Perception and Coordination
22
Perception and Coordination Perception-conscious recognition and interpretation (awareness) of the sensory stimuli that serve as a basis for understanding, learning and knowing or for the motivation of a particular action or reaction Coordination-when action or reaction towards a stimulus is occurring in a purposeful, orderly fashion, appropriate response to a stimulus Role of Nervous System: 1. Reciprocally interact with the environment 2. Maintain homeostasis (with the endocrine system) Function: 1. Sensory-interpret incoming message 2. Integrative-analyze, store, make decisions regarding appropriate behavior 3. Motor-initiating muscular or glandular activity; ongoing and evolving interaction with environment Ventricles and CSF Ventricles- four fluid-filled cavities within the brain that connect one another and with the spinal canal CSF- form in the choroids plexus; about 135 cc o Cushions o Provide nutrients o Allow fluid shifts 3 essential components of skull: 1. Brain tissue-78% 2. Blood -12 % 3. CSF-10% Monro-Kellie Hypothesis If volume added to the cranial vault equals the volume displaced from it, the total intracranial volume will not change Normal ICP: 60-150 mmH 2 0 or 0-15 mmHg Normal Compensatory Adaptations: Initial: o Increases CSF absorption o Displacement of CSF into the spinal subarachnoid space—space between arachnoid and pia mater) o Collapse of the cerebral veins and dural sinuses Other mechanisms: o Distensibility of the dura o Increased venous outflow o Decreased CSF production o Constriction and vasodilation o Slight compression of brain tissue Cerebral Blood Flow Amount of blood in milliliters passing through 100g of brain tissue in 1 minute Global CBF-approximately 50 ml/min Brain needs constant supply of oxygen and glucose (20% of body’s oxygen, 25% of body’s glucose) More than 10 minutes of oxygen deprivation-brain death White matter-less perfusion (bundles of fibers, terminal ends) Gray matter-more perfusion (body of neurons) Sources of Blood supply: 1. Internal carotid arteries-anterior circulation, ipsilateral hemispheres 2. Vertebral arteries-posterior circulation, posterior fossa Circle of Willis act as a safety valve; arises from basilar arteries and internal carotid arteries; vascular network at the base of the brain is important to total brain circulation because it provides equal circulation bilaterally. If one side of the circle of Willis is unable to supply adequate blood, the other side provides blood to the area normally supplied by the damaged side (Phipps, 1998, p. 1892) Cerebral arteries (2 each): Anterior, Middle, Posterior Jugular veins-drains the brain venous blood through dural sinuses Special characteristics of Cerebral Perfusion 1. Autoregulation 3 Physiologic mechanisms under normal circumstances: o Changes in intracranial pressure o Cerebral vasodilation o Metabolic factors Mean arterial pressure at which autoregulation is effective (70-105 mmHg) -Upper limit is 150 mmHg MAP SBP 2 (DBP)
Transcript of Perception and Coordination

Perception and CoordinationPerception-conscious recognition and interpretation (awareness) of the sensory stimuli that serve as a basis for understanding, learning and knowing or for the motivation of a particular action or reaction
Coordination-when action or reaction towards a stimulus is occurring in a purposeful, orderly fashion, appropriate response to a stimulus
Role of Nervous System:1. Reciprocally interact with the environment2. Maintain homeostasis (with the endocrine system)
Function:1. Sensory-interpret incoming message2. Integrative-analyze, store, make decisions regarding
appropriate behavior3. Motor-initiating muscular or glandular activity;
ongoing and evolving interaction with environment
Ventricles and CSF Ventricles- four fluid-filled cavities within the brain
that connect one another and with the spinal canal CSF- form in the choroids plexus; about 135 cc
o Cushionso Provide nutrientso Allow fluid shifts
3 essential components of skull:1. Brain tissue-78%2. Blood -12 %3. CSF-10%
Monro-Kellie HypothesisIf volume added to the cranial vault equals the
volume displaced from it, the total intracranial volume will not change
Normal ICP: 60-150 mmH20 or 0-15 mmHg
Normal Compensatory Adaptations:Initial:
o Increases CSF absorptiono Displacement of CSF into the spinal subarachnoid
space—space between arachnoid and pia mater)o Collapse of the cerebral veins and dural sinuses
Other mechanisms:o Distensibility of the durao Increased venous outflowo Decreased CSF productiono Constriction and vasodilationo Slight compression of brain tissue
Cerebral Blood FlowAmount of blood in milliliters passing through 100g of brain tissue in 1 minuteGlobal CBF-approximately 50 ml/minBrain needs constant supply of oxygen and glucose (20% of body’s oxygen, 25% of body’s glucose)
More than 10 minutes of oxygen deprivation-brain death
White matter-less perfusion (bundles of fibers, terminal ends)
Gray matter-more perfusion (body of neurons)
Sources of Blood supply:1. Internal carotid arteries-anterior circulation,
ipsilateral hemispheres2. Vertebral arteries-posterior circulation, posterior
fossa
Circle of Willisact as a safety valve; arises from basilar arteries and internal carotid arteries; vascular network at the base of the brainis important to total brain circulation because it provides equal circulation bilaterally. If one side of the circle of Willis is unable to supply adequate blood, the other side provides blood to the area normally supplied by the damaged side (Phipps, 1998, p. 1892)
Cerebral arteries (2 each):Anterior, Middle, Posterior
Jugular veins-drains the brain venous blood through dural sinuses
Special characteristics of Cerebral Perfusion1. Autoregulation
3 Physiologic mechanisms under normal circumstances:
o Changes in intracranial pressureo Cerebral vasodilationo Metabolic factors
Mean arterial pressure at which autoregulation is effective (70-105 mmHg)
-Upper limit is 150 mmHg
MAP SBP 2 (DBP) 3
SBP-Systolic blood pressureDBP-Diastolic blood pressure
Cerebral perfusion pressure needed to ensure blood flow to the brain
CPPMAP-ICP As CPP decreases, autoregulation fails and CBF
diminishes-30 mmHg is incompatible with life
2. Blood brain barrierphysiologic barrier between blood capillaries and brain tissue
NEUROPHYSIOLOGY
Neurotransmission-conduction of an impulse throughout the nervous system
NeuronsReceive and transmit impulses; non-mitoticExcitable, conductive and can influence other cellsParts: cell body (soma), dendrites (short) and axonMyelinated and unmyelinated
Note:When injured, centrally located neurons are unable to
reproduce themselves because most cell bodies are located centrally and nerve cell bodies cannot reproduce. However, nerve endings can regenerate (Phipps, 1998, p. 1887).

I. Transmission within the Nerve fiberAction potential
Chemical gradientElectrical gradient
Propagation of Action Potential1. Resting stage (positive outside, negative inside)2. Depolarization phase (negative outside, positive inside)
II. Transmission across SynapseSynapses-small gaps between neurons
Chemical or electricalOne-way junction1. Impulses reaches the presynaptic
terminal2. Vesicles release neurotransmitters3. Neurotransmitters inactivated to prevent sustained response
Neurotransmitters-can be excitatory or inhibitory)Types:
1. Acetylcholine-muscle movement2. Biogenic amines (thinking process)
-Dopamine -Serotonin-Norepinephrine -Histamine
3. Amino acids-GABA-Peptides
Neuroglia-protect and nourish neurons; mitotic - do not transmit impulses
Neuroglia FunctionAstrocytes Supply nutrients to neuronsMicroglia Provide protection against
microorganismsOligodendrocytes Wrap tightly around nerve
fibers to form myelin sheathEpendymal cells Ciliated; line brain cavities;
forms CSFSchwann cells Phagocytic cells that form
myelin sheath around nerve fibers
Satellite cells Found in the PNS; may maintain chemical balance of neurons
Cranium and Cerebral columnCranium-composed of 8 cranial and facial bonesForamen magnum-largest hole through which
the brain stem extends to the spinal cordVertebral column-protects the spinal cord,
supports the head and provides flexibility; strengthened by ligaments and fibrocartilage disc
Cranial meningesDura materArachnoidPia mater
Falx cerebri-divides the left from right hemispheres Subdural-more bleeding
Central Nervous system:I. Cerebrum
a. Consists of 2 hemisphereb. Corpus callosum-connects two hemisphere c. Cerebral cortex-outer surface of the cerebrumd. Basal ganglia-located deep within cerebral
hemispheree. Internal capsule-white matter consisting of
bundle of nerve fibers carrying motor and sensory impulses to and from cerebral cortex
Lobes of the Cerebrum and their Functions
Area FunctionsFrontal Controls movements of
voluntary musclePrimary motor area Facilitates voluntary
movement of skeletal muscle
Speech area (Wernick’s )- Located in the
posterior part of the superior temporal convolution
Understanding of spoken and written words
Motor area (Broca’s)- Located in the lateral,
inferior portion of the frontal lobe
Promotes vocalization of words
Temporal Receives and interpret olfactory and auditory
stimuliParietal Promotes recognition of
pain, coldness, light touch (Contralateral reception)
Occipital Receives and interprets visual stimuli
II. DiencephalonEmbedded in the brain superior to brain stemThalamus-process sensory impulses before it
reaches cerebral cortexHypothalamus-regulates endocrine and autonomic function, temperature, water metabolism, appetite, emotion, sleep-wake cycle and thirstEpithalamus-includes pineal gland (secretes melatonin and inhibits LH), part of endocrine system, affects growth and development.
III. Brain StemMidbrain-center for auditory and visual reflexesPons-contains the fiber tracts; contains nuclei
that controls respiration-contains pneumotaxic center—controls rhythmic quality of respirations
Medulla-control cardiac rate, BP, respirators and swallowing
Reticular activating system (RAS)-influence excitatory and inhibitory control of motor neuron; regulatory system for consciousness

IV. CerebellumHas two hemispheresCoordination of skeletal muscle activity,
maintenance of balance, posture and control of voluntary movements
V. Spinal cordExtends from medulla up to first lumbar vertebraGives rise to 31 pairs of spiral nerves (C1-C8, T1-T12, L1-L5, S1-S5, coccygeal nerve)Center for conducting messages to and from the brain; a reflex center
Divisions:
Ascending (Spinocerebellar)Carry a specific sensory information to higher levels of CNSSpinocerebellar tracts-muscle tension and body positionSpinothalamic-pain and temperature sensation
Descending (Corticospinal)Pyramidal tracts-from the cortex to cranial and peripheral nerves; inhibits muscle toneExtrapyramidal tracts-from brain stem, basal ganglia, and cerebellum; maintains muscle tone and gross body movementsUpper motor neurons-from cerebral cortex to anterior gray column of SC; spasticity and hyperactive reflexesLower motor neurons-“final common pathways” from anterior gray column up to muscles; flaccidity and loss of reflexes
VI. Reflex arcReflexes-automatic action; spinal cord mediates most reflexesAutomatic or perceptible, inhibited or conditioned
Hyperreflexia-disease or injury of certain descending motor tracts
Hyporeflexia-damage or degeneration of the sensory or motor neurons
Peripheral Nervous systemCranial nerves-innervate head and neck
region, except the vagus nerveSpinal nerves
Plexuses-complex cluster of nerve fibers (cervical, brachial, lumbar and sacral region)Dermatomes-area of the skin innervated by cutaneous branches of a single spinal nerve
Somatic Nervous systemConsists of motor and sensory nervesControls skeletal musclesProduces a motor response through
efficient nerve fibers from CNS which transmit impulses to the skin and skeletal muscles
Autonomic Nervous SystemControls involuntary or automatic body functions
Has two subdivisions, serving same organ but have counterbalancing effects; each system can inhibit the organ stimulated by the other
Sympathetic Nervous System originates from lateral horns of first
thoracic through the first lumbar of spinal cord (thoracolumbar)
helps the body cope with events in the external environment
Functions mainly during stress, triggering the fight or flight response
Increases heart rate and respiratory rate, pupil dilation, cold, and sweaty palms
Parasympathetic Nervous System Consist of the vagus nerves originating in
the medulla of the brain stem and spinal nerves originating from the sacral region of the spinal cord (craniosacral)
Activates GI system Supports restorative, resting body
function through such actions as replenishing fluids and electrolytes
Effect organ Sympathetic ParasympatheticHeart Increased rate
and contractilityDecreased rate and contractility
Lungs Relaxation ContractionGIT
Motility Tone
sphincters
Decreased Contraction
Increased Relaxation
Urinary bladderBladder
muscle Sphincter
Relaxation
Contraction
Contraction
Relaxation
Liver Glycogenolysis None
Sensory System (General and special)
Type of receptors:1. Exteroreceptors2. Interoreceptors3. Proprioceptors-specific receptors to detect balance,
sense of position4. Mechanoceptors-detect pressure, touch (any
stimulus that is physical in nature)5. Thermoreceptors-any changes in temperature6. Photoreceptors-light stimulus7. Chemoreceptors-taste, olfactory, pancreatic enzymes8. Nociceptors-severe stimulus9. Cutaneous receptors-touch
Special senses:Sense of Sight
Collect light waves and transmit them as impulses to the brain, which translate them into imagesNormally form of a clear retinal image of an object at 20 ft. awayBinocular vision—ability to judge relative, distances of objects
Anatomical features of the EyeballOuter:
1. Cornea-thin, tough, transparent layer supplied with sensory nerve (touch and pain), no blood supply, oxygen and glucose through diffusion
2. Sclera
Middle:1. Choroid –highly vascular, dark brown membrane
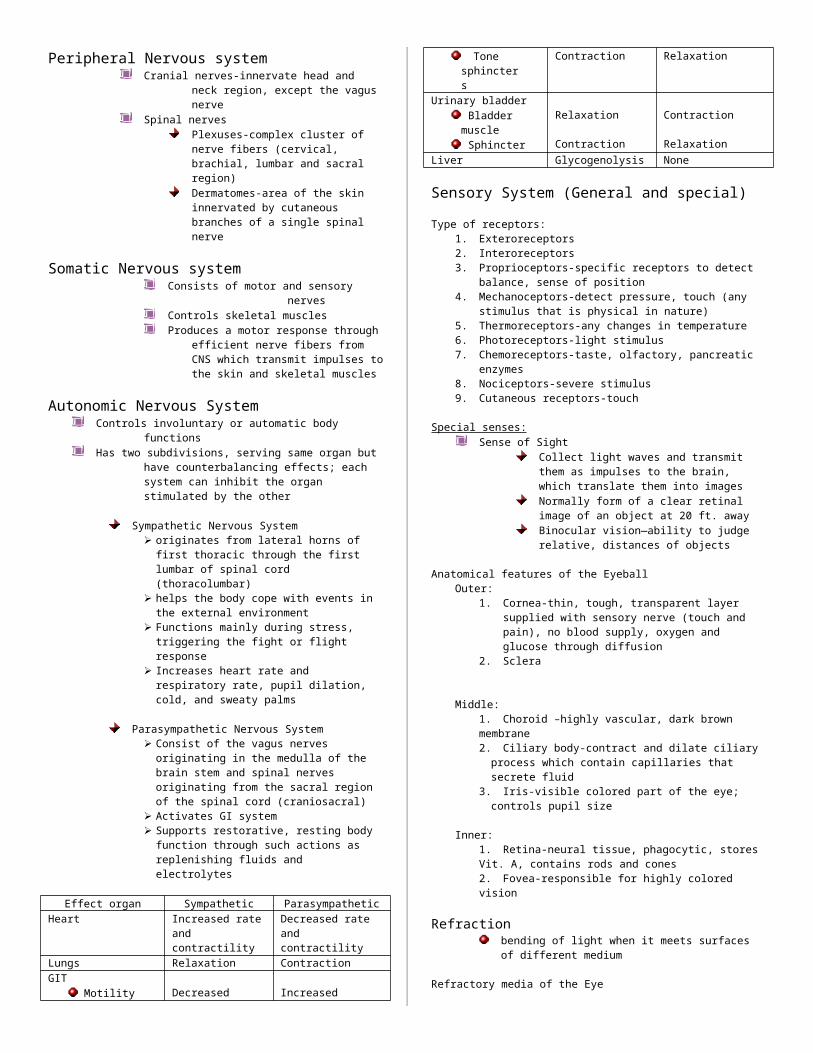
2. Ciliary body-contract and dilate ciliary process which contain capillaries that secrete fluid
3. Iris-visible colored part of the eye; controls pupil size
Inner:1. Retina-neural tissue, phagocytic, stores Vit. A, contains rods and cones2. Fovea-responsible for highly colored vision
Refractionbending of light when it meets surfaces of different medium
Refractory media of the Eye1. Cornea-performs most of the refraction because of
its convex form2. Aqueous humor-fluid at the anterior and posterior
chamber of the anterior cavity3. Crystalline lens-greatest refractive power4. Vitrous humor- thick, gelatinous fluid found at
posterior chamber, give spherical shape to the eye
Physiology of VisionFormation of an image on the retina accomplished by the
following:1. Refraction2. Accomodation3. Constriction of pupils4. Convergence of eyeballs
Stimulation of retinaDim light causes breakdown of the chemical
rhodopsin present in rodsCones-responsible for daylight and color visionPerception of color is dependent on the conesMost cones concentrated on fovea centralisCondition to central area in occipital lobe
Sense of HearingParts of the ear
1. Outer-collects sound2. Inner-conducts sound
Eustachian tube joins the middle ear and nasopharynx transmit sound waves and maintain
equilibrium
Interpretation of sound Loudness- Neurologic or psychologic
interpretation of intensity; the greater intensity of the sound waves stimulating the organ of Corti, the greater will be the size of nerve impulses
Decibels(dB)-unit of measure of intensity of soundNormal conversation= 65 dBAmplified rock music= 120 dBNearby jetplane= about 140 dB
PitchCorresponds to frequency; the higher the frequency the higher the pitch of the soundHumans can potentially hear sounds whose frequency range from 16 to 2000 HzUpper range decreases slight with increasing ageSpeech falls in the range of 85-1050 Hz
Physiology of Hearing1. Sound waves moving through the air enter the canal
and move down to it to strike against the tympanic membrane causing it to vibrate
2. Vibrations of the tympanic membrane move the malleus
3. Movement of the malleus to the incus4. As the incus moves, it moves the stapes against the
oval window, it starts a ripple on the perilymph5. Movement of the perilymph is transmitted to the
endolymph muscle inside the cochlear duct and stimulates the organ of Corti
6. Cochlear nerve conduct impulses from the organ of Corti to the brain; hearing occurs when impulses reaches auditory area in the temporal lobe of cerebral cortex
Mental Status Examination An indication of how patient is functioning as a whole
and how the patient is adapting to the environment
1. General appearance2. State of consciousness
Arousal component Content component
3. Mood and effect-changes in the nervous system4. Thought content5. Intellectual capacity
NEUROLOGIC ASSESSMENTI. Comprehensive History Taking
Demographic DataCurrent healthPast health historyMedication historyGrowth and developmentFamily health historyPsychosocial history
II. V/SIII. Mental Status Assessment
LOCOrientationMemoryMood/affectIntellectual performanceJudgment/InsightLanguage/communication
IV. Motor System assessment-muscle strength, tone, coordination, gait and station movement
V. Sensory Function-superficial sensation, touch/pain, temperature, proprioception, discrimination
VI. Reflex activityVII. Cranial nerve testing
MENTAL STATUS ASSESSMENT WITH ABNORMAL FINDINGS
Unilateral neglect (lack of caring of the other side of the body); strokes involving middle cerebral artery.
Poor hygiene and grooming: dementing disordersAbnormal gait and posture: transient ischemic attacks(TIAs) , strokes, and Parkinson’s diseaseEmotional swings, personality changes: strokesAphasia-defective or absent language function: TIA’s, strokes involving anterior/posterior artery; general term for impairment of languageDysphonia- change in tone of voiceDysarthria- (different in speaking); is indistinctness of words in word articulation resulting from interference with the peripheral speech mechanisms (e.g. muscles of the tongue, palate, pharynx, or lips) [Phipps, 1998, p. 1901]

Decreased level of consciousnessConfusion, Coma
COGNITIVE FUNCTION ASSESSMENT WITH ABNORMAL FINDINGS
Disorientation to time and place: stroke of right cerebral hemisphere
1. Memory deficits2. Emotional defense
CRANIAL NERVE ASSESSMENTSCranial I (Olfactory): Anosmia
1. lesions of frontal lobes2. impaired blood flow to middle cerebral
artery.
Cranial II (Optic)1. blindness in eye: strokes of internal carotid
artery, TIA’s2. Homonymous hemianopia - impaired vision
or blindness in one side of both eyes; blockage of posterior cerebral artery.
3. Impaired vision: strokes of anterior cerebral artery; brain tumors
Note:Visual acquity-mediated by the cones of the retinaField of vision or peripheral vision-portion of space in which objects are visible during the fixation of vision in one direction. The receptors for peripheral fields are the rod neurons of the retina. (Phipps, 1998, p. 1906)
Cranial nerve III, IV, VI (Oculomotor, Trochlear, Abducens)-motor nerves that arise from the brainstem
1. Nystagmus –- involuntary eye movement; strokes of anterior, inferior, superior, cerebellar arteries
2. Constricted pupils: may signify impaired blood flow to vertebralbasilar arteries.
3. Ptosis (eyelid falldown); dropping of the upper eyelid over the globe—strokes of posterior inferior cerebellar artery; myasthenia gravis, palsy of CN III
Cranial nerve V (Trigeminal)—largest cranial nerve with motor and sensory components: changes in facial sensations; impaired blood flow to carotid artery
1. Decreased sensation of face and cornea on same side of body; strokes of posterior inferior cerebral artery
2. Lip and mouth numbness3. Loss of facial sensation: contraction of masseter and
temporal muscles, lesions CN V4. Severe facial pain: trigeminal neuralgia (tic
dorlourex)
Cranial VII (Facial nerve)—mixed nerve concerned with facial movement and sensation of taste
1. Loss of ability to taste2. Decreased movement of facial muscles3. Inability to close eyes, flat nasolabial fold, paralysis
of lower face, inability to wrinkle the forehead 4. Eyelid weakness; paralysis of lower face; paralysis of
upper motor neuron5. Pain, paralysis, sagging of facial muscles: affected
side in Bell’s palsy
Cranial VIII (Acoustic)—composed of a cochlear division related to hearing and a vestibular division
related to equilibrium (Phipps, 1998, p. 1909)
Decreased hearing or deafness: strokes of vertebralbasilar arteries or tumors of CN VIII
Cranial IX(Glossopharyngeal) and cranial X (Vagus)—chief function of cranial nerve IX is sensory to the pharynx and taste to the posterior third of tongue; cranial nerve X is the chief motor nerve to the soft palatal, pharyngeal and laryngeal muscles (Phipps, 1998, p. 1909)
1. Dysphagia (difficulty swallowing)2. Unilateral loss of gag reflex
Cranial XI (Spinal accessory)—motor nerve that supplies the sternocleidomastoid muscle and upper part of trapezius muscles
1. Muscle weakness2. Cortralateral hemiparesis: strokes affecting middle
cerebral artery and internal arteryCranial XII (Hypoglossal)1. Atrophy, fasciculations (twitches): LMN disease2. Tongue deviation toward involved side of the body
SENSORY FUNCTION ASSESSMENT WITH ABNORMAL FINDINGS
Altered sensation occurs with variety of neurologic pathology
Altered sense of position: lesions of posterior column of spinal cord
Inability to discriminate fine touch: injury to posterior columns
MOTOR FUNCTION ASSESSMENT WITH ABNORMAL FINDINGS
Muscle atrophy: LMNs diseaseTremors (groups, large of muscle fibers)-
Parkinson’s disease (tremors at rest), multiple sclerosis (tremors observed in activity)
Fasciculations (single muscle fiber): disease or trauma to LMN, side effects of medications, fever, sodium deficiency, anemia
Flaccidity (decreased muscle tone): disease or trauma to LMN and early stroke
Spasticity (increased muscle tone): disease of corticospinal motor tract
Muscle rigidity: disease of EP motor tractCogwheel rigidity (muscular movement with small
regular jerky movement; parkinson’s disease
Muscle weakness-in arms, legs, hands: TIAsHemiplegia-paralysis of half of body verticallyFlaccid paralysis: strokes of anterior spinal artery,
multiple sclerosis or myasthenia gravisTotal loss of motor function: below level of injurySpasticity of muscle: incomplete cord injuries
CEREBELLAR FUNCTION ASSESSMENT WITH ABNORMAL FINDINGS
Ataxia (lack of coordination and clumsiness of movement, staggering, wide-based and unbalanced gait)
Steppage gait (client drags or lifts foot high, then slaps foot onto floor; inability to walk on heels; disease of LMN
Sensory ataxia (client walks on heels before bringing down toes and feet are held wide apart; gait worsens with eyes closed

Parkinsonian gait (stooped over position while walking with shuffling gait with arms held close to the side)
Romberg’s test (Positive)- With feet approximated, the patient stands with eyes open and then closed; if closing the eyes increases the unsteadiness, a loss of proprioceptive control is indicated
REFLEXHyperactive: reflexesDecreased reflexesClonus of foot (Hyperactive, rhythmic dorsiflexion
and plantar flexion of foot)Superficial reflexes (such as abdominal) and
cremasteric reflex Positive Babinski reflex (dorsiflexion of big toe)
Special Neurologic Assessment
Brudzinski’s sign (pain, resistance, flexion of hips and knees when head flexed to chest with client supine)
Positive Kernig’s sign-excessive pain when examiner attempts to straighten knees with client supine and knees and hips flexed
Decorticate posturing (up)
Decerebrate posturing (down)
#Altered Level of consciousness1. Consciousness
Requires:1. Arousal: alertness; dependent upon reticular
activating system (RAS); system of neurons in thalamus and upper brain stem
2. Cognition: complex process, involving all mental activities; controlled by cerebral hemispheres
Process that affect LOC:a. Increased ICPb. Stroke, hematoma, intracranial hemorrhagec. Tumorsd. Infectionse. Demyelinating disorders
Systemic Conditions affecting LOC Hypoglycemia F/E imbalance Accumulated waste products from liver or
renal failure Drugs affecting CNS: alcohol, analgesics,
anesthetics Seizure activity: exhausts energy
metabolites Level of Consciousness
AlertLethargic-very sleepyObtundedStuporousComa Death
Client Assessment with Decreased LOCa. Increased stimulation required to elicit response from
clientb. More difficult to arouse; client agitated and confused
when awakenedc. Orientation changes: losses orientation to time first,
then place, persond. Continuous stimulation required to maintain
wakefulnesse. Client has no response, even to painful stimulation
Loss of Simultaneous Eye MovementLoss of normal reflex functioning:1. Doll’s eye movement: eye movement in opposite
direction of head rotation (normal function of brain stem)
2. Oculocephalic reflex: eye move upward with passive flexion of neck; downward with passive neck extension (normal function)
3. Oculovestibular response (cold caloric testing): instillation of cold water in ear canal cause nystagmus (lateral tonic deviation of eyes) toward stimulus (normal function)
GLASGOW RESPONSEEye opening responses
4 Opens eyes spontaneously3 Opens eyes in
response to voice 2 Opens eye in response to painful stimuli 1 Does not open eyes
Best verbal response5 Oriented4 Confused3 Utters inappropriate words
2 Incomprehensible words1 None

Best motor response6 Obeys command
5 Localizes pain4 Withdraws with painful stimuli
3 Flexion (Decorticate posturing)2 Extension (Decerebrate posturing1 None
Total 3-1514 – no impairment3 – compatible with brain death7 – state of coma
MOTOR FUNCTION ASSESSMENTa. Client follows verbal commandsb. Pushes away purposely from noxious stimulic. Movements are more generalized and less purposeful
(withdrawal, grimacing)d. Reflexive motor responsese. Flaccid with little or no motor response
COMAIrreversible coma - vegetative state
Permanent condition of complete unawareness of self and environment, death of cerebral hemispheres with continued function of brain stem and cerebellum
Client does not respond meaningfully to environment but has sleep-wake cycles and retains ability to chew, swallow and cough
Eyes may wander but cannot track objectsMinimally conscious state: client aware of
environment, can follow simple commands, indicates yes/no responses; make meaningful movements (blink, smile)
Often results from severe head injury or global anoxia
Locked-in syndrome1. Client is alert and fully aware of environment; intact
cognitive abilities but unable to communicate through speech or movement because of blocked efferent pathways from brain
2. Motor paralysis but cranial nerves may be intact allowing client to communicate through eye movement and blinking
3. Occurs with hemorrhage or infarction of pons, disorders of lower motor neurons or muscles
Brain Death1. Cessation and irreversibility of all brain functions2. General criteria:
a. Absent motor and reflex movementsb. Apneac. Fixed and dilated pupilsd. No ocular responses to head turning and caloric stimulatione. Flat EEG
NURSING DIAGNOSISIneffective airway clearance: limit suctioning to <10-15 seconds, hyperoxygenateRisk for aspirationRisk for impaired skin integrity: preventive measures, continual inspectionImpaired physical mobility: maintain functionality of joints, physical therapyRisk for Imbalanced Nutrition: Less than body requirementsAnxiety (of family)
ICP Increased blood volume, increased brain volume,
increased CSF volume Normal pressure: 5-15 mmHg, with pressure
tranducer with head elevated 30˚; 60-180 cmH20, water manometer with client lateral recumbent
Sustained increases associated with:a. Cerebral edemab. Head traumac. Tumorsd. Abscessese. Strokef. Inflammationg. Hemorrhage
Factors that Increases ICPHypercapnea, hypoxemiaCerebral vasodilating agentsValsalva maneuver; coughing or sneezingBody positioning (prone, neck flexion,
extreme hip flexion)Isometric muscle contractionEmotional upset; noxious stimuliArousal from sleepClustering of activitiesPain and agitation
ICP
Cranial insult Tissue edema Increased ICP Compression of blood vessels
Decreased cerebral blood flow
Decreased oxygen with brain cell death
Edema around necrotic tissue
Increased ICP with brainstem and respiratory center compression
Carbon dioxide accumulation
Vasodilation Increased ICP DEATH
Pathophysiology: pressure results to lack of oxygen and blood supply
Manifestations:Decreasing level of sensorium-most sensitive,
reliable and earliest indicator: due to cerebral hypoxia, interference with RAS function
Increasing BP, decreasing pulsePupillary changes (a reflection of tissue shiftsCushing’s triad-increasing systolic pressure,
widening pulse pressure and bradycardia (final compensatory mechanism to maintain CSF)
Papilledema-due to the compression of optic discRespiratory changes-dependent on site of
pressureMotor changes-dependent on site of pressure;
usually starts contralaterally; then hemiplegia, decortication or decerebation depending on pressure on brain stem

Late signs: coma, apnea, unilateral pupil changes
Medications for Increased ICP Osmotic diuretics increases osmolarity of blood and
draw fluid from edematous brain and tissue into vascular bed
Loop diuretics such as furosemide Antipyretics or hypothermia blanket: used to control
increases in cerebral metabolic rate Anticonvulsants to manage seizure activity Histamine H2 receptors to decrease risk of stress
ulcers Barbiturates: may be given as continuous infusion to
induce coma and decrease metabolic demands of injured brain
Vasoactive medicine may be given to maintain blood pressure to cerebral perfusion
Surgery-include removal of brain tumors, burr holes, insertion of drainage catheter or shunt to drain excessive CSF
ICP monitoring Continuous intracranial pressure monitor is used for
continual assessment of ICP and to monitor effects of medical therapy and nursing interventions
Risk of infection exists with invasive procedure
Nursing Diagnosis1. Ineffective Tissue perfusion2. Risk for infection: open head wounds and intracranial
monitor device requires meticulous aseptic technique3. Anxiety (family)
Client with Seizure DisorderSeizures-alteration in consciousness, sensory and motor
Paroxysmal motor, sensory, or cognitive manifestations of spontaneous abnormal discharges from neurons in cerebral cortex May involve all or part of brain consciousness, autonomic function, motor function and sensation
Epilepsy: any disorder characterized by recurrent seizures
Categorization of seizures:Partial seizures: activation of part of one cerebral
hemispherea. Simple partial seizure: no altered consciousness, recurrent muscle contraction; motor portion of cortex affected
b. Complex partial seizure: impaired consciousness; may engage in automatisms (repetitive nonpurposeful activity such as lip smacking, preceded by aura, originates in the temporal lobe)
Generalized seizures: Involves both brain hemispheres;
consciousness always impaired Absence seizures (petit mal): characterized
by sudden brief cessation of all motor activity, blank stare and unresponsiveness often with eyes fluttering
Tonic-clonic seizures Preceded by aura, sudden loss of
consciousness Tonic phase: rigid muscles, incontinence (as
muscle contracts, bladder relax) Clonic phase: altered contraction,
relaxation, eyes roll back, froths at mouth
Post-ictal phase: unconscious and unresponsive to stimuli
State Epilepticus1. Continuous seizure activity, generally tonic-clonic type2. Client at risk to develop hypoxia, acidosis,
hypoglycemia, hyperthermia, exhaustion3. Life threatening medical emergency requiring
immediate treatment:a. Establish and maintain airwayb. Diazepam (Valium) and Lorazepam (Ativan)
intravenously at c. 50% Dextrose IVd. Phenytoin (Dilantin) IV-increase seizure thresholde. Pentobarbital-lessen nervous irritation
Medications:a. Manage but do not cure seizuresb. Raise seizure thresholdc. Carbamezepined. Phentoine. Valproic acid
Key Interventions:1. Proper client from injury and maintaining airway2. Do not force anything into the client’s mouth3. Loosen clothing around neck
Nursing Diagnosis:1. Risk for Ineffective airway clearance 2. Anxiety
Interventions:1. Assess for signs and symptoms of seizure activity such
as report of aura or twitching of muscle groups2. Have an oral airway oxygen and suction readily
available3. Stay with client to protect him from injury and observe
seizure activity. If he is in bed, remove pillows, raise side rails, put bed on flat position. Loosen any restrictive clothing
4. After seizure, assess respiration and pulse. If they present and he is unresponsive turn him onto his side to keep his airway patent
5. Cover him with a blanket for warmth and privacy6. Observe and document characteristics of the seizure
Client with Headache1. May be due to benign or pathological condition
Pathophysiology: multiple pain sensitive structures within cranial vault, face, and scalp are stimulated and cause pain perception
Types: Tension-characterized by sensation of tightness around head and may have specific localized painful areas; areas caused by sustained contraction of muscles and head and neck; precipitated by stress and anxiety
Migraine (more common in women)- recurring vascular headache often initiated
by triggering event and accompanied by neurologic dysfunction; or increase release of sensory substances (e.g. serotonin); triggers include stress, fluctuating glucose levels, fatigue, hormones, bright lights
Cluster (common in men)- typically awakens client with unilateral pain
around eye accompanied by rhinorrhea, lacrimation, flushing; attacks occur in clusters of 1-8 days for weeks
HEADACHE

1. Tension headache-90% ; noise, stress—sustained contraction of muscles
2. Sinus HeadacheVirus, allergen, bacteria, temp
Nerves in sinuses swell
Headache
e.g. brain freeze due to swallowing of cold substances rapidly
3. Hang-over headacheAlcohol blocks hormonal mechanisms
Dehydration
4. Wine headacheIncreases histamine/tyramine
Dilate blood vessels
Pressure on nerves
5. Migraine headache: 1:4 household Women 3x more than men: 3days a week May be caused by:
LightNoiseIrregular eating and sleepChocolateStrong smellPeanut butter
Electrical impulse altered and triggers trigeminal nerve
Trigeminal nerve=vasodilation and nerve irritation
6. Cluster Headache Excruciating pain 6 x more in men, 30 min to 2 hours
Nerves irritated
Pain signals
Tension Headache
Management:Pharmacological1. Aspirin, Ibuprofen-suppress prostaglandin that dilates
and sensitize nerve fibers2. Acetaminophen-tension headache; works in CNS to
reduce pain without effect on prostaglandin (safe for gastritis)
3. Triptans-anti-migraine; activates serotonin receptors decreasing inflammation of blood vessels
4. Botox (purified botulinum bacteria)- small dosages allow it to be localized;
paralyses muscles locally and is not absorbed into the blood stream (may cause nerve paralysis if given in large doses)
5. Indomethacin-for cluster headaches; with pain killers
Nonpharmacological:1. Biofeedback2. Acupuncture3. Massage4. Yoga5. Herbal remedies
HEAD INJURY
Laceration Hematoma Contussion Bleeding
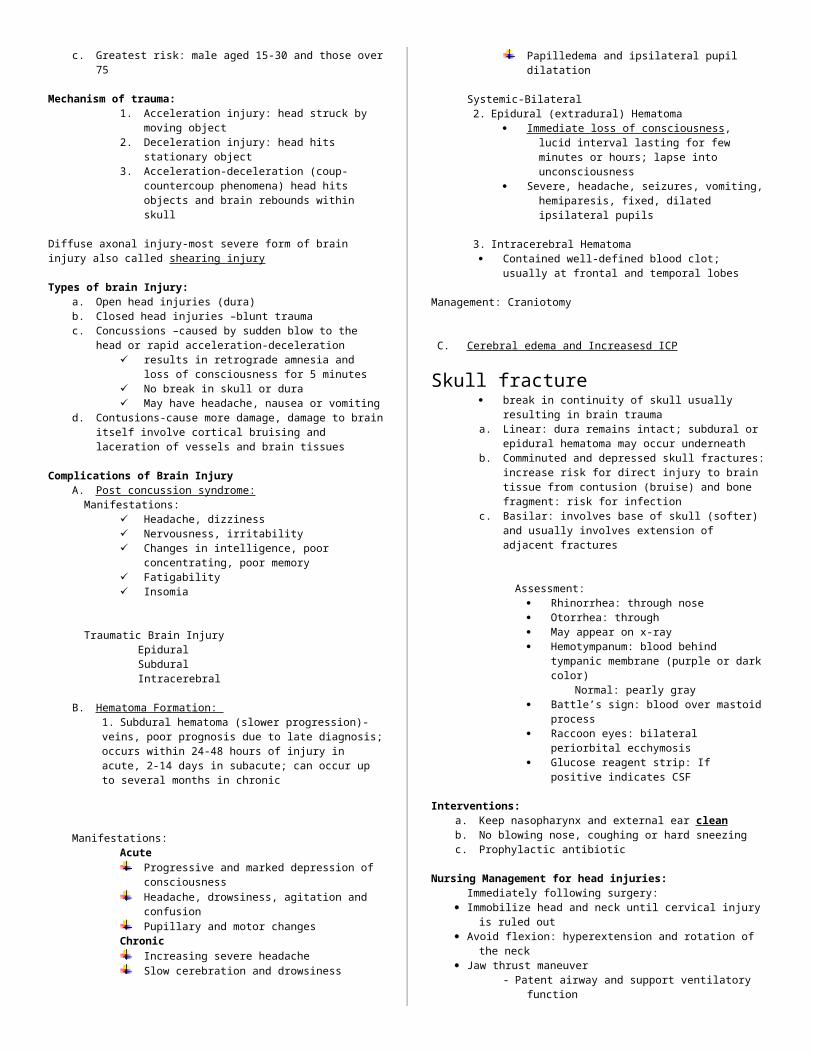
Sources:1. Scalp injury2. Skull fracture3. Brain injury
Risk factors:a. Motor vehicle accidentsb. Elevated blood alcohol levelsc. Greatest risk: male aged 15-30 and those over 75
Mechanism of trauma:1. Acceleration injury: head struck by moving
object2. Deceleration injury: head hits stationary
object3. Acceleration-deceleration (coup-
countercoup phenomena) head hits objects and brain rebounds within skull
Diffuse axonal injury-most severe form of brain injury also called shearing injury
Types of brain Injury:a. Open head injuries (dura)b. Closed head injuries –blunt traumac. Concussions –caused by sudden blow to the head or
rapid acceleration-deceleration results in retrograde amnesia and loss of
consciousness for 5 minutes No break in skull or dura May have headache, nausea or vomiting
d. Contusions-cause more damage, damage to brain itself involve cortical bruising and laceration of vessels and brain tissues
Complications of Brain InjuryA. Post concussion syndrome:
Manifestations: Headache, dizziness Nervousness, irritability Changes in intelligence, poor concentrating,
poor memory Fatigability Insomia
Traumatic Brain InjuryEpiduralSubduralIntracerebral
B. Hematoma Formation: 1. Subdural hematoma (slower progression)-veins, poor prognosis due to late diagnosis; occurs within 24-48 hours of injury in acute, 2-14 days in subacute; can occur up to several months in chronic
Manifestations:Acute
Progressive and marked depression of consciousnessHeadache, drowsiness, agitation and confusionPupillary and motor changes
ChronicIncreasing severe headacheSlow cerebration and drowsinessPapilledema and ipsilateral pupil dilatation
Systemic-Bilateral

2. Epidural (extradural) Hematoma Immediate loss of consciousness , lucid
interval lasting for few minutes or hours; lapse into unconsciousness
Severe, headache, seizures, vomiting, hemiparesis, fixed, dilated ipsilateral pupils
3. Intracerebral Hematoma Contained well-defined blood clot; usually at
frontal and temporal lobes
Management: Craniotomy
C. Cerebral edema and Increasesd ICP
Skull fracture break in continuity of skull usually resulting in
brain traumaa. Linear: dura remains intact; subdural or epidural
hematoma may occur underneathb. Comminuted and depressed skull fractures:
increase risk for direct injury to brain tissue from contusion (bruise) and bone fragment: risk for infection
c. Basilar: involves base of skull (softer) and usually involves extension of adjacent fractures
Assessment: Rhinorrhea: through nose Otorrhea: through May appear on x-ray Hemotympanum: blood behind
tympanic membrane (purple or dark color)
Normal: pearly gray Battle’s sign: blood over mastoid
process Raccoon eyes: bilateral periorbital
ecchymosis Glucose reagent strip: If positive
indicates CSF
Interventions:a. Keep nasopharynx and external ear cleanb. No blowing nose, coughing or hard sneezingc. Prophylactic antibiotic
Nursing Management for head injuries:Immediately following surgery:
Immobilize head and neck until cervical injury is ruled out
Avoid flexion: hyperextension and rotation of the neck Jaw thrust maneuver
- Patent airway and support ventilatory function- Document baseline neurological assessment
After initial stabilization: Monitor neurological status every hour until stable
- LOC, responsiveness- Pupillary size, position, direct and consensual
response- Assess extraocular movements- Note verbal and motor changes
Monitor for complications- Hematoma formation- Infection- Acute hydrocephalus- ARDS
Monitor temperature and maintain normothermia (decrease metabolism)
Report high urine output (over 200 ml/hr for 2 consecutive hours)
Monitor osmolality and serum electrolytes CBC ROM exercises Eye/ear care Nutrition-NGT (high glucose-brain functioning; protein-
tissue repair) Elimination-laxatives, increase fiber
Craniotomy-surgical opening of the skullCraniectomy –permanent removal of the cranium to relieve pressure on the brain by providing space for expansion
Nursing managementPreoperative
Parenteral corticosteroids Scalp preparation Antiembolism stockings
Postoperative1. Neurological assessment2.Head dressings:monitor for CSF leaks3.Control ICP
Assess for signs of increasing ICP Positioning to prevent increase in ICP
Supratentorial surgery-elevate head of bed 30 degrees
Infratentorial-keep flat, turn every 2 hours, but never onto the back (to prevent brain hernation)
Posterior fossa surgery-either side but never on the back
Bone flap-on the unoperated side
STROKEStroke is a brain attack
…needing emergency management, including specific treatment and secondary and tertiary prevention
Stroke is an emergency…where virtually no allowances for worsening
are toleratedStroke is treatable
…optimally, through proven, affordable, culturally-acceptable and ethical means
Stroke is preventable…in implementable ways across all levels of
society
Basic Location of Cerebral Aneurysm
Cerebral embolus-movingCerebral thrombusCerebral hemorrhage
Types of strokes
Ischemic stroke-little blood flow1. Thrombotic formation of a blood clot with
coagulation the results in the narrowing of the lumen of a blood vessel with eventual occlusion
2. Embolic –occlusion of a cerebral artery by an embolus, resulting in necrosis and edema of the area supplied by the involved vessel
Hemorrhagic stroke-disrupted blood flow1. Intracerebral hemorrhage stroke-bleeding within the
brain caused by a rupture of vessels2. Subarachnoid hemorrhagic stroke-cause by
aneurysm or AV malformation
Development of CVA

1. Transient Ischemic attack-brief episodes of neurologic manifestations which clear completely in less than 24 hours
2. Reversible ischemic neurologic deficit-neurologic deficits remain after 24 hours but leaves no residual signs and symptoms after days to weeks
3. Stroke in-evolution-progressing stroke which develops over a period of hours or days; manifestations don’t resolve and leave residual neurologic effects
4. Completed stroke- when neurologic deficits remain unchanged over 2-3 day period
Risk Factors Prior ischemic episodesCardiac diseaseDMAtherosclerotic diseasaeHypertension, hypercholesterolemiaPolycythemiaSmokingOral contraceptivesEmotional stressObesity Family history of strokeAge
Warning signs that may precede CVAParesthesiaTransient loss of speechHemiplegiaSevere occipital or nuchal headachesVertigo or syncopeMotor or sensory disturbances (tingling transient
paralysis)Epistaxis
SPECIFIC DEFICITS
Dependent upon area damagedHemiplegiaAphasia- sensory/receptive-Wernick’s aphasia- motor/expressive-Broca’s aphasia (able to
understand the stimuli but cannot expressGlobal aphasia- Agnosia- Dysarthria- Incontinence- Horner’s syndrome-decrease lacrimation- Unilateral neglect
Emotional or Behavioral Reactions:Severe mood swingsSocial withdrawalInappropriate sexual behaviorOutbursts of frustration and/or angerRegression to an earlier behavior
Right brain damage Left brain damageParalyzed left sideSpatial-perceptual
deficitsTend to deny or
minimize problemsImpaired judgmentImpaired time
conceptsShort term span
Paralyzed right sideImpaired
speech/languageImpaired right and left
discriminationAware of deficits,
depression, anxietyImpaired
comprehensionSlow performance,
cautious
Middle cerebral artery InvolvementContralateral paralysisContralateral anesthesia, loss of proprioception,
fine touch, localizationAphasiaNeglect of opposite sideHomonymous hemianopia-loss of vision for one
half of the visual field
Diagnostic procedures CT scan-determine if vascular or nonvascular lesions Angiography MRI Laboratory (CBC, PT, PTT)-not definitive to conform
diagnosis
Medical management Decreased ICP BP management Fluid volume management Tissue plasminogen activator-must be given within 3
hours of onset of manifestations and will dissolve clot; recombinant altephase (Activase rt-pa)
Antithrombotic (aspirin, clipyridamole)-prevent platelet aggregation
Anticoagulant (heparin, clexane) Steroids or osmotic, diuretics Antihypertensive and diuretics
Nursing management Hourly neurological assessment Monitor and prevent intracranial hypertension
Positioning- bed rest: keep mainly on unaffected side- use of pillows to support to prevent flexion
deformity, thrombus formation- external hip rotation- assist in progressive activity (mobility)- Progressive self-care (ADL)
Prevention of injury- eyes-normal saline, artificial tears, eye
patch- side rails up- decubitus ulcer prevention/management- Oral mucosa care
Nutrition/prevention of aspiration- Communication- Others:
Reorientation Minimize environmental stimuli Emotional support Rehabilitative
Discharge care- Ways to prevent recurrence
dietary modification Stress reduction Smoking cessation Exercise program Drug compliance
- Residual deficits and balancing realistic expectation
- Special methods of feeding- Ensure continuity of care and emotional
support
SPINAL CORD INJURY
Manifestations:Subjective
Loss of sensation below level of injuryInability to moveObjectivity
A. Early symptoms of spinal shockAbsence of reflexes below level of lesionFlaccid paralysis below level of injury
Hypotonia results in bowel and bladder distentionInability to perspire in affected partsHypotension
B. Later symptoms of spinal cord injuryReflex hyperexcitabilityState of diminished reflex hyperexcitability
below site in all instances of cord damage following hyperreflexia
In total cord damage-loss of motor and sensory function is permanent
Sacral region-atonic bladder and bowel with impairment of sphincter control
Lumbar region- spastic bladder and loss of bladder and anal sphincter control
Thoracic-trunk below the diaphragmCervical-from neck down, if above C4
respirations and depressedIn partial cord damage, depends on the type of
neurons affected (spastic vs. flaccid)
Clinical manifestations:Paralysis of muscles of respirationBradycardiaHypotensionUrinary retentionHypomotility Muscle atrophyPoikilothermia-abnormality in sensing change in
temperature
MUSCLE FUNCTION AFTER SPINAL CORD INJURY (((log-rolling)
Spinal Cord Injury Muscle Functioning remaining
Muscle Function Loss
Cervical, above C4 None All including respiration
C5 Neck, scapular elevation
Arm, chest, all below chest
C6-C7 Neck, some chest movement, some arm movement
Some arm, fingers, some chest
movement all below chest
Thoracic Neck, arms (full), some chest
Trunk, all below chest
Lumbo-sacral Neck, arms, chest, turnk
Legs
LaminectomyAutonomic dysreflexia (after spinal shock resolves)
Exaggerated autonomic response to stimuli: such as distended bladder or bowel (e.g. pain)
Severe hypertension Headache Flushed skin Diaphoresis Nasal Congestion
Management1. Place in high-Fowler’s position2. Ensure patency of urinary drainage and assess
for infection.
3. Eliminate other potential stimuli4. Notify physician: administer prescribed
antihypertensive
Nursing Diagnosis1. Impaired gas exchange related to muscle fatigue
and retained secretions.2. Decreased cardiac output r/t venous pooling and
immobility3. Impaired skin integrity r/t immobility and poor
tissue perfusion4. Constipation r/t the injury, inadequate fluid
intake, diet low in roughage and immobility5. Urinary retention6. Impaired physical mobility7. Risk for autonomic dysreflexia r/t reflex
stimulation of SNS8. Altered nutrition less than body requirements r/t
increased metabolic demand9. Sexual dysfunction r/t inability to achieve
erection or perceive pelvic sensations
Medical Management Immoblization—Gardner –well tongs, halo
external fixation Maintenance of heart rate (Atropine) and BP
(dopamine) vasopressors Methylprednisolone therapy Insertion of NGT Intubation, if needed Indwelling urinary catheter Stress ulcer prophylaxis (Proton-pump
inhibitos, H2 blockers) Physical therapy
Parkinson’s Disease(fourth common
neurodegenerative disease)Degeneration of dopamine-providing cells in the substantia nigra, which leads to degeneration of neurons in the basal ganglia; usually develops after 60 age
Associated with decreased levels of dopamine due to destruction of pigmented neuronal cells in the substantia nigra in the basal ganglia of the brain (Smelzer & Bare, 2004, p. 1979)
Imbalance between dopamine and acetylcholine
Three cardinal features:1. Tremors at rest
e.g. rhythmic, slow turning motion (pronation-supination) of the forearm and the hand and a motion of the thumb against the fingers as if rolling a pilltremor is present while at rest, increases when the patient is walking, concentrating, feeling anxious (Smeltzer & Bare, 2004, p. 1980).
2. Rigidity-resistance to passive limb movement3. Bradykinesia-most common features; patients
take longer to complete most activities and have difficulty initiating movement
Clinical Manifestations:Generalized feelings of stiffnessMild, diffuse muscular painHand tremor at rest (pill rolling)Akinesia Gait changes –shuffling gaitCharacteristic stance-stooped posture
Masklike-facial expressionSpeech pattern-slow, low volume monotonous in tone with poor articulationInvoluntary droolingDecreased lacrimation; constipation, incontinenceHeat intolerance; excessive perspirationLack of spontaneous swallowing
Medical ManagementLevodopa-Carbidopa T-synthetic precursor of dopamine for basal ganglia (Sinemet)Anticholinergic-to control symptoms (Cogentin, Artane, Symmetrel); anticholinergics drugs act at central sites to inhibit cerebral motor impulses that cause rigidity of themusculatureMAOI-Bomcriptine; inhibit breakdown of dopaminePhysiotherapy-reduces rigidity of muscles and prevents contracturesSurgical intervention-to destroy globus pallidus (to relieve rigidity) and/or thalamus (relieve tremors)
Nursing ManagementProvide safe environmentNutrition
Small bite pieces of food to prevent choking
Small frequent meals for easy mastication
Adequate intake of roughage to prevent constipation
Encourage diet rich in nutrient-dense foods such as fruits, vegetables, whole grains
Positioning and activity Limit postural activities Maintain gait as normal as possible:
may utilize cane or wheel chair Encourage daily physical therapy to
limit rigidity and prevent contractions Medication compliance; report side
effectsAvoid rushing client as he is unable to work under pressureAssist client in setting achievable goals to improve self-esteemTotal body function support in advanced stages (respiratory elimination)
Myasthenia Gravis Disturbance in the transmission of impulses at the
myoneural junction resulting in profound weakness (muscle of the eyes, eyelid, chewing, swallowing, speaking and breathing)
Believed to be due to reduced acetylcholine receptors due to destruction and blockage attributed to autoimmune process
An autoimmune disorder, characterized by varying degrees of weakness of the voluntary muscles (Smeltzer & Bare, 2004, p. 1956)
Highest in young adult females.
Manifestations Subjective:
Extreme muscle weakness, worsens as the muscle is used but disappears with rest
Dysphagia Diplopia (double vision) Dysarthria
Objective: Ptosis of the eyelid (both eyes) Myasthenia smile (nasal smile) Strabismus
Note:Myasthenia gravis is purely a motor disorder with NO
effect on sensation or coordination (Smeltzer & Bare, 2004, p. 1956)
Diagnostic Test Neostigmine (Prostigmine)—subcutaneous or IV
administration of tensilon (prevents enzymatic breakdown of Ach) to provided relief of symptoms
The thymus gland, which is a site of acetylcholine receptor antibody production is enlarged in myasthenia gravis (Smeltzer & Bare, 2004)
Medical Management Pharmacologic
- Acetylcholinesterase blockers- Corticosteroids to suppress immunity
Plasmapheresis - X-ray or surgical removal of thymus (thymectomy)
Myasthenic CrisisSudden inability to swallow or maintain respirations due to weakness of the muscles of respiration; undermedicationExacerbation of the disease process characterized by severe generalized muscle weakness and respiratory and bulbar weakness that may result in respiratory failure (Smeltzer & Bare, 2004, p.1957)
Cholinergic CrisisOverdose of anticholinergic drugs May mimic the symptoms of exacerbation
Note:Differentiation of myasthenic crisis and cholinergic
crisis can be achieved with the edrophonium chloride (Tensilon) Test. The patient with myasthenic crisis improves immediately following administration, while patient with cholinergic crisis may experience no improvement or deteriorate (Smeltzer & Bare, 2004)
Guillain-Barre SyndromeImmunologic status often follows respiratory or GIT infection, viral immunization, trauma or surgeryAn autoimmune attack of the peripheral nerve myelin (Smeltzer & Bare, 2004).Areas of demyelination in the motor cells of the spinal cord and medulla (ascending loss) vs. ALS (descending)Seen in adults 20-50 yearsAfter initial and plateau periods recovery in 1 year sometimes with residual deficits, other dies of complications
ALS- common in males
Manifestations- begins with muscle weakness and
diminished reflexes of the lower extremities
Subjective: Generalized weakness Paresthesia
DiplopiaObjective
Ascending paralysis within the body usually 24-72 hours
Respiratory paralysis Hypertension, tachycardia and low grade
fever Incontinence
Medical Management1. Steroids2. Plasmapheresis3. Support of vital function
Nursing Management: Supportive care1. Respiratory management2. Nutritional management3. Prevent complications4. Emotional support
Client with Multiple Sclerosis
1. Believed to be autoimmune response to prior viral infection
2. Inflammation destroys myelin leading to axon dysfunction; neurons in spinal cord, brain stem, cerebrum, cerebellum and optic nerve affected
3. Stressors trigger multiple sclerosis—febrile states, pregnancy, physical exertion and fatigue and these can trigger relapses
4. Incidence is highest in young adults (20-40); onset between 20-50; females more than males
Manifestations1. Fatigue2. Optic nerve involvement: blurred vision, haziness3. Brain stem involvement: nystagmus, dysarthria
(scanning speech); cognitive dysfunction, vertigo, deafness
4. Weakness, numbness in legs, spastic paresis, bladder and bowel dysfunction
5. Cerebellar involvement: nystagmus , ataxia, hypotonia
6. Blindness
MeningitisInflammation of pia matter, arachnoid and subarachnoid spaceSpreads rapidly through CNS because of circulation of CSF around brain and spinal cordMay be bacterial, viral, fungal, parasitic in originInfection enters CNS though invasive procedure or through bloodstream, secondary to another infection in body
Bacterial Meningitis Causative organism: Neisseria meningitides,
Streptococcus pneumonia, Haemophilus influenza, Escherichia coli
Manifestationsa. Fever, chillsb. Headache, back and abdominal painc. Nausea and vomitingd. Meningeal irritation:
Nuchal rigidity (stiff neck)-early sign Positive Kernig’s sign Positive Brudzinski’s sign-when the patient’s
neck is flexed, flexion of the knees and hips is produced
Photophobia –extreme sensitivity to lighte. Meningococcal meningitis: rapidly spreading
petechial rash of skin and mucous membrane
f. Increased ICP: decreased LOC, papilledema –edema of optic disc due to increased ICP
Viral Meningitis Less severe, benign course with short duration,
intense headache with malaise, nausea, vomiting, lethargy, signs of meningeal irritation
Encephalitis1. Acute inflammation of parenchyma of brain or spinal
cord2. Usually caused by virus
Medications1. Meningitis: immediate treatment of effective
antibodies for 7-21 days according to culture results; dexamethasone to suppress inflammation
Dilantin—Increase seizure threshold
Health Promotion1. Vaccinations for meningococcal, pneumococcal,
haemophilus meningitis2. Prophylactic rifampins for persons exposed to
meningococcal meningitis3. Mosquito control4. Prompt diagnosis5. Asepsis care for clients with open head injury or
neurosurgery
Hydrocephalus Increase in volume of CSF within ventricular system,
which becomes dilatedCommon Cause:1. Noncommunicating obstruction in CSF drainage from
ventricular system2. Communicating: CSF is not effectively reabsorbed
through arachnoid villi3. Normal pressure hydrocephalus: occurs in
persons>60 in which ventricles enlarge causing cerebral tissue compression
4. Manifestations depend on rate of onset: progressive cognitive dysfunction, gait disruptions, urinary incontinence
Visual changesIncrease in head sizeIncrease ICP
Treatment/Management1. Diuretics2. Surgery3. Protect from injury from altered LOC and immobility
Skeletal muscle
Attach to the skeletonPermits voluntary movementsMaintain postureGenerates heatInnervated by the somatic nervous systemProduce movement by contractionSarcomeres-functional unit of striated muscle
Basic Principles of skeletal muscle action1. Motor unit should be stimulated to contract, absence
of impulse conduction leads to paralysis2. Muscles are attached to at least 2 bones; with each
contraction, muscle’s insertion bone moves and the muscle origin bone remains stationary
3. Bone serve as levers; joint as fulcrums

Fractures- Break in the continuity of bone
Classification: Closed-no break in the skin Open- Complete-involves break across the entire
cross-section of the bone and is frequently displaced
Incomplete e.g. greenstick, the break occurs through only part of the cross-section of the bone
Displaced Comminuted-several bone fragments Impacted or compression Complicated-accompanied by infection Pathologic-systemic, loss of bone density
Clinical ManifestationsDeformitySwellingBruisingMuscle spasmTendernessPainImpaired sensationLoss of normal functionCrepitus- grating sensation resulting from rubbing of bone fragments against each otherAbnormal mobility of affected partHypovolemic shock
Vasogenic shock-due to severe pain
Surgical/Medical Management Open-reduction-alignment during surgery Internal fixation device placement: use of
screws, wires, nails or rods Closed reduction Traction application Management of shock
Nursing Management for Fractures
1. Assess neurovascular status (6 P’s)
ulselessnessallorainaresthesiaoikilothermiaaresia/paralysis
2. Assess skin3. Assess for fat embolism-long bone fracture, may
occur 24-48 hours after injury4. Analgesics-Opioid analgesics5. Rehabilitation
Cast Application
Purposes:1. Immobilization2. Prevention or correction of deformity3. Maintenance support and protection to realign bone4. Promotion of healing which allows early weight
bearing
Nursing Management: CAST
Precast application
- Care- factual and sensory information- Contraindications
IntracastingPostcasting
- Drying 24-48 hours- Proper handling- Watch for neurovascular complications- Watch for infection- Watch for cast syndrome (occurs with body
casts) Prolonged nausea and vomiting Abdominal distention and pain
Cast syndrome-psychological (claustrophobic reaction) and physiologic (superior mesenteric artery syndrome) responses to confinement in body cast (Smeltzer & Bare, 2004)
- Watch for: wet-spots-drainage: hot spots-tissue infection or necrosis under casts
- Elevated injured extremity especially for the first 24-48 hours
- Prevents disuse syndromeExercise joints before and after injured siteIsometric exercises, gluteal setting, abdominal tightening and deep breathing exercisesSkin careEliminationNutrition- Vit C (absorption of calcium)
Cast care Keep cast dry; use plastic when bathing Do not use powder or insert objects inside cast Use of slings/crutches to enhance comfort safety and
ambulation Reportable conditions:
- Increased swelling- Tingling or burning sensation- Inability to move muscle around cast- Foul odor inside or around the edge
Therapeutic Traction- Pulling force
Types:1. Skin2. Skeletal3. Cervical4. Pelvic5. Buck’s traction (unilateral or bilateral) is skin
traction to the lower leg6. Russel’s – one leg is higher than the other
Techniques:1. Running (Straight) applies the pulling force in a
straight line with body part resting on bed2. Suspension (Balanced)-supports the affected
extremity off the bed and allows for some patient movement without disruption of the line of pull
3. Continuous intermittent
Care of Client1. Know the purpose and contraindicated movements2. Pin site care-goal is avoid infection and development
of osteomyelitis; site is covered with a sterile dressing (Smeltzer & Bare, 2004, p. 2028)
3. Ropes and pulley should hang free4. Monitor color, warmth, movement and sensation of
extremity distal to the traction every 4-8 hours ( neurovascular check)
5. Devices such as trapeze, fracture pins

6. Immobility problems (thrombophlebitis, diversional therapies , among others)
After traction: Gradually assume sitting position Lack of proprioception response initially Joints may be unstable; may feel faint or weak for
a while
Principles of Effective Traction Traction must be continuous to be effective in
reducing and immobilizing fractures Skeletal traction is never interrupted Weights are not removed unless intermittent traction
is prescribed Any factor that might reduce the effective pull or
alter its resultant line of pull must be eliminated:- Patient must be in good body alignment in the
center of the bed when traction is applied- Ropes must be unobstructed- Weights must hang free and not rest on the
bed or floor- Knots in the rope or the footplate must not
touch the pulley or the foot of the bed - (Smeltzer & Bare, 2004, p. 2026)
Nursing Care of Clients with Braces or Splints
1. Check body and equipment alignment2. Keep equipment in good condition 3. Examine integumentary integrity
Use of Cane1. Ascertain client capability to bear weight2. Ensure strength of upper extremity opposite lower
extremity3. Ensure proper length of cane
Highest point approximately at level of greater trochanter
30 degrees flexion of elbow Tip of the cane 15 cm (6 inches) lateral to the
base of the fifth toe (Smeltzer & Bare, 2004, p. 174)
4. Ensure proper techniques Opposite affected extremity Affected extremity cane simultaneously Should be close to the body
5. Observe for incorrect use Leaning the body over the cane Shortening the stride of the unaffected side Persistence of abnormal gait
CrutchNursing care
1. Ensure readiness of client Strength of upper torso Psychological fitness
2. Ensure proper fit Axillary bars 5 cm (2 inches below axilla), 15
cm (6 inches infront and lateral) tripod position
3. Assist in use of proper technique Four point- R crutch, L foot, LC, RF Two-point-R crutch with L foot, then LC with
RF Three point-advance both crutches and
weak extremity, then follow good foot Swing to gait-advance crutches then swing
feet to the level of the crutches Swing through gait-advance crutches then
swing through the crutches4. Incorrect position
Walking on ball of foot Hunching shoulders Looking downward Hiking hips (common in amputees) Bearing weight under arms may cause
brachial plexus damage Lifting crutches while still bearing down on
them5. Evaluate client’s response
Arthritis Disease involving degeneration and or
inflammation of joints and surrounding structures
Out of 100 types of with unknown cause Common types:
1. Inflammatory –RA and SLE2. Non-inflammatory –degenerative joint
disease3. Gout-crystal-produce disease from high
protein ingestion
Osteoarthritis Autosomal recessive trait causing cartilages to
wear out or repair less effective; localized; NO synovial membrane swelling
o Wear and tear of jointso Obesity; joint traumao Aging: 55 years old and aboveo Degeneration and atrophy of the
cartilage and calcification of ligamentso Primarily affects weight-bearing joints,
spine and hands Degeneration of cartilages into the bony spur Formation of subchondral osteophyte Secondary synovitis (late manifestation)-pain
and swelling with joint movement
Manifestations: Joint stiffness Pain after exercise; pain with movement Heberden’s (distal) and Bouchard’s (proximal)
nodes Decreased ROM Crepitus
Medical Management Steroids Antiinflammatory Analgesics-salicylates and NSAIDs Physiotherapy/Exercise Surgery-replacement of mobility (knee and hips
common)
Rheumatoid Arthritis

Systemic with synovial membrane inflammation with blood, fibrin, and coagulation deposits
Unknown cause: hereditary, autoimmune psychophysiologic factors, 25-55 years old
Exacerbations linked to physical and emotional stress
Inflammatory changes in the connective tissue
Pathophysiology:Symmetrical joints
Synovial lining of joints become inflamed
Synovitis
Increased fluid with pannus
Pannus destroys cartilage and invade joint capsule
Replaced by fibrous connective tissues
Affects tendons and ligaments
Cause joint subluxation, bony ankylosis and consolidation of joints
Swelling, deformities
PainManifestations:
Subjective Fatigue, malaise, anorexia Joint pain, stiffness after periods of
inactivity especially a.m Paresthesia (destruction of nerve
involved)Objective Joint inflammation and deformity Swan neck and Boutinniere
deformities; ulnar drift, joint subluxation
Increased ESR, low grade fever , positive rheumatoid factor
Anemia, weight loss
Medical Management Coticosteroids, anti-inflammatory,
analgesics, immune suppressive drugs Plasmapheresis Antimalarial drugs—destroys
autoimmune antibodies Cytotoxic drugs
Note:Deformities of the hands and feet are common in RA.
The deformity may be caused by misalignment resulting from swelling, progressive joint destruction, or the subluxation (partial dislocation) that occurs when bone slips over another and eliminates the joint space (Smeltzer & Bare, 2004, p. 1621)
Gouty Arthritis Mono-articular (one joint) Hyperuricemia; 40-50 years old
1. Genetic increase in purine metabolism and production
2. Ingestion of excessive alcohol or high purine diet
Pathophysiology:
Uric acid-major by product of protein and nucleic acid metabolism
Tendency to crystallize especially with dehydration, diuretics use and increased
Tubular resorption to the systemic circulation
Deposited in connective tissues and joints (esp. great toe)
Release of lysosomal enzymes
Inflammation
Joint degeneration and disability and tophaceous (white in color) deposits in the joints
May cause renal tubular damage leading to renal stones and failure
Note: Attacks of gout appear to be related to sudden
increases or decreases of serum uric acid levels. When the urate crystals precipitate within a joint, an inflammatory response occurs and an attack of gout begins. With repeated attacks, accumulation of sodium urate crystals, called tophi, are deposited in peripheral areas of the body, such as great toe, the hands, and the ear (Smeltzer & Bare, 2004, p. 1630).
Manifestations:- Tight/reddened skin around inflamed joint,
edema- Pain- Increase temperature- Hyperuricemia> 7.5 mg/dl
Management of Gout1. Decrease protein in diet2. Weight control and decrease alcohol ingestion3. Increase fluids to 3000 ml/day (the more
dehydration, more crystallization)4. Joint rest5. Allupurinol/Probenecid, Colechicine
High Purine foods1. Poultry2. Organ meats3. Meat extracts4. Seafoods, sardines, anchovies, shrimp herring 5. Asparagus, spinach, mushroom
Surgical intervention1. Arthrodesis-surgical fusion of a joint to render a joint
immobile but decreases pain and increases strength2. Osteotomy-transection of a bone to correct a
deformity or misalignment3. Resection-for partial removal of a degenerated bone
(wrist and foot)4. Replacement arthroplasty-joint replacement
Assistive devices:1. Eating utensils2. Braces3. Walkers4. Cane-single, quad
Therapies1. Diversion2. Exercise, ROM, quadriceps exercise3. TENS4. Cold and warm pack 30 minutes before activities5. Whirl pool bath6. Balance rest and activity7. Assistive devices, elevated chair or toilet to 3-4
inches
Nursing DiagnosisChronic pain related to joint degenerationImpaired physical activity r/t restricted mobilizationActivity intolerance

Self-care deficitBody image disturbance r/t visible body changes/deformities/misalignmentKnowledge deficitSleep pattern disturbance