Pectus excavatum, Advanced Nuss procedure
34
Pectoscopy – Nuss procedure for minimally invasive repair of pectus excavatum (MIRPE) Dr LM.Darlong “Chest wall deformity clinic” Consultant Thoracic Surgery & Thoracic Oncology Fortis Hospital NOIDA www.pectusindia.com
description
Pectoscopy – Nuss procedure for minimally invasive repair of pectus excavatum (MIRPE)Dr LM.Darlong “Chest wall deformity clinic” Consultant Thoracic Surgery & Thoracic Oncology Fortis Hospital NOIDAwww.pectusindia.comPectus excavatum• Funnel chest• Depression chest wall• Symmetric defect • Asymmetric defect • Overgrowth of cartilage • 1 in 500 to 1000• Males 3-4 timesFunnel chestwww.pectusindia.comFacts• M.C congenital chest wall deformity• Effects on the individual -Physio
Transcript of Pectus excavatum, Advanced Nuss procedure

Pectoscopy – Nuss procedure for
minimally invasive repair of pectus
excavatum (MIRPE)
Dr LM.Darlong“Chest wall deformity clinic”Consultant Thoracic Surgery & Thoracic OncologyFortis Hospital NOIDA
www.pectusindia.com

• Funnel chest
• Depression chest wall
• Symmetric defect
• Asymmetric defect
• Overgrowth of cartilage
• 1 in 500 to 1000
• Males 3-4 times
Pectus excavatum

Funnel chest
www.pectusindia.com
Facts
• M.C congenital chest wall deformity
• Effects on the individual-Physiological
-Psychosocial
-Cosmetic
• Medical community –Neglect
feels -Not a Disease, only Cosmetic
Fact-DISEASE www.pectusindia.com
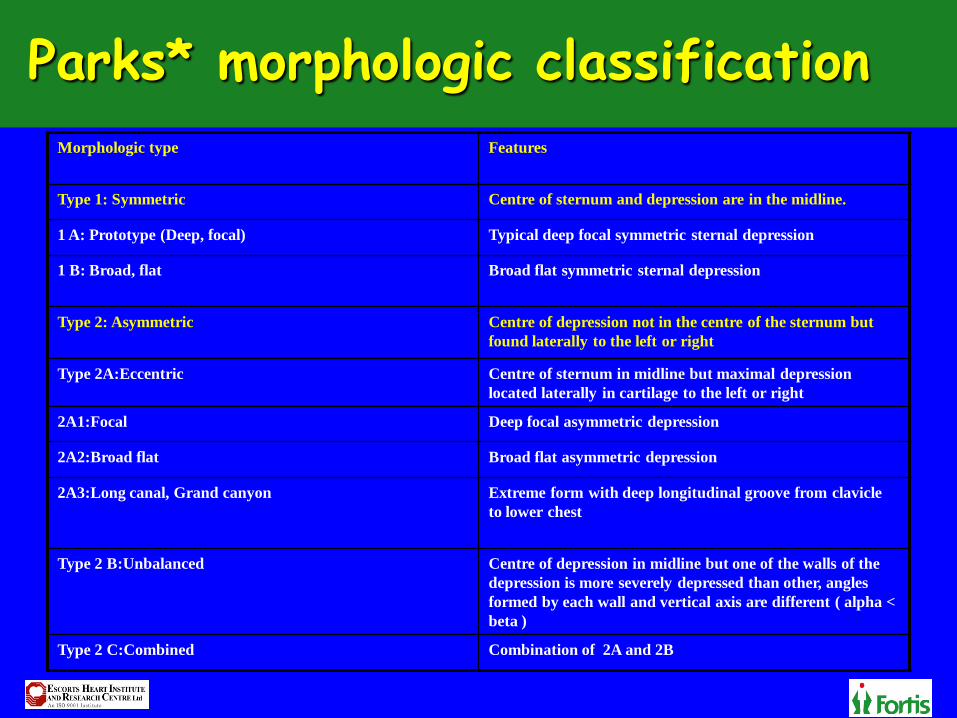
Parks* morphologic classification
Morphologic type Features
Type 1: Symmetric Centre of sternum and depression are in the midline.
1 A: Prototype (Deep, focal) Typical deep focal symmetric sternal depression
1 B: Broad, flat Broad flat symmetric sternal depression
Type 2: Asymmetric Centre of depression not in the centre of the sternum but
found laterally to the left or right
Type 2A:Eccentric Centre of sternum in midline but maximal depression
located laterally in cartilage to the left or right
2A1:Focal Deep focal asymmetric depression
2A2:Broad flat Broad flat asymmetric depression
2A3:Long canal, Grand canyon Extreme form with deep longitudinal groove from clavicle
to lower chest
Type 2 B:Unbalanced Centre of depression in midline but one of the walls of the
depression is more severely depressed than other, angles
formed by each wall and vertical axis are different ( alpha <
beta )
Type 2 C:Combined Combination of 2A and 2B

Symmetrical
Type 1 A Type 1B
Type 2A1 Type 2A2 Type 2A3
Type 2B Type 2C
Type 1A Type 1B

Asymmetrical
Type 1AType 1A
Type 2A1 Type 2A2

Asymmetrical
Grand Canyon / Type 2 A3

Asymmetrical
Type 2B Type 2C
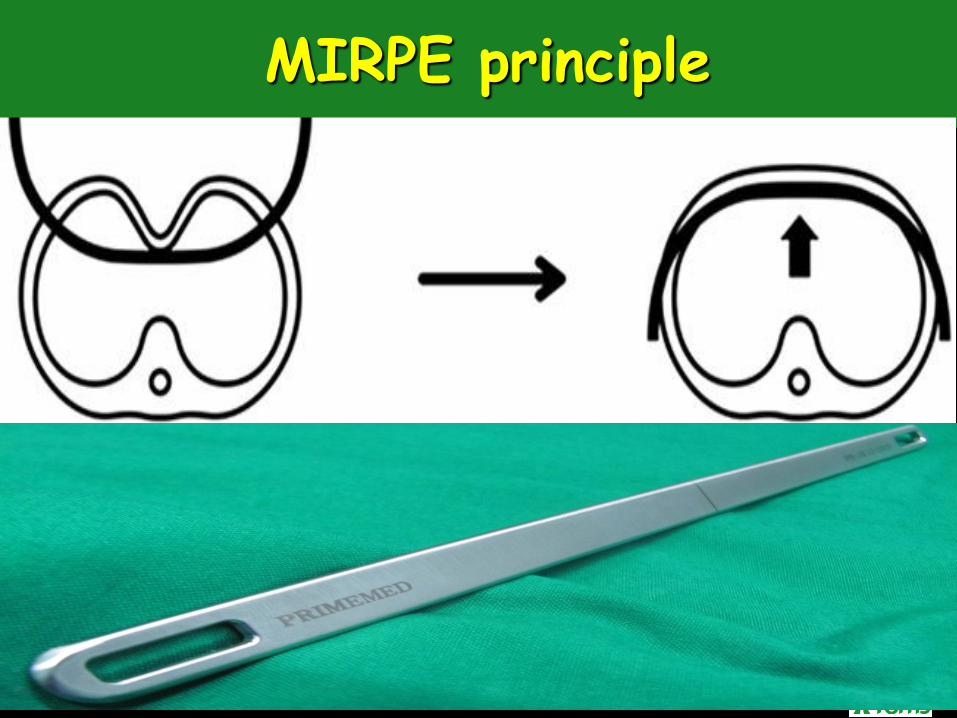
MIRPE principle
MIRPE
• Stainless steel bars placed under sternum
• Forcing the chest to remodel
• No cutting/removal of cartilage
• 2 cm incision on each side of chest

Repair techniques
• Bar bending – Based on morphology type
• Retrosternal tunnel – Crucial for safety
• Bar fixation / stabilization

Bar bending
• Morphology based
• Correct length of bar
• Creation of mirror image
• Multiple bending and reinsertion

Bar bending
Symmetrical Asymmetrical

Bar benders

Bar benders

Retrosternal tunnel
• Crucial - Avoid cardiac injuries
• Crane technique – Sternal lift
• Pectoscopy – Direct endoscopic vision
• Thoracoscopy - limitations

Retrosternal tunnel creation
Pectoscopy Thoracoscopy
View both side of chest View of right side of chest only
www.pectusindia.com

Crane Tech – Sternal lift
www.pectusindia.com

Crane lift
www.pectusindia.com

Pectoscope
www.pectusindia.com
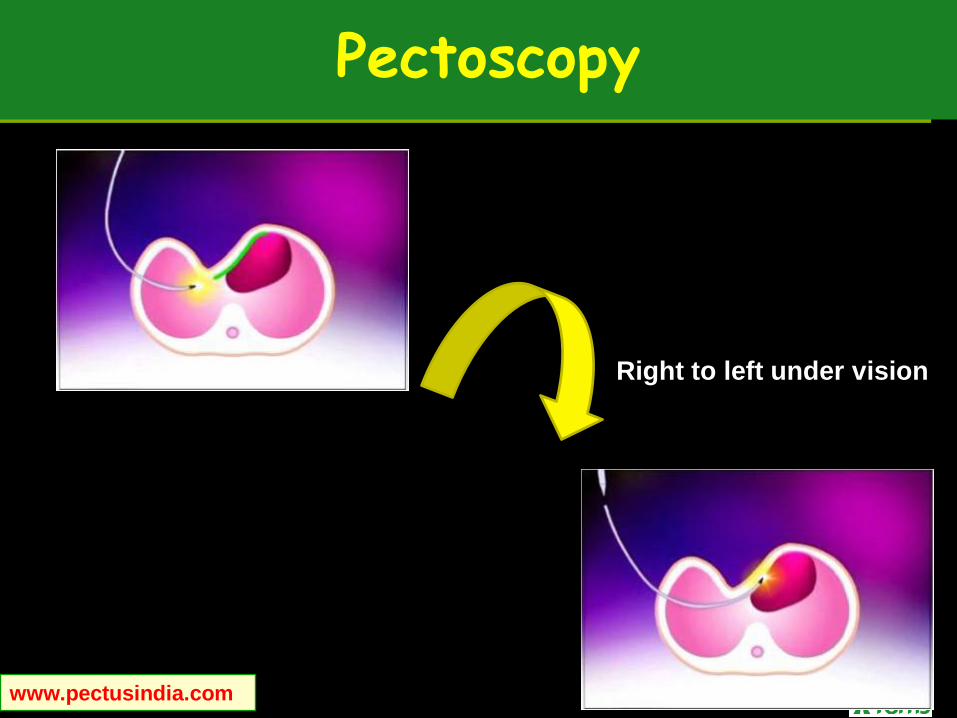
Pectoscopy
www.pectusindia.com
Right to left under vision
Bar stability
• Hinge point stabilization – Hinge plate
• Bar fixation – Claw fixators
• Crucial to prevent
Hinge disruption
Lateral displacement
Flipping

Bar exit site stabilization

Claw Fixators
www.pectusindia.com

Postop images
www.pectusindia.com

Postop images
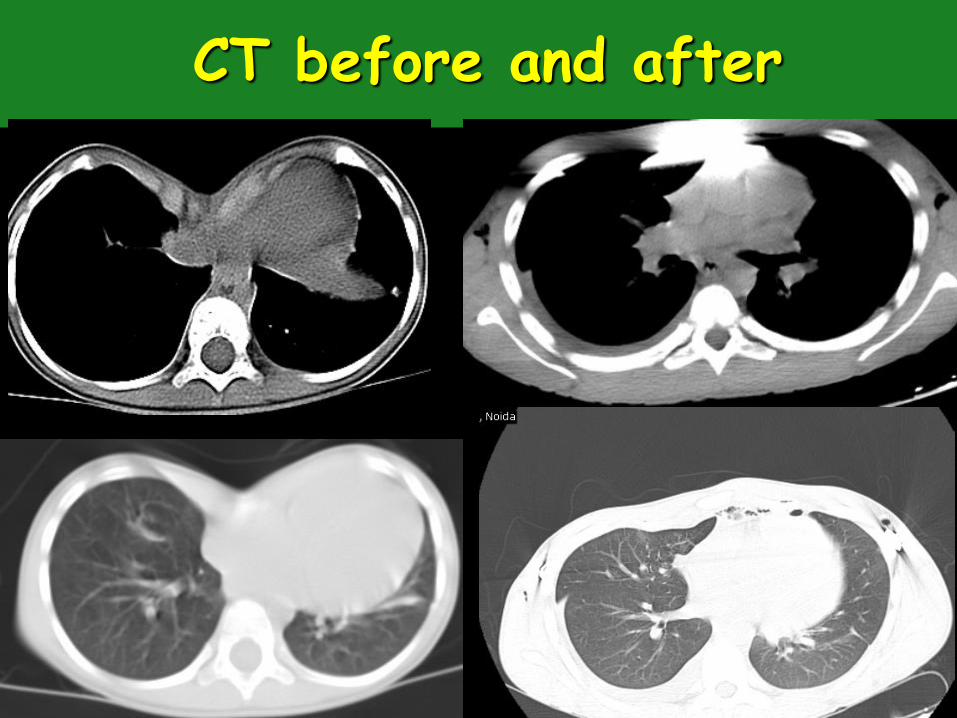
CT before and after

Before and after surgery
www.pectusindia.com

Indications for repair
• Physiological- Improve heart and lung
function
• Psychosocial – Improves self image/esteem
• Cosmetic
Time of repair
• No consensus
• Early repair- Bone softer/malleable
• Adults – Strong bones/less
malleable/multiple bars
• Best at 3yrs age – at 5 yrs Bar removed
and child ready to join school

MIRPE
• Remodeling of Chest wall
• Truly minimally invasive
• Cosmetic – 2 incision, 2 cm size
1.Morpho tailored-Asymmtrc defects
2.Crane technique – Sternal lift
3.Pectoscope – Endoscopic Guidance

Conclusion
• Medical community–Indentify as Disease
• Not neglect it as Cosmetic defects
• Minimally Invasive Techniques
Look good / Feel good

www.pectusindia.com