
Pelvic Masses & Ovarian Cancer. Differential diagnosis of pelvic masses Investigations and...
27
Pelvic Masses & Ovarian Cancer
-
Upload
camilla-lester -
Category
Documents
-
view
268 -
download
0
Transcript of Pelvic Masses & Ovarian Cancer. Differential diagnosis of pelvic masses Investigations and...
Pelvic Masses & Ovarian Cancer
• Differential diagnosis of pelvic masses• Investigations and management• Benign ovarian cysts• Ovarian cancer
Pre-pubertal1. Functional cyst2. Germ cell tumour
Adolescent1. Functional cyst2. Pregnancy3. Dermoid4. Other germ cell tumour5. Obstructing
vaginal/uterine abnormality
6. Epithelial cell tumour
Reproductive1. Pregnancy2. Functional cyst3. Fibroids4. Epithelial tumour
Perimenopausal1. Fibroids2. Epithelial tumour3. Functional cyst
Postmenopausal
1. Ovarian tumour
2. Functional cyst
3. Other malignancy
4. Metastases
Diagnosis
• History and examination
• Ultrasound
• CT/MRI
• Tumour markers – CA125, CEA, CA19,9 hCg, alpha-fetoprotein
• 50 % - asymptomatic
• 30% - menorrhagia
• Irregular bleeding
• Pressure effects
Management
Depends on symptoms and fertility issuesReassure that risk of malignancy tiny• Hysteroscopic removal (small submucosal)• Myomectomy• Embolisation• Hysterectomy
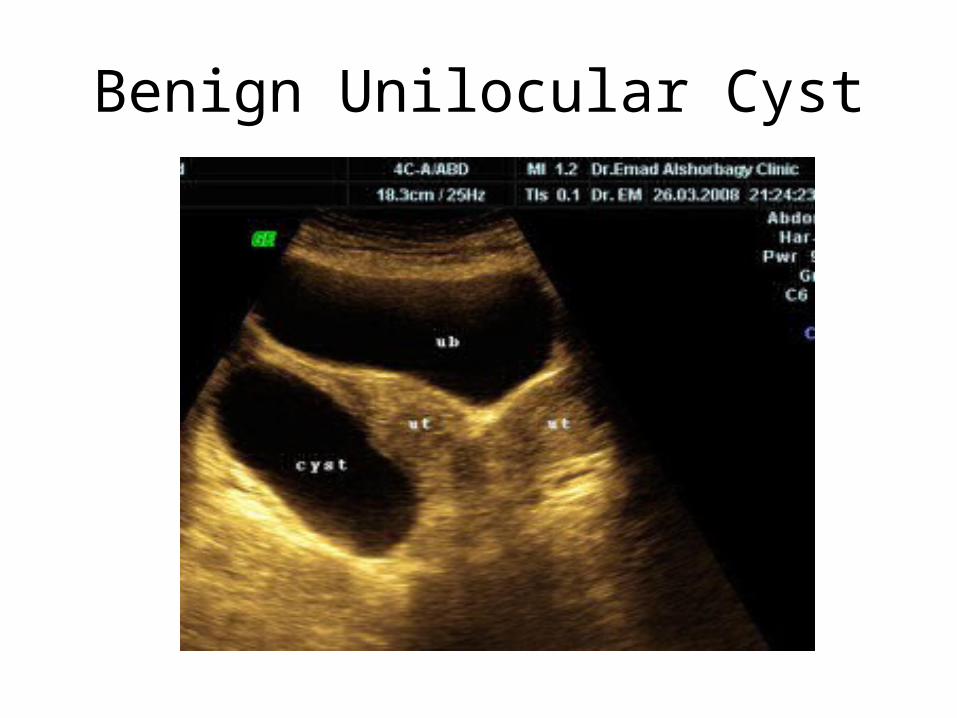
Benign Unilocular Cyst
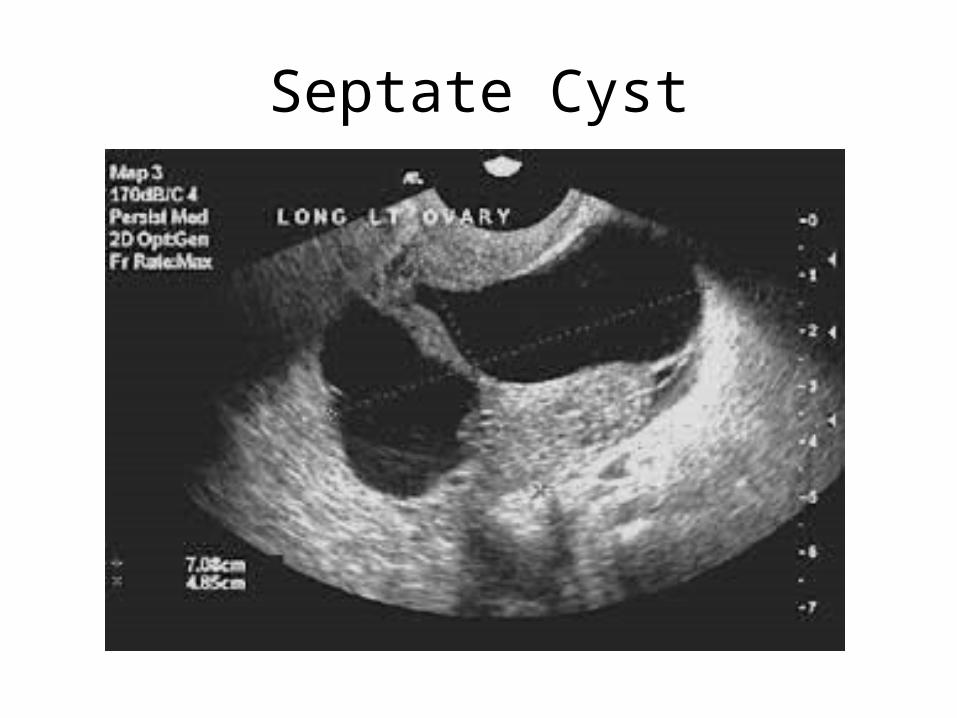
Septate Cyst
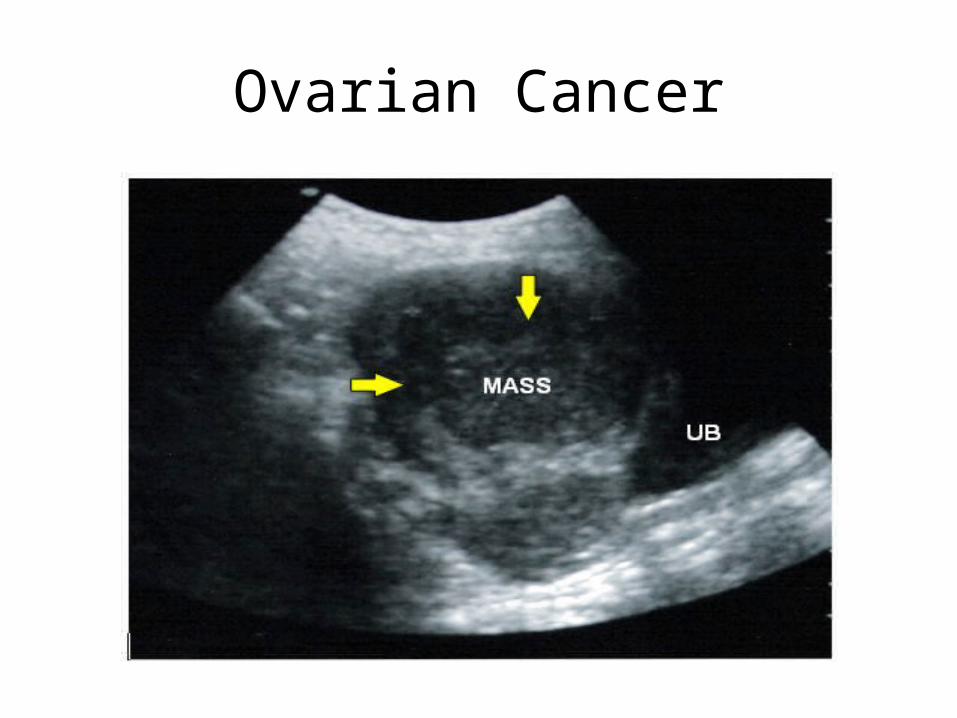
Ovarian Cancer
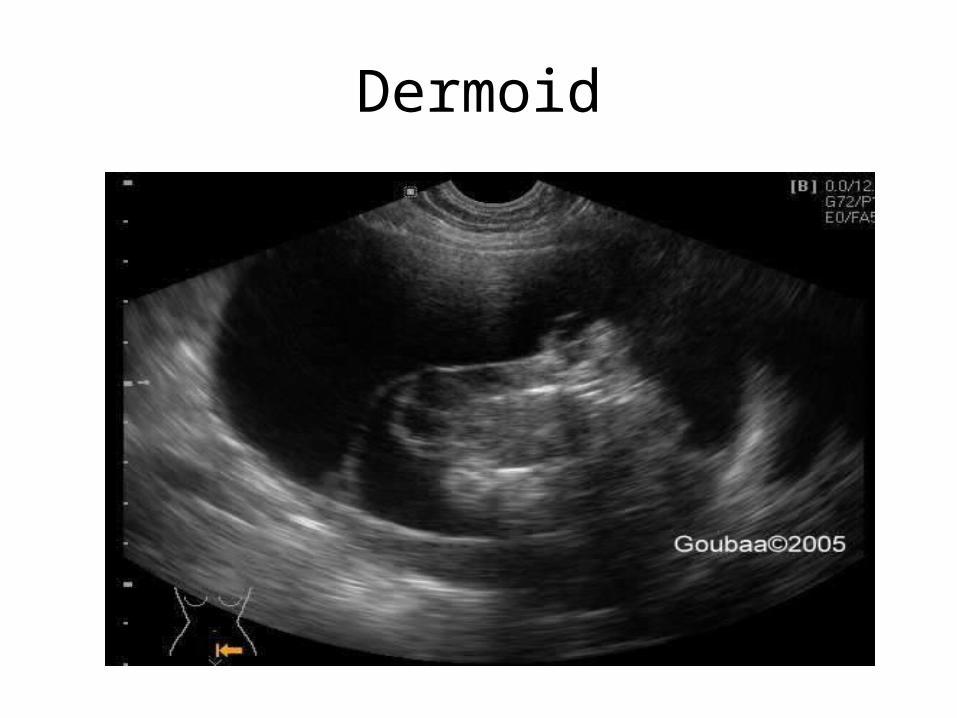
Dermoid
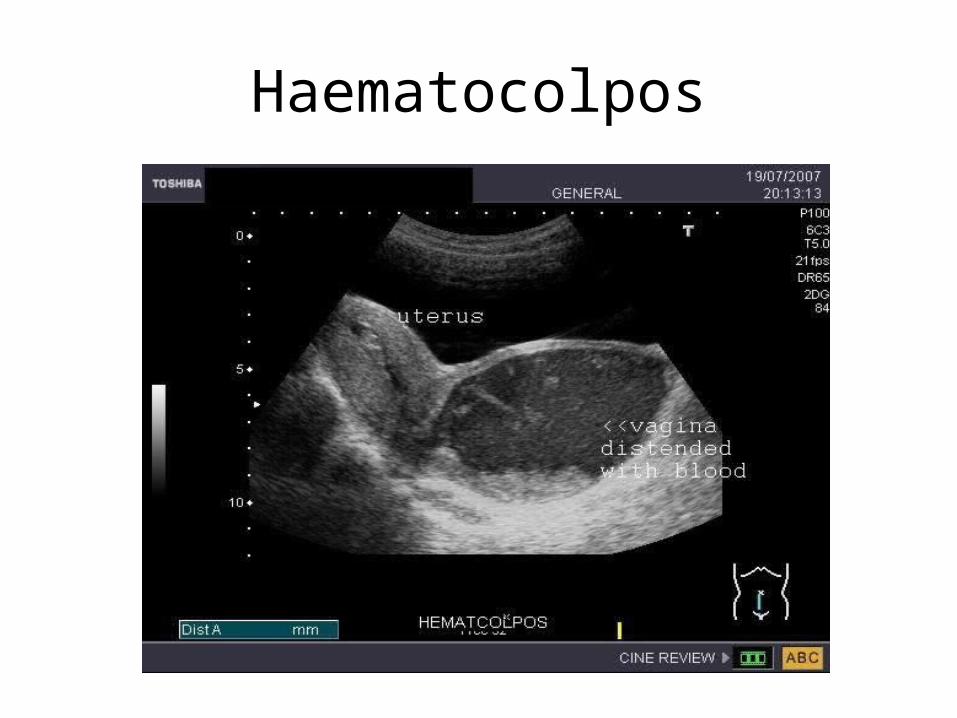
Haematocolpos
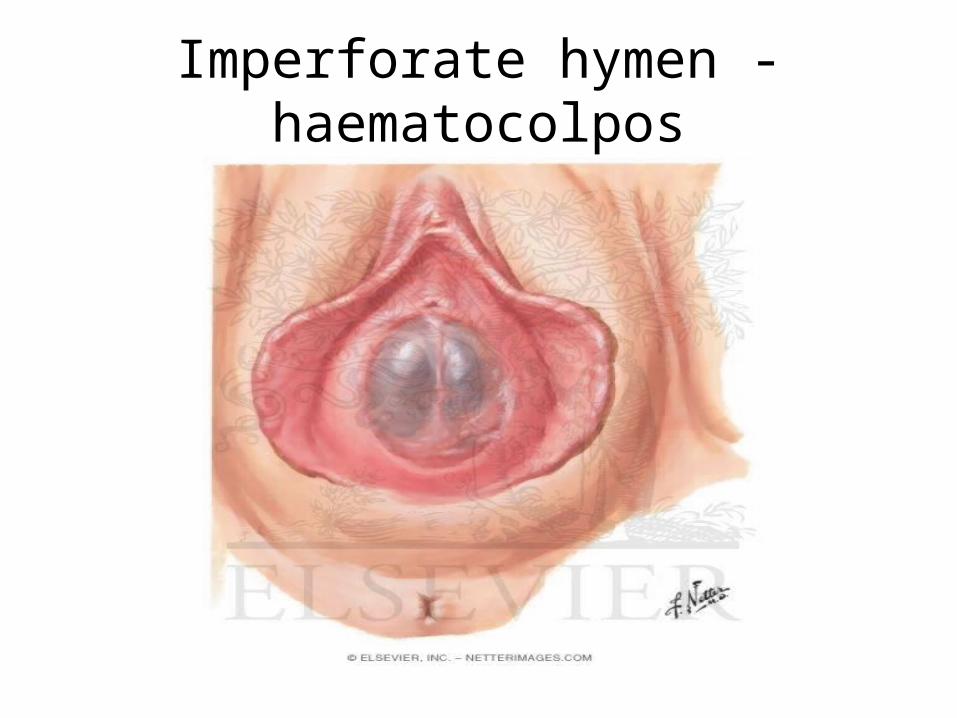
Imperforate hymen - haematocolpos
Management - Young women
• Small, simple, asymptomatic – leave alone and rescan 3 months later
• Complex – ovarian cystectomy or oopherectomy
• MDT involvement if any suspicious features
Management – older women
• Complex in older women – MDT involvement Further imaging Tumour markers TAH/BSO
• Simple, < 5cm, normal tumour markers – consider conservative management with repeat scan.
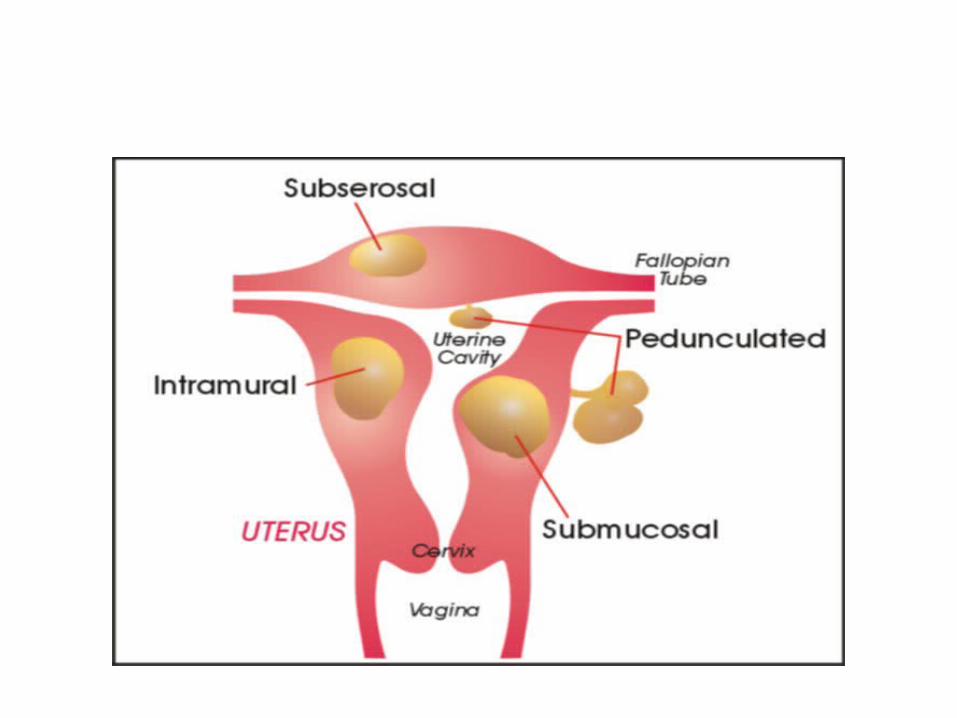
Fibroids
• Present in 25% of women
• More common: perimenopausal family history Afro-Caribbean women
• Sub-mucosal, subserosal, intramural
Ovarian Cancer• 5th, 6th and 7th decades
• Risk inversely correlated with parity.
• Genetic component – BRCA1 & BRCA2
• Presents late – usually with a mass or ascites
• No premalignant stage - screening
• Borderline tumours
• Epithelial
• Sex cord/stromal
• Germ cell
• Metastases
Epithelial Tumours
Serous• Most common• Bilateral in 50%• Cystic and solid components
Mucinous• Contain mucinous fluid• Pseudmyxoma peritonei
Endometrioid• 30% have a coexistent endometrial CA
Sex Cord/Stromal TumoursGranulosa Cell• Secrete oestrogen – IMB or PMB
Fibroma• Usually unilateral• Meig’s Syndrome
Sertoli/Leydig Cell• Young women (20’s)• Secrete testosterone
Germ Cell TumoursDysgerminoma• Ages 10 – 30• May be raised hCG
Yolk sac tumour• Young women• Raised alphafetoprotein, normal hCG
Choriocarcinoma• Secrete hCG• Do not respond to chemotherapy
Teratoma• Usually benign -all 3 embryonic germ layers
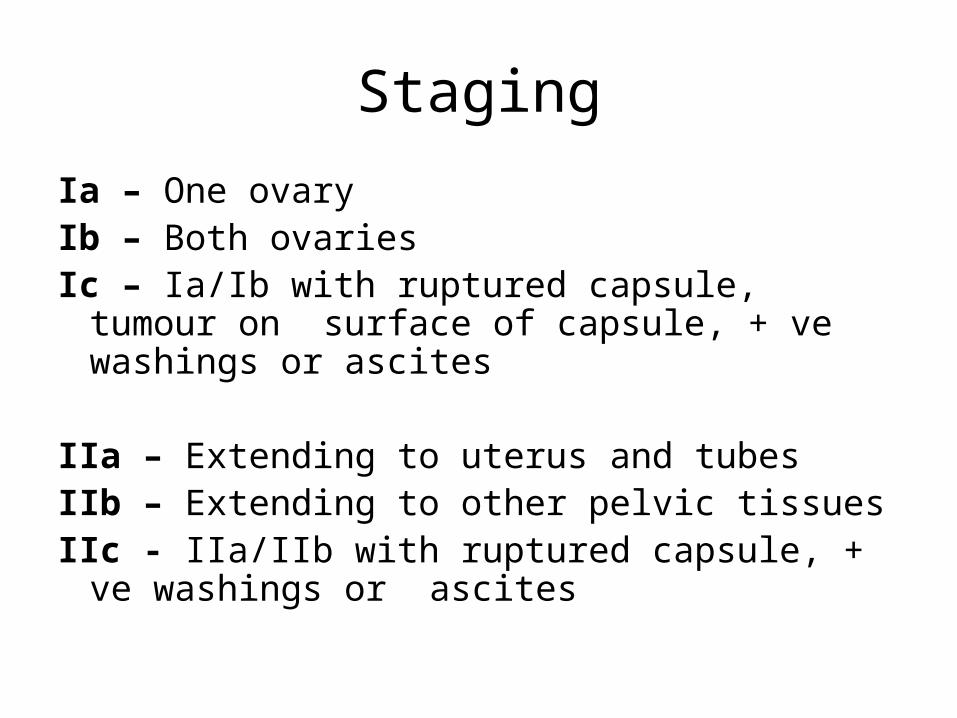
Staging
Ia – One ovaryIb – Both ovariesIc – Ia/Ib with ruptured capsule, tumour on surface
of capsule, + ve washings or ascites
IIa – Extending to uterus and tubesIIb – Extending to other pelvic tissuesIIc - IIa/IIb with ruptured capsule, + ve washings or
ascites
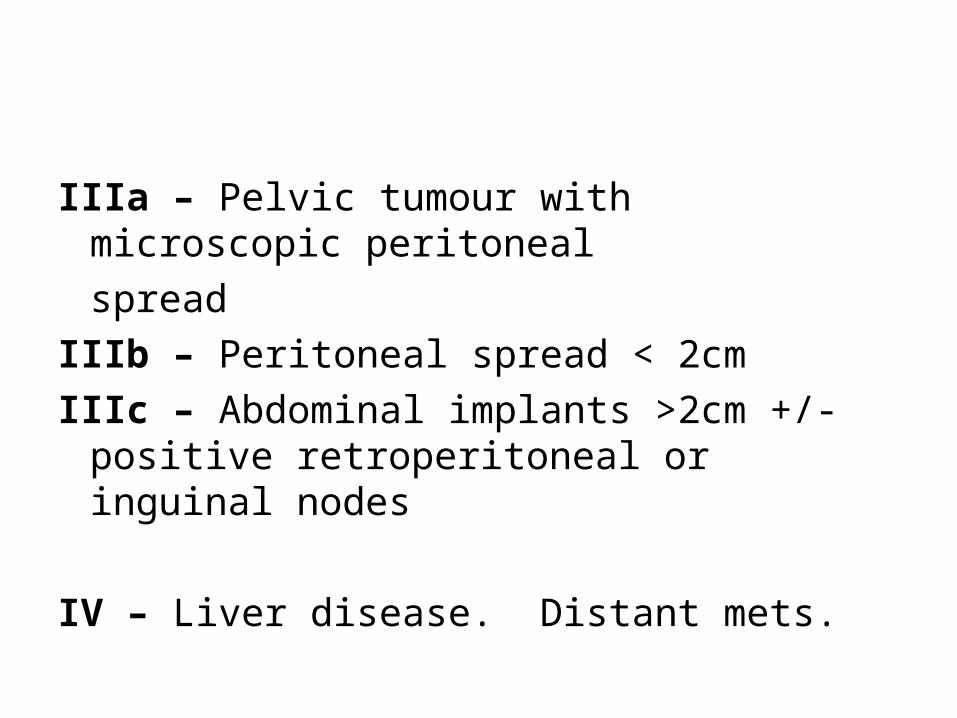
IIIa – Pelvic tumour with microscopic peritonealspread
IIIb – Peritoneal spread < 2cmIIIc – Abdominal implants >2cm +/- positive
retroperitoneal or inguinal nodes
IV – Liver disease. Distant mets.
Management• CT & CXR
• Baseline tumour markers
• Surgical staging
• Debulking surgery & adjuvant chemo
• Neoadjuvant chemo with interval debulking


















