Percutaneous Insertion Use and Contraindications.
32
Percutaneous Insertion Use and Contraindications
-
Upload
abner-cook -
Category
Documents
-
view
231 -
download
0
Transcript of Percutaneous Insertion Use and Contraindications.
Percutaneous InsertionUse and Contraindications

Background
Drive towards minimal invasive surgery Advancement of endovascular techniques Expanding indication Larger device profiles required More aggressive anticoagulation

Vascular Access
transfemoral most common small sheath sizes (<9F) - manual
compression larger sheath sizes - open groin dissection alternative routes: brachial, radial, carotid
and popliteal
Haemostasis:factors
Affected by– 1) Patient factors
age weight comorbid conditions - hypertension, coagulopathies
– 2) Procedural factors use of anticoagulation sheath sizes puncture site
Percutaneous Access
has been limited by sheath size can be achieved by
– smaller device profiles– closure devices

External compression
external compression– manual or mechanical
disadvantages– patient discomfort, mobility restricted– labour intensive (time and effort)– prolonged compression - anticoagulation and
large sheath sizes (>9F)– less effective with high punctures

Access Site Complications
angiogram 0.5-1.5% balloon angioplasty 1-3% coronary stenting 5-17% endoluminal(open groin) 13-14%

Closure Devices
Developed over the last 10 years. Driven by objectives to
– reduce vascular complications– reduce time to ambulation/discharge– reduce patient discomfort

Closure Devices: Types
Extravascular– implantable collagen plug (Vasoseal)– collagen/thrombin injection
Intravascular– bio-absorbable haemostatic anchor (Angio-
Seal)– percutaneous suture device (Prostar XL and
Closer)
Closure Devices
Advantages– secure haemostasis -
large bore/anticoagulation, high punctures
– minimal compression– patient comfort and
mobility
Disadvantages– high costs– steep learning curve– closure related
complications– delayed repuncture

Device Related Complications
persistent bleeding arterial/venous occlusion arterial dissection arteriovenous fistula pseudoaneurysm foreign body embolism infection

Closure Devices
emerging suggestions of new pattern of complications
no decrease in the incidence of complications– reduction in minor complications but no
reduction in major complications complications tend to occur later
Closure Devices
Dangas, G. et al J Am Coll Cardiol 2001– retrospective review of closure devices
(n=516)) versus manual compression (n=5892 more frequent haematoma (9.3% vs 5.1% p<0.001) higher significant haematocrit drop (5.2% vs 2.5%
p<0.001) higher rate of surgery (2.5% vs 1.5%, p=0.03) similar rates of pseudoaneurysms and arteriovenous
fistulae

VasoSeal (Datascope)
biodegradable purified bovine collagen sponge
deployed through an applicator sheath into the soft tissue tract, directly over the arterial puncture site
requires inflow compression during application
followed by manual compression

VasoSeal Trials
Schrader, R. et al. 1992 randomised trial n=100vs manual compression
decreased compressiontime(4 vs 42 min),bleeding(0 vs 6) andhaematomas (4 vs 11)
Edoardo, C. et al. 1994 randomised trial n=124vs manual compression
no significant differencein complications
Silber, S. et al. 1998 randomised n=150.vs manual compressionMatched sheath dwelltime and anticoagulation
significant reduction intime to haemostasis but nodifference in localcomplications
Carere, R. et al. 1999 retrospective study, 204applications in 182patients
complications in 31% ofapplicationssurgical rate 11.5%
VasoSeal: Advantages
extravascular does not enlarge arteriotomy seals diseased arteries early repuncture

VasoSeal: Disadvantages
relies solely on thrombus plug limited to <9F requires 2 operators high failure rate in obese patients ambulation delay (1-3hr) infection - antibiotics, pseudoaneurysms obstruction

Angio-Seal (Sherwood)
3 bioabsorbable components - anchor, collagen plug and connecting suture
contained in a delivery sheath deployed on wire at end of procedure anchor in lumen holds collagen plug in
place

Angio-Seal Trials
Aker, U. et al. 1994 case series n=32 91% deployment success35% required pressure
Henry, M. et al. 1995 case series n=84 96% deployment success2% required pressure
Kussmaul, WG. et al 1995 randomised trial angioseal(n=218) vs manual(n=217)
96% deployment success34% required pressurelower complication rates
Ward. SR. et al 1998 randomised trialamgioseal (n=202) vsmanual (n=102)
earlier haemostasisquicker time to dichargecomplications 9% vs 6%
Eidt, J. et al 1999 retrospective angio-seal(n=425) vs manual(n=1662)
8% failure6% obstruction1.6% surgical rate

Angio-Seal: Advantages
easy to learn one operator secure plug no external compression

Angio-Seal: Disadvantages
intraluminal anchor - obstruction, infection limited to <9F enlarges arteriotomy ambulation delay (1-3hr) repuncture delay (weeks)

Duett (Vascular Solutions)
temporary balloon occlusion and extravascular injection of collagen/thrombin through a sideport.

Duett: Advantages
does not enlarge arteriotomy 1 operator immediate repuncture simple conversion to compression

Duett: disadvantages
intravascular administration ambulation delay (1-3hr) diseased vessels
Perclose Prostar and Closer
percutaneous suturing of vessel wall closure of large sheath sizes (10F) requries one operator immediate repuncture possible immediate ambulation very steep learning curve

Prostar Trial
Sprouse, L.R. et al J Vasc Surg 2001– retrospective review of patients requiring
vascular surgery admission following use of Prostar (n=11) and manual compression (n=14)
pseudoaneurysm are larger and do not respond to ultrasound compression
complications result in more blood loss and increased need for transfusions
infections are more common abd require aggressive surgery
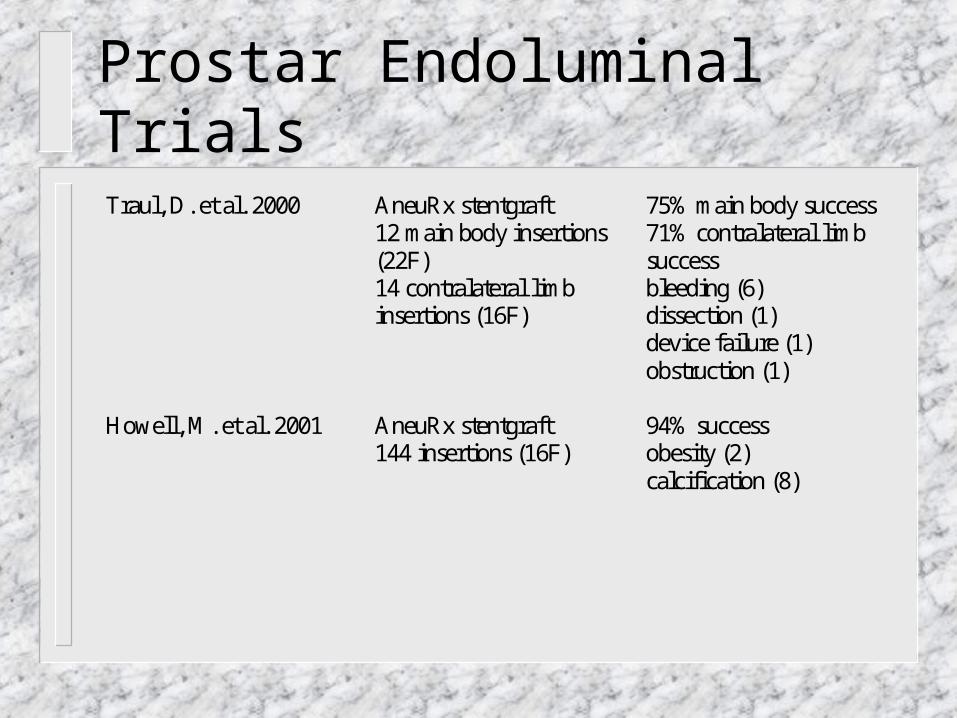
Prostar Endoluminal Trials
Traul, D. et al. 2000 AneuRx stentgraft12 main body insertions(22F)14 contralateral limbinsertions (16F)
75% main body success71% contralateral limbsuccessbleeding (6)dissection (1)device failure (1)obstruction (1)
Howell, M. et al. 2001 AneuRx stentgraft144 insertions (16F)
94% successobesity (2)calcification (8)
Perth Prostar Experience
Aims– evaluate results of our early experience
Methods– 82 percutaneous closures in 44 patients– 10F Prostar XL PVS device– 1 iliac, 1 thoracic and 42 abdominal aortic
aneurysms– product specialist present

Perth Prostar Experience
Preclose method (Haas, P. Et al. 1999)– limited (1cm) incision– subcutaneous tract dilatation– needles deployed prior to endoluminal stent– sutures tied at end of procedure

Perth Prostar Experience
Results– 12 failures requiring surgical intervention (14.6%)– reasons for failure
tortuous iliac artery (2) scarred groin (1) obesity (5) sutures catching (1) high CFA bifurcation (2) pseudoaneurysm (1)
Perth Prostar Experience
Pitfalls– obesity– calcified, turtuous iliofemoral vessels– angled proximal necks

Conclusion
Open groin dissection remains the standard Patient selection is vital Tutorlage and experience vital Monitor for late complications Surgical skills to recognise and deal with
complications