Pediatrics in Review 1992 Bithoney 453 9

of 9
-
Upload
aina-nurlaila -
Category
Documents
-
view
213 -
download
0
Transcript of Pediatrics in Review 1992 Bithoney 453 9
-
8/11/2019 Pediatrics in Review 1992 Bithoney 453 9
1/9
DOI: 10.1542/pir.13-12-4531992;13;453Pediatrics in Review
William G. Bithoney, Howard Dubowitz and Harwood EganFailure to Thrive/Growth Deficiency
http://pedsinreview.aappublications.org/content/13/12/453the World Wide Web at:
The online version of this article, along with updated information and services, is located on
Print ISSN: 0191-9601.Village, Illinois, 60007. Copyright 1992 by the American Academy of Pediatrics. All rights reserved.
trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Groveandpublication, it has been published continuously since 1979. Pediatrics in Review is owned, published,
Pediatrics in Review is the official journal of the American Academy of Pediatrics. A monthly
at Indonesia:AAP Sponsored on September 16, 2014http://pedsinreview.aappublications.org/Downloaded from at Indonesia:AAP Sponsored on September 16, 2014http://pedsinreview.aappublications.org/Downloaded from
http://pedsinreview.aappublications.org/content/13/12/453http://pedsinreview.aappublications.org/content/13/12/453http://pedsinreview.aappublications.org/content/13/12/453http://pedsinreview.aappublications.org/http://pedsinreview.aappublications.org/http://pedsinreview.aappublications.org/http://pedsinreview.aappublications.org/http://pedsinreview.aappublications.org/http://pedsinreview.aappublications.org/http://pedsinreview.aappublications.org/http://pedsinreview.aappublications.org/content/13/12/453 -
8/11/2019 Pediatrics in Review 1992 Bithoney 453 9
2/9
F O CU S Q UE S T IO N S
1 . W hy is an understand ing of th e
concep ts
o f g ro wth
fa ilu re In in -
fan ts and youn g ch ildren im po r-
tan t?
2 . W hat fa ctors ar e comm on to poor
grow th and deve lopm en t o f In -
fan ts regard less o f th e specific
cause?
3 . W hat s tep s shou ld be fo llow ed to
enab le the ped ia tr ic ian to under -
stand th e reasons fo r grow th d e fi-
c ien cy in a ch ild ?
4 . W hat a re the var ious fac to rs th at
m ay in terac t to resu lt In grow th
de f ic iency?
5
H ow m ay grow th d efic ien cy b e
m a na ge d s uc ce ss fu ll y?
RT I LE
P ed ia tr ics in R eview V oL 3 N o 2 D e cem b er
1992
45 3
Fa ilu re to T hrive /G row th
Def ic iency
W illia m G . B ith o n e y , M D , H ow a rd D u b o w itz , M D , a n d
H a rw o o d E g a n , M D
Def in i t ion
CLA SS IF ICA T ION AND TYPO LOGY
A ltho ugh the d iag nos is o f fa ilu re to
th riv e FTT ) is m ad e freq uen tly ,
bo th th e m ean ing o f the te rm and its
va lue as a d iag nos is rem a in deba ta -
b le . B ecause any se rio us d isea se can
cause g row th fa ilu re , the te rm FTF
has little d iagn ostic use fu lness. C la s-
sicab ly , the etio lo gy of FV F h as been
d iv ided in to o rgan ic and nonorg an ic
types, w ith n onorgan ic FTT d efin ed
as g row th d efic iency w ith ou t a d iag -
no sab le m ed ical e tio log y and o rgan ic
FTF d efined a s growth fa ilu re cau sed
by a specif ic m ed ica l illne ss . A num -
be r o f au th o rs have q uestioned the
ad eq uacy of th is d icho tom ous v iew ,
sugg esting the n eed fo r a th ird ca te -
go ry : m ixed e tio lo gy . In th is
gro up of ch ild ren , ch ro n ic , m ild
p ro b lem s, such a s re cu rren t o titis
m ed ia in con ce rt w ith behav io ra l
prob lem s, resu lt in abe rran t b eh av -
io rs , su ch as d iff icu lt tem peram en t,
A ssistan t P ro fes sor
of
Ped ia trics,
Harvard
Med ica l S cho o l; S en ior A s soc ia te in
M ed ic in e , C h i ldren s H osp ita 4
Boston , M A.
tA ss ista n t P ro fe sso r o f P ed ia trics , U n iver sity
o f M aryla nd Schoo l o f M ed ic in e , Ba ltim ore ,
M D ; D irec tor , C h ild P ro te c tio n P rog ium ,
U n iver sity o f M a ryland H osp ita l, B a ltim ore ,
M D
Ins tru cto r in P ed ia tr ics, H arvard M ed ica l
S cho o l; A ssis tan t in P ed ia trics, M assach use tts
G ene ra l H osp ita l Bos to n , M A .
s le ep d iso rd ers , and a lte red eat ing
b eh av io r, w h ich to ge the r im p air
g row th .
Even in ca ses in w h ich th e
growth de fic iency is p rim arily du e to
o rgan ic o r n on organ ic cause s, the
p rob lem s seen in the ch ild ren a re
o ften m ultip le eg , in fan ts w ho have
card ia c fa ilu re a lso have feed in g d is -
o rd ers) . G iv en the m ultip le con trib u -
to ry fac to rs to FTT and the la ck o f
d iag no s tic sp ecific ity o f the te rm , w e
r ecommend
th a t i t b e ab an doned in
favo r o f the te rm grow th d efi-
ciency ,
w hich d esc ribe s the p re sen -
ta tio n o f th is en t ity : A n unde rw eigh t,
o ften s tu n ted , un de rno u rish ed ch ild .
T his te rm avo ids any in ap propriate
su ggestion o f d iag nostic spec ific ity .
A f t e r th e e tio log y of the FTF is d iag -
n osed , the ch ild sh ou ld be refe rred to
as on e su ffe r ing from a specif ic d is-
o rde r eg , an o ppos itio na l fe ed ing
d iso rd er resu l ting in un de rnu tritio n
ra the r than n onorgan ic F IT o r hepa -
titis a ssoc ia ted w ith u nde rnu tr ition ) .
D IAGNOST IC CR ITER IA
A lth ou gh th ere a re d iscrepanc ie s in
th e d iagn os tic c rite ria fo r g row th d e-
fic iency , the term ty p ic al ly is used to
describe infants an d
young ch ild ren
whose w e igh t is p ers is ten tly b elow
th e 5 th pe rcen tile fo r age , on s tan -
d ard ized g row th ch arts , in the ab -
sen ce o f constitu tiona l de lay . G row th
d efic iency du e to n u trition al m ad e-
q uacy is de fined th rou gh su ch an th ro -
pom etr ic m easu rem en ts a s w eig h t fo r
age , he ig h t fo r ag e, and w e ig h t fo r
he igh t .
W e igh t an d he igh t fo r age sho u ld
be cha rted b y u s ing the N ationa l
C en ter fo r H ea lth S tatis tic s g row th
ch arts , w h ich are b o th g en de r-sp e -
c ific and no rm ed to be rac ia l ly
rep re sen ta tive o f the po pu la t ion o f
th e U n ited S tates . T h e W orld H ea lth
O rg an iza tio n h as re com m end ed th a t
th ese cha rts be u sed as an in terna -
tio na l s tan da rd fo r a ll ch ild ren ,
rega rd less o f ra ce . In g en era l, the
fin d ing o f b ow w e ig h t fo r ag e a lon e
-
8/11/2019 Pediatrics in Review 1992 Bithoney 453 9
3/9
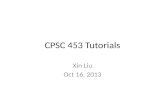
F IGURE. Tanner-Whitehouse char t.
To use
the chart, firs: find
th e
childs height and then
fo l low
the curve until you reach the childs age. Next, p la c e a nder from this point a l o n g t he h or i zo nt al
line a cr oss th e m idd le of the cha rt to the r i g h t side of the c ha rt. N o t e the po in t wh er e th is lin e
c r os ses th e ver tica l lin e of th e mean p a r e n ta l h e igh t and r e c o r d the per cen tile of t he c hi ld s
heigh t g iven mean parental height. R e pr in te d with pennission from Tanner I M G old ste in H
Whitehouse Rh . Standards fo r c hild re ns height a t a g es 2 to 9 ye a r s a l low in g for h eig h t of
parents. A rch D is Child 1 9 7 0 ; 4 5 : 7 5 5
45 4
P e dia tr ic s in Review V oL 13 N o 12 D ec em be r 1992
G R O W T H
ND
D E V E L O P M E N T
a ilu r t o T h rIv
months. In approaching grow th defi-
c iency , the physic ian must be aw are
that the overwhe lm ing preponderance
o f case s seen in the outpatient setting
are w ithout org anic il lne ss. Prev ious
data suggesting that organic illness
caused a high proportion of case s
w ere based on ho spitaliz ed patients
w ho w ere severe cases and no t repre-
sentative o f all children w ho are
growth-defic ient.
P a t h o g e n e s i s
Inadequate nutritio n is central to the
deve lopment o f g row th de fic it. Every
child w ho fails to thrive e ither has
not taken, has no t been offe red, or
has not re tained adequate calorie s to
meet his or her nutritio nal needs
g iv en his or her m edical s tatus . The
ev aluation of pathog enesis in grow th
de fic iency invo lv es the asse ssment o f
risk facto rs that predispo se to inade -
q uate n utri ti on .
N O N O R G A N IC R I S K FA C T O R S
Determ ination o f nonorganic risk
requires as ses sment o f four areas o f
functioning : temperament, interac -
tio n, and feeding behav ior in the
child and psycho soc ial s tre sso rs in
the parents . One must g ather infor-
matio n concerning these issue s in
fam ily interv iew s , o bservatio ns o f
fe eding and play , and care ful dev el-
o pmental assessment. Typical pat-
terns o f risk inc lude : 1 ) a difficult,
s ickly child, an iso lated, ov er-
w helm ed mother, and a father w ho is
emo tio nally unavailable fo r suppo rt;
2 a d iso r d er ed f eed in g sit u a t io n r e -
subting in inadequate calo ric intake o r
re tentio n; 3 ) lim ited interaction dur-
ing feeding ; and 4 ) a so cial env iron-
m ent o f s tress or poverty . These
infants and children are described as
le tharg ic , pass iv e , and immature de -
ve lopmentally and physically . A ffe c-
tive w ithdraw al and negative
affe ctive communications in both
caretaker and child are common. A
spectrum o f behav ioral difficultie s in
grow th defic iency ultim ately create s
t h e p er cep t ion o f a b u r d en som e
child. This spectrum inc ludes prob-
lem atic eating behav iors , poor state
contro l, de fiance, s leeple ssnes s, and
problems of e lim ination. The fam ilies
o f these infants o ften are so c iably iso -
lated and ov erw helm ed and bess ver-
bal than comparison fam ilie s . How -
ev er, the se fam ilies do not have a
higher inc idence o f o vert psy chopath-
o lo gy than those o f comparison
subjects.
TRANSACTIONAL M O D E L
Central to the deve lopment o f grow th
de fic iency is the re lationship be tw een
parental problems and tho se o f the
child and his or her env ironment.
The transac tional model sug ge sts that
ne ither the child nor the env ironment
alone de term ines the childs dev e lop-
mental outcome; rather, each affe c ts
and is affec ted by the o ther. Thus,
once an abnormal feeding pattern is
deve loped, the child may become
malnourished, anem ic, and irritable .
These changes are as soc iated w ith
structural, biomedical alterations in
the child (Table 1 ). The child then
beg ins to interact even more abno r-
mabby w ith his o r her caretaker, re-
subting in perpe tuation of the cy cle o f
irritability , ano re xia, and abn orm al
sleeping . It is the robe of the clinician
to alter this downwardly progressive
spiral. A bnormalities o f attachment,
autonomy, se lf-regulatio n, and sepa-
ration all have been described.
T o ca ll t h is p r o cess sim p ly m a t e r -
nab deprivatio n is an ov ers im plifica-
tion of e tio log y . Only in a mino rity
o f case s is this ex trem e parental be-
hav io r found. M ore commonly , par-
ents m isinterpre t the infants cues o f
hunger o r do not understand the nu-
tritio nab needs of their child. In som e
cases , o verdibutio n o f formula, w hich
has been shown to re late to both pov -
erty
and
poor
educatio n, is responsi-
ble for the
poor
growth.
ORGAN IC RISK F A C T O R S
Organic conditions that can cause a
predilectio n tow ard grow th deficiency
inc lude mino r cong enital anomalie s ,
prenatal and po stnatal m alnutritio n,
m edically com plicated prem aturity ,
and ongo ing medical conditions (eg ,
anem ia and bead po isoning ).
M ultiple m iscellaneous patte rns o f
defo rm ity are assoc iated w ith short
stature and decreased w eight (eg ,
ante ve rte d no strils , m ic ro ce phaly ).
Such dy smorphic feature s pro v ide
c lues to management. Fe tal alcoho l
syndrome and o ther in utero tox ic ex -
posure s resulting in alte red g row th
patterns also are o f interest (eg , fetal
hydanto in syndrome , maternal c iga-
re tte s m ok in g) .
Infants suffe ring fro m intrauterine
g row th re tardation due to poor mater-
nal nutritio n during pregnancy , con-
g enital infec tio ns , o r inadequate
placentatio n are born small for ge sta-
at Indonesia:AAP Sponsored on September 16, 2014http://pedsinreview.aappublications.org/Downloaded from
http://pedsinreview.aappublications.org/http://pedsinreview.aappublications.org/http://pedsinreview.aappublications.org/http://pedsinreview.aappublications.org/ -
8/11/2019 Pediatrics in Review 1992 Bithoney 453 9
4/9
T a b le 1 . M ed ic a l A b n o rm alitie s A s s o c i a t e d with G r o w t h
Def ic iency
Elevated aspartate am ino transferase
Elev ated abanine amino transferase
Anemia
Iro n de fi ci enc y
Z inc de fic ie nc y
Lead poisoning
D ecreased brain w eight
D ecre ase d neuro pib { 1 76 }
D epre ssed monamine ox idase ac tiv ity resulting in decreased central nerv ous
sy ste m se ro to nin, no re pine phrine
Im paire d im munity
Mababsorption
Apparent renal tubular acido sis
D ecreased grow th hormone
D ecreased thy ro id ho rmone
D ecreased somatomedin C
The num ber
o f c el l -t o -c el l
connections
or
synapses in the ce ntra l nerv ous sys tem
T a b le 2 . G o m e z C rite ria fo r C la s s ify in g
Malnut r l t lon
S e v e r i t y o f
P E R C E N T M E D IA N W EIG H T /A G E
G R A D E O F
M A L N U T R I T I O N
Weight
90 -i
10 o f 5 0 th percentile (m edian) no rmal
We ight 7 5 % -8 5 % o f 5 0 th percentile I mild
Weight 60 -74 o f i deal body w e ight II moderate
We ight