Pediatric non-traumatic Surgical Emergencies
80
Dr. H. Flageole Department of Surgery McMaster Children’s Hospital October 15, 2008
description
Dr. H. Flageole Department of Surgery McMaster Children’s Hospital October 15, 2008. Pediatric non-traumatic Surgical Emergencies. Objectives. To familiarize the resident with non-traumatic emergencies - PowerPoint PPT Presentation
Transcript of Pediatric non-traumatic Surgical Emergencies

Dr. H. FlageoleDepartment of SurgeryMcMaster Children’s HospitalOctober 15, 2008

Objectives
To familiarize the resident with non-traumatic emergencies
To familiarize the resident with surgical emergencies encountered in the newborn and early childhood periods.
Identify symptoms of significant disease
Recognize life-threatening surgical conditions

Acute Abdomen
Often unable to get history Importance of congenital anomalies Make sure stomach and bladder are
empty Differential diagnosis
GI surgical and medical problems urinary


ADMISSION TO SURGICAL WARD WITH ACUTE ABDOMINAL PAIN
NSAP 30%Acute appendicitis 28%Constipation 11%URTI 8%UTI 6.9%Gastroenteritis 3.6%Pneumonia 2.2%SBO (incl. Intussusception) 2.2%Mesenteric adenitis (operated) 2.2%Abdominal injuries 1%Hepatitis 1%Torsion of testisPancreatitis < 1%OMDiabetic acidosis

History
Vomiting: reflex vs. obstructive bilious or non-bilious
Abdominal pain: visceral vs. peritoneal crampy vs. constant
GI bleed: colour, amount, signs, association with pain

General Management
• ABC
• Fluids and electrolytes
• NG tube
• Antibiotics
• Pain control



Pyloric Stenosis• Incidence
– Rare in blacks
– 0.5 - 2/1000 live births
• Age: 3 weeks - 3 months
• Non-bilious vomiting
• Olive is not easily palpable
• Ultrasound is very accurate

Pyloric Stenosis
• Beware of acid-base and electrolyte imbalances.
•Hypokalemic, hypochloremic metabolic alkalosis
• surgical complications
•Wound infection – 10%
•Accidental opening of GI tract






Pre-op management
IV fluid:
If alkalotic, when is it safe to operate and why?


Intussusception
CLINICAL SUSPICION
X-RAY
U/S
REDUCTION BY BARIUM / AIR ENEMA

What is the intussuscipiens?


Intussusception
• Age: 3 months – 3 years
• Crampy abdominal pain
• Traction of the mesentery pallor, lethargy
•typically in younger infants
• Blood & mucous in stool (red current jelly)

Intussusception
• Crampy abdominal pain 80%
• Vomiting (early=reflex) 60-80%
• Rectal bleeding 30-50%
• Palpable mass 30-60%
• Others
– Lethargy, diarrhea, fever




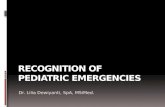
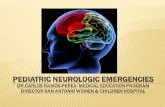
Barium enema

Air enema

Intussusception
• Beware of the 15% who are atypical
• Young infants are often just lethargic
• Don’t hesitate to do an ultrasound when the history is suggestive


In older children, suspect a lead point.
What lesions could act as lead points?

Lead Points
Meckel’s diverticulum Polyps Henoch-Schonlein purpura (HSP) Lymphoma Intestinal duplications

Treatment
Success rate of enema reduction around 80%
Small risk of perforation (2.5%) What would you do?
Laparoscopic reduction When there is lead point, usually
cannot be reduced. Resection with primary anastomosis


Midgut Volvulus
• Secondary to MALROTATION
• Age: 80% under 12 months old
• Sudden onset of GREEN vomiting
• Exam and X-rays may be normal initially

Who knows?
- Normal position of Ligament of Treitz?- Normal position of IC valve?- What we mean by base of mesentery?- Why does malrotation predispose to
volvulus?








Who knows the steps of a Ladd’s procedure?

Ladd’s procedure
Reduction of volvulus Division of Ladd’s bands Widening of mesenteric base Appendectomy


Small Bowel Obstruction

5 pediatric causes

Incarcerated hernia
congenital anomaly/band, internal hernia
Volvulus
Post-operative adhesions
Febrile obstruction: ruptured appendicitis

A small bowel obstruction in a virgin abdomen is a surgical indication


Acute Appendicitis
Symptomatology in 691 Patients < 12 Years
• Pain 98.7%
• Vomiting 81.5%
• Urinary symptoms 14%
• Diarrhea 10%

Acute AppendicitisJ Pediatr Surg 36:5, 2001 pp 780-783
Number of patients 454
Goal: to compare the characteristics and outcomes of patients undergoing appendectomy after clinical evaluation only with those undergoing the procedure after sonography.

Clinical Outcomes
Outcome CG (n=263) SG (n=191) P valuePre-opobservation(%)
4.2 19.4 <0.001
ER to OR (hr) 4.93 8.04 <0.001% Negativeappendectomy
5.7 13.1 0.006
% complicatedappendicitis
37.3 35.1 NS
% post-opabscess
1.2 4.4 0.038
LOS 2.35 2.82 NS

Conclusions
U/S should be reserved for patients who cannot receive a diagnosis on clinical grounds alone.
To obtain an U/S should be a surgical decision after a surgical evaluation
Greater role in post-pubertal females

What are the radiological criteria to make the diagnosis of acute appendicitis?

Size > 6mm Non – compressibility Corresponds to area of maximal
tenderness Identification of a fecalith
Free fluid Fat stranding


CT & Acute Appendicitisin Adults
Sensitivity: 90% for CT 76% for clinical exam (p<0.0005)
Specificity: 97%
Bettina Siewert et al., Beth Israel Hospital Harvard
Medical School 1/1997

Used infrequently Occasionally in older, obese
teenagers Concern about radiation
CT & Acute Appendicitisin Children


Gastrointestinal Bleeding
• Upper GI: tarry, melena stool
• Lower GI: red blood, clot
• Injury to mucosa: mixture of blood & mucous

GI Bleeding
• Rarely life-threatening
• Upper GI causes:
– Most: ASA, viral
– Massive bleed: varices, ulcer
• Lower GI causes
– Most: fissure, polyp, IBD, HUS etc.
– Massive bleed: Meckel’s diverticulum, intestinal duplication.


Who knows the rule of 2’s?

2% of population 2 types of mucosa (gastric and
pancreatic) 2 feet from the ileocecal valve 2 types of presentation
Obstruction Bleeding
2 inches long 2 other things I likely forgot


Meckel’s diverticulum
Will cause massive, painless LGI bleed to the point of requiring transfusion.
It is important to give H2 blockers for 3-5 days prior to doing a Meckel scan to increase its sensitivity.


Polyps
• Solitary or multiple
• Histology
– Hyperplastic
– Inflammatory - UC, nodular lymphoid HP
– Hamartomas-Juvenile, Peutz Jeghers
– Adenomatous (neoplastic) - Familial,Turcots syndromes




Polyps
Juvenile polyps will cause LGI bleed usually solitary In rectosigmoid (sometimes felt on DRE) May protrude or auto-amputate Endoscopic removal
Small bowel polyps will cause??


Foreign Body Ingestion
• X-ray: foreign body search
•soft tissues neck, CXR, AXR
• Most foreign bodies will pass through the GI tract uneventfully
• FB in the esophagus, alkaline batteries and long sharp ones must be removed.