Pediatric Spastic Equinus Deformity - The Podiatry Institute
6
CHAPTER 5 Pediatric Spastic Equinus Deformity Stepben J. Miller, D. P A4. CEREBRAL PALSY The term "cerebral palsy," coined by William Osler in 1BB9 and also known as "static encephalopathy,,, refers to the symptom complex produced by a non-progressive central neryous system (CNS) iesion occurring during gestation or at birth, and resulting in some motor deficit. Cerebral palsy affects approximately 0.1 -0.20/o of all children, however, there is no familial or genetic inheritance pattern. There are approximately 2,500 new cere- bral palsy patients born each year, with an approximate total population of 1 million patients in the United States at any one time. The degree of functional impairment depends on the part of the brain which is damaged. There may be pyramidal (associated with the motor cor- tex) or extrapyramidal involvement. Spasticity occurs when the pre-motor cofiex is damaged, whereas flaccidity or atonia is present when the motor cortex is damaged. Extrapyramidal basal ganglia damage results in athetosis, while damage to the cerebellum results in ataxia. \7hen there is diffuse brain damage, it is manifested by various amounts of rigidity. This paper will focus on patients diagnosed with spastic cerebral palsy. Spasticity refers to a pattern of muscle hyperreflexia, hypertonicity, and clonus. The cause is brain damage which results in a reduction of inhibitory control from the CNS. This causes dysfunction of the gamma motor sys- tem with a subsequent increase in lower motor neuron impulse. Hence, spastic cerebral palsy is characteized by an increased stretch reflex medi- ated through the gamma motor neuron system. As a result, attempted movement of a muscle results in instant and various resistance. Since we are dealing with ambulatory spastic cerebral palsy, it is impofiant to understand the anatomic classification of this disorder, which depends on the limbs involved. Spastic monoplegia, a rare presentation, indicates one limb involvement only. Spastic paraplegia refers to involvement of the lower limbs only, whereas spastic diplegia indi- cates the lower limbs are involved to a greater degree than the upper extremities. Spastic quadri- plegia means that all four limbs are involved, whereas spastic hemiplegia involves the limbs on one side of the body only. SPASTIC EQTIINUS The most common spastic deformity in cerebral palsy is equinus, which involves contracture of the gastrocnemius or the gastrocnemius-soleus muscle tendon complex (triceps surae). It may be com- bined with an equinovalgus deformity of the foot when there is associated pronation due to spastic peroneal muscles, or equinovarus deformity when associated with over-activity or spasm of the tibialis posterior muscle. There are two types of equinus deformity. "Dynamic contracture" is due to marked hyper- tonicity of the triceps surae mechanism. Attempted passive stretch results in immediate resistance due to increased muscle tone. The muscle will ultimately yield to a sustained stretching force. "Myostatic contracture" occurs when the muscle becomes intrinsically, irreversibly shortened. No amount of stretching will produce any additional length without tissue damage. CLIMCAL ASSESSMENT OF CEREBRAL PALSY The initial assessment begins with an obseryation of the patient's daily activities. This will give a gen- eral idea of the intelligence level and physical capabilities of the patient. Pathologic reflexes seen in cerbral palsy include: Babinski's reflex, hyperac- tive tendon reflexes, and the neck-righting reflex. If these persist for greater than 20 weeks of age, the
Transcript of Pediatric Spastic Equinus Deformity - The Podiatry Institute
CHAPTER 5
Pediatric Spastic Equinus DeformityStepben J. Miller, D. P A4.
CEREBRAL PALSY
The term "cerebral palsy," coined by William Oslerin 1BB9 and also known as "static encephalopathy,,,refers to the symptom complex produced by anon-progressive central neryous system (CNS)iesion occurring during gestation or at birth, andresulting in some motor deficit. Cerebral palsyaffects approximately 0.1 -0.20/o of all children,however, there is no familial or genetic inheritancepattern. There are approximately 2,500 new cere-bral palsy patients born each year, with anapproximate total population of 1 million patientsin the United States at any one time.
The degree of functional impairment dependson the part of the brain which is damaged. Theremay be pyramidal (associated with the motor cor-tex) or extrapyramidal involvement. Spasticityoccurs when the pre-motor cofiex is damaged,whereas flaccidity or atonia is present when themotor cortex is damaged. Extrapyramidal basalganglia damage results in athetosis, while damageto the cerebellum results in ataxia. \7hen there isdiffuse brain damage, it is manifested by variousamounts of rigidity.
This paper will focus on patients diagnosedwith spastic cerebral palsy. Spasticity refers to apattern of muscle hyperreflexia, hypertonicity, andclonus. The cause is brain damage which results ina reduction of inhibitory control from the CNS.This causes dysfunction of the gamma motor sys-tem with a subsequent increase in lower motorneuron impulse. Hence, spastic cerebral palsy ischaracteized by an increased stretch reflex medi-ated through the gamma motor neuron system. Asa result, attempted movement of a muscle results ininstant and various resistance.
Since we are dealing with ambulatory spasticcerebral palsy, it is impofiant to understand theanatomic classification of this disorder, whichdepends on the limbs involved. Spastic monoplegia,
a rare presentation, indicates one limb involvementonly. Spastic paraplegia refers to involvement ofthe lower limbs only, whereas spastic diplegia indi-cates the lower limbs are involved to a greaterdegree than the upper extremities. Spastic quadri-plegia means that all four limbs are involved,whereas spastic hemiplegia involves the limbs onone side of the body only.
SPASTIC EQTIINUS
The most common spastic deformity in cerebralpalsy is equinus, which involves contracture of thegastrocnemius or the gastrocnemius-soleus muscletendon complex (triceps surae). It may be com-bined with an equinovalgus deformity of the footwhen there is associated pronation due to spasticperoneal muscles, or equinovarus deformity whenassociated with over-activity or spasm of the tibialisposterior muscle.
There are two types of equinus deformity."Dynamic contracture" is due to marked hyper-tonicity of the triceps surae mechanism. Attemptedpassive stretch results in immediate resistancedue to increased muscle tone. The muscle willultimately yield to a sustained stretching force."Myostatic contracture" occurs when the musclebecomes intrinsically, irreversibly shortened. Noamount of stretching will produce any additionallength without tissue damage.
CLIMCAL ASSESSMENT OFCEREBRAL PALSY
The initial assessment begins with an obseryationof the patient's daily activities. This will give a gen-eral idea of the intelligence level and physicalcapabilities of the patient. Pathologic reflexes seenin cerbral palsy include: Babinski's reflex, hyperac-tive tendon reflexes, and the neck-righting reflex. Ifthese persist for greater than 20 weeks of age, the
22 CI{APTER 5
prognosis for unsuppottive walking is poor.Examination of seven postural reflexes, as
outlined by Bleck, can help determine a patient'spotential for unassisted gait. These include:
1. Asymmetric tonic neck reflexes (ASTNR)
2. Neck-righting reflex3. Moro reflex4" Symmetric tonic neck reflex (TNR)
5. Parachute reaction6. Foot placement reaction7. Extensor thrust
If any one of these is still present at lwelvemonths or older, then the ambulatory prognosis is
guarded. If two abnormal reflexes are present, theprognosis is poor. It is also poor if there is a posi-tive parachute reaction (absence of protectiveresponse).
DIAGNOSIS OF SPASTIC EQUINIUS
Equinus is present when dorsiflexion of the foot at
the ankle is equal to or less than neutral (90
degrees), when the subtalar joint is held in a neu-tral position.
Initial evaiuation of the equinus deformityshould determine whether it is "primary" due tomuscle imbalance (usually spasticity of the tricepssurae or its components), or "secondary" toanother deformity such as hip or knee flexionl or aresult of "overflow." Overflow refers to the invol-untary activity of one muscle group caused by the
voluntary activity of another muscle group.Determining which components of the triceps
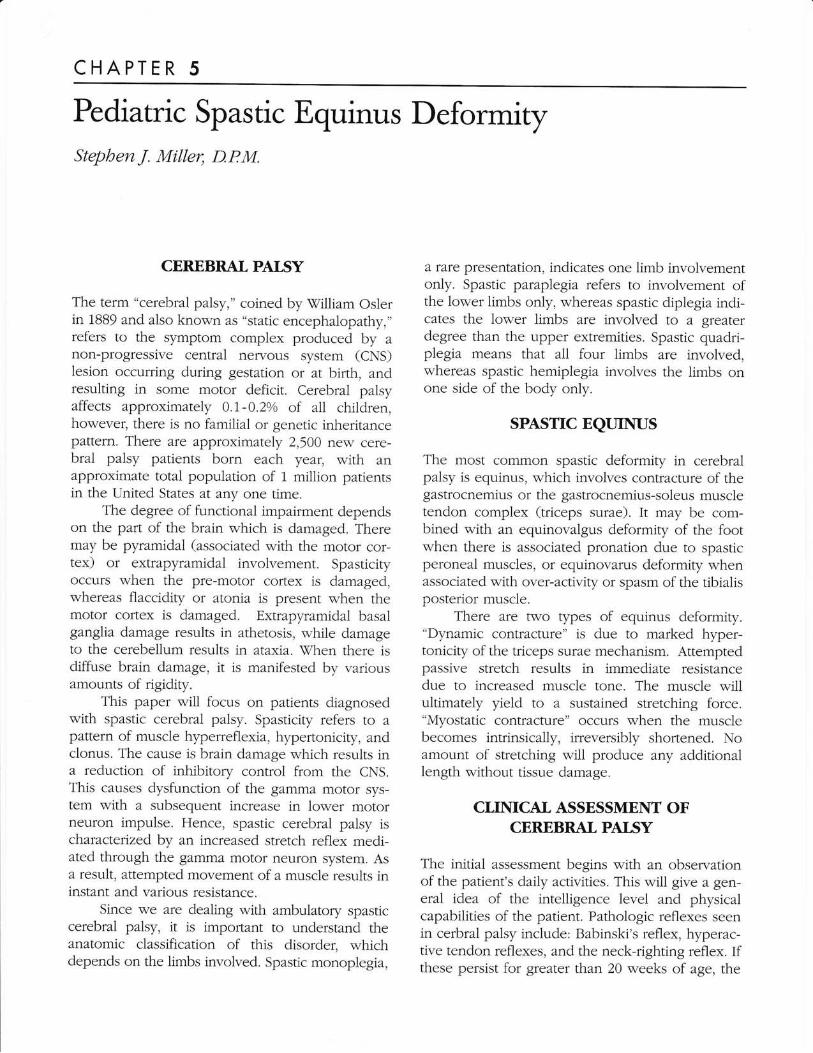
surae are responsible for the equinus is best deter-mined by the Silverskiold test, where ankledorsiflexion range of motion is measured with theknee extended as compared with when the knee isflexed (Fig. 1). Even though this may determinewhen the gastrocnemius muscle is the primary con-tracture, this has been challenged by Perry, whofelt that the soleus can cause recurrence of theequinus after selective lengthening of the gastroc-nemius muscie in the spastic patient. Nevertheless,each of the component muscles of the triceps surae
should be analyzed for strength, clonus, rigidity,resistance to rapid passive stretch, and resistance toslow steady pressure with the knee both extendedand flexed. In-depth muscle testing includes evalu-ating the amount of voluntary control, strength,
Figurr 1. The Siiverskiold test to differentiate
betlveen gastrocnemius equinus and gastrocnemius-
soleus equinus.
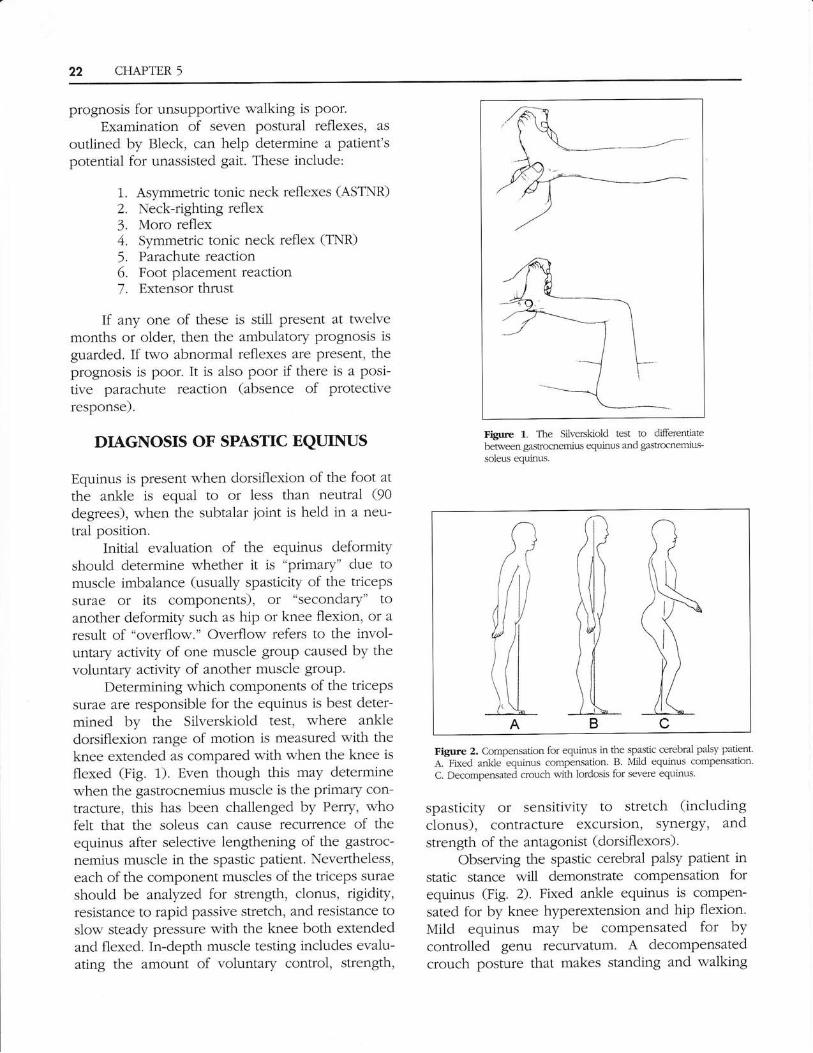
Figure 2. Compensation for equinus in the spastic cerebral palsy patient
A. Fired ankle equinus compensation. B Mild equinus compensation
C. Decompensated crouch with lordosis for severe equinus.
spasticity or sensitivity to stretch (including
clonus), contracture excursion, synergy, andstrength of the antagonist (dorsiflexors).
Observing the spastic cerebral palsy patient instatic stance will demonstrate compensation forequinus (Fig. 2). Fixed ankle equinus is compen-
sated for by knee hyperextension and hip flexion.Mild equinus may be compensated for bycontrolled genu recurvatum. A decompensatedcrouch posture that makes standing and waiking
CFLAPTER 5 23
virtually impossible without assisted devices is themost severe form of compensation, especiallywhen other contractures are present.
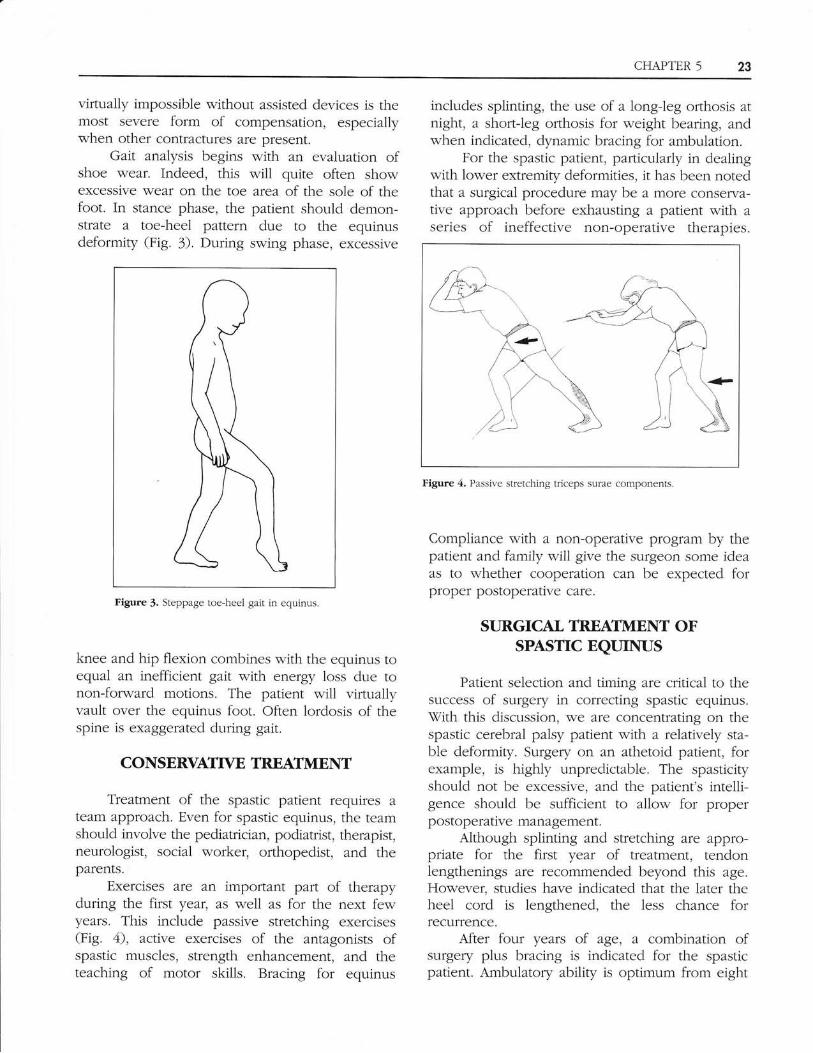
Gait analysis begins with an evaluation ofshoe wear. Indeed, this will quite often showexcessive wear on the toe area of the sole of thefoot. In stance phase, the patient should demon-strate a toe-heel pattern due to the equinusdeformity (Fig. 3). During swing phase, excessive
includes splinting, the use of a long-leg orthosis atnight, a short-leg orthosis for weight bearing, andwhen indicated, dynamic bracing for ambulation.
For the spastic patient, particularly in dealingwith lower extremity deformities, it has been notedthat a surgical procedure may be a more conserva-tive approach before exhausting a patient with aseries of ineffective non-operative therapies.
Figufe 3. Steppage toe-heel gait in equinus.
knee and hip flexion combines with the equinus toequal an inefficient gait with energy loss due tonon-forward motions. The patient will virtuallyvault over the equinus foot. Often lordosis of thespine is exaggerated during gait.
CONSERVATTYE TREATMENT
Treatment of the spastic patient requires a
team approach. Even for spastic equinus, the teamshould involve the pediatrician, podiatrist, therapist,neurologist, social worker, orthopedist, and theparents.
Exercises are an imporlant part of therapyduring the first year, as well as for the next fewyears. This include passive stretching exercises(Fig. 4), active exercises of the antagonists ofspastic muscles, strength enhancement, and theteaching of motor skills. Bracing for equinus
Figure 4. Passive stretching triceps surae components.
Compliance with a non-operative program by thepatient and family will give the surgeon some ideaas to whether cooperation can be expected forproper postoperative care.
SURGICAL TREATMENT OFSPASTIC EQUINIUS
Patient selection and timing are critical to thesuccess of surgery in correcting spastic equinus.With this discussion, we are concentrating on thespastic cerebral palsy patient with a relatively sta-ble deformity. Surgery on an athetoid patient, forexample, is highly unpredictable. The spasticityshould not be excessive, and the patient's intelli-gence should be sufficient to allow for properpostoperative management.
Although splinting and stretching are appro-priate for the first year of treatment, tendonlengthenings are recommended beyond this age.However, studies have indicated that the later theheel cord is lengthened, the less chance forrecuffence.
After four years of agel a combination ofsurgery plus bracing is indicated for the spasticpatient. Ambulatory ability is optimum from eight

24 CHAPTER 5
to twelve years, so this is the window for optimumsurgical intervention of the contracted tricepssurae. Such procedures may be augmented byother tendon lengthening and/or tendon transfers.
For bony procedures on patients under ten totwelve years, a calcaneal osteotomy or a subtalarjoint arthrodesis is recommended. For patients overten to twelve years, a triple arthrodesis is moreappropriate when indicated. Surgery on teenagers
is difficult due to emotional, developmental, andsocial considerations.
There is an interesting history of surgical pro-cedures developed to correct the variouscomponents of spastic equinus. The proceduresfavored for correction of spastic equinus are simi-lar to those for non-spastic equinus. However, theirtiming, selection, and combination are very impor-tant to insure success and prevent recurrence. Thegenerai goal of surgical interuention for spastic
equinus is to stabilize the lower extremity, and effi-ciently use available strength to allow the patient towalk as independently as possible. The idea is tofacilitate function, rather than to "stamp out defor-miry." The specific goal is to allow the foot to beflat on the floor without evoking a stretch reflex.
Attention must be paid to associated deformi-ties, such as hip and knee contractures, whichneed to be corrected prior to or simultaneouslywith equinus repair especially to prevent overstretching of a lengthened gastrocnemius in gaitpostoperatively. Hip contracture must be releasedprior to equinus correction, and knee contracturecan be treated at the same time or later. If thepatient has a short limb, it is important not to fullycorrect the equinus so as to allow compensatoryweight bearing.
Surgical correction is primarily directed toeither lengthening of the Achilles tendon or thegastrocnemius aponeurosis. Tendoachiliis length-ening (TAL) can be accomplished via a Z-slide ofthe tendon in the sagittal plane, cutting threefourths of the tendon on opposite sides at differentlevels. If a strict Z-slide is to be done based on theorientation of the Achilles fibers, then attentionmust be paid to the torsion in the tendon itself.
Vhite observed the torsion of the Achillestendon. Looking posteriorly, the posterior fibersrotale towards the lateral malleolus. Thus, the leftachilles tendon rotates clockwise and theright achilles tendon rotates counter-clockwise.Cummins et al. recommended specific cuts by
refining White's technique. They suggested cuttingthe posterior tlvo thirds of the Achilles tendonproximally, and the medial two thirds distally, toeffect a Z-slide. \fith this orientation in mind, thecuts can be made either percutaneously, orthrough an open incision for the more severe
deformity. A frontal plane Z-lengthening is also an
excellent approach to severe deformities, by allow-ing controlled reapproximation of the tendon withthe foot in its corrected position.
In spastic equinus surgery, one of the difficul-ties is in determining the amount of lengtheningnecessary for adequate correction. Over-lengtheningcan result in a functionally disastrous calcaneusdeformity which is virtually impossible to correct.Garbarino and Clancy devised a "geometricmethod" of calculating tendoachillis lengthening(Figs. 5A, B). They determined that the increasedlength of the achilles tendon necessary to bring thefoot into its corrected position is approximateiyone-half of the distance that the forefoot can travel.This can be calculated by measuring the distance
betlveen the heel pad and the bali of the foot in itsequinus position, and dividing it in half. This willbe the approximate measurement for lengtheningthe tendon. By this method, they experienced 0%
recurrence in 100 patients.Gastrocnemius recession is a commoniy used
method to lengthen the isolated gastrocnemius
muscle when it is the primary source of themyostatic or spastic contracture. However, a lowrecession can involve the aponeuroses to includeboth the soleus and the gastrocnemius muscles. Inthis case, healing and rehabilitation is much faster
than for a tendoachillis lengthening. The reverse
Baker technique, described by McGlamry and
Fulp, for tongue-in-groove recession is the recom-
mended procedure.Craig and VanVuren were so concerned about
recurrence that they recommended a combinationtendoachillis lengthening and gastrocnemius reces-
sion. This was treated postoperatively in a
full-length plaster cast, with the knee fullyextended and the foot in about 40 degrees of dor-siflexion, for three weeks. The patient was thenswitched into a weight-bearing cast for an addi-tional three weeks, followed by a retention braceuntil active dorsiflexion was of adequate strength.Of 276 cases, they recorded an overall recurrencerale of 9o/0.
Neurectomies of the gastrocnemius muscle

CI{APTER 5 25
F = FulcrumA and A1 = Achilles insertion before and
after correctionB and Bl = Head of 1st metatarsal before
and after correctionSolid line = Equinus footDotted line = Corrected foot
Figure 5A. Garbarino and Clancy's "Geometric method" ofcalculating the correct amount of tendoachillis lengthening.
weight bearing. For gastrocnemius recession, fourweeks of non-weight bearing is followed by twoweeks in a weight-bearing cast.
Once the cast is removed, gait trainingexercises are instituted with crutch assistance.Strengthening and stretching exercises are taught tothe patient, including active dorsiflexion and plan-tarflexion exercises, especially to augment thedorsiflexion antagonist muscles. A night splint is
essential throughout the growth period, or recuffencecan be expected. Bracing is usually not necessary.
The success of the surgery is measured by therate of recurrence. The rate of recurrences for ten-doachillis lengthening has ranged tp to 27o/o (Table1). It seems that the younger the patient at the timeof the lengthening, the greater the chance of recur-rence. For gastrocnemius recession, the rate ofrecurrence was generally slightly less, but in onestudy was as high as 29o/o (Table 2). Even when thegastrocnemius recession was combined with a TAL,the recurrence rate was 9o/0.
Table 1
RECLIRRENCE-TAL
YEAR AUTHOR(S)
1958 Banks & Green7959 Silver & Simon7959 Graham & Fksen1969 Conrad & Frost1.959 Lemperg7971 Frost1972 Sherrard & Bemstein1975. Sgarlato7976* Craig & vanVuren7977 Banks1980 Lee & Bleck1985 Garbarino & Clancy
NT]MBER RECI.]RRENCERAIE
764?
769848210
5.5%4.50/o1Jo/o
z)"/o72.50/o270/o
Flgure 58. Garbarino and Clancy's "Geometric method" of calculatingthe correct amount of tendoachillis lengthening. 1/2 "Y" is theappropriate amount of lengthening required.
heads should be avoided to prevent the develop-ment of myofibrosis. Attention should be paid tothe plantaris tendon, which must be released in allcases of equinus correction. The posterior ankleand subtalar joint capsules rarely have to bereleased. Younger patients spontaneously ruptureduring forced dorsiflexion at the time of the length-ening procedures. Other posterior group flexorsmust be evaluated and lengthened as necessary.
Postoperative care is essential to obtaining a
good result. For the spastic patient, a straight leg,knee extended cast, is recommended for the firsttwo to four weeks, followed by a below-knee cast,as long as the quadriceps are not in severe spasm.The position of the foot should be at least tendegrees dorsiflexed on the leg. For a tendo achillislengthening, total cast time is six weeks non-
* Nonspastic equinus# Combined TAL and gastroc recession
771581002007126
)10/"
4o/o
9o/o
7o/o
9o/o
0o/o
Table 2
RECf]RRENCE - GASTROCNEMIUS RECESSION
YEAR AUTHOR(S)
L959 Calandriello1965 Bassett and Baker1970 Baker, Basset & Dyas1972 Sharard & Bemstein1976* Craig and vanVuren1980 Lee and Bleck1.989# Downey and Banks
NUMBER RECI]BBENCERATE
?
44/t68151005136
8o/o
4o/o
5.60/o150/o
9o/o
290/o
0o/o
26 CHAPTER 5
* Nonspastic equinus+ Combined TAL and gastroc recession
SUMMARY
Although the technical procedures for lengtheningof the achiiies tendon in spastic equinus are weilknown and similar to those for non-spastic equi-nus, the importance of timing, patient seiection,and postoperative management cannot be over-stated. This is a yery special patient who requires ateam approach for correction of spastic equinus,which is the most common deformity seen in thecerebral palsy patient.
REFERENCES
Baker lD: Triceps surae syndrome in cerebral palsy.Med 36:88, 1955.Banks H, Green \l/: The correction of equinus deformity in cerebral
palsy. J BoneJoint Surg, 4O1r 1359-1,379, 1958.Banks HH, Panagakos P: Orthopaedic Evaluation of the Lower
Extremity in Cerebral Palsy. Clin Ortbop Rel Res 47:1.17, 7966.Bassett FH, Baker LD: Equinus Deformity in Cerebral Palsy. In Adams
lP (ed). Cuffent Practice in Ortbopaedic SurgetyYol 3. St. Louis,CV Mosby, 1956, p.59.
ConradJA, Frost HM: Evaluation of subcutaneous heel-cord lengthen-ing. Clin Orthop Rel Res 64:1.21.-1.27, 1.957.
Craig lJ, Vanvuren J: The importance of gastrocnemius recession inthe correction of equinus deformity in cerebral palsy. J BoneJointSurg 588:84, 1.976.
Cummins EJ, Ansun BJ, Carr ts.W: The structure of the calcanealtendon in relation to orthopedic surgery with additional obserwa-tion on the plantaris muscle, Szrg Gl,necol Obstetr83t707, 1.946.
Downey MS, Banks AS: Gastrocnemius recession in the treatment ofnon-spastic ankle equinus: A retrospective study. J Am PodidtrMed Assoc 79:1i9-1 r-4, 1989.
Frost HMr Subcutaneous tendo Achilles lengthening. Am J Ofibopi256-257, 1963.
Fulp MJ, McGlamry ED: Gastrocnemius tendon recession: tongue ingroove procedure to lengthen gastrocnemius tendon. J AmPodiatry Assoc 64L63-171, 1974.
Garbarino JL, Clancy Mr A geometdc method of calculating tendoachilles lengthentng. .J Pediatr Orthop 5:573-576, L985.
Green $7T, McDermott LJ: Operative Treatment of Cerebral Palsy ofSpastic Type. J Am Med Assoc 778:434, 1912.
Lee Cl, Bleck EE: Surgical corection of equinus deformity in cerebralpalsy. Der l[ecl Child Neurol 22:287, 7980.
Martz CDt Talipes equinus coffection in cerebral palsy. J Bone JointSurg 62A: 679, 7960.
PerryJ, Hoffer MM, Grovan P, et al.: Gait analysis of the triceps suraein cerebral paisy; A preoperative and postoperative clinical andelectromyographic study. J BoneJoint Surg 56A:511-520. 1971.
Pheips 1MM: Long-term Results of Orthopaedic Surgery in CerebralPalsy. J Bone Joint Surg 39A:53, 1957.
Pollock GA: Lengthening of the Gastrocnemius Tendon in Cases ofSpastic Equinus Deformity. J Bone Joint Surg 358:148, 1.953.
Pollock GA: Surgical Treatment of Cerebral Palsy. J BoneJoint Surg448,68,1962.
Schwartz JR, Cau W, Basset FH, Coonrad RIW: Lessons learned in thetreatment of equinus deformity in ambulatory spastic cerebralpalsy. Orthop Trans 7:81, 1-977.
Sharrard W], Bernstein S: Equinus defonnity in cerebral palsy. J BoneJoint SurglBrl, 518:272 276, 1972.
Silver CM, Simon DD: Gastrocnemius muscle recession (Silverskioldoperation) for spastic equinus deformity in cerebral palsy. J BoneJoint Surg 41A: 1021, 7959.
Silverskiold N: Reduction of the uncrossed t$'o-loint muscles of the legto one-joint muscles in spastic conditions. Acta Chir Scandiuau56;315, 1923-1924.
Stoffel A: The Treatment of Spastic Contractures. AmJ O?rhop Surg 70,6ti.. 1913.
Strayer LM Jr: Recession of the gastrocnemius and operation to relievespastic contracture of the calf muscles. /EoneJoint Surg 32A677-676, 1910.
Strayer LM Jr: Gastrocnemius recession. Five year report of cases.
J BoneJoint Surg 40A: 701,9, 19i8.\X/Lrite JW: Torsion of the Achilles tendon: Its surgical significance.
Arch Surg +6:-8-r. lo rJ.
Tardieu C, Lespargot A, Tabary C, et al: Toe walking in children withcerebral palsy: contributions of contracture and excessivecontraction of triceps surae muscle. Pbys Ther 69:8, 1989.
Vulpius O, Stoffel A: Ortbopadische Operationsblebre. Second edition.Stuttgart: Ferdinand Enke