Perinatal Mental Health Data Presentation to the Perinatal ERG

Perinatal Safety
Initiative:
EliminatingElective Delivery
<39 wks gestation
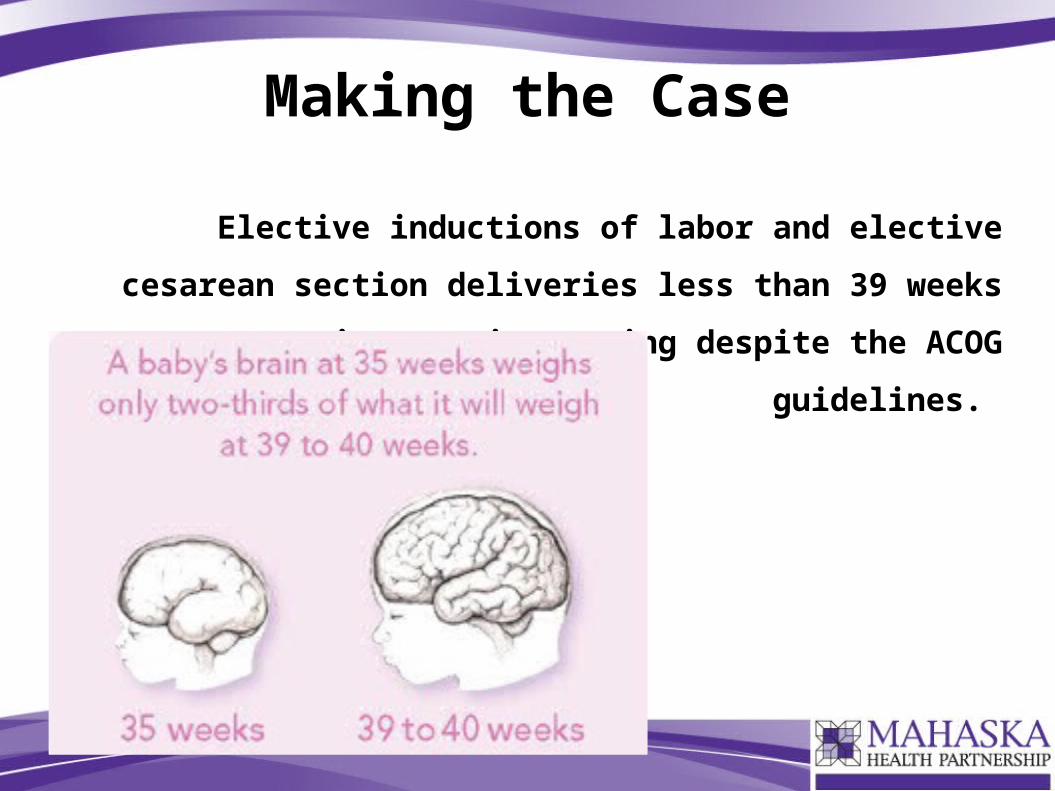
Making the Case
Elective inductions of labor and elective
cesarean section deliveries less than 39 weeks
gestation are increasing despite the ACOG
guidelines.
Making the Case
Non-medically indicated (elective) deliveries before 39 weeks gestation carry significant risks for the baby with no known benefit to the mother.
The odds of a serious neonatal complications increase with decreasing gestational duration. Common serious morbidities include respiratory complications, sepsis and hypoglycemia.
These risks are not diminished despite amniocentesis documenting a mature lung profile. Clinicians are advised that a mature lung profile does not necessarily lessen the risk of morbidity.
Making the Case• Early term deliveries: The delivery of infants who are born between 37 0/7 through
38 6/7 weeks gestation.
• Elective induction of labor: Induction of labor without an accepted medical or obstetrical indication before the spontaneous onset of labor or rupture of membranes.
• Gestational age confirmation:
Below are the ACOG criteria for determining term gestational age:
• Ultrasound measurement at less than 20 weeks of gestation supports a gestation age of 39 weeks or greater.
• Fetal heart rate tones have been documented as present for 30 weeks by Doppler ultrasonography.
• It has been 36 weeks since a positive serum or urine human chorionic gonadotropin pregnancy test.
Accepted Indications for Delivery < 39 Weeks Gestation
Things that should be taken into account:
• Maternal and fetal conditions
• Gestational age
• Cervical status
• Other factors
Gestation should be ≥ 39 weeks or a mature fetal lung test should be established, but a mature fetal lung test before 39 weeks, is not an indication for delivery, nor does it mean that the baby will experience breathing difficulties after birth.
Joint Commission Statement
Performance Measure: Elective Delivery
Description: Patients with elective vaginal deliveries or elective cesarean sections at >=37 and <39 weeks of gestation completed.
Improvement noted as: Decrease in rate
Numerator Statement: Patients with elective deliveries
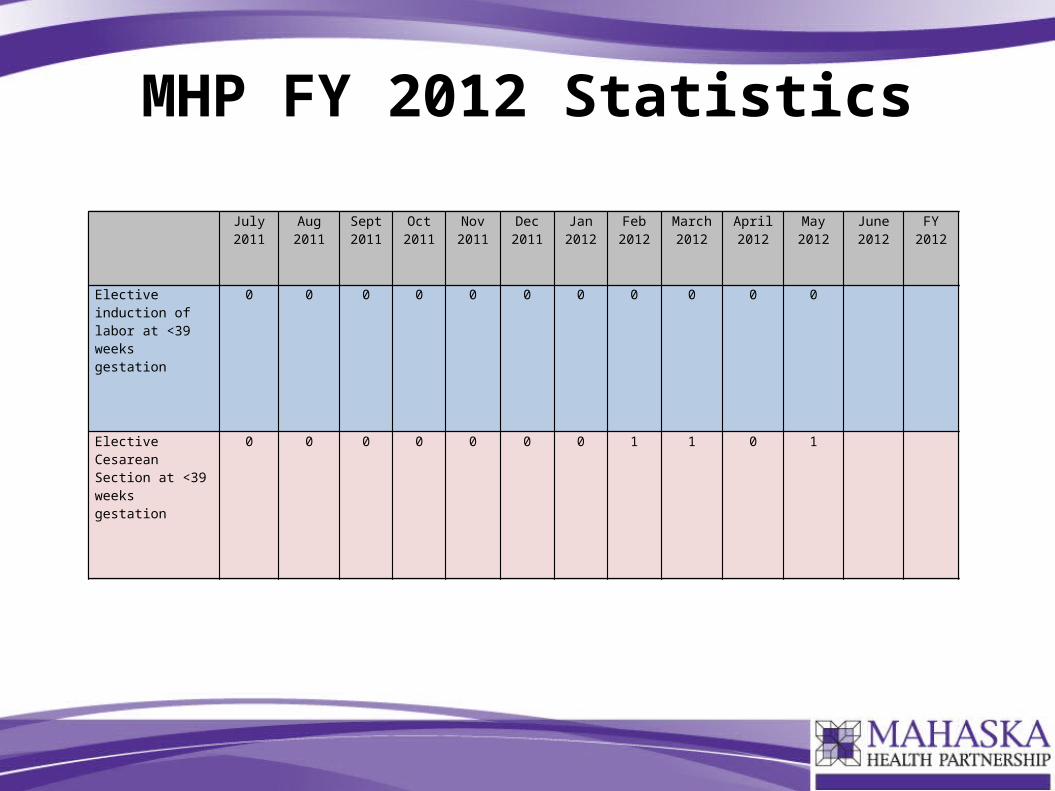
MHP FY 2012 Statistics
July2011
Aug2011
Sept2011
Oct2011
Nov2011
Dec2011
Jan2012
Feb2012
March 2012
April 2012
May2012
June2012
FY2012
Elective induction of labor at <39 weeks gestation
0 0 0 0 0 0 0 0 0 0
Elective Cesarean Section at <39 weeks gestation
0 0 0 0 0 0 0 1 2 1
July2011
Aug2011
Sept2011
Oct2011
Nov2011
Dec2011
Jan2012
Feb2012
March 2012
April 2012
May2012
June2012
FY2012
Elective induction of labor at <39 weeks gestation
0 0 0 0 0 0 0 0 0 0 0
Elective Cesarean Section at <39 weeks gestation
0 0 0 0 0 0 0 1 1 0 1

MHP FY 2012 Statistics
Jul-11 Aug-11 Sep-11 Oct-11 Nov-11 Dec-11 Jan-12 Feb-12 Mar-12 Apr-12 May-12 Jun-12
Elective induction of labor at <39 weeks gestation
0 0 0 0 0 0 0 0 0 0 0 NaN
Elective Cesarean Section at < 39 weeks gestation
0 0 0 0 0 0 0 1 1 0 1 NaN
0.5
1.5
2.5
3.5
FY 2012 - Mahaska Health Partnership
Ele
ctiv
e D
eliv
ery
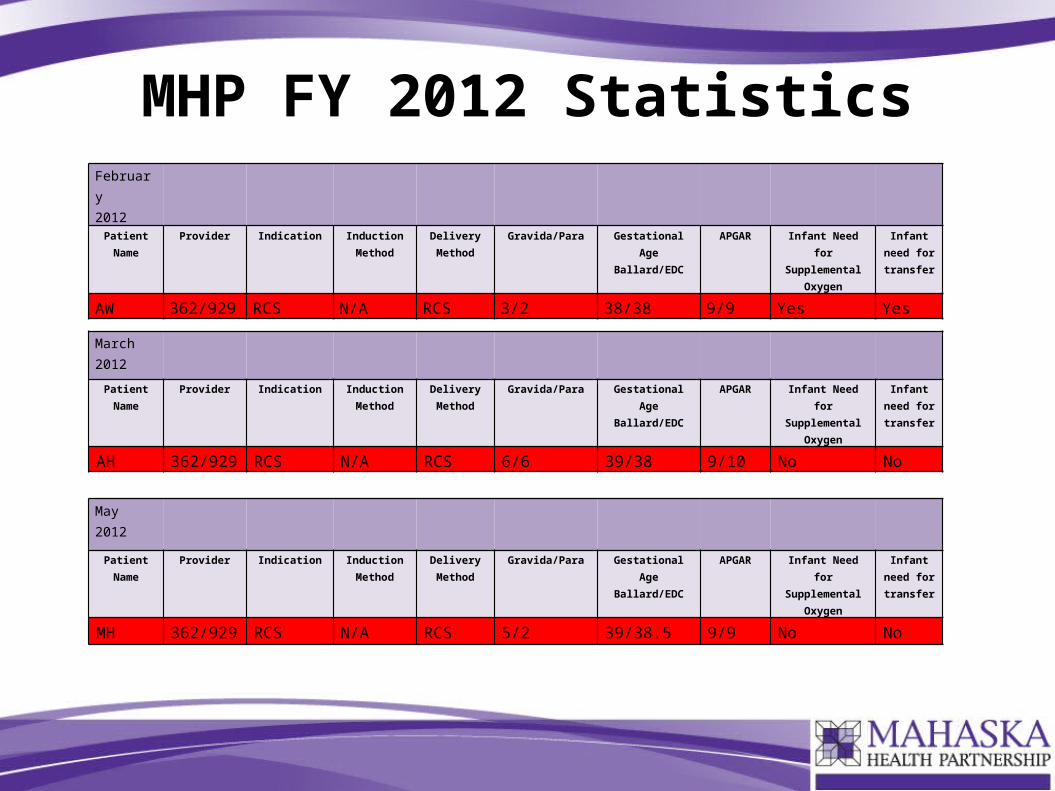
MHP FY 2012 StatisticsFebruary2012
Patient Name
Provider Indication Induction Method
Delivery Method
Gravida/Para Gestational AgeBallard/EDC
APGAR Infant Need for Supplemental
Oxygen
Infant need for transfer
AW 362/929 RCS N/A RCS 3/2 38/38 9/9 Yes Yes
March2012
Patient Name
Provider Indication Induction Method
Delivery Method
Gravida/Para Gestational AgeBallard/EDC
APGAR Infant Need for Supplemental
Oxygen
Infant need for transfer
AH 362/929 RCS N/A RCS 6/6 39/38 9/10 No No
May2012
Patient Name
Provider Indication Induction Method
Delivery Method
Gravida/Para Gestational AgeBallard/EDC
APGAR Infant Need for Supplemental
Oxygen
Infant need for transfer
MH 362/929 RCS N/A RCS 5/2 39/38.5 9/9 No No
Policy Changes
Current policy does not address elective inductions.
Recommendations include:
New Policy: Cesarean Section/Induction of Labor Scheduling Policy
Revise Policies:
- All induction policies to be combined into one Induction of Labor policy
- Define gestations as Preterm (<37 weeks, late preterm 34-36 wks), Term (37-42 wks, early term 37-39 wks), Post term (>42 wks).
- Include reporting and re-education processes
Create scheduling form
Revise Pitocin and Cytotec/Cervidil consents
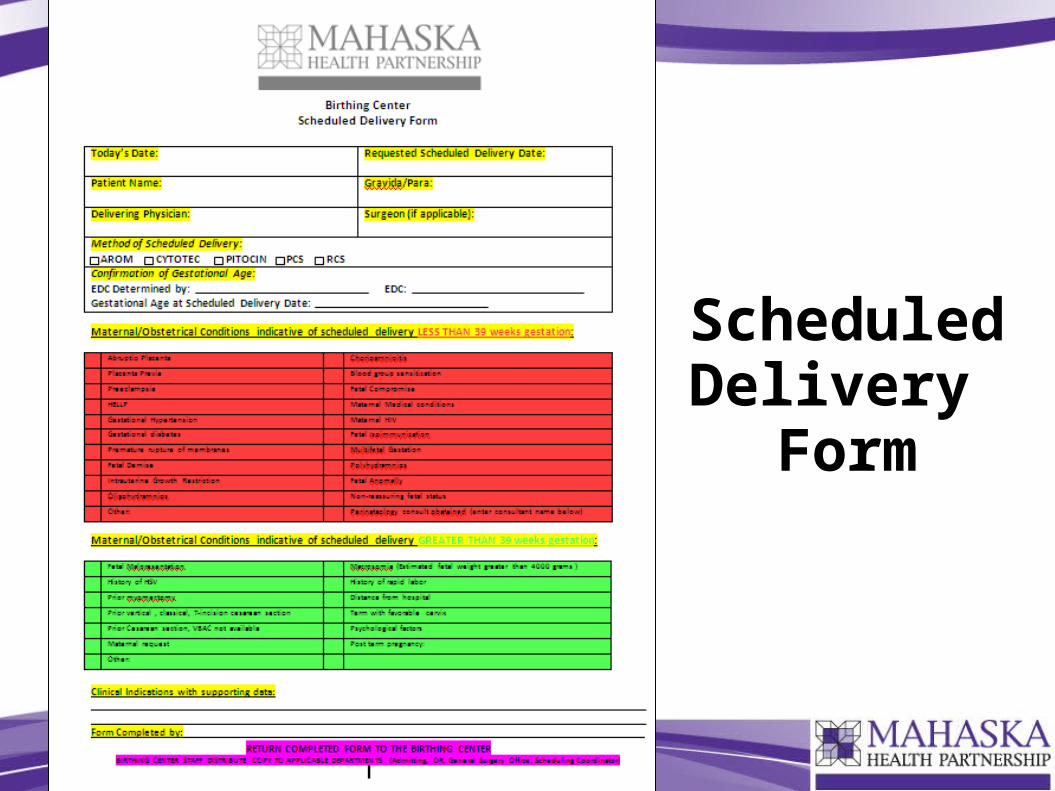
Scheduled Delivery
Form
Pitocin Checklist/Consent
Cytotec or Cervidil Checklist/Consent
Questions?
Assessment of Gestational Age by what factor? Gestation being the amount of time a baby has been in the womb.
Ultrasound <20 wks supports gestation 39 wks or greater
Elective Induction >39 wks
Monitoring for normal FHR
Completed Pelvic assessment
Monitoring and management of tachysystole
Tracking TechniquesIf an elective induction or c-section is performed at less than 39 wks
gestation, the following will be tracked and shared monthly with the Clinical Quality Committee and with clinicians at the bi-monthly Birthing Center Committee meeting.
Provider
Indication
Induction method
Delivery method
Gravida/Para
Gestational Age of Fetus (EDC)
APGAR
Infant need for supplemental oxygen
Infant need for transfer
Goals
Reduce morbidity to mother and baby, provide risk appropriate care, increase patient centered care delivery.
• Add elective induction to list of OB Committee Review Triggers
• Confirm method of determining Gestational Age (Ballard/EDC)
• Change policy and procedures to prohibit physicians from performing elective inductions or c-sections on women who are less than 39 weeks gestation, unless medically indicated.
Reasons and Implications
By following the safest elective induction process, a hospital care team can reduce the chance of harm for
both mother and baby and means that separating mother and infant from delivery is less likely. Oxytocin, used for labor augmentation and induction, has been
classified as a High-Alert Medication by the Institute for Safety Medication Practices (ISMP) and proper
informed consent should be received before administering this medication.