
Perineural invasion: Independent prognostic factor in oral ...
8
ORIGINAL ARTICLE Perineural invasion: Independent prognostic factor in oral cancer that warrants adjuvant treatment Deepa Nair MS 1 | Manish Mair MCh 1 | Hitesh Singhvi MDS 1 | Aseem Mishra MS 1 | Sudhir Nair MCh 1 | Jaiprakash Agrawal MD 2 | Pankaj Chaturvedi MS 1 1 Department of Head and Neck Oncosurgery, Tata Memorial Hospital, Mumbai, India 2 Department of Radiation Oncology, Tata Memorial Hospital, Mumbai, India Correspondence Deepa Nair, Department of Head and Neck Oncosurgery, Tata Memorial Hospital, Dr. E. Borges Road, 12th floor, Homi Bhabha Block, Parel, Mumbai 212, India. Email: [email protected] Abstract Background: Controversy exists regarding the administration of adjuvant radiother- apy (RT) when perineural invasion (PNI) is the only adverse histological feature. The purpose of this study was to evaluate the impact of PNI on the survival of patients with oral cavity squamous cell carcinoma (SCC). Methods: A retrospective study of 1524 treatment naive patients with oral cavity SCC who underwent surgery from January 2012 to March 2015 was conducted. Sur- vival analysis was performed using Cox regression model. Results: The incidence of PNI was 20.3% and higher in tongue cancers (odds ratio 2.43). The PNI significantly affected both disease-free survival (DFS; hazard ratio [HR] 1.84) as well as overall survival (OS; HR 1.7). Patients with early node- negative oral cavity SCC with PNI are more likely to develop recurrences and have mortality (HR 2.79 for DFS; HR 2.54 for OS). However, the addition of adjuvant radiation in these patients showed improvement in survival (p 5 .022). Forest plot analysis showed a trend toward poor survival across all subgroups in patients with PNI. Conclusion: Aggressive treatment of the primary cancer with the coincident manage- ment of the neck is important in the presence of PNI. The PNI worsens survival and warrants intensification of adjuvant treatment. KEYWORDS adjuvant treatment, disease-free survival, oral cancer, overall survival, perineural invasion 1 | INTRODUCTION Oral cancer is the most common cancer in India among men, the fifth most frequently occurring cancer among women, and the third most frequently occurring cancer in India among both men and women. 1,2 Advanced T classification, nodal metastasis, extracapsular spread, and poorer differen- tiation are a few known poor prognostic factors for oral can- cers. Although perineural invasion (PNI) is a known poor prognostic factor with higher local recurrences, its impact on overall survival (OS) is still under debate. Determination of PNI is generally accepted when at least 33% of the nerve circumference is surrounded by tumor cells; anything <33% is considered as the tumor proximity. 3 Cases of PNI in patients with squamous cell carcinoma (SCC) of the skin, 4,5 lip, 6 and oral cavity 7–10 are associated with locore- gional recurrences. It has been clearly demonstrated that patients at high risk for recurrent disease or metastasis should be treated aggressively after surgery and use of adjuvant radio- therapy (RT) has shown to decrease locoregional recurrences. 11 However, controversy still exists regarding the role of adjuvant RT when PNI is the only adverse histological factor. Even the Received: 21 July 2017 | Revised: 14 November 2017 | Accepted: 8 February 2018 DOI: 10.1002/hed.25170 1780 © 2018 Wiley Periodicals, Inc. wileyonlinelibrary.com/journal/hed Head & Neck. 2018;40:1780–1787.
Transcript of Perineural invasion: Independent prognostic factor in oral ...
OR I G I NAL ART I C L E
Perineural invasion: Independent prognostic factor in oral cancerthat warrants adjuvant treatment
Deepa Nair MS1 | Manish Mair MCh1 | Hitesh Singhvi MDS1 |
Aseem Mishra MS1 | Sudhir Nair MCh1 | Jaiprakash Agrawal MD2 |
Pankaj Chaturvedi MS1
1Department of Head and NeckOncosurgery, Tata Memorial Hospital,Mumbai, India2Department of Radiation Oncology, TataMemorial Hospital, Mumbai, India
CorrespondenceDeepa Nair, Department of Head andNeck Oncosurgery, Tata MemorialHospital, Dr. E. Borges Road, 12th floor,Homi Bhabha Block, Parel, Mumbai212, India.Email: [email protected]
Abstract
Background: Controversy exists regarding the administration of adjuvant radiother-apy (RT) when perineural invasion (PNI) is the only adverse histological feature. Thepurpose of this study was to evaluate the impact of PNI on the survival of patientswith oral cavity squamous cell carcinoma (SCC).
Methods: A retrospective study of 1524 treatment naive patients with oral cavitySCC who underwent surgery from January 2012 to March 2015 was conducted. Sur-vival analysis was performed using Cox regression model.
Results: The incidence of PNI was 20.3% and higher in tongue cancers (odds ratio2.43). The PNI significantly affected both disease-free survival (DFS; hazard ratio[HR] 1.84) as well as overall survival (OS; HR 1.7). Patients with early node-negative oral cavity SCC with PNI are more likely to develop recurrences and havemortality (HR 2.79 for DFS; HR 2.54 for OS). However, the addition of adjuvantradiation in these patients showed improvement in survival (p 5 .022). Forest plotanalysis showed a trend toward poor survival across all subgroups in patients withPNI.
Conclusion: Aggressive treatment of the primary cancer with the coincident manage-ment of the neck is important in the presence of PNI. The PNI worsens survival andwarrants intensification of adjuvant treatment.
KEYWORD S
adjuvant treatment, disease-free survival, oral cancer, overall survival, perineural invasion
1 | INTRODUCTION
Oral cancer is the most common cancer in India among men,the fifth most frequently occurring cancer among women,and the third most frequently occurring cancer in Indiaamong both men and women.1,2 Advanced T classification,nodal metastasis, extracapsular spread, and poorer differen-tiation are a few known poor prognostic factors for oral can-cers. Although perineural invasion (PNI) is a known poorprognostic factor with higher local recurrences, its impact onoverall survival (OS) is still under debate.
Determination of PNI is generally accepted when at least33% of the nerve circumference is surrounded by tumor cells;anything <33% is considered as the tumor proximity.3 Casesof PNI in patients with squamous cell carcinoma (SCC) of theskin,4,5 lip,6 and oral cavity7–10 are associated with locore-gional recurrences. It has been clearly demonstrated thatpatients at high risk for recurrent disease or metastasis shouldbe treated aggressively after surgery and use of adjuvant radio-therapy (RT) has shown to decrease locoregional recurrences.11
However, controversy still exists regarding the role of adjuvantRT when PNI is the only adverse histological factor. Even the
Head & Neck. 2018;1–8. wileyonlinelibrary.com/journal/hed VC 2018 Wiley Periodicals, Inc. | 1
Received: 21 July 2017 | Revised: 14 November 2017 | Accepted: 8 February 2018
DOI: 10.1002/hed.25170
1780 © 2018 Wiley Periodicals, Inc. wileyonlinelibrary.com/journal/hed Head & Neck. 2018;40:1780–1787.
National Comprehensive Cancer Network advises the use ofclinical judgment when PNI is the only adverse factor fordeciding postoperative RT. This study was performed to deter-mine the association of PNI with other histological factors andwhether PNI affects survival outcomes in patients with oralcancers. Our secondary purpose was to find out whether theaddition of adjuvant RT improves survival in patients withnode-negative oral cancer with PNI.
2 | MATERIALS AND METHODS
We performed a retrospective chart review of 1524 patientswith treatment naive biopsy proven SCC of the oral cavity oper-ated at a tertiary cancer center. All these patients underwent sur-gery as a primary modality of treatment from January 2012 toMarch 2015. All patients underwent appropriate imaging beforesurgery. We excluded patients who received any other priortreatment as well as those patients with the epicenter of diseasein the oropharynx. After surgery, the surgical specimens wereexamined for the presence of PNI on microscopic examinationby a pathologist and considered positive when at least 33% ofthe nerve circumference was surrounded by tumor cells. Theclinical and demographic details, as well as the histopathologicaldata of these patients, were obtained from the medical records.
2.1 | Treatment details
All patients underwent surgery as the primary treatment oforal cancer. Unilateral neck dissection was done in 1233cases (80.9%), bilateral neck dissection was done in 281cases (18.4%), and the neck was observed in 10 cases(0.7%). Postoperative RT and concurrent chemoradiotherapy(CRT) were given as per institutional policy. Adjuvant RTwas given when the tumor depth was >10 mm or >5 mmwith other adverse factors like PNI, poor grade of differentia-tion, or in the presence of positive neck nodes and/or closeand positive margins. Adjuvant concurrent CRT was givenin cases of positive margins and/or nodes with extracapsularspread (ECS). Adjuvant RT was given to 704 patients(46.2%), adjuvant concurrent CRT was given to 468 patients(30.7%), and 352 patients (23.09%) did not require furtheradjuvant treatment. Patients were followed up as per NationalComprehensive Cancer Network guidelines.
2.2 | Statistical analysis
Statistical analysis was done using the software SPSS version20.0 (IBM, Armonk, NY). To identify factors associated withPNI, univariate analysis was done using the chi-square test.Multivariate analysis was done using binary logistic regression.Information regarding patient survival and disease status wasalso retrieved from the medical records. Disease-free survival
(DFS) and OS were calculated using Kaplan-Meier analysis.We defined DFS as the period from the date of diagnosis untilthe date of the first recurrence, either locoregional or systemic.
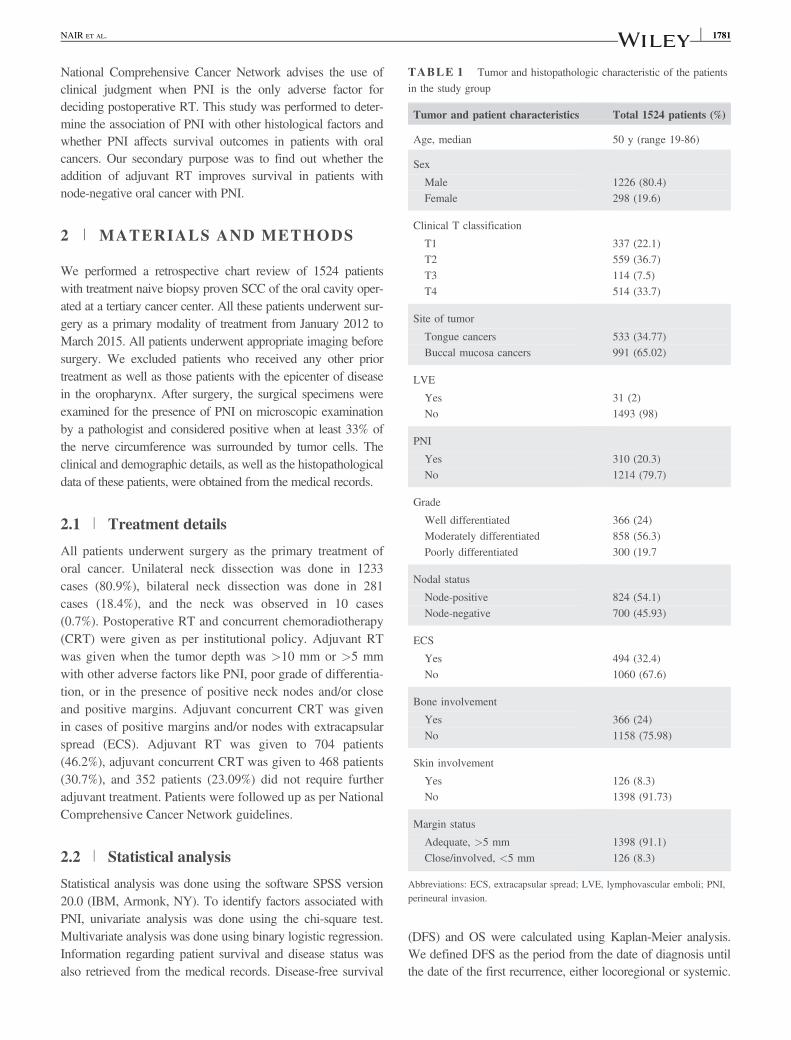
TABLE 1 Tumor and histopathologic characteristic of the patientsin the study group
Tumor and patient characteristics Total 1524 patients (%)
Age, median 50 y (range 19-86)
Sex
Male 1226 (80.4)Female 298 (19.6)
Clinical T classification
T1 337 (22.1)T2 559 (36.7)T3 114 (7.5)T4 514 (33.7)
Site of tumor
Tongue cancers 533 (34.77)Buccal mucosa cancers 991 (65.02)
LVE
Yes 31 (2)No 1493 (98)
PNI
Yes 310 (20.3)No 1214 (79.7)
Grade
Well differentiated 366 (24)Moderately differentiated 858 (56.3)Poorly differentiated 300 (19.7
Nodal status
Node-positive 824 (54.1)Node-negative 700 (45.93)
ECS
Yes 494 (32.4)No 1060 (67.6)
Bone involvement
Yes 366 (24)No 1158 (75.98)
Skin involvement
Yes 126 (8.3)No 1398 (91.73)
Margin status
Adequate, >5 mm 1398 (91.1)Close/involved, <5 mm 126 (8.3)
Abbreviations: ECS, extracapsular spread; LVE, lymphovascular emboli; PNI,perineural invasion.
2 | NAIR ET AL.NAIR ET AL. 1781
The OS is defined as the period from the date of diagnosis untildeath of any cause. Dates of disease recurrences were collectedfrom the medical records when they were diagnosed histologi-cally or radiologically. For survival analysis, the variables forunivariate analysis were selected based on their clinical rele-vance as well as those previously described in the literatureand done using the log-rank test. All significant (p < .05) vari-ables were subsequently tested (multivariate) with the Coxregression analysis using forward stepwise selection. In addi-tion, we performed subgroup analysis based on factors thatwere known to have an effect on survival.
3 | RESULTS
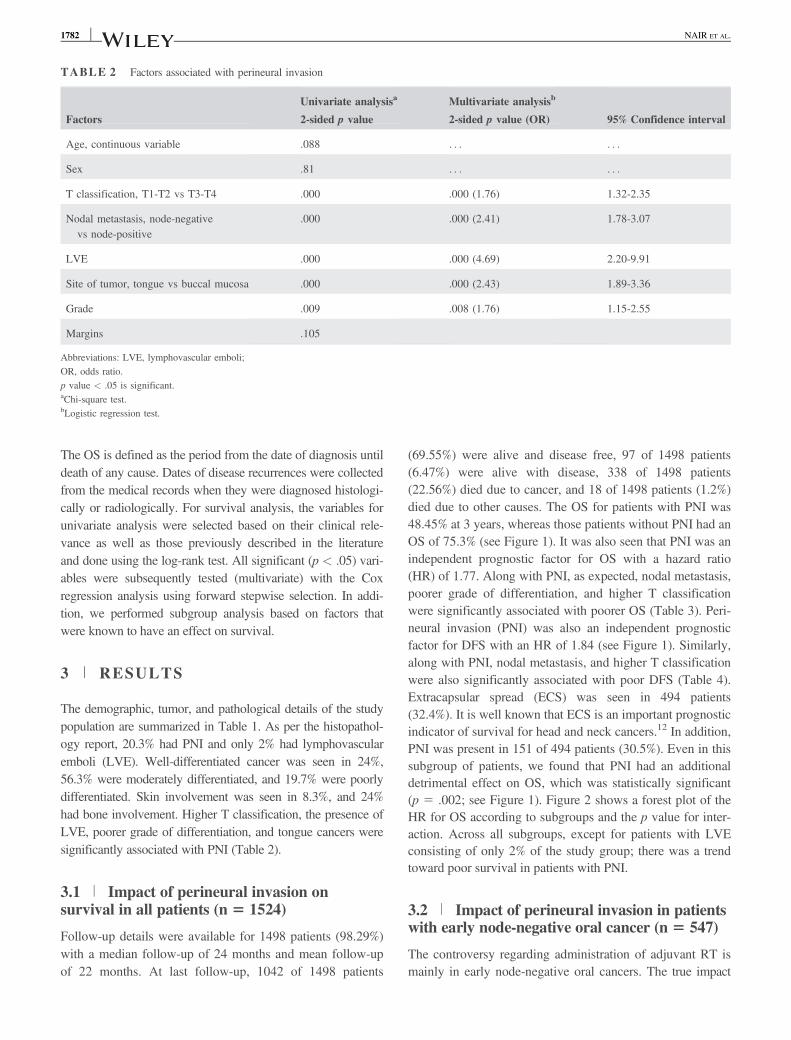
The demographic, tumor, and pathological details of the studypopulation are summarized in Table 1. As per the histopathol-ogy report, 20.3% had PNI and only 2% had lymphovascularemboli (LVE). Well-differentiated cancer was seen in 24%,56.3% were moderately differentiated, and 19.7% were poorlydifferentiated. Skin involvement was seen in 8.3%, and 24%had bone involvement. Higher T classification, the presence ofLVE, poorer grade of differentiation, and tongue cancers weresignificantly associated with PNI (Table 2).
3.1 | Impact of perineural invasion onsurvival in all patients (n 5 1524)
Follow-up details were available for 1498 patients (98.29%)with a median follow-up of 24 months and mean follow-upof 22 months. At last follow-up, 1042 of 1498 patients
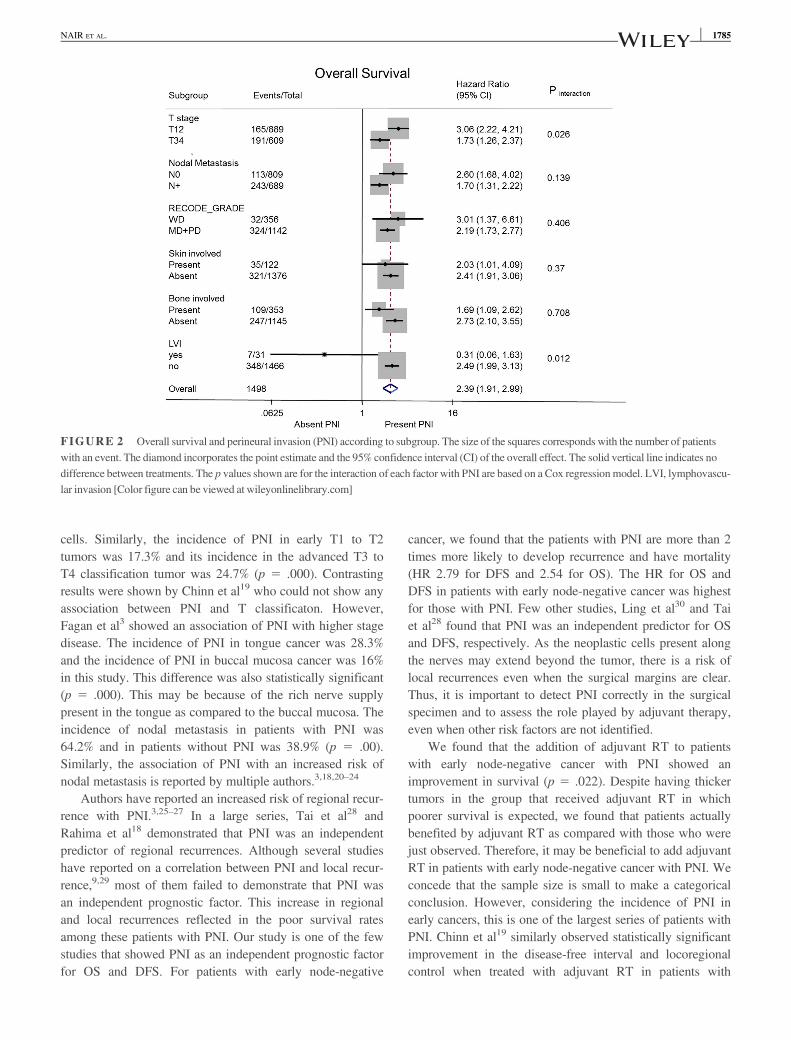
(69.55%) were alive and disease free, 97 of 1498 patients(6.47%) were alive with disease, 338 of 1498 patients(22.56%) died due to cancer, and 18 of 1498 patients (1.2%)died due to other causes. The OS for patients with PNI was48.45% at 3 years, whereas those patients without PNI had anOS of 75.3% (see Figure 1). It was also seen that PNI was anindependent prognostic factor for OS with a hazard ratio(HR) of 1.77. Along with PNI, as expected, nodal metastasis,poorer grade of differentiation, and higher T classificationwere significantly associated with poorer OS (Table 3). Peri-neural invasion (PNI) was also an independent prognosticfactor for DFS with an HR of 1.84 (see Figure 1). Similarly,along with PNI, nodal metastasis, and higher T classificationwere also significantly associated with poor DFS (Table 4).Extracapsular spread (ECS) was seen in 494 patients(32.4%). It is well known that ECS is an important prognosticindicator of survival for head and neck cancers.12 In addition,PNI was present in 151 of 494 patients (30.5%). Even in thissubgroup of patients, we found that PNI had an additionaldetrimental effect on OS, which was statistically significant(p 5 .002; see Figure 1). Figure 2 shows a forest plot of theHR for OS according to subgroups and the p value for inter-action. Across all subgroups, except for patients with LVEconsisting of only 2% of the study group; there was a trendtoward poor survival in patients with PNI.
3.2 | Impact of perineural invasion in patientswith early node-negative oral cancer (n 5 547)
The controversy regarding administration of adjuvant RT ismainly in early node-negative oral cancers. The true impact
TABLE 2 Factors associated with perineural invasion
Factors
Univariate analysisa
2-sided p value
Multivariate analysisb
2-sided p value (OR) 95% Confidence interval
Age, continuous variable .088 . . . . . .
Sex .81 . . . . . .
T classification, T1-T2 vs T3-T4 .000 .000 (1.76) 1.32-2.35
Nodal metastasis, node-negativevs node-positive
.000 .000 (2.41) 1.78-3.07
LVE .000 .000 (4.69) 2.20-9.91
Site of tumor, tongue vs buccal mucosa .000 .000 (2.43) 1.89-3.36
Grade .009 .008 (1.76) 1.15-2.55
Margins .105
Abbreviations: LVE, lymphovascular emboli;OR, odds ratio.p value < .05 is significant.aChi-square test.bLogistic regression test.
NAIR ET AL. | 31782 NAIR ET AL.

of PNI independent of other known factors can be assessedonly in early pathological node-negative oral cancers. In thissubgroup of patients, we found PNI was an independent prog-nostic factor for OS with the highest HR of 2.54. We foundthat OS at 3 years for patients with PNI was 58.4%, whereasthose patients without PNI had an OS of 86.7% (see Figure 1).Along with PNI, poor grade of differentiation and deep tumorswere associated with poorer OS, as shown in Table 5. Even forDFS (Table 6), PNI was a significant prognostic factor with ahighest HR of 2.79 (see Figure 1).
3.3 | Impact of adjuvant therapy on survivalin patients with early node-negative oralcancers with perineural invasion (n 5 60)
The next question was to find out whether the addition ofadjuvant RT would improve outcomes in this subgroup. Theincidence of PNI in early node-negative oral cancer was10.96% (60/547). Among these 60 patients, 45 patientsreceived adjuvant RT and 15 patients were observed. Theindication of adjuvant RT in these patients was tumor depth
FIGURE 1 Kaplan-Meier survival curves showing: A, overall survival (OS) in the study group; B, disease-free survival (DFS) in the study group; C,OS in patients with extracapsular spread (ECS); D, OS in patients with early node-negative oral cancers; E, DFS in patients with early-node negative oralcancers; and F, OS in patients with early-node negative cancer with perineural invasion (PNI). Cum, cumulative; OSCC, oral squamous cell carcinoma;RT, radiotherapy [Color figure can be viewed at wileyonlinelibrary.com]
4 | NAIR ET AL.NAIR ET AL. 1783

�1 cm (34 patients) or the tumor had poor differentiation(11 patients). We found that the addition of adjuvant therapywas the only significant factor affecting OS (p 5 .022) withan HR of 2.9. Other factors like the grade of differentiation(p 5 .468), T classification (p 5 .622), tumor depth (p 5.202), and margins (p 5 .897) did not have a significantimpact on OS.
4 | DISCUSSION
It is important to distinguish perineural spread from PNIbecause these terms are often used interchangeably in the lit-erature. The PNI is a histologic diagnosis that is beyond theresolution of macroscopic imaging modalities, whereas peri-neural spread is the dissemination of tumor cells along anerve that can be detected with imaging techniques.13
Perineural invasion (PNI) is defined as a tropism oftumor cells for nerve bundles in the surrounding tissues.There is a rich vascular network (vasa nervorum) includinglymphatics on the outside of loose areolar connective tissuein the epineurium. The inner layer of the epineurium has adense structure made of collagen and elastin fibers. Formany years, it was believed that these lymphatic vessels rep-resented the path for the neoplastic spread. In an article
published by Batsakis,14 in 1985, PNI was described astumor invasion in, around, and through the nerves. However,it is generally accepted that at least 33% of the nerve circum-ference has to be surrounded by tumor cells to consider PNI;anything less than 33% is just tumor proximity.3 The samecriteria have been used to consider a patient as PNI-positivein this study. However, this being a retrospective study, vari-ous parameters, such as the location of PNI, number ofnerves involved per section (PNI density), and patterns ofPNI could not be assessed. The incidence of PNI was 20.3%in this study. This is similar to the incidence of PNI reportedin head and neck cancer by various authors ranging from 6%to 30%.7,10,15,16
We found that higher T classification, nodal metastasis,poorer grade of differentiation, and tongue cancer are signifi-cantly associated with PNI. In our study, 57 of the 366patients (15.6%) with well differentiated tumors had PNI,253 of the 1158 patients (21.8%) with moderately or poorlydifferentiated tumors had PNI, and the values were statisti-cally significant (p 5 .009). A similar correlation betweentumor differentiation and PNI has been reported by Carteret al17 and Rahima et al.18 In poorly differentiated tumors,single or small groups of tumor cells can gain access to theperineural space much more easily than cohesive sheets of
TABLE 3 Factors affecting overall survival in the study group
Factors
Univariateanalysisa
p value
Multivariate analysisb
p value (HR) f95% CIg
Age, continuousvariable
.077 . . .
Sex .159 . . .
T classification,T1-T2 vs T3-T4
.000 .000 (1.6) f1.27-2.22g
Nodal metastasis,node positive vsnode negative
.000 .000 (2.5) f2.05-3.25g
Grade .000 .000 (2.1) f1.51-3.15g
Skin involvement .033 .331
Bone involvement .000 .225
PNI .000 .000 (1.7) f1.40-2.22g
LVE .540 . . .
Margins .083
Abbreviations: CI, confidence interval; HR, hazard ratio; LVE, lymphovascularemboli; PNI, perineural invasion.p value < .05 is significant.aKaplan-Meier analysis.bCox regression analysis.
TABLE 4 Factors affecting disease-free survival in the studygroup
Factors
Univariateanalysisa
p value
Multivariate analysisb
p value (HR) f95% CIg
Age, continuousvariable
.99 . . .
Sex .387 . . .
T classification,T1-T2 vs T3-T4
.000 .001 (1.59) f1.24-2.05g
Nodal metastasis,node-negative vsnode-positive
.000 .000 (2.49) f2.05-3.06g
Grade .000 .789
Skin involvement .026 .719
Bone involvement .000 .775
PNI .000 .000 (1.84) f1.50-2.27g
LVE .047 .517
Margins .031 .217
Abbreviations: CI, confidence interval; HR, hazard ratio; LVE, lymphovascularemboli; PNI, perineural invasion.p value < .05 is significant.aKaplan-Meier analysis.bCox regression analysis.
NAIR ET AL. | 51784 NAIR ET AL.
cells. Similarly, the incidence of PNI in early T1 to T2tumors was 17.3% and its incidence in the advanced T3 toT4 classification tumor was 24.7% (p 5 .000). Contrastingresults were shown by Chinn et al19 who could not show anyassociation between PNI and T classificaton. However,Fagan et al3 showed an association of PNI with higher stagedisease. The incidence of PNI in tongue cancer was 28.3%and the incidence of PNI in buccal mucosa cancer was 16%in this study. This difference was also statistically significant(p 5 .000). This may be because of the rich nerve supplypresent in the tongue as compared to the buccal mucosa. Theincidence of nodal metastasis in patients with PNI was64.2% and in patients without PNI was 38.9% (p 5 .00).Similarly, the association of PNI with an increased risk ofnodal metastasis is reported by multiple authors.3,18,20–24
Authors have reported an increased risk of regional recur-rence with PNI.3,25–27 In a large series, Tai et al28 andRahima et al18 demonstrated that PNI was an independentpredictor of regional recurrences. Although several studieshave reported on a correlation between PNI and local recur-rence,9,29 most of them failed to demonstrate that PNI wasan independent prognostic factor. This increase in regionaland local recurrences reflected in the poor survival ratesamong these patients with PNI. Our study is one of the fewstudies that showed PNI as an independent prognostic factorfor OS and DFS. For patients with early node-negative
cancer, we found that the patients with PNI are more than 2times more likely to develop recurrence and have mortality(HR 2.79 for DFS and 2.54 for OS). The HR for OS andDFS in patients with early node-negative cancer was highestfor those with PNI. Few other studies, Ling et al30 and Taiet al28 found that PNI was an independent predictor for OSand DFS, respectively. As the neoplastic cells present alongthe nerves may extend beyond the tumor, there is a risk oflocal recurrences even when the surgical margins are clear.Thus, it is important to detect PNI correctly in the surgicalspecimen and to assess the role played by adjuvant therapy,even when other risk factors are not identified.
We found that the addition of adjuvant RT to patientswith early node-negative cancer with PNI showed animprovement in survival (p 5 .022). Despite having thickertumors in the group that received adjuvant RT in whichpoorer survival is expected, we found that patients actuallybenefited by adjuvant RT as compared with those who werejust observed. Therefore, it may be beneficial to add adjuvantRT in patients with early node-negative cancer with PNI. Weconcede that the sample size is small to make a categoricalconclusion. However, considering the incidence of PNI inearly cancers, this is one of the largest series of patients withPNI. Chinn et al19 similarly observed statistically significantimprovement in the disease-free interval and locoregionalcontrol when treated with adjuvant RT in patients with
FIGURE 2 Overall survival and perineural invasion (PNI) according to subgroup. The size of the squares corresponds with the number of patientswith an event. The diamond incorporates the point estimate and the 95% confidence interval (CI) of the overall effect. The solid vertical line indicates nodifference between treatments. The p values shown are for the interaction of each factor with PNI are based on a Cox regressionmodel. LVI, lymphovascu-lar invasion [Color figure can be viewed at wileyonlinelibrary.com]
6 | NAIR ET AL.NAIR ET AL. 1785

pathological node-negative cancer with PNI. However, theyhad only 14 patients in the group who received adjuvant RTand 6 patients who did not receive adjuvant RT. Given the
controversy in the literature regarding PNI as an absoluteindication for adjuvant radiation, a larger randomized pro-spective trial would better answer this question.
5 | CONCLUSION
The presence of PNI should be carefully evaluated and docu-mented in every surgical specimen with SCC of the oral cav-ity because it has a significant prognostic value. Tonguecancers have a higher incidence of PNI. Perineural invasion(PNI) should be considered as a marker that signifies aggres-sive biologic and metastatic behavior. Thus, aggressive treat-ment of the primary cancer by adding adjuvant radiationwith the coincident management of neck lymph nodes isimportant in the presence of PNI. The addition of adjuvantRT may add survival benefit in these cases.
ORCID
Deepa Nair MS http://orcid.org/0000-0002-3560-9655Manish Mair MCh http://orcid.org/0000-0003-3957-2738
REFERENCES[1] Bray F, Ren JS, Masuyer E, Ferlay J. Global estimates of cancer
prevalence for 27 sites in the adult population in 2008. Int JCancer. 2013;132(5):1133-1145.
[2] Ferlay J, Soerjomataram I, Dikshit R, et al. Cancer incidenceand mortality worldwide: sources, methods and major patterns inGLOBOCAN 2012. Int J Cancer. 2015;136(5):E359-E386.
[3] Fagan JJ, Collins B, Barnes L, D’Amico F, Myers EN, Johnson JT.Perineural invasion in squamous cell carcinoma of the head andneck. Arch Otolaryngol Head Neck Surg. 1998;124(6):637-640.
[4] Ampil FL, Hardin JC, Peskind SP, Stucker FJ. Perineural inva-sion in skin cancer of the head and neck: a review of nine cases.J Oral Maxillofac Surg. 1995;53(1):34-38.
[5] Goepfert H, Dichtel WJ, Medina JE, Lindberg RD, Luna MD.Perineural invasion in squamous cell skin carcinoma of the headand neck. Am J Surg. 1984;148(4):542-547.
[6] Byers RM, O’Brien J, Waxler J. The therapeutic and prognosticimplications of nerve invasion in cancer of the lower lip. Int JRadiat Oncol Biol Phys. 1978;4(3-4):215-217.
[7] O’Brien CJ, Lahr CJ, Soong SJ, et al. Surgical treatment ofearly-stage carcinoma of the oral tongue–wound adjuvant treat-ment be beneficial? Head Neck Surg. 1986;8(6):401-408.
[8] Conte CC, Ergin MT, Ricci A Jr, Deckers PJ. Clinical and path-ologic prognostic variables in oropharyngeal squamous cell car-cinoma. Am J Surg. 1989;157(6):582-584.
[9] Lydiatt DD, Robbins KT, Byers RM, Wolf PF. Treatment of stageI and II oral tongue cancer. Head Neck. 1993;15(4):308-312.
[10] Brown B, Barnes L, Mazariegos J, Taylor F, Johnson J, WagnerRL. Prognostic factors in mobile tongue and floor of mouth car-cinoma. Cancer. 1989;64(6):1195-1202.
[11] Peters LJ, Goepfert H, Ang KK, et al. Evaluation of the dose forpostoperative radiation therapy of head and neck cancer: first
TABLE 6 Factors affecting disease-free survival in early node-negative oral cancers
Factors
Univariateanalysisa
p value
Multivariate analysisb
p value (HR) f95% CIg
Age, continuousvariable
.947 . . .
Sex .850 . . .
T classification,T1-T2 vs T3-T4
.113
Grade .026 .121
PNI .000 .000 (2.79) f1.72-4.52g
Tumor depth, con-tinuous variable
.002 .038 (1.32) f1.01-1.71g
LVE .931
Margins .202
Abbreviations: CI, confidence interval; HR, hazard ratio; LVE, lymphovascularemboli; PNI, perineural invasion.p value < .05 is significant.aKaplan-Meier analysis.bCox regression analysis.
TABLE 5 Factors affecting overall survival in early node-negativeoral cancers
Factors
Univariateanalysisa
p value
Multivariate analysisb
p value (HR) f95% CIg
Age, continuousvariable
.111 . . .
Sex .907 . . .
T classification T1-T2 vs T3-T4
.131
Grade .002 .008 (2.10) f1.34-7.29g
PNI .000 .001 (2.54) f1.46-4.49g
Tumor depth, con-tinuous variable
.001 .011 (1.47) f1.09-2.00g
LVI .396
Margins .088
Abbreviations: CI, confidence interval; HR, hazard ratio; LVE, lymphovascularemboli; PNI, perineural invasion.p value < .05 is significant.aKaplan-Meier analysis.bCox regression analysis.
NAIR ET AL. | 71786 NAIR ET AL.

report of a prospective randomized trial. Int J Radiat Oncol BiolPhys. 1993;26(1):3-11.
[12] Johnson JT, Myers EN, Bedetti CD, Barnes EL, Schramm VLJr, Thearle PB. Cervical lymph node metastases. Incidence andimplications of extracapsular carcinoma. Arch Otolaryngol.1985;111(8):534-537.
[13] Ginsberg LE. Imaging of perineural tumor spread in head andneck cancer. Semin Ultrasound CT MR. 1999;20(3):175-186.
[14] Batsakis JG. Nerves and neurotropic carcinomas. Ann Otol Rhi-nol Laryngol. 1985;94(4 Pt 1):426-427.
[15] Soo KC, Carter RL, O’Brien CJ, Barr L, Bliss JM, Shaw HJ. Prog-nostic implications of perineural spread in squamous carcinomas ofthe head and neck. Laryngoscope. 1986;96(10):1145-1148.
[16] Maddox WA. Hayes Martin lecture. Vicissitudes of head andneck cancer. Am J Surg. 1984;148(4):428-432.
[17] Carter RL, Tanner NS, Clifford P, Shaw HJ. Perineural spreadin squamous cell carcinomas of the head and neck: a clinicopa-thological study. Clin Otolaryngol Allied Sci. 1979;4(4):271-281.
[18] Rahima B, Shingaki S, Nagata M, Saito C. Prognostic signifi-cance of perineural invasion in oral and oropharyngeal carci-noma. Oral Surg Oral Med Oral Pathol Oral Radiol Endod.2004;97(4):423-431.
[19] Chinn SB, Spector ME, Bellile EL, et al. Impact of perineural inva-sion in the pathologically N0 neck in oral cavity squamous cell car-cinoma. Otolaryngol Head Neck Surg. 2013;149(6):893-899.
[20] Binmadi NO, Basile JR. Perineural invasion in oral squamouscell carcinoma: a discussion of significance and review of the lit-erature. Oral Oncol. 2011;47(11):1005-1010.
[21] Sutton DN, Brown JS, Rogers SN, Vaughan ED, Woolgar JA. Theprognostic implications of the surgical margin in oral squamouscell carcinoma. Int J Oral Maxillofac Surg. 2003;32(1):30-34.
[22] Woolgar JA. Histopathological prognosticators in oral and oro-pharyngeal squamous cell carcinoma. Oral Oncol. 2006;42(3):229-239.
[23] Woolgar JA. T2 carcinoma of the tongue: the histopatholo-gist’s perspective. Br J Oral Maxillofac Surg. 1999;37(3):187-193.
[24] Woolgar JA, Scott J. Prediction of cervical lymph node metasta-sis in squamous cell carcinoma of the tongue/floor of mouth.Head Neck. 1995;17(6):463-472.
[25] Wallwork BD, Anderson SR, Coman WB. Squamous cell carci-noma of the floor of the mouth: tumour thickness and the rate ofcervical metastasis. ANZ J Surg. 2007;77(9):761-764.
[26] Ross GL, Soutar DS, MacDonald DG, Shoaib T, Camilleri IG,Robertson AG. Improved staging of cervical metastases in clini-cally node-negative patients with head and neck squamous cellcarcinoma. Ann Surg Oncol. 2004;11(2):213-218.
[27] Larsen SR, Johansen J, Sørensen JA, Krogdahl A. The prognos-tic significance of histological features in oral squamous cell car-cinoma. J Oral Pathol Med. 2009;38(8):657-662.
[28] Tai SK, Li WY, Yang MH, et al. Treatment for T1-2 oral squa-mous cell carcinoma with or without perineural invasion: neckdissection and postoperative adjuvant therapy. Ann Surg Oncol.2012;19(6):1995-2002.
[29] Wang B, Zhang S, Yue K, Wang XD. The recurrence and sur-vival of oral squamous cell carcinoma: a report of 275 cases.Chin J Cancer. 2013;32(11):614-618.
[30] Ling W, Mijiti A, Moming A. Survival pattern and prognosticfactors of patients with squamous cell carcinoma of the tongue:a retrospective analysis of 210 cases. J Oral Maxillofac Surg.2013;71(4):775-785.
How to cite this article: Nair D, Mair M, Singhvi H,et al. Perineural invasion: Independent prognostic factorin oral cancer that warrants adjuvant treatment. Head &Neck. 2018;00:1–8. https://doi.org/10.1002/hed.25170
8 | NAIR ET AL.
et al. Perineural invasion: Independent prognostic factor inoral cancer that warrants adjuvant treatment.Head&Neck.2018;40:1780–1787. https://doi.org/10.1002/hed.25170
NAIR ET AL. 1787


















