Performance Measurement - amga.org Patel.pdf · Pathway for Quality and Cost Measurement Core Core...
26
The Engelberg Center for Health Care Reform at Brookings | The Dartmouth Institute April 8, 2013 Kavita Patel MD, MS Fellow and Managing Director, The Brookings Institution [email protected] Performance Measurement
-
Upload
nguyencong -
Category
Documents
-
view
216 -
download
0
Transcript of Performance Measurement - amga.org Patel.pdf · Pathway for Quality and Cost Measurement Core Core...

The Engelberg Center for Health Care Reform at Brookings | The Dartmouth Institute
April 8, 2013
Kavita Patel MD, MS
Fellow and Managing Director, The Brookings Institution
Performance Measurement

The Engelberg Center for Health Care Reform at Brookings | The Dartmouth Institute
ACO Implementation Across the Country
{Not exhaustive}
ACO implementation is now accelerating
across the country
*Upwards of 390
ACOs*
Private Sector
= Beacon Communities
= PGP Demonstration, MHCQ
Public Sector
= Pioneer
= MSSP
= Private Sector ACO’s


The Engelberg Center for Health Care Reform at Brookings | The Dartmouth Institute
Accountable-care payment reforms
Medical Homes for
Primary Care • Supports care coord,
prevention, chronic disease
mgmt, and other key
primary-care activities
• Rewards reductions in
primary care-related cost
trends
Bundled Payments for
Specialty/Intensive Care
and Post-Acute Care • Combine payments across
providers/ settings for specific
episodes for better coord
• Linked to quality measures and
resource use measures
Accountable Care Organizations • Reimburses population-level improvements in quality and overall
per-capita costs
• Encourages coordination across care continuum
• Can reinforce/ support “piecewise” accountable-care reforms
• Performance measures
for quality and cost
(outcome-oriented)
• Timely and consistent
methods for sharing
underlying data with
providers, suppliers to
improve performance
• Rapid evaluation
methods based on
common measures
Performance-Based Payments for Drugs, Devices • Supports targeting treatments to patients likely to benefit, not
necessarily greater volume
• Likely to succeed with timely performance measures and
differences across patients
The Engelberg Center for Health Care Reform at Brookings | The Dartmouth Institute
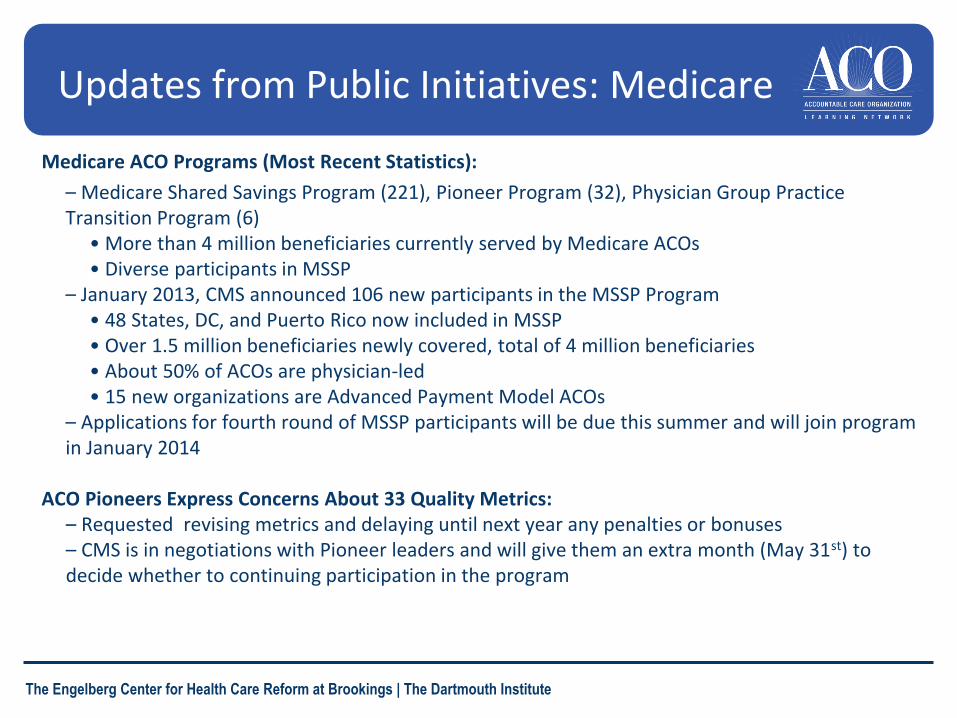
Updates from Public Initiatives: Medicare
Medicare ACO Programs (Most Recent Statistics):
– Medicare Shared Savings Program (221), Pioneer Program (32), Physician Group Practice Transition Program (6)
• More than 4 million beneficiaries currently served by Medicare ACOs • Diverse participants in MSSP
– January 2013, CMS announced 106 new participants in the MSSP Program • 48 States, DC, and Puerto Rico now included in MSSP • Over 1.5 million beneficiaries newly covered, total of 4 million beneficiaries • About 50% of ACOs are physician-led • 15 new organizations are Advanced Payment Model ACOs
– Applications for fourth round of MSSP participants will be due this summer and will join program in January 2014
ACO Pioneers Express Concerns About 33 Quality Metrics:
– Requested revising metrics and delaying until next year any penalties or bonuses – CMS is in negotiations with Pioneer leaders and will give them an extra month (May 31st) to decide whether to continuing participation in the program

The Engelberg Center for Health Care Reform at Brookings | The Dartmouth Institute
Updates from Public Initiatives: Medicaid
6
• At least 14 states undertaking ACO initiatives in Medicaid and SCHIP
– Example: Oregon Community Care Organizations
• Large-scale demonstration programs for Medicare-Medicaid Financial Alignment
– 3 states likely starting in 2013, and many more in 2014
– Example: Massachusetts

Our quality improvement strategy is to concurrently pursue three aims
7
Better Care Improve overall quality by making health
care more patient-centered, reliable,
accessible and safe.
Healthy People /
Healthy Communities
Improve population health by supporting
proven interventions to address
behavioral, social and environmental
determinants of health, in addition to
delivering higher-quality care.
Affordable Care Reduce the cost of quality health care for
individuals, families, employers and
government.

CMS Vision for Quality Measurement
• Align measures with the National Quality Strategy and Six Measure Domains
• Implement measures that fill critical gaps within the 6 domains
• Align measures across CMS programs whenever possible
• Parsimonious sets of measures; core sets of measures
• Removal of measures that are no longer appropriate (e.g., topped out)
• Align measures with external stakeholders, including private payers and boards and specialty societies
• Major aim of measurement is improvement over time
8

Quality Measurement & Performance for ACOs
Quality measures are separated into the
following four key domains that will serve
as the basis for assessing, benchmarking,
rewarding and improving ACO quality
performance:
– Better Care
1. Patient/Caregiver Experience
2. Care Coordination/Patient Safety
– Better Health
3. Preventative Health
4. At-Risk Population

Quality Measurement & Performance for ACOs Continued
ACO Quality Performance Standard made up of 33 measures
intended to do the following:
• Improve individual health and the health of populations
• Address quality aims such as prevention, care of chronic
illness, high prevalence conditions, patient safety, patient
and caregiver engagement and care coordination
• Support the Shared Savings Program goals of better care,
better health and lower growth in expenditures
• Align with other incentive programs like PQRS and EHR
• Exhibit sensitivity to administrative burden

Quality Data Reporting
• Quality data collected three ways:
– Claims and other internal data
– ACO-GPRO tool
– CG-CAHPS (Survey)
• Complete and accurate reporting in the first year qualifies the
ACO to share in the maximum available quality sharing rate
• Pay for reporting is phased in for the remaining performance
years
• Shared savings payments are linked to quality performance
based on a sliding scale that rewards attainment
– High performing ACOs receive a higher sharing rate

• ACO quality measures are monitored to determine if
ACOs are avoiding at risk beneficiaries
• ACOs must meet minimum attainment level on 70
percent of the measures in a given domain in order to
avoid poor performance sanctions
• An ACO determined to be avoiding at risk
beneficiaries could receive sanctions or be
terminated
Quality Measurement and ACO Monitoring

Next Steps for Performance Measurement for ACOs
• Development of Outcome measures, specified at the
ACO level
– Complications of outpatient procedures/surgeries
(colonoscopy, cataract) within 7 days
– All-cause unplanned admissions for individual chronic
diseases and patients with MCCs
– PROs (function, symptom resolution, etc.)
• Expand reporting options
– Clinical Data Registry
– EHRs
• starting 2014, groups can report CQMs as a group for stage 2 of
MU
13

Ongoing Work Related to Aligning CMS Programs with other Measure Reporting Efforts
• Registries (many led by physician specialty societies) are the
fastest growing portion of PQRS
– all payer data
– robust set of measures
– success rates via registries are very high
• PQRS incentive related to MOC
• ATRA requirement to allow measures reported to registries
count for PQRS
• Increased bidirectional communication and engagement
between CMS and Boards and Specialty Societies
• Significant work to align measures across public and private
payers
14

© 2011 Advocate Physician Partners
Value a la Porter
Advocate Porter
• Inpatient Mortality • Survival
• Inpatient Complications and Intermediate Measures to Reduce Complications
• Degree of Recovery
• Amb. Sensitive ER Visits/1000
• Disutility of Care
• Functional Status in MSSP • Functional Status
• Access • Time to Recovery

© 2011 Advocate Physician Partners
Exhibit 2. Pathway for Quality and
Cost Measurement
Core
Core Plus
Advanced
Interim Process
Diabetes: HbA1c Testing CAD: ACE Inhibitor or ARB Therapy
Diabetes: HbA1c Control (<8%) CAD: LDL-C Level <100 mg/dl
Diabetes: Cost of Care Over 1-Year Period CAD: Drug Therapy for Lowering LDL Cholesterol
Diabetes: Physical Functioning CAD: 10-Year Risk of Developing Hard CHD

17
Domain Measure Title
Quality and Cost Measures: Ramp-Up Strategy
B-D Pilot Initial Contracts CMS Proposal for MSSP Final MSSP Core Core Plus Interim Process Advanced
Patient / Care Giver Experience CAHPS: Getting Timely Care, Appointments, and Information X X X X
CAHPS: How Well Your Doctors Communicate X X X X
CAHPS: Patients' Rating of Doctor X X X X
CAHPS: Health Promotion and Education X X X
CAHPS: Shared Decision Making X X X
CAHPS: Access to Specialists X X
CAHPS: Health Status/Functional Status X X X
Family Evaluation of Hospice Care (NHPCO) X
Care Coordination / Patient Safety Risk-Standardized, All Condition Readmission X X X
Care Transition Measure X X
Ambulatory Sensitive Conditions Admissions: Chronic Obstructive Pulmonary Disease X X X
Ambulatory Sensitive Conditions Admissions: Congestive Heart Failure X X X
Annual Monitoring for Patients on Persistent Medications X X
Percent of PCPs who Successfully Qualify for an EHR Incentive Program Payment X X
Medication Reconciliation: Reconciliation After Discharge from an Inpatient Facility X X X
Falls: Screening for Fall Risk X X X
Preventive Health Breast Cancer Screening X X X X
Cervical Cancer Screening X X
Proportion of Adults 18+ who had their Blood Pressure Measured within the preceding 2 years X X
Cholesterol Management for Patients with Cardiovascular Conditions X X X
Influenza Immunization X X X
Pneumococcal Vaccination X X X
Colorectal Cancer Screening X X X X
Adult Weight Screening and Follow-up X X X
Tobacco Use Assessment and Tobacco Cessation Intervention X X X
Depression Screening X X X
Health Risk Assessment X

4/11/2013 18
Domain Measure Title
Quality and Cost Measures: Ramp-Up Strategy
B-D Pilot Initial Contracts CMS Proposal for MSSP Final MSSP Core Core Plus Interim Process Advanced
At-Risk Population
Diabetes Hemoglobin A1c Management (testing) X X
LDL-C Screening X X
Hemoglobin A1c Control (<8%) X X X X
Low Density Lipoprotein (LDL-C) Control X X X X
Hemoglobin A1c Poor Control (>9%) X X X X
High Blood Pressure Control X X X X
Urine Screening for Microalbumin or Medical Attention for Nephropathy X X X
Dilated Eye Exam X X
Total Cost of Care: Diabetes over a 1-Year Period X
Tobacco Non-Use X X X
Aspirin Use X X X
Foot Exam X X
Quality of Life in Patients with Diabetes (DQOL, ADDQoL) X
Psychological Functioning in Patients with Diabetes (DHP) X
Heart Failure Left Ventricular Function (LVF) Assessment X X
Left Ventricular Function (LVF) Testing X X
Total Cost of Care: CHF Over 1-Year Period X
Weight Measurement X X
Patient Education X X
Beta-Blocker Therapy for Left Ventricular Systolic Dysfunction (LVSD) X X X
Angiotensin-Converting Enzyme (ACE) Inhibitor or Angiotensin Receptor Blocker (ARB) Therapy for Left Ventricular Systolic Dysfunction (LVSD) X X
Warfarin Therapy for Patients with Atrial Fibrillation X X
Physical Function in Patients with Heart Failure (KCCQ) X
Quality of Life in Patients with Heart Failure (KCCQ) X
Cardiac and Vascular Conditions
Angiotensin-Converting Enzyme (ACE) Inhibitor or Angiotensin Receptor Blocker (ARB) Therapy for Patients with CAD and Diabetes and/or Left Ventricular Systolic Dysfunction (LVSD) X X X X
LDL-C level <100 mg/dl X X
IVD: Complete Lipid Panel and LDL Control X X
Total Cost of Care: CAD Over 1-Year Period X
Composite: All or Nothing Scoring X X
Oral Antiplatelet Therapy Prescribed for Patients with CAD X X
Drug Therapy for Lowering LDL Cholesterol X X X
Beta-Blocker Therapy for CAD Patients with Prior Myocardial Infarction (MI) X X
Ischemic Vascular Disease (IVD): Use of Aspirin or Another Antithrombotic X X
6-Month Mortality Following CABG Surgery X
10-Year Risk of Developing Hard CHD (Framingham Risk Score) X
Physical Limitation from Angina (SAQ) X
Quality of Life in Patients with CAD (KCCQ) X

4/11/2013 19
Domain Measure Title
Quality and Cost Measures: Ramp-Up Strategy
B-D Pilot Initial Contracts CMS Proposal for MSSP Final MSSP Core Core Plus Interim Process Advanced
Hypertension Blood Pressure Control X X X X
Plan of Care X
Quality of Life in Patients with Hypertension (CAMPHOR) X
COPD
Total Cost of Care: Patients with Stable COPD Over a 1-Year Period X
Total Cost of Care: Patients with Unstable COPD Over a 1-Year Period X
Spirometry Evaluation X X
Smoking Cessation Counseling Received X X
Bronchodilator Therapy based on FEV1 X X
Respiratory Function in Patients with COPD (SGRQ) X
Emotional Functioning in Patients with COPD (CRQ) X
Frail /Elderly Osteoporosis Management in Women Who had a Fracture X X
Monthly INR for Beneficiaries on Warfarin X X
Total Cost of Care: Management of Frail Elderly X
Physical Functioning (IADL) X
Depression in Older Adults (GDS) X
Pediatrics Appropriate Testing for Children with Pharyngitis X X
Treatment for Children with Upper Respiratory Infection X X
Childhood Immunization Status X X
Immunization for Adolescents X X
Physical Functioning in Children (CHQ) X
Asthma Use of Appropriate Medications for People with Asthma X X
Functional Status: Asthma Impact (PROMIS) X
Palliative Care and End-of-life Care*
Patients with Advanced Cancer Assessed for Pain at an Outpatient Visit (RAND) X
Patients Admitted to ICU Who Have Care Preferences Documented (RAND) X
Pain Management: Pain Brought to a Comfortable Level with 48 Hours of Initial Assessment (NHPCO) X
Percentage of Hospice or Palliative Care Patients Who Were Screened for Dyspnea during the Hospice Admission Evaluation/Palliative Care Initial Encounter (UNC/PEACE) X
Overuse Low Back Pain: Use of Imaging Studies X X
Antibiotic Treatment for Adults with Acute Bronchitis: Avoidance of Inappropriate Use X X
Other Conditions ESRD: Plan of Care for Inadequate Peritoneal Dialysis, Adult X
Ambulatory Status at 6 Months Following Knee Replacement Surgery X
Cost of Care
Per Capita Resource Utilization for All Patients over a 1-Year Period (risk adjusted) X
All Populations Functional Status: Physical Functioning (PROMIS, SF-36) X
Functional Status: Physical Activity (UCLA Activity Scale) X
Functional Status: Emotional Distress (Anxiety/Depression) (PROMIS) X
Functional Status: Depression Severity (PHQ-9) X
Functional Status: Social Functioning (SF-36) X

The Engelberg Center for Health Care Reform at Brookings | The Dartmouth Institute
• In year 1, scoring is based on complete and accurate reporting
• Benchmarks are calculated based on FFS/MA or ACO performance
• Beginning in year 2, CMS will set a performance benchmark and a minimum attainment level. For each measure: 1) performance below minimum attainment level = 0 quality points; 2) between minimum attainment level and benchmark, quality points are awarded on a sliding scale; 3) above benchmark = 2 quality points
0% 100%
Quality
Points
Minimum
Attainment Level
Performance
Benchmark
2
1
0 Points
Maximum quality
score: 2 Points
Quality measure scoring
The Engelberg Center for Health Care Reform at Brookings | The Dartmouth Institute
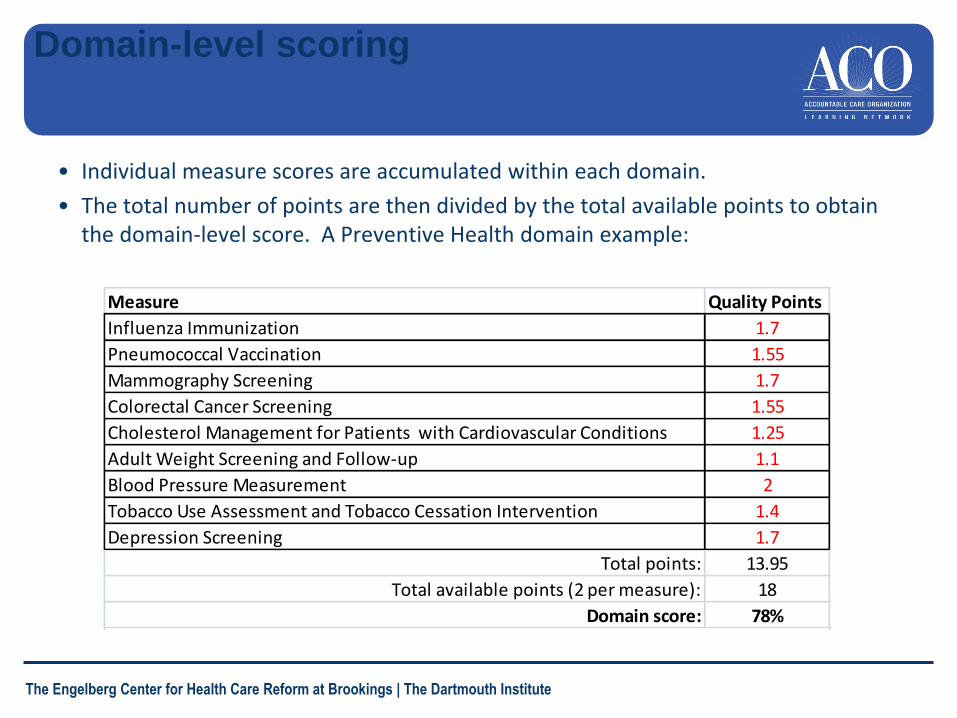
• Individual measure scores are accumulated within each domain.
• The total number of points are then divided by the total available points to obtain the domain-level score. A Preventive Health domain example:
Measure Quality Points
Influenza Immunization 1.7
Pneumococcal Vaccination 1.55
Mammography Screening 1.7
Colorectal Cancer Screening 1.55
Cholesterol Management for Patients with Cardiovascular Conditions 1.25
Adult Weight Screening and Follow-up 1.1
Blood Pressure Measurement 2
Tobacco Use Assessment and Tobacco Cessation Intervention 1.4
Depression Screening 1.7
Total points: 13.95
Total available points (2 per measure): 18
Domain score: 78%
Domain-level scoring

The Engelberg Center for Health Care Reform at Brookings | The Dartmouth Institute
• Each of the five domains is weighted equally to determine the quality performance sharing rate.
• For example:
Domain Year 1 Year 2 Year 3
Patient/Caregiver Experience 57% 71%
Care Coordination 75% 78%
Patient Safety 50% 50%
Preventive Health 78% 78%
At-Risk Population/Frail Elderly Health 80% 75%
Quality performance sharing rate: 100% 68% 70%
Must report all
measures for
payment
Note: CMS is reserving the right to audit submitted performance data; proposed is
audit mechanism as in PGP demo.
Calculating the Quality Performance Sharing
rate

The Engelberg Center for Health Care Reform at Brookings | The Dartmouth Institute Courtesy of HealthReformWatch

4/11/2013 25
The Engelberg Center for Health Care Reform at Brookings | The Dartmouth Institute
Thank You [email protected]