Pediatric Trauma - Western University · Discuss the components of the primary survey in the...
61
Pediatric Trauma Sept 2nd, 2015 Patrick Murphy Neil Merritt
-
Upload
phungnguyet -
Category
Documents
-
view
215 -
download
0
Transcript of Pediatric Trauma - Western University · Discuss the components of the primary survey in the...
Pediatric Trauma
Sept 2nd, 2015
Patrick Murphy
Neil Merritt

Objectives

Objectives – Medical Expert 1. Describe the types of pediatric injuries sustained with a given mode of trauma, and
identify the most common injuries occurring in various age groupings.
2. Identify unique anatomic or physiologic differences in children, when compared to
adult patients.
3. Discuss the components of the primary survey in the pediatric trauma patient
4. Outline the secondary survey, and identify controversies in pediatric shock trauma
management
5. Differentiate between mild, moderate, and severe head injuries in children
Objectives – Medical Expert 6. Describe unique traumatic injuries to the spine that occur in children and
measures to treat these injuries
7. Differentiate the types of cardiothoracic trauma, and list appropriate management
of each type
8. Identify signs, symptoms, and management of pediatric abdominal and
genitourinary trauma
9. Recognize the risks and appropriate management of traumatic amputation and
soft tissue trauma in children
10. Recognize the risks and appropriate interventions in the management of
orthopedic pediatric trauma
Objectives - Collaborator 1. Understand the post injury components of care for pediatric trauma patients
2. Describe the levels of pediatric trauma care and how to prepare an ER for
treatment of the injured child
Objectives – Health Advocate 1. Describe the impact of pediatric trauma on Canadian society and healthcare.
2. Identify the importance of pain management with practical strategies for
managing pain in pediatric trauma patients
3. Outline the role of family centered care in pediatric trauma

Objectives - Scholar 1. Identify and understand the implications of one recent sentinel paper in pediatric
trauma care

Case 1

Patient LK 7 yo, biking and hit by car
Wearing a helmet
Unresponsive on arrival, tachypnea
with pale, dusky extremities
HR 144; RR 38; BP 84/60; GCS 5 (E =
1; V = 2; M = 2)
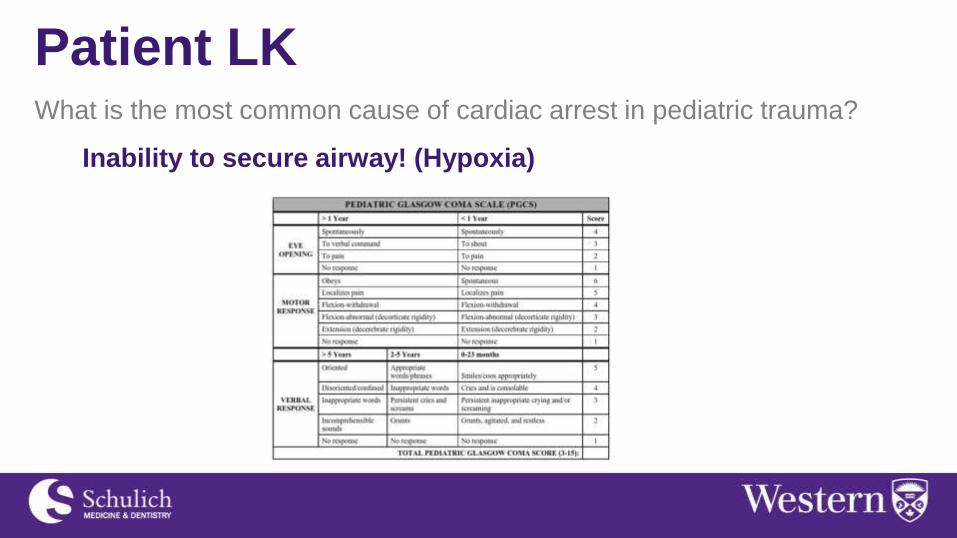
Patient LK What is the most common cause of cardiac arrest in pediatric trauma?
Inability to secure airway! (Hypoxia)
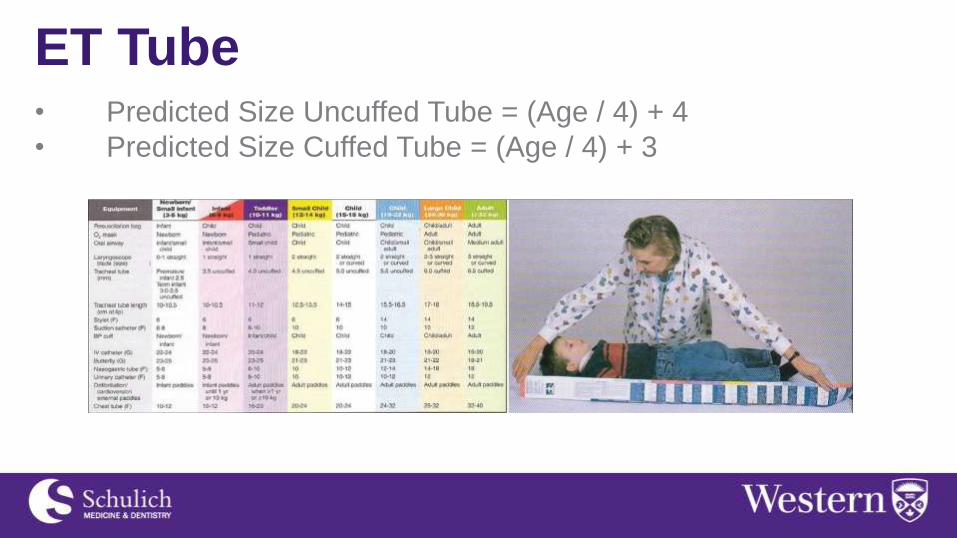
ET Tube • Predicted Size Uncuffed Tube = (Age / 4) + 4
• Predicted Size Cuffed Tube = (Age / 4) + 3
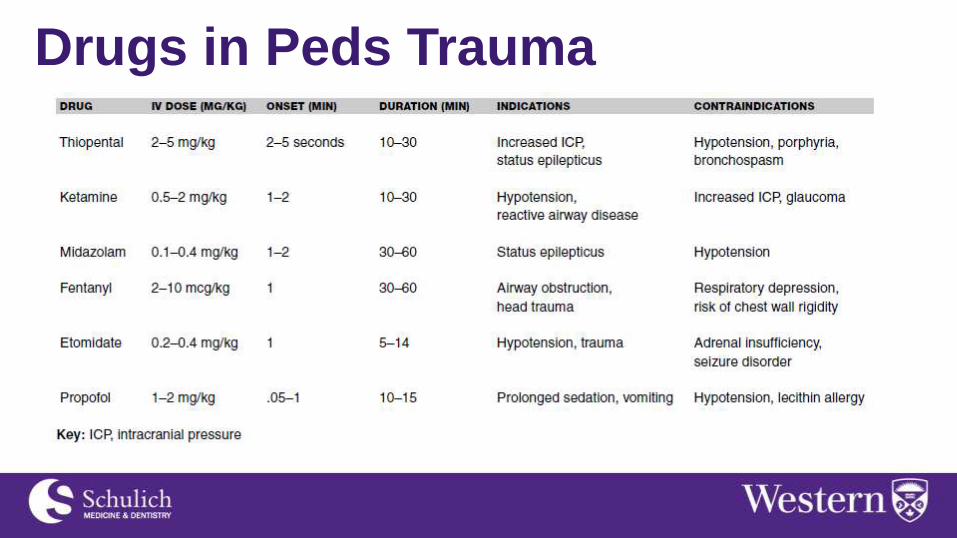
Drugs in Peds Trauma
Case 2

Patient BA 9 yo, unsupervised on ATV;
collisions with tree; no helmet
No LOC at scene
PMx: Fragile X Syndrome

Patient BA - Arrival C-Spine Collar
2IVs
HR 69; BP 123/58; RR 18; 100% NRB
O/E
Trachea Midline, GAEBL
Fast is Negative
GCS 8

Patient BA - Arrival Pan CT
Liver Lac
Right Epidural, left subdural, right
frontal bone #
To PCCU
Pediatric Trauma

Facts • 50% of childhood deaths result from preventable injury
• Injury prevention through awareness and increased
safety measures = 1/3 reduction in death from trauma in
Canada
• Seatbelts
• Vehicle Design
• Car seats

Mortality
Incident 1987 2004 Change
Motor vehicle crash
3,587 2,431 32%
Drowning 1,363 761 44%
Pedestrian injury
1,283 583 55%
Fire and/or burn injury
1,233 512 58%
Suffocation 690 963 28%
Falls 149 107 28%
Poisoning 100 86 14%
Firearm 247 63 74%

Etiology - Mortality
UNDER 1 1 to 4 5 to 9 10 to 14 15 to 19
Breathing (50%)
MVC (22%) MVC (60%) MVC (55%) MVC (70%)
MVC (18%) Drowning (20%)
Drowning/Fall/Flame
(18%)
Drowning (13%)
Poisoning (7%)
Drowning (15%)
Breathing (20%)
Breathing (5%)
Fall (7%) Drowning (6%)
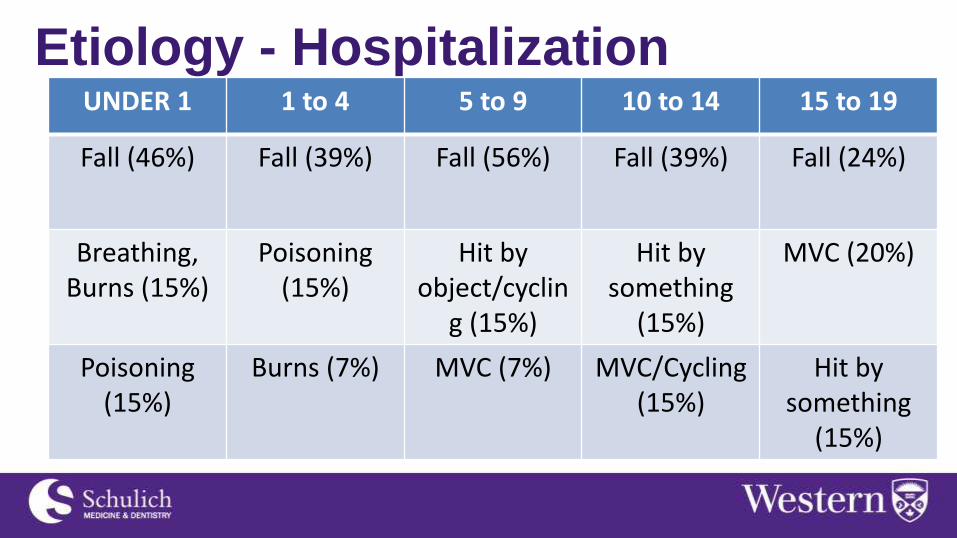
Etiology - Hospitalization
UNDER 1 1 to 4 5 to 9 10 to 14 15 to 19
Fall (46%) Fall (39%) Fall (56%) Fall (39%) Fall (24%)
Breathing, Burns (15%)
Poisoning (15%)
Hit by object/cyclin
g (15%)
Hit by something
(15%)
MVC (20%)
Poisoning (15%)
Burns (7%) MVC (7%) MVC/Cycling (15%)
Hit by something
(15%)
How are kids different?
ANATOMY

Airway • Compared to adult, 3 major differences
1) Smaller (Foreign bodies/teeth)
2) Larger tongue (risk of obstruction)
3) Epiglottis (project posterior)

Airway • Where is the narrowest point in the pediatric
airway?
• Cricoid ring
• Cuffed or uncuffed tube? Why?
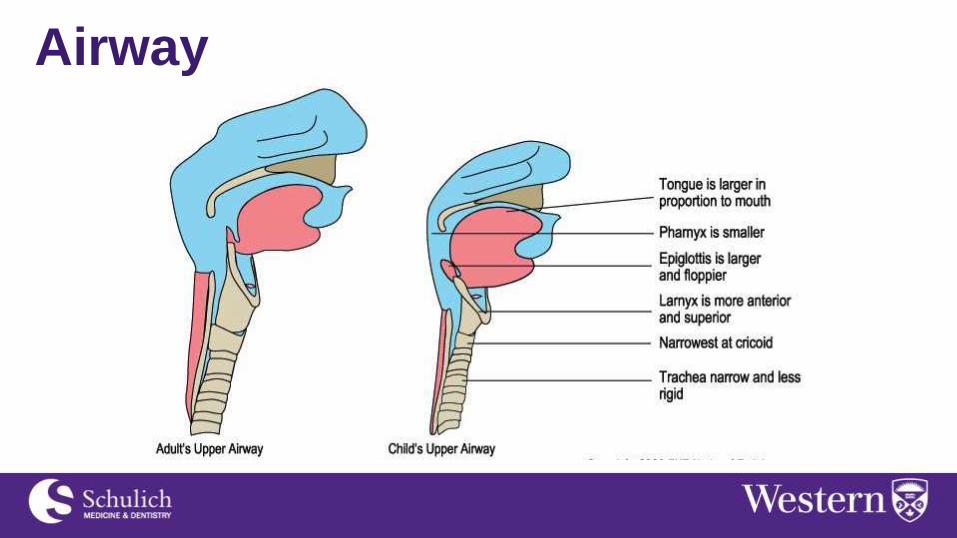
Airway

Breathing • Which way do the ribs move?
Horizontally
• More or less compliant than adult?
More!
Diaphragmatic Breathing • Infants and young children have very compliant
chest walls which explains intercostal retraction
in airway obstruction
• Need to decompress the stomach to reduce
pressure on diaphragm

Diaphragmatic Breathing

Summary
Anatomy PEDIATRIC ADULT
Tongue Large Normal
Epiglottis Shape Floppy, omega shaped Firm, flatter
Epiglottis Level Level of C3 - C4 Level of C5 - C6
Trachea Smaller, shorter Wider, longer
Larynx Shape Funnel shaped Column
Larynx Position Angles posteriorly away
from glottis
Straight up and down
Narrowest Point Sub-glottic region At level of Vocal cords
Lung Volume 250ml at birth 6000 ml as adult
Abdomen • Thin abdominal wall
• Which two organs are more likely to be injured in children
• Liver and Spleen
• Which organ is intra-abdominal in infants but not adults?
• Bladder
Bones • When do children reach skeletal maturity
• Post-puberty
• Why is this important
• Growth plate fractures
• Interpretation of X-Rays

Bones • What is a green stick fracture?
• Why do they occur in children and
not adults?
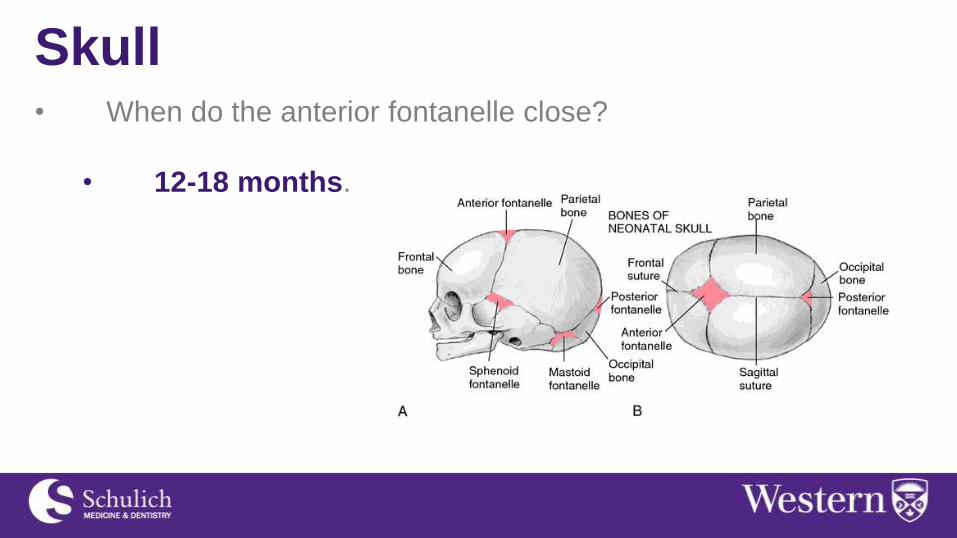
Skull • When do the anterior fontanelle close?
• 12-18 months.
General • Smaller size = more likelihood for multiple organ systems
injured
• Higher metabolic rate and larger surface area to body-mass
ratio = greater heat loss

How are kids different?
PHYSIOLOGY

Circulation • Blood volume is larger but absolute volume is smaller
• Small volume loss = significant % of total blood
volume
• Need to record even small volume loses you
might ignore in an adult
• SVR is lower

Circulation • Fixed Stroke Volume in infants
• Why is this important?
• Is hypotension an early or late sign?
• LATE!
• Best method is U/O
• 1-2 mL/kg/hr in children/infants

Normal Vitals
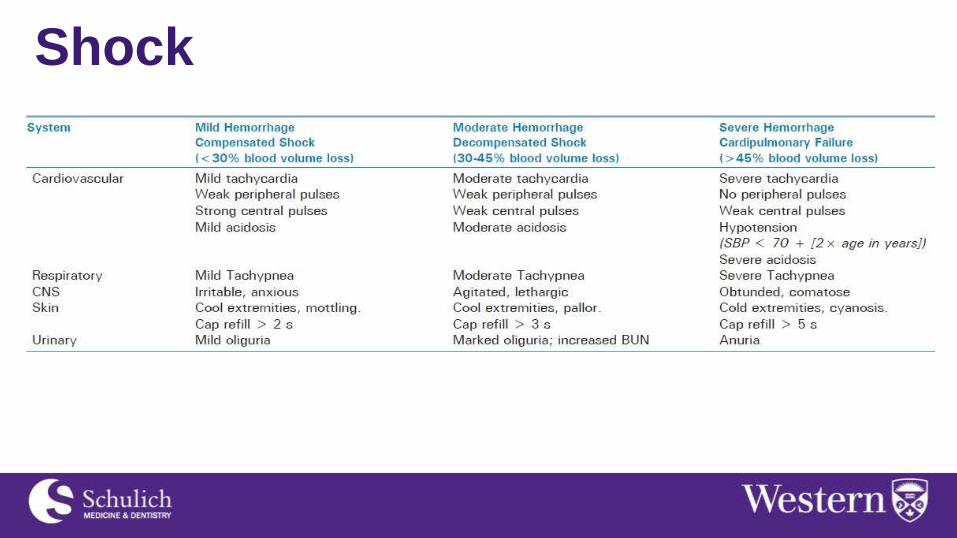
Shock
Access/Fluids • Typically more challenging in pediatrics
• I/O
• IV
• How much fluid to give? What kind?

Access/Fluids

Case 2

Patient HI 6 mo infant sitting in carrier on top
of a stroller
Fell approximately 3 ft to pavement
No loss of conscious, crying
HR 120; RR 18; BP 92/50
Swelling over right temporal region

Patient HI

Head/Spinal Injury

Head • Leading cause of death from trauma
• Significant lifelong disability
• >80% are mild TBI
• Classified similarly to adults
• Mild (Ped-GCS 13-15)
• Moderate (Ped-GCS 9-12)
• Severe (Ped-GCS <8)

Head - Management • Principles are same as adult
• Secure airway
• Avoid hypoxia – give O2
• Avoid hypotension
• Ensure adequate resuscitation
• ICP monitoring in those with severe head injury
• Correct raised ICP
• Hypertonic saline 0.1-1cc/kg
• Mannitol 0.25-1cc/kg
Spine • Very rare in children < 17 yo, prevalence < 5%
• C2 lesions in young, C4 in teen (A-O dislocation)
• Mechanism MVC in young, sports in teens
• SCIWORA – need high suspicion of injury (PH Exam)
• MRI Important
• Neurologic Recovery
• Likely better compared to adult population
• No evidence for hypothermia/steroids
Cardiothoracic
Thoracic • Much less common secondary to small size
• Approximately 6%, almost all blunt
• Highly fatal second only to head injury
• Male:Female 3:1 ratio
• Greater flexibility = pulmonary contusion of pneumatocele
without rib fractures
• Miss 30-40% of injuries on initial CXR
• Vast majority only require observation +/- chest tube

Thoracic – Hemo/Pneumothorax • Clinical findinds of a tension may be impressive (mobile
mediastinum)
• What size tube? How much output for OR?
• Nipple Level (R5/6); Do not use sharp trocar
Thoracic – Rib # • Marker of energy transfer OR child abuse (20% of all
thoracic trauma) – particularly in young (< 3 yo)
• 1st/2nd rib raise suspicion of vascular injury
• Management
• Analgesia (discussed later)
• Suspect pulmonary contusion if deteriorating

Abdominal
Abdominal – Solid Organ • 8-12% of pediatric trauma
• Similar to adults, spleen and liver most common
• Management largely Non-operative now (>90% success
even in high grade injuries)
• Management
• Non-operative
• Continued instability = OR – similar principles to adult,
damage control lap, control bleeding and pack

Abdominal – Solid Organ

Abdominal – Hollow Viscus • Crush, burst and sheer injuries
• Rapid contamination of abdominal cavity
• Frequent physical exam is more sensitive than CT
• Management
• Early recognition and repair are key
• High index of suspicion in unwell patient

Pain Management
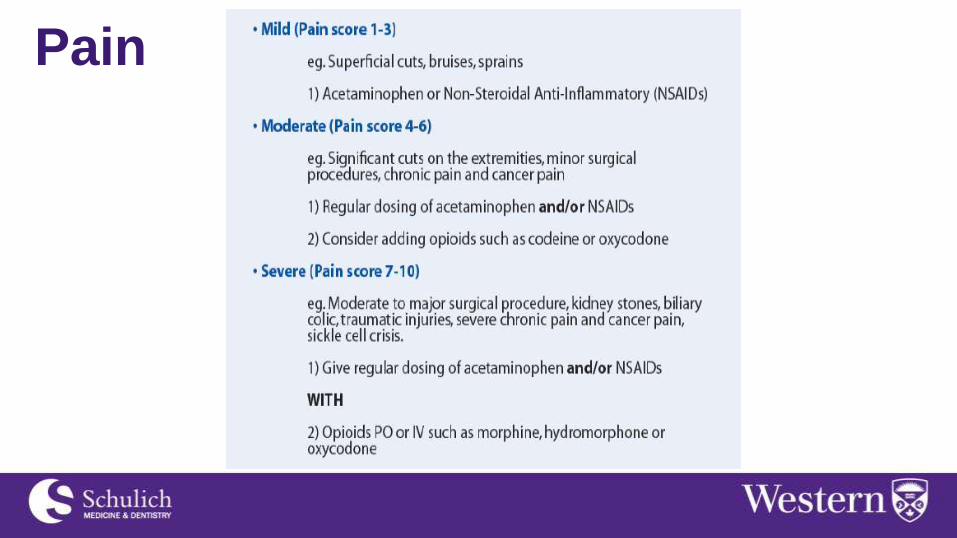
Pain

Pain

Pain Assess and adjust regularly, start with low doses. Multimodal
is key
MEAC = minimum effective analgesia concentration
Non-Pharmacologic
Breathing, distraction (movies, video games)

THANKS!!











![Trauma Reach Workshop - Pediatric Trauma.pptx [Read-Only]...Pediatric Trauma Trauma REACH Workshop May 5th, 2015 Tamer A. Ahmed, MD Pediatric Trauma Medical Director Upstate’s GolisanoChildren’s](https://static.fdocuments.us/doc/165x107/5fe9ec9ba1b3915c9800251e/trauma-reach-workshop-pediatric-read-only-pediatric-trauma-trauma-reach.jpg)