Percko T-shirt effects on the posture in a sitting and ... · Percko T-shirt effects on the posture...
17
Percko T-shirt effects on the posture in a sitting and standing position Longuet 1 S, LE BORGNE 2 P, BAUCHER 2 J, GOSSARD 1,2 C 1 Ostéobio, 19 rue de Gare, 94230 Cachan 2 Cogitobio, 19 rue de Gare, 94230 Cachan Abstract Introduction The spine is organized into a segmental pattern. It performs its own function of equilibrium. A "bad" posture usually results in a forward position of the upper block relative to the lower one. Holding this posture creates stress, increasing muscle stiffness, which can lead to pain. The purpose of this study is to analyze the effects of a t-shirt, designed to bring the thoracic spine above the pelvis, in a standing and sitting position and during scaption. Materials and Methods 12 adults with history of low-back pain have maintained a standing and sitting position and performed a scaption movement. Each condition was performed with and without t-shirt. Several angles of the standing and sitting postures were measured as well as scapular plane elevation, COP motion and EMG activity. The results were calculated based on intra-individual changes. Results In standing and sitting position, wearing the T-shirt leads to a pelvic anteversion (4 ± 2), which increases lumbar lordosis (5°± 2). It decreases thoracic kyphosis (30% ± 20) unrelated to the orientation of the head (r² = 0.30). In the frontal plane, an outward motion of the chest is observed (standing: 5°± 2; sitting: 4 ± 2 °). It reduces COP motion in the anteroposterior axis (35 ± 13%) and decreases EMG activity (standing: 28% ± 12; sitting: 37% ± 14). Discussion Wearing T-shirt results in the straightening of the spine, bringing back the thoracic spine above the gravity line going through the pelvis. Overall balance is improved, and muscle fatigue risks are reduced.
Transcript of Percko T-shirt effects on the posture in a sitting and ... · Percko T-shirt effects on the posture...

Percko T-shirt effects on the posture in a sitting and standing position
Longuet1 S, LE BORGNE2 P, BAUCHER2 J, GOSSARD1,2 C
1-‐ Ostéobio, 19 rue de Gare, 94230 Cachan
2-‐ Cogitobio, 19 rue de Gare, 94230 Cachan
Abstract
Introduction
The spine is organized into a segmental pattern. It performs its own function of equilibrium. A "bad" posture usually results in a forward position of the upper block relative to the lower one. Holding this posture creates stress, increasing muscle stiffness, which can lead to pain. The purpose of this study is to analyze the effects of a t-shirt, designed to bring the thoracic spine above the pelvis, in a standing and sitting position and during scaption.
Materials and Methods
12 adults with history of low-back pain have maintained a standing and sitting position and performed a scaption movement. Each condition was performed with and without t-shirt. Several angles of the standing and sitting postures were measured as well as scapular plane elevation, COP motion and EMG activity. The results were calculated based on intra-individual changes.
Results In standing and sitting position, wearing the T-shirt leads to a pelvic anteversion (4 ± 2), which increases lumbar lordosis (5°± 2). It decreases thoracic kyphosis (30% ± 20) unrelated to the orientation of the head (r² = 0.30). In the frontal plane, an outward motion of the chest is observed (standing: 5°± 2; sitting: 4 ± 2 °). It reduces COP motion in the anteroposterior axis (35 ± 13%) and decreases EMG activity (standing: 28% ± 12; sitting: 37% ± 14).
Discussion Wearing T-shirt results in the straightening of the spine, bringing back the thoracic spine above the gravity line going through the pelvis. Overall balance is improved, and muscle fatigue risks are reduced.

Introduction
According to the French association of rheumatology [1] and the ANAES [2], lumbago is defined as "lumbosacral pain at iliac crest level or lower, middle or lateral, with the possibility of spreading although not higher than the knee but with a predominance of lumbosacral pain.” Lumbago is a common condition that affects about 70% of the French population [2]. According to Andersson[3], it affects between 70 and 85% of people at some point in their lives.
Lumbagos are particularly common among young adults with a greater impact at adolescence and towards the age of 45-50. [4]. It later decreases among men, but there is another spike in frequency among women starting at the age of sixty, the reason for that is the postmenopausal osteoporosis [3,5]. This constant increase in frequency in the last 50 years in all of the industrial countries has led to heavy and costly repercussions in the socio-professional environment. According to the HAS in a 2005 study [6], lumbago cases are responsible in France for about 6 million medical appointments per year and represent the main cause of disability at work for people aged under 45. [4]
And according to the data published in 2010 by the INRS, lumbago has also become the main cause for sick leave and is the cause for about a quarter of work injuries with sick leave reaching 55 days [4].
It is therefore a public health problem but also an economic one and because of the high costs for society, improving the treatment of this pathology remains a top priority, hence a high number of frequent consultation motives with healthcare professionals [7].
Lumbago is a general term used to describe pain felt in the lumbar region but it is not the only description for it because in the majority of cases, the pathophysiological mechanisms at the source of the lumbar pain are complicated, multifactorial and difficult to explain. In literature among the many risk factors of the initial stages of lumbago and other factors favoring the transition to a chronic state, apart from the psychosocial factors, there is also adapting a maladjusted posture for an extended period of time. It is true, mechanical and physical stress that the individual experiences can wear the spinal muscles down [8]. A nociceptive reflex is added to the sensory and proprioceptive reflexes regulating posture and movement. This nociceptive reflex is the cause for active muscular stiffness [9] and responsible for lumbar pain [8].
People with chronic lumbago have a posture imbalance because of an antalgic position. People affected by chronic lumbago should develop postural strategies in order to manage and regulate this imbalance.
Studies on people with lumbago in a standing position in comparison to healthy test subjects have revealed an increase of the pressure center movement relative to the center of gravity. Nies and Sinott [10] have shown by studying the position of the pressure center on the anteroposterior axis, that the backward tilt is more pronounced among people suffering from chronic lumbago. It was explained with a lack of knee extension which is a position taken by

people suffering from chronic lumbago to relieve lumbar pain. There is a difference in amplitude between the postural oscillations depending on the pain. Compared to healthy people, people with chronic lumbago experience high amplitude oscillations with constant pain [11]. People with chronic lumbago who experience episodic pain have similar postural oscillations as healthy people. [12]
Other studies on lumbago patients have shown an increase of the contraction of the antagonist muscles during a brutal trunk discharge [13], as well as an increase in activation of the erector spinae muscles while walking [14]. There is also a delay in activation of the trunk stabilizer muscles and therefore an injury risk [15, 16]. In case of exhaustion people with lumbago will easily develop strategies to activate the abdominal muscles faster in the purpose of stabilizing the lumbar spine [17]. A more pronounced inhibitory action of the quadriceps muscles has also been observed in people with lumbago in comparison to healthy subjects [18]. The person with lumbago uses his lower limb muscles more in order to adapt his posture during movement and thus tilts the pelvis backwards to diminish the lumbar curvature and the pressure applied on the tissues.
The combination of the balancing strategies allows a participant suffering from lumbago to compensate his imbalances. These strategies are based on the segmental model modified by antalgic postures.
Study in standing position.
In the sagittal plane, the spine alternates between flexible rods (lordosis) and rigid as well as semi-rigid segments (kyphosis [19, 20, 21]; the direction of deformation of this group stays in the sagittal plane. Muscles are active elements of the balancing system. Because of the existence of curvatures a small range of movement is enough to re-balance the spine. The energy spent on balancing the spine, the polyarticular curve structure, is not very significant or at least less than the one that would be useful if the vertebral column was straight-lined from every angle. The main function of this curvature configuration is to adapt to the gravity pressure and to maintain it in a state of orthostatic balance while allowing locomotion.
A number of studies have been done in order to understand what the spine does to react to this balancing action. The vertebral column is similar to a deformable spring that cushions pressure applied by gravity [22]. In 1955, Dempster [23] suggests segmental modeling in the sagittal plane. In 1988, Johansson and al [24], compare the standing position to an inverted pendulum. This pendulum starts at the ankle and manages the balance of the whole body; the balance is maintained thanks to the alignment of the vertical projection of the gravity center with the pressure center [25]. In 1999, Runge & al [26] suggest a segmental modeling of the musculoskeletal system that alternates between three flexible rods (one lower limb rod, one lumbar and one cervical) and three rigid segments (the pelvic, thoracic and cephalic segments (cf. Figure1). The rods that support the segments have for foundation corresponding hinge regions (lumbosacral region and cervicothoracic region) that is to say regions of movement change. To maintain balance it is essential to have an alignment of the hinges on the gravity axis [27] and superposition of the segments.
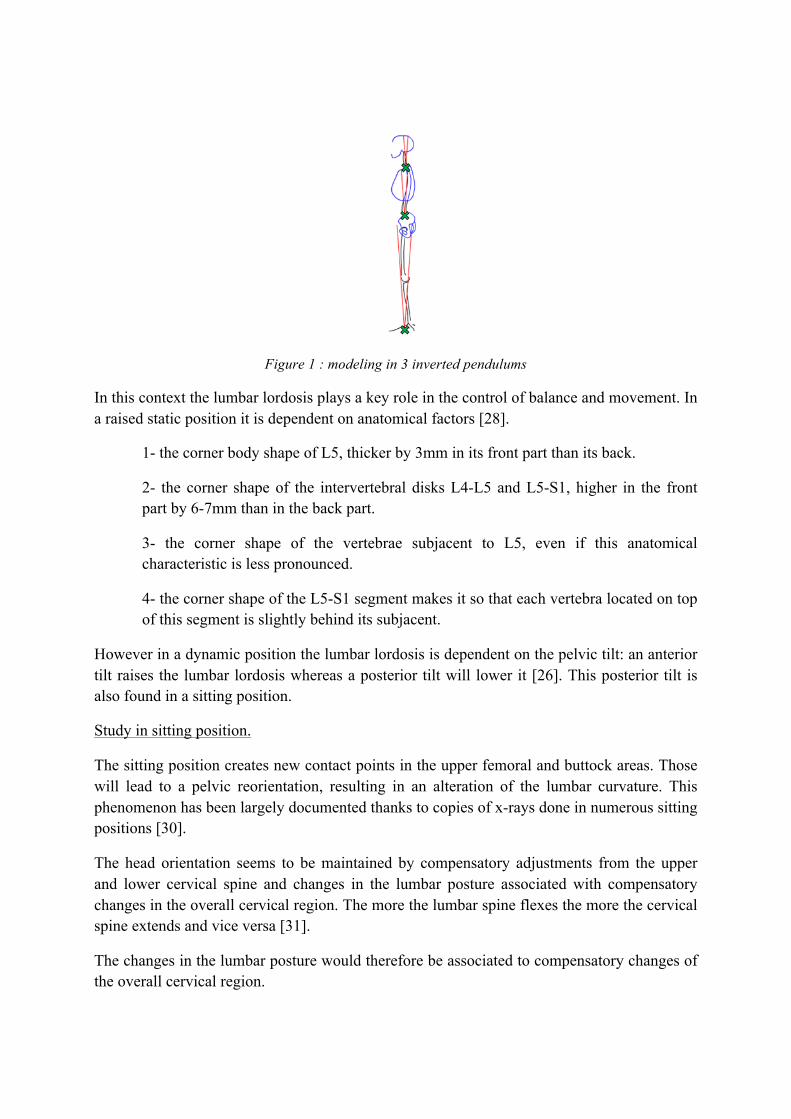
Figure 1 : modeling in 3 inverted pendulums
In this context the lumbar lordosis plays a key role in the control of balance and movement. In a raised static position it is dependent on anatomical factors [28].
1- the corner body shape of L5, thicker by 3mm in its front part than its back.
2- the corner shape of the intervertebral disks L4-L5 and L5-S1, higher in the front part by 6-7mm than in the back part.
3- the corner shape of the vertebrae subjacent to L5, even if this anatomical characteristic is less pronounced.
4- the corner shape of the L5-S1 segment makes it so that each vertebra located on top of this segment is slightly behind its subjacent.
However in a dynamic position the lumbar lordosis is dependent on the pelvic tilt: an anterior tilt raises the lumbar lordosis whereas a posterior tilt will lower it [26]. This posterior tilt is also found in a sitting position.
Study in sitting position.
The sitting position creates new contact points in the upper femoral and buttock areas. Those will lead to a pelvic reorientation, resulting in an alteration of the lumbar curvature. This phenomenon has been largely documented thanks to copies of x-rays done in numerous sitting positions [30].
The head orientation seems to be maintained by compensatory adjustments from the upper and lower cervical spine and changes in the lumbar posture associated with compensatory changes in the overall cervical region. The more the lumbar spine flexes the more the cervical spine extends and vice versa [31].
The changes in the lumbar posture would therefore be associated to compensatory changes of the overall cervical region.

Furthermore the sitting position raises the intradiscal pressure [32]; the disk is subjected to creep [33]. This excess pressure is on the one hand linked with the non-involvement of the rear apophyseal joints when the spine is bending slightly. On the other hand it is linked to the high resistance offered by the rear ligament formation. The rear articulations withstand 16% of the pressure in the standing position, whereas in the sitting position they do not sustain any pressure while in compression [34]. There is a link between the intradiscal pressure and the minimum stress posture.
The results show a forces balance mechanism in Lordosis postures under static pressure, whereas postures in flexion lead to a high rise of tension forces in the rear area of the annulus [35]. Yet excessive tension for extended periods of time is damaging to the preservation of the mechanical properties of the ligaments [36]: for a number of participants adopting a sitting position entails that they have already reached maximum vertebral flexion and therefore maximum pull on the rear ligaments [37].
This postural load has been identified by Adams and Hutton in 1985 [38], it has revealed that the sitting position is not as harmless as one might think. Sitting relaxes the lower limbs but transfers pressure towards the lower back. Additionally the vertebral column of the sitting person stays under pressure from the load even though the person feels relaxed. The extended sitting position is harmful if the physiological curvatures are not respected.
In conclusion, the lumbar lordosis linked with the pelvic tilt appears to be a key element in the balancing and stressing of the different structures and in the response of the active elements involved by this stress. The objective of this study is to analyze the effects of the second skin (T-shirt with tensors) on the posture. The goal of the second skin is to bring the thoracic block on top of the pelvis, in order to avoid and/or decrease lumbar pain in a standing or sitting position. To do so we have compared postures with and without second skin in a sitting and standing position during scaption movement.
Materials and methods.
The majority of the experiments were performed in the laboratory of Ostéobio. Twelve adults, 7 men and 5 women aged between 22 and 45 (27±7years), have volunteered to participate in the study. Thanks to x-rays of the participants we were able to choose people with different morphotypes as described by Roussouly [39]. Similarly we wanted to represent the diversity of the population with subject sizes going from the 5th percentile for women to the 95th for men (norm EN IS0 15537).
The participants have all stated that they have already felt pain in the lumbar area in the past but not at the moment of the tests. The participant selection has been done after a postural qualitative study based on photos done in a sagittal view. The bent posture has been found by visualizing the bending of the different blocks in relation to the vertical line passing through the ankles. (cf. Figure 2). Participants are then given "second skin" T-shirts described below. A photo is done in similar conditions with the "second skin (cf. Figure 2)

a) b)
Figure 2 : a) photo without the second skin and gravity axis modeling - b) superimposing postures with and without the “second skin”.
Participants were not informed on the purpose of the "second skin".
Participants were equipped with 18 retroreflective markers and were filmed with 6 Vicon cameras at a 100HZ frequency. These different markers were placed in a way that represents different segments like the pelvis, thorax, head, arm and forearm and then monitor the development of the external spinal curvatures. They were also equipped with 2 EMG electrodes located on the spine erector muscles, longissimus muscle. The electrodes placement is made following the recommendations of SENIAM.
The participants positioned themselves bare feet on a force platform AMTI set to 1000HZ, with their arms parallel to their bodies.

Figure 3 : a) T-shirt seen from the back - b) description of the different features of the T-shirt.
The T-shirt (cf. Figure 3) is comprised of a thoracic part (A) done with a material that is not deformable vertically. It encompasses the rib cage and thoracic vertebrae and is maintained by a tensor (B) at rib level K10.
The (C) part of the T-shirt is made with a very stretchable material that can be stretched in both directions.
From a rear point of view, the tensors (D) are glued on the thoracic part, go through the shoulders and extend by 5cm on the front of the thorax.
The (E) tensors are attached on the (B) tensor that is on the sides of the rib cage. They merge with the (D) tensors and secure it in the lumbar curvature at L4 level.
The belt (F) enables to secure the T-shirt in the pelvic area.
A number of tests were done with and without the second skin:
- Staying in standing position for 30 seconds ("natural" position of the individual) with the sight fixed horizontally.
- Staying in a horizontal sitting position for 15 minutes. This study was measured at T=5minutes.
- Arm rotation in the "natural" scaption in a standing and sitting position.
In order to analyze the changes in posture, different parameters were measured:
• Pelvic orientation (Pel in °): the angle projected in the sagittal plane between the straight line passing through the middle of the greater trochanters and the middle of the anterior superior iliac spines and the vertical line.

• Thoracic orientation (Tho in °), calculated from the angle of projection in the sagittal plane between the straight line passing through the xiphoid process (AX) and spinous process of (T9) and the horizontal.
• Thoracic bending (Dtho in mm) calculated as the distance between the middle of the segment [AX; T9] and the straight vertical line passing through the middle of the greater trochanters.
• The cephalic bending (Cerv en °): is the angle between the straight line passing through the middle of the two mastoid processes and the middle of the acromion and the vertical line.
• Horizontal sight (Eye in °): angle between the straight line passing through the middle of the two mastoid processes and the middle of the eyes and the horizontal plane.
• Opening of the thorax (OT in °): angle projected on the horizontal plane between the straight lines passing through the spinous process of T4 and the right and left acromion.
• Thoracic kyphosis (RT in mm): curvature radius of a circle passing through the spinous processes of T1, T4, T9, T12.
• Scapular plane (Scap in °): Angle calculated between the arm and straight line passing through the acromion during scaption movement when the arm is on a horizontal plane.
• The pressure center movement: major axis (LCp in mm) and minor axis (lCp in mm) of the movement area of the pressure center.
• The area under the EMG curvature (SurfEMG) calculated over a 30s interval of time.
The results of the measured parameters vary according to each individual because of the morphometric heterogeneity of each participant (size and morphotype among others). Our goal is not to compare the participants between each other but to measure the effect of the T-shirt, which is why we have calculated the variations as a percentage of the different parameters with and without the T-shirt, in a sitting and standing position.
Results
The results shown below are based on the tests with the T-shirt.
Posture in the sagittal plane:

Board 1 : Posture angle in a standing position with and without the "second skin"
(A positive difference of Pel represents a forward tilt of the pelvis, a positive difference of Tho represents an extension of the thorax, a positive difference of DTho represents a decline of the thorax. A positive difference of Cerv represents a decline of the head; a positive difference of the eye represents an extension of the head. The difference of Tho as a percentage matches the percentage of thorax straightening to get closer to the vertical line by going through the middle of the great trochanters).
Board 2 : Angle of sitting posture with and without the « second skin »
The results in terms of posture (Board 1 and Board 2) show, that in a standing position as well as in a sitting position wearing the T-shirt increases the forward tilt of the pelvis. On average the pelvis tilts more forward, Pelv increases between 4°±2 in a sitting as well as standing
sujet Δ Pel (°) Δ Tho (°) Δ Dtho (mm) Δ Dtho (%) Δ Cerv (°) Δ Eye (°)1 4 7 20 50 3 -‐12 2 5 29 83 10 23 8 8 49 82 15 04 3 2 28 93 7 15 8 6 40 77 3 16 2 4 12 50 3 07 5 5 43 78 5 -‐18 3 5 33 97 2 09 4 2 9 43 11 010 6 5 32 73 4 111 2 2 14 93 9 112 4 4 22 69 7 -‐1
moyenne 4 5 28 74 7 0ecartype 2 2 12 17 4 1
variation entre la position debout sans et avec "seconde peau"
sujet Δ Pel (°) Δ Tho (°) Δ Dtho (mm) Δ Dtho (%) Δ Cerv (°) Δ Eye (°)1 3 8 26 52 5 02 2 4 17 74 8 13 7 10 41 91 10 04 2 2 11 48 13 -‐15 6 5 22 65 2 06 2 4 11 73 4 37 3 4 43 78 8 18 4 7 31 74 3 29 4 3 9 43 5 110 4 5 22 65 3 -‐211 3 4 14 93 8 012 5 4 28 82 8 0
moyenne 4 5 23 70 6 0ecartype 2 2 11 15 3 1
variation entre la position assise sans et avec "seconde peau"

position. This tilt allows an increase of the lordosis and a backward tilt of the thoracic block (Tho= 5°±2 in a sitting as well as standing position). The bigger the backward tilt of the Pelvis the greater the thoracic block decline is. The middle point of [AX; T9] aims to approximately represent the gravity center of the thoracic block. The latter declines (on average by 23mm±11 in a sitting position and 28mm±12 in a standing position) and mostly corrects the anterior tilt of the block (on average 70%±15 in a sitting position and 74%±17) with a maximum of 93%. There is no significant linear correlation between the pelvic and thoracic difference (R²=0.36) which could be explained by different behavior in the lumbar area (shape and flexibility of the lumbar column).
At the same time wearing the T-shirt leads to a lower kyphosis (cf. Figure 4), causing a straightening of the thoracic segment (increase of the bending radius by 30%±20)
Figure 4: dekhyphosis and bending radius.
In the cervical area the gravity center of the head is pulled back while remaining in front of the shoulders gravity line (on average Cerv =6°±3 in sitting position and Cerv= 7°±4). We can notice once again that there is no statistical link between the decrease of the cephalic and thoracic tilting (R²=0.30)
We can notice that despite the postural changes of different blocks of the vertebral column, the orientation of the head stays the same (0°±1 in a sitting as well as standing position). It should be noted that it was the only postural instruction given to the subjects.
Posture in the horizontal plane:

Board 3 : Angle change of the scapular plane with and without the T-shirt
In the horizontal plane the straightening is followed by an opening of the Thorax.
Regarding the requirement for arm bending, the straightening in the sagittal plane is followed by an opening of the thorax (Board 3) (on average 5°±2 in standing position and on average 4°±2 in a sitting position); this leads to a change of the physiologic angle that goes backwards in the scaption (on average 9°± 3 in a standing position and on average 7°± 2 in a sitting position).
Global balance and EMG :
Board 4: percentage variation of the ellipse major and minor axis in a standing position, with and without the T-shirt.
sujet Δ OT debout (°) Δ Scap debout (°) Δ OT assis (°) Δ Scap assis (°)1 4 7 4 62 4 5 3 43 8 12 8 84 6 10 5 95 7 13 5 116 3 5 2 67 8 12 7 108 7 10 4 99 2 5 2 510 6 9 5 711 4 7 2 712 5 9 5 7
moyenne 5 9 4 7ecartype 2 3 2 2
variation dans le plan horizontal sans et avec tee-‐shirt
sujet Δ LCp (%) Δ lCp (%)1 35 72 27 -‐23 50 44 22 15 34 56 25 -‐57 67 98 35 39 21 910 30 311 29 -‐312 44 7
moyenne 35 3ecartype 13 4
variation axe ellipse sans et avec tee-‐shirt

Figure 5 : example of pressure center movement, without the second skin in red and with the second skin in green (the axis x represents the antero-‐posterior axis, the Y axis represents the lateral.
In terms of global balance, in a standing position we can notice a decrease of the ellipse axis in the antero-posterior direction (on average 35%±13), with no significant modifications in the lateral direction (on average 3% ±4). (cf. Figure 5 and Board 4: Percentage variation of the major and minor axis of the ellipse in a standing position with and without the T-shirt).
The EMG amplitude varies greatly between individuals. It is not only linked to the interindividual postural tonicity but also to the experimental errors regarding the placement of the electrodes. To assess the muscular activity fluctuations we sought to normalize the results for the same individual. To do this we took the maximum area under the curve matching the sitting position without “second skin” and compared this result to the other test conditions.
Figure 6 : Variation of muscular activity in percentage.
287
288
289
290
291
292
293
294
295
296
297
173 178 183 188 193 198 203
sans ellipse avec
0
20
40
60
80
100
0
20
40
60
80
100
avec sans avec sans
debout assis
VariaQons de l'acQvité musculaire en pourcentage par rapport à la situaQon assise sans "seconde peau"
moyenne max min
The EMG activities decrease systematically while wearing the T-shirt (cf: figure 6) no matter the experimental condition: 28%±12 in a standing position and 37%±14 in a sitting position.
Discussion
The objective of the study was to prove that wearing the T-shirt improves the posture. Almost systematically a “bad” posture, in a mechanical sense, results in the movement to the front of the upper block in relation to the lower block. A bad posture translates in the cervical area by pain in the trapezius muscle region and in the lumbar area by pain in the rachis erectors region (iliocostalis and rachis erector)
A number of authors have demonstrated the importance of the pelvic orientation on the overlying curvatures and the bending in relation to the gravity axis [40, 41]. In the same way our results show that wearing the T-shirt leads to a pelvic anteversion. Based on the working principle of the inverted pendulum [25], this forward tilt leads to an increase of the lumbar lordosis and a backward lean of the thoracic block, this leads to a straightening in order to return this block on top of the gravity line passing through the pelvis.
At kinetic level the fluctuations of the pressure center translate the oscillations of the different blocks that need permanent balance readjustment with muscular action [42]. The smaller the ellipse in which the pressure center varies, the more stable and efficient the posture will be [42]. Thus considering the results of the pressure center, by modifying the superposition of the blocks the T-shirt improves the posture. This improvement seems to be confirmed by the results of the EGM that showed a decrease of muscular activity in the posture stabilizing area. Thus because the different spinal blocks were returned towards the gravity axis thanks to the effect of the tensors, the active intervention of the superficial stabilizer muscles is in the long term less important. This leads to a decrease of muscular fatigue [43] as well as a decrease of the stiffness [44]. In a sitting as well as standing position the EMG activity of people suffering from lumbago is linked to pain [45], the decrease of the stabilizing activity of the muscles when wearing the T-shirt leads to a decrease of the pain. The study will be supplemented by an analysis of the evolution of posture and EMG activity when maintaining a sitting position for a long period of time (2 hours).
However it should be noted that the independent contribution of the tensors and the thoracic part of the T-shirt cannot be precisely defined after this study. That is why an additional study done with x-rays on the deformation of the vertebral column should be done. It would allow in particular measuring more specifically the thoracic straightening by using the Cobb angle [46].
Furthermore, the dekhyphosis enables the movement of the scapula on the ribs and decreases the pressure in the shoulder articulation, thus enabling a more functional range of movement. In addition in a sitting position this dekhyphosis, followed by the opening of the thorax (cf. Figure 8), improves the breathing capacity involved in the control of the posture by releasing the diaphragm. [47,48].
Finally no matter the experimental condition, the results have shown a decline of the head’s center of gravity with no link to the underlying changes. Despite an ascending posture organization [49], the horizontal position of the head, which is a necessary requirement to keep the sight horizontal, [50], seems to be preserved. (cf. Figure 7)

Figure 7 : Posture evolution with Percko second skin in a sitting position. Without (in red) vs with (in green).
Figure 8 : Opening of the thorax
This study has helped show that wearing the T-shirt changes the superposition of the blocks, this allows to decrease the pressures and discomfort, while preserving the horizontality of the sight which is essential to control the posture. However it would be interesting to study even further the effect of the T-shirt on the different morphotypes as well as on subjects suffering from sharp and chronic lumbago. Finally since the posture is based on a postural body image [51, 52] powered by sensory information [53], wearing the T-shirt for extended periods of time helps adopt a lasting and perfect posture.

Références
1. Duquesnoy B, Defontaine MC, Grardel B, Maigne JY, Thevenon A,Vignon E. Définition de la lombalgie chronique. Rev Rhum (Ed Fr). 1994, 61(4bis): 9S-10S.
2. Agence Nationale d'Accréditation et d'Evaluation en Santé (ANAES) (2000). Diagnostic, prise en charge et suivi des malades atteints de lombalgie chronique. Paris.
3. Andersson GBJ. The epidemiology of spinal disorders. In: Frymoyer JW, ed. The adult spine: principles and practice, 2nd ed. Philadelphia: Lippincort-Raven; 1997.
4. Goupille P, Avimadje AM, Zerkak D, Valat JP. Eléments cliniques d'orientation diagnostique devant une lombalgie. Rev Prat. 2000, 50(16):1760-4.
5. Stebler R, Putzib R, Michela B. Douleurs lombaires, diagnostic. Forum Med Suisse. 2001, Fev;9: 205-208.
6. Haute Autorité de Santé (HAS). Prise en charge masso-kinésithérapique dans la lombalgie commune: modalités de prescription. HAS. Paris. 2005.
7. Wipf JE, Deyo RA. Low back pain. Med Clin North Am. 1995; 79: 231-46. 8. Hoogendoorn WE, Bongers PM, de Vet HC, Ariëns GA, van Mechelen W, Bouter
LM. High physical work load and low job satisfaction increase the risk of sickness absence due to low back pain: results of a prospective cohort study. Occup Environ Med. 2002, May;59(5):323-8.
9. Clark, RW, Harris J. The organization of motor responses to noxious stimuli. Brain Research Reviews. 2004, 46, 163-172.
10. Nies N, Sinnott PL. Variations in balance and body sway in middle-aged adults. Subjects with healthy backs compared with subjects with low-back dysfunction. Spine (Phila Pa 1976). 1991 Mar;16(3):325-30.
11. Hamaoui A, Do M, Poupard L, Bouisset S (2002) Does respiration perturb body balance more in chronic low back pain subjects than in healthy subjects? Clinical Biomechanics, 17, 548-50.
12. Mok NW, Brauer SG, Hodges PW. Hip strategy for balance control in quiet standing is reduced in people with low back pain. Spine (Phila Pa 1976). 2004 Mar 15;29(6):E107-12.
13. Radebold A, Cholewicki J, Polzhofer GK, Greene HS. Impaired postural control of the lumbar spine is associated with delayed muscle response times in patients with chronic idiopathic low back pain. Spine (Phila Pa 1976). 2001 Apr 1;26(7):724-30.
14. Arendt-‐Nielsen L, Graven-‐Nielsen T, Svarrer H, Svensson P. The influence of low back pain on muscle activity and coordination during gait: a clinical and experimental study. Pain, 1996 Feb;64(2):231-40
15. Hodges PW, Richardson CA. Inefficient muscular stabilization of the lumbar spine associated with low back pain. A motor control evaluation of transversus abdominis. Spine (Phila Pa 1976). 1996 Nov 15;21(22):2640-50.
16. MacDonald D, Moseley GL, Hodges PW. Why do some patients keep hurting their back? Evidence of ongoing back muscle dysfunction during remission from recurrent back pain. Pain. 2009 Apr;142(3):183-8. doi: 10.1016/j.pain.2008.12.002. Epub 2009 Jan 30.
17. Marshall PW, Murphy BA. Evaluation of functional and neuromuscular changes after exercise rehabilitation for low back pain using a Swiss ball: a pilot study. J Manipulative Physiol Ther. 2006 Sep;29(7):550-60.
18. Hart JM, Fritz JM, Kerrigan DC, Saliba EN, Gansneder BM, Ingersoll CD. Quadriceps Inhibition After Repetitive Lumbar Extension Exercise in Persons With a History of Low Back Pain. J Athl Train. 2006; 41(3): 264–269.
19. Panjabi MM, Brand RA, White AA., Three-dimensional flexibility and stiffness properties of the human thoracic spine..Journal of Biomechanics 1976. 9, 185–192.

20. Oxland TR, Lin RM, Panjabi MM. Three-dimensional mechanical properties of the thoracolumbar junction. J Orthop Res. 1992 Jul;10(4):573-80.
21. Lavaste F, Skalli W, Roy-Camille R, Mazel C, Robin S. 3D Geometrical and mechanical modeling of the human lumbar spine. J. Biomech., 1992,25-10,1153-1164.
22. Dufour M, Pillu M. Biomécanique fonctionnelle Membres-Tête-Tronc. Paris: Elsevier / Masson. 2006. 568p.
23. Dempster WT. 1955. Space Requtrenwnts of the Seated Operator, Wright Air DevelopmentCenter TIA-55-159, Wright-Patterson Air Force Base, Ol'io (AD 87 892).
24. Johansson R, Magnusson M, Akesson M. Identification of human postural dynamics. IEEE Transactions on Biomedical Engineering. 1988;35:858–869
25. Winter DA. Human balance and posture control during standing and walking. Gait and Posture. 1995, 3, 193-214.
26. Runge CF, Shupert CL, Horak FB, Zajac FE. Ankle and hip postural strategies defined by joint torques. Gait Posture. 1999 Oct;10(2):161-70.
27. Duval-Beaupere G,Legaye J. Composante sagittale de la statique rachidienne. Revue du Rhumatisme. 2004, 71(2):105-119
28. Levine D, Whittle MW. The effects of pelvic movement on lumbar lordosis in the standing position. J Orthop Sports Phys Ther. 1996; 24; pp 130-135.
29. Lord MJ, Small JM, Dinsay JM, Watkins RG. Lumbar lordosis. Effects of sitting and standing. Spine. 1997; 22; pp 2571-2574.
30. Keegan JJ. Alterations to the lumbar curve related to posture and seating. J. Bone Jt.Surg. 1953; 35; pp 589-603
31. Black KM, Mc Clure P, Polansky M. The influence of different sitting positions on cervical and lumbar posture. Inclinaison pelvienne. 1996 ; 21; pp 65-70.
32. Nachemson AL, Schultz AB, Berkson MH. Mechanical properties of human lumbar spine motion segments. Influences of age, sex, disc level and degeneration. Spine. 1979; 4; pp 1-8
33. Hedman TP, Fernie GR. In vivo measurement of lumbar spinal creep in two seated postures using magnetic resonance imaging. Spine. 1995 ; 20; pp 178-183
34. Adams MA. The effect of posture on the role of the apophyseal joints in resisting intervertebral compressive forces. J. Bone Jt. Surg.(1980) ; 62B
35. Hedman TP, Fernie GR. Mechanical response of the lumbar spine to seated postural loads. Spine. 1997 ; 22; pp 734-743
36. Pintar FA, Yogananda MM, Myers T, Elhagediab A. Biomechanical properties of human spine ligaments. J. Biomech. 1992; 25; pp 1351-1356
37. Sullivan MS, Dickinson CE, Troup JDG. The influence of age and gender on lumbar spine sagittal plane range of motion, a study of 1126 healthy subjects. Spine. 1994; 19; pp 682-686
38. Adams A, Hutton WC. The effect of posture on the fluid content of the lumbar intervertebral discs. Spine. 1983 ; 8; pp 665-671
39. Roussouly P, Gollogly S, Berthonnaud E, Dimnet J. Classification of the normal variation in the sagittal alignment of the human lumbar spine and pelvis in the standing position. Spine. 2005 Feb 1;30(3):346-5
40. Lafage V, Schwab F, Skalli W, Hawkinson N, Gagey PM, Ondra S, Farcy JP. Standing balance and sagittal plane spinal deformity: analysis of spinopelvic and gravity line parameters. Spine 2008 Jun 15;33(14):1572-8
41. Legaye J, Duval-Beaupere G, Hecquet J, et al. Pelvic incidence: a fundamental pelvic parameter for three-dimensional regulation of spinal sagittal curves. Eur Spine J 1998;7:99-103.
42. Gurfinkel VS. Physical foundations of stabilography. Agressologie. 1973. 14, C, 9-14.

43. Portero F. Evaluation des propriétés mécaniques des muscles cervicaux : analyse du comportement dynamique du segment tete-cou lors de l'application de détentes rapides. [Thèse de doctorat]. [Paris]: Université Pierre et Marie Curie. 2010. 150p.
44. Ettema GJ. Mechanical behaviour of rat skeletal muscle during fatiguing stretchshortening cycles. Experimental physiology 1997 ; 82 (1) : 107-19
45. Sheeran L1, Sparkes V, Caterson B, Busse-Morris M, van Deursen R. Spinal position sense and trunk muscle activity during sitting and standing in nonspecific chronic low back pain: classification analysis. Spine 2012 Apr 15;37(8):E486-95.
46. Marty C. Comment examiner un trouble de la statique rachidienne. Revue du Rhumatisme. 2004, 71, 137-144.
47. Hunter IW, Keamey RE. Respiratory components of human postural sway. Neurosci. Lett. 1981, pp155-159.
48. Hamaoui A, Gonneau E, Le Bozec. Respiratory disturbance to posture varies according to the respiratory mode. Neuroscience Letters. 2010. 475, 141-4.
49. Assaiante C, Amblar, B. An ontogenetic model for the sensorimotor organization of balance control in humans. Human Movement Science. 1995, 14, 13-43.
50. Berthoz A. Physiologie de la perception et de l’action. Annuaire du Collège de France. 2008. p. 453-511.
51. Clément G, Gurfinkel VS, Lestienne F, Lipchits MI, Popov KE. Adaptation of postural control to weightlessness. 1984. Exp Brain Res, 57, 61-72.
52. Gurfinkel VS, Levik YS, Popov KE. Body scheme in the control of postural activity. In: V.S. Gurfinkel, J. Massion & J.P. Roll (Eds.). Stance and motion: facts and concepts. New York: Plenum Press. 1988. pp. 185-193.
53. Massion J. (1997). Cerveau et Motricité. Fonctions sensori-motrices. Paris : Presses Universitaires de France. 1997. 192p.