Pediatrics 1981 Gunn 61 7
9
1981;67;61 Pediatrics Tania Gunn, Elena R. Reece, Katherine Metrakos and Eleanor Colle Depressed T Cells Following Neonatal Steroid Treatment http://pediatrics.aappublications.org/content/67/1/61 the World Wide Web at: The online version of this article, along with updated information and services, is located on ISSN: 0031-4005. Online ISSN: 1098-4275. Print Illinois, 60007. Copyright © 1981 by the American Academy of Pediatrics. All rights reserved. by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, it has been published continuously since 1948. PEDIATRICS is owned, published, and trademarked PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly publication, at Indonesia:AAP Sponsored on April 10, 2014 pediatrics.aappublications.org Downloaded from at Indonesia:AAP Sponsored on April 10, 2014 pediatrics.aappublications.org Downloaded from
-
Upload
marlon-soselisa -
Category
Documents
-
view
219 -
download
0
Transcript of Pediatrics 1981 Gunn 61 7

1981;67;61PediatricsTania Gunn, Elena R. Reece, Katherine Metrakos and Eleanor Colle
Depressed T Cells Following Neonatal Steroid Treatment
http://pediatrics.aappublications.org/content/67/1/61
the World Wide Web at: The online version of this article, along with updated information and services, is located on
ISSN: 0031-4005. Online ISSN: 1098-4275.PrintIllinois, 60007. Copyright © 1981 by the American Academy of Pediatrics. All rights reserved.
by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village,it has been published continuously since 1948. PEDIATRICS is owned, published, and trademarked PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly publication,
at Indonesia:AAP Sponsored on April 10, 2014pediatrics.aappublications.orgDownloaded from at Indonesia:AAP Sponsored on April 10, 2014pediatrics.aappublications.orgDownloaded from

PEDIATRICS Vol. 67 No. 1 January 1981 61
Depressed T Cells Following Neonatal SteroidTreatment
Tania Gunn, MD, Elena R. Reece, MD, Katherine Metrakos, MD, and
Eleanor Colle, MD
From the Departments of Neonatology, Clinical Immunology, Electroencephalographyand Endocrinology, McGill University, and Montreal Children ‘s Hospital ResearchInstitute, Montreal
ABSTRACT. Forty-four patients received two doses of12.5 mg/kg of hydrocortisone or placebo on the first dayof life in attempted therapy for respiratory distress syn-
drome. Follow-up studies were performed on survivors at5 years of age in ten steroid-treated and seven placebo-treated respiratory distress syndrome subjects. Therewere no significant differences in growth, inteffigence
tests, or neurologic examinations in the patients assessed.Abnormal EEGs are present in both groups. Immunologictests showed no differences in lymphocyte counts, im-munoglobulin levels, diphtheria and tetanus antibody
titers, or complement components. Diminished percent-ages of T lymphocytes were found in steroid patients(53%) compared to control subjects (69%). There were
also increased percentages of lymphocytes with C3 recep-
tors in steroid patients (20.1%) compared to control pa-tients (13.8%). Episodes of otitis and/or pneumonia were
documented in eight of 1 1 steroid-treated patients be-tween the ages of 1 and 5 years, compared to two of sevenpatients in the placebo group in the same time period. Itis concluded that large doses of steroids on the first dayof life may induce lasting immunologic abnormalities andmay predispose to an increased incidence of infections.Pediatrics 67:61-67, 1981; corticosteroids, T cells, respi-ratory distress syndrome, neonates.
The short history of neonatal medicine is replete
with therapeutic misadventures. Any new pharma-
cologic regimen must be carefully evaluated for
both unexpected side effects and long-term seque-lae.
Received for publication Sep 26, 1978; accepted July 6, 1980.Read in part at the 48th Annual Meeting of the Society forPediatric Research, New York, April 26-28, 1978.Reprint requests to (ERR.) Department of Clinical Immunol-ogy, Montreal Children’s Hospital, Montreal, Quebec H3H 1P3.
Dr Gunn’s present address: St Helen’s Hospital, Auckland, NewZealand.PEDIATRICS (ISSN 0031 4005). Copyright © 1981 by theAmerican Academy of Pediatrics.
The efficacy of glucocorticoid treatment in accel-
erating the rate of lung development in late fetal
life has been shown by numerous animalt3 and
human studies.4 Potential toxicity for the fetus and
newborn infant may be inferred from the late effects
of neonatally administered corticoids found in ani-
mal studies. These studies have been reviewed re-
cently,5 and effects include impaired central ner-
vous system development71’ diminished placental
growth,’2 thymolymphatic cellular depletion,7t�6
lasting impairment of immunologic responsive-
ness,8”6”7 runting similar to that seen in neonatal
thymectomy,’3’�2#{176} and decreased life span with in-
creased infections.’8
In 1971 a controlled trial using postnatal hydro-
cortisone in pharmacologic doses for infants with
the respiratory distress syndrome was carried out
in the neonatal intensive care unit of the Montreal
Children’s Hospital and showed no benefit to the
steroid-treated infants.2’ Blood levels of cortico-
steroids which exceeded 500 mg/100 ml in a few
infants were found in the steroid-treated group.
Pathologic findings from the infants who died in
the neonatal period showed a significant association
between intraventncular hemorrhage and steroid
treatment.22
Follow-up studies of the infants who survived for
the first year of life showed a trend toward an
increased incidence of neurologic and encephalo-
graphic abnormalities and a significant difference
in motor development in the steroid-treated infants
at 1 year of age.23
This paper presents continued follow-up investi-
gation of the children from the same study.
PATIENTS AND METHODS
Of the original 44 patients admitted to the study,
22 received 12.5 mg/kg of hydrocortisone in two
at Indonesia:AAP Sponsored on April 10, 2014pediatrics.aappublications.orgDownloaded from

62 DEPRESSED T CELLS FOLLOWING NEONATAL STEROID TREATMENT
doses 12 hours apart in the first day of life and 22
received placebo. The neonatal courses of the two
groups were similar. Fourteen infants in each group
survived the neonatal period and 12 infants in each
group were available for study at 1 year of age.
These children have been followed at yearly in-
tervals in the neonatal follow-up clinic with records
of interim infections, measurements of height,
weight, and head circumference, and neurologic and
developmental examinations.
At 4 years of age 12 children from the steroid
group and ten of the placebo group were still fol-
lowed in the clinic. Of the 12 surviving placebo-
treated children who were evaluated at 1 year of
age, ten were studied completely for four years but
only seven were still available for study at 5 years
of age. At this time weight index and height index
were calculated for each child from the expected
date of delivery and the formula: weight (height)
index = weight (height)/age24 with percentiles from
the Stuart grid25 and age from estimated date of
conception. The head circumferences were plotted
on the Nelihaus grid.26
The children were retested with psychometric
evaluations using the Wechsler Preschool and Pri-
mary Scale of Intelligence (WPPSI),27 and Bender-
Gestalt, scored according to Koppitz,� or Rutger’s
A Drawing Age?� Electroencephalograms were re-
peated and were interpreted without knowledge of
steroid treatment status. Each abnormal tracing
was classified according to severity and the abnor-
mality described as, focal, paroxysmal, asymmetri-
cal, or epileptiform.
Immune competence was reassessed at 5 years of
age. Total lymphocyte counts were estimated from
the peripheral white blood cell and differential
counts. Levels of the complement components C3
and C4 were determined by radial immunodiffusion
using commercial plates. Ci-esterase inhibitor and
Clq levels were estimated by Ouchterlony double
diffusion. Assessments of B-cell function included
protein electrophoresis, determinations of IgG, IgA,
1gM, and IgD using commercial plates and IgE by
paper radioimmunosorbent test (PRIST, Pharma-
cia). Antibodies to tetanus and diphtheria were
measured by hemagglutination. Cell-mediated im-
munity was assessed by intradermal delayed skin
tests using dermatophytin, purified protein denva-
tive, Candida, streptokinase, and streptodornase
(Varidase), and histoplasmin or tetanus toxoid. T-
and B-cell quantitation was performed utilizing
mononuclear cells separated from heparimzed
whole blood by Ficoll-Hypaque density gradient
centrifugation.3#{176} The cell suspension was washed in
medium 199 and incubated with latex particles for
one hour at 37 C.3’ Monocytes ingesting latex were
not counted when lymphocyte subpopulations were
quantitated. This incubation also allowed labile
membrane immunoglobulin to elute from cells with
Fc receptors.32 T lymphocytes (E-RFC) were iden-
tified by the formation of rosettes with sheep red
cells.33 Receptors for the third component of com-
plement (C3) were detected by the adherence of
fluoresceinated Salmonella typhi, sensitized with
human complement, to lymphocytes.� Fc receptors
were determined by rosette formation of lympho-
cytes with human type 0 Rh+ red cells sensitized
with Ripley anti-CD antiserum.� Surface mem-
brane immunoglubulin (SmIG) was detected with
fluoresceinated antisera, both polyvalent and spe-
cific for individual heavy and light chains.36 All
studies were performed without knowledge of the
patients’ treatment status.
RESULTS
Of the 12 surviving children who had received
hydrocortisone and were evaluated at 1 year of age,
1 1 were studied completely for five years. Reports,
including neurologic evaluation were obtained from
another hospital for one other boy who is retarded,
hyperactive, and mute with moderate spastic diple-
gia. This boy probably had an intracranial hemor-
rhage in the neonatal period. The 1 1 other steroid-
treated and seven placebo-treated children studied
at 5 to 6 years of age had normal neurologic exam-
inations.
Mean weight and height indices and head circum-
ferences are shown in Table 1. All measurements
for both groups are between the 25th and 50th
percentiles and are not significantly different. The
mean heights and weights of the parents (fathers:
173 ± 8 cm, 77 ± 10 kg; mothers:160 ± 7 cm, 52 ±
7 kg) were similar to the Canadian average.37
Table 2 shows the results of psychometric testing.
The mean IQ was 100.7 ± 10.8 in the steroid group
and 108 ± 1 1.3 in the control group; these scores
are not significantly different nor are the mean
verbal or performance scores from the WPPSI. The
mean Rutger or Bender-Gestalt scores also show no
significant differences between the two groups. The
socioeconomic level was similar in the two groups.23
Not all of the children had started school yet. One
child in the placebo group has a history of poor
writing and poor fine motor coordination in school.
One child in the steroid group has both emotional
and learning problems, but two of his older brothers
also have severe learning problems.
EEG abnormalities are seen in both groups and
are shown in Table 3. One child in the steroid group
who has an active epileptogenic disturbance has
had no seizures. One child in the placebo group,
whose parents refused an EEG, has had a febrile
convulsion.
at Indonesia:AAP Sponsored on April 10, 2014pediatrics.aappublications.orgDownloaded from

TABLE 1 . Growth at 1 and 4 Years of Age in Steroid-Treated and Control Patients*
ARTICLES 63
-- Patients Weight Index Height Index Head Circumference
1 year of age
Steroid-treated (12)t 0.93 ± 0.27 0.97 ± 0.18 47.2 ± 1.0Control (12) 0.98 ± 0.4 0.99 ± 0.18 46.6 ± 1.5
4 years of ageSteroid-treated (12) 0.91 ± 0.23 0.90 ± 0.15 51.5 ± 1.1Control (10) 0.97 ± 0.25 0.93 ± 0.14 51.3 ± 1.7
* Values are mean number (±1 SD).
t Number of children in each group is shown in parentheses.
TABLE 2. Psychometric Testing�WPPSI* in Steroid-Treated and Control Patients
Patients Full IQ Scores Verbal Performance Perceptual
Steroid-treated (10) 107.1 ± 10.8 101 104 2.5 moControl (7) 108.2 ± 11.3 105 109 4.0 mo
S Wechsler Preschool and Primary Scale of Intelligence.
TABLE 3. Electroencephalograms in Steroid-Treated and Control Patients
. - - RefusedPatients Epileptogen,c Paroxysmal Irregular Test Normal
Steroid-treated (10) 2 0 1 1 6
Control (7) 0 1 3 2* 1
* One febrile convulsion.
IMMUNOLOGIC DATA
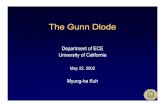
The results of immunologic testing are shown in
Table 4 and the Figure. There were no significant
differences in total lymphocyte counts, levels of
immunoglobulins, diphtheria and tetanus titers, or
complement components in the two groups. All
children had at least one positive delayed skin test.
Patients who had received steroids had a signifi-
cantly lower percentage of E-RFC than the control
group: 53% and 69%, respectively (P < .0005). In
some patients decreased E-RFC percentages were
associated with higher percentages of cells with C3
receptors (20. 1%) than observed in the adult or
control groups (10.4% and 13.8%, respectively, P <
.025) . No significant differences were observed in
percentages of cells with surface immunoglobulins
or Fc receptors.The number of infections between 1 and 5 years
of age was greater in the steroid group with eight of
11 patients having otitis and/or x-ray proven pneu-
monia compared to only two of seven patients in
the control group having otitis (Table 5). One child
in each group has had asthmatic attacks.
DISCUSSION
Although this follow-up study was designed to
address the major categories of long-term sequelae
reported in animals given neonatal steroids, it was
surprising to the authors to find diminished per-
centages of E-RFC at 5 years of age in children who
had received steroids on the first day of life. Man,
along with monkeys and guinea pigs, has been con-
sidered relatively resistant to steroid effects on the
immune system. Claman et al� evaluated steroid-
induced thymocyte lysis in humans, mice, and
guinea pigs and found human thymocytes relatively
resistant to this treatment. However, the thymo-
cytes of the youngest subject studied (age 11
months) demonstrated greater susceptibility to lysis
than thymocytes of older subjects. Reduction in
thymic size with oral steroid administration has
also been demonstrated radiologically in human
neonates.39 Evaluation of cardiothymic/thoracic ra-
tios immediately after birth in these infants and in
those who received prenatal steroids 40,41 revealed
a slightly more rapid decline in cardiothymic/tho-
racic ratios in postnatally steroid-treated infants
compared to those given placebo, while in prena-
tally treated infants the cardiothymic/thoracic ra-
tio was greater in patients who developed respira-
tory distress syndrome, but no effect of steroids was
found.Human and animal studies have shown diverse
effects of glucocorticoids on blood leukocyte kinet-
ics and function. T-lymphocyte numbers and func-
tion are more susceptible to their effects than are B
lymphocytes, although many of the effects on cell-
mediated immune functions are secondary to the
relative steroid sensitivity of the monocyte-macro-
phage system.42 It is thought that T cells develop
resistance to functional effects of steroids, in part
at Indonesia:AAP Sponsored on April 10, 2014pediatrics.aappublications.orgDownloaded from

because of maturational changes in the thymus43’ �
� and the differentiating effects ofthymic hormones,45
� 0 � and in part because of further differentiation after
E! � � exposure to antigen.46 In mature mice, thymectomyii or cortisone administration leads to no detectable
long-term effects.47 Conversely, low concentrations
.5 � � of steroids in vitro have been shown to enhance
� � � 0 � thymocyte differentiation rather than to cause cy-:�. : .� � ,:� totoxicity,48 and glucocorticoid antagonists interfere� � 0 with the normal ontogeny of cell-mediated immune
function.49
�c � The long-term implications of the immunologic
� :g � � findings in these patients are not readily apparentC,, �; � C\t as various disorders are associated with diminished
numbers of T cells, including immunodeficiency
states, autoimmune disorders, malignancies, and
� Lt� Lt� acute infections. A null population is suggested by� � �;; � �; � the failure to identify large percentages of the cells
-� - � - � from several steroid-treated children by the tech-
niques utilized. That the association of diminished
E-RFC and elevated numbers of cells with comple-
� �. � � � ment receptors may indicate an early T cell popu-� � � ,:� ;� lation is supported by a recent report that comple-
ment receptors may be a marker of early T cells in
�. � man.�#{176}Additionally young mice injected with cor-.2� � � � � tisone demonstrate a relative enrichment of C3L) � - 2� receptor-bearing thymocytes.5’
� The increased incidence of bronchopneumonia
.� � and otitis media in the children who received hy-
� � c� � � � drocortisone was, again, unexpected. Elucidation of-� - � ? � g � whether this was a chance occurence, as the num-
� bers of children in each group are small and the
� - incidence of childhood infections is widely variable,
-� � � � � or secondary to the therapy depends on further.� .� � � :� � � careful follow-up of these children and others who
� ,� V V receive steroids at an early age.
� There were no differences in height, weight, or� .� � � head circumference at 1 year or 4 years of age
.� � � � c�1 � �i between corticosteroid-treated children and the
� � � � control group. There were also no significant differ-
.� ences in the results of psychometric testing or in
�c � the general behavior of the children at 5 years of
� � � � � �2 � age. School performance wifi be evaluated as theE� � � � S� “ � children progress through school..�c � The differences in motor skills found at 1 year by
-� = Fitzhardinge et al23 in the steroid-treated group
� c� � � � were not apparent at 5 years of age. The results of
� .� � � � the mean performance and verbal scores were not
: � � significantly different in the two groups. No differ-� ences were apparent in testing for perceptual prob-
-� lems but the children are stifi too young for this to
� � be fully assessed. The EEG results showed an in-
.� ! crease in severe abnormalities in the steroid-treated“2W � � group, but one child in the control group had a
� :� 7 � � � � febrile convulsion, and an EEG was refused. There� � I>< � � I>< � were abnormal EEGs found in four of 12 steroid-I- &� L) treated children at 1 year of age. There are no
64 DEPRESSED T CELLS FOLLOWING NEONATAL STEROID TREATMENT
at Indonesia:AAP Sponsored on April 10, 2014pediatrics.aappublications.orgDownloaded from

E-RFC Fc C3 Sm IG
100 35
I � N.onatal steroid tr.at.d
90 30 � � 0 N.onatal controls
. 0 A � #{149}Adult controls-� 80
25E
�C;; 70 20 -
a #{149} 0� T oo#{224}
: 08� #{149} A� 60 A 15 #{149} I
.� � A #{149} I A0
�L - #{149}1 �0A: so A I AA . -
10 _00 � AA � 0AA0
. I 0 #{149}. 0 A&- A #{149}#{176}AA #{149} . 0 A
I 00 AA � � . A
I40 A
A o
I30 0 oA
p’0.0005 p< 0.025
Figure. Lymphocyte surface markers. Percentage of lymphocytes expressing Fc and C3receptors and bearing surface-membrane immunoglobulins represented on the same scale.
ARTICLES 65
TABLE 5. Infections Between the Ages of 1 and 5 Years in Steroid-Treated and ControlPatients
Steroid-tre
Control (7)
Patients
ated (11)
Pneumonia
3. . .
Otitis Media
62
Upper RespiratoryInfections Only
3
5
clinical effects correlated with these changes at this
time.
The children receiving steroids were all prema-
turely born. The mean plasma levels of cortisol
resulting were greater than 100 mg/100 ml for 48
hours following injection as compared with values
of 30 mg/100 ml for the stressed placebo-treated
infants. The most frequently used steroid prepara-
tions in the treatment of the fetus and newborn, at
this time, are dexamethasone and betamethasone
administered to the mother, often on a schedule
which requires weekly repetition of the dose. Data
on peak levels of the steroids measured following
birth of the infant52’� are difficult to compare with
those found in this study because of differences in
plasma protein and tissue binding, duration of ac-
tion, and variable estimates of comparable poten-
cies of various steroid analogues.
RELEVANCE
The finding of diminished T cells at 5 years of
age in children who received steroids on the first
day of life emphasizes the importance of ongoing
follow-up investigations to assess the long-term ef-
fects of steroids in infants who receive them at an
early age or prenatally. Since corticosteroid effects
in developing organisms vary depending on the age
of administration and dose administered, careful
stratification of study populations by gestational
age and steroid dosage should be a cardinal feature
of such studies.
SUMMARY
At 5 years of age ten children who received hy-
drocortisone on the first day of life in attempted
therapy of respiratory distress syndrome and seven
placebo-treated infants were assessed for growth,
psychometric testing, neurologic status, electroen-
cephalograms, immunologic status, and incidence
of infections. Diminished percentages of T cells
were found in children who had received steroids,
associated in some with increased percentages of
cells with complement receptors. There was also an
increased number of infections in steroid-treated
children. It is concluded that even brief therapy
with corticosteroids in infants may result in lasting
immunologic impairment.
at Indonesia:AAP Sponsored on April 10, 2014pediatrics.aappublications.orgDownloaded from

66 DEPRESSED T CELLS FOLLOWING NEONATAL STEROID TREATMENT
ACKNOWLEDGMENT
This work was supported by the Nathan Steinberg
Family Foundation.
REFERENCES
1. Liggins GC: Premature delivery of foetal lambs infused with
glucocorticoids. J Endocrinol 45:515, 19692. DeLemos TA, Shermetta DW, Knelson JH, et al: Accelera-
tion of appearance of pulmonary surfactant in the fetal lambby administration of corticosteroids. Am Rev Respir Dis 102:
459, 1970
3. Taeusch HW Jr, Heitner M, Avery ME: Acceleration of lungmaturation and increased survival in premature rabbits
treated with hydrocortisone. Am Rev Respir Dis 105:971,1972
4. Ballard PL, Ballard RA: Corticosteroids and respiratorydistress syndrome: Status 1979. Pediatrics 63:163, 1979
5_ Taeusch HW Jr: Glucocorticoid prophylaxis for respiratory
distress syndrome: A review of potential toxicity. J Pediatr87:617, 1975
6� Howard E, Granoff D: Increased voluntary running anddecreased motor coordination in mice after neonatal corti-
costeroid implantation. Exp Neurol 22:661, 19687. Schapiro 5: Neonatal cortisol administration: Effect on
growth, the adrenal gland and pituitary-adrenal response to
stress. Proc Soc Exp Biol Med 120:771, 19658. Schapiro S: Some physiological, biochemical and behavioral
consequences of neonatal hormone administration: Cortisol
and thyroxine. Gen Comp Endocrinol 10:214, 19689. Cotterrell M, Balaz R, Johnson AL: Corticosteroids on the
biochemical maturation of rat brain: Postnatal cell forma-
tion. J Neurochem 19:2151, 1972
10. Schapiro 5, Salas M, Vukovich K: Hormonal effects on
ontogeny of swimming ability in the rat: Assessment of
central nervous system development. Science 168: 147, 1970
1 1 . Howard E: Reduction in size and total DNA of cerebrum
and cerebellum in adult mice after corticosterone treatment
in infancy. Exp Neurol 22:191, 196812. Wellman K, Volk B: Fine structure changes in the rabbit
placenta induced by cortisone. Arch Pathol 94:147, 1972
13. Fachet �J, Palkovits M, Vallent K, et al: Effect of a singleglycocorticoid infection on the first day of life in rats. ActaEndocrinol 51:71, 1966
14. Lee RE, Domm LV: A histological and histochemical study
on the effects of adrenal cortical steroids in the fetal and
neonatal rat thymus. Anal Rec 157:105, 196715. Fein A, Ornoy A, Nebel L: Effects of cortisone on fetal and
neonatal thymo-lymphatic organs in rats. J Anal 117:223,
1974
16. Branceni D, Arnason B: Thymic involution and recovery:
Immune responsiveness and immunoglobulins after neonatal
prednisolone in rats. Immunology 10:35, 1966
17. Russell A, Ornoy A, Ritchie J, et al: Transplacental andneonatal effects of hypercorti.sonism in the rat in thymo-
lymphatic system differentiation and serum immunoglobulin
levels. Adu Exp Med Biol 27:257, 197218. Ulrich R, Levy L, Kasson B, et al: Developmental changes
of immunoglobulins in rats treated neonatally with hydro-
cortisone. Proc Soc Exp Biol Med 154:107, 197719. loachim HL: The cortisone induced wasting disease of new-
born rats: Histopathological and autoradiographic studies. JPathol 104:201, 1971
20. Schlesinger M, Mark R: Wasting disease induced in young
mice by cortisol acetate administration. Science 143:965,
1964
21. Baden M, Bauer CR, Colle E, et al: A controlled trial of
hydrocortisone therapy in infants with respiratory distress
syndrome. Pediatrics 50:526, 1972
22. Taeusch HW Jr, Wang NS, Baden M, et al: A controlled
trial of hydrocortisone therapy in infants with respiratory(listress syndrome. II. Pathology. Pediatrics 52:859, 1973
23. Fitzhardinge PM, Eisen A, Lejtenyi C, et al: Sequelae of
early steroid administration to the newborn infant. Pediat-rics 53:877, 1974
24. Drash A, Heese D, Brasel JA: in Cheek DB(ed): HumanGrowth. Philadelphia, Lea & Febiger, 1968, p 62
25. Stuart HC, Reed RB: Longitudinal studies of child health
and development. Pediatrics 24(suppl):875, 1959
26. Nellhaus G: Head circumference from birth to 18 years.
Pediatrics 41:106, 196827. WechslerPreschool and Primary Scale oflntelligence. New
York, The Psychological Corporation, 196728. Koppitz EM: The Bender Gestalt Test for Young Children.
New York, Grune & Stratton, mc, 1964
29. Yudin LW: The Rutger’s Drawing Test and intelligence: Apreliminary comparative study. Percept Mot Skill.s 24:1038,1967
30. B#{246}yumA: A one-stage procedure for isolation of granulo-cytes and lymphocytes from human blood: General sedimen-tation properties of white blood cells in a 1 g gravity field.
Scand J Clin Lab Invest 97(suppl):21, 1968
31. Cline MJ, Lehrer RI: Phagocytosis of human monocytes.Blood 32:423, 1968
32. Horwitz DA, Lobo P1: Characterization of two populations
of human lymphocytes bearing easily detectable surface
immunoglobulin. J Clin Invest 56:1464, 1975
33. Bach JF: Evaluation of T cells and thymic serum factors inman using the rosette technique. Transplant Rev 16:196,
1973
34. Gelfand JA, Fauci AS, Green I, et al: A simple method for
the determination of complement receptor-bearing mono-nuclear cells. J Immunol 116:595, 1976
35. Fr#{248}landSS, Wisl#{248}ffF, Michaelsen RE: Human lymphocyteswith receptors for IgG. A population of cells distinct from Tand B-lymphocytes. mt Arch Allergy Appl Immunol 47:124,
1974
36. Preudhomme JL, Labaume S: Immunofluorescent staining
of human lymphocytes for the detection of surface immu-noglobulins. Ann NY Acad Sci 254:254, 1975
37. Pett LB: A Canadian table of average weights. Can MedAssocJ73:12, 1955
38. Claman HN, Moorhead JW, Benner WH: Corticosteroidsand lymphoid cells in vitro. I. Hydrocortisone lysis of human,
guinea pig, and mouse thymus cells. J Lab Clin Med 78:499,1971
39. Caffey J, Silber R: Regrowth and overgrowth of the thymusafter atrophy induced by the oral administration of adreno-
corticosteroids of human infants. Pediatrics 26:762, 196040. Gewolb IH, Lebowitz RL, Taeusch HW Jr: Thymus size and
its relationship to the respiratory distress syndrome. J Pe-diatr95:108, 1979
41. Fletcher BD, Masson M, Lisbona A, et al: Thymic response
to endogenous and exogenous steroids in premature newborn
infants. JPediatr95:111, 1979
42. Paulo JE, Fauci AS: Mechanisms of glucocorticoid action
on immune process. Annu Rev Pharmacol Toxicol 19:179,
1979
43. Andersson B, Blomgren H: Evidence for a small pool of
immunocompetent cells in the mouse thymus. Its role in thehumoral antibody response against sheep erythrocytes, bo-vine serum albumin, ovalbumin and the NIP determinant.Cell Immunol 1:362, 1970
44. Cohen JJ, Claman HN: Thymus-marrow immunocompet-
ence. V. Hydrocortisone-resistant cells and processes in thehemolytic antibody response of mice. J Exp Med 133:1026,
1971
45. Trainin N, Levo Y, Rotter V: Resistance to hydrocortisone
conferred on thymocytes by a thymic humoral factor. Eur JImmunol 4:634, 1974
46. Segal 5, Cohen IR, Feldman M: Thymus-derived lym-
phoctes: Humoral and cellular reactions distinguished byhydrocortisone. Science 175:1126, 1972
47. Peter CP, Perkins EH, Peterson WJ, et al: The late effects
ofselected immunosuppressants on immunocompetence, dis-
ease incidence, and mean life-span. III. Disease incidence
and life expectancy, Mech Ageing Dec 4:251, 1975
at Indonesia:AAP Sponsored on April 10, 2014pediatrics.aappublications.orgDownloaded from

ARTICLES 67
48. Ritter MA: Embryonic mouse thymocyte development: En- of thymocytes bearing C3 receptors following cortisone in-
hancing effect of corticosterone at physiological leveLs. Im- volution. Cell Immunol 43:176, 1979
munology 33:241, 1977 52. Osathanondh R, Rulchinsky D, Kamali H, et al: Dexameth-
49. VanI)ijk H, Jacobse-Geels HEL: Evidence for the involve- asone levels in treated pregnant women and newborn infants.ment of corticosterone in the ontogeny of the cellular im- J Pediatr 90:617, 1977mune apparatus of the mouse. Immunology 35:637, 1978 53. Balard PL, Granberg P, Ballard RA: Glucocorticoid levels in
50. Stein H, M#{252}ller-Hermelink HK: Simultaneous presence of maternal and cord serum after prenatal dexamethasone ther-
receptors for complement and SRBC on human fetal thy- apy to prevent respiratory distress syndrome. J Clin Investmocytes. Br J Haematol 36:225, 1977 56:1548, 1975
51. Walia AS, Andersson B, Fuson EW, et al: The enrichment
THE SAD FATE OF DR MICHAEL UNDERWOOD’S WIDOWED DAUGHTER
The most advanced writer on diseases of children in the 18th century,
according to G. F. Still, was Michael Underwood.’ He was the first to describe
sclerema neonatorum, apneic attacks in the newborn, “malignant familial jaun-
dice” of the newborn, and the first to write about congenital heart disease of
children. His Treatise on the Diseases of Children (1784) passed through at
least 17 editions and remained in favor for more than 60 years; the last American
edition appeared in 1842.
Unfortunately, Underwood apparently received no royalties from his textbook
and died without being able to provide for his widowed daughter. Friends tried
to help her by putting together a book entitled Extracts from the Diary of the
Late Michael Underwood, M.D. (1823) that would then be sold to subscribers.
In the prospectus for this book Underwood’s friends poignantly described
their reasons for publishing this book as follows:
It is confidently hoped that the Friends of the late Dr Underwood, and more especiallythose in the Profession who are acquainted with the estimable works which he publishedon the “Diseases and Disorders of Children” &c. wifi feel an interest in the case of hiswidowed Daughter, who now stands in need of the benevolent exertions of her Friends.She is in her fiftieth year, and is borne down by an accumulation of troubles, arising
partly from the loss of relatives and friends, and partly from serious mental debility,which frequently incapacitates her for the humble and precarious employment ofneedlework, in which she is at other times engaged. Thus reduced, she has at lengthconsented to make an appeal to the liberality of her Friends and humbly to solicit theirkind support of the Publication now projected, which she hopes will enable her to raisea small sum to provide her with a few comforts in the decline of life. The situation of theapplicant is the more painful to her feelings from the recollection of those enjoyments,and even indulgences, which in the plenitude of her father’s fame, she had the happinessto experience.2
As far as I can determine, approximately 500 copies of the book were sold to
subscribers. I doubt whether the profit made from this sale was large enough to
really benefit Dr Underwood’s daughter.
Noted by T.E.C., Jr, MD
REFERENCES
1. Still GF: The History ofPaediatrics. London, Oxford University Press, 1931, pp 476-477.2. Extracts from the Diary of the Late Michael Underwood, M.D. London, Hatchard and Son,
1823.
at Indonesia:AAP Sponsored on April 10, 2014pediatrics.aappublications.orgDownloaded from

1981;67;61PediatricsTania Gunn, Elena R. Reece, Katherine Metrakos and Eleanor Colle
Depressed T Cells Following Neonatal Steroid Treatment
ServicesUpdated Information &
http://pediatrics.aappublications.org/content/67/1/61including high resolution figures, can be found at:
Permissions & Licensing
http://pediatrics.aappublications.org/site/misc/Permissions.xhtmlor in its entirety can be found online at: Information about reproducing this article in parts (figures, tables)
Reprints http://pediatrics.aappublications.org/site/misc/reprints.xhtml
Information about ordering reprints can be found online:
Online ISSN: 1098-4275.Copyright © 1981 by the American Academy of Pediatrics. All rights reserved. Print ISSN: 0031-4005. American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois, 60007.has been published continuously since 1948. PEDIATRICS is owned, published, and trademarked by the PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly publication, it
at Indonesia:AAP Sponsored on April 10, 2014pediatrics.aappublications.orgDownloaded from