Personalised omega-3 therapeutics: an update
66
An updated practitioner’s guide to the Opti-O-3 biomarker test Nina Bailey BSc (hons) MSc PhD ANutr
-
Upload
igennus-healthcare-nutrition -
Category
Health & Medicine
-
view
526 -
download
2
Transcript of Personalised omega-3 therapeutics: an update

An updated practitioner’s guide to the Opti-O-3 biomarker test
Nina BaileyBSc (hons) MSc PhD ANutr

What is the Opti-O-3
The importance of determining baseline omega-3 levels
Comparison of laboratories
Reference ranges
How personalised dosing optimises clinical outcomes
How to interpret the results: what the biomarkers mean

Full fatty acid screen (24 fatty acids): Saturated Trans fats Monounsaturated Polyunsaturated
Omega-6 Omega-3
Biomarkers: Omega-3 index Omega-6 to omega-3 ratio AA to EPA ratio

Primary structural function & anti-inflammatory
docosanoid productionResolvins Protectins
Anti-inflammatory eicosanoid production
REDUCED INFLAMMATIONSeries-3 prostaglandinsSeries-3 thromboxanesSeries-5 leukotrienes
Hydroxy fatty acidsResolvins
DHA
Anti-inflammatory eicosanoid production
REDUCED INFLAMMATIONSeries-1 prostaglandinsSeries -1 thromboxanes
DGLA
GLA
LA
EPA
ETA
SDA
ALADelta -6 desaturase
Elongase/desaturaseDelta -5 desaturase
Cyclooxygenase (COX)/lipoxygenase (LOX)
Elongase
Pro-inflammatory eicosanoid production
INFLAMMATIONSeries-2 prostaglandinsSeries-2 thromboxanesSeries-4 leukotrienes
Hydroxy fatty acids
AA
COX/LOX
COX
Pro-resolving Lipoxins
Omega-6 to omega-3 ratio

Resolvins Protectins
Omega-3DHA
ANTI-INFLAMMATORY
Omega-6 DGLA
Omega-3EPA
PRO-INFLAMMATORY
Omega-6AA
Lipoxins Resolvins Protectins
AA to EPA ratio
Omega-3 index
Using fatty acids as biomarkers of health and disease
ANTI-INFLAMMATORY

Greenland Inuit
Japanese Western populations Disease biomarker
Optimal Acceptable Suboptimal Poor
0 1.5 3 7 15 20
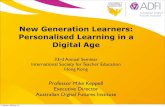
The AA to EPA ratio as a potential biomarker of pro-inflammatory to anti-inflammatory balance

AA to EPA ratio in health and disease
Fasted blood samples from 1432 [Italian] subjects, who were referred by their physicians, were analysed to assess their AA to EPA and total omega-6 to omega-3 ratios in whole blood and in RBC membrane phospholipids
Individuals with no diagnosable conditions had lower AA to EPA ratios than those with diagnosable health conditions
Rizzo AM, Montorfano G, Negroni M, Adorni L, Berselli P, Corsetto P, Wahle K, Berra B A rapid method for determining arachidonic:eicosapentaenoic acid ratios in whole blood lipids: correlation with erythrocyte membrane ratios and validation in a large Italian population of various ages and pathologies. Lipids Health Dis. 2010 Jan 27;9:7.
AA/EPA and omega-6/omega-3 ratios in whole blood of healthy subjects and in a group of patients with various pathologies, with and without consumption of omega-3. Mean ± S.E; Student's t-test: ## p < 0.01 with omega-3 vs without omega-3; ** p < 0.01 pathological vs healthy

AA/EPA ratios in whole blood of patients grouped according to their specific pathologies. The horizontal lines indicate the mean value for all the healthy subjects that do not use omega-3.
Rizzo AM, Montorfano G, Negroni M, Adorni L, Berselli P, Corsetto P, Wahle K, Berra B A rapid method for determining arachidonic:eicosapentaenoic acid ratios in whole blood lipids: correlation with erythrocyte membrane ratios and validation in a large Italian population of various ages and pathologies. Lipids Health Dis. 2010 Jan 27;9:7.
Individuals with allergic, skin and neurodegenerative diseases had higher ratios of AA to EPA compared to the values for subjects with other pathologies, possibly due to a higher turnover of EPA
Subjects who did not take omega-3 supplements and suffered from allergic, neurodegenerative, skin and inflammatory diseases had higher values for AA to EPA ratios than those with the other diseases (heart, metabolic, cancer)

Silva V, Green P, Singer P: Membrane fatty acid composition of different target populations: importance of baseline on supplementation. Clinical Nutrition 2014 33:206
The importance of baseline on supplementation efficacy

Resolvins Protectins
Omega-3DHA
ANTI-INFLAMMATORY
Omega-6 DGLA
Omega-3EPA
PRO-INFLAMMATORY
Omega-6AA
Lipoxins Resolvins Protectins
AA to EPA ratio
Omega-3 index
Combining biomarkers
ANTI-INFLAMMATORY

The Seattle study, the Physicians' Health Study (PHS), the Cardiovascular Health Study (CHS), the Diet and Reinfarction Trial (DART), the study on the prevention of coronary atherosclerosis by intervention with marine omega-3 fatty acids (SCIMO), and the GISSI-Prevenzione study. Taken together, these data suggest a desirable target value for the Omega-3 Index of ≥8% and an undesirable level of ≤4%.
4% 6% 8% 10%
GISSI-P & DART: 9.5%
CHS 8.9%
PHS 3.9%
SCIMO: 3.4%Seattle: 3.3%
SCIMO: 8.3%
PHS: 7.3%Seattle: 6.5%
LEAST PROTECTION GREATEST PROTECTION
Summary of evidence for the proposed cut points for the Omega-3 Index
Harris WS, Von Schacky C: The Omega-3 Index: a new risk factor for death from coronary heart disease? Prev Med 2004, 39:212-220.

The relative risk for sudden cardiac death (RR SCD) by quartile of the Omega-3 Index compared to other, more traditional blood-borne risk factors.
Only two risk factors demonstrated statistically significant trends: C-reactive protein and the Omega-3 Index
With the relative risk reduced by approximately 90% in the highest quartiles, the Omega-3 Index is both a strong and an independent predictor of risk for sudden cardiac death.
CRP = C-reactive protein; Hcy = homocysteine; TC = total cholesterol; LDL = low density lipoprotein cholesterol; HDL = high density lipoprotein cholesterol; Tg = triglycerides; n-3 Index = Omega-3 Index.
William S Harris, Clemens von Schacky The Omega-3 Index: a new risk factor for death from coronary heart disease? Preventive Medicine, Volume 39, Issue 1, 2004, 212–220

Omega-3 index The Omega-3 Index is the result of Dr. William Harris's 30 years of research in
fatty acids and cardiovascular disease
The Omega-3 Index is a measure of omega-3 fatty acids, EPA+DHA, in red blood cells, which relates to risk for heart disease
The omega-3 index is now recognised as a valuable biomarker of risk for numerous other health conditions and disease
Baseline levels of omega-3 should be evaluated and considered individually before generalised supplementation to strengthen the concept of personalised nutrition

Omega-3 index an early cardiovascular risk indicatorOmega-6 to omega-3 ratio an established marker of long-term health and chronic illnessAA to EPA ratio a measure of ’silent’ or chronic inflammation
A personalised plan aims to achieve:an omega-3 index of more than 8% an omega-6 to omega-3 ratio of between 3 and 4an AA to EPA ratio of between 1.5 and 3

Combining the AA to EPA ratio with the omega-3 index gives us a comprehensive overview of health status

Plasma vs red blood cell membranes (RBC)

Fatty acids can be measured in various blood fractions and tissues including plasma, erythrocytes and adipose tissue
PUFAs and trans fatty acids in adipose tissue correlated with intake measured by FFQs
Availability of adipose tissue limits its use and blood is therefore more widely used!
Saturated fatty acids and MUFAs in plasma and erythrocytes do not directly reflect intake, because these 2 classes of fatty acids can be made by endogenous synthesis from carbohydrates
In contrast, PUFAs and trans fatty acids in plasma and erythrocytes are a direct reflection of dietary intake – FOCUS on PUFA
Plasma fatty acids = recent intake Erythrocytes =long-term intake

• Fatty acid levels from red blood cells (RBCs), plasma and plasma phospholipids (PL) obtained from 20 healthy volunteers tested weekly over 6 weeks
• The average intake of oily fish (tuna or other non-fried fish) was 3 ± 2.9 times per month, and 5 subjects reported taking stable doses of fish oil supplements (providing between 300 and 1800 mg of EPA + DHA per day)
• All subjects reported stable dietary and supplementation habits throughout the study
Harris WS, Thomas RM. Biological variability of blood omega-3 biomarkers. Clin Biochem.2010 Feb;43(3):338-40.
Variability in plasma and RBC omega-3 index isolated whole blood

Considerable fluctuations are observed in plasma vs RBC
Within-subject coefficient of variation (CV) for the omega-3 index in RBCs vs plasma was 4.1%±1.9% and 15.9%±6.4%, respectively
Thus, the RBC test had the lowest biological variability, which means that a single measurement (not several) is all that is needed to determine the true omega-3 index
Harris WS, Thomas RM. Biological variability of blood omega-3 biomarkers. Clin Biochem. 2010 Feb;43(3):338-40.

Fasting vs Fed
Plasma fatty acids are prone to considerable fluctuations
Consuming a meal with fat/omega-3 will not affect the omega-3 index within RBC
Consuming a meal with fat/omega-3 will affect the omega-3 index within plasma
Plasma omega-3 index rises when omega-3s are consumed prior to testing
A non-omega-3 fat-containing meal will dilute plasma omega-3 with non-omega-3 fatty acids, thereby lowering the omega-3 index
Harris WS, Thomas RM. Biological variability of blood omega-3 biomarkers. Clin Biochem. 2010 Feb;43(3):338-40.

Effects of a single dose of EPA + DHA (3.4 g) taken with breakfast on the percentage of change from baseline (hour 0) in EPA + DHA levels in plasma (expressed as a percentage of total fatty acids, top; and expressed as concentrations, middle) and in RBCs (expressed as a percentage of total fatty acids; bottom) over 24 hours (n = 20)
Mean estimate and 95% Dunnett-adjusted confidence intervals are shown. *Difference from baseline, P < .05. DHA, docosahexaenoic acid; EPA, eicosapentaenoic acid; RBC, red blood cell.
Harris WS, Varvel SA, Pottala JV, Warnick GR, McConnell JP. Comparative effects of an acute dose of fish oil on omega-3 fatty acid levels in red blood cells versus plasma: implications for clinical utility. J Clin Lipidol. 2013 Sep-Oct;7(5):433-40

Whole blood vs blood spot

Whole blood Blood spotRequires phebotomist (client inconvenience) Client can take test (no phebotomist required)
Invasive Minimally invasive
More analytical steps Less analytical steps
Higher costs Lower costs
Inconvenience to client Convenient for practitioner and client
Can measure plasma or RBC Measures plasma and RBC (fasting required)
Whole blood vs blood spot

Dried blood spot (DBS)Minimally invasiveConvenient (can be performed by the client)Data derived from RBC & plasma
Whole bloodInvasive (requires a phlebotomist)Higher cost than DBSData derived from RBC only
High correlation between RBC omega-3 and DBS omega-3 (R=0.96, p<0.0001)

Why choose Igennus?

Why choose Igennus?
How it the omega-3 index determined?
William Harris who validated the Omega-3 index, is the founder of OmegaQuant Analytics
The number and type of fatty acids will affect the omega-3 index
Laboratory Genova Genova Genova Biolab Igennus OmegaMetrix OmegaQuantUK or USA based UK UK UK UK UK USA USAFatty acid analysis Plasma RBC Blood spot RBC Blood spot RBC Blood spotPhlebotomist required Yes Yes No Yes No Yes NoTotal number of fats analysed 33 23 7 32 24 23 24Expressed as μmol/L % total fat % area μmol/L % total % total % total

Laboratory Genova Genova Genova Biolab Igennus OmegaMetrix OmegaQuantUK or USA based UK UK UK UK UK USA USA
Fatty acid analysis Plasma RBC Blood spot RBC Blood spot RBC Blood spotPhlebotomist required Yes Yes No Yes No Yes No
Total number of fats analysed 33 23 7 32 24 23 24Expressed as μmol/L % total fat % area μmol/L % total % total % total
Saturated fat 14 8 0 31 6 4 6Capric 10:0
Lauric acid 12:0Myristic acid 14:0
Pentadecanoic acid 15:0Palmitic acid 16:0
Margaric acid 17:0Stearic acid 18:0
Nonadecanoic 19:0Arachidic acid 20:0
Heneicosanoic acid 21:0Behenic acid 22:0
Tricosanoic acid 23:0Lignoceric acid 24:0
Hexacosanoic 26:0Monounsaturated fat 6 4 0 6 4 3 4
Myristoleic acid n-5 14:1Palmitoleic acid n-7 16:1
Vaccenic acid n-7 18:1Oleic acid n-9 18:1
Eicosenoic acid n-9 20:1Euric cid n-6 22:1
Nervonic acid n-9 24:1Polyunsaturated fat n-9 1 0 0 1 0 0 0
Mead acid n-9 20:3

Laboratory Genova Genova Genova Biolab Igennus OmegaMetrix OmegaQuantUK or USA based UK UK UK UK UK USA USA
Fatty acid analysis Plasma RBC Blood spot RBC Blood spot RBC Blood spotPhlebotomist required Yes Yes No Yes No Yes No
Total number of fats analysed 33 23 7 32 24 23 24Expressed as μmol/L % total fat % area μmol/L % total % total % total
Polyunsaturated fat n-6 7 6 4 7 7 7 7Linoleic acid (LA) 18:2
Gamma-linolenic acid (GLA) 18:3Eicosadienoic acid (EDA) 20:2
Dihomo-gamma linolenic acid (DGLA) 20:3Arachidonic acid (AA) 20:4
Docosadienoic acid 22:2Docosatetraenoic acid n-6 22:4Docosapentaenoic acid n-6 22:5
Polyunsaturated fat n-3 4 4 3 4 4 4 4Alpha-linolenic acid (ALA) 18:3
Stearidonic acid (SDA) 18:4Eicosatetraenoic acid (ETA) 20:4Eicosapentaenoic acid (EPA) 20:5
Docosapentaenoic (DPA) 22:5Docosahexaenoic acid (DHA) 22:6
Trans fat 1 1 ?? 3 3 5 3Trans palmitoleic acid n-7 16:1
Trans vaccenic acid n-7 18:1Trans oleic acid n-9 18:1
Trans linoleic acid n-6 18:2Cis/trans linoleic acid 18:2
Trans/cis linoleic acid n-6 18:2Total trans

Laboratory Igennus OmegaQuantUK or USA based UK USA
Fatty acid analysis Blood spot Blood spotPhlebotomist required No No
Total number of fats analysed 24 24Expressed as % total % total
Saturated fat 6 6Myristic acid 14:0Palmitic acid 16:0Stearic acid 18:0Arachidic acid 20:0Behenic acid 22:0Lignoceric acid 24:0Monounsaturated fat 4 4Palmitoleic acid n-7 16:1Oleic acid n-9 18:1Eicosenoic acid n-9 20:1Nervonic acid n-9 24:1Polyunsaturated fat n-6 7 7Linoleic acid (LA) 18:2Gamma-linolenic acid (GLA) 18:3Eicosadienoic acid (EDA) 20:2Dihomo-gamma linolenic acid (DGLA) 20:3Arachidonic acid (AA) 20:4Docosatetraenoic acid n-6 22:4Docosapentaenoic acid n-6 22:5Polyunsaturated fat n-3 4 4Alpha-linolenic acid (ALA) 18:3Eicosapentaenoic acid (EPA) 20:5Docosapentaenoic (DPA) 22:5Docosahexaenoic acid (DHA) 22:6Trans fat 3 3Trans palmitoleic acid n-7 16:1Trans oleic acid n-9 18:1Trans linoleic acid n-6 18:2

What’s in the kit?
1 x test information sheet1 x Spot Saver card 2 x finger-prick lancets1 x resealable plastic bag with moisture-absorbent gel sachet 1 x sterile alcohol cleansing pad 1 x return envelope 1 x personal information form

Taking the test

Taking the test

Taking the test


Taking the test

Fatty acid stability in transit
Pre-treating blood slot cards with Butylated hydroxytoluene (BHT) prevents PUFA degradation for up to 8 weeks
BHT-mediated protection of PUFA is most likely due to free radical scavenging by BHT
The phenol group in BHT is thought to donate a proton to free radicals, thusneutralising the free radicals and preventing them from accepting hydrogen protons from the methylene groups in PUFA and thereby preventing degradation
Additionally, storing dried blood spots in sealable containers/bags further prevents PUFA loss
Metherel AH, Hogg RC, Buzikievich LM, Stark KD. Butylated hydroxytoluene can protect polyunsaturated fatty acids in dried blood spots from degradation for up to 8 weeks at room temperature. Lipids Health Dis. 2013 Feb 20;12:22.

Weight % of fatty acids in dried, untreated (BHT) blood spots over 28 days
Metherel AH, Hogg RC, Buzikievich LM, Stark KD. Butylated hydroxytoluene can protect polyunsaturated fatty acids in dried blood spots from degradation for up to 8 weeks at room temperature. Lipids Health Dis. 2013 Feb 20;12:22.

Weight % of fatty acids in dried blood spots treated with BHT (5 mg/ml) over 28 days
Metherel AH, Hogg RC, Buzikievich LM, Stark KD. Butylated hydroxytoluene can protect polyunsaturated fatty acids in dried blood spots from degradation for up to 8 weeks at room temperature. Lipids Health Dis. 2013 Feb 20;12:22.

The nutraceutical approach to managing inflammation: shift the balance!
AA, EPA and DHA contents of cell membranes can be altered through consumption of omega-3 (marine products/marine oils)
Improves cardiovascular health Improves cognitive function Improves immune function Improves inflammatory resolution Reduces disease risk
How much omega-3 do we need?
Knowledge of a person’s baseline omega-3 allows us to calculate a mg/kg dose of EPA/DHA to raise their omega-3 to a predetermined level
Flock MR, Skulas-Ray AC, Harris WS, Etherton TD, Fleming JA, Kris-Etherton PM Determinants of erythrocyte omega-3 fatty acid content in response to fish oil supplementation: a dose-response randomized controlled trial. J Am Heart Assoc. 2013 Nov 19;2(6):e000513. doi: 10.1161/JAHA.113.000513.

• It is suggested that whilst dietary intervention with fish oil results in the incorporation of EPA and DHA into cell membranes, the omega-3 index must reach the level suggested to be optimal (≥8% in the case of cardiovascular patients) to obtain clinical efficacy
• From a therapeutic stance, dietary intervention for clinical outcomes must therefore focus on ensuring that an ideal omega-3 index is achieved
Kagan I, Cohen J, Stein M, Bendavid I, Pinsker D, Silva V, Theilla M, Anbar R, Lev S, Grinev M, Singer P: Preemptive enteral nutrition enriched with eicosapentaenoic acid, gamma-linolenic acid and antioxidants in severe multiple trauma: a prospective, randomized, double-blind study. Intensive care medicine 2015.

Distribution of the percentage of red blood cell (RBC) EPA+DHA values (omega 3 index) in the study population ‐at baseline. Lines at 8% and 4% indicate proposed low and high risk horizons respectively, and the dotted line ‐ ‐at 4.3% is the population average
7%
2%
4.3%
Flock MR, Skulas-Ray AC, Harris WS, Etherton TD, Fleming JA, Kris-Etherton PM Determinants of erythrocyte omega-3 fatty acid content in response to fish oil supplementation: a dose-response randomized controlled trial. J Am Heart Assoc. 2013 Nov 19;2(6):e000513. doi: 10.1161/JAHA.113.000513.

Omega-3 dosing – ‘one size fits all?’
40 individuals with a baseline omega-3 index <5% (black bar) and post treatment (white bar) after a 6-week intervention with omega-3 EPA & DHA (0·5 g/d)
• The mean omega-3 index increased from 4·37% to 6·80% and inter-individual variability in response was high (varied by a factor of up to 13 inter-individually) (Kohler et al. 2010)
Köhler A, Bittner D, Löw A, von Schacky C. Effects of a convenience drink fortified with n-3 fatty acids on the n-3 index. Br J Nutr. 2010 Sep;104(5):729-36.

The Opti-O-3 results and recommendations

Interventions use a ‘one size fits all’ approach irrespective of personal requirements
Factors that influence the omega-3 index
age physical activity gender body weight
We are metabolically unique and using biomarkers to identify personal requirements for omega-3 can optimise clinical outcomes
omega-3 baseline levels and body weight will determine the dose needed to optimise the omega-3 index

Example 1



Example 2



Example 3



Opti-O-3 biomarker summary
Average Low High
Omega-3 index 5.47 1.21 17.91Omega-6 to omega-3 ratio 5.26 0.96 14.70AA to EPA ratio 9.27 0.42 54.43
In 1992, the BNF Task Force on Unsaturated Fatty Acids suggested a desirable population intake for EPA and DHA of 0.5% of energy, which equates to about 8g/week (1.14g/day) for women and 10g/week (1.42g/day) for men, equivalent to 2-3 medium servings of oil-rich fish per week
• Current recommendations are set at 450mg EPA and DHA daily (2 portions fish weekly of which one should be oily)
• Mean consumption of oily fish (all age groups) was below the recommended one portion (140g) per week (rolling programme for 2008 and 2009 to 2011 and 2012)
• Mean consumption in adults aged 19 to 64 years was 54g per week (52g for men and 54g for women) and for adults aged 65 years and over mean consumption was 90g per week (103g for men and 81g for women)
https://www.gov.uk/government/statistics/national-diet-and-nutrition-survey-results-from-years-1-to-4-combined-of-the-rolling-programme-for-2008-and-2009-to-2011-and-2012
British Nutrition Foundation. Unsaturated fatty acids nutritional and physiological significance: the report of the British Nutrition Foundation's task force. New York: Chapman & Hall, 1992.

Using reference ranges
Laboratories provide reference ranges using in-house data
In-house data is skewed because it fails to provide information gathered from ‘normal’ population
There are no validated reference ranges for individual fatty acids
However...........

Genova blood spot

Genova blood spot
0.41 - 4.06?

Q1 Q2 Q3 Q4 Q5Low Average High
Saturated fatMyristic acid 14:0 0.17 0.47 0.62 0.85 2.01Palmitic acid 16:0 15.5 21.55 23.01 24.38 29.26Stearic acid 18:0 1.45 13.17 14.48 15.62 23.07
Arachidic acid 20:0 0.05 0.14 0.16 0.18 0.75Behenic acid 22:0 0.15 0.36 0.43 0.51 1.13
Lignoceric acid 24:0 0.19 0.51 0.64 0.76 2.36Monounsaturated fat
Palmitoleic acid n-7 16:1 0.1 0.69 0.92 1.28 3.51Oleic acid n-9 18:1 12.38 17.96 21.03 32.97 32.97
Eicosenoic acid n-9 20:1 0.08 0.18 0.22 0.26 0.85Nervonic acid n-9 24:1 0.07 0.4 0.51 0.65 1.69
Polyunsaturated fat n-6Linoleic acid (LA) 18:2 11.08 16.83 18.56 21.15 28.74
Gamma-linolenic acid (GLA) 18:3 0.02 0.13 0.18 0.27 0.97Eicosadienoic acid (EDA) 20:2 0.10 0.16 0.19 0.22 0.98
Dihomo-gamma linolenic acid (DGLA) 20:3 0.39 0.99 1.23 1.48 2.47Arachidonic acid (AA) 20:4 2.5 8.56 10.05 11.38 16.51
Docosatetraenoic acid n-6 22:4 0.12 0.64 0.85 1.13 2.58Docosapentaenoic acid n-6 22:5 0.03 0.14 0.17 0.23 1.53
Polyunsaturated fat n-3Alpha-linolenic acid (ALA) 18:3 0.16 0.34 0.41 0.51 1.4
Eicosapentaenoic acid (EPA) 20:5 0.2 0.86 1.4 2.44 10.68Docosapentaenoic (DPA) 22:5 0.41 0.89 1.11 1.45 3.97
Docosahexaenoic acid (DHA) 22:6 0.96 2.49 3.35 4.37 8.89Trans fat
Trans palmitoleic acid n-7 16:1 0.11 0.19 0.23 0.28 0.84Trans oleic acid n-9 18:1 0.01 0.09 0.12 0.18 0.54
Trans linoleic acid n-6 18:2 0.07 0.16 0.19 0.23 1.7


Q1 Q2 Q3 Q4 Q5RESULT Low Average High
Saturated fatMyristic acid 14:0 0.53Palmitic acid 16:0 24.2Stearic acid 18:0 17.81
Arachidic acid 20:0 0.14Behenic acid 22:0 0.43
Lignoceric acid 24:0 0.57Monounsaturated fat
Palmitoleic acid n-7 16:1 0.88Oleic acid n-9 18:1 17.26
Eicosenoic acid n-9 20:1 0.20Nervonic acid n-9 24:1 0.43
Polyunsaturated fat n-6Linoleic acid (LA) 18:2 20.37
Gamma-linolenic acid (GLA) 18:3 0.23Eicosadienoic acid (EDA) 20:2 0.16
Dihomo-gamma linolenic acid (DGLA) 20:3 1.37Arachidonic acid (AA) 20:4 10.05
Docosatetraenoic acid n-6 22:4 0.76Docosapentaenoic acid n-6 22:5 0.12
Polyunsaturated fat n-3Alpha-linolenic acid (ALA) 18:3 0.27
Eicosapentaenoic acid (EPA) 20:5 0.79Docosapentaenoic (DPA) 22:5 0.74
Docosahexaenoic acid (DHA) 22:6 2.31Trans fat
Trans palmitoleic acid n-7 16:1 0.14Trans oleic acid n-9 18:1 0.06
Trans linoleic acid n-6 18:2 0.17
Base line fatty acids

Q1 Q2 Q3 Q4 Q5RESULT Low Average High
Saturated fatMyristic acid 14:0 0.33Palmitic acid 16:0 22.32Stearic acid 18:0 14.62
Arachidic acid 20:0 0.15Behenic acid 22:0 0.34
Lignoceric acid 24:0 0.57Monounsaturated fat
Palmitoleic acid n-7 16:1 0.69Oleic acid n-9 18:1 20.43
Eicosenoic acid n-9 20:1 0.29Nervonic acid n-9 24:1 0.51
Polyunsaturated fat n-6Linoleic acid (LA) 18:2 19.04
Gamma-linolenic acid (GLA) 18:3 0.10Eicosadienoic acid (EDA) 20:2 0.22
Dihomo-gamma linolenic acid (DGLA) 20:3 1.07Arachidonic acid (AA) 20:4 9.16
Docosatetraenoic acid n-6 22:4 0.38Docosapentaenoic acid n-6 22:5 0.10
Polyunsaturated fat n-3Alpha-linolenic acid (ALA) 18:3 0.37
Eicosapentaenoic acid (EPA) 20:5 3.58Docosapentaenoic (DPA) 22:5 1.82
Docosahexaenoic acid (DHA) 22:6 3.58Trans fat
Trans palmitoleic acid n-7 16:1 0.13Trans oleic acid n-9 18:1 0.06
Trans linoleic acid n-6 18:2 0.15
6-month fatty acids

RESTORE with pure EPAMAINTAIN with EPA, DHA
and GLAMinimum 3-6 months
Therapeutic role of Pharmepa®RESTORE & MAINTAIN™
AA to EPA ratio Inflammatory regulation Symptoms of inflammatory illness Optimum brain, cell, heart, immune
and CNS function Optimum wellbeing
Omega-3 index Omega-6 to 3 ratio Long-term general and cellular
health Heart, brain and eye health Prevent chronic illness and protect
against inflammatory disease

1 RESTORE 2 RESTORE 3 RESTORE 4 RESTORE 1 MAINTAIN 2 MAINTAIN 3 MAINTAIN 4 MAINTAIN
EPA (mg) 500 1000 1500 2000 250 500 750 1000
DHA (mg) 0 0 0 0 83 167 250 333GLA (mg) 0 0 0 0 20 40 60 80
Vitamin E (mg) 5 10 15 20 3 6 9 12Vitamin D (μg) 0 0 0 0 10 20 30 40
EPA/DHA ratio - - - 3 3 3 3
Total Omega-3 (mg) 500 1000 1500 2000 333 666 1000 1333
RESTORE & MAINTAIN mixed doses
1 RESTORE 2 RESTORE 3 RESTORE 4 RESTORE 1 MAINTAIN 2 MAINTAIN 3 MAINTAIN 4 MAINTAIN0
500
1000
1500
2000
2500GLA (mg) DHA (mg) EPA (mg)
Dose
(mg)

0
500
1000
1500
2000
2500
3000GLA (mg) DHA (mg) EPA (mg)
1 RESTORE1 MAINTAIN
1 RESTORE4 MAINTAIN
2 RESTORE1 MAINTAIN
2 RESTORE2 MAINTAIN
2 RESTORE3 MAINTAIN
1 RESTORE3 MAINTAIN
1 RESTORE2 MAINTAIN
2 RESTORE4 MAINTAIN
1 RESTORE 1 RESTORE 1 RESTORE 1 RESTORE 2 RESTORE 2 RESTORE 2 RESTORE 2 RESTORE
1 MAINTAIN 2 MAINTAIN 3 MAINTAIN 4 MAINTAIN 1 MAINTAIN 2 MAINTAIN 3 MAINTAIN 4 MAINTAIN
EPA (mg) 750 1000 1250 1500 1250 1500 1750 2000DHA (mg) 83 167 250 333 83 167 250 333GLA (mg) 20 40 60 80 20 40 60 80
Vitamin E (mg) 8 11 14 17 13 16 19 22Vitamin D (mg) 10 20 30 40 10 20 30 40
EPA/DHA ratio 9 6 5 5 15 9 7 6
Total Omega-3 (mg) 833 1167 1500 1833 1333 1667 2000 2333
Dose
(mg)
RESTORE & MAINTAIN mixed doses

Benefits of the Opti-O-3
Knowledge of baseline levels will guide the practitioner recommendations—unsurprisingly, low baseline values may require a larger dose than a high baseline value!
The omega-3 index and AA to EPA ratio are invaluable for assessing both baseline risk and the change in risk (as function of intake – retesting is advisable ≥6 months)
Dose response studies show us that high doses of omega-3 are required to reduce the AA to EPA ratio and achieve an omega-3 index ≥8%, especially where the baseline levels are suboptimal ≤4%
Use in conjunction with Pharmepa RESTORE & MAINTAIN
Pre-loading with pure EPA for 6 months (RESTORE) is advised to reduce the AA to EPA ratio, before the introduction of EPA/DHA with GLA (MAINTAIN) for long-term support of the omega-3 index

Education Technical
Sophie TullyNutrition Education
Dr Nina Bailey Head of Nutrition