PITUITARY HORMONAL LOSS AND RECOVERY AFTER TRANSSPHENOIDAL ADENOMA

336 © 2018 Journal of Neurosciences in Rural Practice | Published by Wolters Kluwer - Medknow
Background: Endonasal endoscopic approach for transsphenoidal excision ofpituitary adenoma has undergone remarkable evolution in the last two decades.It is considered less invasive and less stressful, with results comparable to theprevious “gold standard” technique of microscopic transsphenoidal excision ofpituitaryadenoma.Theaimofthisstudywastocomparethevariousperioperativeanestheticandsurgical factorswhichdiffer in the twoapproaches(endoscopicvs.microscopic) for pituitary adenoma excision, during the period when surgeonsincreasingly started using endoscope at our center. Materials and Methods:Dataof307patients fromJanuary2011 toDecember2013were reviewed in thisretrospective study. Various parameters were divided and compared on the basisof the typeofapproachforpituitary tumorresectionvis‑à‑vismicroscope‑assistedsublabial transsphenoidal (MSLTS) resection or microscope‑assisted transnasaltranssphenoidal (MTNTS) resection or endoscope‑assisted endonasaltranssphenoidal (ETSS) resection. Results: Demographic variables (except age);tumor type, dimensions, and invasiveness; patients’ comorbidities; postoperativenausea/vomiting, electrolyte imbalance, respiratory, and cardiovascular problemswere comparable among three groups. Duration of surgery and anesthesia wereshortest forMTNTS group and longest for ETSS group (P < 0.001). Blood losswas higher in ETSS technique (median 300 mL) and least in MTNTS (median100mL), and thedifferencewas significant across all threegroups (P=0.0003).Postoperative cerebrospinal fluid rhinorrhea was 17% in the MSLTS groupcomparedto6.5%inMTNTSand7.9%inETSS(P=0.047).Conclusion:ETSSwith the expected advantage of being less invasive offers a better chance forcompleteresectionofadenoma.Neuroanesthesiologistmustbepreparedforlongersurgical timeandmorebloodlossascomparedtopreviousmicroscopicapproach,atleasttillthesurgeonsexpertiseinthisnewertechnique.
Keywords: Endoscopic, microscopic, perioperative, transsphenoidal pituitary surgery
Perioperative Course of Transsphenoidal Pituitary Surgery through Endoscopic versus Microscopic Approach: Interim Concerns for Neurosurgical AnesthesiologyVarun Jain, Arvind Chaturvedi, Mihir Prakash Pandia, Parmod Kumar Bithal1
Access this article onlineQuick Response Code:
Website: www.ruralneuropractice.com
DOI: 10.4103/jnrp.jnrp_22_18
Address for correspondence: Dr. Varun Jain, Department of Neuroanesthesiology and Critical Care, Room No. 711, CN Center, All India Institute of Medical Sciences,
New Delhi ‑ 110 029, India. E‑mail: [email protected]
of pituitary adenoma.[1‑3] Despite having its owndisadvantages,likenotbeingabletoprovidestereoscopicvision to surgeon and a learning curve, endoscopic
Original Article
Introduction
Endoscopic approach for endonasal skull basesurgery has undergone a remarkable evolution in
the last two decades.[1] Endonasal endoscopic approachfor transsphenoidal excision of pituitary adenoma isconsidered less invasive and less stressful to patients,with results comparable to theprevious “gold standard”technique of microscopic transsphenoidal excision
DepartmentofNeuroanesthesiologyandCriticalCare,AllIndiaInstituteofMedicalSciences,NewDelhi,India,1DepartmentofAnesthesiology,KingFahadMedicalCity,Riyadh,SaudiArabia
Abs
trac
t
How to cite this article: Jain V, Chaturvedi A, Pandia MP, Bithal PK. Perioperative course of transsphenoidal pituitary surgery through endoscopic versus microscopic approach: Interim concerns for neurosurgical anesthesiology. J Neurosci Rural Pract 2018;9:336-43.
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
For reprints contact: [email protected]
Published online: 2019-09-02

Jain, et al.: Perioperative anesthetic course of transsphenoidal pituitary surgery through endoscopic versus microscopic approach
337Journal of Neurosciences in Rural Practice ¦ Volume 9 ¦ Issue 3 ¦ July-September 2018
technique, still, has the advantage of providing apanoramic view of the sella.Many centers are thereforegraduallyshiftingovertothenewerendoscopicapproachfor transsphenoidal excision of pituitary adenoma. Dataabout management of pituitary surgery are surplusin literature, but none of the studies have comparedanestheticproblemsandcomplicationsencounteredinthenewer endoscopic resection with the older microscopictechniqueforresectionofpituitarytumors.
We planned this study to compare the variousperioperativeanestheticandsurgicalfactorswhichdifferin the two approaches (endoscopic vs. microscopic)and influence patients’ outcome after transsphenoidalpituitarysurgery.
Materials and MethodsAfterobtainingInstituteEthicsCommitteeapproval,thisretrospective study was conducted. Hospital records ofall patients operated through transsphenoidal approachfor pituitary adenoma excision from January 2011 toDecember 2013 were reviewed. Pituitary adenomapatients operated under neuronavigation in MRI suitewere excluded. The microscopic technique was furtherdivided into sublabial or transnasal route. Variousparameterswere recordedandcomparedon thebasisofthetypeofapproachforpituitarytumorresection,thatis,microscope‑assisted sublabial transsphenoidal (MSLTS)resection or microscope‑assisted transnasaltranssphenoidal (MTNTS) resection orendoscope‑assisted endonasal transsphenoidal (ETSS)resection.
Data collectionVarious preoperative parameters recorded weredemographic profile, type, and dimensions of pituitaryadenoma and baseline investigations. Intraoperativedata included the type of anesthetic techniques, amountof blood loss, amount of fluids infused, hemodynamicchanges,anesthesiaandsurgicalduration,andextubationdetails. Postoperative details noted were anesthesia orsurgicalcomplications,computedtomography(CT)‑headfinding, number of days on ventilator, and durationof Intensive Care Unit (ICU) and hospital stay.Post‑operative recovery was assessed using Glasgowoutcomescale(GOS)atdischarge.
Intraoperatively, the patient was considered to havea bradycardia if heart rate (HR) was <50/min,tachycardia if HR was >100/min, hypotension ifsystolic blood pressure (SBP) decreased to <90mmHg,and hypertension if SBP increased to >160 mmHg.Maximum and minimum values of HR, SBP, diastolicbloodpressure (DBP), andmeanbloodpressure (MAP)recorded intraoperatively were noted. Chief operating
neurosurgery consultant was classified based on yearsof experience as “senior consultant” with more than6 years of experience or “junior consultant” with lessthan 6 years of experience, after obtaining masters inpostgraduatedegree.
Statistical analysisStatistical analysis was done using the softwareStata 11.0 (College Station, TX, USA). Data werepresented as number (%), mean ± standard deviation,or median (range), as appropriate. The three‑groupanalysis for continuous variables which followed thenormal distribution was done byANOVA test, and forvariables which did not follow normal distribution byKruskal–Wallis test. Two‑group comparison was donefor continuousvariablesusing the t‑test for independentvariables,andforvariableswhichdidnotfollownormaldistribution by theWilcoxon rank‑sum test. Categoricalvariables were compared using the Chi‑square test/Fisher exact test. P < 0.05 was considered statisticallysignificant.
ResultsRecord of 307 patients operated for pituitary adenomaexcision through transsphenoidal route were retrievedand analyzed. Table 1 shows the increasing numberof cases being done through ETSS technique overprogressiveyears.
Anesthesia protocolA similar management protocol was observed forall patients. Monitoring included electrocardiogram,SpO2, invasive blood pressure, EtCO2 and skintemperature in all patients. General anesthesia wasinduced with either propofol or thiopentone alongwith fentanyl and rocuronium and was maintainedwith oxygen, nitrous oxide, and isoflurane/sevoflurane/desflurane alongwith intermittent bolusesof fentanyl and vecuronium. Few of the patients alsoreceived dexmedetomidine infusion intraoperatively.Mechanical ventilation was adjusted to EtCO2 of35 ± 2 mmHg. Crystalloids ringer lactate and 0.9%normal saline and colloid 6% hydroxyethyl starchwere infused tomaintain intravascular volume status.At theendofsurgery, tracheawaseitherextubatedor
Table 1: Year‑wise distribution of number of casesMSLTS (n=135) MTNTS (n=46) ETSS (n=126)
2011 75 17 32012 46 18 432013 14 11 80MSLTS:Microscope‑assisted sublabial transsphenoidal surgery,MTNTS:Microscope‑assisted transnasal transsphenoidal surgery,ETSS:Endoscope‑assistedendonasaltranssphenoidalsurgery
Jain, et al.: Perioperative anesthetic course of transsphenoidal pituitary surgery through endoscopic versus microscopic approach
338 Journal of Neurosciences in Rural Practice ¦ Volume 9 ¦ Issue 3 ¦ July-September 2018
patient shifted with the endotracheal tube in situ forfurthermanagement in theneurosurgicalICU.
Preoperative dataDemographic variables (sex, weight),American SocietyofAnesthesiology (ASA) grade, and blood groupswerecomparableamong the threegroups [Table2].However,age of patients inMTNTS groupwas higher than othergroups (P < 0.05). Although record for the type anddescriptionofthetumorwasavailableforallcases,exactdimensionsofmacroadenoma(pituitaryadenoma>10mmin dimension) were available for 70 (59.3%) patientsin MSLTS group, 27 (67.5%) in MTNTS group, and74(65.4%)inETSSgroup.Overall,116patients(37.8%)had a functioning pituitary adenoma. Hypothyroidismdue to the pressure effect of adenoma on normal glandwas present in 72 patients (23.4%). Comorbidities werecomparableamongallgroups[Table3].
A total of thirteen neurosurgery consultants operated onthe cases over 3 years [Table 4].More number ofETSSwasconductedbythe“seniorconsultants”inneurosurgeryteamascomparedtomicroscopictechnique(P<0.001).
Intraoperative dataHigher percentage of patients inMSLTS andMTNTSgroups (12.6% and 15.2%, respectively) receiveddexmedetomidine infusion compared to 4% in ETSS
group (P = 0.016).Duration of surgery and anesthesiawere shortest forMTNTSgroupand longest forETSSgroup(P<0.001)[Table5].
Analgesic requirement as judgedbynumberof fentanylboluses repeated intraoperatively, besides the induction
Table 2: Preoperative variables (n [%]/median [range] or mean±standard deviation)MSLTS (n=135) MTNTS (n=46) ETSS (n=126) P
Age(years) 39.0±14.2 45.5±13.6 38.6±13.3 0.01Sex(male:female) 76(56.3):59(43.7) 25(54.3):21(45.6) 77(61.1):49(38.9) 0.6Weight(kg) 69.7±15.3 66.7±10.9 65.9±13.4 0.08ASAgrade(1:2:3) 65(48.1):48(35.6):22(16.3) 23(50):17(37):6(13.0) 74(58.7):44(34.9):8(6.3) 0.1CategorizationoftumorMicroadenoma 17(12.6) 6(13) 13(10.3) 0.4Macroadenoma 93(68.9) 36(78.2) 86(68.2)Giant 25(18.5) 4(8.7) 27(21.4)
Dimensionsofmacroadenoma(mm)n(numberofpatientswithavailabledata) 70/118 27/40 74/113Length 30(10‑68) 31(14‑65) 26(10‑57) 0.2Breadth 26(7‑75) 24(10‑45) 22(7‑54) 0.5Height 23(9‑72) 25(11‑43) 24(6‑51) 0.9
ClassificationforextensionoftumorExtension(%)(0:1:2:3:4) 22.9:50.4:8.9:11.1:6.7 13.0:58.7:15.2:6.5:6.5 19.8:47.6:11.9:10.3:10.3 0.7
Functionalityofthetumor(n=116/307)Functioning 51(37.8) 17(37) 48(38.1) 1Acromegaly 28 10 30 0.8Cushing 15 5 13 1Prolactinoma 8 2 5 0.7
Extensionofpituitaryadenomawasratedas0:Intrasellaradenoma,1:Suprasellarextensionofadenomamaximumuptosuprasellarcistern,2:Suprasellarextensionofadenomauptofloorof3rdventricle,3:Parasellarextensionmedialto/uptocarotidsorsuprasellarfillingofthe3rdventricle,and4:Parasellarextensionbeyondcarotids.IntergroupPvalue‑1:MSLTS,2:MTNTS,3:ETSS‑Age1versus2:0.02,2versus3:0.01,1versus3:1.ASA:AmericanSocietyofAnesthesiologists,MSLTS:Microscope‑assistedsublabialtranssphenoidalsurgery,MTNTS:Microscope‑assistedtransnasaltranssphenoidalsurgery,ETSS:Endoscope‑assistedendonasaltranssphenoidalsurgery
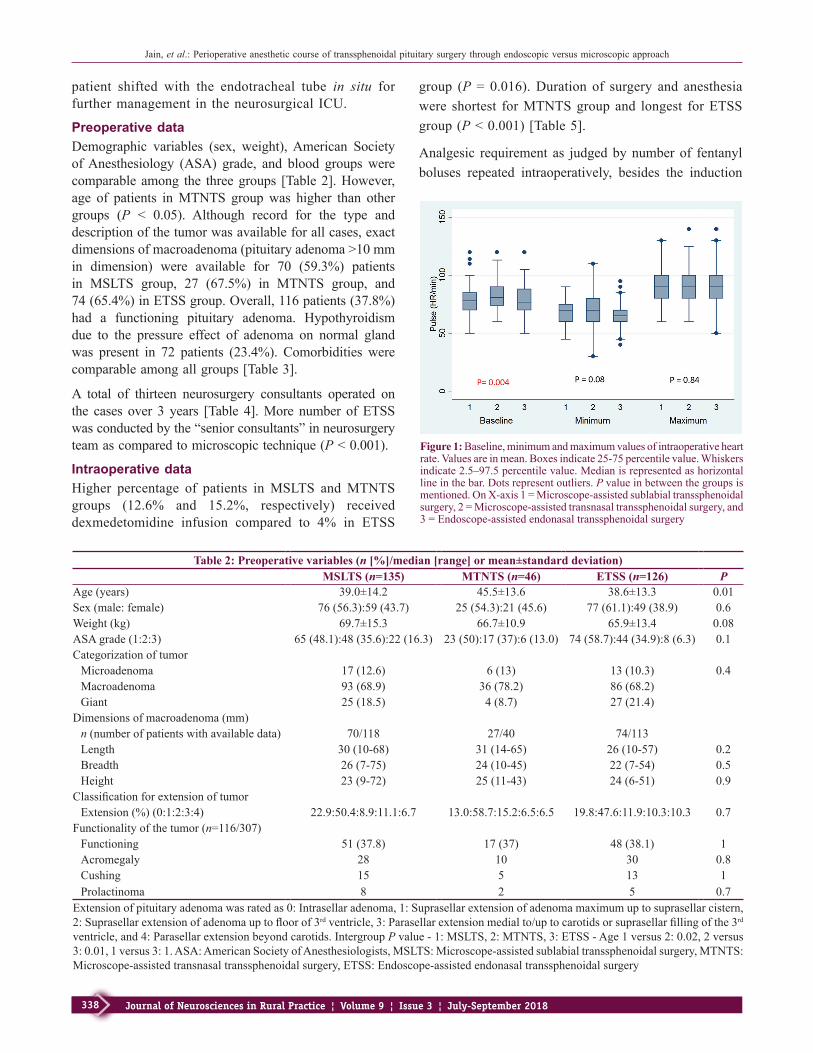
Figure 1:Baseline,minimumandmaximumvaluesofintraoperativeheartrate.Valuesareinmean.Boxesindicate25‑75percentilevalue.Whiskersindicate2.5–97.5percentilevalue.Medianisrepresentedashorizontallineinthebar.Dotsrepresentoutliers. P valueinbetweenthegroupsismentioned.OnX‑axis1=Microscope‑assistedsublabialtranssphenoidalsurgery,2=Microscope‑assistedtransnasaltranssphenoidalsurgery,and3=Endoscope‑assistedendonasaltranssphenoidalsurgery
Jain, et al.: Perioperative anesthetic course of transsphenoidal pituitary surgery through endoscopic versus microscopic approach
339Journal of Neurosciences in Rural Practice ¦ Volume 9 ¦ Issue 3 ¦ July-September 2018
Table 4: Classification of neurosurgery consultants based on experience (n [%])MSLTS (n=135)
MTNTS (n=46)
ETSS (n=126)
P
Seniorconsultants(n=4)
64(47.4) 18(39.1) 104(82.5) <0.001
Juniorconsultants(n=9)
71(52.6) 28(60.9) 22(17.5)
IntergroupPvalue‑1:MSLTS,2:MTNTS,3:ETSS‑1versus2:0.42,2versus3:<0.001,1versus3:<0.001.MSLTS:Microscope‑assistedsublabial transsphenoidal surgery,MTNTS:Microscope‑assistedtransnasal transsphenoidal surgery, ETSS: Endoscope‑assistedendonasaltranssphenoidalsurgery
dose, was similar across all three groups (P = 0.8).Likewise, number of patients who did not need anyrepeat fentanyl bolus was also similar across all threegroups(P=0.9).
Blood loss was highest in ETSS technique and leastin MTNTS. In proportion to the blood loss, volumeof crystalloids infused was least inMTNTS group andmost in ETSS group.Number of patientswho receivedcolloidwasalsomoreinETSSgroup.
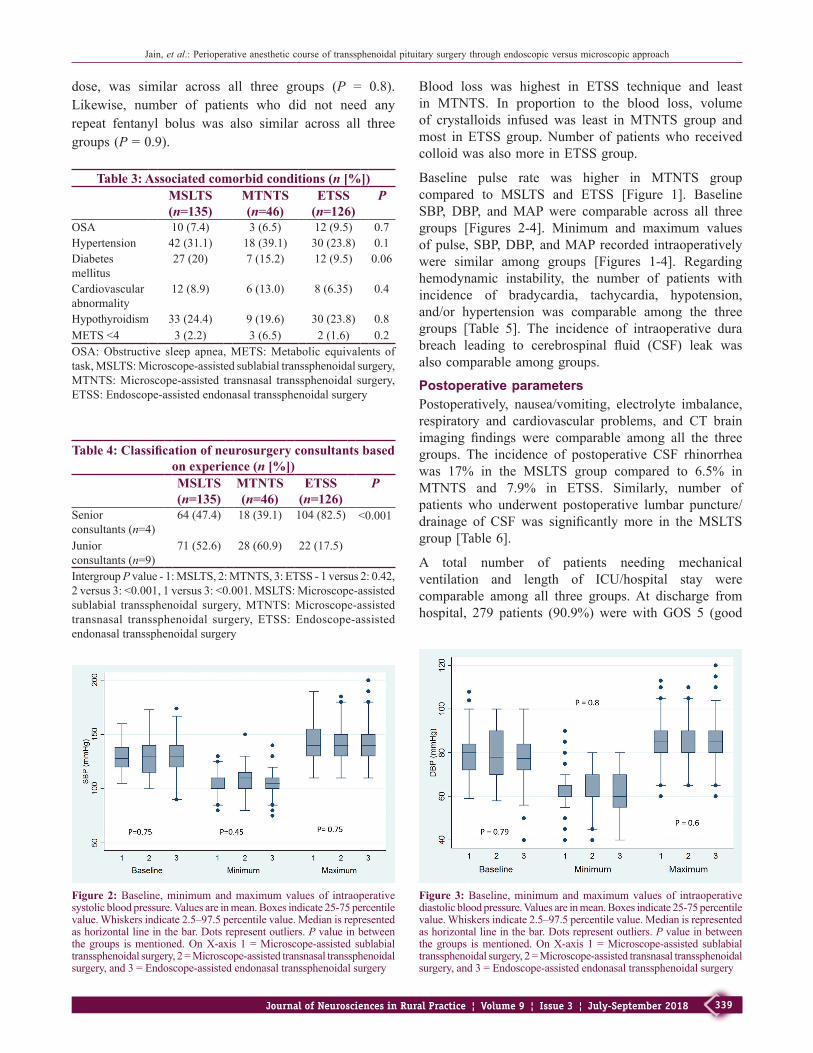
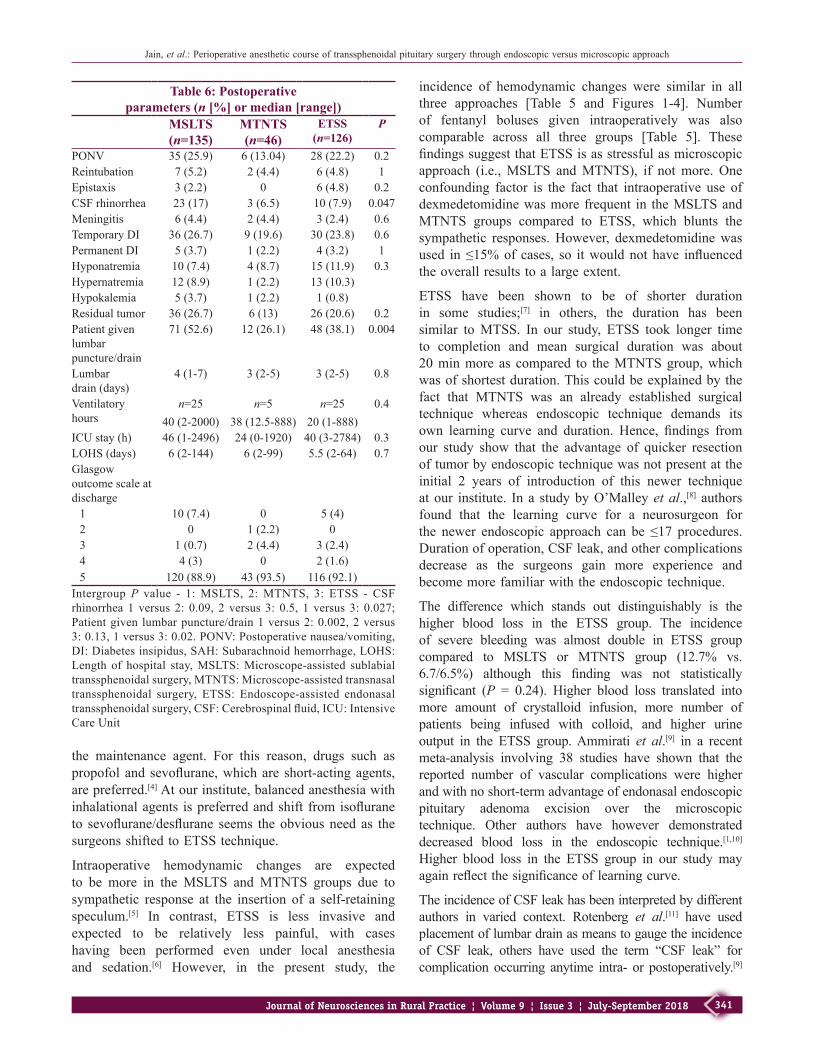
Baseline pulse rate was higher in MTNTS groupcompared to MSLTS and ETSS [Figure 1]. BaselineSBP, DBP, andMAP were comparable across all threegroups [Figures 2‑4]. Minimum and maximum valuesofpulse,SBP,DBP,andMAP recorded intraoperativelywere similar among groups [Figures 1‑4]. Regardinghemodynamic instability, the number of patients withincidence of bradycardia, tachycardia, hypotension,and/or hypertension was comparable among the threegroups [Table 5]. The incidence of intraoperative durabreach leading to cerebrospinal fluid (CSF) leak wasalsocomparableamonggroups.
Postoperative parametersPostoperatively, nausea/vomiting, electrolyte imbalance,respiratory and cardiovascular problems, and CT brainimaging findings were comparable among all the threegroups. The incidence of postoperative CSF rhinorrheawas 17% in the MSLTS group compared to 6.5% inMTNTS and 7.9% in ETSS. Similarly, number ofpatients who underwent postoperative lumbar puncture/drainage of CSF was significantly more in theMSLTSgroup[Table6].
A total number of patients needing mechanicalventilation and length of ICU/hospital stay werecomparable among all three groups.At discharge fromhospital, 279 patients (90.9%) were with GOS 5 (good
Table 3: Associated comorbid conditions (n [%])MSLTS (n=135)
MTNTS (n=46)
ETSS (n=126)
P
OSA 10(7.4) 3(6.5) 12(9.5) 0.7Hypertension 42(31.1) 18(39.1) 30(23.8) 0.1Diabetesmellitus
27(20) 7(15.2) 12(9.5) 0.06
Cardiovascularabnormality
12(8.9) 6(13.0) 8(6.35) 0.4
Hypothyroidism 33(24.4) 9(19.6) 30(23.8) 0.8METS<4 3(2.2) 3(6.5) 2(1.6) 0.2OSA:Obstructive sleep apnea,METS:Metabolic equivalents oftask,MSLTS:Microscope‑assistedsublabialtranssphenoidalsurgery,MTNTS:Microscope‑assisted transnasal transsphenoidal surgery,ETSS:Endoscope‑assistedendonasaltranssphenoidalsurgery
Figure 2:Baseline,minimumandmaximumvaluesof intraoperativesystolicbloodpressure.Valuesareinmean.Boxesindicate25‑75percentilevalue.Whiskersindicate2.5–97.5percentilevalue.Medianisrepresentedashorizontallineinthebar.Dotsrepresentoutliers. P valueinbetweenthegroups ismentioned.OnX‑axis1=Microscope‑assisted sublabialtranssphenoidalsurgery,2=Microscope‑assistedtransnasaltranssphenoidalsurgery,and3=Endoscope‑assistedendonasaltranssphenoidalsurgery
Figure 3:Baseline,minimumandmaximumvaluesof intraoperativediastolicbloodpressure.Valuesareinmean.Boxesindicate25‑75percentilevalue.Whiskersindicate2.5–97.5percentilevalue.Medianisrepresentedashorizontallineinthebar.Dotsrepresentoutliers. P valueinbetweenthegroups ismentioned.OnX‑axis1=Microscope‑assisted sublabialtranssphenoidalsurgery,2=Microscope‑assistedtransnasaltranssphenoidalsurgery,and3=Endoscope‑assistedendonasaltranssphenoidalsurgery

Jain, et al.: Perioperative anesthetic course of transsphenoidal pituitary surgery through endoscopic versus microscopic approach
340 Journal of Neurosciences in Rural Practice ¦ Volume 9 ¦ Issue 3 ¦ July-September 2018
Table 5: Intraoperative parameters (n [%]/median [range] or mean±standard deviation)MSLTS (n=135) MTNTS (n=46) ETSS (n=126) P
Numberoffentanylboluses 1(0‑4) 1(0‑3) 1(0‑4) 0.8Zero(0)fentanylbolus 39(29.1) 15(32.6) 39(30.7) 0.9IncidenceofhemodynamiceventsBradycardia 2(1.48) 2(4.4) 4(3.2) 0.5Tachycardia 15(11.1) 5(10.9) 15(11.9) 1Hypotension 10(7.4) 4(8.7) 13(10.3) 0.7Hypertension 44(32.6) 14(30.4) 36(28.6) 0.8
Intraoperativeinput/output(ml)Bloodloss 200(20‑3000) 100(50‑5000) 300(50‑2500) 0.0003Crystalloid 2000(1000‑4000) 1500(1000‑9500) 2000(1000‑5500) 0.0001
Numberofpatientsgivencolloid 30(22.2) 8(17.4) 46(36.5) 0.009Colloid(ml) 500(150‑1500) 500(500‑2000) 500(500‑1500) 0.4Numberofpatientsgivenbloodtransfusion 10(7.4) 6(13) 12(9.5) 0.5Bloodtransfusion(units) 1(1‑4) 1.5(1‑10) 2(1‑4) 0.2ExtubationinOT 113(83.7) 41(89.1) 102(80.9) 0.1Durationsurgery(min) 139.6±55.9 102.2±75.4 144.5±50.9 0.0001Durationanesthesia(min) 214.2±56.7 181.1±79.8 222.56±50.1 0.0002IntraoperativeCSFleak 60(44.4) 15(32.6) 51(40.5) 0.4Excessivebleeding 9(6.7) 3(6.5) 16(12.7) 0.2IntergroupPvalue‑1:MSLTS,2:MTNTS,3:ETSS‑Bloodloss1versus2:0.014,2versus3:<0.001,1versus3:0.02;Crystalloidgiven1versus2:0.01,2versus3:<0.001,1versus3:<0.001;Numberofpatientsgivencolloid1versus2:0.49,2versus3:0.02,1versus3:0.01;Durationsurgery1versus2:0.001,2versus3:<0.001,1versus3:1;Durationanesthesia1versus2:0.003,2versus3:<0.001,1versus3:0.76.MSLTS:Microscope‑assistedsublabialtranssphenoidalsurgery,MTNTS:Microscope‑assistedtransnasaltranssphenoidalsurgery,ETSS:Endoscope‑assistedendonasaltranssphenoidalsurgery,CSF:Cerebrospinalfluid,OT:Operationtheater
functional recovery), and the distribution was similarin all three groups. Overall mortality (GOS = 1) was4.9%(15patients),ofwhich10patientswereinMSLTSgroupand5patients inETSSgroup.Rateofgross totalexcision as judged by incidence of residual tumor onpostoperative CT scan was also comparable among allthreegroups.
Microscope‑assisted TSS versus endoscope‑ assisted TSS–two‑group analysisAll the findings were reanalyzed by combining theMSLTS and MTNTS approaches into one group asmicroscope‑assistedtranssphenoidalsurgery(MTSS)andcomparedwiththeETSS.Statisticallysignificantfindingsof the earlier three‑group analysiswhen reanalyzed intotwogroups(MTSSandETSS)arepresented inTable7.Differences observed earlier between three groups withrespect to age, baseline pulse, and postoperative CSFrhinorrhea were not seen when two‑group analyseswas performed. The duration of surgery and anesthesiawas more in ETSS group than MTSS, and the formertechnique was associated with more blood loss andfluid infusion, intraoperatively. This is despite the factthat ETSS was predominantly conducted by “seniorconsultants”ofneurosurgery(82.5%).
DiscussionThe newly introduced endoscopic technique fortranssphenoidal pituitary adenoma excision (ETSS)requires the neuroanesthesiologist to be more watchfulwith the steps of the procedure. Although surgicalduration of ETSS may be prolonged, completion maybe sudden and surgeon may not pack the nasal cavityunlike the sublabial approachwhere tissue closuremaygive an opportunity to neuroanesthesiologist to titrate
Figure 4:Baseline,minimumandmaximumvaluesof intraoperativemeanbloodpressure (MAP).Values are inmean.Boxes indicate25‑75percentilevalue.Whiskersindicate2.5–97.5percentilevalue.Medianisrepresentedashorizontallineinthebar.Dotsrepresentoutliers. P valueinbetweenthegroupsismentioned.OnX‑axis1=Microscope‑assistedsublabial transsphenoidal surgery, 2=Microscope‑assisted transnasaltranssphenoidal surgery, and 3 = Endoscope‑assisted endonasaltranssphenoidalsurgery
Jain, et al.: Perioperative anesthetic course of transsphenoidal pituitary surgery through endoscopic versus microscopic approach
341Journal of Neurosciences in Rural Practice ¦ Volume 9 ¦ Issue 3 ¦ July-September 2018
the maintenance agent. For this reason, drugs such aspropofolandsevoflurane,whichare short‑actingagents,arepreferred.[4]Atourinstitute,balancedanesthesiawithinhalationalagents ispreferredandshift fromisofluraneto sevoflurane/desflurane seems theobviousneed as thesurgeonsshiftedtoETSStechnique.
Intraoperative hemodynamic changes are expectedto be more in the MSLTS and MTNTS groups due tosympathetic response at the insertion of a self‑retainingspeculum.[5] In contrast, ETSS is less invasive andexpected to be relatively less painful, with caseshaving been performed even under local anesthesiaand sedation.[6] However, in the present study, the
incidence of hemodynamic changes were similar in allthree approaches [Table 5 and Figures 1‑4]. Numberof fentanyl boluses given intraoperatively was alsocomparable across all three groups [Table 5]. ThesefindingssuggestthatETSSisasstressfulasmicroscopicapproach (i.e.,MSLTS andMTNTS), if notmore. Oneconfounding factor is the fact that intraoperative use ofdexmedetomidinewasmore frequent in theMSLTSandMTNTS groups compared to ETSS, which blunts thesympathetic responses.However, dexmedetomidinewasused in≤15%of cases, so itwouldnothave influencedtheoverallresultstoalargeextent.
ETSS have been shown to be of shorter durationin some studies;[7] in others, the duration has beensimilar toMTSS. In our study, ETSS took longer timeto completion and mean surgical duration was about20minmore as compared to theMTNTSgroup,whichwasofshortestduration.Thiscouldbeexplainedbythefact that MTNTS was an already established surgicaltechnique whereas endoscopic technique demands itsown learning curve and duration. Hence, findings fromour study show that the advantage of quicker resectionoftumorbyendoscopictechniquewasnotpresentattheinitial 2 years of introduction of this newer techniqueatour institute. In a studybyO’Malleyetal.,[8] authorsfound that the learning curve for a neurosurgeon forthe newer endoscopic approach can be ≤17 procedures.Durationofoperation,CSFleak,andothercomplicationsdecrease as the surgeons gain more experience andbecomemorefamiliarwiththeendoscopictechnique.
The difference which stands out distinguishably is thehigher blood loss in the ETSS group. The incidenceof severe bleeding was almost double in ETSS groupcompared to MSLTS or MTNTS group (12.7% vs.6.7/6.5%) although this finding was not statisticallysignificant (P = 0.24). Higher blood loss translated intomore amount of crystalloid infusion, more number ofpatients being infused with colloid, and higher urineoutput in the ETSS group.Ammirati et al.[9] in a recentmeta‑analysis involving 38 studies have shown that thereported number of vascular complications were higherandwithnoshort‑termadvantageofendonasalendoscopicpituitary adenoma excision over the microscopictechnique. Other authors have however demonstrateddecreased blood loss in the endoscopic technique.[1,10]Higher blood loss in the ETSS group in our study mayagainreflectthesignificanceoflearningcurve.
TheincidenceofCSFleakhasbeeninterpretedbydifferentauthors in varied context. Rotenberg et al.[11] have usedplacementoflumbardrainasmeanstogaugetheincidenceof CSF leak, others have used the term “CSF leak” forcomplication occurring anytime intra‑ or postoperatively.[9]
Table 6: Postoperative parameters (n [%] or median [range])
MSLTS (n=135)
MTNTS (n=46)
ETSS (n=126)
P
PONV 35(25.9) 6(13.04) 28(22.2) 0.2Reintubation 7(5.2) 2(4.4) 6(4.8) 1Epistaxis 3(2.2) 0 6(4.8) 0.2CSFrhinorrhea 23(17) 3(6.5) 10(7.9) 0.047Meningitis 6(4.4) 2(4.4) 3(2.4) 0.6TemporaryDI 36(26.7) 9(19.6) 30(23.8) 0.6PermanentDI 5(3.7) 1(2.2) 4(3.2) 1Hyponatremia 10(7.4) 4(8.7) 15(11.9) 0.3Hypernatremia 12(8.9) 1(2.2) 13(10.3)Hypokalemia 5(3.7) 1(2.2) 1(0.8)Residualtumor 36(26.7) 6(13) 26(20.6) 0.2Patientgivenlumbarpuncture/drain
71(52.6) 12(26.1) 48(38.1) 0.004
Lumbardrain(days)
4(1‑7) 3(2‑5) 3(2‑5) 0.8
Ventilatoryhours
n=2540(2‑2000)
n=538(12.5‑888)
n=2520(1‑888)
0.4
ICUstay(h) 46(1‑2496) 24(0‑1920) 40(3‑2784) 0.3LOHS(days) 6(2‑144) 6(2‑99) 5.5(2‑64) 0.7Glasgowoutcomescaleatdischarge1 10(7.4) 0 5(4)2 0 1(2.2) 03 1(0.7) 2(4.4) 3(2.4)4 4(3) 0 2(1.6)5 120(88.9) 43(93.5) 116(92.1)
IntergroupP value ‑ 1:MSLTS, 2:MTNTS, 3: ETSS ‑ CSFrhinorrhea 1 versus 2: 0.09, 2 versus 3: 0.5, 1 versus 3: 0.027;Patientgiven lumbarpuncture/drain1versus2:0.002,2versus3:0.13,1versus3:0.02.PONV:Postoperativenausea/vomiting,DI:Diabetesinsipidus,SAH:Subarachnoidhemorrhage,LOHS:Length of hospital stay,MSLTS:Microscope‑assisted sublabialtranssphenoidalsurgery,MTNTS:Microscope‑assistedtransnasaltranssphenoidal surgery, ETSS: Endoscope‑assisted endonasaltranssphenoidalsurgery,CSF:Cerebrospinalfluid,ICU:IntensiveCareUnit

Jain, et al.: Perioperative anesthetic course of transsphenoidal pituitary surgery through endoscopic versus microscopic approach
342 Journal of Neurosciences in Rural Practice ¦ Volume 9 ¦ Issue 3 ¦ July-September 2018
We observed that despite the incidence of intraoperativeCSFleakbeingsimilaracrossallthreegroups,theincidenceof postoperative CSF rhinorrhea was almost double inthe MSLTS group compared to ETSS (17% vs. 7.9%; P = 0.027). Placement of lumbar drain/puncturewas alsomoreintheMSLTSgroup(P=0.004).LowerincidenceofCSF leak inETSSmay be because of better visualizationof tumor boundaries, thereby avoiding trauma to theduramater and confirmation of better seal of duramater,oncemembrane breaches.However, Strychowsky et al.[10]haveobserved increased incidenceof “post‑operativeCSFleak” in the endoscopic approach, possibly implicated byefforts of the surgeons to extend their limits to achievecomplete resection. On the contrary, Rotenberg et al.[11]haveshownadecreaseintheincidenceofCSFleakintheETSS group in their meta‑analysis and stated that bettersuccessof reconstructive technique followingdissection isthemajordeterminantoflesserCSFleak.
Postoperatively, the incidence of diabetesinsipidus (transient or permanent) and meningitis
was comparable between the groups. The incidenceof epistaxis, nausea/vomiting, respiratory, andcardiovascular complications [Table 6] were, also,comparable between the groups; which is in agreementwith recentmeta‑analysis byGaoetal.[7] andAmmiratiet al.[9] Neal et al.[12] in a three‑group analysis as ourshave shown a much higher incidence of diabetesinsipidus in sublabial approach (33%) compared to theMTNTS (5%) and ETSS (7%). Several other studieshave shown comparable or lesser incidence of DI inETSS compared to MTSS.[13] Meticulous preservationof the neurovascular structures of the hypothalamus,infundibulum, and neurohypophysis helps to decreasetheincidenceofdiabetesinsipidus.[13]
Regarding the effectiveness of tumor debulking, thenumber of patients with residual pathology though lessin ETSS than MSLTS was not statistically significant.A major limiting factor for complete pituitary tumorremoval is the extent of cavernous sinus and internalcarotid artery involvement.[14] Endoscopes withpanoramic vision and ability to reach previouslyinaccessible areas have the advantage over tunneledvision provided bymicroscopes. Likewise, Gao et al.[7]intheirmeta‑analysisof15studiesfoundthattherateofgrosstumorremovalwashigherintheendoscopicgroupthaninthemicroscopicgroup.
A shorter length of hospital stay gives an indirectevidenceoflesscomplicatedhospitalcourse.Adecreasedhospital stay has been shown a clear advantage ofendoscopic procedure in recent meta‑analysis.[7,11]However, the hours of ICU stay and days of hospitalstay were comparable among all groups in our study.However, it could be that discharge to home policy isdifferentinourhospitalcomparedtootherinstitutes.
We compared the data as three‑group analysis ofMSLTS, MTNTS, and ETSS; and later as two‑groupanalysis by combining both the microscope‑assistedtechniques (viz., MSLTS and MTNTS) as MTSS andcomparingwithETSS.This helped us to better analyzethe surgical and anesthesia technique. For example,while if only MTSS and ETSS were to be compared,no difference would have been found between twotechniques; but a three‑group analysis highlighted thatthepostoperativeCSFrhinorrheaandnumberofpatientsrequiring lumbarpuncture/drainwerehighest inMSLTSgroup compared to other techniques. Similarly, when atwo‑group analysis showed lesser number of diabeticand betterASA grade patients in the ETSS group thanMTSS group, which would have suggested selectionbiasofhealthierpatientstoETSSgroup,thethree‑groupanalysis, however, suggested that such distribution wasonly incidental and not clinically significant. Thus, if
Table 7: Demographic profile and other perioperative parameters in microscope‑assisted transsphenoidal surgery and endoscope‑assisted
endonasal transsphenoidal surgery (n [%]/median [range] or mean±standard deviation)
MTSS (n=181) ETSS (n=126) PAge(years) 40.7±14.36 38.6±13.3 0.2Diabetesmellitus 34(18.8) 12(9.52) 0.02ASAgrade(1:2:3) 88:65:28 74:44:8 0.03Pulse(h/min) 80(50‑120) 77(50‑120) 0.3Bloodloss(mL) 200(0‑5000) 300(0‑2500) 0.04Crystalloid(mL) 2000(1000‑9500) 2000(1000‑5500) 0.001Numberofpatientsgivencolloid
38(21) 46(36.5) 0.003
Durationsurgery(min)
129.8±63.6 144.4±50.9 0.03
Durationanesthesia(min)
205.5±65 222.6±50.2 0.01
CSFrhinorrhea 26(14.4) 10(7.9) 0.08Patientgivenlumbarpuncture/drain
83(45.8) 48(38.1) 0.2
ClassificationofneurosurgeryconsultantsbasedonyearsofexperienceSeniorconsultants(n=4)
82(45.3) 104(82.5) <0.001
Juniorconsultants(n=9)
99(54.7) 22(17.5)
MTSS:Microscope‑assisted transsphenoidal surgery, ETSS:Endoscope‑assisted endonasal transsphenoidal surgery,ASA:AmericanSocietyofAnesthesiologists,CSF:Cerebrospinalfluid

Jain, et al.: Perioperative anesthetic course of transsphenoidal pituitary surgery through endoscopic versus microscopic approach
343Journal of Neurosciences in Rural Practice ¦ Volume 9 ¦ Issue 3 ¦ July-September 2018
MTSS is not separated into the MSLTS and MTNTSsubgroups and analysis is done under two broadcategories (i.e., MTSS and ETSS), the results mayconceal some of the relevant findings and highlightothers; therefore,onemustbe carefulwhile interpretingfindingsoffewearlierstudies.[1,15]
This study has few limitations. First, this beingretrospective study carries all the drawbacks of suchstudyplans.Second, a largenumberof consultants (13)have conducted the cases over 3‑year period. Itwas not possible to remove the bias arising fromhierarchy (experience) of neurosurgical consultants.Third, we have not used hormonal assay to measurethe success of tumor debulking and have only usedpostoperative imaging to check for residual pathology.Fourth, the study duration is limited till the period ofhospital stay of the patients. Long‑term follow‑up andoutcome of the procedures cannot be derived from thisdata, and it only reflects short‑term results. Finally,although the MTNTS may seem a better approach inseveralaspects, the smaller sample size failsus todrawadefinitivejudgment.
ConclusionEndoscope‑assisted technique is gradually replacingthe microscope‑assisted technique for transsphenoidalresection of pituitary adenomas. ETSS with theexpected advantage of being less invasive offers abetter chance for complete resection of adenoma.However, neuroanesthesiologist must be prepared forlonger surgical time and more blood loss as comparedto previous microscopic approach, at least untilthe surgeons have achieved expertise in this newertechnique. While lesser incidence of postoperativeCSF rhinorrhea is observed in endoscopic approach,incidence of rest of the complications seems similar topreviousMTSSapproachinourstudy.
Financial support and sponsorshipNil.
Conflicts of interestTherearenoconflictsofinterest.
References1. Goudakos JK, Markou KD, Georgalas C. Endoscopic versus
microscopic trans‑sphenoidal pituitary surgery: A systematicreviewandmeta‑analysis.ClinOtolaryngol2011;36:212‑20.
2. Lucas JW, Zada G. Endoscopic surgery for pituitary tumors.NeurosurgClinNAm2012;23:555‑69.
3. Smith M, Hirsch NP. Pituitary disease and anaesthesia. Br JAnaesth2000;85:3‑14.
4. DunnLK,NemergutEC.Anesthesiafortranssphenoidalpituitarysurgery.CurrOpinAnaesthesiol2013;26:549‑54.
5. Ali Z, Prabhakar H, Bithal PK, Dash HH. Bispectralindex‑guided administration of anesthesia for transsphenoidalresection of pituitary tumors: A comparison of 3 anesthetictechniques.JNeurosurgAnesthesiol2009;21:10‑5.
6. ZhangQ,Zou J,LiuS,AnH,LiangC.Anesthesia selection inhypophysectomy by endoscopic transnasal sphenoidal approach.LinChuangErBiYanHouKeZaZhi2006;20:348‑50.
7. GaoY,ZhongC,WangY,XuS,GuoY,DaiC,et al.Endoscopicversus microscopic transsphenoidal pituitary adenoma surgery:Ameta‑analysis.WorldJSurgOncol2014;12:94.
8. O’MalleyBWJr.,GradyMS,GabelBC,CohenMA,HeuerGG,Pisapia J, et al. Comparison of endoscopic and microscopicremoval of pituitary adenomas: Single‑surgeon experience andthelearningcurve.NeurosurgFocus2008;25:E10.
9. AmmiratiM,WeiL,Ciric I. Short‑termoutcomeof endoscopicversus microscopic pituitary adenoma surgery: A systematicreview and meta‑analysis. J Neurol Neurosurg Psychiatry2013;84:843‑9.
10. Strychowsky J, Nayan S, Reddy K, Farrokhyar F, Sommer D.Purely endoscopic transsphenoidal surgery versus traditionalmicrosurgery for resection of pituitary adenomas: Systematicreview.JOtolaryngolHeadNeckSurg2011;40:175‑85.
11. Rotenberg B, Tam S, RyuWH, Duggal N. Microscopic versusendoscopicpituitarysurgery:Asystematicreview.Laryngoscope2010;120:1292‑7.
12. Neal JG, Patel SJ, Kulbersh JS, Osguthorpe JD, Schlosser RJ.Comparison of techniques for transsphenoidal pituitary surgery.AmJRhinol2007;21:203‑6.
13. Schreckinger M, Szerlip N, Mittal S. Diabetes insipidusfollowing resection of pituitary tumors. Clin Neurol Neurosurg2013;115:121‑6.
14. Gondim JA, Schops M, de Almeida JP, de Albuquerque LA,GomesE,FerrazT,et al.Endoscopicendonasal transsphenoidalsurgery: Surgical results of 228 pituitary adenomas treated in apituitarycenter.Pituitary2010;13:68‑77.
15. D’Haens J,Van RompaeyK, StadnikT, Haentjens P, PoppeK,VelkeniersB,et al.Fullyendoscopictranssphenoidalsurgeryforfunctioningpituitaryadenomas:Aretrospectivecomparisonwithtraditional transsphenoidal microsurgery in the same institution.SurgNeurol2009;72:336‑40.







![Workspace Determination and Robot Design of A Prototyped .... Jackrit's Papers/international proceedings/Workspace Determination...Endonasal transsphenoidal surgery [2]. Surgical Tool](https://static.fdocuments.us/doc/165x107/5e7d3f6dfc1005351034dbcd/workspace-determination-and-robot-design-of-a-prototyped-jackrits-papersinternational.jpg)


![Transsphenoidal Hypophysectomy - American Journal of ... · The transsphenoidal approach is contraindicated when the sellar lesion involves the brain [7, 8], cavernous sinus, or middle](https://static.fdocuments.us/doc/165x107/5ec9e438caa2204df94a718f/transsphenoidal-hypophysectomy-american-journal-of-the-transsphenoidal-approach.jpg)