
Periulnar Injuries Associated with Distal Radius Fractures414864/FULLTEXT01.pdf · al. 2008) (Fig...
66
Linköping University Medical Dissertations No. 1236 Periulnar Injuries Associated with Distal Radius Fractures Johan Scheer Division of Orthopaedic Surgery Department of Clinical and Experimental Medicine Faculty of Health Sciences Linköping University Sweden Linköping 2011
Transcript of Periulnar Injuries Associated with Distal Radius Fractures414864/FULLTEXT01.pdf · al. 2008) (Fig...

Linköping University Medical Dissertations
No. 1236
Periulnar Injuries Associated with
Distal Radius Fractures
Johan Scheer
Division of Orthopaedic Surgery Department of Clinical and Experimental Medicine
Faculty of Health Sciences Linköping University
Sweden
Linköping 2011

© Johan Scheer 2011 Cover design: Johan Scheer Paper I is reprinted with permission from Elsevier. Papers II and IV are re-printed with permission from Sage publications. Printed in Sweden by LiU-Tryck, Linköping, 2011 ISBN: 978-91-7393-201-1 ISSN: 0345-0082

This is for not becoming a grumpy old doctor
That which was dimly said was dimly thought
Essias Tegnér, 1820

CONTENTS
CONTENTS
ABSTRACT.............................................................................................................................. 7
SVENSK SAMMANFATTNING ........................................................................................ 8
ABBREVIATIONS ................................................................................................................. 9
LIST OF PAPERS ................................................................................................................ 10
INTRODUCTION ................................................................................................................ 11
CONNECTIONS ABOUT THE DISTAL ULNA........................................................... 12 Forearm rotation........................................................................................................................... 12 The concept of joint stability ...................................................................................................... 13 Anatomy and function about the DRU joint ........................................................................... 13 The effect of malunion on functional outcome........................................................................ 21 Techniques of corrective osteotomy of the distal radius ...................................................... 22 Pathomechanisms of TFCC injuries associated with distal radius fractures. ................ 22 The effect of ligament injuries on functional outcome ......................................................... 23 Diagnosis of a TFCC injury ........................................................................................................ 23
AIMS OF THIS THESIS .................................................................................................... 25
MATERIAL AND SUBJECTS .......................................................................................... 26 Cadaveric specimens .................................................................................................................... 26 Patients ........................................................................................................................................... 26
METHODS ............................................................................................................................ 28 Functional outcome measurements .......................................................................................... 28 Imaging ........................................................................................................................................... 30 Injury classifications .................................................................................................................... 31 Radioulnar stress test.................................................................................................................. 32 Cadaveric testing .......................................................................................................................... 33 Surgical procedures ...................................................................................................................... 35 Bald ulnar head test..................................................................................................................... 36
STATISTICAL METHODS................................................................................................ 38
RESULTS .............................................................................................................................. 39 Effects of corrective osteotomy on outcome............................................................................. 39 Non-invasive diagnosis of foveal TFCC injury ....................................................................... 39

CONTENTS
Correlation between radioulnar stress test and functional outcome ................................ 41 TFCC elongation limit ................................................................................................................. 42 Pathomechanisms of TFCC injuries ......................................................................................... 42
DISCUSSION ....................................................................................................................... 47 How can skeletal malunion limit forearm rotation? ............................................................. 47 What do we know about the patterns and pathomechanisms of TFCC injuries? .......... 48 What is the relationship between an ulnar styloid fracture and a TFCC injury? ......... 50 Aspects on repair of a TFCC injury .......................................................................................... 52 What are the possible implications of an sECU injury? ...................................................... 54 Can acute TFCC injuries be detected using non-invasive methods? ................................ 55 Which patients benefit from an acute TFCC reconstruction? ............................................ 57
CONCLUSIONS................................................................................................................... 59
FUTURE RESEARCH ........................................................................................................ 60
ACKNOWLEDGEMENTS ................................................................................................. 61
REFERENCES ..................................................................................................................... 62
APPENDIXES Papers I-V.................................................................................................. 67

ABSTRACT
7
ABSTRACT Residual dysfunction after a fracture of the distal radius is most often mild but may give rise to significant impairment especially in the younger active popula-tion. The symptoms often manifest around the distal ulna when loading the hand or rotating the forearm. In this region are found articular and soft tissue connec-tions running from the distal ulna to the distal radius as well as to the ulnar side of the carpus. The aims of this thesis were to investigate the effects of distal ra-dius fractures on the structures about the distal ulna and to what extent malun-ion and ulnar soft tissue lesions affect function. Both patients and cadaver specimens were used in the five different studies. In a retrospective study of 17 malunited distal radius fractures supination im-pairment improved significantly by correction of the skeletal malunion. This highlights the importance of distal radioulnar joint congruity for forearm rotation in a subset of cases. The pathomechanisms of injury to the triangular fibrocartilage complex (TFCC) were studied. In a cadaveric distal radius fracture model different restraining properties and injury patterns were investigated. Similar patterns of injury were then observed in 20 patients with a displaced distal radius fracture. It was found that a TFCC injury can be expected with dorsal displacement of the distal radius fragment of 32o or more from the anatomically correct position. The distribution of a TFCC injury apparently differs depending on the size of an associated ulnar styloid fracture. In cases of an intact ulnar styloid or a concomitant tip fracture (Type 1) the first stage of injury seems to be extensor carpi ulnaris subsheath separation from the distal ulna and the dorsal radioulnar ligament. Thereafter follows a disruption of the deep insertions into the fovea of the ulna starting from the palmar and extending dorsally and radially. An extensive injury can be de-tected with a novel non-invasive test called the ‘bald ulnar head test’, which is performed under anaesthesia. Diagnosis of an acute TFCC injury is difficult using non-invasive methods. In a prospective study of 48 patients, CT scanning to detect pathologic subluxation was found to be of little use in both acute and chronic cases, and is therefore not endorsed on this indication. A radioulnar stress test, which in previous studies has correlated well to a deep TFCC injury, was found to be highly reliable but not to correspond with significant disability in self-administered questionnaires of functional outcome two years or more after injury. This indicates that the subset of patients possibly benefiting from acute repair must be identified by other means.

SVENSK SAMMANFATTNING
8
SVENSK SAMMANFATTNING (Popular scientific abstract in Swedish)
Handledsbrott är den vanligaste frakturen hos vuxna. Skadan har i olika studier visats ge kvarstående påtaglig invaliditet i 7-8% av fallen beroende på svårig-hetsgrad och given behandling. Besvären finns ofta på lillfingersidan av handle-den i form av värk och rörelsesmärta och ibland svårigheter att rotera i under-armen; en påtagligt handikappande inskränkning. Syftet med denna avhandling är att fördjupa kunskapen om dessa frakturers effekter på den nedre leden mel-lan strålben (radius) och armbågsben (ulna) – kallad distala radioulnara (DRU) leden - både med avseende på ledbandsförbindelser och skelettär ledpassning. Dessa ledbandsförbindelser går under samlingsbegreppet TFCC (triangulära kartilaginära komplexet) och binder både ihop radius med ulna och ulna med handloven. I avhandlingen ingår fem delarbeten baserade på studier av patienter och prepa-rat från frivilliga donatorer. Fynden är i huvudsak följande:
1. Hos patienter, som därför att handledsfrakturen läkt i ett ogynnsamt läge har svårt att rotera i underarmen, kan rotationsförmågan förbättras ge-nom att passningen i DRU-leden återställs. Detta sker genom att det fel-läkta brottet sågas upp och återställs till nära ursprungligt läge.
2. Skador på TFCC är mycket vanliga vid dessa handledsfrakturer och kan
uppkomma både vid uttalat felställda skador, och även vid enklare sprick-bildningar.
3. De skador som iakttagits vid akut undersökning av patienter med fraktu-
rer som inte engagerar ledytorna kan enkelt reproduceras vid laboratorie-försök av liknande frakturtyp. Därför kan mekanismerna och mönstren av dessa ledbandsskador nu beskrivas.
4. Vid diagnostik av dessa ledbandsskador är skiktröntgen med röntgen-
strålning (datortomografi) inte till någon hjälp.
5. Majoriteten av vuxna patienter under 50 år med en TFCC-skada förefaller inte få några större besvär av denna, troligen på grund av att de kan kom-pensera med omgivande muskulatur. Fortfarande saknas metoder att för-utsäga vilka patienter som kommer att få besvär av sin ledbandsskada.
6. Precis reparation av skadorna kan utföras med ledning av de i avhand-
lingen beskrivna skademönstren.

ABBREVIATIONS
9
ABBREVIATIONS
CT Computed tomography DASH Disabilities of the Arm, Shoulder and Hand questionnaire DRU Distal radioulnar dRUL Dorsal radioulnar ligament dUT Dorsal ulnotriquetral ligament ECU Extensor carpi ulnaris FCU Flexor carpi ulnaris L-T Luno-triquetral MRI Magnetic resonance imaging NNH Numbers needed to harm, the surgical equivalent to NNT (Numbers
needed to treat) in pharmaceuticals pRUL Palmar radioulnar ligament RUR Radioulnar ratio S-L Scapho-lunate sECU Subsheath of the extensor carpi ulnaris tendon TCP Tricalcium phosphate TFCC Triangular fibrocartilage complex UC Ulnocarpal UL Ulnolunate UT Ulnotriquetral

LIST OF PAPERS
10
LIST OF PAPERS This thesis is based on the following papers. They will be referred to by their ro-man numerals:
I. Scheer JH, Adolfsson LE. Tricalcium phosphate bone substitute in cor-rective osteotomy of the distal radius. Injury. 2009, 40: 262-7
II. Scheer JH, Hammerby S, Adolfsson LE. Radioulnar ratio in detection of
distal radioulnar joint instability associated with acute distal radius fractures. J Hand Surg Eur Vol. 2010, 35: 730-4
III. Scheer JH, Adolfsson LE. Pathomechanisms of ulnar ligament lesions
of the wrist in a cadaveric distal radius fracture model. Accepted for publication in Acta Orthopaedica.
IV. Scheer JH, Adolfsson LE. Radioulnar laxity and clinical outcome after a
distal radius fracture do not correlate. Accepted for publication in J Hand Surg Eur Vol.
V. Scheer JH, Adolfsson LE. TFCC-injuries associated with severely
displaced Colle’s fractures: a clinical study. Submitted to J Hand Surg Eur Vol.

INTRODUCTION
11
INTRODUCTION ”One consolation only remains, that the limb will at some remote period again enjoy perfect freedom in all its motions, and be completely exempt from pain...” Abraham Colles; Edinburgh Med Surg 1814
Residual symptoms after fracture of the distal radius Fracture of the distal radius may be extraarticular, intraarticular or both. The distal fragments can be displaced in almost any direction, but typically and most commonly a dorsal angulation and axial shortening is present, i.e. a Colles’ type fracture as described by Abraham Colles 1814. His achievement was recognising the injury as a fracture and not a carpal dislocation before the era of radiology. Residual symptoms after a distal radius fracture are common and may cause sig-nificant impairment in 7-8% of cases regardless of treatment (Bacorn and Kurtzke 1953, Cooney et al. 1980, Kopylov et al. 1993, Abramo et al. 2008). Malunion is a major cause of dysfunction, at least in younger patients (Gliatis et al. 2000, Grewal and MacDermid 2007) whereas elderly patients with a low level of activity may do well regardless of severe malunion (Gehrmann et al. 2008). Although the united fracture is at the distal radius, patients with dysfunction may somewhat unexpectedly often have symptoms around the distal ulna (af Ekenstam et al. 1985, Oskam et al. 1996, Prommersberger et al. 2002) with ulnar pain when loading the hand and sometimes at rest. This may be combined with restricted forearm rotation especially in cases of malunion (Hirahara et al. 2003, Ishikawa et al. 2005), which can cause significant functional impairment (Flinkkilä et al. 2000). Indeed, most patients do well with restricted radiocarpal motion, whereas rotational limitation may confine activities of daily living such as opening doors, receiving small change, personal hygiene and a smooth golf swing. However, despite proper bony fracture union and with normal range of forearm rotation, ligament injuries on the ulnar side may be a source of ulnar wrist pain and functional impairment, possibly even more so in the younger population (Lindau et al. 2000a, Lindau et al. 2000b) because of higher functional demands.

CONNECTIONS ABOUT THE DISTAL ULNA
12
CONNECTIONS ABOUT THE DISTAL ULNA
Forearm rotation The forearm can functionally be considered as a joint, in which pro- and supina-tion are carried out (Hagert 1994). This forearm joint has one separate articula-tion in each end. The hand (via the carpus) is relatively fixed to the distal radius, which rotates approximately 180o around the ulna (Stuart et al. 2000, Shaaban et al. 2008) (Fig 1). The radius must therefore be S-shaped to accommodate for the ulna throughout rotation. The axis of rotation runs through the radial head proximally and through the ulnar head distally (Fig 2) and location of the axes varies slightly during the arc of motion (Tay et al. 2008, Tay et al. 2010). To maximise the range of motion and at the same time maintain ulnocarpal (UC) and DRU stability, the ligaments aiding in this emerge from the fovea of the ul-nar head or from the ulnar styloid, both of which are close to the centre of rota-tion (Garcia-Elias 1998, Tay et al. 2010) – see also below on page 17.
Figure 1. Forearm rotation. The hand is relatively fixed to the S-shaped radius (grey), which rotates about 180o around the ulna.
Figure 2. Forearm; lateral view. At the proximal end is the proximal radioulnar joint (PRU) in which the radial head rotates within the anular ligament. At the distal end the radius (R) rests on and rotates around the head of the ulna (U) and forms the distal radioulnar (DRU) joint. Grey line: indicates the axis of rotation.
Supination Pronation
R
U
Anular ligament (cut)

CONNECTIONS ABOUT THE DISTAL ULNA
13
The supinator and the biceps brachii muscles are the main motors for supination whilst pronation is mainly provided by the proximally located pronator teres and the superficial head of the distally positioned pronator quadratus (PQ) muscle. The deep head of the latter might primarily function as a stabiliser of the distal radioulnar joint (Stuart 1996, Gordon et al. 2004).
The concept of joint stability Stability of a joint can be defined as the restraint of surrounding musculoskeletal tissues against joint subluxation/dislocation. These factors include joint congru-ity, supporting ligaments (passive systems) but also active neuromuscular con-trol, mediated by proprioceptive reflexes and voluntary control. Many joints are not highly congruent, e.g. the glenohumeral-, knee- and DRU joints. In these there is no clear-cut definition of when the joint is subluxed and instability is of-ten defined as the patient’s discomfort of perceiving loss of joint control (e.g. ap-prehension of the shoulder or the feeling of giving way in the knee) (Kuhn 2010). Injuries to the stabilising structures (causing laxity) can thus be present without producing instability symptoms, since the patient may compensate with remain-ing intact structures and systems. Ulnar wrist instability can be radioulnar, ul-nocarpal or both and can manifest itself as pain on the ulnar side at rest or dur-ing activity (with or without painful clicking) or feeling of giving way (discomfort when the joint is subluxing).
Anatomy and function about the DRU joint
1. Articular surfaces and joint spaces The rounded expansion of the distal ulna is called the head (Fig 3). It is to 3/4 covered by hyaline cartilage and the remaining bony surfaces - mainly the ulnar fovea, the ulnar styloid and the dorsal groove of the extensor carpi ulnaris (ECU) subsheath - serve as insertion points for soft tissue stabilisers (Garcia-Elias 1998). The cartilage-covered part is not spherical in either transverse, coronal or sagittal planes and its configuration varies between individuals (Bade et al. 1996).
The distal radius, in the transverse plane, is covered with hyaline cartilage formed into two facets, which articulate with the scaphoid and lunate bones re-spectively, creating the radiocarpal articulation. Load from the carpus, via the lunate and articular disc of the triangular fibrocartilage complex (TFCC), is also

CONNECTIONS ABOUT THE DISTAL ULNA
14
transmitted to the distal ulna (Rikli et al. 2007) which is the ulnocarpal ar-ticulation. The joint space formed be-tween the distal radius plus the disc of the TFCC and the proximal carpal row is a continuum. There is thus no true sepa-rate ulnocarpal joint space and the common space is often referred to as the radiocarpal joint (Fig 4). On its ulnar side the distal radius has an articular surface, the sigmoid notch (Fig 3), resting on the ulnar head throughout pronation and supination. This joint space is called the distal radioulnar (DRU) joint and is separated from the radiocarpal joint by the articular disc of the TFCC only (Kleinman and Graham 1998) (Fig 4).
2. Morphology and kinematics of the dis-tal radioulnar joint When the forearm rotates, the sigmoid notch of the radius both rotates and slides around the 270o articular circum-ference of the ulnar head (af Ekenstam and Hagert 1985). The sigmoid notch also slides longitudinally in the distal direc-tion from pronation to supination (Tay et al. 2010). In the transverse plane, the DRU joint is not highly congruent since the circular radius of the ulnar head is significantly less than that of the sigmoid notch. There is however inter-individual variability of DRU joint congruency (af Ekenstam and Hagert 1985, Tolat et al. 1996). At least in unloaded forearm rotation the contact area in the sigmoid notch shifts from dorsal to palmar when the forearm rotates from pronation to supination (Ishii et al. 1998b, Xu and Tang 2009) (Fig 5). Additional restraints are impor-tant to keep the joint reduced. In cadaver
Figure 3. Dorsal view of the distal ra-dius and ulna. a) The sigmoid notch of the radius (bold arrow) is the articular seat for the ulnar head. b) Head of ulna with articular cartilage facing both the sigmoid notch and the carpal bones. Ar-row: groove for the ECU subsheath and tendon. The shape and size of the ulnar styloid (US) can vary considerably be-tween individuals.
a) b)
Figure 4. Joint spaces of the wrist in grey. MC: Midcarpal joint. RC: Radio-carpal joint (contain radiocarpal and ul-nocarpal articulations). DRU: Distal ra-dioulnar joint, Arrow: fibrocartilage disc of the TFCC that separates the DRU from the RC joint. R: radius. U: ulna.
US

CONNECTIONS ABOUT THE DISTAL ULNA
15
tests, after detachment of all restraining soft tissue the restraint provided by ar-ticular contact was estimated to be about 20-30% (Stuart et al. 2000). However, the shape of the sigmoid notch can vary (Tolat et al. 1996) and there have been case reports of successful osseous reconstruction of flat sigmoid notches in persis-tent DRU joint instability (Wallwork and Bain 2001, Tham and Bain 2007).
Figure 5. Transverse view over the DRU joint in unloaded rotation. Note that the con-tact area between the ulnar head and the sigmoid notch alters during the unloaded arc of motion. The ECU tendon is maintained in its groove throughout this motion path by means of its fibrous sheath. U: Ulna.
In the coronal plane, three different DRU joint types have been described in rela-tion to the inclination of the sigmoid notch relative to the long axis of the ulna (De Smet and Fabry 1993, Tolat et al. 1996, Hollevoet et al. 2006) (Fig 6). The coronal joint types are related to ulnar variance (De Smet and Fabry 1993, Sagerman et al. 1995), which is denominated as positive when the ulnar head is distal to the joint surface of the distal radius. Functionally, ulnar variance in-creases with pronation (Tay et al. 2010) and with exertion of significant grip force (Friedman et al. 1993), but may also be influenced by elbow flexion (Fu et al. 2009).
Figure 6. DRU types (According to de Smet 1993 and Tolat 1996). Type I: The sig-moid notch is parallel to the long axis of the radius and cylindrical in shape. Type II: The sigmoid notch is oblique facing proximally towards the ulnar head and hemispheri-cal in shape. Associated with negative ulnar variance. Type III: Reverse oblique angle. The sigmoid notch is coniform. Associated with positive ulnar variance.
I. II III.

CONNECTIONS ABOUT THE DISTAL ULNA
16
An ulnocarpal impaction (or abutment syndrome (Fig 7) can be a source of ulnar wrist pain, especially in cases of axial shortening after a distal radius fracture. The relationship between DRU joint types and ulnocarpal impaction syndrome (Fig 7) has not been investigated, neither in post-traumatic nor degenerative cases. The syndrome is unlikely to occur in Type II DRU joint types unless secon-dary to a distal radius fracture.
Figure 7. Ulnocarpal impaction. Dege-nerative changes of the articular carti-lage of the ulna (U) and lunate (L) and the intermediate disc of the TFCC due to repetitive collision/overloading. (Re-produced with the kind permission of Elsevier. From Palmer 1989).
Figure 8. Interosseous Membrane, right forearm, medial view. Membranous portions with holes for the interosseous artery. R: Radius. U: Ulna. CB: Central Band, stoutest portion of IOM. DOB: Distal Oblique Band, not invariably present. (Reproduced with the kind permission of Elsevier. From Noda et al. 2009)
3. Soft tissue passive stabilisers of the DRU and UC connections A. Interosseous membrane Between radius and ulna runs the interosseous membrane (IOM) (Fig 8), which consists of several different ligaments of which the central band is the stoutest and considered functionally the most important (Noda et al. 2009) transferring loads between the radius and ulna. The IOM affects radioulnar but not ulnocar-pal stability. In the absence of distal stabilisers, sectioning of the IOM decreases DRU stability in cadaveric models (Kihara et al. 1995, Gofton et al. 2004). A dis-
U

CONNECTIONS ABOUT THE DISTAL ULNA
17
tal oblique band (DOB), that may only occur in 40% of the population (Noda et al. 2009), blends distally into the DRU joint capsule and may be of importance in cases of disruption of the triangular fibrocartilage complex (TFCC) (Watanabe et al. 2005, Moritomo et al. 2009). B. The TFCC The triangular fibrocartilage complex (TFCC) is a general term for the confluent ligamentous structures that aid both radioulnar and ulnocarpal stability (Figs 9 and 10) (Garcia-Elias 1998, Berger 2010). It consists of a non vascularised, trian-gular articular disc surrounded by ligaments which bind together both the radius and ulna and the ulna and carpus (Palmer and Werner 1981). The term fibrocar-tilage stems from the tissue structure of the triangular central articular disc, which cushions and transfers loads from the lunate and triquetrum to the ulna. The radial insertion of the disc is histologically indistinguishable from the carti-lage of the sigmoid notch. The transition between the disc and the vascularised ligaments in the periphery is abrupt (Berger 2010). Between the ulnar styloid and the triquetrum covering the ulnar styloid is loosely arranged connective tis-sue called the meniscus homologue (Fig 11). On both the palmar and the dorsal side there are ligaments that both contribute to radioulnar and ulnocarpal stability. These structures will be described sepa-rately below. As mentioned above, at the ulnar head all these structures insert closely to the axis of rotation. The precise location of this axis is however a mat-ter of controversy. In vivo imaging studies have made it clear that the location of the axis varies during pronation and supination (Fu et al. 2009, Tay et al. 2010) and that it may vary between normal subjects, but not within (comparing sides) (Tay et al. 2010). C. The palmar ligaments of the TFCC (Figs 9 and 10) The palmar radioulnar ligament (pRUL) runs from the distal palmar ulnar cor-ner of the distal radius and inserts into the fovea of the ulnar head (Fig 11) (Ishii et al. 1998a). The ulnotriquetral (UT) and ulnolunate (UL) ligaments insert into the pRUL itself close to the foveal region (Garcia-Elias 1998, Ishii et al. 1998a, Sasao et al. 2003). The layer outside these is the ulnocapitate (UC) ligament which runs from the base of the styloid process to the capitate bone (Feipel and Rooze 1997). This ligament however appertains to the extrinsic carpal ligaments. D. The dorsal ligaments of the TFCC (Figs 9 and 10) The dorsal radioulnar ligament (dRUL) forms the dorsal border of the articular disc and runs from the distal ulnar corner of the sigmoid notch toward the styloid process, which it envelops. It is not clear whether the dRUL also inserts into the fovea (Garcia-Elias and Domenech-Mateu 1987, Ishii et al. 1998a, Sasao et al.

CONNECTIONS ABOUT THE DISTAL ULNA
18
2003) or slightly distal to it (Berger 2010). At the ulnar insertion level, the fibres of the dRUL blend with the fibrous tunnel of the extensor carpi ulnaris (ECU) tendon, also known as the ECU tendon subsheath (sECU), which has a close ana-tomical and functional relationship to the TFCC (Gupta et al. 2002) and by some considered to be a part of the TFCC (Palmer and Werner 1981, Ishii et al. 1998a, Sasao et al. 2003). E. Function of the TFCC
Several experiments, mainly cadaveric but also on 3D CT animations, have been carried out to investigate the contribution of the TFCC to DRU joint stability. Little is known about the contributions to ulnocarpal stability. Since the middle 80’s attention has been drawn to the insertion of the pRUL and dRUL into the fovea (Figure 11) and its importance for radioulnar stability (af Ekenstam and Hagert 1985, Haugstvedt et al. 2006). As the forearm rotates the radioulnar ligaments tauten (Nakamura et al. 1996, Ward et al. 2000), however which of the limbs that tautens in various pronation and supination positions and with various loads on the hand is not entirely clear (Stuart et al. 2000).
Figure 9. The DRU joint and TFCC of the right wrist seen from a distal viewpoint. A). Bold arrow: Fovea of the ulnar head. U: Ulnar head. US: Ulnar styloid process. L: Lunate facet of the radius. S: Scaphoid facet of the radius. B) The TFCC. sECU: ECU subsheath (with ten-don). dRUL: Dorsal radioulnar ligament. pRUL: Palmar radioulnar ligament. UT: Ulnotri-quetral ligament. UL: Ulnolunate ligament. Also included in the picture SRL: Short radiolu-nate ligament. UCap: Ulnocapitate ligament.
U L S
US
sECU
dRUL
pRUL
UT
UL
SRL UCap
Disc
A) B)

CONNECTIONS ABOUT THE DISTAL ULNA
19
Some have argued for the presence of a distal, superficial layer of both the radi-oulnar ligaments (Ishii et al. 1998a) having importance for DRU stability (Hagert 1994, Xu and Tang 2009), whereas others have found no evidence of such fibres (Nakamura et al. 2001). Such a layer would implicate a subdivision of ligament structures that all in all are approximately 2 mm in thickness and that the su-perficial part of this would lengthen between 25-80% (Xu and Tang 2009). These could hardly be considered to display ligamentous properties. In conclusion it seems plausible that the dRUL and pRUL work as reins to stabi-lise the DRU joint during loaded and unloaded pronation and supination and that the insertion into the fovea of the ulna is functionally the cardinal attach-ment of these ligaments. When it comes to ulnocarpal stability, data are sparse. The sECU, UT and UL (Fig 9-10) ligaments are thick bundles of longitudinal fibres running towards the carpus (Ishii et al. 1998a, Nakamura et al. 2001, Sasao et al. 2003) and as the forearm rotates, they tighten, perhaps more in supination (DiTano et al. 2003) and contribute to anteroposterior stability of the ulnar carpus vis-à-vis the ulna (Wiesner et al. 1996). However the incidence and pathomechanisms of such inju-ries are rarely described (Tay et al. 2007).
Figure 10. The DRU joint and TFCC of the right wrist seen from a dorsal viewpoint. A). US: Ulnar styloid process. L: Lunate. T: Triquetrum. B) The TFCC. ECU: ECU sheath with tendon. dRUL: Dorsal radioulnar ligament. pRUL: Palmar radioulnar liga-ment. UT: Ulnotriquetral ligament. UL: Ulnolunate ligament. Also included in the pic-ture SRL: Short radiolunate ligament.
L T
US pRUL
dRUL
ECU
UL UT
SRL
A) B)

CONNECTIONS ABOUT THE DISTAL ULNA
20
Figure 11. Coronal cross section of the DRU joint. The deep insertion of the RULs into the fovea is magnified. MH: Meniscus homologue, loose connective tissue enclosing the styloid.
4. Dynamic stabilisers of the DRU and UC connections Once again it must be emphasised that joint stability is dependent on several fac-tors. Perhaps the most important and the most difficult to isolate in the labora-tory environment is dynamic proprioceptive neuromuscular control involving both the courses of both the individual muscle-tendon units and central nervous reflexes. Little is known about this system, but two muscles have been pointed out as probably being the most important for both DRU and UC joint stability, namely the deep head of the PQ muscle (Gordon et al. 2004) and the ECU muscle via its tendon (Spinner and Kaplan 1970, Gupta et al. 2002), the former only con-tributing to DRU stability whereas the ECU has the potential of stabilising both systems.
MHDeep RUL insertion MH
Ulnar styloid

CONNECTIONS ABOUT THE DISTAL ULNA
21
The effect of malunion on functional outcome
There is no simple correlation between the degree of malunion and functional outcome as measured by various scoring instruments. Various factors such as level of activity (Young and Rayan 2000, Grewal and MacDermid 2007, Gehrmann et al. 2008), concomitant soft tissue injury (see below) and inter-individual anatomical differences can possibly account for some of this variabil-ity. Several studies, however, show a correlation between malunion and func-tional outcome (McQueen et al. 1996, Foldhazy et al. 2007, Grewal and MacDermid 2007, Brogren et al. 2011) especially in adult patients below 50 years of age (Gliatis et al. 2000, Grewal and MacDermid 2007). The malunion (Fig 12) may result in pain at rest and during activity, weakness of grip and joint stiffness in the radiocarpal, midcarpal and forearm joints. In pa-tients with malunion and such complaints, corrective osteotomy of the distal ra-dius may improve functional outcome both in terms of range of motion and scor-ing (af Ekenstam et al. 1985, Ring et al. 2002, Wieland et al. 2005) thus indicat-ing that skeletal anatomy is of importance. Especially interesting is that a dis-abling restriction of pronation or supination can be significantly improved by malunion correction.
Figure 12. A malunited distal radius fracture (Case 11 in Paper I) with shortening and dorsal angulation of the distal radius. Note the possibility for collision between the ulnar head and the lunate (arrow). Pro/supination was limited to 30o/30o.
Injured Injured UninjuredUninjured

CONNECTIONS ABOUT THE DISTAL ULNA
22
Techniques of corrective osteotomy of the distal radius An extraarticular malunion from a dorsally displaced distal radius fracture may display both angular deformity (both in the lateral and frontal plane) as well as axial shortening. An additional rotational deformity can be present, but is of un-known significance (Prommersberger et al. 2004). Correction of this deformity is most commonly accomplished either by creating a void (opening wedge osteot-omy) or by removing bone from the radius (closing wedge osteotomy) and simul-taneously performing an ulnar shortening osteotomy to adjust for the resulting length discrepancy. The osteotomy then has to be stabilised, most often by inter-nal fixation either from the dorsal side (Flinkkilä et al. 2000, Ring et al. 2002) or the palmar side (Prommersberger and Lanz 2004). If an opening wedge osteotomy is made, common practice is to fill the void with autologous bone from the iliac crest (Ring et al. 2002, Krukhaug and Hove 2007). This additional pelvic surgery, however, is associated with donor site morbidity still 1 year after surgery (Silber et al. 2003, Sasso et al. 2005). In order to avoid this, several bone-replacement products are now commercially available with dif-ferent properties. One of them is tricalcium phosphate (TCP), which is available as structural implants. It is resorbed very slowly and has mainly been used in high tibial osteotomy (van Hemert et al. 2004).
Pathomechanisms of TFCC injuries associated with distal radius fractures. When sustaining an extraarticular fracture of the distal radius both bending, compressing, shearing as well as rotational forces may contribute to the pattern of injury (Fernandez and Jupiter 2002b). Previous studies have speculated on distracting forces (Adams et al. 1996) being responsible for TFCC injuries whereas others have hypothesised rotational forces (Palmer 1989) though this has not has been verified experimentally (Heiple et al. 1962). The ulnar inser-tions converge around the ulnar styloid, but the relationship between ulnar sty-loid fractures and patterns of TFCC injuries is unknown. Most investigators have focused on the DRU-stabilising properties of the TFCC. There are reports on the coexistence of a dorsal sECU rupture in combination with an injury to the deep RUL insertion (Melone and Nathan 1992, Adolfsson 1994), indicating possible impact on ulnocarpal stabilising structures as well.

CONNECTIONS ABOUT THE DISTAL ULNA
23
The effect of ligament injuries on functional outcome Several studies have documented a high frequency of ruptures of intracarpal ligaments as well as of the TFCC in displaced distal radius fractures using ar-throscopy for diagnosis (Geissler et al. 1996, Lindau et al. 1997, Richards et al. 1997, Adolfsson and Jorgsholm 1998). Three studies have linked a TFCC injury (of the radioulnar connections) as an independent variable, to poorer clinical out-come after a distal radius fracture (Lindau et al. 2000a, Lindau et al. 2000b, Lindau et al. 2002). These injuries may manifest themselves as ulnar wrist pain at rest and during activity and also the feeling of giving way. In patients with DRU joint instability symptoms, late reinsertion can improve symptoms (Chou et al. 2003, Anderson et al. 2008).
Diagnosis of a TFCC injury 1. Wrist arthroscopy Wrist arthroscopy of the radiocarpal joint has long been considered the gold standard for diagnosing injuries to the TFCC and the method with which other modalities are compared. However, it is invasive and a relatively costly and lim-ited resource. It is further is limited by the fact that the DRU joint and the deep RUL insertions are not directly visualised, but assessed by testing the tension of the radioulnar ligaments and disc with a probe (Lee et al. 2005). 2. MRI MRI visualises soft tissues well. Until now the resolution, distance between slices and slice thickness have not been sufficient to delineate the thin ligaments ap-pertaining to the TFCC (Blazar et al. 2001). New techniques are now emerging and high resolution equipment will probably enhance sensitivity and specificity (Tanaka et al. 2006) and possibly be even better when injecting contrast medium into the radiocarpal joint (Ruegger et al. 2007). 3. Radiology. Some 20-30 years ago wrist arthrography was a common method. It has fallen out of practice because of low accuracy when compared to arthroscopy (Vanden Eynde et al. 1994, Trumble et al. 1997).

CONNECTIONS ABOUT THE DISTAL ULNA
24
4. Computed tomography
This method is only described in assessment of radioulnar laxity. When using CT-scanning to create transverse sections of the DRU joint, the relative positions of the distal radius and ulna to one another can be visualised. Different methods have been proposed to assess whether pathologic subluxation is present in prona-tion and/or supination indicating an injury to the insertions of the radioulnar ligaments. Two studies (Lo et al. 2001, Park and Kim 2008) have compared dif-ferent criteria and both found the radioulnar ratio (RUR) method to be the most reliable one. The method creates a ratio that describes the relative location of the distal radius to the centre of the ulnar head (See below under Methods page 30). 5. Clinical examination A. Injuries to the radioulnar connections Only a few studies have evaluated the correlation between clinical testing and TFCC injury. A radioulnar stress test (Fig 14) in neutral rotation has been found to be reliable (Lindau et al. 2002) and to correlate to a peripheral TFCC injury when compared to arthroscopy (Lindau et al. 2000b). In a cadaveric study this test was the only one, out of three evaluated, to demonstrate significant accuracy in detecting a foveal TFCC lesion (Moriya et al. 2009). B. Injuries to the ulnocarpal connections The only clinical test described is the ulnar fovea sign (Tay et al. 2007). This is simply done with the forearm in neutral rotation by palpating the soft spot be-tween the FCU, pisiform bone, ulnar head and ulnar styloid. If pain is elicited this may indicate injury to the palmar ulnocarpal ligaments.

AIMS OF THIS THESIS
25
AIMS OF THIS THESIS The aims of this thesis were to investigate the effects of distal radius fractures on the distal radioulnar joint and its surrounding soft tissues and their implications for function.
1. In cases of symptomatic malunion:
a. To investigate if TCP bone replacement can be safely used in open-ing wedge osteotomy of the distal radius
b. If previous observations of improved forearm rotation could be veri-fied?
2. To investigate non-invasive ways of detecting acute TFCC injuries. 3. To describe pathomechanisms and patterns of TFCC injury associated with
dorsally displaced distal radius fractures.
4. To investigate the effect of untreated TFCC injuries on functional outcome using modern self-administered questionnaires.

MATERIAL AND SUBJECTS
26
MATERIAL AND SUBJECTS
Cadaveric specimens (Paper III) Donated fresh frozen cadaveric arms, transsected at the mid-humerus, obtained through a non-profitable foundation, were used. The median age of the donors was 53 years (42-72 years). Eight were from females and eight from males. There was no radiographic evidence of previous distal radius or ulnar styloid fracture or DRU joint osteoarthritis in any of the specimens. A radioulnar stress test (Fig 19) (Lindau et al. 2000b, Kim and Park 2008) and an ulnocarpal stability test in neu-tral positions were performed in order to rule out pathologic laxity on the ulnar side of the wrist. The specimens were used in two separate experiments after creating a dorsal wedge in the distal radius; a) one investigating the restraining properties of the TFCC; b) one forcing the TFCC into disruption and recording the injuries in-flicted. (Methods page 33).
Patients 1. Study of corrective osteotomy of the distal radius (Paper I) Seventeen consecutive patients, who had undergone corrective osteotomy of a malunited, dorsally displaced, extraarticular fracture of the distal radius because of significant residual symptoms, were reviewed retrospectively. Mean age of the patients was 56 (21-79 years). 2. Prospective observational study (Papers II and IV) Patients aged 18-50 years with a dorsally- or non-displaced distal radius fracture were included. After six months the patients attended a follow-up visit. The main author then performed a radioulnar stress test as described below. Another or-thopaedic surgeon was then asked to repeat the test on both wrists. The second

MATERIAL AND SUBJECTS
27
examiner conducted the examination alone with the patient unaware of the re-sults of any of the previous stress tests. The patient was instructed not to engage in any conversation. In four cases there was disagreement between the two exam-iners on stability and these were excluded from the analysis. The study cohort (Fig 13) was then used in two different studies; a) RUR-study: evaluating the correlation between radioulnar stress test performed at six months and the radioulnar ratio both in the acute setting and after six months; b) functional outcome study: evaluating the correlation between the radioulnar stress test and functional outcome.
Figure 13. Flowchart of the prospective cohort of patients with distal radius fractures (Papers II and IV).
3 In vivo confirmation of cadaveric results (Paper V) 20 consecutive patients with a distal radius fracture AO type A2 or A3 (page 31), with an initial dorsal angulation of 20° or more (using the long axis of the radius as a reference), with an intact ulnar styloid or with a concomitant Type 1 fracture were included. Mean age of the patients was 49 years (SD 13, 21-68 years) and three were men.

METHODS
28
METHODS
Functional outcome measurements 1. Disability of the Arm, Shoulder and Hand (DASH) (Papers I and IV) The first, now outdated outcome measures, such as the Gartland-Werley score (designed for distal radius fracture outcome assessment) often combined objective and subjective estimates into one score (Sarmiento et al. 1975). DASH is a region-specific (whole upper extremity) self-administered questionnaire used to assess self-rated upper extremity disability and symptoms (Beaton et al. 2001). In this way disability and function are kept apart and observer bias is reduced. The DASH consists of 30 items (Fig 14) with both specific tasks and general pain es-timates. The sum of the estimates is then transformed into a score between 0 and 100, where zero denotes no disability at all. There are also optional modules for work and sports/music.
Figure 14. Excerpt from the English DASH questionnaire, items 1, 2, 22 and 23
DASH has been translated into many languages, and the Swedish version has been found to be reliable and valid (Atroshi et al. 2000). The DASH score corre-lates strongly with PRWE (Patient-Related Wrist Evaluation) (Wilcke et al.

METHODS
29
2009), which is a more wrist-specific self-administered outcome measure (MacDermid et al. 2000) as well as with PEM (Patient Evaluation Maesure), yet another hand-specific score (Forward et al. 2007).
2. Open questionnaire (Paper IV) In a letter, patients were asked to list the three most difficult tasks to perform with their injured wrist and to separately assess how difficult this task was on a visual analogue scale (VAS) (Fig 15). The design of this questionnaire was in-spired by the Canadian Occupational Performance Measure (Carswell et al. 2004), which in its original form is a structured interview format to assess change in impairments important to the patient. 3. Forearm rotation (Paper I) Measurement of pronation and supination was made using a Baseline® goniome-ter (Fabrication Enterprises, Inc., New York, USA) with the elbow at 90o of flex-ion, supported by an armrest. Two observers performed all measurements, using the same instrument. It has been shown that measurement error is reduced if the same instrument is used, preferably by the same observer (Armstrong et al. 1998). Task 1, in which I experience difficulties due to my injured wrist: Crisscross on the line the extent of the difficulty you experience in performing this task: No difficulty Completely impossible
Figure 15. Part of the open questionnaire used in Paper IV. Patients were asked to list the three most difficult tasks to perform and to grade them on the line.

METHODS
30
Imaging Radioulnar ratio (RUR) (Paper II) CT scanning has been suggested as a method to detect static DRU subluxation, which is suggestive of a TFCC injury affecting radioulnar stability (Lo et al. 2001). Transverse images encompassing the DRU joint were made in both prona-tion and supination and measurements were made on digitized radiographs as outlined in Figure 16 (Lo et al. 2001). Increased laxity in pronation supposedly produces higher values and the inverse applies to supination. Normal values have been calculated from measurements on healthy subjects (Table 1)
Figure 16. The RUR method. The centre of the ulnar head is found and marked on digi-tized radiographs. A line is drawn between the dorsal and volar corner of the sigmoid notch (AB). Perpendicular to this, a line is drawn to the previously determined centre of the ulnar head. D is the point where it intersects with AB. Radioulnar Ratio (RUR) is calculated as AD/AB. Dorsal subluxation of the radius (in supination) gives a smaller ratio and palmar subluxation (in pronation) gives a larger ratio. (Reproduced with the kind permission of Elsevier from Lo et al, J Hand Surg Am, 26: 236-43).
Table 1 – Normal values of RUR.
Supination Pronation No of 95% CI 95% CI wrists Lo et al. 2001 0.19 - 0.55 0.50 - 0.71 13 Park and Kim 2008 0.28 - 0.52 0.48 - 0.86 45
A
B CD RUR =
ADAB

METHODS
31
Injury classifications 1. Distal radius fracture classification (Papers II, IV and V) Distal radius fractures were classified according to the AO classification system (Müller et al. 1994), but subgroups were limited to obtain reliable classification data (Ploegmakers et al. 2007) This divides the fractures into A: extraarticular. B: partially intraarticular (e.g. Barton type fractures). C: both extra- as well as intraarticular. 2. Ulnar styloid fracture classification (Papers II-V) Ulnar styloid fractures were classified on PA radiographs into three different types (Fig 17) depending on their relation to a fracture through the base (Type 2 fracture). This is a modification of a previously proposed classification (Fernandez and Jupiter 2002a) which takes the anatomical insertions of the TFCC into consideration. The base fracture is defined such that it appears likely that the fracture must involve the area of the deep RUL insertions. Thereby a displaced base fracture most likely involves disruption of the foveal insertions of the TFCC.
Figure 17. Classification of ulnar styloid fractures, palmar view. Type 1: Distal to the base where superficial fibres of the TFCC insert as well as the dorsal UT ligament (Sasao et al. 2003). Type 2: Base fracture: goes through a line perpendicular to the ulnar shaft and into the proximal limitation of the fovea, but does not involve the articular surface of the ulnar head. Type 3: Proximal to a Type 2 fracture.
MH sECU

METHODS
32
3. TFCC injury classification (Papers III and V) The most widely used classification system for TFCC lesions was proposed by Palmer and includes both traumatic (Class 1 lesions, Fig 18) and degenerative (Class 2 lesions) (Palmer 1989). This was used when applicable; other lesions were recorded using drawings.
Figure 18. The Palmer classification of traumatic TFCC lesions (Class 1). Dorsal view of the right wrist. Classes 1A-1D. L: Lunate. T: Triquetrum.
Radioulnar stress test (Papers II -IV) A radioulnar stress test aims to test radioulnar laxity. Laxity varies between in-dividuals and it is therefore important to compare the findings with the contra-lateral side, if this is uninjured. The test used in our studies was done in neutral rotation only, with the elbow resting on a table. It was carried out by stabilising the carpus to the radius with one hand then gripping the ulnar head between the

METHODS
33
thumb and index finger of the other hand after which the ulnar head was moved in both dorsal and palmar directions (Fig 19). Laxity was graded as 0 if there was a firm end-point resistance in both directions and as 1 if such an end-point was absent. There is a strong correlation between pathologic laxity (or a positive test) and injuries to the peripheral insertions of the TFCC (Lindau et al. 2000a, Moriya et al. 2009).
Figure 19. Radioulnar stress test. The forearm is placed in neutral rotation in a relaxed position with support under the elbow. The distal radius including potential fracture fragments is stabilised to the carpus with one hand encasing the radial side to eliminate rotational movements (A). With the other hand, the ulnar head is gripped and translated vis-à-vis the radius and carpus (B+C). Presence or absence of a firm (or hard) end-point in both directions is noted. Since physiologic (normal) laxity varies between healthy subjects it is important to compare the injured wrist to the contralateral, healthy side.
Cadaveric testing (Paper III) The specimens were divided between two experiments. In each experiment a dor-sal open wedge osteotomy was made in the distal radius proximal to the DRU joint to mimic an extraarticular distal radius fracture with dorsal comminution.
1. TFCC restraint experiment The wedge created in the distal radius was 50°. With the forearm in neutral rota-tion and the elbow resting on a digital scale the hand of the specimen was dorsi-flexed 90o. Pressure was applied with the palm of the investigator’s hand against the palm of the specimen’s hand. A lateral radiograph was obtained and reading
A B C

METHODS
34
of the scale was recorded by a separate observer. The soft tissues were then stepwise severed in the following order: (1) Firstly the floor of the ECU tendon sheath was sharply dissected off its ulnar groove and separated sharply from the dorsal radioulnar ligament. (2) Secondly the palmar DRU joint capsule was transversely incised over the ulnar head and the foveal insertions of the TFCC were sharply dissected from it. After each step pressure was reapplied and a lat-eral radiograph obtained. Dorsal angulation was then measured on digitized ra-diographs. 2. TFCC injury experiment A 25° dorsal wedge was created in the distal radius. The wrist was then posi-tioned in dorsiflexion and the forearm in neutral rotation on a table and axial pressure applied along the forearm (Fig 20). The pressure was gradually in-creased until the soft tissues on the ulnar side audibly or visibly ruptured. The ligaments on the ulnar side were then dissected and injuries recorded.
US ECU
Figure 20. The TFCC is forced into rupture. The ulnar head is bald. Note the ECU tendon sheath torn out of its groove in the distal ulna. US: ulnar styloid with a Type 1 fracture. Bold arrow: longitudinal force applied to the forearm.

METHODS
35
Surgical procedures
1. Corrective osteotomy of the distal radius
(Paper I) An opening wedge osteotomy was performed in all patients. Ten patients were osteotomised from a dorsal approach and 7 from a palmar. Cut pieces of TCP were fitted into the gap created and the osteotomy stabilised with a plate and screws.
2. Wrist arthroscopy (Paper V) Arthroscopy was performed using conventional longitudinal traction, utilising standard 3/4 and 6R portals for the radiocarpal joint and a radial midcarpal por-tal for inspection of the midcarpal space. A probe was used from accessory portals to assess ligament integrity and tension. Presence of injuries within the first car-pal row was classified according to Geissler into Grades I-IV (Geissler et al. 1996). Classification of TFCC lesions is described above.
3. Ulnopalmar exploration of the TFCC (Papers III and V) A lazy S-shaped incision was made with its centre at the dome of the ulnar head, its distal limb in line with the ulnar styloid and its proximal limb just ulnar to the FCU tendon (Fig 21). The superficial branch of the ulnar nerve was identified and protected. The retinaculum was split longitudinally ulnar to the FCU and consequently the palmar capsule with potential ruptures as well as the palmar part of the TFCC became visible. Dissection was then carried to the ECU tendon sheath and dorsal TFCC injuries identified. The injuries were then recorded in a protocol, one for each specimen or patient.

METHODS
36
Figure 21. Ulnopalmar exploration of the TFCC. A) Lazy-S shaped incision. B) Sen-sory branch of the ulnar nerve identified. C) After splitting the flexor retinaculum, ac-cess to the palmar capsule is gained under which the palmar parts of the TFCC are visu-alised. Further dissection dorsally gives easy access to the subsheath of the ECU.
Bald ulnar head test (Paper V) The test was performed under anaesthesia before stabilising the distal radius fracture. The hand was brought into dorsiflexion and light pressure applied to the palm in order to reproduce maximum fracture displacement. In a lateral fluoroscopic view it was assessed whether any carpal bones projected distal to the dome of the ulnar head, in a sector created between the extension of the dorsal and palmar border of the cortex of the ulnar head shaft. The test was judged posi-tive when no carpal bones were in this sector in a lateral projection (Fig 22).
A. B. C.

METHODS
37
Figure 22. Bald ulnar head test performed under general anaesthesia, before stabilising the distal radius fracture. The hand is forced into dorsiflexion to reproduce maximum fracture displacement. In fluoroscopy, using a lateral projection, it is assessed whether any carpal bones project over the dome of the ulnar head in a sector (s) created between the extensions of the cortices of the distal ulna. A. Test positive. B. Test negative.
s s
s
A B

STATISTICAL METHODS
38
STATISTICAL METHODS For continuous variables such as RUR-values, age, radiographic parameters Stu-dent’s T-test was used: paired when appropriate. The Mann-Whitney U-test was used either when numbers were small or distribution skewed. The Shapiro-Wilk test was used to assess normality. This means that DASH can either be analysed with the Student’s t-test (Paper I) or the Man-Whitney U-test (Paper IV) depend-ing on the distribution of variables. The general assumption of both analyses is that the individual steps of the scale are equal. For paired non-normally distrib-uted data the Wilcoxon signed rank test was used. Fisher’s exact test was used for 2x2 tables. Confidence intervals for the non-parametric analyses (Paper IV) were calculated by stepwise modification of the estimate (McKean and Ryan JR 1977, Casella and Berger 1990). Inter-rater agreement of laxity testing (Paper II) was calculated using the kappa-value and graded as outlined in Table 2 (Altman 1991). Table 2 – Grading of inter-rater agreement
Value of Κ Strength of agreement
< 0.20 Poor
0.21-0.40 Fair
0.41-0.60 Moderate
0.61-0.80 Good
0.81-1.00 Very good

RESULTS
39
RESULTS
Effects of corrective osteotomy on outcome All but one osteotomy healed uneventfully but with a mean longitudinal subsi-dence of 1.2 mm (range 0-3 mm, 95% CI 0.8 to 1.7, p<0.0001) and osteolytic zones were seen around the TCP implant 8 weeks after implantation in 10/14 cases. Three improved less than 10 points in DASH. In the 13/17 patients that com-pleted both DASH questionnaires, score improved from a mean of 52 (S.D. 22, range 80 to 18) preoperatively to 30 (SD 21, range 72 to 0) 6 months postopera-tively (95% CI 7 to 36, p=0.008). Changes in range of motion are displayed in Ta-ble 3. The major preoperative impairments (extracted from DASH) were: difficul-ties in opening a lid or a heavy door and in carrying heavy objects, as well as gen-eral pain and weakness during activity.
Table 3 – Range of motion
Pronation [deg]
Supination[deg]
Preop median (range) 71 (30 to 90) 61 (15 to 90)
Postop* median (range) 79 (60 to 90) 78 (70 to 90)
p-value p=0.03 p=0.01
* After 6 months
Non-invasive diagnosis of foveal TFCC injury 1. Radioulnar stress test (Paper II) The distribution of radioulnar stress test results at the six-month follow-up is displayed in Table 4. There was agreement between the independent investiga-tors in 44/48 cases. In four cases there was no agreement. Inter-rater agreement was calculated as a kappa-value of 0.84 (95% CI 0.68 to 0.99); values >0.8 are rated as very good (Table 2).
RESULTS
40
Table 4 – Outcome of radioulnar stress test
Examiner 1*
Stable Lax
Stable 21 3 Examiner 2 Lax 1 23
*Author 2. Radioulnar ratio (Paper II) The wrists were grouped in concordance with the results of the radioulnar stress test. No differences were seen between the different groups at 6 months (Table 5). The acute RUR-measurements of the lax wrists were compared to their own un-injured side. The mean RUR-value at two weeks in pronation was 0.61 (SD 0.13) and in supination 0.43 (SD 0.09). Comparison with the contralateral uninjured side showed no sig-nificant difference in pronation (p=0.8) or supination (p=0.2).
Table 5 – RUR measurements at 6 months Uninjured
wrists n=44
Mean (SD)
Stable wrists
n=21/44 Mean (SD)
Lax wrists
n=23/44 Mean (SD)
Diff lax- unin-jured wrist
n=23/44 Mean (95% CI)
Diff stable-lax wrist n=44
Mean (95% CI)
Pronation
0.60 (0.11)
0.66 (0.11)
0.61 (0.12)
0.01 (-0.04 to 0.04) p=0.95
0.05 (-0.03 to 0.12) p=0.21
Supination
0.38 (0.10)
0.44 (0.11)
0.40 (0.08)
0.01 (-0.02 to 0.05) p=0.63
0.05 (-0.01 to 0.10) p=0.12
3. Bald ulnar head test (Paper V) Twelve out of twenty patients were subjected to the bald ulnar head test. Pa-tients were grouped according to the extent of palmar injury (see below and Fig 24). A positive bald ulnar head test (Fig 22) was only present in cases of palmar

RESULTS
41
injury Types 2 or 3 (4/12 patients, p=0.002), which were grouped together as ex-tensive types.
Correlation between radioulnar stress test and functional outcome (Paper IV) Again patients were grouped according to the result of the radioulnar stress tests into a lax and a stable group. No significant difference using DASH could be seen between the groups (Table 6) after 2 years or with an open questionnaire after 4-5 years. In the latter both the highest VAS rating (Max VAS) and mean of the two highest rated were compared. In the cohort (see flowchart in Fig 13) one pa-tient underwent a TFCC reconstruction due to DRU instability symptoms 9 months after injury and was therefore not included in the final outcome analysis. However at 6 months this patient’s DASH score was 2.
Table 6 – Functional outcome in different laxity groups
DASH at 6 months
n=38
DASH at 2 years n=40
Max VAS at 4-5 years n=39
Mean VAS of two highest rated
n=39
Stable group (Median, min-max) 4 (0 to 37) 5 (0 to 52) 38 (0 to 93) 32 (0 to 76)
Lax group (Median, min-max) 10 (2 to 50) 2 (0 to 27) 36 (0 to 94) 29 (0 to 76)
Diff* (95% CI)
-5 (-12 to -1) p=0.01
0 (-2 to 5) p=0.86
-8 (-30 to 14) p=0.43
-6 (-23 to 11) p=0.40
*Shifted point estimates (See statistics)

RESULTS
42
TFCC elongation limit 1. Cadaver experiment (Paper III) With the ulnar soft tissues intact the distal fragment could be angulated dorsally a median of 32o (16-34o) from the anatomical position. After dissecting the ECU tendon sheath from its ulnar groove and from its attachments to the dorsal radi-oulnar ligaments, dorsal angulation increased with a median of 8o (p=0.02), or in absolute values to a median of 40o (31-43o). The complete severing of all ulnar insertions of the TFCC enabled the distal fragment to be displaced the whole os-teotomy width, an additional median angulation of 9o (p=0.01). 2. In vivo study (Paper V) Mean dorsal displacement of the fractures was 41o (SD 10o, min-max 26-70o). All (20/20) patients had a rupture of the subsheath of the ECU (sECU). In addition to this 18/20 patients also had different patterns of disruption of the foveal RUL attachments.
Pathomechanisms of TFCC injuries
1. Ulnar styloid fractures and radioulnar laxity (Paper II) Among the 44 cases there were 21 Type 1 ulnar styloid fractures with a mean displacement of 3.2 mm. Nine had healed at follow-up. There was no correlation between a Type 1 ulnar styloid fracture and DRU joint laxity after six months (p=0.60). A fracture through the base of the ulnar styloid (type 2) was present in 3/44 patients. One was initially displaced >2mm and was lax at follow-up. Two of the Type 2 fractures healed. One of these was found to be lax and one to be stable at follow-up. 9/44 patients showed laxity without having an ulnar styloid frac-ture. A minimally displaced fracture (dorsal angulation <10o of the contralateral side and no short-ening of the radius) was present in 4/23 cases with radioulnar laxity at six months. None of these had an ulnar styloid fracture.

RESULTS
43
2. Cadaver experiment (Paper III) When attempting to force the TFCC into rupture nothing happened just by clos-ing the 25o osteotomy gap and leaving the palmar cortex in continuity. It was first when dorsal shearing of the distal fragment occurred that the restraining soft tissues would yield. None of the specimens displayed ruptures of the TFCC insertions into the radius (Palmer 1D), or ruptures of the ulnolunate and ulnotri-quetral ligaments (Palmer 1C) (Fig 18). Different patterns of TFCC injury were seen depending on the type of concomitant fracture of the ulnar styloid. A. Ulnar styloid fractures Type 2. In cases with a Type 2 fracture (2/8 specimens), the whole TFCC complex was displaced dorsally together with the ulnar styloid (Fig 23). In these cases the base fracture audibly (confirmed on x-ray) preceded the subsequent palmar soft tissue disruption.
B. No ulnar styloid fracture or Type 1 fracture In cases of no ulnar styloid fracture (3/8 specimens) or Type 1 fracture (3/8 specimens) the pattern was different. These all displayed a combination of a dor-sal and a palmar injury. On the dorsal side the tissues that were avulsed from the tip of the ulnar styloid contained both superficial horizontal radioulnar fibres
Figure 23. Type 2 ulnar styloid fracture and TFCC disruption. A. Ulnopalmar view. B. Transverse view.
ECU
ECU

RESULTS
44
and fibres running longitudinally to the dorsoulnar aspect of the triquetrum. Separate from this was the floor of the ECU tendon sheath, which was also torn from its ulnar groove (Fig 20). Rupture of the foveal insertion of the RULs appeared to start on the palmar side and progress dorsally. In all cases some dorsal foveal fibres remained attached (Fig 24).
Figure 24. Ulnopalmar view of a right wrist. Various patterns of palmar injury observed in specimens with no or with a Type 1 ulnar styloid fracture. In addition to these injuries an sECU injury was present. A. Hole in the ulnopalmar corner. Deep RUL insertion par-tially ruptured (1/8 specimens). B. No ulnar styloid fracture (2/8 specimens). Only some dorsal fibres remained. C. Type 1 ulnar styloid fracture (3/8 specimens). Only some dorsal fibres remained.
3. In vivo study (Paper V) Only patients with an intact ulnar styloid or a Type 1 fracture were included in this study. All patients (20/20) displayed a dorsal injury as described above. Two patients did not have additional palmar injury. When reviewing the protocols the palmar injuries (18/20 cases) fell into three different types depending on the ex-tent of disruption of the foveal fibres of the RULs (Fig 25). There were nine Type 1 injuries, seven Type 2 injuries and two Type 3 injuries. 11/20 patients also underwent wrist arthroscopy (Table 7). The extent of the palmar injury was impossible to assess from radiocarpal viewing and working portals.
A. B. C.

RESULTS
45
Type 1 Type 2 Type 3
Uln
opal
mar
vie
w
Tran
sver
se v
iew
Palmar hole in axilla between ulnar styloid and ulnar head Foveal fibres partially ruptured
Complete palmar hori-zontal disruption Some dorsal fibres still attached to the fovea (arrow)
Complete palmar hori-zontal disruption Ulnar head devoid of soft tissue attachments
Figure 25. Staging of palmar injuries, right wrist. US: Ulnar styloid. ECU: Extensor carpi ulnaris tendon.
U US US ECU ECU ECU
pRUL pRUL pRUL

RESULTS
46
Table 7 – Findings of wrist arthroscopy and ulnopalmar exploration in 11/20 cases.
Case sECU1 Palmar
injury1 Class 1A2
Class 1C2
Class 1D2
S-L3 L-T3
10 Yes Type 2 II 11 Yes Type 2 III 12 Yes Type 1 Yes 13 Yes Type 1 II 14 Yes Old II* 15 Yes Type 1 II II 16 Yes Type 1 17 Yes Type 2 Yes Old III* 18 Yes Type 1 Yes 19 Yes Type 1 I 20 Yes Type 1
1Open exploration (Fig 25) 2Palmer classification (Fig 18) 3Grading according to Geissler (Grade I-IV) *Absence of capsular bleeding, disappearance of synovial tuft.

DISCUSSION
47
DISCUSSION
How can skeletal malunion limit forearm rotation? Limitation of forearm rotation correlates with poor clinical outcome (Flinkkila et al. 2000). Our finding of increased active forearm rotation after skeletal correc-tion of a malunion is in concordance with the findings of others (Fernandez 1982, af Ekenstam et al. 1985, Brown and Bell 1994, Ring et al. 2002). There may be several reasons, possibly combined, that contribute to this. This has been visual-ised in biomechanical studies using cadaveric specimens.
First of all despite the low degree of congruency between the head of the ulna and sigmoid notch, incongruency itself (Fig 26) may limit the range of motion, especially at the endpoints (Kihara et al. 1996, Ishikawa et al. 2005, Fraser et al. 2009). In fact the torque needed to reach end positions increases with increasing simulated dorsal malunion (Hirahara et al. 2003). This restriction may be ampli-fied when the deformity is increased by factors such as translation and shortening of the radius depending on the anatomic type of DRU joint (Fraser et al. 2009). An isolated dor-sal angulation of about 20o (with the radial shaft as a reference) seems to significantly increase the risk for im-paired forearm rotation (Kihara et al. 1996). Secondly, altered tension of the soft
tissues due to bony malunion may restrict motion. Examining rotational im-pairment, using a cadaveric malunion model (Fraser et al. 2009), demonstrated that restricted forearm rotation increased significantly by sectioning of the TFCC, but not to normal values (Hirahara et al. 2003). It seems likely that an osteotomy both restores joint congruity and normalises strain in the surrounding soft tissues.
Figure 26. Schematic representation of DRU incongruity. A. Normal situa-tion. B. Angulation and/or shortening of the sigmoid notch (SN) vis-à-vis the ulnar head (U) causing malalign-ment.
DISCUSSION
48
What do we know about the patterns and pathomechanisms of TFCC injuries? The predominating TFCC injury classification used stems from Palmer’s work (Palmer 1989). His classification (Fig 18) was based on a retrospective review of 75 cases who underwent open surgery from the dorsal side over a 10-year period. It is not stated whether any of the patients reviewed in this work also sustained an associated distal radius fracture. Most studies, using arthroscopy, of TFCC lesions in distal radius fractures have described their findings according to this classification (Geissler et al. 1996, Lindau et al. 1997, Richards et al. 1997). Some lesions, such as a rupture of the subsheath of the ECU (sECU) are not covered in this classification. Melone and Nathan (1992) observed other patterns in 42 patients with traumatic lesions of the TFCC, also subjected to open dorsal surgery. They suggested a pe-ripheral detachment of the TFCC from the fovea and ulnar styloid to be the first stage of injury followed by an sECU detachment (Stage II), UT and UL injury (Stage III) and then a disruption of the interosseous L-T ligament (Stage IV). Dis-tal radius fractures are not mentioned in this paper either. This attempt to refine Palmer’s classification, however, has passed almost unnoticed. Since the emerging era of wrist arthroscopy the inability to fit all the findings into the Palmer classification has been noticed (Adolfsson 1994, Estrella et al. 2007) and a sub-classification of peripheral TFCC lesions has been proposed, di-viding peripheral lesions into deep and superficial (Atzei 2009). It is possible that the dorsal injury that we have identified as an sECU disruption is what others have classified as a disruption of the superficial limb of the dRUL (Moritomo et al. 2010). What we have found in both the cadaver experiments (Paper III) and a clinical study (Paper V), is that the patterns of TFCC injury in dorsally displaced distal radius fractures probably differ depending on the type of associated ulnar styloid fracture. Dorsal sECU separation from the dRUL and the distal ulna can coexist with a foveal fibre detachment. In fact, with the exception of Type 2 ulnar styloid fractures, it appears likely that this sECU injury is the first stage of injury since it was universally present in both cadaver specimens and clinical cases. This is further supported by other similar observations (Protopsaltis and Ruch 2010). 1. Pathomechanisms of an sECU injury The carpus dorsiflexes and possibly rotates relative to the ulna in a fall on an outstretched hand. For disruption to take place, the course of ECU with its sub-sheath must ‘bowstring’ relative to the dRUL and distal ulna (Fig 27). Simulta-neous contraction of the ECU may possibly enhance this bowstring effect.

DISCUSSION
49
In the cadaver study (Paper III) we observed that there was soft tissue with or without an attached Type 1 fracture fragment that was separated from both the sECU and the dRUL running towards the carpus. It seems probable that this represents fibres running in a direction different from the sECU. Sasao et al have described ligamentous components, histologically different from the tissue of the sECU, which they tentatively named the dorsal ulnotriquetral (dUT) ligament. It originates on the styloid process and inserts into the dorsal side of the tri-quetrum, in contrast to the sECU, which runs from the dorsal groove of the ulna and the styloid process and ends in the base of the fifth metacarpal (Sasao et al. 2003).
Figure 27. Possible mechanism of ECU subsheath rupture, dorsoulnar view. A. Ulnar styloid intact. B. Type 1 fracture of the ulnar styloid attached to the dUT ligament. When the carpus displaces dorsally with the distal radius fragment, the ECU is torn out of its groove and the tendon sheath separates from the rest of the TFCC. R: Radius. U: Ulna. Tr: Triquetrum. ECU: Extensor carpi ulnaris tendon with its subsheath. dRUL: Dorsal radioulnar ligament. Bold arrows: ulnolunate and ulnotriqetral ligaments pulling out foveal TFCC insertions
2. Pathomechanisms of deep foveal RUL fibre disruption The various patterns of palmar injury found in both the cadaveric experiments and the clinical study suggest a progressive pullout of the deep RUL insertion from the fovea (Fig 28), starting on the palmar side and continuing dorsally. A complete foveal detachment was only seen in 2 cases that both involved motor vehicle accidents, suggesting that frank dislocations of the DRU joint are rare. The palmar patterns also suggest that the disruption simultaneously extends radially on the palmar side, rupturing the DRU joint capsule, that has a possible stabilising role (Kleinman and Graham 1998).
ECU ECU
Tr Tr
U U
A. B.
dRUL dRUL
RR
DISCUSSION
50
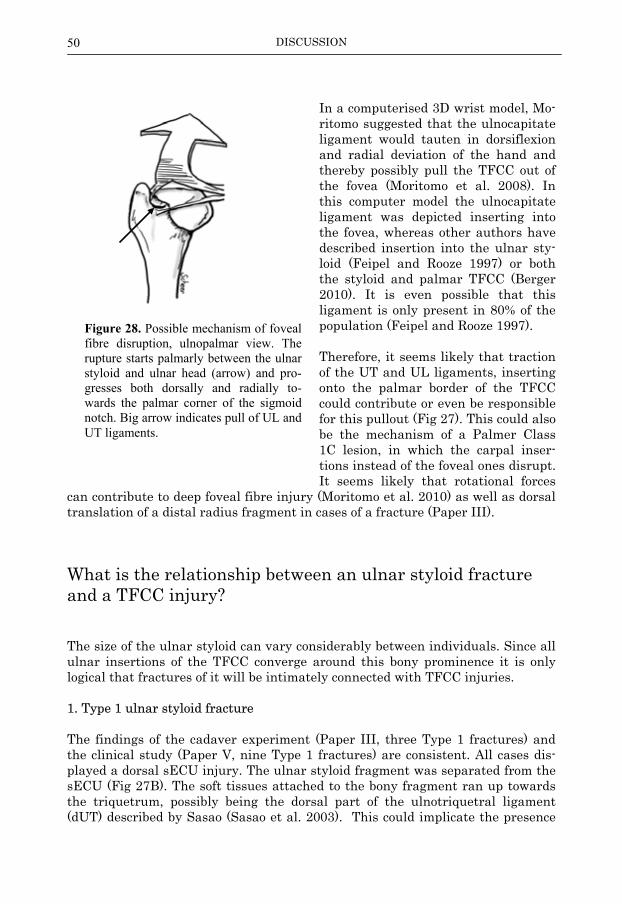
In a computerised 3D wrist model, Mo-ritomo suggested that the ulnocapitate ligament would tauten in dorsiflexion and radial deviation of the hand and thereby possibly pull the TFCC out of the fovea (Moritomo et al. 2008). In this computer model the ulnocapitate ligament was depicted inserting into the fovea, whereas other authors have described insertion into the ulnar sty-loid (Feipel and Rooze 1997) or both the styloid and palmar TFCC (Berger 2010). It is even possible that this ligament is only present in 80% of the population (Feipel and Rooze 1997). Therefore, it seems likely that traction of the UT and UL ligaments, inserting onto the palmar border of the TFCC could contribute or even be responsible for this pullout (Fig 27). This could also be the mechanism of a Palmer Class 1C lesion, in which the carpal inser-tions instead of the foveal ones disrupt. It seems likely that rotational forces
can contribute to deep foveal fibre injury (Moritomo et al. 2010) as well as dorsal translation of a distal radius fragment in cases of a fracture (Paper III).
What is the relationship between an ulnar styloid fracture and a TFCC injury? The size of the ulnar styloid can vary considerably between individuals. Since all ulnar insertions of the TFCC converge around this bony prominence it is only logical that fractures of it will be intimately connected with TFCC injuries. 1. Type 1 ulnar styloid fracture The findings of the cadaver experiment (Paper III, three Type 1 fractures) and the clinical study (Paper V, nine Type 1 fractures) are consistent. All cases dis-played a dorsal sECU injury. The ulnar styloid fragment was separated from the sECU (Fig 27B). The soft tissues attached to the bony fragment ran up towards the triquetrum, possibly being the dorsal part of the ulnotriquetral ligament (dUT) described by Sasao (Sasao et al. 2003). This could implicate the presence
Figure 28. Possible mechanism of foveal fibre disruption, ulnopalmar view. The rupture starts palmarly between the ulnar styloid and ulnar head (arrow) and pro-gresses both dorsally and radially to-wards the palmar corner of the sigmoid notch. Big arrow indicates pull of UL and UT ligaments.

DISCUSSION
51
of a much disputed (Palmer and Werner 1981, Garcia-Elias 1998, Nakamura et al. 2001) ulnar collateral ligament of the wrist. As stated above, this is probably an injury preceding foveal disruption 2. Type 2 ulnar styloid fractures Correlation between a base fracture with ≥2 mm initial displacement and acute or chronic DRU joint instability has been reported (May et al. 2002) and in cases of painful non-union of a Type 2 fracture, DRU joint instability is common (Hauck et al. 1996). The cadaver experiment (Paper III) produced two Type 2 fractures. Both of these displayed common features (Fig 23):
a. The base fracture preceded the TFCC injury b. There was no dorsal injury, instead the TFCC displaced as a unit together
with the ulnar styloid with the injury starting on the palmar side.
Figure 29. Proposed mechanism of Type 2 ulnar styloid fracture and TFCC disruption, right wrist dorsoulnar view. Pull of palmar ulnocarpal ligaments (UT, UL and ulnocapi-tate) exceeds the bowstringing of the ECU and failure starts on the palmar side. The Type 2 fragment displaces with the whole TFCC. R: Radius. U: Ulna. Tr: Triquetrum. ECU: Extensor carpi ulnaris.
Since this pattern deviates from the pattern seen with intact styloid or a Type 1 fracture it appears likely that forces act differently in these cases. The reasons may be variations in the anatomical properties of the ulnar styloid and the
ECU
Tr
Ulnocapitate lig
U
R

DISCUSSION
52
TFCC, different force vectors or by a combination of these factors. A possible mechanism might be a pull by the ulnocapitate ligament mentioned above, which is inserted in the styloid . Excessive strain in this could be responsible for both the base fracture and subsequent TFCC displacement (Fig 29). It appears in con-clusion that the strain in the palmar ulnocarpal ligaments exceeds that of the dorsal TFCC components so that failure starts on the palmar side. Aspects on repair of a TFCC injury
If soft tissue repair is indicated it ap-pears likely that precision addressing all injured components would improve out-come. In cases of Type 2 fracture a com-pression osteosynthesis between the base fragment and the ulnar head is eas-ily performed e.g. with smooth k-wires and a tension band (Fig 30), which effec-tively reduces all components of the TFCC and permits early mobilisation. It should however be recognised that, in the absence of a Type 2 fracture, an sECU lesion may be present without gross laxity of the DRU joint and that instability of this joint after a Colles’ fracture will always imply a palmar in-jury. There are thus two components of the TFCC injury that need to be ad-dressed: 1. The deep RUL fibres that needs reat-
tachment to the entire foveal foot-print (Fig 31A).
2. In cases of an intact ulnar styloid or a
Type 1 fracture, an sECU separation that should be reattached to the dRUL and possibly to the distal ulna (Fig 31D).
The importance of reattaching a Type 1 ulnar styloid fragment, or its appertain-ing soft tissues is unclear. Repair of all peripheral tears of the TFCC can be performed through the previ-ously described ulnopalmar approach (Fig 21) and is outlined in Figure 31. The
Figure 30. Tension band osteo-synthesis of a type 2 ulnar styloid fracture.

DISCUSSION
53
arthrotomy is made dorsal to the UT ligament. Sutures through bone tunnels spaced apart (de Araujo et al. 1996, Anderson et al. 2008) are preferred to suture anchors (Chou et al. 2003, Moritomo et al. 2010), since anchors give a one-point fixation and fitting two separate anchors into the fovea can be difficult.
Figure 31. Suggested repair of both a dorsal and a palmar TFCC injury. A: Footprint of intended foveal repair, which is cleared from synovial tissue B: Transosseous bone tun-nels are drilled into the fovea. C: Sutures passed through bone tunnels. Suture 1 ties the deep RUL fibres to the fovea. Suture 2 may be optional but completes the footprint re-construction by reducing the ulnopalmar-most corner. D: sECU repair. Tethering of the ECU itself must be avoided. Arthrotomy and ECU tendon sheaths are closed.
The sECU injury repair can be made via the same approach (Fig 31D). The repair can be arthroscopy-assisted or by open surgery. The safety of an all arthroscopic repair can be questioned because of the close proximity of the dorsal branch of the ulnar nerve, which varies in its course between individuals (Waterman et al. 2010).
A. B.
C. D.
Suture 2
Suture 1
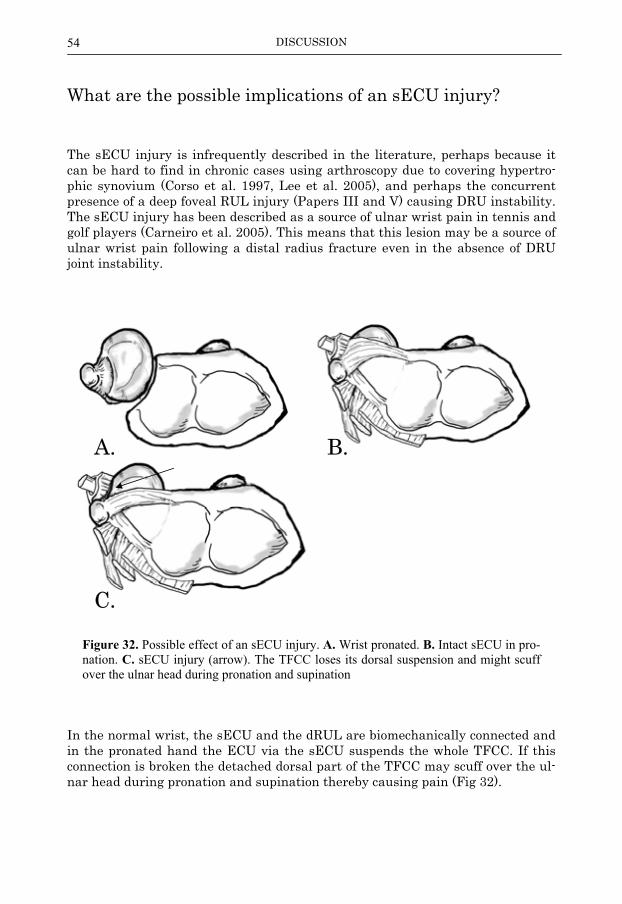
DISCUSSION
54
What are the possible implications of an sECU injury? The sECU injury is infrequently described in the literature, perhaps because it can be hard to find in chronic cases using arthroscopy due to covering hypertro-phic synovium (Corso et al. 1997, Lee et al. 2005), and perhaps the concurrent presence of a deep foveal RUL injury (Papers III and V) causing DRU instability. The sECU injury has been described as a source of ulnar wrist pain in tennis and golf players (Carneiro et al. 2005). This means that this lesion may be a source of ulnar wrist pain following a distal radius fracture even in the absence of DRU joint instability.
Figure 32. Possible effect of an sECU injury. A. Wrist pronated. B. Intact sECU in pro-nation. C. sECU injury (arrow). The TFCC loses its dorsal suspension and might scuff over the ulnar head during pronation and supination
In the normal wrist, the sECU and the dRUL are biomechanically connected and in the pronated hand the ECU via the sECU suspends the whole TFCC. If this connection is broken the detached dorsal part of the TFCC may scuff over the ul-nar head during pronation and supination thereby causing pain (Fig 32).
A. B.
C.

DISCUSSION
55
One may thus conclude that if injuries of both the sECU the deep foveal RUL fi-bres are concurrently present, both need to be addressed as outlined in Figure 31.
Can acute TFCC injuries be detected using non-invasive methods? There are currently three non-invasive methods used in detecting a TFCC injury, two of which are evaluated in this thesis:
1. Clinical examination 2. CT scanning 3. MRI
It must be remembered that in chronic cases the diagnosis of a TFCC injury can be coupled with symptoms to suggest treatment, whereas in acute cases such an association is unclear (Paper IV). 1. Clinical examination DRU joint laxity can be assessed by the radioulnar stress test. This test shows good (Lindau et al. 2002) or very good (Paper II) intra-observer reliability in chronic cases. In a cadaver model this test alone (out of three evaluated) could accurately detect surgically created TFCC detachment (Moriya et al. 2009). A clinical follow-up of patients that underwent diagnostic arthroscopy because of a displaced distal radius fracture, showed a strong correlation between complete peripheral TFCC tear at arthroscopy and a pathologic radioulnar stress test 12 months after injury (Lindau et al. 2000a). Hence, this test is useful in evaluating chronic cases and predicting peripheral RUL disruption. The use of a radioulnar stress test in acute cases can probably only be done on a anaesthetised patient and with a distal radius fracture stabilised, since pain, swelling and instability of distal radius fragments may confound the assessment. The only test described in the literature to evaluate ulnocarpal injuries is the ul-nar fovea sign (Tay et al. 2007). This is simply done with the forearm in neutral rotation by palpating the soft spot between the FCU, pisiform bone, ulnar head and ulnar styloid. If pain is elicited this may indicate injury to the ulnocarpal ligaments.

DISCUSSION
56
2. CT scanning The use of CT scanning in the assessment of DRU joint pathology is widespread. Bony surfaces and subchondral step-offs are well depicted. There are several at-tempts to quantify DRU joint subluxation thereby indirectly disclosing an under-lying peripheral TFCC disruption (supposedly of the RULs stabilising the DRU joint). The Mino criteria, the epicentre method, the congruency method have all been found to be inferior to the RUR method (Lo et al. 2001, Park and Kim 2008) as used in Paper II when it comes to inter- and intra-observer reliability. When we evaluated this method, however, we found it to be of little use in both chronic and acute cases (Paper II). Previously stated normal values (Table 1) en-closed almost all measurements and when grouping was made by means of the radioulnar stress test the RUR method did not contribute further information (Fig 33). Of interest is that normal values of pronation and supination overlap (Table 1).
Stable case Lax case
RUR uninjured 0.29 0.46 RUR injured 0.34 0.49
Figure 33. CT-scans in supination at the six-month follow-up, one from each laxity group. With this method, lower figures are expected in supination with increasing lax-ity. The lax case subsequently underwent a TFCC reconstruction and a peripheral de-tachment of the RULs was verified during surgery. Normal values: see page 30.
It is not surprising, that the momentary subluxation, occasionally perceived by symptomatic patients, cannot be captured in on a CT scan. CT scanning of the DRU joint should therefore be used for indications other than disclosing a sub-luxation, e.g. flatness of the sigmoid notch or malunion.
Stable case Lax case
Uninjured Injured Injured Uninjured

DISCUSSION
57
3. MRI As described in the background section, until recently MRI has lacked the resolu-tion to depict the thin ligaments of the TFCC. Emerging high-resolution tech-niques appear to enhance sensitivity and specificity when compared to wrist ar-throscopy (Tanaka et al. 2006, Magee 2009) although not reaching 90% sensitiv-ity unless adding radiocarpal contrast (Magee 2009). Only one study has de-scribed the use of MRI in acute cases and the imaging findings were not com-pared to wrist arthroscopy (Bombaci et al. 2008). Consequently it is unknown whether this affects sensitivity.
Which patients benefit from an acute TFCC reconstruction? As pointed out several times throughout this thesis, a ligament lesion does not automatically correlate to instability symptoms. The consequence of this is that despite accurate diagnosis of a ligament lesion (e.g. clinical examination, MRI) the risk for surgical overtreatment is obvious. In Paper IV, there was no correla-tion between laxity, assessed by radioulnar stress test and clinical outcome. There are several possible explanations for this:
1. Other factors such as age, level of activity, osseous joint congruency and ability to compensate by neuromuscular control affect outcome.
2. The extent of TFCC injury (Papers III and V) is important 3. The outcome measures used (Paper IV) are not sensitive to instability
symptoms. A. Outcome measures Two previous cohorts of patients participating in three studies (Lindau et al. 2000a, Lindau et al. 2000b, Lindau et al. 2002) showed strong correlation be-tween a pathologic radioulnar stress test and functional outcome assessed with selected parts (Lindau et al. 2000b, Lindau et al. 2002) or the complete (Lindau et al. 2000a) modified Gartland-Werley score (Sarmiento et al. 1975). On the ba-sis of this acute repair of the TFCC is frequently advocated in cases of a pe-rioperative pathologic radioulnar stress test (Ruch et al. 2004, Wulf et al. 2007, Atzei 2010). The correlation between the Gartland-Werley score and DASH is at best moder-ate (Lozano-Calderon et al. 2010). Because of this, comparison between the re-sults in Paper IV and Lindau’s work is cumbersome and we believe that the ex-tensively validated DASH score (Atroshi et al. 2000, MacDermid et al. 2000, Wilcke et al. 2009) more accurately reflects wrist disability.

DISCUSSION
58
One of the cases in Paper IV had a DASH score of 2 after six months, and yet ex-perienced instability symptoms severe enough to opt for surgical TFCC reat-tachment. This raises concern about the conclusions in Paper IV. However, there are other studies that have showed improvement in DASH when evaluating out-come after TFCC reconstruction (Reiter et al. 2008, McAdams et al. 2009, Protopsaltis and Ruch 2010). The symptoms of ulnar wrist instability may vary. Many patients experience pain at rest and during activity and this is probably covered by most outcome measures. If the main symptom is the feeling of giving way (subluxation of the DRU joint), when lifting objects or rotating the forearm under load, then the ef-fect on DASH and similar instruments will be minimal. It is likely that this symptom will be more pronounced at higher activity levels in the absence of pain. B. The magnitude of injury As shown in Papers III and V the extent of a palmar injury may vary. It is possi-ble that this is a factor affecting instability symptoms. Extensive injury can eas-ily be disclosed by the bald ulnar head test (Paper V). C. Conclusions regarding acute repair It appears that most patients do well despite a TFCC injury (Paper IV) since case numbers needed to harm (NNH) on the basis of a radioulnar stress test or a posi-tive MRI finding would be high (20 based on the results in Paper IV) even in a population in the ages 18-50 of age. It is likely, however, that acute repair has greater chance of a better end result than one performed later. To reduce NNH, possible criteria for acute repair include:
1. Patients with a very high level of activity (professional athletes, workers highly dependent on good wrist function).
2. Younger patients, possibly below the age of 30. 3. A positive bald ulnar head test.
Remaining patients are probably better off with physiotherapy to gain neuromus-cular control of ulnar wrist stability. In cases of persistent ulnar wrist symptoms reconstruction can be performed later with good results (Reiter et al. 2008, McAdams et al. 2009, Protopsaltis and Ruch 2010).

CONCLUSIONS
59
CONCLUSIONS
The aim of this thesis was to learn more about periulnar injuries associated with distal radius fractures. The following were found:
1. In cases of symptomatic malunion of a distal radius fracture a corrective osteotomy will improve rotational impairment and disability assessed with DASH. TCP can be used instead of iliac crest bone graft, but there may be more favourable products that do not produce osteolytic zones during con-solidation of the osteotomy.
2. Patterns of a TFCC injury will differ depending on the size or presence of
an associated ulnar styloid fracture.
3. A peripheral TFCC injury may be accompanied by dorsal and palmar inju-ries, both of which should be addressed at repair.
4. The extent of a TFCC disruption to the DRU stabilising fibres inserting
into the fovea can vary. The bald ulnar head test can detect extensive in-jury.
5. In the diagnosis of a TFCC injury, CT scanning to detect pathologic sub-
luxation is of little use in both acute and chronic cases. 6. Pathologic laxity of the DRU joint due to a TFCC injury is common after a
fracture of the distal radius, but does not, in the majority of cases cause significant disability two years or more after injury. There is no doubt that some patients would benefit from an acute reconstruction but selection cri-teria remain unclear.

FUTURE RESEARCH
60
FUTURE RESEARCH As often in research, more questions are raised than answered. Here are some questions that I find particularly interesting: 1. The effects of an sECU injury. What are the effects of this injury on wrist mechanics? In symptomatic patients: what symptoms can be attributed to this and what are the clinical findings? 2. Differentiation of level of activity It is frequently stated in this thesis that level of activity is important for residual symptoms after a distal radius fracture. Can this be quantified? An instrument for assessing activity level could possibly be used in decision making in the man-agement of a distal radius fracture as regards both skeletal and ligament proce-dures. 3. Patterns of TFCC injury in Type 2 ulnar styloid fractures Can the cadaver study finding, that a base fracture exists without a dorsal in-jury, be confirmed vivo? 4. The bald ulnar head test This test should be applicable in Type 2 ulnar styloid fractures and intraarticular fractures. Another possibility would be to randomise (young?) patients into TFCC repair or not in the presence of a positive test. Unfortunately this will probably require a very large number of young patients with a displaced distal radius frac-ture.

ACKNOWLEDGEMENTS
61
ACKNOWLEDGEMENTS There are some people who greatly have contributed to the papers included in this thesis, in sharpening the thesis itself or both. Lars Adolfsson (‘Lasse’), my mentor. He’s so rarely wrong, that I can remember all five times. Never satisfied when reality does not fit into the reigning para-digm, with a healthy distrust towards authorities, reluctant to see himself as one. Vendela, my wife. Very supportive and much loved. Shows a genuine interest towards my research. Saved me by forcing me to Rome when my capacity for sen-sory perception and social interaction became seriously impaired. Per Aspenberg, our professor at the Orthopaedic department. Has taught me a lot about science, first of all the joy of it, and secondly that if a question ‘is of aca-demic interest’ it means that it is highly relevant. Source of ‘Thesis at a glance’, that is often seen in theses in Sweden. Olle Eriksson, statistician at Linkoping University, with an intimate and natu-ral understanding of statistics. Has delivered crucial insights into statistics and elegantly solved problems not covered in Altman’s textbook. Peter Cox, merry Englishman and anaesthesiologist, for language revision my thesis. Listing ‘a smooth golf swing’ as an example of daily activities that re-quires good forearm rotation is one of his contributions. I am very impressed that he actually appears to understand the subject. On the list of people who actually have read this book. Swemac Orthopaedics, a local orthopaedic implant manufacturer that with-out any counter-demands supplied the necessary means for the cadaveric ex-periments, I believe out of sheer curiosity.

REFERENCES
62
REFERENCES
Adams BD, Samani JE, Holley KA. Triangular fibrocartilage injury: a laboratory model. J Hand Surg Am.
1996; 21 (2): 189-93. Adolfsson L. Arthroscopic diagnosis of ligament lesions of the wrist. J Hand Surg Br. 1994; 19 (4): 505-12. Adolfsson L, Jorgsholm P. Arthroscopically-assisted reduction of intra-articular fractures of the distal radius. J
Hand Surg Br. 1998; 23 (3): 391-5. af Ekenstam F, Hagert CG. Anatomical studies on the geometry and stability of the distal radio ulnar joint.
Scand J Plast Reconstr Surg. 1985; 19 (1): 17-25. af Ekenstam F, Hagert CG, Engkvist O, Tornvall AH, Wilbrand H. Corrective osteotomy of malunited fractures
of the distal end of the radius. Scand J Plast Reconstr Surg. 1985; 19 (2): 175-87. Altman DG. Inter-rater Agreement. In: Practical Statistics for Medical Research. Chapman & Hall. London
1991; 403-9. Anderson ML, Larson AN, Moran SL, Cooney WP, Amrami KK, Berger RA. Clinical comparison of
arthroscopic versus open repair of triangular fibrocartilage complex tears. J Hand Surg Am. 2008; 33 (5): 675-82.
Armstrong AD, MacDermid JC, Chinchalkar S, Stevens RS, King GJ. Reliability of range-of-motion measurement in the elbow and forearm. J Shoulder Elbow Surg. 1998; 7 (6): 573-80.
Atroshi I, Gummesson C, Andersson B, Dahlgren E, Johansson A. The disabilities of the arm, shoulder and hand (DASH) outcome questionnaire: reliability and validity of the Swedish version evaluated in 176 patients. Acta Orthop Scand. 2000; 71 (6): 613-8.
Atzei A. New trends in arthroscopic management of type 1-B TFCC injuries with DRUJ instability. J Hand Surg Eur Vol. 2009; 34 (5): 582-91.
Atzei A. Arthroscopic Management of DRUJ Instability Following TFCC Ulnar Tears. In: Arthroscopic Management of Distal Radius Fractures. (Ed. del Pinal F, Mathoulin C, Luchetti R). Springer. Heidelberg 2010; 73-88.
Bade H, Koebke J, Schluter M. Morphology of the articular surfaces of the distal radio-ulnar joint. Anat Rec. 1996; 246 (3): 410-4.
Beaton DE, Katz JN, Fossel AH, Wright JG, Tarasuk V, Bombardier C. Measuring the whole or the parts? Validity, reliability, and responsiveness of the Disabilities of the Arm, Shoulder and Hand outcome measure in different regions of the upper extremity. J Hand Ther. 2001; 14 (2): 128-46.
Berger RA. Wrist Anatomy. In: The Wrist: Diagnosis and Operative Treatment. (Ed. Cooney WP). Lippincott Williams & Wilkins. Philadelphia 2010; 25-76.
Blazar PE, Chan PS, Kneeland JB, Leatherwood D, Bozentka DJ, Kowalchick R. The effect of observer experience on magnetic resonance imaging interpretation and localization of triangular fibrocartilage complex lesions. J Hand Surg Am. 2001; 26 (4): 742-8.
Bombaci H, Polat A, Deniz G, Akinci O. The value of plain X-rays in predicting TFCC injury after distal radial fractures. J Hand Surg Eur Vol. 2008; 33 (3): 322-6.
Brogren E, Hofer M, Petranek M, Wagner P, Dahlin LB, Atroshi I. Relationship between distal radius fracture malunion and arm-related disability: A prospective population-based cohort study with 1-year follow-up. BMC Musculoskelet Disord. 2011; 12 (1): 9.
Brown JN, Bell MJ. Distal radial osteotomy for malunion of wrist fractures in young patients. J Hand Surg Br. 1994; 19 (5): 589-93.
Carneiro RS, Fontana R, Mazzer N. Ulnar wrist pain in athletes caused by erosion of the floor of the sixth dorsal compartment: a case series. Am J Sports Med. 2005; 33 (12): 1910-3.
Carswell A, McColl MA, Baptiste S, Law M, Polatajko H, Pollock N. The Canadian Occupational Performance Measure: a research and clinical literature review. Can J Occup Ther. 2004; 71 (4): 210-22.
Casella GC, Berger RL. Inverting a test statistic. In: Statistical Interference. (Ed. Casella G, Berger RL). Brooks/Cole Pub. Co. Pacific Grove, Calif. 1990; 406-13.
Chou KH, Sarris IK, Sotereanos DG. Suture anchor repair of ulnar-sided triangular fibrocartilage complex tears. J Hand Surg Br. 2003; 28 (6): 546-50.
Corso SJ, Savoie FH, Geissler WB, Whipple TL, Jiminez W, Jenkins N. Arthroscopic repair of peripheral avulsions of the triangular fibrocartilage complex of the wrist: a multicenter study. Arthroscopy. 1997; 13 (1): 78-84.
de Araujo W, Poehling GG, Kuzma GR. New Tuohy needle technique for triangular fibrocartilage complex repair: preliminary studies. Arthroscopy. 1996; 12 (6): 699-703.

REFERENCES
63
De Smet L, Fabry G. Orientation of the sigmoid notch of the distal radius: determination of different types of the distal radioulnar joint. Acta Orthop Belg. 1993; 59 (3): 269-72.
DiTano O, Trumble TE, Tencer AF. Biomechanical function of the distal radioulnar and ulnocarpal wrist ligaments. J Hand Surg Am. 2003; 28 (4): 622-7.
Estrella EP, Hung LK, Ho PC, Tse WL. Arthroscopic repair of triangular fibrocartilage complex tears. Arthroscopy. 2007; 23 (7): 729-37, 37 e1.
Feipel V, Rooze M. The capsular ligaments of the wrist. Eur J Morphol. 1997; 35 (2): 87-94. Fernandez DL. Correction of post-traumatic wrist deformity in adults by osteotomy, bone-grafting, and internal
fixation. J Bone Joint Surg Am. 1982; 64 (8): 1164-78. Fernandez DL, Jupiter JB. Acute and Chronic Derangement of the Distal Radioulnar Joint Associated with
Distal Radius Fracture. In: Fractures of the Distal Radius. (Ed. Fernandez DL, Jupiter JB). Springer-Verlag. New York 2002a; 367-99.
Fernandez DL, Jupiter JB. Extraarticular Bending Fractures. In: Fractures of the Distal Radius. (Ed. Fernandez DL, Jupiter JB). Springer-Verlag. New York 2002b; 129-86.
Flinkkilä T, Raatikainen T, Kaarela O, Hamalainen M. Corrective osteotomy for malunion of the distal radius. Arch Orthop Trauma Surg. 2000; 120 (1-2): 23-6.
Foldhazy Z, Tornkvist H, Elmstedt E, Andersson G, Hagsten B, Ahrengart L. Long-term outcome of nonsurgically treated distal radius fractures. J Hand Surg Am. 2007; 32 (9): 1374-84.
Forward DP, Sithole JS, Davis TR. The internal consistency and validity of the Patient Evaluation Measure for outcomes assessment in distal radius fractures. J Hand Surg Eur Vol. 2007; 32 (3): 262-7.
Fraser GS, Ferreira LM, Johnson JA, King GJ. The effect of multiplanar distal radius fractures on forearm rotation: in vitro biomechanical study. J Hand Surg Am. 2009; 34 (5): 838-48.
Friedman SL, Palmer AK, Short WH, Levinsohn EM, Halperin LS. The change in ulnar variance with grip. J Hand Surg Am. 1993; 18 (4): 713-6.
Fu E, Li G, Souer JS, Lozano-Calderon S, Herndon JH, Jupiter JB, et al. Elbow position affects distal radioulnar joint kinematics. J Hand Surg Am. 2009; 34 (7): 1261-8.
Garcia-Elias M. Soft-tissue anatomy and relationships about the distal ulna. Hand Clin. 1998; 14 (2): 165-76. Gehrmann SV, Windolf J, Kaufmann RA. Distal radius fracture management in elderly patients: a literature
review. J Hand Surg Am. 2008; 33 (3): 421-9. Geissler WB, Freeland AE, Savoie FH, McIntyre LW, Whipple TL. Intracarpal soft-tissue lesions associated
with an intra-articular fracture of the distal end of the radius. J Bone Joint Surg Am. 1996; 78 (3): 357-65. Gliatis JD, Plessas SJ, Davis TR. Outcome of distal radial fractures in young adults. J Hand Surg Br. 2000; 25
(6): 535-43. Gofton WT, Gordon KD, Dunning CE, Johnson JA, King GJ. Soft-tissue stabilizers of the distal radioulnar
joint: an in vitro kinematic study. J Hand Surg Am. 2004; 29 (3): 423-31. Gordon KD, Pardo RD, Johnson JA, King GJ, Miller TA. Electromyographic activity and strength during
maximum isometric pronation and supination efforts in healthy adults. J Orthop Res. 2004; 22 (1): 208-13. Grewal R, MacDermid JC. The risk of adverse outcomes in extra-articular distal radius fractures is increased
with malalignment in patients of all ages but mitigated in older patients. J Hand Surg Am. 2007; 32 (7): 962-70.
Gupta R, Allaire RB, Fornalski S, Osterman AL, Lee TQ. Kinematic analysis of the distal radioulnar joint after a simulated progressive ulnar-sided wrist injury. J Hand Surg Am. 2002; 27 (5): 854-62.
Hagert CG. Distal radius fracture and the distal radioulnar joint--anatomical considerations. Handchir Mikrochir Plast Chir. 1994; 26 (1): 22-6.
Hauck RM, Skahen J, 3rd, Palmer AK. Classification and treatment of ulnar styloid nonunion. J Hand Surg Am. 1996; 21 (3): 418-22.
Heiple KG, Freehafer AA, Van't Hof A. Isolated Traumatic Dislocation of the Distal End of the Ulna or Radio-Ulnar Joint. J Bone Joint Surg Am. 1962; 44 (7): 1387-94.
Hirahara H, Neale PG, Lin YT, Cooney WP, An KN. Kinematic and torque-related effects of dorsally angulated distal radius fractures and the distal radial ulnar joint. J Hand Surg Am. 2003; 28 (4): 614-21.
Hollevoet N, Verdonk R, Van Maele G. The influence of articular morphology on non-traumatic degenerative changes of the distal radioulnar joint. A radiographic study. J Hand Surg Br. 2006; 31 (2): 221-5.
Ishii S, Palmer AK, Werner FW, Short WH, Fortino MD. An anatomic study of the ligamentous structure of the triangular fibrocartilage complex. J Hand Surg Am. 1998a; 23 (6): 977-85.
Ishii S, Palmer AK, Werner FW, Short WH, Fortino MD. Pressure distribution in the distal radioulnar joint. J Hand Surg Am. 1998b; 23 (5): 909-13.
Ishikawa J, Iwasaki N, Minami A. Influence of distal radioulnar joint subluxation on restricted forearm rotation after distal radius fracture. J Hand Surg Am. 2005; 30 (6): 1178-84.
Kihara H, Palmer AK, Werner FW, Short WH, Fortino MD. The effect of dorsally angulated distal radius fractures on distal radioulnar joint congruency and forearm rotation. J Hand Surg Am. 1996; 21 (1): 40-7.

REFERENCES
64
Kihara H, Short WH, Werner FW, Fortino MD, Palmer AK. The stabilizing mechanism of the distal radioulnar joint during pronation and supination. J Hand Surg Am. 1995; 20 (6): 930-6.
Kim JP, Park MJ. Assessment of distal radioulnar joint instability after distal radius fracture: comparison of computed tomography and clinical examination results. J Hand Surg Am. 2008; 33 (9): 1486-92.
Kleinman WB, Graham TJ. The distal radioulnar joint capsule: clinical anatomy and role in posttraumatic limitation of forearm rotation. J Hand Surg Am. 1998; 23 (4): 588-99.
Krukhaug Y, Hove LM. Corrective osteotomy for malunited extra-articular fractures of the distal radius: A follow-up study of 33 patients. Scand J Plast Reconstr Surg Hand Surg. 2007: 1-7.
Kuhn JE. A new classification system for shoulder instability. Br J Sports Med. 2010; 44 (5): 341-6. Lee JH, Taylor NL, Beekman RA, Rosenwasser MP. Arthroscopic Wrist Anatomy. In: Wrist Arthroscopy. (Ed.
Geissler WB). Springer. New York 2005; 7-14. Lindau T, Adlercreutz C, Aspenberg P. Peripheral tears of the triangular fibrocartilage complex cause distal
radioulnar joint instability after distal radial fractures. J Hand Surg Am. 2000a; 25 (3): 464-8. Lindau T, Arner M, Hagberg L. Intraarticular lesions in distal fractures of the radius in young adults. A
descriptive arthroscopic study in 50 patients. J Hand Surg Br. 1997; 22 (5): 638-43. Lindau T, Hagberg L, Adlercreutz C, Jonsson K, Aspenberg P. Distal radioulnar instability is an independent
worsening factor in distal radial fractures. Clin Orthop Relat Res. 2000b; (376): 229-35. Lindau T, Runnquist K, Aspenberg P. Patients with laxity of the distal radioulnar joint after distal radial
fractures have impaired function, but no loss of strength. Acta Orthop Scand. 2002; 73 (2): 151-6. Lo IK, MacDermid JC, Bennett JD, Bogoch E, King GJ. The radioulnar ratio: a new method of quantifying
distal radioulnar joint subluxation. J Hand Surg Am. 2001; 26 (2): 236-43. Lozano-Calderon SA, Brouwer KM, Doornberg JN, Goslings JC, Kloen P, Jupiter JB. Long-term outcomes of
corrective osteotomy for the treatment of distal radius malunion. J Hand Surg Eur Vol. 2010; 35 (5): 370-80. MacDermid JC, Richards RS, Donner A, Bellamy N, Roth JH. Responsiveness of the short form-36, disability of
the arm, shoulder, and hand questionnaire, patient-rated wrist evaluation, and physical impairment measurements in evaluating recovery after a distal radius fracture. J Hand Surg Am. 2000; 25 (2): 330-40.
Magee T. Comparison of 3-T MRI and arthroscopy of intrinsic wrist ligament and TFCC tears. AJR Am J Roentgenol. 2009; 192 (1): 80-5.
May MM, Lawton JN, Blazar PE. Ulnar styloid fractures associated with distal radius fractures: incidence and implications for distal radioulnar joint instability. J Hand Surg Am. 2002; 27 (6): 965-71.
McAdams TR, Swan J, Yao J. Arthroscopic treatment of triangular fibrocartilage wrist injuries in the athlete. Am J Sports Med. 2009; 37 (2): 291-7.
McKean JW, Ryan JR TA. ALGORITHM 516 An Algorithm for Obtaining Confidence Intervals and Point Estimates Based on Ranks in the Two-Sample Location Problem [G1]. ACM Transactions on Mathematical Software. 1977; 3 (2): 183-5.
McQueen MM, Hajducka C, Court-Brown CM. Redisplaced unstable fractures of the distal radius: a prospective randomised comparison of four methods of treatment. J Bone Joint Surg Br. 1996; 78 (3): 404-9.
Melone CP, Jr., Nathan R. Traumatic disruption of the triangular fibrocartilage complex. Pathoanatomy. Clin Orthop Relat Res. 1992; (275): 65-73.
Moritomo H, Masatomi T, Murase T, Miyake J, Okada K, Yoshikawa H. Open repair of foveal avulsion of the triangular fibrocartilage complex and comparison by types of injury mechanism. J Hand Surg Am. 2010; 35 (12): 1955-63.
Moritomo H, Murase T, Arimitsu S, Oka K, Yoshikawa H, Sugamoto K. Change in the length of the ulnocarpal ligaments during radiocarpal motion: possible impact on triangular fibrocartilage complex foveal tears. J Hand Surg Am. 2008; 33 (8): 1278-86.
Moritomo H, Noda K, Goto A, Murase T, Yoshikawa H, Sugamoto K. Interosseous membrane of the forearm: length change of ligaments during forearm rotation. J Hand Surg Am. 2009; 34 (4): 685-91.
Moriya T, Aoki M, Iba K, Ozasa Y, Wada T, Yamashita T. Effect of triangular ligament tears on distal radioulnar joint instability and evaluation of three clinical tests: a biomechanical study. J Hand Surg Eur Vol. 2009; 34 (2): 219-23.
Müller ME, Nazarian S, Koch P, Schatzker. The Comprehensive Classification of Fractures of Long Bones. 1st ed. Springer: Berlin 1994.
Nakamura T, Takayama S, Horiuchi Y, Yabe Y. Origins and insertions of the triangular fibrocartilage complex: a histological study. J Hand Surg Br. 2001; 26 (5): 446-54.
Nakamura T, Yabe Y, Horiuchi Y. Functional anatomy of the triangular fibrocartilage complex. J Hand Surg Br. 1996; 21 (5): 581-6.
Noda K, Goto A, Murase T, Sugamoto K, Yoshikawa H, Moritomo H. Interosseous membrane of the forearm: an anatomical study of ligament attachment locations. J Hand Surg Am. 2009; 34 (3): 415-22.
Oskam J, Bongers KM, Karthaus AJ, Frima AJ, Klasen HJ. Corrective osteotomy for malunion of the distal radius: the effect of concomitant ulnar shortening osteotomy. Arch Orthop Trauma Surg. 1996; 115 (3-4): 219-22.

REFERENCES
65
Palmer AK. Triangular fibrocartilage complex lesions: a classification. J Hand Surg Am. 1989; 14 (4): 594-606. Palmer AK, Werner FW. The triangular fibrocartilage complex of the wrist--anatomy and function. J Hand Surg
Am. 1981; 6 (2): 153-62. Park MJ, Kim JP. Reliability and normal values of various computed tomography methods for quantifying distal
radioulnar joint translation. J Bone Joint Surg Am. 2008; 90 (1): 145-53. Ploegmakers JJ, Mader K, Pennig D, Verheyen CC. Four distal radial fracture classification systems tested
amongst a large panel of Dutch trauma surgeons. Injury. 2007; 38 (11): 1268-72. Prommersberger KJ, Froehner SC, Schmitt RR, Lanz UB. Rotational deformity in malunited fractures of the
distal radius. J Hand Surg Am. 2004; 29 (1): 110-5. Prommersberger KJ, Lanz UB. Corrective osteotomy of the distal radius through volar approach. Tech Hand Up
Extrem Surg. 2004; 8 (2): 70-7. Prommersberger KJ, Van Schoonhoven J, Lanz UB. Outcome after corrective osteotomy for malunited fractures
of the distal end of the radius. J Hand Surg Br. 2002; 27 (1): 55-60. Protopsaltis TS, Ruch DS. Triangular fibrocartilage complex tears associated with symptomatic ulnar styloid
nonunions. J Hand Surg Am. 2010; 35 (8): 1251-5. Reiter A, Wolf MB, Schmid U, Frigge A, Dreyhaupt J, Hahn P, et al. Arthroscopic repair of Palmer 1B
triangular fibrocartilage complex tears. Arthroscopy. 2008; 24 (11): 1244-50. Richards RS, Bennett JD, Roth JH, Milne K, Jr. Arthroscopic diagnosis of intra-articular soft tissue injuries
associated with distal radial fractures. J Hand Surg Am. 1997; 22 (5): 772-6. Rikli DA, Honigmann P, Babst R, Cristalli A, Morlock MM, Mittlmeier T. Intra-articular pressure
measurement in the radioulnocarpal joint using a novel sensor: in vitro and in vivo results. J Hand Surg Am. 2007; 32 (1): 67-75.
Ring D, Roberge C, Morgan T, Jupiter JB. Osteotomy for malunited fractures of the distal radius: a comparison of structural and nonstructural autogenous bone grafts. J Hand Surg Am. 2002; 27 (2): 216-22.
Ruch DS, Weiland AJ, Wolfe SW, Geissler WB, Cohen MS, Jupiter JB. Current concepts in the treatment of distal radial fractures. Instr Course Lect. 2004; 53: 389-401.
Ruegger C, Schmid MR, Pfirrmann CW, Nagy L, Gilula LA, Zanetti M. Peripheral tear of the triangular fibrocartilage: depiction with MR arthrography of the distal radioulnar joint. AJR Am J Roentgenol. 2007; 188 (1): 187-92.
Sagerman SD, Zogby RG, Palmer AK, Werner FW, Fortino MD. Relative articular inclination of the distal radioulnar joint: a radiographic study. J Hand Surg Am. 1995; 20 (4): 597-601.
Sarmiento A, Pratt GW, Berry NC, Sinclair WF. Colles' fractures. Functional bracing in supination. J Bone Joint Surg Am. 1975; 57 (3): 311-7.
Sasao S, Beppu M, Kihara H, Hirata K, Takagi M. An anatomical study of the ligaments of the ulnar compartment of the wrist. Hand Surg. 2003; 8 (2): 219-26.
Sasso RC, LeHuec JC, Shaffrey C. Iliac crest bone graft donor site pain after anterior lumbar interbody fusion: a prospective patient satisfaction outcome assessment. J Spinal Disord Tech. 2005; 18 Suppl: S77-81.
Silber JS, Anderson DG, Daffner SD, Brislin BT, Leland JM, Hilibrand AS, et al. Donor site morbidity after anterior iliac crest bone harvest for single-level anterior cervical discectomy and fusion. Spine. 2003; 28 (2): 134-9.
Spinner M, Kaplan EB. Extensor carpi ulnaris. Its relationship to the stability of the distal radio-ulnar joint. Clin Orthop Relat Res. 1970; 68: 124-9.
Stuart PR, Berger RA, Linscheid RL, An KN. The dorsopalmar stability of the distal radioulnar joint. J Hand Surg Am. 2000; 25 (4): 689-99.
Tanaka T, Yoshioka H, Ueno T, Shindo M, Ochiai N. Comparison between high-resolution MRI with a microscopy coil and arthroscopy in triangular fibrocartilage complex injury. J Hand Surg Am. 2006; 31 (8): 1308-14.
Tay SC, Tomita K, Berger RA. The "ulnar fovea sign" for defining ulnar wrist pain: an analysis of sensitivity and specificity. J Hand Surg Am. 2007; 32 (4): 438-44.
Tay SC, van Riet R, Kazunari T, Amrami KK, An KN, Berger RA. In-vivo kinematic analysis of forearm rotation using helical axis analysis. Clin Biomech (Bristol, Avon). 2010; 25 (7): 655-9.
Tham SK, Bain GI. Sigmoid notch osseous reconstruction. Tech Hand Up Extrem Surg. 2007; 11 (1): 93-7. Tolat AR, Stanley JK, Trail IA. A cadaveric study of the anatomy and stability of the distal radioulnar joint in
the coronal and transverse planes. J Hand Surg Br. 1996; 21 (5): 587-94. Trumble TE, Gilbert M, Vedder N. Isolated tears of the triangular fibrocartilage: management by early
arthroscopic repair. J Hand Surg Am. 1997; 22 (1): 57-65. Wallwork NA, Bain GI. Sigmoid notch osteoplasty for chronic volar instability of the distal radioulnar joint: a
case report. J Hand Surg Am. 2001; 26 (3): 454-9. van Hemert WL, Willems K, Anderson PG, van Heerwaarden RJ, Wymenga AB. Tricalcium phosphate granules
or rigid wedge preforms in open wedge high tibial osteotomy: a radiological study with a new evaluation system. Knee. 2004; 11 (6): 451-6.

REFERENCES
66
Vanden Eynde S, De Smet L, Fabry G. Diagnostic value of arthrography and arthroscopy of the radiocarpal joint. Arthroscopy. 1994; 10 (1): 50-3.
Ward LD, Ambrose CG, Masson MV, Levaro F. The role of the distal radioulnar ligaments, interosseous membrane, and joint capsule in distal radioulnar joint stability. J Hand Surg Am. 2000; 25 (2): 341-51.
Watanabe H, Berger RA, Berglund LJ, Zobitz ME, An KN. Contribution of the interosseous membrane to distal radioulnar joint constraint. J Hand Surg Am. 2005; 30 (6): 1164-71.
Waterman SM, Slade D, Masini BD, Owens BD. Safety analysis of all-inside arthroscopic repair of peripheral triangular fibrocartilage complex. Arthroscopy. 2010; 26 (11): 1474-7.
Wieland AW, Dekkers GH, Brink PR. Open Wedge Osteotomy for Malunited Extraarticular Distal Radius Fractures with Plate Osteosynthesis without Bone Grafting. Eur J Trauma. 2005; 31 (2): 148-53.
Wiesner L, Rumelhart C, Pham E, Comtet JJ. Experimentally induced ulno-carpal instability. A study on 13 cadaver wrists. J Hand Surg Br. 1996; 21 (1): 24-9.
Wilcke MT, Abbaszadegan H, Adolphson PY. Evaluation of a Swedish version of the patient-rated wrist evaluation outcome questionnaire: good responsiveness, validity, and reliability, in 99 patients recovering from a fracture of the distal radius. Scand J Plast Reconstr Surg Hand Surg. 2009; 43 (2): 94-101.
Wulf CA, Ackerman DB, Rizzo M. Contemporary evaluation and treatment of distal radius fractures. Hand Clin. 2007; 23 (2): 209-26, vi.
Xu J, Tang JB. In vivo changes in lengths of the ligaments stabilizing the distal radioulnar joint. J Hand Surg Am. 2009; 34 (1): 40-5.
Young BT, Rayan GM. Outcome following nonoperative treatment of displaced distal radius fractures in low-demand patients older than 60 years. J Hand Surg Am. 2000; 25 (1): 19-28.


















