Peptic Ulcer Disease - nleaders.orgnleaders.org/.../S05-Peptic-Ulcer-Disease.pdf · Peptic Ulcer...
13
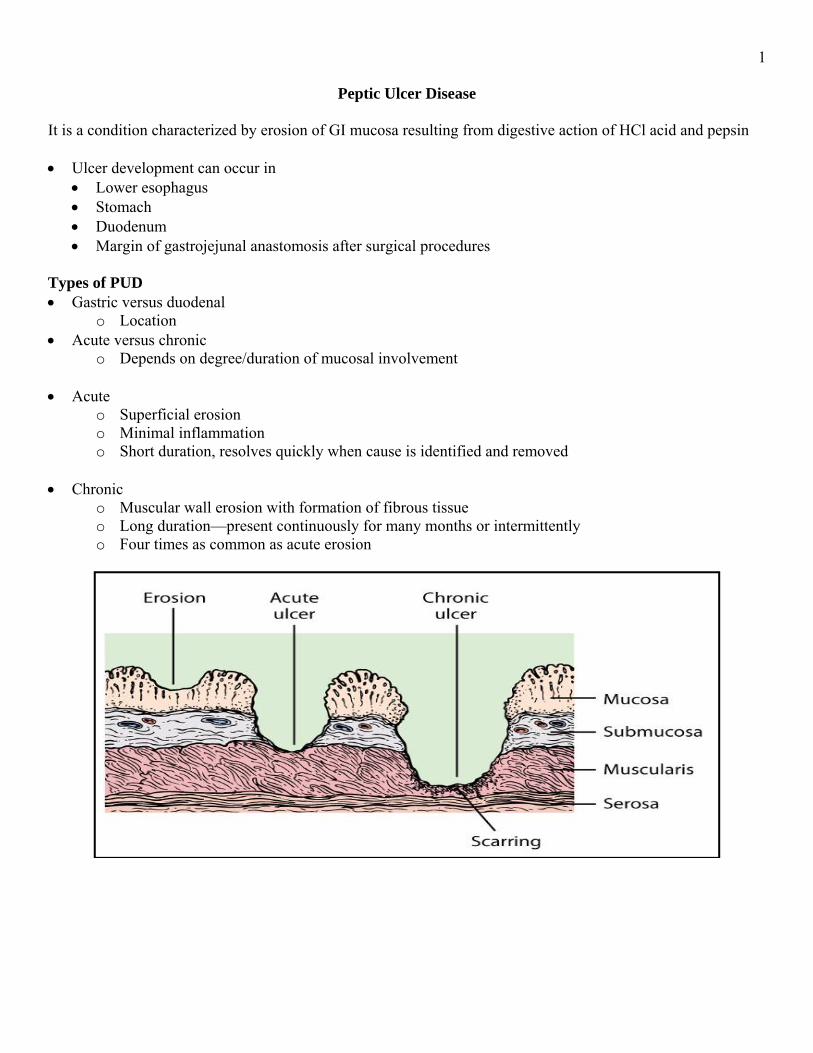
1 Peptic Ulcer Disease It is a condition characterized by erosion of GI mucosa resulting from digestive action of HCl acid and pepsin • Ulcer development can occur in • Lower esophagus • Stomach • Duodenum • Margin of gastrojejunal anastomosis after surgical procedures Types of PUD • Gastric versus duodenal o Location • Acute versus chronic o Depends on degree/duration of mucosal involvement • Acute o Superficial erosion o Minimal inflammation o Short duration, resolves quickly when cause is identified and removed • Chronic o Muscular wall erosion with formation of fibrous tissue o Long duration—present continuously for many months or intermittently o Four times as common as acute erosion
Transcript of Peptic Ulcer Disease - nleaders.orgnleaders.org/.../S05-Peptic-Ulcer-Disease.pdf · Peptic Ulcer...
1
Peptic Ulcer Disease It is a condition characterized by erosion of GI mucosa resulting from digestive action of HCl acid and pepsin • Ulcer development can occur in
• Lower esophagus • Stomach • Duodenum • Margin of gastrojejunal anastomosis after surgical procedures
Types of PUD • Gastric versus duodenal
o Location • Acute versus chronic
o Depends on degree/duration of mucosal involvement • Acute
o Superficial erosion o Minimal inflammation o Short duration, resolves quickly when cause is identified and removed
• Chronic
o Muscular wall erosion with formation of fibrous tissue o Long duration—present continuously for many months or intermittently o Four times as common as acute erosion

2 Etiology and Pathophysiology • Develops only in presence of acid environment
o Excess of gastric acid not necessary for ulcer development • Pepsinogen is activated to pepsin in presence of HCl acid and at pH of 2 to 3
o Secretion of HCl acid by parietal cells has a pH of 0.8 o pH reaches 2 to 3 after mixing with stomach contents o When stomach acid is neutralized by food, antacids or acid blocking drugs, pH increases to 3.5 or
more o Pepsin has little or no proteolytic activity
• Stomach normally protected from autodigestion by gastric mucosal barrier o Surface mucosa of stomach is renewed about every 3 days
Mucosa can continually repair itself except in extreme instances o Water, electrolytes, and water-soluble substances can pass through barrier o Mucosal barrier prevents back-diffusion of acid and pepsin from gastric lumen through mucosal
layers to underlying tissue • Mucosal barrier can be impaired and back-diffusion can occur
o Cellular destruction and inflammation occur o Release of histamine
Vasodilation Increased capillary permeability Secretion of acid and pepsin
Back-Diffusion of Acids

3 Destroyers of Mucosal Barrier
• Helicobacter pylori o Produces enzyme urease
Mediates inflammation making mucosa more vulnerable • Aspirin and NSAIDs
o Inhibit syntheses of prostaglandins Cause abnormal permeability
• Corticosteroids o ↓ Rate of mucosal cell renewal
↓ Protective effects • Lipid-soluble cytotoxic drugs
o Pass through and destroy it • ↑ Vagal nerve stimulation
o Emotions o ↑ in HCl acid
• When mucosal barrier is disrupted, compensatory mechanisms (e.g., histamine) ↑ blood flow • As blood flow ↑
o Hydrogen ions removed o Buffers neutralize ions present o Nutrients for cell function arrive o ↑ Rate of mucosal cell replication
• If increase is sufficient to dilute buffer and remove excess H+ ions o Minor or no tissue damage
• If blood flow is not sufficient o Tissue injury results
• More Protective Mechanisms
o Mucus secreted to form a layer that entraps or slows diffusion of H+ ions across mucosal barrier o Bicarbonate is secreted
Neutralizes HCl acid in lumen of GI tract Disruption of Gastric Mucosal Barrier

4 Gastric Ulcers
• Occur in any portion of stomach • Most common—lesser curvature in close to antral junction • Characterized by
o Normal to low secretion of gastric acid o Some intraluminal acid essential
• Causes o Drugs o Aspirin, NSAIDs, corticosteroids o Chronic alcohol abuse o Chronic gastritis o Bile reflux o Nicotine
• 60% to 80% present with H. pylori o H. pylori—more destructive when drugs or smoking involved
Duodenal Ulcers
• Associated with increased HCl acid secretion • H. pylori is found in 90% to 95% of patients
o Not all individuals with H. pylori develop ulcers • Increased risk of duodenal ulcers in those with patients treated for these conditions:
o COPD o Cirrhosis of liver o Chronic pancreatitis o Hyperparathyroidism
• Increased risk of duodenal ulcers with smoking and alcohol use Stress-Related Mucosal Disease
• Also called physiologic stress ulcer • Acute ulcers that develop after major physiologic insult
o Trauma or surgery • Form of erosive gastritis • Prophylaxis with antisecretory agents

5 Clinical Manifestations
• Common—no pain or other symptoms o Due to lack of sensory pain fibers
• If pain exists o Gastric ulcer pain
High in epigastrium 1 to 2 hours after meals Burning or gaseous
o Duodenal ulcer pain Midepigastric region beneath xiphoid process Back pain—if located posterior aspect 2 to 4 hours after meals Tendency to occur, then disappear, then occur again
Complications
• Three major complications include o Hemorrhage o Perforation o Gastric outlet obstruction
• All considered emergency situations Hemorrhage
• Most common complication of peptic ulcer disease • Develops from erosion of
o Granulation tissue found at base of ulcer during healing o Ulcer through a major blood vessel
Task: See Peptic Ulcer Video Perforation
• Most lethal complication of peptic ulcer • Common in large penetrating duodenal ulcers that have not healed and are located on posterior mucosal
wall • Perforated gastric ulcers often located on lesser curvature of stomach • Mortality rates higher with perforation of gastric ulcers • When ulcer penetrates serosal surface with spillage of contents into peritoneal cavity • Size proportional to length of time ulcer existed • Large perforations: Immediate surgical closure • Clinical manifestations
o Sudden, dramatic onset o Severe upper abdominal pain spreads throughout abdomen o Possible shoulder pain o Rigid, boardlike abdominal muscles o Shallow, rapid respirations o Bowel sounds absent o Nausea/vomiting o History reporting symptoms of indigestion or previous ulcer
• Bacterial peritonitis may occur within 6 to 12 hours • Difficult to determine from symptoms alone if gastric or duodenal ulcer has perforated
6 Gastric Outlet Obstruction
• Predisposition to gastric outlet obstruction include • Ulcers located in
o Antrum and prepyloric and pyloric areas of stomach o Duodenum
• Obstruction due to o Edema o Inflammation o Pylorospasm o Fibrous scar tissue formation o All contribute to narrowing of pylorus
• Early phase: Gastric emptying normal • Over time, ↑ contractile force needed to empty stomach
o Hypertrophy of stomach wall • After long-standing obstruction
o Stomach dilates and becomes atonic • Clinical manifestations
o Usually long history of ulcer pain o Pain progresses to generalized upper abdominal discomfort o Pain worsens toward end of day as stomach fills and dilates o Relief obtained by belching or vomiting o Vomiting is common o Constipation is a common complaint
Dehydration, lack of roughage in diet o Swelling in stomach and upper abdomen o Loud peristalsis o Visible peristaltic waves o If stomach grossly dilated, may be palpable
Diagnostic Studies
• To determine presence and location of ulcer • Endoscopy with biopsy
o Most often used Allows for direct viewing of mucosa
o Determines degree of ulcer healing after treatment o During procedure, tissue specimens can be obtained to identify H. pylori and rule out gastric
cancer • Tests for H. pylori
Serum or whole blood antibody tests • Immunoglobin G (IgG)
o 90% to 95% sensitive o Will not distinguish between active or recently treated disease
Urea breath test • Urea is by product of metabolism of H. pylori
Stool antigen test • Not as accurate as breath test

7
• Barium contrast studies o Widely used o Not accurate for shallow, superficial ulcers o Used in diagnosis of gastric outlet obstruction
• X-ray studies o Ineffective in distinguishing a peptic ulcer from a malignant tumor o Do not show degree of healing like that of endoscope
• Gastric analysis o Analyze gastric contents for acidity and volume o NG tube is inserted, and gastric contents are aspirated o Contents analyzed for HCl acid o Histalog and pentagastrin may be used to stimulate HCl acid secretion o Helps determine presence of gastrinoma (Zollinger-Ellison syndrome)
• Laboratory analysis o CBC
Anemia o Urinalysis o Liver enzyme studies o Serum amylase determination
Pancreatic function o Stool examination
Blood presence Collaborative Care
• Medical regimen consists of o Adequate rest o Dietary modification o Drug therapy o Elimination of smoking and alcohol o Long-term follow-up care o Stress management
• Aim of treatment program o Reduce degree of gastric acidity o Enhance mucosal defense mechanisms o Minimize harmful effects on mucosa
• Aspirin and nonselective NSAIDs may be stopped
Drug Therapy
• Use of o H2R blockers o PPIs o Antibiotics o Antacids o Anticholinergics
• Recurrence of peptic ulcer is frequent o Interruption or discontinuation of therapy can have detrimental results
• No other drugs, unless prescribed by health care provider, should be taken o Ulcerogenic effect

8
• Histamine-2 receptor blocks (H2R blockers) o Frequently used o Block action of histamine on H2 receptors
↓ HCl acid secretion ↓ Conversion of pepsinogen to pepsin ↑ Ulcer healing
o Therapeutic effects last up to 12 hours o Oral or IV o Examples
Ranitidine (Zantac) Famotidine (Pepsid)
• Proton pump inhibitors (PPI) o Block ATPase enzyme—important for secretion of HCl acid o ↑ Effective than H2R blockers—reducing acid and promoting healing o Examples
Esomeprazole (Nexium) Omeprazole (Prilosec)
• Antibiotic therapy o Eradicate H. pylori infection o Most important in treatment if H. pylori present o No single agents have been effective in eliminating H. pylori o Usual treatment 7 to 14 days o Example of therapy
Dual therapy—ranitidine bismuth citrate (Tritec) with clarithromycin (Biaxin) • Antacids
o Adjunct therapy for PUD o Increase gastric pH by neutralizing HCl acid o Effects on empty stomach 20 to 30 minutes o If taken after meals may last 3 to 4 hours o Magnesium hydroxide
Watch for diarrhea o Aluminum hydroxide
Watch for constipation o ↑ Sodium preparations: Not be used in elderly or patients with ↑BP, heart failure, liver cirrhosis,
or renal disease o Magnesium preparations: Not be used in patients with renal failure
• Anticholinergic drugs o Occasionally used o ↓ Cholinergic stimulation of HCl acid o ↓ Gastric motility: Not used for gastric outlet obstruction
Nutritional Therapy
• Dietary modifications: Food and beverages irritating to patient are avoided or eliminated • Bland diet • Six small meals a day during symptomatic phase • List of foods to avoid
o Hot, spicy foods and pepper, alcohol, carbonated beverages, tea, coffee, broth • Foods high in roughage may irritate mucosa

9
• Protein: Best neutralizing food o But also stimulates gastric secretions
• Carbohydrates and fats are least stimulating to HCl acid secretion o Do not neutralize well
Therapy Related to Complications
• Acute exacerbation o Treated with same regimen used for conservative therapy o Situation is more serious because of possible complications of perforation, hemorrhage, gastric
outlet obstruction o Accompanied by bleeding, increased pain and discomfort, nausea, vomiting o Recurrent vomiting or gastric outlet obstruction
NG tube placed in stomach with intermittent suction for ~24 to 48 hours Fluids and electrolytes are replaced by IV infusion until patient is able to tolerate oral
feedings without distress o Management is similar to that for upper GI bleeding o Endoscopic evaluation
Reveals degree of inflammation or bleeding and ulcer location o 5-year follow-up program recommended after acute exacerbation
• Perforation o Immediate focus:
Stop spillage of gastric or duodenal contents into peritoneal cavity Restore blood volume
o NG tube is placed into stomach Continuous aspiration Placement of tube near to perforation site facilitates decompression
o Circulating blood volume: Replaced with lactated Ringer’s and albumin solutions o Blood replacement in form of packed RBCs may be necessary o Central venous pressure line inserted and monitored hourly o Indwelling urinary catheter inserted and monitored hourly o ECG—if history of cardiac disease o Broad-spectrum antibiotics o Pain medication o Open or laparoscopic repair
• Gastric outlet obstruction o Decompress stomach o Correct any existing fluid and electrolyte imbalances o Improve patient’s general state of health o NG tube inserted in stomach, attached to continuous suction o Continuous decompression allows
Stomach to regain its normal muscle tone Ulcer to begin to heal Inflammation and edema to subside
o After several days, NG clamped and residual volumes checked o Common to clamp tube overnight for 8 to 12 hours and measure residual in morning o When aspirate below 200 ml
Within normal range Oral intake of clear liquids can begin
o Watch patient carefully for signs of distress or vomiting

10
o As residual ↓ solid foods added and tube removed o IV fluids and electrolytes
Administered according to degree of dehydration, vomiting, electrolyte imbalance o Pyloric obstruction: Endoscopically treated with balloon dilations o Surgery may be necessary to remove scar tissue
Nursing Diagnoses
• Acute pain • Ineffective therapeutic regimen management • Nausea
Nursing Overall Goals
• Comply with prescribed therapeutic regimen • Experience a reduction or absence of discomfort • Exhibits no signs of GI complications • Have complete healing • Lifestyle changes to prevent recurrence
Nursing Implementation
• Health promotion o Identify patients at risk o Early detection and treatment o Encourage patients to take ulcerogenic drugs with food or milk o Teach to report symptoms related to gastric irritation to health care provider
• Acute intervention o General complaints are increased pain, nausea, vomiting, and some bleeding o Convey treatment measures to patient/family o Regular mouth care o Cleanse and lubricate nares o Vital signs hourly o Physical and emotional rest o Sedatives can mask symptoms of shock
• Care for Complications o Assessment and management accordingly [preoperative and postoperative care]
• Nurse education o Disease
Teach basic etiology/pathophysiology o Drugs
Actions, side effects, danger of taking any medication without health care provider approval
Lifestyle changes Appropriate changes in diet
Regular follow-up care Encourage compliance with plan of care Importance of immediate reporting of N/V, epigastric pain, bloody emesis or tarry stools

11 Surgical Therapy
• Uncommon because of antisecretory agents • Indications for surgical interventions
o Unresponsive to medical management o Concern about gastric cancer o Drug induced but cannot be withdrawn from drugs
Surgical Procedures
Billroth I: Gastroduodenostomy • Partial gastrectomy with removal of distal 2/3 stomach and anastomosis of gastric stump to
duodenum
Billroth II: Gastrojejunostomy • Partial gastrectomy with removal of distal 2/3 stomach and anastomosis of gastric stump to
jejunum

12
Vagotomy • Severing of vagus nerve • Done in conjunction with gastrectomy
Pyloroplasty • Surgical enlargement of pyloric sphincter • Commonly done after vagotomy • ↓ Gastric motility and gastric emptying • If accompanying vagotomy, ↑gastric emptying
Preoperative Care
• Laparoscopic or open surgery techniques • Surgeon should educate family/patient on surgical procedure • Nurse can clarify questions • Instructions should be given on
o Comfort measures o Pain relief o Coughing and deep breathing o NG tube o IV fluids
Postoperative Complications
Dumping Syndrome o 33% to 50% of patients experience after surgery o Direct result of surgical removal of a large portion of stomach and pyloric sphincter o ↓ Ability of stomach to control amount of gastric chyme entering small intestine
Large bolus of hypertonic fluid enters intestine ↑ Fluid drawn into bowel lumen
o Occurs at end of meal or 15 to 30 minutes after eating o Symptoms include
Weakness, sweating, palpitations, dizziness, abdominal cramps, borborygmi, urge to defecate Last no longer than an hour
Postprandial Hypoglycemia o Variant of dumping syndrome o Result of uncontrolled gastric emptying of a bolus of fluid high in carbohydrate into small intestine
↑ Blood sugar Release of excessive amounts of insulin into circulation
o Secondary hypoglycemia occurs with symptoms ~2 hours after meals o Symptoms include sweating, weakness, mental confusion, palpitations, tachycardia and anxiety o When symptoms occur, immediate ingestion of sugared fluids or candy relieves symptoms
Bile Reflux Gastritis o Surgery can result in reflux alkaline gastritis
Prolonged contact of bile causes damage to gastric mucosa May result in back-diffusion of H+ ions through gastric mucosa PUD may reoccur Continuous epigastric distress that ↑ after meals Administration of cholestyramine (Questran) relieves irritation Aluminum hydroxide antacids also used

13 Nutritional Therapy Postoperatively
• Start as soon as immediate postoperative period is successfully passed • Patient should be advised to reduce drinking fluid (4 oz) with meals • Diet should consist of
o Small, dry feedings daily o Low in carbohydrates o Restrict sugar with meals o Moderate amounts of protein and fat o 30 minutes of rest after each meal
Postoperative Care
• Similar to postop care after abdominal laparotomy • NG tube used to decompress and decrease pressure on suture line • Aspirate observed for
o Color Bright red at first with darkening within first 24 hours Color changes yellow-green within 36 to 48 hours
o Amount o Odor
• NG suction must be in working order and patency maintained • Observe for signs of ↓ peristalsis and lower abdominal discomfort
o Intestinal obstruction • Accurate I/O essential • Vital signs every 4 hours • Frequent position changes • IV therapy • Observe for signs of infection • Long-term complication—pernicious anemia