Pediatric Readmissions After Hospitalizations for Lower … · substantial morbidity and mortality....
11
Pediatric Readmissions After Hospitalizations for Lower Respiratory Infections Mari M. Nakamura, MD, MPH, a,b,c Alan M. Zaslavsky, PhD, d Sara L. Toomey, MD, MPhil, MSc, MPH, a,c Carter R. Petty, MA, e Maria C. Bryant, BA, a Alexandra T. Geanacopoulos, BA, a Ashish K. Jha, MD, MPH, f,g,h Mark A. Schuster, MD, PhD a,c abstract BACKGROUND AND OBJECTIVE: Lower respiratory infections (LRIs) are among the most common reasons for pediatric hospitalization and among the diagnoses with the highest number of readmissions. Characterizing LRI readmissions would help guide efforts to prevent them. We assessed variation in pediatric LRI readmission rates, risk factors for readmission, and readmission diagnoses. METHODS: We analyzed 2008–2009 Medicaid Analytic eXtract data for patients <18 years of age in 26 states. We identified LRI hospitalizations based on a primary diagnosis of bronchiolitis, influenza, or community-acquired pneumonia or a secondary diagnosis of one of these LRIs plus a primary diagnosis of asthma, respiratory failure, or sepsis/bacteremia. Readmission rates were calculated as the proportion of hospitalizations followed by ≥ 1 unplanned readmission within 30 days. We used logistic regression with fixed effects for patient characteristics and a hospital random intercept to case-mix adjust rates and assess risk factors. RESULTS: Of 150 590 LRI hospitalizations, 8233 (5.5%) were followed by ≥ 1 readmission. The median adjusted hospital readmission rate was 5.2% (interquartile range: 5.1%–5.4%), and rates varied across hospitals (P < .0001). Infants (patients <1 year of age), boys, and children with chronic conditions were more likely to be readmitted. The most common primary diagnoses on readmission were LRIs (48.2%), asthma (10.0%), fluid/electrolyte disorders (3.4%), respiratory failure (3.3%), and upper respiratory infections (2.7%). CONCLUSIONS: LRI readmissions are common and vary across hospitals. Multiple risk factors are associated with readmission, indicating potential targets for strategies to reduce readmissions. Readmission diagnoses sometimes seem related to the original LRI. Divisions of a General Pediatrics and b Infectious Diseases, and e Clinical Research Center, Boston Children’s Hospital, Boston, Massachusetts; Departments of c Pediatrics and d Health Care Policy, Harvard Medical School, and f Department of Health Policy and Management, Harvard T.H. Chan School of Public Health, Harvard University, Boston, Massachusetts; g Division of General Medicine, Brigham and Women’s Hospital, Boston, Massachusetts; and h Veterans Affairs Boston Healthcare System, Boston, Massachusetts Dr Nakamura conceptualized and designed the study, participated in analysis and interpretation of the data, drafted the initial manuscript, and revised the manuscript critically for important intellectual content; Dr Zaslavsky, Ms Bryant, Ms Geanacopoulos, and Dr Jha participated in analysis and interpretation of the data and revised the manuscript critically for important intellectual content; Dr Toomey participated in acquisition, analysis, and interpretation of the data and revised the manuscript critically for important intellectual content; Mr Petty performed the analysis, participated in interpretation of the data, and revised the manuscript critically for important intellectual content; Dr Schuster conceptualized and designed the study, participated in acquisition, analysis, and interpretation of the data, and revised the manuscript critically for important intellectual content; and all authors approved the final manuscript as submitted To cite: Nakamura MM, Zaslavsky AM, Toomey SL, et al. Pediatric Readmissions After Hospitalizations for Lower Respiratory Infections. Pediatrics. 2017; 140(2):e20160938 WHAT’S KNOWN ON THIS SUBJECT: Readmission rates are widely used as a measure of health care quality. Lower respiratory infections (LRIs; bronchiolitis, influenza, and community-acquired pneumonia) are among the most common reasons for pediatric hospitalizations and lead to numerous readmissions. WHAT THIS STUDY ADDS: In a large, multistate sample of Medicaid-insured children, readmission rates after LRI admissions varied across hospitals. LRIs were the most common readmission diagnosis, suggesting that some readmissions were related to the initial admission. ARTICLE PEDIATRICS Volume 140, number 2, August 2017:e20160938 by guest on April 27, 2020 www.aappublications.org/news Downloaded from
Transcript of Pediatric Readmissions After Hospitalizations for Lower … · substantial morbidity and mortality....

Pediatric Readmissions After Hospitalizations for Lower Respiratory InfectionsMari M. Nakamura, MD, MPH, a, b, c Alan M. Zaslavsky, PhD, d Sara L. Toomey, MD, MPhil, MSc, MPH, a, c Carter R. Petty, MA, e Maria C. Bryant, BA, a Alexandra T. Geanacopoulos, BA, a Ashish K. Jha, MD, MPH, f, g, h Mark A. Schuster, MD, PhDa, c
abstractBACKGROUND AND OBJECTIVE: Lower respiratory infections (LRIs) are among the most common reasons for pediatric hospitalization and among the diagnoses with the highest number of readmissions. Characterizing LRI readmissions would help guide efforts to prevent them. We assessed variation in pediatric LRI readmission rates, risk factors for readmission, and readmission diagnoses.METHODS: We analyzed 2008–2009 Medicaid Analytic eXtract data for patients <18 years of age in 26 states. We identified LRI hospitalizations based on a primary diagnosis of bronchiolitis, influenza, or community-acquired pneumonia or a secondary diagnosis of one of these LRIs plus a primary diagnosis of asthma, respiratory failure, or sepsis/bacteremia. Readmission rates were calculated as the proportion of hospitalizations followed by ≥1 unplanned readmission within 30 days. We used logistic regression with fixed effects for patient characteristics and a hospital random intercept to case-mix adjust rates and assess risk factors.RESULTS: Of 150 590 LRI hospitalizations, 8233 (5.5%) were followed by ≥1 readmission. The median adjusted hospital readmission rate was 5.2% (interquartile range: 5.1%–5.4%), and rates varied across hospitals (P < .0001). Infants (patients <1 year of age), boys, and children with chronic conditions were more likely to be readmitted. The most common primary diagnoses on readmission were LRIs (48.2%), asthma (10.0%), fluid/electrolyte disorders (3.4%), respiratory failure (3.3%), and upper respiratory infections (2.7%).CONCLUSIONS: LRI readmissions are common and vary across hospitals. Multiple risk factors are associated with readmission, indicating potential targets for strategies to reduce readmissions. Readmission diagnoses sometimes seem related to the original LRI.
Divisions of aGeneral Pediatrics and bInfectious Diseases, and eClinical Research Center, Boston Children’s Hospital, Boston, Massachusetts; Departments of cPediatrics and dHealth Care Policy, Harvard Medical School, and fDepartment of Health Policy and Management, Harvard T.H. Chan School of Public Health, Harvard University, Boston, Massachusetts; gDivision of General Medicine, Brigham and Women’s Hospital, Boston, Massachusetts; and hVeterans Affairs Boston Healthcare System, Boston, Massachusetts
Dr Nakamura conceptualized and designed the study, participated in analysis and interpretation of the data, drafted the initial manuscript, and revised the manuscript critically for important intellectual content; Dr Zaslavsky, Ms Bryant, Ms Geanacopoulos, and Dr Jha participated in analysis and interpretation of the data and revised the manuscript critically for important intellectual content; Dr Toomey participated in acquisition, analysis, and interpretation of the data and revised the manuscript critically for important intellectual content; Mr Petty performed the analysis, participated in interpretation of the data, and revised the manuscript critically for important intellectual content; Dr Schuster conceptualized and designed the study, participated in acquisition, analysis, and interpretation of the data, and revised the manuscript critically for important intellectual content; and all authors approved the final manuscript as submitted To cite: Nakamura MM, Zaslavsky AM, Toomey SL, et al. Pediatric Readmissions
After Hospitalizations for Lower Respiratory Infections. Pediatrics. 2017; 140(2):e20160938
WhaT’s KnoWn on This subjecT: Readmission rates are widely used as a measure of health care quality. Lower respiratory infections (LRIs; bronchiolitis, influenza, and community-acquired pneumonia) are among the most common reasons for pediatric hospitalizations and lead to numerous readmissions.
WhaT This sTudy adds: In a large, multistate sample of Medicaid-insured children, readmission rates after LRI admissions varied across hospitals. LRIs were the most common readmission diagnosis, suggesting that some readmissions were related to the initial admission.
ArticlePEDIATRICS Volume 140, number 2, August 2017:e20160938 by guest on April 27, 2020www.aappublications.org/newsDownloaded from

Because factors other than health care quality influence readmissions, including natural disease course, family and community supports, and sociodemographic factors, using readmission rates as a quality measure is controversial.1 – 3 Nevertheless, reducing hospital readmissions has become a widespread quality improvement goal. Readmissions are generally undesirable because they disrupt the lives of patients and families, 4 – 7 expose patients to the risk of harms associated with hospitalization, 8 and are costly.9 – 12 Hain et al13 found that 20% of pediatric 15-day readmissions “were more likely preventable... by changing care or discharge planning during the index admission.” Using chart review and interviews with parents, adolescent patients, and providers, Toomey et al14 determined that 29.5% of pediatric 30-day readmissions were potentially preventable.
As part of the Pediatric Quality Measures Program under the Centers for Medicare & Medicaid Services and the Agency for Healthcare Research and Quality, we developed a publicly available measure, endorsed by the National Quality Forum, to assess readmissions after hospitalization for lower respiratory infections (LRIs).15, 16 We focused on LRIs (bronchiolitis, influenza, and community-acquired pneumonia) because these conditions are prevalent in children and result in substantial morbidity and mortality. Bronchiolitis due to respiratory syncytial virus is the top reason for hospitalization of children aged <1 year.17 Pneumonia and influenza are among the top 10 reasons for hospitalization in children ≤17 years of age and the top 10 causes of death in children aged 29 days to 9 years.18, 19
Few studies have investigated readmissions after pediatric LRI hospitalizations, but findings to date indicate that such readmissions are common and account for a large proportion of overall pediatric
readmissions.20, 21 Using our LRI readmission measure, we examined readmissions after LRI acute care hospitalizations in a large sample of Medicaid-insured children. We assessed whether readmission performance varied across hospitals. We also examined risk factors for readmissions and determined the most common primary diagnoses on readmission, thus identifying potential targets for strategies to reduce LRI readmissions.
MeThods
data and study Population
We used 2008–2009 Medicaid Analytic eXtract inpatient claims data for 26 states (Supplemental Information), 22 selected based on the quality and completeness of encounter data. We evaluated hospitalizations with discharge dates from December 1, 2007 to November 30, 2009. Our study population consisted of patients aged <18 years at the time of the initial LRI admission, hereafter referred to as the index admission. The Boston Children’s Hospital Institutional Review Board approved the study with a waiver of informed consent.
definitions and outcome Measures
Our readmission measure identifies LRI admissions as those with either (1) a primary International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) diagnosis code for bronchiolitis, influenza, or community-acquired pneumonia, or (2) a secondary diagnosis code for one of these LRIs plus a primary diagnosis code for asthma, respiratory failure, or sepsis/bacteremia (Supplemental Information). We compiled diagnosis codes for identifying LRI admissions by reviewing the literature for studies that used ICD-9-CM codes for LRI case ascertainment, 23 –47 as well as by manually reviewing ICD-9-CM
code sets. We define a readmission as the first unplanned admission within 30 days of discharge from an LRI index hospitalization, where the readmission occurred at either the index hospital or a different hospital. To make observations independent and keep readmission rates from being dominated by relatively few patients with multiple readmissions within short time periods, repeated LRI admissions are counted as new index admissions only if they occurred >30 days after discharge from the previous index admission. If an inpatient claim has the same date for admission and discharge and this date was the same as the discharge date for an index admission, the claim is considered to be part of the index admission rather than indicative of a readmission. If a patient was transferred from 1 hospital to another during an index admission, records from the hospitals are combined and evaluated as a single index admission, and a potential subsequent readmission is attributed to the final hospital.
Our primary outcome measure was the hospital-level 30-day LRI readmission rate during the 2-year study period, defined as the number of LRI index admissions followed by ≥1 readmission within 30 days, divided by the total number of LRI index admissions at a given hospital during the study period.
exclusion criteria
The measure excludes admissions with missing or inconsistent data for key variables, including patient identifier; sex; dates of birth, admission, and discharge; diagnosis and procedure codes; disposition status; and hospital type. We include only hospitalizations at general acute care hospitals, defined as including both children’s hospitals and non–children’s hospitals with a pediatric ward. We exclude records from specialty (eg, those focused on specific conditions, such as burns) and
NAKAMuRA et al2 by guest on April 27, 2020www.aappublications.org/newsDownloaded from

non–acute care (eg, rehabilitation) hospitals. We exclude index admissions during which a patient died or left against medical advice.
The measure excludes planned admissions, defined as those for a planned procedure or for chemotherapy (Supplemental Information), from readmissions based on the rationale that planned admissions are part of a patient’s intended course of care and are thus less likely to be related to health system quality. To identify planned procedure admissions, we developed an algorithm by asking pediatric clinicians in 14 procedure-oriented specialties to review procedures typically performed by their specialty and to indicate which procedures are planned >80% of the time and could serve as the primary reason for a hospitalization. Admissions for which the primary procedure coded was 1 of these procedures are excluded from readmissions.
In addition, the measure excludes hospitalizations for obstetric care, birth of healthy newborns, and mental health conditions (see Supplemental Information for detailed definitions). We exclude obstetric hospitalizations because obstetric care generally does not fall within the purview of pediatrics. We exclude hospitalizations for the birth of healthy newborns because these patients, unlike others, are not hospitalized for management of disease. Mental health hospitalizations are excluded because we found a negative correlation between readmission performance for mental health conditions and for other conditions (hospitals with high readmission rates for mental health hospitalizations tend to have low readmission rates for hospitalizations for other conditions and vice versa), suggesting that readmission performance for mental health conditions should be evaluated separately from performance for other conditions.
case-Mix adjustment and LRi Readmission Risk Factors
The measure adjusts readmission rates for age, sex, and chronic conditions at the index admission because distributions of these characteristics vary across hospitals, and although they are associated with readmission risk, they are independent of hospital quality of care.48 Age is specified by using developmentally relevant categories of <1, 1 to 4, 5 to 7, 8 to 11, and 12 to 17 years. We identify chronic conditions using the Agency for Healthcare Research and Quality Chronic Condition Indicator (CCI) system, which classifies ICD-9-CM diagnosis codes as chronic or acute and places each code into 1 of 18 mutually exclusive categories (organ systems, disease categories, or other categories) (Supplemental Information). The case-mix adjustment model incorporates a binary variable for each CCI category, indicating whether a patient has ≥1 chronic condition in that category. We exclude the category “Complications of pregnancy, childbirth, and the puerperium” because exclusion of obstetric hospitalizations leaves few or no patients with obstetric diagnosis codes, which could create model-fitting issues for the case-mix adjustment model. In addition, we model the effect of multiple types of chronic conditions on readmission risk by including a variable indicating the number of CCI categories in which a patient had ≥1 chronic condition. We use categories of 0 or 1, 2, 3, or ≥4 because few index admissions have diagnoses in >4 categories. We assessed each of the case-mix adjustment variables (age, sex, CCI category, and CCI count) as potential risk factors for readmission after hospitalization for LRI.
Because the purpose of the measure is assessment of health care quality, the measure does not adjust readmission rates for factors that could be related to both readmission risk and quality of care, such as length of stay or regional variation in readmission rates.
analyses
To compare the frequency of readmission after hospitalizations with a primary diagnosis of an LRI versus hospitalizations with other primary diagnoses, we calculated the number of readmissions in our total sample for each index admission primary diagnosis. Because we wished to compare readmissions after hospitalizations for LRI versus readmissions after hospitalizations for other conditions, we performed this analysis by using all index hospitalizations for our study cohort rather than just LRI index hospitalizations. Because it was not feasible to develop a complex case definition for each other possible condition, for this analysis only, we did not use the full LRI measure case definition (detailed above); rather, we evaluated all index hospitalizations based simply on their primary diagnosis code, identifying LRI index hospitalizations as those with a primary diagnosis code for an LRI.
To identify the most common reasons for readmission after an LRI index admission, we determined the most frequent primary diagnosis codes on readmission. To case-mix adjust readmission rates and assess risk factors for readmission, we used a 2-level mixed-effects logistic regression model with fixed effects for patient-level variables and a random intercept for each hospital. The model estimated 3 types of parameters. The coefficients of patient demographic and clinical characteristics represent the influence of these characteristics on predicted probabilities of readmission for an individual patient. The random intercept estimates for each hospital correspond to greater or lesser adjusted probability of readmission, after controlling for patient-level fixed effects, for patients discharged from each hospital. The estimated variance of the hospital random effects summarizes the amount of variation among the intercepts for different
PEDIATRICS Volume 140, number 2, August 2017 3 by guest on April 27, 2020www.aappublications.org/newsDownloaded from

hospitals and hence the amount of variation in adjusted readmission rates across hospitals, at least some of which may have been due to variation in health system quality. A 2-sided P < .05 was used as the criterion for statistical significance for this analysis. Finally, for hospitals with higher pediatric volumes (≥500 index admissions for any condition and ≥50 LRI index admissions over the 2-year study period), we determined the number of hospitals with adjusted readmission rates significantly better or worse than the overall unadjusted readmission rate across hospitals (ie, hospitals whose readmission rate confidence intervals did not overlap with the overall unadjusted readmission rate).
ResuLTs
Patient and hospital characteristics
Infants (<1 year of age) and young children (1–4 years of age) comprised the age groups with the largest share (47.0% and 36.9%, respectively) of 150 590 total LRI index admissions (Table 1). The majority of index admissions (89.6%) were for patients with no chronic conditions or chronic conditions in only 1 body system. Approximately one-quarter of index admissions (23.6%) occurred at children’s hospitals. Among the 1929 hospitals, 4.1% were children’s hospitals and 6.3% were teaching hospitals (Table 2). Approximately one-third of hospitals were in urban locations.
Readmission Rates and Variation
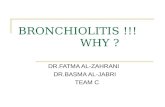
Applying the measure definition for an LRI index admission (ie, a primary diagnosis of bronchiolitis, influenza, or pneumonia, or a secondary diagnosis of one of these LRIs with a primary diagnosis of asthma, respiratory failure, or sepsis/bacteremia), 8233 of 150 590 total LRI index admissions were followed by ≥1 readmission (Fig 1). The overall unadjusted LRI readmission
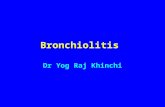
rate across all hospitals was thus 5.5%. Adjusted hospital-level readmission rates ranged from 3.8% to 8.8%, with a median adjusted hospital-level readmission rate of 5.2% (interquartile range: 5.1%–5.4%). Adjusted readmission rates varied significantly across hospitals (P < .0001). The estimated SD of the hospital random effects offers a sense of how much a patient’s readmission risk varied depending on which hospital provided his or her care; our results indicated that a patient whose probability of readmission was 5.2% (the overall average) at a hospital of median quality would have had a predicted probability of readmission of 6.5% if cared for at a hospital with a random effect 1 SD above the mean, whereas the same patient would have had a predicted probability of readmission of 4.2% at a hospital with a random effect 1 SD below the mean. Among the 338 hospitals with higher pediatric volume (≥500 index admissions for any condition and ≥50 LRI index admissions), we found that 2 had readmission rates significantly better and 5 had rates significantly worse than the overall unadjusted readmission rate across all hospitals (Fig 2).
index admission Primary diagnoses associated With the highest number of Readmissions
LRI was the index admission primary diagnosis with the highest number (6711) of 30-day readmissions, followed by asthma (1933), epilepsy and convulsions (1632), device- and procedure-related complications (1597), and anemia (1585).
diagnoses on Readmission
LRI was the primary diagnosis for 48.2% of LRI readmissions. The next most common primary readmission diagnoses were asthma (10.0%), fluid/electrolyte disorders (3.4%), respiratory failure (3.3%), and upper respiratory infections (2.7%).
Risk Factors for LRi Readmission
In our multivariate case-mix adjustment model, age had a nonlinear statistically significant relationship with LRI readmission risk (Table 3). Boys had a small but statistically significant increase in readmission risk (Table 3). Having ≥1 chronic condition in a CCI category was also associated with increased readmission risk for most categories, including neoplasms, neurologic disorders, and congenital anomalies. The odds ratios for having chronic conditions in 3 or ≥4 categories were <1, indicating that the effects of having chronic conditions in multiple CCI categories were less than the additive effects of conditions in individual categories. For example, supposing that subject
NAKAMuRA et al4
TabLe 1 Patient Characteristics (Total N = 150 590)
Patient Characteristic Index Admissions, n (%)
Age, y <1 70 781 (47.0) 1–4 55 532 (36.9) 5–7 11 498 (7.6) 8–11 6 962 (4.6) 12–17 5 817 (3.9)Sex Girl 65 417 (43.4)CCI count 0 or 1 body system 134 879 (89.6) 2 body systems 10 036 (6.7) 3 body systems 3 732 (2.5) ≥4 body systems 1 943 (1.3)Race/ethnicity Asian/Pacific Islander 1 954 (1.4) African American 32 090 (23.0) Latino 46 627 (33.4) Mixed 1 285 (0.9) Native American 7 230 (5.2) White 50 606 (36.2)
TabLe 2 Hospital Characteristics (Total N = 1929)
Hospital Characteristic Hospitals, n (%)
Children’s hospital 79 (4.1)Teaching hospital 119 (6.3)Rural/urban locationa
urban 662 (34.4) Suburban 97 (5.0) Large town 408 (21.2) Small town 502 (26.1) Rural 255 (13.2)
a Rural/urban location could not be determined for 5 hospitals.
by guest on April 27, 2020www.aappublications.org/newsDownloaded from

1 had conditions in organ systems A, B, and C, whereas subject 2 only had conditions in organ system A, subject 3 only had conditions in organ system B, and subject 4 only had conditions in organ system C, the combined impact of subject 1’s conditions on his or her readmission risk may have been smaller than the sum (impact of subject 2’s conditions + impact of subject 3’s conditions + impact of subject 4’s conditions).
discussion
Analyzing a large, multistate sample of Medicaid-insured children
cared for at both children’s and non–children’s hospitals, we found a median adjusted hospital-level LRI readmission rate of 5.2% (interquartile range: 5.1%–5.4%). Using as a comparator the overall unadjusted readmission rate across hospitals of 5.5%, only 7 of the 338 high-volume hospitals were outliers. However, readmission rates varied significantly across hospitals. Although our study could not offer insight into the preventability of readmissions and thus whether the hospital-level rate of 5.2% was higher than it should have been, the presence of significant variation suggests that at least some hospitals
have room to improve their readmission performance for patients with LRIs. We also found that LRIs are the index admission diagnosis followed by the greatest number of 30-day readmissions, indicating that efforts to reduce LRI readmissions, to the extent that some of them could be prevented, may be a worthwhile focus for reducing pediatric readmissions overall.
For 48.2% of readmissions after an LRI index admission, an LRI was also the primary diagnosis on readmission, with asthma and respiratory failure among the next most common
PEDIATRICS Volume 140, number 2, August 2017 5
FiGuRe 1Study cohort, LRI index admissions, and readmissions. a Pediatric admissions are for patients who were ≤18 years, 29 days of age at the time of admission.
by guest on April 27, 2020www.aappublications.org/newsDownloaded from

readmission diagnoses. These results suggest that some readmissions may have been related to the index admission (although related readmissions are not necessarily preventable; related readmissions could also reflect clinical fluctuations that are part of the natural disease course). At the same time, the occurrence of diagnoses other than LRI for just over half of readmissions suggests that some readmissions were unrelated to the index admission or that some index admission diagnoses were simply incorrect.
Infants and subjects with various types of chronic conditions were at greatest risk of readmission, perhaps reflecting that these populations are also at greatest risk of severe or complicated LRIs.49 – 51 These patients may be the best target groups for efforts to decrease readmissions. Our study was not designed to determine definite strategies for preventing readmissions, but to the degree that some readmissions could be prevented, optimizing care during the initial admission may help to
reduce readmissions. For example, implementation of a management algorithm for complicated pneumonia at a tertiary children’s hospital was associated with decreased readmissions without increased lengths of stay.52 One important set of interventions to improve inpatient LRI care may be strategies to avoid premature discharges. We do not propose increased lengths of stay regardless of clinical status as a solution to preventing readmissions. Rather, strategies such as standardized, evidence-based discharge criteria might help to prevent some patients from being discharged before they are ready while avoiding longer-than-necessary hospitalizations for others. Implementation of a clinical pathway for bronchiolitis was associated with a reduction in 14-day readmissions, seemingly due to improvements in discharge planning and achievement of explicit clinical outcomes before discharge.53
In addition to improvements in inpatient care, optimizing transitions and postdischarge care to prevent,
promptly detect, and effectively address clinical worsening may also be key in preventing LRI readmissions. Recovery after a hospitalization for an LRI can take several days and require ongoing care by parents or other caregivers.54 Studies assessing the effectiveness and cost-effectiveness of interventions to reduce pediatric readmissions are still rare, but promising approaches have included 1-on-1 inpatient education and postdischarge support by telephone or clinic visit.55, 56
Our finding of an overall unadjusted 30-day readmission rate of 5.5% after LRI index admissions was the same as the all-cause readmission rate reported by Bardach et al57 for pediatric respiratory disease (asthma, pneumonia, and bronchiolitis) hospitalizations in a multistate, all-payer sample of children admitted to children’s and non–children’s hospitals. A 30-day all-cause readmission rate of 7.7% was found by Neuman et al21 for patients hospitalized for pneumonia at 43 freestanding children’s hospitals, possibly reflecting the tendency of these institutions to care for children with greater severity of illness or underlying medical complexity. It remains true for LRI hospitalizations, as for other hospitalizations, that the “optimal” readmission rate is not known. Even if some readmissions could be prevented, others would be appropriate and unavoidable, and our study was not designed to distinguish among these possibilities. Our study was consistent with previous studies focusing on bronchiolitis and pneumonia readmissions in finding significant variation across hospitals in LRI readmission performance.23, 58 Likewise, our results corresponded with those of previous investigations in demonstrating that younger children and those with chronic conditions are most at risk for LRI readmission.21, 50, 57
Among the strengths of our study was the inclusion of pediatric admissions from both children’s and
NAKAMuRA et al6
FiGuRe 2Adjusted hospital-level readmission rates for hospitals with high pediatric volume. The red line indicates the overall unadjusted all-hospital rate of 5.5%. Intervals are 60% posterior intervals under the case-mix adjustment model, such that hospitals whose rates do not overlap with the overall rate are 80% certain to have better or worse performance than average.
by guest on April 27, 2020www.aappublications.org/newsDownloaded from

non–children’s hospitals in half of US states. Our data source, Medicaid claims, captured readmissions to any hospital rather than just the index hospital. However, the study also had several limitations. Because the latest data available to us were from 2008 to 2009, our findings do not reflect changes that may have occurred in LRI readmissions more recently, including possible reductions in readmission rates that may have resulted from increased focus on readmissions. In using claims data, we relied on ICD-9-CM codes for identification of index admissions, chronic conditions, conditions and procedures for exclusions, and diagnoses on readmission. ICD-9-CM codes offer limited detail regarding severity of illness, and they may not fully reflect a patient’s clinical picture.59 Furthermore, although our planned procedure algorithm was developed with input from clinical experts, it has not been externally validated. In addition, our use of Medicaid claims allowed us to examine readmissions for a potentially high-risk population, 60 but it precluded evaluating the relationship between insurance status and readmission risk. We also lacked data to investigate other factors potentially associated with LRI readmission, including other socioeconomic factors, such as family income and parental/caregiver education level, and community factors, such as access to primary care.
concLusions
Using a large sample of Medicaid-insured children hospitalized at
children’s and non–children’s hospitals, we determined that LRI readmission rates vary across hospitals, suggesting that there is room for improvement for at least some hospitals. Readmissions could be a fruitful target for improving inpatient and postdischarge care for LRIs.
PEDIATRICS Volume 140, number 2, August 2017 7
and agree to be accountable for all aspects of the work in ensuring questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
doi: https:// doi. org/ 10. 1542/ peds. 2016- 0938
Accepted for publication Apr 7, 2017
Address correspondence to Mari M. Nakamura, MD, MPH, Division of Infectious Diseases, Boston Children’s Hospital, BCH 3118, LO-650, 300 Longwood Ave, Boston, MA 02115. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2017 by the American Academy of Pediatrics
abbReViaTions
CCI: Chronic Condition IndicatorICD-9-CM: International
Classification of Diseases, Ninth Revision, Clinical Modification
LRI: lower respiratory infection
TabLe 3 Risk Factors for LRI Readmission
OR (95% CI) P
Age, y <1 Reference — 1–4 0.60 (0.57–0.64) <.001 5–7 0.44 (0.40–0.49) <.001 8–11 0.41 (0.36–0.46) <.001 12–17 0.53 (0.47–0.59) <.001Sex Girl Reference — Boy 1.11 (1.06–1.16) <.001CCIa, b
1: Infectious and parasitic disease 1.49 (0.58–3.86) .408 2: Neoplasms 2.86 (2.21–3.70) <.001 3: Endocrine, nutritional, and metabolic diseases and
immunity disorders2.18 (1.94–2.46) <.001
4: Diseases of blood and blood-forming organs 1.76 (1.57–1.96) <.001 5: Mental disorders 1.47 (1.29–1.68) <.001 6: Diseases of the nervous system and sense organs 2.45 (2.19–2.75) <.001 7: Diseases of the circulatory system 1.87 (1.63–2.14) <.001 8: Diseases of the respiratory system 1.19 (1.11–1.26) <.001 9: Diseases of the digestive system 2.01 (1.82–2.21) <.001 10: Diseases of the genitourinary system 2.05 (1.47–2.86) <.001 12: Diseases of the skin and subcutaneous tissue 1.57 (1.14–2.17) .006 13: Diseases of the musculoskeletal system 1.74 (1.35–2.25) <.001 14: Congenital anomalies 2.16 (1.98–2.36) <.001 15: Certain conditions originating in the perinatal period 1.38 (0.58–3.29) .466 16: Symptoms, signs, and ill-defined conditions 1.06 (0.65–1.72) .806 17: Injury and poisoning 2.37 (0.45–12.45) .308 18: Factors influencing health status and contact with health
services2.80 (2.49–3.14) <.001
CCI count 0 or 1 body systems Reference — 2 body systems 1.00 (0.89–1.12) .994 3 body systems 0.75 (0.62–0.90) .002 ≥4 body systems 0.38 (0.29–0.50) <.001
CI, confidence interval; OR, odds ratio. —, no P value.a The reference group for each CCI variable is no condition in the body system.b We excluded the CCI variable for body system 11, “Complications of pregnancy, childbirth, and the puerperium, ” because patients who have a primary diagnosis code for an obstetric condition or any diagnosis or procedure code for delivery are excluded from the cohort.
by guest on April 27, 2020www.aappublications.org/newsDownloaded from

ReFeRences
1. Ashton CM, Wray NP. A conceptual framework for the study of early readmission as an indicator of quality of care. Soc Sci Med. 1996;43(11):1533–1541
2. Jencks SF. Defragmenting care. Ann Intern Med. 2010;153(11):757–758
3. Nakamura MM, Toomey SL, Zaslavsky AM, et al. Measuring pediatric hospital readmission rates to drive quality improvement. Acad Pediatr. 2014;14(suppl 5):S39–S46
4. Marks C, Loehrer S, McCarthy D. Hospital readmissions: measuring for improvement, accountability, and patients. Issue Brief (Commonw Fund). 2013;24:1–8
5. Van Horn ER, Kautz D. Promotion of family integrity in the acute care setting: a review of the literature. Dimens Crit Care Nurs. 2007;26(3):101–107; quiz 108–109
6. Lapillonne A, Regnault A, Gournay V, et al. Impact on parents of bronchiolitis hospitalization of full-term, preterm and congenital heart disease infants. BMC Pediatr. 2012;12:171
7. Schuster MA, Chung PJ, Vestal KD. Children with health issues. Future Child. 2011;21(2):91–116
8. Calfee DP. Crisis in hospital-acquired, healthcare-associated infections. Annu Rev Med. 2012;63:359–371
9. Berry JG, Hall DE, Kuo DZ, et al. Hospital utilization and characteristics of patients experiencing recurrent readmissions within children’s hospitals. JAMA. 2011;305(7):682–690
10. Friedman B, Basu J. The rate and cost of hospital readmissions for preventable conditions. Med Care Res Rev. 2004;61(2):225–240
11. Leader S, Jacobson P, Marcin J, Vardis R, Sorrentino M, Murray D. A method for identifying the financial burden of hospitalized infants on families. Value Health. 2002;5(1):55–59
12. Romley JA, Shah AK, Chung PJ, Elliott MN, Vestal KD, Schuster MA. Family-provided health care for children with
special health care needs. Pediatrics. 2017;139(1):e20161287
13. Hain PD, Gay JC, Berutti TW, Whitney GM, Wang W, Saville BR. Preventability of early readmissions at a children’s hospital. Pediatrics. 2013;131(1). Available at: www. pediatrics. org/ cgi/ content/ full/ 131/ 1/ e171
14. Toomey SL, Peltz A, Loren S, et al. Potentially preventable 30-day hospital readmissions at a children’s hospital. Pediatrics. 2016;138(2):e20154182
15. Agency for Healthcare Research and Quality. Pediatric quality measures program: quality measures. Available at: www. ahrq. gov/ policymakers/ chipra/ factsheets/ index. html. Accessed June 2, 2015
16. National Quality Forum. NQF: pediatric lower respiratory infection readmission measure. Available at: www. qualityforum. org/ QPS/ 2414. Accessed December 16, 2015
17. Paes BA, Mitchell I, Banerji A, Lanctôt KL, Langley JM. A decade of respiratory syncytial virus epidemiology and prophylaxis: translating evidence into everyday clinical practice. Can Respir J. 2011;18(2):e10–e19
18. Yu H, Wier LM, Elixhauser A. Hospital Stays for Children, 2009: Statistical Brief #118. Rockville, MD: Agency for Health Care Policy and Research (uS); 2006. Available at: www. ncbi. nlm. nih. gov/ books/ NBK65134/ . Accessed April 30, 2013
19. Heron M. Deaths: Leading Causes for 2010. Hyattsville, MD: National Center for Health Statistics; 2013
20. Berry JG, Toomey SL, Zaslavsky AM, et al. Pediatric readmission prevalence and variability across hospitals. JAMA. 2013;309(4):372–380
21. Neuman MI, Hall M, Gay JC, et al. Readmissions among children previously hospitalized with pneumonia. Pediatrics. 2014;134(1):100–109
22. Centers for Medicare & Medicaid Services. Medicaid Analytic eXtract (MAX) general information. Available at: www. cms. gov/ Research- Statistics- Data- and- Systems/ Computer- Data- and- Systems/ MedicaidDataSourc esGenInfo/ MAXGeneralInforma tion. html. Accessed October 7, 2013
23. Christakis DA, Cowan CA, Garrison MM, Molteni R, Marcuse E, Zerr DM. Variation in inpatient diagnostic testing and management of bronchiolitis. Pediatrics. 2005;115(4):878–884
24. Howard TS, Hoffman LH, Stang PE, Simoes EA. Respiratory syncytial virus pneumonia in the hospital setting: length of stay, charges, and mortality. J Pediatr. 2000;137(2):227–232
25. Joffe S, Escobar GJ, Black SB, Armstrong MA, Lieu TA. Rehospitalization for respiratory syncytial virus among premature infants. Pediatrics. 1999; 104(4 pt 1):894–899
26. Kemper AR, Kennedy EJ, Dechert RE, Saint S. Hospital readmission for bronchiolitis. Clin Pediatr (Phila). 2005;44(6):509–513
27. Nachman SA, Navaie-Waliser M, Qureshi MZ. Rehospitalization with respiratory syncytial virus after neonatal intensive care unit discharge: a 3-year follow-up. Pediatrics. 1997;100(6). Available at: www. pediatrics. org/ cgi/ content/ full/ 100/ 6/ e8
28. Stockman LJ, Curns AT, Anderson LJ, Fischer-Langley G. Respiratory syncytial virus-associated hospitalizations among infants and young children in the united States, 1997-2006. Pediatr Infect Dis J. 2012;31(1):5–9
29. Hassan F, Lewis TC, Davis MM, Gebremariam A, Dombkowski K. Hospital utilization and costs among children with influenza, 2003. Am J Prev Med. 2009;36(4):292–296
30. Marsden-Haug N, Foster VB, Gould PL, Elbert E, Wang H, Pavlin JA. Code-based syndromic surveillance for influenzalike
NAKAMuRA et al8
FinanciaL discLosuRe: The authors have indicated they have no financial relationships relevant to this article to disclose.
FundinG: Support for this work was provided by the uS Department of Health and Human Services Agency for Healthcare Research and Quality and Centers for Medicare & Medicaid Services, CHIPRA Pediatric Quality Measures Program Centers of Excellence under grant numbers u18 HS 020513 and u18 HS 025299 (principal investigator: Dr Schuster). The content is solely the responsibility of the authors and does not necessarily represent the official views of the Agency for Healthcare Research and Quality.
PoTenTiaL conFLicT oF inTeResT: The authors have indicated they have no potential conflicts of interest to disclose.
by guest on April 27, 2020www.aappublications.org/newsDownloaded from

illness by International Classification of Diseases, Ninth Revision. Emerg Infect Dis. 2007;13(2):207–216
31. Placzek H, Madoff L. Identification of influenza cases during the H1N1 pandemic in Massachusetts using population-based hospital discharge data. PLoS Curr. 2011;3:RRN1256
32. Simonsen L, Taylor RJ, Young-Xu Y, Haber M, May L, Klugman KP. Impact of pneumococcal conjugate vaccination of infants on pneumonia and influenza hospitalization and mortality in all age groups in the united States. MBio. 2011;2(1):e00309–e00310
33. Yorita KL, Holman RC, Sejvar JJ, Steiner CA, Schonberger LB. Infectious disease hospitalizations among infants in the united States. Pediatrics. 2008;121(2):244–252
34. Christensen KLY, Holman RC, Steiner CA, Sejvar JJ, Stoll BJ, Schonberger LB. Infectious disease hospitalizations in the united States. Clin Infect Dis. 2009;49(7):1025–1035
35. Cohen SA, Klassen AC, Ahmed S, Agree EM, Louis TA, Naumova EN. Trends for influenza and pneumonia hospitalization in the older population: age, period, and cohort effects. Epidemiol Infect. 2010;138(8):1135–1145
36. Simonsen L, Conn LA, Pinner RW, Teutsch S. Trends in infectious disease hospitalizations in the united States, 1980-1994. Arch Intern Med. 1998;158(17):1923–1928
37. Aronsky D, Haug PJ, Lagor C, Dean NC. Accuracy of administrative data for identifying patients with pneumonia. Am J Med Qual. 2005;20(6):319–328
38. Jackson ML, Neuzil KM, Thompson WW, et al. The burden of community-acquired pneumonia in seniors: results of a population-based study. Clin Infect Dis. 2004;39(11):1642–1650
39. Yu O, Nelson JC, Bounds L, Jackson LA. Classification algorithms to improve the accuracy of identifying patients hospitalized with community-acquired pneumonia using administrative data. Epidemiol Infect. 2011;139(9):1296–1306
40. Jackson LA, Neuzil KM, Yu O, et al; Vaccine Safety Datalink. Effectiveness of pneumococcal polysaccharide vaccine in older adults. N Engl J Med. 2003;348(18):1747–1755
41. Zhou F, Kyaw MH, Shefer A, Winston CA, Nuorti JP. Health care utilization for pneumonia in young children after routine pneumococcal conjugate vaccine use in the united States. Arch Pediatr Adolesc Med. 2007;161(12):1162–1168
42. Weissman JS, Ayanian JZ, Chasan-Taber S, Sherwood MJ, Roth C, Epstein AM. Hospital readmissions and quality of care. Med Care. 1999;37(5):490–501
43. Nelson JC, Jackson M, Yu O, et al. Impact of the introduction of pneumococcal conjugate vaccine on rates of community acquired pneumonia in children and adults. Vaccine. 2008;26(38):4947–4954
44. van de Garde EMW, Oosterheert JJ, Bonten M, Kaplan RC, Leufkens HGM. International classification of diseases codes showed modest sensitivity for detecting community-acquired pneumonia. J Clin Epidemiol. 2007;60(8):834–838
45. Lindenauer PK, Normand S-LT, Drye EE, et al. Development, validation, and results of a measure of 30-day readmission following hospitalization for pneumonia. J Hosp Med. 2011;6(3):142–150
46. Palepu A, Sun H, Kuyper L, Schechter MT, O’Shaughnessy MV, Anis AH. Predictors of early hospital readmission in HIV-infected patients with pneumonia. J Gen Intern Med. 2003;18(4):242–247
47. Joynt KE, Orav EJ, Jha AK. Thirty-day readmission rates for Medicare beneficiaries by race and site of care. JAMA. 2011;305(7):675–681
48. Eselius LL, Cleary PD, Zaslavsky AM, Huskamp HA, Busch SH. Case-mix adjustment of consumer reports about managed behavioral health care and health plans. Health Serv Res. 2008;43(6):2014–2032
49. Brogan TV, Hall M, Sills MR, et al. Hospital readmissions among children with H1N1 influenza infection. Hosp Pediatr. 2014;4(6):348–358
50. Leyenaar JK, Lagu T, Shieh M-S, Pekow PS, Lindenauer PK. Management and outcomes of pneumonia among children with complex chronic conditions. Pediatr Infect Dis J. 2014;33(9):907–911
51. Keren R, Zaoutis TE, Bridges CB, et al. Neurological and neuromuscular disease as a risk factor for respiratory failure in children hospitalized with influenza infection. JAMA. 2005;294(17):2188–2194
52. Pillai D, Song X, Pastor W, et al. Implementation and impact of a consensus diagnostic and management algorithm for complicated pneumonia in children. J Investig Med. 2011;59(8):1221–1227
53. Cheney J, Barber S, Altamirano L, et al. A clinical pathway for bronchiolitis is effective in reducing readmission rates. J Pediatr. 2005;147(5):622–626
54. Robbins JM, Kotagal uR, Kini NM, Mason WH, Parker JG, Kirschbaum MS. At-home recovery following hospitalization for bronchiolitis. Ambul Pediatr. 2006;6(1):8–14
55. Auger KA, Kenyon CC, Feudtner C, Davis MM. Pediatric hospital discharge interventions to reduce subsequent utilization: a systematic review. J Hosp Med. 2014;9(4):251–260
56. Kirsch SD, Wilson LS, Harkins M, Albin D, Del Beccaro MA. Feasibility of using a pediatric call center as part of a quality improvement effort to prevent hospital readmission. J Pediatr Nurs. 2015;30(2):333–337
57. Bardach NS, Vittinghoff E, Berry JG, Asteria-Penaloza R, Dudley RA. Is there meaningful hospital performance variation in readmissions or revisits for children with respiratory illnesses? Available at: http:// www. abstracts2view. com/ pasall/ view. php? nu= PAS14L1_ 1440. 7. Accessed June 26, 2014
58. Brogan TV, Hall M, Williams DJ, et al. Variability in processes of care and outcomes among children hospitalized with community-acquired pneumonia. Pediatr Infect Dis J. 2012;31(10):1036–1041
59. Gidengil C, Mangione-Smith R, Bailey LC, et al. using Medicaid and CHIP claims data to support pediatric quality measurement: lessons from 3 centers of excellence in measure development. Acad Pediatr. 2014;14(suppl 5):S76–S81
60. Jiang HJ, Wier LM. All-cause hospital readmissions among non-elderly Medicaid patients, 2007: statistical brief #89. In: Healthcare Cost and Utilization Project (HCUP) Statistical Briefs. Rockville, MD: Agency for Health Care Policy and Research (uS); 2010. Available at: www. hcup- us. ahrq. gov/ reports/ statbriefs/ sb89. jsp. Accessed October 23, 2013
PEDIATRICS Volume 140, number 2, August 2017 9 by guest on April 27, 2020www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2016-0938 originally published online July 31, 2017; 2017;140;Pediatrics
Bryant, Alexandra T. Geanacopoulos, Ashish K. Jha and Mark A. SchusterMari M. Nakamura, Alan M. Zaslavsky, Sara L. Toomey, Carter R. Petty, Maria C.
Pediatric Readmissions After Hospitalizations for Lower Respiratory Infections
ServicesUpdated Information &
http://pediatrics.aappublications.org/content/140/2/e20160938including high resolution figures, can be found at:
Referenceshttp://pediatrics.aappublications.org/content/140/2/e20160938#BIBLThis article cites 53 articles, 10 of which you can access for free at:
Subspecialty Collections
nsition_-_discharge_planning_subhttp://www.aappublications.org/cgi/collection/continuity_of_care_traContinuity of Care Transition & Discharge Planninghttp://www.aappublications.org/cgi/collection/hospital_medicine_subHospital Medicinesubhttp://www.aappublications.org/cgi/collection/quality_improvement_Quality Improvement_management_subhttp://www.aappublications.org/cgi/collection/administration:practiceAdministration/Practice Managementfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtmlin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://www.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by guest on April 27, 2020www.aappublications.org/newsDownloaded from
http://www.aappublications.org/cgi/collection/continuity_of_care_transition_-_discharge_planning_sub

DOI: 10.1542/peds.2016-0938 originally published online July 31, 2017; 2017;140;Pediatrics
Bryant, Alexandra T. Geanacopoulos, Ashish K. Jha and Mark A. SchusterMari M. Nakamura, Alan M. Zaslavsky, Sara L. Toomey, Carter R. Petty, Maria C.
Pediatric Readmissions After Hospitalizations for Lower Respiratory Infections
http://pediatrics.aappublications.org/content/140/2/e20160938located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://pediatrics.aappublications.org/content/suppl/2017/07/20/peds.2016-0938.DCSupplementalData Supplement at:
1073-0397. ISSN:60007. Copyright © 2017 by the American Academy of Pediatrics. All rights reserved. Print
the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois,has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
by guest on April 27, 2020www.aappublications.org/newsDownloaded from