
PEDIATRIC DYSRHYTHMIA 2015
31
Pediatric Dysrhythmias Board Review Dr. Sahar K.K. Attia Dr. Sahar K.K. Attia Pediatric Specialist,KKH Pediatric Specialist,KKH. May ,2015
-
Upload
sahar-kamal -
Category
Health & Medicine
-
view
530 -
download
0
Transcript of PEDIATRIC DYSRHYTHMIA 2015

Pediatric DysrhythmiasBoard Review
Dr. Sahar K.K. AttiaDr. Sahar K.K. Attia
Pediatric Specialist,KKHPediatric Specialist,KKH.
May ,2015


Pediatric dysrhythmias
Treatment not requiredTreatment not required Treatment Treatment isis required required
Sinus arrhythmiaSinus arrhythmia Supraventricular Supraventricular tachycardiatachycardia
Wandering atrial Wandering atrial pacemakerpacemakerIsolated premature atrial Isolated premature atrial contractionscontractionsIsolated premature Isolated premature ventricular contractionsventricular contractions
Ventricular tachycardiaVentricular tachycardia
First degree AV blockFirst degree AV block Third degree AV block Third degree AV block with symptomswith symptoms

Pediatric dysrhythmias
• Vital to be aware of arrhythmias that occur in
otherwise healthy children
• Management is individualized
• Does child have history of heart disease?
• Are symptoms present?

Sinus arrhythmia
• Most common irregularity of heart rhythm seen in children
• Normal variant
• Reflects healthy interaction between autonomic respiratory and cardiac control
activity in CNS.
• Heart rate increases during inspiration and decreases during respiration

Sinus arrhythmia

Wandering atrial pacemaker
• Atrial pacemaker shifts from sinus node to another atrial site.
• Normal variant, irregular rhythm

Isolated PAC’sIsolated PAC’s
• Premature atrial contractions• Benign in absence of underlying heart dz• Common in newborn period• Early p wave, sometimes with different
morphology than a sinus p wave• Can be either:
– Not conducted to ventricle, apparent pause– Conducted to ventricle with aberrant or
widened QRS complex ( careful not to mix up with PVC’s)

Isolated PAC’sIsolated PAC’s

Premature Ventricular ContractionsPremature Ventricular Contractions (PVC’s) (PVC’s)
• Not very commonly seen in children
• Incidence of 0.3 to 2.2 %
• Early, wide QRS complexes
• T waves in opposite direction of QRS
• Unifocal PVC’s are most encountered type.
• Bigeminy, sinus beat followed by PVC, repeating as a pattern, also frequently seen.

PVC’s
• If unifocal, disappear with exercise, and associated with structurally and functionally
normal heart, then considered benign, no therapy needed.

PVC’s evaluation
• 12 lead EKG, Echocardiogram
• Perhaps Holter monitoring
• Brief exercise in office to see if ectopy suppressed or more frequent
• Multifocal or paired PVC’s more worrisome
• Medications usually not needed
• Advise patients to avoid caffeine and other stimulants

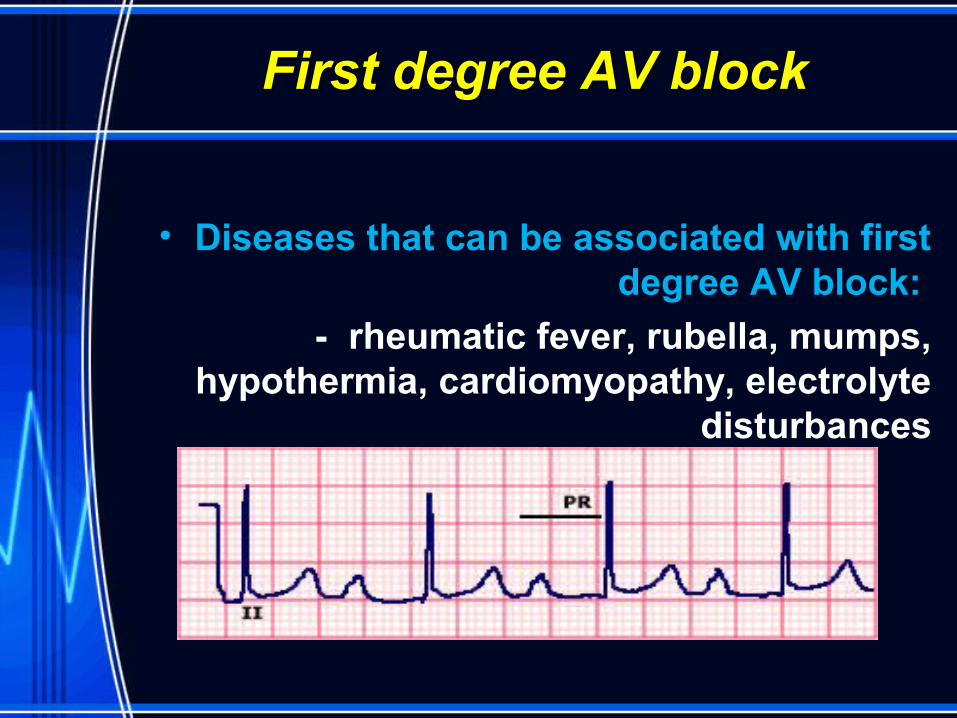
First degree AV block
• Commonly seen (up to 6% normal neonates)
• PR interval is greater than upper limits of normal for a given age
• PR interval is age and rate dependent
• 70-170 msec in newborns is normal
• 80-220 msec in young children and adults
• Generally does not cause bradycardia since AV conduction remains intact
First degree AV blockFirst degree AV block
• Diseases that can be associated with first degree AV block:
- rheumatic fever, rubella, mumps, hypothermia, cardiomyopathy, electrolyte
disturbances

Third degree AV block
• AKA complete heart block
• Most common cause of abnormal bradycardia in infants and children.
• Complete disassociation between P waves and QRS complexes

Third degree AV block
• Can be congenital – in this case it is strongly associated with maternal SLE.
• Mom of an infant should be worked up.
• Most common structural heart defect associated is corrected transposition of
great vessels

Third degree AV block
• May be asymptomatic – follow clinically
• Slower the heart rate, and wide QRS escape rhythms place into high risk group
• May need implantable pacemaker:
-significant bradycardias, syncope, exercise intolerance, ventricular dysrhythmias, or ventricular arrhythmias, structural disease.
• Possible acute treatment: isoproterenol

Supraventricular tachycardia
• Most common abnormal tachycardia seen in pediatric practice
• Most common arrhythmia requiring treatment in pediatric population
• Most frequent age presentation: 1st 3 months of life, 2nd peaks @ 8-10 and in
adolescense• Rapid, regular, usually narrow QRS
rhythm, originating above the ventricles

SVT
Figure 5-42 Supraventricular tachycardia
- Note a normal QRS complex tachycardia at a rate of 214 beats/minute without visible P
waves.

SVT
• Paroxysmal, sudden onset & offset
• Rates of SVT vary with age
• Overall average rate for all ages: 235 bpm
– 1st 9 months of life: avg rate is 270 bpm
– Older children: avg rate is 210 bpm( 180-250)
• P waves difficult to define, but 1:1 with QRS
• Important to differentiate from sinus tach

SVTSVT
• Older kids can describe a sensation of a fast heart rate, palpitations, or
chest tightness.
• Hemodynamic compromise in newborns and those with structural
heart disease
• Those with typical symptoms would benefit from cardiac consultation

SVT - Treatment
Goal: - Identify unstable patients, differentiate from
sinus tachycardia, and terminate the rhythm
- Vagal maneuvers in stable patients.
Adenosine if IV access readily available– Stop conduction through AV node– Helps to define p waves if unsure of etiology– 0.1 mg/kg (max 6 mg), repeat 0.2 mg/kg ( max 12
mg) in line closest to central circulation– Need continuous ECG and BP monitoring

SVT - Treatment
• Synchronized cardioversion
• Amiodarone, Procainamide if above unsuccessful.
• Transesophageal atrial pacing can also be performed

SVT - Treatment
• Need post conversion EKG – identify those with WPW syndrome ( 25 % pts with SVT)
• Will also need an echo – identify structural problems
• Radiofrequency catheter ablation – Frontline treatment– Very effective– Cutoff points usually are 5 y.o. and 15 kg, unless severe
SVT
• Observation and expectant management• Medications
– Digoxin and beta blockers as first line– Flecainide, sotalol, amiodarone

Other SVT’s
• A flutter, A fib, ectopic atrial tachycardia, junctional tachycardias.
• Not commonly seen in pediatric patients
• Adenosine does not terminate these rhythms, originate above AV node
• Treatments: procainamide, amiodarone, cardioversion, or ablation

SVT - WPW
Figure 5-43 Wolff-Parkinson-White syndrome. Note the characteristic findings of a short P-R interval, slurred
upstroke of QRS (delta wave), and prolongation of the QRS
interval.

Ventricular tachycardiaVentricular tachycardia
• Sustained V-tach is uncommon, needs workup
• Regular wide complex tachycardia
• Atrioventricular dissociation
• Life threatening arryhthmia
• Often presents in those who have had open heart surgical repair, or those with
cardiomyopathies, myocarditis, or tumors

V-Tach
Treatment: IV lidocaine, procainamide, amiodarone.
- If critically ill: synchronized cardioversion
- Long term: meds, ablation, or defibrillator

Ventricular fibrillation
• Seen in children with EKG abnormalities such as long QT syndrome, or Brugada syndrome
• Cardiomyopathies, structural heart disease causing ventricular dysfunction
• Treatment: immediate defibrillation, CPR

V-fib
• Brugada syndrome – inherited arrhythmia, autosomal dominant person goes into v-fib, faints, dies suddenly.
Treatment: defibrillator, careful screening



















