pediatric Sleep disorders
58
Pediatric Sleep Disorders Marwa Elhady lecturer of pediatrics Al-Azhar univerisity 2015
-
Upload
marwa-elhady -
Category
Health & Medicine
-
view
317 -
download
0
Transcript of pediatric Sleep disorders

Pediatric Sleep Disorders
Marwa Elhadylecturer of pediatricsAl-Azhar univerisity
2015

Objectives
• Understand normal sleep in children• Review common pediatric sleep disorders• Discuss proper treatment options for
childhood sleep disorders

The Sleep Cycle

The Sleep Cycle• Each sleep cycle 90 – 120 minutes• First REM period is shortest• Most NREM deep sleep occurs early• Most REM occurs late

Children’s Sleep Differs from Adults
• More frequent REM • Earlier REM• More Total Hours of Sleep• Sleep disorders common in pediatrics than adults

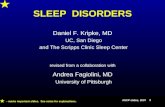
REM & NREM Sleep by Age
02468
1012141618
1 - 3M
3 - 5M
6-23M
2 - 3Y
3 - 5Y
5 - 9Y
10-13Y
14-18Y
19-30Y
Tot
al H
rs S
leep
Total daily sleep by age
During childhood sleep accounts for 40% of the dayAt birth, REM ≈ 50% of total sleep, ↓ to 25% in adult

prevalence ≈25% - 43%of children ages 1-5 years
interfere with daily patient and family functioning.
sleep problems cause significant emotional, behavioral, and cognitive dysfunction.
common among children with neurodevelopmental, medical and psychiatric disorders.
Lehmkuhl et al.,2008


Owens, 2011


Sleep disorders divided into 3 categories:1- Dyssomnias (# duration, timing of sleep)
Primary Insomnia Primary Hypersomnia Breathing-Related Sleep Disorder Narcolepsy Circadian Rhythm Sleep Disorder
2- Parasomnias (abnormal events during sleep) Nightmare Night Terrors Sleep walking
3- Medical psychiatric disordersAPA, 2013

The clinical evaluation involves: obtaining a careful medical history assess for medical cause of sleep disturbance Current sleep patterns, including sleep duration,
sleep-wake schedule, sleep habits, Nocturnal symptoms
Polysomnogram (PSG) record: EEG, EMG, EOG, Vital Signs and Other Physiologic ParametersOwens, 2011



Difficult initiate or maintain sleep or early morning awake with difficult return to sleep
Occur 3 nights/week, for at least 3 months, despite sufficient time for sleep.
Not due to the effects of a substance
Not explained by mental/medical illness
Prevalence 1 – 6 % in pediatrics but higher in children with chronic med/psych conditions
Czeisler et al., 2010

Insomnia is subdivided into: 1. Sleep onset insomnia: difficulty falling asleep.
2. Sleep maintenance insomnia: frequent or sustained awakenings.
3. Sleep offset insomnia: early morning awakenings
4. Non-restorative sleep: persistent sleepiness despite adequate sleep duration
Czeisler et al., 2010

• Mainly treated with behavioral interventions• Media removal from bedroom• Avoid caffeine• Consistent bedtime routine and positive
reinforcement from parents/caregivers• Correct the underlying med/psycho factors
Treatment of insomnia
Owens, 2011

prolonged sleep episodes, excessive sleepiness
prolonged sleep > 9 h/day that is not refreshing
Difficulty being fully awake after abrupt awakening
The complaint is present for at least 6 months.
Not due to med/psycho disorder
Common in in late adolescence.American Academy of Sleep Medicine, 2001

Obstructive Sleep Apnea (1 – 4 %)Results in blood oxygen desaturations
Upper Airway Resistance SyndromeSimilar to OSA but not result in desaturations
Primary Snoring (7 – 12%)regular snoring without changes in sleep architecture, alveolar ventilation or oxygenation
APA, 2013

• Periodic apneas due to sleep-related airway obstruction - ↓ patency (obstruction and/or ↓diameter)
- ↑ collapsibility (↓ pharyngeal muscle tone)
-↓ drive to breath (↓ central ventilatory drive)
•Not all snorers have OSA
Bradley and Floras,2009

Sequelae of OSA • Disrupt ventilation and sleep patterns
• intermittent hypoxia and multiple arousals cause significant metabolic, CVS, neurocog/behavioral and academic morbidity
• Daytime Sleepiness, Enuresis as short-term squeal
• Pulmonary hypertension and right heart failure, FFT as long term sequel

Treatment of Sleep Apnea • Weight loss
• Positional (sleep on one side or prone)
• CPAP prevents obstruction by soft-tissue and keeps airway open
• Surgical intervention (e.g., tonsiloadenectomy)
• Avoid sedatives (which prevent reawakening to breath)

uncontrollable excessive daytime sleep attacks interfere with normal daily functioning
Person goes directly into REM sleep Common in adolescence & early adulthood Genetic defect in hypothalamic orexin/hypocretin
neurotransmitter prevalence is 3-16/10,000
Owens, 2011

Symptoms associated with narcolepsy

Cataplexy (pathognomonic for narcolepsy)Abrupt bilateral partial or complete loss of m. tone. triggered by intense positive emotion (e.g., laught)last for seconds to minutes with complete recovery
Hallucinations (visual, auditory, tactile)occur during transitions bet. sleep and wakefulnessAt sleep onset → hypnogogic At sleep offset → hypnopompic
Sleep paralysis: inability to move or speak for sec- min at sleep onset or offset; accompanies hallucination
Owens, 2011

DD Potential causes of EDS:Extrinsic: 2ry to insufficient/fragmented sleep Intrinsic: CNS disorder with ↑ need for sleep.
Treatment include:Education, good sleep hygiene, behavioral changes (eg. Scheduled naps). Medications as:
• psychostimulants and modafinil to control EDS. • TAD and SSRI to control REM-associated
phenomena, such as cataplexy
Owens, 2011

Circadian Rhythm Sleep Disorder caused by Circadian Rhythm Sleep Disorder caused by mismatch between sleep-wake schedule mismatch between sleep-wake schedule required by a person’s environment and required by a person’s environment and his/her circadian sleep-wake pattern (e.g., his/her circadian sleep-wake pattern (e.g., shift work). shift work).

It is a circadian rhythm disorder
significant, persistent, intractable phase shift in sleep wake schedule (later sleep onset and wake time)
Patients has inability to get to sleep until the early morning, but little difficulty sleeping once asleep
Interfere with school, work and lifestyle demands.
Common in adolescents and young adults (7-16%)
Owens, 2011

Treatment
Treatment is primarily behavioral
•Shifting the sleep-wake schedule to an earlier time
•Maintaining the new schedule. → Gradual shifting bedtime/wake time earlier by 15-30 min increments → Exposure to light in morning and avoidance of evening light exposure
Oral melatonin supplementation in the afternoon or early evening is effective in advancing the sleep phase.


Uncomfortable sensations in the LL accompanied by irresistible urge to move legs →Disturbs sleep
Severe leg pain is main symptom, missed as ‘growing pains’.
partially relieved by movement (walking, stretching, rubbing) but only as long as the motion continues.
Diagnosis of RLS is a clinical.
Prevalence in children is 1-6 %
Khatwa and Kothare, 2010

periodic, repetitive, brief (0.5-10 sec) highly stereotyped limb jerks (rhythmic extension of big toe and dorsiflexion at ankle).
occurring at 20 to 40 sec intervals.
occur mainly during sleep → Disrupts sleep
Prevalence in children is 8-12%

Diagnosis of PLMs requires overnight polysomnography to document the characteristic limb movements with anterior tibialis EMG leads.
Owens, 2011

Treatment according to: severity (intensity, frequency, periodicity) degree of sleep disturbancedaytime sequelae
•an index (PLMs per hr) < 5 → no treatment •index > 5 → promote good sleep hygiene → iron supplements if ferritin <50
•Medications that ↑ dopamine in CNS are effective in adults but limited data in children.

repetitive, stereotyped, rhythmic movements involve large muscle groups.
include head banging, body rocking, head rolling common in the 1st yr of life and disappear by age 4 yr occur with the transition at sleep at bedtime. It is a means of soothing themselves to sleep significant injury is rare not indicate neurological or psychological problem. reassurance to the family
Owens, 2011

• Episodic nocturnal behaviors involve cognitive disorientation and autonomic and skeletal muscle disturbance.

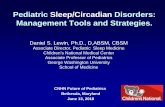
0%10%20%30%40%50%60%70%80%

0% 5% 10% 15% 20% 25% 30%
Sleepwalking
Bruxism
Sleep Terrors
Enuresis

• Sleep disorder characterized by high arousal and appearance of being terrified
• ≈ 2/3 of all kids experience them• Common in preschoolers ages 3-6 y• Occur during REM sleep• Child believes them to be real.
Owens, 2011

repeated abrupt awakenings from sleep characterized by intense fear, panicky screams, autonomic symptoms (tachycardia, rapid breathing, sweating), absence of detailed dream recall, amnesia for the episode, and relative unresponsiveness to attempts to comfort the person.
Lasts ~ 10 min then returns to undisturbed sleep.

During Stage 3-4 of NREM sleep (1st third of night)
Prevalence is 3–6.5% in children.
can occur at any age.
Common in male
resolves spontaneously
Nocturnal administration of benzodiazepines has been reported to be beneficial

Nightmares Night Terrors
Age 3 - 6 yrs 4 - 8 yrs
Sleep Stage REM NREM (3/4)
Time of Night Late Early
State on waking Upset / Scared Disoriented
Response to parents Consolable Unaware of
Parents
Return to Sleep Difficult Easy / Rapid
Memory of Event occasional None

involuntary, forceful grinding of teeth during sleep Up to 88% of children; 20 % of adults Any stage of sleep May result in damage to the teeth Periodicity of 20 to 30 seconds. May represent symptom different disorders Patient is usually unaware of the problem In severe cases, rubber tooth guard is necessary. Stress
management or biofeedback.

Begins during school ageDuring NREM and REM sleepNo treatment just reassurance

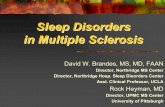
One or more waking from midnight to 5 am for at least four of seven nights per week for at least four consecutive weeks
0%5%
10%15%20%25%30%35%40%45%50%
All Infants BreastfedInfants
1-2 YrOlds
4-5 YrOlds
Owens, 2011

More than just walking around…
Simple Behaviors
Complex Behaviors While sleepwalking, patient has a blank staring face,
relatively unresponsive to others confused or disoriented on being aroused. Complete amnesia Occur during Stage 3-4 Sleep; 1st third of night.

Begins in ages 4-8 yrs 17% in children (4% of adults) sleep-walking most likely to persist it is important to institute safety precautions (use of
gates, locking doors and windows, and bedroom door alarms).
No treatment is established, but may respond to benzodiazepines or sedating antidepressants at bedtime.

During NREM sleep
May be restricted to Stage 3-4
Common in Males with Family History prevalence is 30% at age 4 y
10% at age 6 y 5% at age 10 y 3% at age 12 y 1% at age 15 y.
Owens, 2011

Usually during first 1/3 of night Usually only one event/night Common in Toddler and school-aged kids. prevalence rates 15% in children ages 3-13 yr. co-occur with sleepwalking and sleep terrors Usually resolve with time Not tired the next day No stereotypic motor movements Last 5-30 minutes
Stores, 2009

parent education and reassurance
good sleep hygiene
avoidance of exacerbating factors such as sleep deprivation and caffeine.
Scheduled awakenings, parent wake the child 15 to 30 min before the time of first parasomnia episode.
Pharmacotherapy is rarely necessary, include benzodiazepines and tricyclic antidepressants.
Stores, 2009

• Have a set bedtime and bedtime routine• Bedtime and wake-up time should be the
same time on school & non-school nights. • No more than 1hour difference from one
day to another.• Make the hour before sleep quiet time.• Avoid high-energy activities before bed.
Owens, 2011

• Don't go to bed hungry, but avoid Heavy meals.
• Avoid caffeine products before bedtime. • spend time outside every day and involve
in regular exercise.• Keep bedroom quiet and dark with
comfortable temperature • Don't use bedroom for punishment.
Owens, 2011

• Naps should be short (no > 1hr) and scheduled in the early to midafternoon.
• Keep TV out of child's bedroom. • Use bed for sleeping only. Don't study,
read, watch TV on bed.• Relaxing, calm, enjoyable activities help
you to get to sleep. • Smoking disturbs sleep. • Don't use sleeping pills
Owens, 2011

Foods That Helps You Sleep Better
tryptophan in it convert to serotonin & melatonin which induces sleep, Ca, Mg helps m. relaxation
Cherries rich source of melatonin
rich in Vit. B6 for melatonin production
Kale
source of sleep inducing agents (K, Ca, Mg, Vit.B6)
salmon & tuna Oat

All Sleep Phenomenon could
be a Seizure…

Anything that is recurrent, stereotyped, and inappropriate may be manifestation of a seizure
Some forms of epilepsy occur more commonly during sleep than during wakefulness
Most often confused with sleep terrors,
More common in the first 2 hours of sleep, or around 4-6 am.
More common in kids than adults.
Nocturnal seizuresNocturnal seizures

REFERENCES
• Gerd Lehmkuhl, Alfred Wiater, Alexander Mitschke, Leonie Fricke-Oerkermann (2008): Sleep Disorders in Children Beginning School: Their Causes and Effects. Dtsch Arztebl Int; 105(47): 809–14
• Judith A. Owens (2011): sleep disorders in Nelson text book of pediatrics. Chapter17.
• Bradley TD, Floras JS: Obstructive sleep apnoea and its cardiovascular consequences. Lancet 2009; 373:82-90.
• Khatwa U, Kothare SV: Restless legs syndrome and periodic limb movements disorder in the pediatric population. Curr Opin Pulm Med 2010; 16:559-567.
• Stores G: Aspects of parasomnias in children and adolescence. Arch Dis Child 2009; 94:63-69.