixed-angle construct is gain-ing popularity. Understanding the bio-mechanics of these devices is neces-sary to appreciate fully the currentindications, clinical results, and com-plications of locking plate technology.
Historical Perspective
Certain periarticular fractures, suchas the comminuted distal femoral frac-ture, historically have been difficultto treat. The distal fragment is short,and options for fixation often are lim-ited because of the concurrent pres-ence of lag screws or coronal fractureplanes. Any internal fixation device
must provide coronal plane stabilityto maintain correct alignment duringhealing. Several 95° fixed-angle devic-es, such as the blade plate or dynam-ic condylar screw, have been used suc-cessfully to manage such injuries;however, these devices cannot be usedin all situations. This shortcoming ne-cessitated the development of othermethods to achieve fixed-angle or“locked” internal fixation constructs.
Early attempts to gain angular sta-bility of conventional screws placedthrough commercially availableplates led to the development of theSchuhli nut (Synthes, Paoli, PA).9 Thisdevice, essentially a threaded wash-er, served two purposes: it allowedscrews to lock to the plate, thereforepreventing screw toggle, and it lim-ited the contact of the plate with theunderlying bone in an attempt to pre-serve periosteal perfusion. The resultsof biomechanical studies and clinicalseries have documented the im-proved stability and clinical utility of
Dr. Haidukewych is an Orthopaedic Traumatol-ogist, Tampa General Hospital and Florida Or-thopedic Institute, Tampa, FL.
Dr. Haidukewych or the department with whichhe is affiliated serves as a consultant to or is anemployee of DePuy, a Johnson & Johnson Com-pany.
Reprint requests: Dr. Haidukewych, FloridaOrthopedic Institute, 13020 Telecom Parkway,Temple Terrace, FL 33637.
Copyright 2004 by the American Academy ofOrthopaedic Surgeons.
Plating techniques remain the mainstay for managing most periarticular and se-lected long bone fractures. However, movement toward more biologically appropri-ate plating techniques is occurring in an attempt to minimize soft-tissue stripping,decrease the need for bone grafting, and improve union rates. Internal fixation withlocking plates creates a toggle-free, fixed-angle construct. Early data on the biome-chanical and clinical performance of these implants are encouraging. Current in-dications for locked plating include periarticular fractures, typically those with me-taphyseal comminution. Although impressive union rates have been reported,malunion remains a concern, especially when percutaneous techniques are used. Fur-ther clinical and biomechanical research on locking plate technology is needed todefine its place fully alongside existing technology in orthopaedic trauma.
J Am Acad Orthop Surg 2004;12:205-212
Perspectives on Modern Orthopaedics
Vol 12, No 4, July/August 2004 205

these devices in managing difficultnonunions and malunions.10
A locking plate prototype devel-oped by Koval et al,11 consisting ofthreaded nuts welded to the distal as-pect of a condylar buttress plate (Syn-thes), was intended to improve thefixation stability of distal femoral frac-tures in elderly patients. In a cadav-eric model, the authors documentedthe biomechanical superiority of thislocked construct over an identical butunlocked plate as well as over a 95°fixed-angle blade plate.11 Concurrentplate designs continued to minimizethe contact between the undersurfaceof the plate and the bone. The pointcontact fixator device (PC-Fix; Syn-thes) incorporates unicortical screwsthat lock into a plate using a Morsecone mismatch that prevents screwtoggle as the screws are tightened tothe plate.12 The undersurface of theplate is undercut to allow minimalpoints of contact with the bone, fur-ther reducing bony devasculariza-tion.13 Initial biomechanical testingand a recent prospective randomizedclinical trial revealed no significantdifference between the performanceof the PC-Fix and conventional bicor-tical plate constructs.14,15
Multiple European clinical serieshave documented high union ratesand low complication rates using thePC-Fix for fractures of the fore-arm.16,17 Locking plate technologyalso has been used successfully inboth oral maxillofacial surgery andspine surgery, where stability is re-quired without bicortical screw pur-chase.18,19 Success with such devicesled to the development of anatomi-cally precontoured locking plates de-signed primarily for periarticularfractures of the lower extremity, forwhich fixed-angle stability is fre-quently desirable because of me-taphyseal comminution.
The development of locking plateshas resulted in relatively unusual fix-ation constructs of long plates that usefew, often unicortical, screws. Under-standing the design rationale and po-
tential clinical applications of suchunconventional plates requires a ba-sic understanding of the biomechan-ics of plate fixation.
Biomechanics
The aspects of load transmissionacross a fracture stabilized with alocking screw plate device have notbeen studied; however, comparisonto existing devices demonstrates thetheoretical, practical, and compara-tive advantages of the locking plate.To understand this comparison re-quires an appreciation of the conceptsof working length, mechanics of stan-dard plate stability, and the effect ofcantilever bending.
The working length of a plate-boneconstruct is defined as the length ofplate unsupported by bone becauseof comminution, segmental bone loss,or other reasons.4 Bridge plates spanlarge areas of comminution and thustypically have long working lengths.4
Although biologically advantageousbecause they help preserve soft tis-sue, such constructs are often at a me-chanical disadvantage, especially whenthey are used for periarticular inju-ries, a common application. These frac-tures frequently have short periarticu-lar fragments and long workinglengths; the result is coronal planeinstability and consequent collapsewhen standard nonlocking plates areused.1,4,20,21 To avoid this, a fixed an-gle must be provided between the plateand the fixation into the periarticu-lar segment. This can be achieved with95° fixed-angle devices. The lockingscrew-plate design facilitates a sim-ilar mechanical advantage with mul-tiple points of screw fixation. This ismost important in fractures with longworking lengths, short periarticularsegments, and the absence of bony sup-port on the side of the fracture oppo-site the plate.
When standard bicortical screws areapplied through a plate, the tighten-ing of the screws compresses the plate
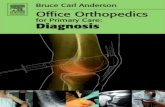
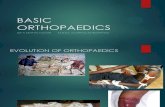
onto the bone. The stability of this con-struct results from friction between theundersurface of the plate and thebone22,23 (Fig. 1,A). Because the screwsare free to toggle in the plate, stabil-ity requires bicortical purchase of thesescrews. However, with a locking plateconstruct, threads on the screw headlock into corresponding threads on thescrew hole of the plate (Fig. 2), elim-inating toggle. The forces are trans-ferred from the bone to the plate acrossthe screw-plate threaded connec-tion22,23 (Fig. 1, B). Compression of theplate to the underlying bone thereforeis not required to achieve constructstability, and the blood supply to thebone directly under the plate is pre-served. Accordingly, bicortical pur-chase is less important than with non-locking plates. Avoiding bicorticaldrilling also theoretically minimizesfurther damage to the endosteal cir-culation and may decrease the risk ofrefracture after plate removal.22 Cur-rent locking plate designs have usedself-tapping unicortical screws (PC-Fix,Less Invasive Stabilization System[LISS]; Synthes); this has eliminatedthe need to measure the length for per-cutaneous screw insertion, has de-creased inventory, and has minimizedsurgical time.
Full understanding of the mechan-ics of locking plates and unicorticalscrews requires an appreciation of theprevailing forces these fixation con-structs must withstand in differentanatomic regions of a bone. Bonequality is less dense in the metaphy-sis than in the diaphysis. Therefore,locked screws usually are placed inlong rows perpendicular to the ap-plied load and the limb axis. When,in a medial bony defect, a cantileverbending force is applied, the screwsfunction like small blade plates, re-sisting the bending moment. Underthe same circumstances, standardscrew-plate fixation allows toggle andthus progressive varus deformity. Inthe diaphysis, locked screws also canbe inserted perpendicular to the ax-ial load, but they are then more com-
Innovations in Locking Plate Technology
206 Journal of the American Academy of Orthopaedic Surgeons

monly loaded in shear, similar to theprevailing conditions when half pinsare inserted for external fixation.22
The pullout strength of a unicor-tical locked screw is about 60% thestrength of a standard bicorticalscrew.20,22 In fact, a locked screw-plateconstruct can be thought of as being
similar to an implanted external fix-ator. Studies of the biomechanics ofmonolateral external fixation haveshown improved stability of constructsthat incorporate wide spacing of halfpins and placement of the connect-ing bar as close to the bone as pos-sible.24 Alocking plate construct mightbe considered the ultimate external fix-ator, with minimal soft-tissue dissec-tion, wide screw spacing, lockedscrews, and the plate functioning asthe connecting bar, placed extremelyclose to the mechanical axis of thebone. Although a direct comparisonhas not been made, the ability to movethe plate closer to the mechanical axisshould markedly increase stabilitycompared with a monolateral exter-nal fixator, in which the bar is far fromthe limb axis, creating a large bend-ing moment.
Few biomechanical studies havebeen published that compare currentlocking plate designs to convention-al implants.11,14,17 One recent studycompared the LISS distal femoral
plate to the 95° angled blade plate anda retrograde nail in osteoporotic ca-daveric specimens; the LISS was bio-mechanically superior in axial cata-strophic load to failure testing.25 Martiet al26 compared the LISS distal fem-oral plate to the dynamic condylarscrew and the unlocked condylar but-tress plate; the LISS demonstrated su-perior ability to resist applied loadsand had less irreversible deformation.Although limited, these early biome-chanical studies demonstrate thatlocking plates can provide stabilitycomparable or superior to currentcommercially available fixed-angledevices.
Indications andTechniques
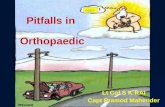
The current indications for lockingplate fixation are complex periartic-ular fractures, especially those withcomminution of the metaphyseal re-gion. Comminuted distal femoralfractures with multiplanar articularinvolvement are excellent indica-tions27 (Figs. 3 and 4). Locking platesallow the surgeon more options forfixed-angle fixation while avoidingpreviously placed lag screws or frac-ture lines, such as the coronal (Hoffa)fracture of the distal femur.20 In thepast, these obstacles sometimes pre-cluded the use of traditional fixed-angle devices, such as the blade plateor the dynamic condylar screw.28 Bi-condylar tibial plateau fractures, inwhich coronal plane stability is re-quired, may benefit from this type offixation29 (Fig. 5). In some patients,use of a lateral locking plate is analternative to double-plating tech-niques. Locked plating also may pro-vide an alternative to external fixa-tion, thus minimizing associatedcomplications such as pin-site infec-tion and patient tolerance. The impor-tance of anatomic reduction of the ar-ticular surface with lag screw fixationremains paramount. The metaphy-seal comminution is then “bridged”
Figure 1 A, Stability of a conventional plate-and-screw construct relies on friction betweenthe undersurface of the plate and the underlying bone (arrows). This is augmented by bi-cortical screw purchase, which also decreases toggle between the screw and plate hole (rep-resented by the rectangles). B, With a locked plate and screw construct, no screw toggle canoccur (arrows). Bicortical fixation and contact between the plate and the underlying bone(represented by the rectangles) is not required for stability. (Adapted with permission fromAppenzeller A, Christensen R, Frenk A, Gilbert S, Schavan R: The development of the distalfemur LISS. Injury 2001;32[suppl 3]:5-25.)
Figure 2 Corresponding threads on thescrew head and the plate hole eliminate screwtoggle when the screw is tightened, creatinga fixed-angle or “locked” screw. (Courtesy ofSynthes, Paoli, PA.)
George J. Haidukewych, MD
Vol 12, No 4, July/August 2004 207

by the plate with locked screw fixa-tion of the articular segment and witheither locked or conventional bicor-tical screw fixation of the diaphysealsegment20 (Figs. 3 through 5). Greatcare is taken to preserve soft-tissue in-tegrity, and therefore bony viability,in the metaphyseal region, regardlesswhether an open or a percutaneoussubmuscular plate application tech-nique is chosen.
Other potential indications forlocking plate technology includeperiprosthetic fractures involving to-tal knee arthroplasty.30-32 Retrogradeintramedullary fracture fixation is dif-ficult to use with posterior cruciateligament–substituting total knee ar-throplasty designs because of theclosed femoral housing. Lugs, stems,or other portions of the femoral com-ponent also may preclude the use offixed-angle devices, such as the bladeplate or dynamic condylar screw.Locking plates afford fixed-angle sta-bility and permit the use of multipledistal locked screws, which often canbe inserted around such obstacles andprovide stable distal fixation even forvery short distal fragments.
In some series, extra-articular orsimple intra-articular fractures of thedistal femur and proximal tibia withshort periarticular fragments have
demonstrated unacceptable rates ofmalalignment with intramedullarynailing.33,34 The use of locked platingconstructs may provide improved fix-ation in these patients and result inless malalignment. If intramedullarynailing cannot be used for selectedlong-bone fractures with long work-ing lengths, a bridge plate techniquewith locked screw fixation may be aviable alternative. Other evolving ap-plications for locking plate technol-ogy include fixation of corrective os-teotomies, malunions, and nonunions,as well as applications for orthopaediconcology and other difficult fractures,such as the comminuted proximal hu-merus and distal radius; however,published clinical data for these ap-plications are currently lacking.
Disadvantages andComplications
Several potential disadvantages oflocking plate fixation exist. Whentightening the screws, the surgeon has
Figure 3 A, Anteroposterior radiograph of a comminuted distal femoral fracture. B, Healedfracture treated with a locked distal femoral plate. Note slight valgus malalignment. (Cour-tesy of Synthes, Paoli, PA.)
Figure 4 A, Anteroposterior radiograph of a comminuted open distal femoral fracture sta-bilized with temporary external fixation. B, Healed fracture. Note multiplanar lag screwsused for articular reduction and bridging of metaphyseal comminution. (Courtesy of Syn-thes, Paoli, PA.)
Innovations in Locking Plate Technology
208 Journal of the American Academy of Orthopaedic Surgeons

no tactile feedback as to the qualityof screw purchase into the bone. Be-cause they lock into the plate, allscrews abruptly stop advancingwhen the threads are completely seat-ed into the plate, regardless of bonequality. In addition, current lockingplate designs can be used to maintainfracture reduction but not to obtainit. This is in sharp contrast to tradi-tional techniques of internal fixationusing blade plates or dynamic condy-lar screws, in which the 95° angle ofthe implant can be used as a reduc-tion aid.5,6,20 For example, for the com-plex distal femoral fracture, the dis-tal fragment can be prepared to accepta dynamic condylar lag screw or ablade plate by placing the implant ex-actly parallel to the knee joint.35 Whenthe side plate is applied, limb align-ment will be correct.1,3 With currentlocking plate designs, the fracturemust be reduced and the limb align-ment, length, and rotation must be setproperly before placement of any
locked screws.20 Once a locked screwis placed above and below a fractureline, no further reduction adjustmentis possible unless the screws are com-pletely removed. Locked screws willnot “pull” the plate down to bone.This lack of construct reduction ca-pability, combined with percutaneousplating techniques, can result in high-er rates of fracture malalignment thanoccur with formal open reduction andinternal fracture fixation.36 New tech-niques are evolving to facilitate theaccuracy of closed reduction of suchdifficult fractures. Surgeons contem-plating a percutaneous approachshould be experienced in convention-al open techniques and be cognizantof the differences.
Another concern is the rigidity ofa locked screw plate construct. For ex-ample, in diaphyseal or metadiaphy-seal areas, any fracture distraction atthe time of reduction or fracture re-sorption during healing will be heldrigidly by such constructs and may
potentially result in delayed union ornonunion. In this situation, no loadsharing can occur with locked screwson either side of a fracture. If the frac-ture is repetitively loaded, the plateeventually may fracture or fixationmay be lost. Because of these concernsand the additional cost of a lockingplate compared with an equivalentbut nonlocking plate, locking platesprobably should be used selectivelyfor fractures that have demonstratedhigh failure rates with conventionalplating techniques.
Another disadvantage of currentlocking plate design is the inabilityof the surgeon to alter the angle of thescrew within the hole and still achievea locked screw. The use of certainscrew holes in the plate potentiallycould be blocked by lag screws placedfor articular reduction, unique frac-ture geometry, anatomic variations, orimplanted components of a joint ar-throplasty. Any attempt to contourlocked plates could potentially distort
Figure 5 A, Anteroposterior radiograph of a comminuted tibial plateau fracture. B, Postoperative radiograph after internal fixation witha locked tibial plate. C, Healed fracture at 1-year follow-up. (Courtesy of Synthes, Paoli, PA.)
George J. Haidukewych, MD
Vol 12, No 4, July/August 2004 209

the screw holes and adversely affectscrew purchase.11 Newer develop-ments have focused on plates with so-called polyaxial locking screws to ad-dress this concern (eg, Versalock,DePuy, Warsaw, IN).Abushing insidethe plate hole expands because ofhoop stresses as the screw is tight-ened, thereby allowing freedom ofscrew angulation and the mechanicalbenefits of a locking screw. Clinicaldata on this technology, however, arecurrently lacking.
When using locking plates, hard-ware removal may be more difficult,especially if locked screws becomecold-welded to the plate. Current sys-tems offer torque-limiting screwdriv-ers that may minimize this concern.
Clinical Experience
Most published clinical studies oflocking plate fixation have focused onthe results of the LISS plate in frac-tures of the distal femur and proxi-mal tibia. This device is an externallytargeted plate designed for submus-cular, extraperiosteal application,with all screws locking to the plate.In one prospective trial that encom-passed nine European trauma cen-ters, 112 patients with 116 fracturesof the distal femur were treated.37
Ninety-six patients with 99 fracturescompleted the study (mean follow-up, 14 months). Twenty-nine percentof fractures were open; 91% of frac-tures healed. Six patients requiredbone grafting to achieve union, andfour infections were reported. Aver-age knee flexion at union was 107°.Deviations >5° from normal coronalor sagittal alignments were noted onapproximately 40% of postoperativeradiographs.
In a series of 66 patients with frac-tures of the distal femur treated withthe LISS plate, all fractures healed
without loss of distal femoral fixa-tion.27 Only three fractures (5%) re-quired bone grafting to achieveunion. Three patients (5%) had mala-lignments ≥5° in any plane. In anoth-er study, 54 fractures of the distal fe-mur were treated with the LISS distalfemoral plate.28 Four had loss of prox-imal fixation, attributed to errors insurgical technique resulting in im-plant misplacement on the femoraldiaphysis. Two infections and threedelayed unions were reported. Of the27 patients that completed a mini-mum 1-year follow-up, 20 (74%) hadgood or excellent results; 7 (26%) hadalignment deviations >5° in anyplane.
When the femoral LISS was usedfor 13 periprosthetic fractures abovetotal knee arthroplasties, only onepatient required bone grafting toachieve union.32 No cases of varuscollapse or distal fixation failure werenoted. In another study, 46 complexintra-articular and extra-articularfractures of the proximal tibia (45 pa-tients) were treated with the tibialLISS plate.29 Of the 16 open fractures,there was one infection. One patientrequired bone grafting to achieveunion, and no varus collapse or lossof proximal fixation was reported. Sixof the 46 fractures (13%) had mala-lignment ≥5°. Gosling et al38 and Ertland Smith39 reported encouraging re-sults using lateral locked plating asan alternative to double plating in bi-condylar tibial plateau fractures.
An obvious interdependence hasdeveloped between locked internalfixation technology and minimally in-vasive techniques of plate applica-tion.Although impressive union rateshave been reported, this may be theresult of improved soft-tissue han-dling techniques, a favorable biolog-ic environment, and the improvedmechanical stability provided bylocking plate technology. Additional-
ly, it appears that unicortical fixationis adequate to achieve union; in theabsence of errors in surgical tech-nique, reported rates of fixation fail-ure are very low. When percutaneoustechniques are used, malalignmentsare more common, and the surgeriesremain technically demanding.33
With increased experience and the de-velopment of new techniques to im-prove the accuracy of closed reduc-tion, the frequency of such malunionsshould decrease. The long-term clin-ical significance of this malalignmentremains unknown.
Summary
Initial clinical data demonstrate ex-cellent union rates, low rates of fix-ation failure, and few associated com-plications with the use of lockingplates for internal fixation of frac-tures, particularly periarticular frac-tures. Locking plate technology willundoubtedly proliferate for fracturesin other anatomic locations. Hybridplates offering the versatility ofchoosing either a locked or unlockedscrew will probably enjoy wide-spread use. The clinical success ofthese implants is likely the result ofthe improved biologic environmentprovided by minimally invasive plateinsertion as well as the stable mechan-ical environment. As with all newtechnology, caution is warranted. Be-cause these implants are used for dif-ficult fractures, complications bothold (eg, malalignment, infection) andnew (eg, difficult hardware removal,misplaced screws, pullout) will occur.When such plates are inserted percu-taneously, malalignment is common.Further clinical and biomechanical re-search on locking plate technology isneeded to fully define its place along-side existing technology in ortho-paedic trauma.
Innovations in Locking Plate Technology
210 Journal of the American Academy of Orthopaedic Surgeons

References1. Stover M: Distal femoral fractures: Cur-
rent treatment, results and problems.Injury 2001;32(suppl 3):SC3-SC13.
2. Perren SM: Evolution and rationale oflocked internal fixator technology: Intro-ductory remarks. Injury 2001;32(suppl 2):B3-B9.
3. Schatzker J: Changes in the AO/ASIFprinciples and methods. Injury 1995;26(suppl 2):B51-B56.
4. Mast J, Jakob R, Ganz R (eds): Planningand Reduction Technique in Fracture Sur-gery. Berlin, Germany: Springer-Verlag,1989.
5. Bolhofner BR, Carmen B, Clifford P:The results of open reduction and inter-nal fixation of distal femur fractures us-ing a biologic (indirect) reduction tech-nique. J Orthop Trauma 1996;10:372-377.
6. Ostrum RF, Geel C: Indirect reductionand internal fixation of supracondylarfemur fractures without bone graft.J Orthop Trauma 1995;9:278-284.
7. Krettek C, Müller M, Miclau T: Evolu-tion of minimally invasive plate osteo-synthesis (MIPO) in the femur. Injury2001;32(suppl 3):SC14-SC23.
8. Farouk O, Krettek C, Miclau T, Schan-delmaier P, Guy P, Tscherne H: Mini-mally invasive plate osteosynthesis:Does percutaneous plating disruptfemoral blood supply less than the tra-ditional technique? J Orthop Trauma1999;13:401-406.
9. Kolodziej P, Lee FS, Patel A, et al: Bio-mechanical evaluation of the Schuhlinut. Clin Orthop 1998;347:79-85.
10. Kassab SS, Mast JW, Mayo KA: Patientstreated for nonunions with plate andscrew fixation and adjunctive lockingnuts. Clin Orthop 1998;347:86-92.
11. Koval KJ, Hoehl JJ, Kummer FJ, SimonJA: Distal femoral fixation: A biome-chanical comparison of the standardcondylar buttress plate, a locked but-tress plate, and the 95-degree bladeplate. J Orthop Trauma 1997;11:521-524.
12. Perren SM, Buchanan JS: Basic conceptsrelevant to the design and developmentof the Point Contact Fixator (PC-Fix).Injury 1995;26(suppl 2):B1-B4.
13. Hofer HP, Wildburger R, SzyszkowitzR: Observations concerning differentpatterns of bone healing using the PointContact Fixator (PC-Fix) as a new tech-nique for fracture fixation. Injury 2001;32(suppl 2):B15-B25.
14. Leung F, Chow SP: A prospective, ran-domized trial comparing the limitedcontact dynamic compression platewith the point contact fixator for fore-
arm fractures. J Bone Joint Surg Am 2003;85:2343-2348.
15. Tepic S, Perren SM: The biomechanicsof the PC-Fix internal fixator. Injury1995;26(suppl 2):B5-B10.
16. Haas N, Hauke C, Schütz M, Kääb M,Perren SM: Treatment of diaphysealfractures of the forearm using the PointContact Fixator (PC-Fix): Results of 387fractures of a prospective multicentricstudy (PC-Fix II). Injury 2001;32(suppl2):B51-B62.
17. Miclau T, Remiger A, Tepic S, LindseyR, McIff T: A mechanical comparison ofthe dynamic compression plate, limitedcontact-dynamic compression plate,and point contact fixator. J Orthop Trau-ma 1995;9:17-22.
18. Herford AS, Ellis E III: Use of a lockingreconstruction bone plate/screw sys-tem for mandibular surgery. J Oral Max-illofac Surg 1998;56:1261-1265.
19. Richter M, Wilke HJ, Kluger P, Claes L,Puhl W: Biomechanical evaluation of anewly developed monocortical expan-sion screw for use in anterior internal fix-ation of the cervical spine: In vitro com-parison with two established internalfixation systems. Spine 1999;24:207-212.
20. Kregor PJ: Distal femur fractures withcomplex articular involvement: Man-agement by articular exposure and sub-muscular fixation. Orthop Clin NorthAm 2002;33:153-175.
21. Jazrawi LM, Kummer FJ, Simon JA, etal: New technique for treatment of un-stable distal femur fractures by lockeddouble-plating: Case report and biome-chanical evaluation. J Trauma 2000;48:87-92.
22. Frigg R, Appenzeller A, Christensen R,Frenk A, Gilbert S, Schavan R: The de-velopment of the distal femur Less In-vasive Stabilization System (LISS). Inju-ry 2001;32(suppl 3):SC24-SC31.
23. Frigg R: Locking Compression Plate(LCP): An osteosynthesis plate basedon the Dynamic Compression Plate andthe Point Contact Fixator (PC-Fix). In-jury 2001;32(suppl 2):B63-B66.
24. Behrens F, Johnson W: Unilateral exter-nal fixation: Methods to increase andreduce frame stiffness. Clin Orthop1989;241:48-56.
25. Zlowodzki M, Williamson RS, ZardiackasLD, Kregor PJ: Biomechanical evaluationof the less invasive stabilization system,angled blade plate, and retrograde in-tramedullary nail for the fixation of dis-tal femur fractures: An osteoporotic ca-daveric model, in Orthopaedic Trauma
Association 18th Annual Meeting Final Pro-gram. Rosemont, IL: Orthopaedic Trau-ma Association, 2002, pp 178-179.
26. Marti A, Fankhauser C, Frenk A, Cor-dey J, Gasser B: Biomechanical evalua-tion of the less invasive stabilizationsystem for the internal fixation of distalfemur fractures. J Orthop Trauma 2001;15:482-487.
27. Kregor PJ, Stannard J, Zlowodzki M,Cole PA, Alonso J: Distal femoral frac-ture fixation utilizing the Less InvasiveStabilization System (LISS): The tech-nique and early results. Injury 2001;32(suppl 3):SC32-SC47.
28. Schandelmaier P, Partenheimer A, Koen-emann B, Grün OA, Krettek C: Distal fem-oral fractures and LISS stabilization. In-jury 2001;32(suppl 3):SC55-SC63.
29. Cole PA, Kregor PJ: Prospective clinicaltrial of the less invasive stabilizationsystem (LISS) for proximal tibia frac-tures, in Orthopaedic Trauma Association16th Annual Meeting Final Program.Rosemont, IL: Orthopaedic Trauma As-sociation, 2000, p 344.
30. Althausen PL, Lee MA, Finkemeier CG,Meehan JP, Rodrigo JJ: Operative stabi-lization of supracondylar femur frac-tures above total knee arthroplasty: Acomparison of four treatment methods.J Arthroplasty 2003;18:834-839.
31. Bong MR, Egol KA, Koval KJ, et al: Com-parison of the LISS and a retrograde-inserted supracondylar intramedullarynail for fixation of a periprosthetic dis-tal femur fracture proximal to a totalknee arthroplasty. J Arthroplasty 2002;17:876-881.
32. Kregor PJ, Hughes JL, Cole PA: Fixationof distal femoral fractures above totalknee arthroplasty utilizing the Less In-vasive Stabilization System (LISS). Inju-ry 2001;32(suppl 3):SC64-SC75.
33. Ricci WM, O’Boyle M, Borrelli J, Bella-barba C, Sanders R: Fractures of the prox-imal third of the tibial shaft treated withintramedullary nails and blocking screws.J Orthop Trauma 2001;15:264-270.
34. Ricci WM, Bellabarba C, Lewis R, et al:Angular malalignment after intramed-ullary nailing of femoral shaft fractures.J Orthop Trauma 2001;15:90-95.
35. Sanders R, Regazzoni P, Ruedi TP: Treat-ment of supracondylar-intracondylarfractures of the femur using the dynam-ic condylar screw. J Orthop Trauma 1989;3:214-222.
36. Collinge CA, Sanders RW: Percutane-ous plating in the lower extremity. J AmAcad Orthop Surg 2000;8:211-216.
George J. Haidukewych, MD
Vol 12, No 4, July/August 2004 211

37. Schütz M, Müller M, Krettek C, et al:Minimally invasive fracture stabiliza-tion of distal femoral fractures with theLISS: A prospective multicenter study.Results of a clinical study with specialemphasis on difficult cases. Injury 2001;32(suppl 3):SC48-SC54.
38. Gosling T, Muller M, Richter M, HufnerT, Krettek C: The less invasive stabili-zation system for bicondylar fractures ofthe proximal tibia, in Orthopaedic TraumaAssociation 18th Annual Meeting Final Pro-gram. Rosemont, IL: Orthopaedic TraumaAssociation, 2002, pp 168-169.
39. Ertl W, Smith DG: Bicondylar tibial pla-teau fractures: Comparison of early re-sults with a locking plate compared withmedial and lateral plating, in OrthopaedicTrauma Association 18th Annual MeetingFinal Program. Rosemont, IL: OrthopaedicTrauma Association, 2002, pp 170-171.
Innovations in Locking Plate Technology
212 Journal of the American Academy of Orthopaedic Surgeons