Periodontal Infections and Adverse Pregnancy Outcomes: The Oral Health—Fetal Connection
4
Review Article Periodontal Infections and Adverse Pregnancy Outcomes: The Oral Health—Fetal Connection Haritha Avula, MDS, and Jayakumar Avula, MDS Abstract Objective: The increasing awareness of the relationship between maternal oral health and adverse pregnancy outcomes is well documented in the dental literature.The present review aims at summing up the current state of evidence and research on the same and sharing the available literature with the obstetric and other general practitioners so that the patients are diagnosed and treated with an interdisciplinary approach. Materials and methods: A search of the dental literature, including Medline Ò =PubMed through 2009, was conducted focusing on periodontal disease, preterm delivery, low birth weight, and intrauterine growth restriction was undertaken, and a hand search of other gray literature and text books was performed. Conclusions: It has been widely reported that pregnant women with periodontitis have more chances of having adverse pregnancy outcomes such as preterm birth, low birth-weight infants, preeclampsia, gestational diabetes, small-for-gestational age infants, and fetal loss. At the same time, there have been sporadic reports that contradict this potential association. Clinicians need to remain abreast with available and emerging information, and exercise prudence while considering the possible adverse pregnancy outcomes from chronic periodontal infections. (J GYNECOL SURG 27:1) Introduction D ental infections causing systemic diseases in dis- tant parts of the body have been known for decades. The concept, called focal infection, reported by Miller in 1891 was very popular in the beginning of the twentieth century. 1 It got an impetus after William Hunter’s forceful pleas for action against dental sepsis in 1910. 2 The concept fell into oblivion because of thoughtless and unmindful sacrifice of teeth and tonsils for their alleged roles in causing systemic disease. In 1989, the concept got support, when a couple of Danish re- searchers reported an increasing incidence of coronary heart disease in the presence of periodontal disease. 3 From that point there was a surge of interest in dental infections causing systemic disease. Cardiocavascular disease, stroke, preterm babies, pulmonary disease, total mortality, Alzheimer’s dis- ease, dementia, and many other systemic conditions are di- rectly or indirectly attributed to—or associated with chronic periodontal infections—as is total mortality. Periodontal diseases comprise a group of diseases that af- fect the supporting structures of the teeth. The involved teeth are normal but the the gums and alveolar bone are affected adversely. Called pyorrhea in earlier literature, periodontal disease is prevalent universally, and no continent or country is unaffected by this chronic ailment. Characterized by gum bleeding, discharge of pus, and progressive mobility of teeth and their ultimate loss, the disease is chronic, painless, and produces no compelling urge for seeking treatment in the absence of severe pain. Contrary to dental caries, which in- volve few teeth, periodontal disease involves most teeth and is the most common cause of tooth loss (Fig.1). Periodontal disease also represents an infectious disease affecting >23% of women between the ages of 30 and 54. 4 What the Research Shows Given that there is a potential association between peri- odontal disease and preterm births, it makes sense to explore this association. A search of the dental literature, including Medline Ò =PubMed through 2009, was conducted focusing on periodontal disease, preterm delivery, low birth weight, and intrauterine growth restriction was undertaken, and a hand search of other gray literature and text books was performed. Complicated pregnancies include preterm births, low- birth-weight babies, small-for-gestational-age (SGA) infants and cause considerable social, psychologic, and economic burdens on the families affected. Preterm delivery is associ- ated with risk factors such as smoking and alcohol consump- tion, race, parity, low maternal weight, older and younger maternal age, short cervical length, stress, low socioeconomic status, poor nutritional status of the mother, genitourinary Department of Periodontics, Sri Sai College of Dental Surgery, Vikarabad, Andhra Pradesh, India. JOURNAL OF GYNECOLOGIC SURGERY Volume 27, Number 1, 2011 ª Mary Ann Liebert, Inc. DOI: 10.1089=gyn.2009.0104 1
Transcript of Periodontal Infections and Adverse Pregnancy Outcomes: The Oral Health—Fetal Connection

Review Article
Periodontal Infections and Adverse Pregnancy Outcomes:The Oral Health—Fetal Connection
Haritha Avula, MDS, and Jayakumar Avula, MDS
Abstract
Objective: The increasing awareness of the relationship between maternal oral health and adverse pregnancyoutcomes is well documented in the dental literature.The present review aims at summing up the current state ofevidence and research on the same and sharing the available literature with the obstetric and other generalpractitioners so that the patients are diagnosed and treated with an interdisciplinary approach. Materials andmethods: A search of the dental literature, including Medline�=PubMed through 2009, was conducted focusingon periodontal disease, preterm delivery, low birth weight, and intrauterine growth restriction was undertaken,and a hand search of other gray literature and text books was performed. Conclusions: It has been widely reportedthat pregnant women with periodontitis have more chances of having adverse pregnancy outcomes such as pretermbirth, low birth-weight infants, preeclampsia, gestational diabetes, small-for-gestational age infants, and fetal loss.At the same time, there have been sporadic reports that contradict this potential association. Clinicians need toremain abreast with available and emerging information, and exercise prudence while considering the possibleadverse pregnancy outcomes from chronic periodontal infections. ( J GYNECOL SURG 27:1)
Introduction
Dental infections causing systemic diseases in dis-tant parts of the body have been known for decades. The
concept, called focal infection, reported by Miller in 1891 wasvery popular in the beginning of the twentieth century.1 It gotan impetus after William Hunter’s forceful pleas for actionagainst dental sepsis in 1910.2 The concept fell into oblivionbecause of thoughtless and unmindful sacrifice of teeth andtonsils for their alleged roles in causing systemic disease. In1989, the concept got support, when a couple of Danish re-searchers reported an increasing incidence of coronary heartdisease in the presence of periodontal disease.3 From thatpoint there was a surge of interest in dental infections causingsystemic disease. Cardiocavascular disease, stroke, pretermbabies, pulmonary disease, total mortality, Alzheimer’s dis-ease, dementia, and many other systemic conditions are di-rectly or indirectly attributed to—or associated with chronicperiodontal infections—as is total mortality.
Periodontal diseases comprise a group of diseases that af-fect the supporting structures of the teeth. The involved teethare normal but the the gums and alveolar bone are affectedadversely. Called pyorrhea in earlier literature, periodontaldisease is prevalent universally, and no continent or countryis unaffected by this chronic ailment. Characterized by gumbleeding, discharge of pus, and progressive mobility of teeth
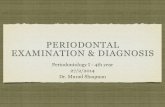
and their ultimate loss, the disease is chronic, painless, andproduces no compelling urge for seeking treatment in theabsence of severe pain. Contrary to dental caries, which in-volve few teeth, periodontal disease involves most teeth andis the most common cause of tooth loss (Fig.1). Periodontaldisease also represents an infectious disease affecting>23% ofwomen between the ages of 30 and 54.4
What the Research Shows
Given that there is a potential association between peri-odontal disease and preterm births, it makes sense to explorethis association. A search of the dental literature, includingMedline�=PubMed through 2009, was conducted focusingon periodontal disease, preterm delivery, low birth weight,and intrauterine growth restriction was undertaken, and ahand search of other gray literature and text books wasperformed.
Complicated pregnancies include preterm births, low-birth-weight babies, small-for-gestational-age (SGA) infantsand cause considerable social, psychologic, and economicburdens on the families affected. Preterm delivery is associ-ated with risk factors such as smoking and alcohol consump-tion, race, parity, low maternal weight, older and youngermaternal age, short cervical length, stress, low socioeconomicstatus, poor nutritional status of the mother, genitourinary
Department of Periodontics, Sri Sai College of Dental Surgery, Vikarabad, Andhra Pradesh, India.
JOURNAL OF GYNECOLOGIC SURGERYVolume 27, Number 1, 2011ª Mary Ann Liebert, Inc.DOI: 10.1089=gyn.2009.0104
1

infections, and other generalized systemic infections. Theseinfections trigger the release of proinflammatory mediatorssuch as interleukin 1(IL-1), tumor necrosis factor alpha (TNF-a) and prostaglandin E2 (PGE2), which initiate preterm laborand low birth weight. Periodontitis, a chronic and subclinicaldisease, is also suspected for providing an inflammatorycomponent in the fetal environment.
During pregnancy,the incidence of gingivitis and period-ontitis is increased and many pregnant women suffer frombleeding and spongy gums. Changing hormone levels duringpregnancy, coupled with lack of oral hygiene, account formost of the gingival changes. Fifty percent (50%)–70% of allpregnant women develop gingivitis; this condition is called‘‘pregnancy gingivitis.’’ Increases in progesterone and estro-gen levels during pregnancy affect small blood vessels of thegingiva, leading to their increased permeability. This increasedinflammatory nature of the gingiva predisposes pathogenicbacteria to take advantage of the situation and frank diseaseresults. The result is a host response to the microbial attack byproducing increased proinflammatory cytokines.
It has been increasingly reported that pregnant womenwith periodontitis have more chances of having adversepregnancy outcomes such as preterm birth, low birth weightinfants, preeclampsia, gestational diabetes, SGA infants andfetal loss.
Galloway5 reported in 1931 that focal infection in teeth andtonsils affected the fetus. His was probably the first interven-tional study. He extracted abscessed teeth in patients and ob-served no incidents of miscarriage or stillbirth in these patients.He suggested that all foci of infection should be removed ortreated early in pregnancy to avoid unwanted sequelae.
Periodontitis and Preterm Birth
It all started 13 years ago, when Offenbacher et al.,6 at theUniversity of North Carolina conducted a study to determinewhether prevalence of maternal periodontal infection was as-sociated with preterm low birth weight. The researchers con-trolled for known risk factors and potential covariates in astudy of 124 pregnant women or postpartum mothers. Asses-sing other known obstetric risk factors, the researchers dem-onstrated that periodontal disease is a statistically significant
risk factor for preterm low birth weight and concluded thatperiodontal disease represents a previously unrecognized andsignificant risk factor for preterm low birth weight.
Since 1996, there has been a deluge of research papers onthis topic. There have been articles supporting the hypothe-ses, some that do not report any association, and some thatreport a weak association.
In another study,7 the average weight of the newborns in aperiodontitis group was lower than infants in the controlgroup, and it was concluded that localized periodontitis ofthe patient during pregnancy can be regarded as an impor-tant risk factor for preterm birth. In an article published inThe Lancet, Pihlstrom and coworkers8 stated that periodontaldisease has been associated with adverse pregnancy out-comes, cardiovascular disease, stroke, pulmonary disease,and diabetes, but the causal relationships have not been es-tablished. Controlling bacterial biofilm, arresting periodontaldisease, and restoring lost periodontal support has beensuggested to improve pregnancy.
In a prospective study called the Oral Conditions andPregnancy (OCAP) study, Offenbacher et al.9 reported an11.2% incidence of preterm births among periodontallyhealthy women, compared with an incidence of 28.6% inwomen with moderate–severe periodontal disease and con-cluded that maternal periodontal disease increases relativerisk for preterm or spontaneous preterm births.
Xiong,10 in an article published in the British Journal ofObstetrics and Gynaecology, reviewed status of periodontaldisease and adverse pregnancy outcomes. Of twenty-fivestudies, 18 suggested an association between periodontitisand adverse pregnancy outcomes, and 7 studies found noevidence of an association. In three studies, prior scaling andperiodontal treatment led to a 57 % reduction in preterm lowbirth weight and a 50% reduction in preterm births.
Delivery of an SGA infant in mothers with moderate orsevere periodontal disease early in pregnancy was reportedby Boggess et al.11
Linking gingivitis to bacterial vaginosis, Persson12 reportedthat higher vaginal bacterial counts are possible in womenwith gingivitis in comparison to women with bacterial vagi-nosis but who have no gingivitis. Organisms such as Prevotellabivia and Prevotella disiens may be specific to a relationshipbetween vaginal and gingival infections.
In a thorough review of literature on the subject,13 twenty-six epidemiologic studies reported an association betweenperiodontal disease and adverse pregnancy outcomes. How-ever, most studies did not control for confounders, thusraising serious doubts about the researchers’ conclusions. Theconclusions drawn by various researchers also had method-ological limitations and could not be relied upon to establishan association between periodontal disease and adversepregnancy outcomes. Despite conflicting risk factors andcontradicting statements, most of the clinical studies indicateda positive correlation between periodontal disease and pre-term birth. Microbiologic and immunologic findings stronglysupport the association. Placental–fetal exposure to peri-odontal infection and resulting fetal inflammatory responsecan lead to preterm delivery.
Discussing whether maternal periodontitis was associatedwith an increased risk of preeclampsia, researchers wrote anarticle about a case-control study in Brazil that reported such anassociation.14 In a study in Turkey, Tygor15 suggested that
FIG. 1. Advanced periodontal disease with severe inflam-mation, gross sepsis, and loosening of teeth.
2 AVULA AND AVULA

maternal periodontal disease may be a risk factor for an adversepregnancy outcome. In a case-controlled study of 1305 Brazi-lians,16 Siqueira and workers reported that maternal period-ontitis was associated with an increased risk for preterm birth,low birth weight, and intrauterine growth restriction, and theyfocused on the importance of periodontal care in prenatalhealth programs. In a prospective cohort study in Pakistan,1152 women were assessed for dental status and followed forpregnancy outcomes.17 Low birth weight was not related tomeasures of periodontal disease but stillbirth and neonatal andperinatal deaths increased with severity of periodontal disease.
In a study of 1404 pregnant women in Spain, Lopez18 re-ported a modest association between periodontitis and pre-term birth. Although not all of the actual data supported theperiodontal–pregnancy connection, assessment of the peri-odontal status of pregnant women during an early pregnancymight be useful for minimizing future obstetric complications.A review of 31 published studies showed that 22 showed apositive association between premature birth and periodontaldisease.19 Preterm low birth weight was reported to be re-lated to periodontal infections that might influence the fetus–placenta complex.
If periodontal inflammation is directly or indirectly respon-sible for adverse pregnancy outcomes, the natural corollarywould be treatment or elimination of such inflammation,which would result in fewer occurrences of adverse events.There are contradictory reports in about this strategy. Tostudy this strategy, it would be necessary to expose pregnantwomen to good oral hygiene and oral prophylaxis, and ob-serve postpartum events and compare these events with thosein pregnant women who did not receive any dental treatment.The hypotheses would be tenable only if a significant numberof pregnant women who had dental care had fewer adverseoutcome events compared to controls. Few studies have ex-amined the potential effects of periodontal treatment duringpregnancy on pregnancy outcomes, periodontal status, andinflammatory biomarkers.
In a pilot study in 2003, Jeffcoat20 and coworkers per-formed periodontal treatment on pregnant women and ob-served them for pregnancy outcomes. Performing scalingand root planing produced reduction of preterm births in thewomen who received this treatment.
Periodontal treatment in another study resulted in a sig-nificant decrease in periodontopathic bacteria, serum IL-6,and gingival crevicular fluid IL-1ß. This particular researchsupports the view that periodontal treatment has beneficialvalue on pregnancy outcomes. A 3.8-fold decrease in the rateof preterm delivery with periodontal intervention is a wel-come development. 21
Gazolla et al.22 also attempted to evaluate the efficacy ofperiodontal treatment with respect to pregnancy outcomes.Mothers who had treatment for periodontal conditionsfared better than those who did not receive such interven-tions. Periodontal disease was related significantly to pre-term delivery.
Another study of particular relevance was an Indian onefrom Bangalore conducted by Tarannum and Faizuddin23 whotested the efficacy of periodontal treatment during pregnancyand versus no treatment for any adverse outcomes. Periodontaltreatment during pregnancy included plaque control instruc-tions, scaling, and root planing. There was a significant effect ofperiodontal treatment on birth outcomes in this study.
Porphyromonas gingivalis is a microorganism involved inperiodontal disease and has been found in the amniotic fluidof a few pregnant women, some of whom experiencedthreatened premature labor.24 Pregnant mice infected withP. gingivalis had elevated levels of TNF-a, suppressed levelsof maternal IL-10, and enhanced fetal-growth restriction.
With respect to awareness of periodontal health and preg-nancy outcomes among obstetricians and physicians, an in-teresting survey in North Carolina25 showed that mostrespondents answered correctly that periodontal disease iscaused by bacteria and 84% the of respondents consideredperiodontal disease to be an important a risk factor for ad-verse pregnancy events. The respondents were aware ofperiodontal disease and its implications for pregnancy out-comes. However, such a healthy awareness has yet to bedisseminated among physicians and obstetricians in manyparts of the world.
Contrasting Research
Not all of the evidence supports the oral health–pregnancyconnection. In a study of 328 Caucasian women, Hei-monnen et al.26 found no differences between mothers whohad preterm births and mothers who had full-term birthswith respect to periodontal status. Primiparity, low weight-gain, and antimicrobial drug use during pregnancy werethe significant predictors for preterm birth in this study.The study could not establish any linkage between peri-odontal parameters and pregnancy outcomes and attrib-uted the preterm births to only established systemic riskfactors.
In a multicenter, randomized controlled clinical trial pub-lished in The New England Journal of Medicine, Michalowicz andcoworkers27 could not establish any association betweentreatment of periodontal disease during pregnancy and sub-sequent pregnancy outcomes. This has sparked an interestingdebate, and the topic continues to enliven researchers toprobe the potential relationship further. However, it has alsobeen pointed that a single randomized trial does not have fi-nality, and additional research is critical for supporting thishypothesis.
Wimmer and Pihlstrom28 were more categorical andforthright in highlighting the inadequacies of research forestablishing the association between periodontal status andbirth outcome. Definitions of what constitutes periodontaldisease and inadequate control of confounding factors makestudies in this area difficult. There is no conclusive evidencethat treatment of periodontal infection results in better birthoutcomes. While maternal treatment of periodontal diseasewill reduce signs of gum disease, this treatment does notreduce the rate of preterm birth.
Srinivas and coworkers29 from the Department of Obstetricsand Gynecology, in the University of Pennsylvania HealthSystem, conducted a multicenter prospective cohort study in-volving 311 patients with and 475 patients without periodontaldisease. The researchers could not establish any associationbetween periodontal disease and any composite outcome orpreterm birth. They had the last word in this regard whenthey concluded that ‘‘despite the body of literature sugges-ting an association between periodontal disease and adversepregnancy outcomes in urban populations, this large prospec-tive study failed to demonstrate an association.’’29
PERIODONTITIS AND PRETERM BIRTH 3

Conclusions
Preterm birth is a major cause of infant mortality andmorbidity, and has considerable social, medical, and eco-nomic impacts. The rate of preterm birth appears to be in-creasing worldwide and efforts to prevent or reduce itsprevalence have been largely unsuccessful. Adverse preg-nancy outcomes have many risk factors. If periodontal diseasewere recognized as a risk factor, identification of a suchcausal=contributory relationship to preterm birth would havefar reaching and long-lasting effects on society. Concedingthat there is an ongoing debate, it has to be borne in mind thatreports showing a positive association have come from world-class researchers and have been published in peer-reviewedjournals. It pays to be prudent, not ignore shouts and whis-pers about a potential connection, and continue to remainvigilant about pregnancy and oral health.
Disclosure Statement
The authors report no conflict of interest and the study didnot receive any funding from any source.
References
1. Miller WD, The human mouth as a focus of infection. DentCosmos 1891;33:689–713.
2. Hunter W. The role of sepsis and antisepsis in medicine.Lancet 1910;1:79–86.
3. Mattila K, Nieminen M, Valtonen V et al. ‘‘Association be-tween dental health and acute myocardial infarction’’ BMJ298:779–82.
4. American Academy of Periodontology. Protecting OralHealth Throughout Your Life. Online document at: www.perio.org=consumer=women.htmAccessed March 1, 2010.
5. Galloway CE. Focal infection. Am J Surg 1931;14:643.6. Offenbacher S, Katz V, Fertik G, Collins J, Boyd D, Maynor
G, et al. Periodontal infection as a possible risk factor forpreterm low birth weight. J Periodontol 1996;67:1103.
7. Radnai M, Gorzo I, Nagy E, Urban E, Novak T, Pal A.A possibleassociation between preterm birth and early periodontitis. Apilot study. J Clin Periodontol. 2004 Sep;31(9):736–41.
8. Pihlstrom BL, Michalowicz BS, Johnson NW. Periodontaldiseases. Lancet 2005;366:1809.
9. Offenbacher S, Boggess KA, Murtha AP, et al. Progressiveperiodontal disease and risk of very preterm delivery.Obstet Gynecol 2006;107:29.
10. Xiong X, Buekens P, Fraser WD, Beck J, Offenbacher S.Periodontal disease and adverse pregnancy outcomes: Asystematic review. Br J Obstet Gynaecol 2006;113:135.
11. Boggess KA, Beck JD, Murtha AP, Moss K, Offenbacher S.Maternal periodontal disease in early pregnancy and risk fora small-for-gestational-age infant. Am J Obstet Gynacol 2006;194:1316.
12. Persson R, Hitti J, Verhelst R, et al. The vaginal microflora inrelation to gingivitis. BMC Infect Dis 2009;9:6.
13. Vettore MV, Lamarca Gde A, Leao AT, Thomaz FB, SheihamA, Leal Mdo C. Periodontal infection and adverse pregnancyoutcomes: a systematic review of epidemiological studies.Cad Saude Publica. 2006 Oct;22(10):2041–53.
14. Cota LO, Guimaraes AN, Costa JE, Lorentz TC, Costa FO.Association between maternal periodontitis and an in-creased risk of preeclampsia. J Periodontol 2006;77:2063.
15. Toygar HU, Seydaoglu G, Kurklu S, Guzeldemir E,Arpak N. Periodontal health and adverse pregnancyoutcome in 3,576 Turkish women. J Periodontol 2007;78:2081.
16. Siqueira FM, Cota LO, Costa JE, Haddad JP, Lana AM, CostaFO. Intrauterine growth restriction, low birth weight, andpreterm birth: Adverse pregnancy outcomes and their as-sociation with maternal periodontitis. J Periodontol 2007;78:2266.
17. Mobeen N, Jehan I, Banday N, et al. Periodontal disease andadverse birth outcomes: A study from Pakistan. Am J ObstetGynecol 2008;198:514.e1–8.
18. Lopez R. Periodontal disease and adverse pregnancy out-comes. Evid Based Dent 2008;9:48.
19. Clothier B, Stringer M, Jeffcoat MK. Periodontal disease andpregnancy outcomes: Exposure, risk and intervention. BestPract Res Clin Obstet Gynaecol 2007;21:451.
20. Jeffcoat MK, Hauth JC, Geurs NC, et al. Periodontal diseaseand preterm birth: Results of a pilot intervention study.J Periodontol 2003;74:1214.
21. Offenbacher S, Lin D, Strauss R, et al. Effects of periodontaltherapy during pregnancy on periodontal status, biologicparameters, and pregnancy outcomes: A pilot study. J Per-iodontol 2006;77:2011.
22. Gazolla CM, Ribeiro A, Moyses MR, Oliveira LA, Pereira LJ,Sallum AW. Evaluation of the incidence of preterm low birthweight in patients undergoing periodontal therapy. J Peri-odontol 2007;78:842.
23. Tarannum F, Faizuddin M. Effect of periodontal therapyon pregnancy outcome in women affected by periodontitis.J Periodontol 2007;78:2095.
24. Leon R, Silva N, Ovalle A, et al . Detection of Porphyromonasgingivalis in the amniotic fluid in pregnant women witha diagnosis of threatened premature labor. J Periodontol2007;78:1249.
25. Wilder R, Robinson C, Jared HL, Lieff S, Boggess K. Ob-stetricians’ knowledge and practice behaviors concerningperiodontal health and preterm delivery and low birthweight. J Dent Hyg 2007;81:81.
26. Heimonen A, Rintamaki H, Furuholm J, Janket SJ, KaajaR, Meurman JH. Postpartum oral health parameters inwomen with preterm birth. Acta Odontol Scand 2008;66:334.
27. Michalowicz BS, Hodges JS, DiAngelis AJ, et al. Treatmentof periodontal disease and the risk of preterm birth. N Engl JMed 2006;355:1885.
28. Wimmer G, Pihlstrom BL. A critical assessment of adversepregnancy outcomes and periodontal disease. J Clin Peri-odontol 2008;35:380.
29. Srinivas SK, Sammel MD, Stamilio DM, et al. Periodontaldisease and adverse pregnancy outcomes: Is there an asso-ciation? Am J Obstet Gynecol 2009;200:497.e1–8.
Address correspondence to:Haritha Avula, MDS
Department of PeriodonticsSri Sai College of Dental Surgery
Vikarabad, Andhra Pradesh 501101India
E-mail: [email protected]
4 AVULA AND AVULA