
Pediatric soft tissue tumor of the upper arm with...
7
Case study Pediatric soft tissue tumor of the upper arm with LMNA-NTRK1 fusion ☆,☆☆ Shinji Kohsaka MD, PhD a,1 , Tsuyoshi Saito MD, PhD b, ⁎ ,1 , Keisuke Akaike MD, PhD b,c , Yoshiyuki Suehara MD, PhD c , Takuo Hayashi MD, PhD b , Tatsuya Takagi MD, PhD c , Kazuo Kaneko MD, PhD c , Toshihide Ueno PhD d , Shinya Kojima PhD d , Ken-ichi Kohashi MD, PhD e , Hiroyuki Mano MD, PhD d,f , Yoshinao Oda MD, PhD e , Takashi Yao MD, PhD b a Department of Medical Genomics, Graduate School of Medicine, The University of Tokyo, Tokyo, 113-0033, Japan b Department of Human Pathology, Juntendo University School of Medicine, Tokyo, 113-8421, Japan c Department of Orthopaedic Surgery, Juntendo University School of Medicine, Tokyo, 113-8421, Japan d Department of Cellular Signaling, Graduate School of Medicine, The University of Tokyo, 113-0033 e Department of Anatomic Pathology, Kyushu University, Graduate School of Medical Sciences, Fukuoka, 812-8582, Japan f National Cancer Center Research Institute, 104-0045 Received 4 May 2017; revised 31 July 2017; accepted 7 August 2017 Keywords: NTRK1 fusion; Pediatric soft tissue tumor; Fibrosarcoma; Inflammatory myofibroblastic tumor; Molecular target therapytumor Summary A 6-year-old girl was admitted to our hospital because of the presence of a slow-growing tumor in her right elbow. Biopsy specimens showed a round to spindle cell neoplasm with uncertain malignant potential, leading to the decision of surgical resection. Histologically, the resected tumor was encapsulated by fibrous tissue but focally invaded the surrounding skeletal muscles. The tumor was composed of ganglion cell–like short spindle cells with lymphocytic infiltration in the collagenous background. Tumor cells with large bizarre nuclei were occasionally observed, and multinucleated giant cells were scattered at the periphery. Hemangiopericytoma-like patterns and adipose tissue elements were not evident, and mitotic figures were rarely observed (b1 per 10 high-power fields). Immunohistochemically, the tumor cells were positive for S-100 and CD34 and focally positive for epithelial membrane antigen and AE1/AE3. RNA sequencing and subsequent reverse-transcription polymerase chain reaction revealed alternative splicing forms of LMNA-NTRK1 fusion (Ex2-Ex10 and Ex2-Ex15). © 2017 Elsevier Inc. All rights reserved. 1. Introduction Recent genome-wide and RNA sequence analyses have constantly identified new fusion genes in soft tissue tumors previously thought to be of unknown origin without characteristic histological features, leading to the establishment of certain tumor entities. Doebele et al [1] ☆ Competing interests: The authors declare that there is no conflict of interest. ☆☆ Funding/Support: This study was supported in part by a grant, Leading Advanced Projects for Medical Innovation, from the Japan Agency for Medical Research and Development and by a Grant-in-Aid for General Scientific Research from the Ministry of Education, Science, Sports, and Culture (#17K08730), Tokyo, Japan. ⁎ Corresponding author. E-mail address: [email protected] (T. Saito). 1 These 2 authors equally contributed. www.elsevier.com/locate/humpath http://dx.doi.org/10.1016/j.humpath.2017.08.017 0046-8177/© 2017 Elsevier Inc. All rights reserved. Human Pathology (2018) 72, 167–173
Transcript of Pediatric soft tissue tumor of the upper arm with...

www.elsevier.com/locate/humpath
Human Pathology (2018) 72, 167–173
Case study
Pediatric soft tissue tumor of the upper arm withLMNA-NTRK1 fusion☆,☆☆
Shinji Kohsaka MD, PhDa,1, Tsuyoshi Saito MD, PhDb,⁎,1, Keisuke Akaike MD, PhDb,c,Yoshiyuki Suehara MD, PhDc, Takuo Hayashi MD, PhDb, Tatsuya Takagi MD, PhDc,Kazuo Kaneko MD, PhDc, Toshihide Ueno PhDd, Shinya Kojima PhDd,Ken-ichi Kohashi MD, PhDe, Hiroyuki Mano MD, PhDd,f,Yoshinao Oda MD, PhDe, Takashi Yao MD, PhDb
aDepartment of Medical Genomics, Graduate School of Medicine, The University of Tokyo, Tokyo, 113-0033, JapanbDepartment of Human Pathology, Juntendo University School of Medicine, Tokyo, 113-8421, JapancDepartment of Orthopaedic Surgery, Juntendo University School of Medicine, Tokyo, 113-8421, JapandDepartment of Cellular Signaling, Graduate School of Medicine, The University of Tokyo, 113-0033eDepartment of Anatomic Pathology, Kyushu University, Graduate School of Medical Sciences, Fukuoka, 812-8582, JapanfNational Cancer Center Research Institute, 104-0045
Received 4 May 2017; revised 31 July 2017; accepted 7 August 2017
in
AMSC
h0
Keywords:NTRK1 fusion;Pediatric soft tissue tumor;Fibrosarcoma;Inflammatorymyofibroblastic tumor;
Molecular targettherapytumor
SummaryA 6-year-old girl was admitted to our hospital because of the presence of a slow-growing tumor inher right elbow. Biopsy specimens showed a round to spindle cell neoplasm with uncertain malignantpotential, leading to the decision of surgical resection. Histologically, the resected tumor was encapsulatedby fibrous tissue but focally invaded the surrounding skeletal muscles. The tumor was composed of ganglioncell–like short spindle cells with lymphocytic infiltration in the collagenous background. Tumor cellswith large bizarre nuclei were occasionally observed, and multinucleated giant cells were scattered at theperiphery. Hemangiopericytoma-like patterns and adipose tissue elements were not evident, and mitoticfigures were rarely observed (b1 per 10 high-power fields). Immunohistochemically, the tumor cells werepositive for S-100 and CD34 and focally positive for epithelial membrane antigen and AE1/AE3. RNAsequencing and subsequent reverse-transcription polymerase chain reaction revealed alternative splicingforms of LMNA-NTRK1 fusion (Ex2-Ex10 and Ex2-Ex15).© 2017 Elsevier Inc. All rights reserved.
☆ Competing interests: The authors declare that there is no conflict ofterest.☆☆ Funding/Support: This study was supported in part by a grant, Leadingdvanced Projects for Medical Innovation, from the Japan Agency foredical Research and Development and by a Grant-in-Aid for Generalcientific Research from the Ministry of Education, Science, Sports, andulture (#17K08730), Tokyo, Japan.
⁎ Corresponding author.E-mail address: [email protected] (T. Saito).
1 These 2 authors equally contributed.
ttp://dx.doi.org/10.1016/j.humpath.2017.08.017046-8177/© 2017 Elsevier Inc. All rights reserved.
1. Introduction
Recent genome-wide and RNA sequence analyses haveconstantly identified new fusion genes in soft tissue tumorspreviously thought to be of unknown origin withoutcharacteristic histological features, leading to theestablishment of certain tumor entities. Doebele et al [1]
168 S. Kohsaka et al.
described that NTRK1 fusions were detected in only 5 of 1272soft tissue sarcomas. A recent study reported that of 2031tumors, comprising leukemias, solid tumors, and primarycentral nervous system tumors and identified in patients underthe age of 21 years, 9 harbored NTRK fusions; 5 of these 9tumors were identified to have NTRK1 fusions [2]. NTRK1fusions in soft tissue sarcomas are extremely rare; however,they tend to be preferentially observed in pediatric patients [1].These tumors with NTRK1 fusions, especially LMNA-NTRK1fusions, have been described to be fibrosarcoma, fibroblastictumors with hemangiopericytoma- or myopericytoma-likepatterns with a relatively higher mitotic rate, or benign tolow-grade neuroectodermal tumors [1,2]. Another tumorentity, lipofibromatosis-like neural tumor with a lower mitoticrate, has recently been described [3]. In addition, a recentmanuscript described a case of generalized eruptive histiocytosisassociated with an LMNA-NTRK1 fusion [4]. We encountereda case of a soft tissue tumor, arising from the right upper arm(elbow) of a 6-year-old girl, detected with LMNA-NTRK1 genefusion that did not correspond well with the descriptions ofeither of these abovementioned tumor entities.
2. Materials and methods
2.1. Immunohistochemistry
Immunohistochemical staining was performed usingthe streptavidin-biotin method [A], with antibodies to thefollowing: epithelial membrane antigen (EMA) (Clone: E29,Dako, Glostrup, Denmark), S-100 protein (Clone: Rabbit Poly,Dako), CD34 (Clone: QBEnd/10, Leica Biosystems, Newcastle,UK), p53 (Clone: DO-7, Dako), and Ki-67 (Clone: MIB-1,
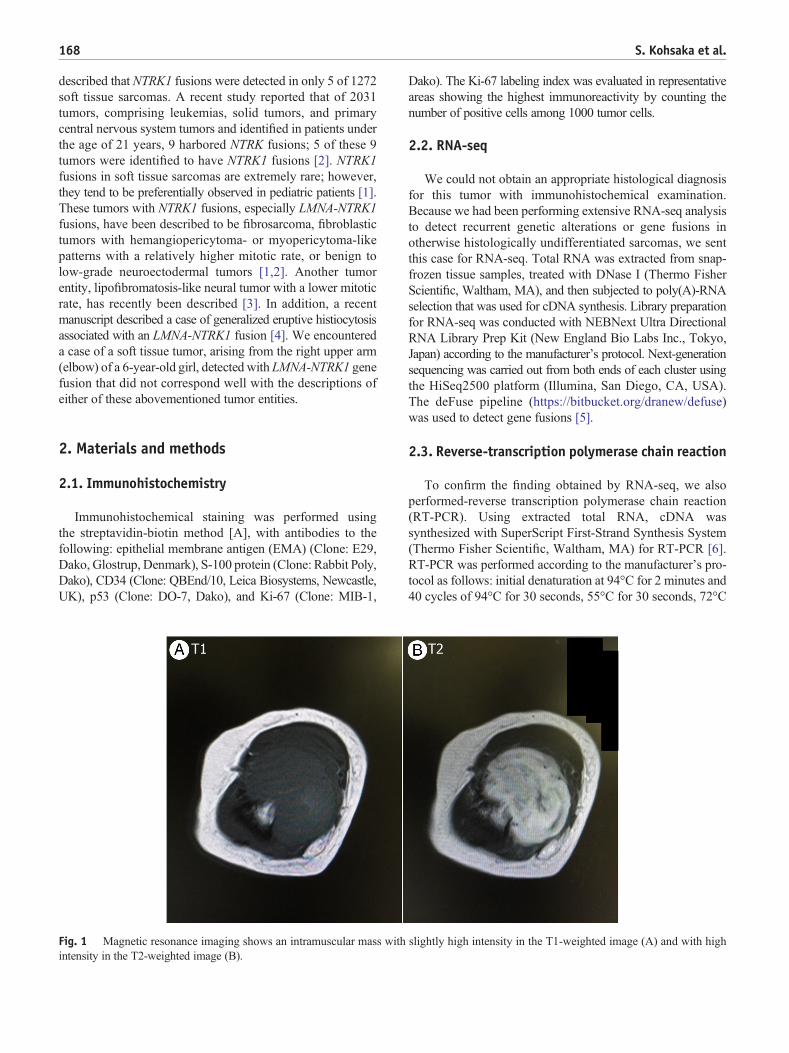
Fig. 1 Magnetic resonance imaging shows an intramuscular mass withintensity in the T2-weighted image (B).
Dako). The Ki-67 labeling index was evaluated in representativeareas showing the highest immunoreactivity by counting thenumber of positive cells among 1000 tumor cells.
2.2. RNA-seq
We could not obtain an appropriate histological diagnosisfor this tumor with immunohistochemical examination.Because we had been performing extensive RNA-seq analysisto detect recurrent genetic alterations or gene fusions inotherwise histologically undifferentiated sarcomas, we sentthis case for RNA-seq. Total RNA was extracted from snap-frozen tissue samples, treated with DNase I (Thermo FisherScientific, Waltham, MA), and then subjected to poly(A)-RNAselection that was used for cDNA synthesis. Library preparationfor RNA-seq was conducted with NEBNext Ultra DirectionalRNA Library Prep Kit (New England Bio Labs Inc., Tokyo,Japan) according to the manufacturer's protocol. Next-generationsequencing was carried out from both ends of each cluster usingthe HiSeq2500 platform (Illumina, San Diego, CA, USA).The deFuse pipeline (https://bitbucket.org/dranew/defuse)was used to detect gene fusions [5].
2.3. Reverse-transcription polymerase chain reaction
To confirm the finding obtained by RNA-seq, we alsoperformed-reverse transcription polymerase chain reaction(RT-PCR). Using extracted total RNA, cDNA wassynthesized with SuperScript First-Strand Synthesis System(Thermo Fisher Scientific, Waltham, MA) for RT-PCR [6].RT-PCR was performed according to the manufacturer's pro-tocol as follows: initial denaturation at 94°C for 2 minutes and40 cycles of 94°C for 30 seconds, 55°C for 30 seconds, 72°C
slightly high intensity in the T1-weighted image (A) and with high
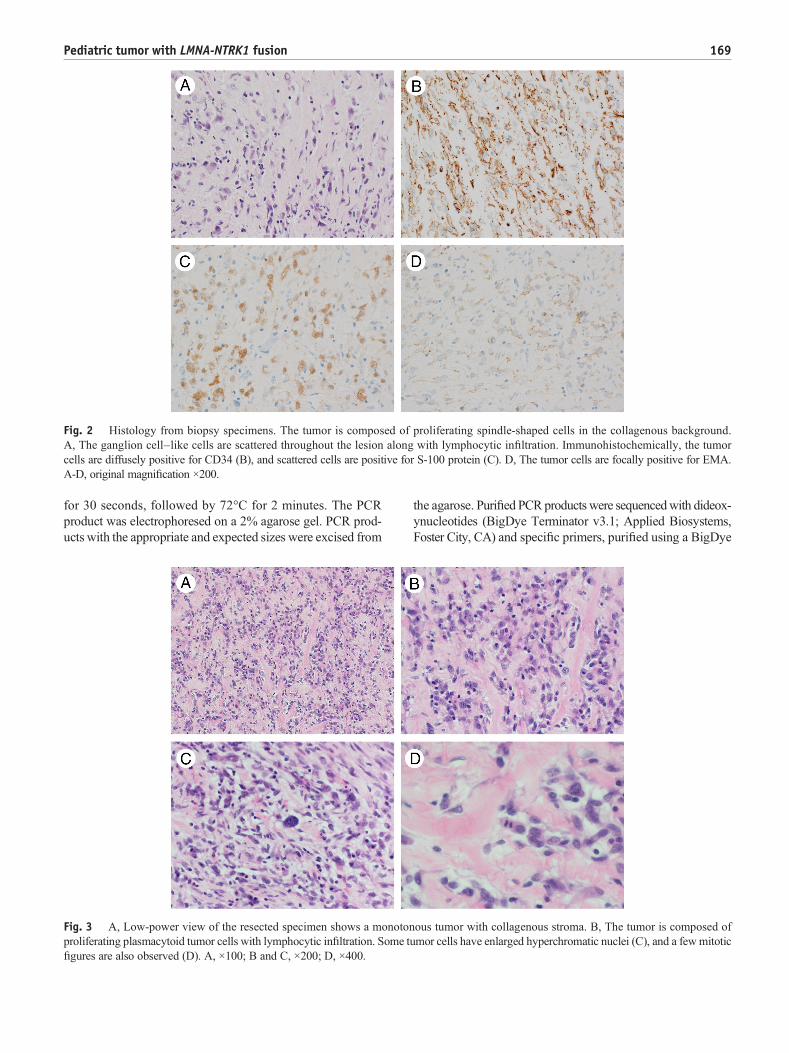
Fig. 2 Histology from biopsy specimens. The tumor is composed of proliferating spindle-shaped cells in the collagenous background.A, The ganglion cell–like cells are scattered throughout the lesion along with lymphocytic infiltration. Immunohistochemically, the tumorcells are diffusely positive for CD34 (B), and scattered cells are positive for S-100 protein (C). D, The tumor cells are focally positive for EMA.A-D, original magnification ×200.
169Pediatric tumor with LMNA-NTRK1 fusion
for 30 seconds, followed by 72°C for 2 minutes. The PCRproduct was electrophoresed on a 2% agarose gel. PCR prod-ucts with the appropriate and expected sizes were excised from
Fig. 3 A, Low-power view of the resected specimen shows a monotonproliferating plasmacytoid tumor cells with lymphocytic infiltration. Some tfigures are also observed (D). A, ×100; B and C, ×200; D, ×400.
the agarose. Purified PCRproducts were sequencedwith dideox-ynucleotides (BigDye Terminator v3.1; Applied Biosystems,Foster City, CA) and specific primers, purified using a BigDye
ous tumor with collagenous stroma. B, The tumor is composed ofumor cells have enlarged hyperchromatic nuclei (C), and a fewmitotic

Fig. 4 Immunohistochemistry of the resected specimen showed diffuse staining for CD34 (A) and focal staining for S-100 protein (B) and EMA(C). D, The MIB-1 labeling index was approximately 25%. A-D, ×200.
170 S. Kohsaka et al.
X Terminator Purification Kit (Applied Biosystems), and ana-lyzed with a capillary sequencing machine (3730xl Genetic An-alyzer; Applied Biosystems). The primer sequences used are asfollows:LMNA exon 2, 5′-ACCAAGAAGGAGGGTGACCT-3′; NTRK1 exon 10, 5′-CAAGGAGCAGCGTAGAAAGG-3′; exon 13, 5′-CGTGCCGCATATACTCAAAG-3′; andexon 15, 5′-ATGATGGCGTAGACCTCTGG-3′. Threeindependent PCRs were performed using a combination ofthe LMNA primer and either of the NTRK1 primers to detectLMNA-NTRK1 fusion.
Fig. 5 A, RT-PCR was performed to confirm the findings of RNA sequlocated on exon 2 of LMNA, reverse primer located on exon 10 of NTRK1located on exon 13 ofNTRK1; PCR3: forward primer located on exon 2 of Lfor each PCR product were 216, 282, and 384 base pairs, respectively. B analternative forms of LMNA-NTRK1. PCR1 and PCR2 detected the sameLMNA-NTRK1 fusion (Ex2-Ex15). D, A drawing showing the organization
3. Case report
A 6-year-old girl noticed a mass on her right elbow inJanuary 2016 and was admitted to our hospital for a slow-growing tumor. The tumor was approximately 5 cm indiameter. Tenderness was observed, but Tinel's sign was notevident. Magnetic resonance imaging revealed a mass withslightly high intensity on T1-weighted imaging (Fig. 1A) andhigh intensity on T2-weighted imaging (Fig. 1B). A biopsywas performed, and on histological examination, the specimen
ences. Three different PCRs were performed (PCR1: forward primer; PCR2: forward primer located on exon 2 of LMNA, reverse primerMNA, reverse primer located on exon 15 ofNTRK1). Anticipated sizesd C, RT-PCR followed by direct sequencing revealed the presence ofform of LMNA-NTRK1 fusion (Ex2-Ex10), whereas PCR3 detectedof fusion proteins and the functional domains in the 2 variants.

Fig. 5. (continued)
171Pediatric tumor with LMNA-NTRK1 fusion
showed proliferation of round- to spindle-shaped cells(Fig. 2A). Immunohistochemistry revealed that the tumor cellswere diffusely positive for CD34 (Fig. 2B), partially positivefor S-100 protein (Fig. 2C), and focally positive for EMA(Fig. 2D), leading to a tentative diagnosis of a hybrid nervesheath tumor. However, the possibility of a round to spindlecell neoplasm with uncertain malignant potential could notbe ruled out. Therefore, surgical resection of the tumorwas performed.
Grossly, the cut surface of the solid tumor was white toyellowish in color, without apparent bleeding and necrosis.
Histologically, the resected tumor was encapsulated by fibroustissue but focally invaded the surrounding skeletal muscles.The tumor was uniform throughout the lesion (Fig. 3A). Thetumor was composed of ganglion cell–like short spindle cellswith lymphocytic infiltration in the collagenous background(Fig. 3B). Tumor cells with large bizarre nuclei were occasion-ally observed (Fig. 3C), and multinucleated giant cells werescattered at the periphery. Hemangiopericytoma-like patternswere not evident, and an admixture with adipose elementswas also not observed. Mitotic figures were rarely observed(b1 per 10 high-power fields) (Fig. 3D). Immunohisto-

172 S. Kohsaka et al.
chemically, the tumor cells were positive for CD34 (Fig. 4A)and S-100 protein (Fig. 4B), focally positive for EMA(Fig. 4C) and AE1/AE3, but negative for other markers includ-ing myogenic markers. Tumor cells were immunohistochemi-cally also positive for p53 (40% of tumor cells), and theMIB-1labeling index was approximately 25% (Fig. 4D). However,we could not obtain an appropriate histological diagnosis forthis tumor.
Frozen tissue samples were available for this case, andRNA sequencing revealed the presence of an LMNA-NTRK1fusion transcript. Subsequent RT-PCR showed alternativesplicing forms of LMNA-NTRK1 (Ex2-Ex10 and Ex2-Ex15)(Fig. 5A-C).
The patient is presently alive and well, 10 months aftersurgery, without recurrence or metastasis.
4. Discussion
Recent genome-wide and RNA sequence analyses haveidentified new fusion genes in tumors, including soft tissuetumors, previously thought to be of unknown origin withoutcharacteristic histological features. NTRK1 fusions in softtissue sarcomas are extremely rare. Doebele et al [1] describedthatNTRK1 fusions were detected in only 5 of 1272 soft tissuesarcomas; 3 of these patients were less than 5 years old.Furthermore, only 1 among the 5 cases was an LMNA-NTRK1fusion-positive fibrosarcoma [1]. In addition, a recent studydemonstrated that of 2031 tumors, comprising leukemias, sol-id tumors, and primary central nervous system tumors andidentified in patients under the age of 21 years, 5 tumorsharbored NTRK1 fusions and that 2 of these 5 tumors wereidentified to have LMNA-NTRK1 fusions [2]. However, thefrequency ofNTRK1 fusion sarcomas in Japan is still not clear.We could not obtain an appropriate histological diagnosis inthis case and were unaware of the fact that this tumor couldharbor NTRK1 fusion. We accidently identified this case tobe having LMNA-NTRK1 fusion by RNA-seq, and we alsoconfirmed this finding by RT-PCR.
Regarding the soft tissue tumors with NTRK1 fusion, arecent study has reported 2 pediatric cases of soft tissuesarcomas with NTRK1 fusion, one of which had an LMNA-NTRK1 fusion and another had TPM3-NTRK1 fusion [7].Another recent study described a case of infantile fibrosarcomawith LMNA-NTRK1 fusion in a 1-month-old infant whoshowed remarkable response to the tyrosine kinase inhibitor(TKI) crizotinib [8]. Two soft tissue tumors with LMNA-NTRK1 fusion have been described in a recent report [2].One of them was a fibrosarcoma arising in a 1-year-old boy,and the other was a benign to low-grade neuroectodermaltumor in a 14-year-old adolescent girl [2]. Two of these threeabovementioned pediatric fibroblastic tumors with LMNA-NTRK1 fusion showed high cellularity of spindle cells,suggesting that these tumors were low-grade sarcomas.The remaining case with LMNA-NTRK1 fusion was describedto be a metastatic fibrosarcoma without information on the
primary tumor [2]. Two pediatric cases with NTRK1 fusionshowed histological hemangiopericytoma and myopericytomapatterns and high mitotic rates [7]. However, in our case,hemangiopericytoma and myopericytoma patterns were notevident, and mitosis was rarely observed. The two aforemen-tioned cases were described to be immunohistochemicallypositive for myogenic markers, but our case was negative formyogenic markers. However, the current case was positivefor CD34 and S-100 protein. It would be interesting to notethat CD34 positivity is reminiscent of infantile fibrosarcomawith NTRK3 fusion [9] and that the LMNA-NTRK1 fusion,detected in the current study, has been reported in spitzoidmelanomas with neurogenic differentiation [10].
In view of the proliferation of spindle-shaped cells withlymphocytic infiltration, we considered the possibility ofinflammatory myofibroblastic tumor, of which a subset hasbeen shown to have anETV6-NTRK3 fusion [11,12]. However,in our case, this possibility was ruled out based on the absenceof immunohistochemical positivity for myogenic markers.
A recent study demonstrated a subset of soft tissue tumorswith distinct lipofibromatosis (LPF)–like morphology withNTRK1 fusions, with predominance of LMNA-NTRK1 fusions[3]. These tumors were described to occur in children andadults ranging from 4 to 36 years old and were immunohisto-chemically positive for S-100 and CD34. Furthermore, thesetumors showed lowermitotic rates [3]. Our case did not fit wellwith these previously described tumors having LMNA-NTRK1fusion, although our case did seem to be closely relatedto LPF-like neural tumors except for the absence of the adi-pose tissue element. In addition, a recent study demonstratedthat an infantile spindle cell sarcoma with neural featuresharbored TFG-MET fusion [13].
Two forms of LMNA-NTRK1 fusion transcripts weredetected in our case. The LMNA (exon 2)–NTRK1 (exon 10)variant could be the active form of tyrosine kinase becausethe other one is expected to not contain the protein kinase do-main (Fig. 5D), although we did not confirm this on functionalstudies. However, the real target activity of TKI could also de-pend on other genetic abnormalities; detailed investigationsfor the presence of other genetic alterations were not carriedout in this present case.
In addition to the low frequency in sarcomas, NTRK1fusions have also been detected in various tumors includingpapillary thyroid carcinoma, lung adenocarcinoma, intrahepaticcholangiocarcinoma, colorectal carcinoma, and glioblastoma[14-18]. Currently, several tyrosine receptor kinase (TRK)–targeting compounds are under clinical development [19].Recent studies demonstrated a positive response to the TRKinhibitor LOXO-101 in 2 tumors with LMNA-NTRK1 fusion[1,20]. Furthermore, 1 of those 2 tumors was an undifferentiatedsoft tissue sarcoma [1]. However, the presence of an NTRK1fusion does not necessarily indicate that a tumor wouldrespond to a TRK inhibitor as much as expected. We needto keep in mind that the status of other genetic alterationsbesides NTRK1 fusion might affect the therapeutic efficacyof TKI [21]. Although the patient in this case is well and alive

173Pediatric tumor with LMNA-NTRK1 fusion
with no evidence of recurrence or metastasis, treatment withthese TRK inhibitors would be applicable for such patients.
Acknowledgment
We appreciate Dr Abbas Agaimy, Institute of Pathology,University Hospital, Friedrich-Alexander University Erlangen-Nuremberg, Erlangen, Germany, for his comments on this case.
References
[1] Doebele RC, Davis LE, Vaishnavi A, et al. An oncogenic NTRK fusionin a patient with soft-tissue sarcoma with response to the tropomyosin-related kinase inhibitor LOXO-101. Cancer Discov 2015;5:1049-57.http://dx.doi.org/10.1158/2159-8290.
[2] Pavlick D, Schrock AB,Malicki D, et al. Identification of NTRK fusionsin pediatric mesenchymal tumors. Pediatr Blood Cancer 2017;64. http://dx.doi.org/10.1002/pbc.26433.
[3] Agaram NP, Zhang L, Sung YS, et al. Recurrent NTRK1 gene fusionsdefine a novel subset of locally aggressive lipofibromatosis-like neuraltumors. Am J Surg Pathol 2016;40:1407-16.
[4] Pinney SS, Jahan-Tigh RR, Chon S. Generalized eruptive histiocytosisassociated with a novel fusion in LMNA-NTRK1. Dermatol Online J2016;22 [pii: 13030/qt07d3f2xk].
[5] McPherson A, Hormozdiari F, Zayed A, et al. deFuse: an algorithm forgene fusion discovery in tumor RNA-Seq data. PLoS Comput Biol2011;7:e1001138.
[6] Akaike K, Kurisaki-Arakawa A, Hara K, et al. Distinct clinicopatholog-ical features of NAB2-STAT6 fusion gene variants in solitary fibrous tu-mor with emphasis on the acquisition of highly malignant potential. HUM
PATHOL 2015;46:347-56.[7] Haller F, Knopf J, Ackermann A, et al. Paediatric and adult soft tissue
sarcomas with NTRK1 gene fusions: a subset of spindle cell sarcomasunified by a prominent myopericytic/haemangiopericytic pattern. JPathol 2016;238:700-10. http://dx.doi.org/10.1002/path.4701.
[8] Wong V, Pavlick D, Brennan T, et al. Evaluation of a congenital infantilefibrosarcoma by comprehensive genomic profiling reveals an LMNA-
NTRK1 gene fusion responsive to crizotinib. J Natl Cancer Inst 2015;108. http://dx.doi.org/10.1093/jnci/djv307 [pii: djv307].
[9] Knezevich SR, McFadden DE, Tao W, Lim JF, Sorensen PH. A novelETV6-NTRK3 gene fusion in congenital fibrosarcoma. Nat Genet1998;18:184-7.
[10] Wiesner T, He J, Yelensky R, et al. Kinase fusions are frequent in Spitztumours and spitzoid melanomas. Nat Commun 2014;3116. http://dx.doi.org/10.1038/ncomms4116.
[11] Yamamoto H, Yoshida A, Taguchi K, et al. ALK, ROS1 and NTRK3gene rearrangements in inflammatory myofibroblastic tumours. Histopa-thology 2016;69:72-83. http://dx.doi.org/10.1111/his.12910.
[12] Alassiri AH, Ali RH, Shen Y, et al. ETV6-NTRK3 is expressed in a sub-set of ALK-negative inflammatory myofibroblastic tumors. Am J SurgPathol 2016;40:1051-61.
[13] Flucke U, van Noesel MM, Wijnen M, et al. TFG-MET fusion in an in-fantile spindle cell sarcoma with neural features. Genes ChromosomesCancer 2017;56:663-7.
[14] Park DY, Choi C, Shin E, et al. NTRK1 fusions for the therapeutic inter-vention of Korean patients with colon cancer. Oncotarget 2016;7:8399-412. http://dx.doi.org/10.18632/oncotarget.6724.
[15] Lee SJ, Li GG, Kim ST, et al. NTRK1 rearrangement in colorectal cancerpatients: evidence for actionable target using patient-derived tumor cellline. Oncotarget 2015;6:39028-35. http://dx.doi.org/10.18632/oncotar-get.5494.
[16] Vaishnavi A, Capelletti M, Le AT, et al. Oncogenic and drug-sensitiveNTRK1 rearrangements in lung cancer. Nat Med 2013;19:1469-72.http://dx.doi.org/10.1038/nm.3352.
[17] Ross JS, Wang K, Gay L, et al. New routes to targeted therapy of intra-hepatic cholangiocarcinomas revealed by next-generation sequencing.Oncologist 2014;19:235-42. http://dx.doi.org/10.1634/theoncologist.2013-0352.
[18] Zheng Z, Liebers M, Zhelyazkova B, et al. Anchored multiplex PCR fortargeted next-generation sequencing. Nat Med 2014;20:1479-84. http://dx.doi.org/10.1038/nm.3729.
[19] Khotskaya YB, Holla VR, Farago AF, et al. Targeting TRK family pro-teins in cancer. Pharmacol Ther 2017;173:58-66.
[20] RussoM,Misale S,Wi G, et al. Acquired resistance to the TRK inhibitorentrectinib in colorectal cancer. Cancer Discov 2016;6:36-44. http://dx.doi.org/10.1158/2159-8290.
[21] Fuse MJ, Okada K, Oh-Hara T, Ogura H, Fujita N, Katayama R. Mech-anisms of resistance to NTRK inhibitors and therapeutic strategies inNTRK1-rearranged cancers. Mol Cancer Ther 2017;16:2130-43.










![Recurrent primary mediastinal giant cell tumor of soft tissue ......Discussion Giant cell tumor of soft tissue (GCT-ST) is a rare tumor. GCT-ST, which resembles osseous GCT [2], broadly](https://static.fdocuments.us/doc/165x107/608dfb4a7de20e33185e8616/recurrent-primary-mediastinal-giant-cell-tumor-of-soft-tissue-discussion.jpg)







