Peer Learning Group 2 (November 2010)

of 28
-
Upload
cmiller5143 -
Category
Documents
-
view
212 -
download
0
Transcript of Peer Learning Group 2 (November 2010)
-
8/8/2019 Peer Learning Group 2 (November 2010)
1/28
HRSA State Health Access ProgramPeer Learning Group 2: Benefit Design
1
STATE HEALTH ACCESS PROGRAM:Peer Learning Group 2
Benefit Design
Supported by the Health Resources and Services Administration
Thursday, November 18, 2010This event will begin at 2:00pm Eastern
Please hold until Anne Gauthier starts the conferenceThe audio portion of this web event can be accessed by dialing
866.740.1260Access Code: 5077588
*6 to Mute* 7 to Unmute
-
8/8/2019 Peer Learning Group 2 (November 2010)
2/28
HRSA State Health Access ProgramPeer Learning Group 2: Benefit Design
2
Todays Agenda
2:00-2:05 Introduction and Roll Call (Anne Gauthier, NASHP)
2:05-2:40States are invited to briefly update on benefit design issuesrelated to their SHAP grants and new provisions for the ACA.
Auto-assigned states: ME, MN, NC, OR, TX, VA, WA, WI, WV
2:40-3:10 Presentation from Jeanene Smith in Oregon about value-basedinsurance design
3:10-3:15 Final Questions and Wrap Up
-
8/8/2019 Peer Learning Group 2 (November 2010)
3/28
HRSA State Health Access ProgramPeer Learning Group 2: Benefit Design
3
Benefit Design:State Updates
-
8/8/2019 Peer Learning Group 2 (November 2010)
4/28
HRSA State Health Access ProgramPeer Learning Group 2: Benefit Design
4
State Spotlight: Oregon
-
8/8/2019 Peer Learning Group 2 (November 2010)
5/28
5
Oregon s Value-Based Essential BenefitPackage
& Initial Pricing Estimates
Jeanene Smith, MD, MPHOffice for Oregon Health Policy and Research
November 2010
-
8/8/2019 Peer Learning Group 2 (November 2010)
6/28
6
Typical Insurance Benefit Package Design
Portion a person pays (cost-sharing) is applied:By specific service orBy the location wherethe service is providedMay tier prescriptiondrugs by generic versusbrand name
Service
HMO-type
plan
PPO-type
planH ospital $50/day up
to $250/stay15%
coinsurance
Office Visit $5-$20copay
15%coinsurance
Ambulance $75 copay 15%coinsurance
EmergencyRoom
$75 copay 15%coinsurance
-
8/8/2019 Peer Learning Group 2 (November 2010)
7/28
7
Value-Based Essential Benefits Package(VBEBP)
Value-based services, basic diagnostic, comfort care No/low cost share For prevention/chronic disease management
Tiered coinsurance based on best evidence
Goal is to steer patients towards more valuable and cost-effective services
Evidence-based drug formulary
-
8/8/2019 Peer Learning Group 2 (November 2010)
8/28
8
20 Sets of Value-Based Services in the EssentialBenefit Package
Value-based services are medications, tests, or treatments thatare highly effective, low cost, and have a lot of evidencesupporting their use
Most of these services should be provided via outpatient care ideally in a patient-centered primary care home
These services should be offered at NO cost to patients (nocopays or coinsurance) in order to encourage use of theseservices given their high level of benefit
Goal: Have these services used as much as possible
-
8/8/2019 Peer Learning Group 2 (November 2010)
9/28
9
VBEBP sT iered Benefits for Other Services:Cost Sharing Applied Based On Best Evidence
T ier I :Lower cost shareH
ighly effective care for severe chronicdisease and life-threatening illness & injuryExamples:
Emergent dental careH ead injuriesAppendicitisH eart attackThird degree burnsKidney failureRheumatoid arthritisLow birth weight
T ier II:Next level of cost share
Effective care of other chronic diseaseand life-threatening illness & injuryExamples:
Breast cancerBladder infectionsCOPD/emphysemaMultiple sclerosisPost-Traumatic Stress DisorderAttention Deficit DisorderEpilepsyGlaucoma
-
8/8/2019 Peer Learning Group 2 (November 2010)
10/28
10
VBEBP sT iered Benefits:Cost Sharing Applied Based On Best Evidence
T ier III:3 rd level of cost shareEffective care for non-life-threatening
illness & injuryExamples:
Broken armEar/sinus infectionsDenturesKidney stonesH
erniated diskRefluxMigrainesFibroidsCataractsObsessive-Compulsive Disorder
T ier IV:Highest level of cost shareLess effective care and care for self-
limited illness and minor illness & injuryExamples:
ColdChronic low back painSprained ankleCracked rib
Seasonal allergiesAcneViral sore throatTension headacheDental implantsLiver transplant for cancer
-
8/8/2019 Peer Learning Group 2 (November 2010)
11/28
11
How The VBEBP ComparesOregon s Health Leadership
Council s DesignVBEBP
Categories WithNo Cost Share
T ier 1
Tests and treatments for six chronicdiseases (asthma, CAD, C H F, COPD,depression, diabetes)Annual exam & Preventive screeningsImmunizations
Value-Based Services
Same plus coverage for 14 additionalconditions/chronic diseases (e.g.,ETOH Tx, bipolar Dz, H TN, lipids,maternity/newborn)Basic diagnostics & Comfort care
Next Level (s) of Cost- sharing
T ier 2
Standard medical product design Portion of hospital services Portion of outpatient services Portion of Emergency Room cost
T iers I-III
Encourages care in primary careTiered cost sharing bycondition/associated service basedon evidence
Highest CostSharing or NotCovered
T ier 3H ave higher cost sharing
Preference sensitive treatmentsComplex outpatient imaging
Excluded Services
T ier IV less effective/self-limitingOther
Excluded conditions (no coverage)Discretionary Services (separatebenefit limit)
-
8/8/2019 Peer Learning Group 2 (November 2010)
12/28
12
Preliminary Actuarial Analysis
Using earlier model developed for initial EBP design
based on Medicaid dataApplied for first time to commercial dataOEBB claims data from ODS plansOH A/DH S Actuarial Services Unit significant
programming and data handlingAnalysis begins with ODS 200 9 claims
-
8/8/2019 Peer Learning Group 2 (November 2010)
13/28
13
Preliminary Actuarial Analysis (2)
Costs are trended to 2010
Categorizing four tiers relatively straightforwardJudgment, rules of thumb, and many assumptions totease out first estimates for value-based services, 2 visitsper year, diagnostic servicesMacro comparison of 4 Plan Designs ODS Plan 7 (200 9 ) baseline ODS Plan 7 (2010), H ealth Leadership Council, Value Based
Essential Benefits Package
-
8/8/2019 Peer Learning Group 2 (November 2010)
14/28
14
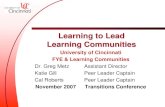
Asthma as a Value-Based Service
-15%
-10%
-5%
0%
5%
10%
15%
20%
25%
30%
35%
40%
% Change
Ma in tenan ceRX Poss e ssio n ER Use Hospit a liza tions
-
8/8/2019 Peer Learning Group 2 (November 2010)
15/28
15
Asthma as a Value-Based Service(In Terms of Cost)
Overall cost goes down $0.29 P MPM
Cost to plan goes up $1.11 P MPM
Member saves (on average) $1.40
Members with asthma save (on average) $14.00 per month out-of-pocket
-
8/8/2019 Peer Learning Group 2 (November 2010)
16/28
16
Actuarial Analysis Assumptions, Approach,Qualifiers
All work is based on PMPM costs, separate utilization
and unit costs were not availableSome copays were converted to coinsurance for pricingCollaboration effort to ballpark impacts of plan design especially on value based services (room for additionalresearch and improvement)This version includes medical and Rx, but not vision ordental
-
8/8/2019 Peer Learning Group 2 (November 2010)
17/28
17
Example Used: OEBB Plan 7Medical has $500 deductible/$2,500 OOP max20% coinsurance for most other servicesPreventive services have no cost sharingDrug has $1,000 OOP max$5 copay for generic, $25 copay for preferred brand, 50% copayfor nonpreferredStarting with 2010-2011 added some value-based features added additional cost tier ($500 copays for certain procedures) added $100 copays for sleep studies, MRI, PET scans , CT scans No incentive tier like some of the other OEBB plans Rx value copay level added ($4/$ 8 instead of flat $5)
-
8/8/2019 Peer Learning Group 2 (November 2010)
18/28
18
Example Used: HLC Version of OEBB Plan 7
Begin with OEBB 2009 planAdd 6 Value Based ServicesAdd Preference Sensitive Tier
-
8/8/2019 Peer Learning Group 2 (November 2010)
19/28
19
Example Used: VBEBP Version of Plan 7
Medical $500 deductible, $2,500 OOP
Rx separate $1,000 OOPValue based services, 2 visits, comfort care at 0%Tiered coinsurance 10%/20%/30%/50%
Tiered coinsurance 0%/20%/50% for diagnosticRX plan $0/$5/$25/50% with shared $1,000 OOP
-
8/8/2019 Peer Learning Group 2 (November 2010)
20/28
20
Preliminary PMPM Cost Comparison
$-
$50
$100
$150
$200
$250
$300
$350
$400
2009 2010
OEBB 7 2009
OEBB 7 2010
HLC
VBEBP
-
8/8/2019 Peer Learning Group 2 (November 2010)
21/28
21
Preliminary PMPM Cost Comparison
$ 00
$ 50
$400
$450
$500
$550
$600
2009 2010 2011 2012 201 2014
O EBB 7O EBB 7
L
VBEB P
-
8/8/2019 Peer Learning Group 2 (November 2010)
22/28
22
Let s ReviewAll these plan designs are making efforts to encouragethe best care, and discourage ineffective careCarrots are more expensive than sticks and savings calculations are more challenging
VBEBP has largest spread between the best and the
rest and so is a way to dampen across-the-board cuts
-
8/8/2019 Peer Learning Group 2 (November 2010)
23/28
23
G oing ForwardIf the VBEBP concepts are attractive
more work on each VBS to weigh costs and savingsof each intervention additional modeling work to tighten up all aspects and, of course, continue work with all stakeholders
-
8/8/2019 Peer Learning Group 2 (November 2010)
24/28
24
Focus G roup Progress Report
Conducting focus groups for insurers, providers,large and small employers, consumers (insured and
uninsured)Conducting in Portland, Southern Oregon, CentralOregon and Eastern Oregon as well as onlineH olding 15 in-person focus groups and 4 onlinediscussions. Groups are mostly complete.Results will be available for the November meeting
-
8/8/2019 Peer Learning Group 2 (November 2010)
25/28
25
VBEBP: SummaryFurthers Oregon s Triple Aim Improves health without increasing overall costs
Improves quality by encouraging most effective services Controls costs by discouraging less effective servicesPreliminary analysis suggests an impact on costcurveAnalysis of longer term impact will continueVBEBP offers a way to soften the impact of budgetcost sharing increasesIn an exchange, VBEBP would ensure that moremoney is steered toward higher-value care
-
8/8/2019 Peer Learning Group 2 (November 2010)
26/28
26
Questions?
-
8/8/2019 Peer Learning Group 2 (November 2010)
27/28
HRSA State Health Access ProgramPeer Learning Group 2: Benefit Design
MaxEnroll: Self-Assessment Toolkit Launch! Thursday November 18, 2010 4:00pm ES T
SHAP National Webinar: S tate-to-State Exchange on HealthInsurance Exchanges
Monday November 22, 2010 1:30pm EST
Next PLG: Enrollment and retention
Tuesday December 7, 2010 2:00 pm EST
All-Grantee MeetingWashington, DC, January 12-1 3 , 2010
27
Save the Date!
-
8/8/2019 Peer Learning Group 2 (November 2010)
28/28
HRSA State Health Access ProgramPeer Learning Group 2: Benefit Design
28
Thank You!
Anne Gauthier Sonya Schwartz Kathy WitgertSenior Fellow Program Director Program [email protected] [email protected] [email protected]
Chris Cantrell Christina MillerResearch Assistant Research [email protected] [email protected]
NASHP s SHAPTeamP lease feel free to contact us with any questions.
www.nashp.org