Peaceful Uses of Nuclear Energy Non-power Applications A ...
33
Peaceful Uses of Nuclear Energy Non-power Applications A Public Health Perspective Thematic Seminar on Peaceful Uses of Nuclear Energy – Vienna, Austria, 20 th November 2019 Dr Emilie van Deventer Radiation Team Leader Department of Public Health, Environmental and Social Determinants of Health Geneva, Switzerland
Transcript of Peaceful Uses of Nuclear Energy Non-power Applications A ...
Peaceful Uses of Nuclear EnergyNon-power Applications
A Public Health Perspective
Thematic Seminar on Peaceful Uses of Nuclear Energy – Vienna, Austria, 20th November 2019
Dr Emilie van Deventer
Radiation Team Leader
Department of Public Health, Environmental and Social Determinants of Health
Geneva, Switzerland

Peaceful uses of nuclear energy
Outside the nuclear power sector, nuclear and
radiation technologies are essential in medicine,
and also have industrial and research applications,
such as:
• non-destructive testing (e.g. industrial
gammagraphy), radioactive gauges (e.g.
measurement of density and liquid levels), food
irradiation, sterilization (e.g. medical devices,
blood products), treatment of effluents, security
checks, radiotracers in molecular biology, plague
and vector control (e.g. fruit flies, mosquitoes),
This presentation will focus on medical use of radiation

Early medical use of radiation
Röntgen discovered X-rays and
noted that, while it could pass
through human tissue, it could not
pass through bone or metal
Marie Curie pushed for
radiography to be used
to treat wounded
soldiers in World War I

Outline
• Introduction
• Medical applications (diagnostics to therapy)
• Public health considerations
• Discussion
The World Health Organization
WHO’s objective is the attainment by all peoples
of the highest possible level of health
HEALTH
a state of complete physical,
mental and social well-
being and not merely the
absence of disease or
infirmity"
(WHO Constitution, 1948)

Sustainable Development Goals (2015-30)
The UN Member States made a commitment towards the 17
Sustainable Development Goals (SDGs) by 2030

SDG 3. Ensure healthy lives and promote well-being for all at all ages

Key Themes of WHO’s
13th General Programme of Work
2019-2023
Mission Promote Health - Keep the World Safe - Serve the Vulnerable
Strategic
Priorities
Health Coverage: 1 billion more people with health coverage
Health Emergencies: 1 billion more people made safer
Health Priorities: 1 billion lives improved
2

Modified from , Health systems financing: the path to universal coverage. Executive summary, The World Health Report,
WHO/IER//WHR/10.1, 2010
To achieve SDG3, require universal health coverage,
including financial risk protection, access to quality
essential health-care services for those in need

Priority setting and decision making by income level
Fragile states:
MOH needs to define:
Basic interventions packages
Emergency kits
Disaster planning
Priorities
Low income countries with low coverage,
Primary health care interventions, limited coverage for specialized care
MOH needs to define:
Essential interventions mainly for mother and child and vulnerable population;
Vaccination package
Priority medical devices for diagnostic and limited treatment Essential medicines , Which interventions to add, and to whom.
Middle and high income countries with medium coverage:
MOH has to define:
Package of interventions on prevention, promotion, and diagnostics, limited treatment and rehabilitation.
Need to define extension for :
Specialized NCD interventions depending on local burden of disease.
Vertical programs locally,
For specific or vulnerable populations, depending on resources.
Strong health system, Integrated –care, People-centred, Universal health coverage.
High coverage: Prevention, Diagnostic, Treatment, Rehabilitation, Palliative care, Home care
Vaccines, Medicines, Medical Devices, all interventions
For all: children, Adolescents Mothers and Ageing population
Need to define innovative more cost effective, extra services and disinvestment!
Population Coverage, financial, technological resources and health work force
Health
Syste
ms fo
r UH
C
Need to prioritize
and perform
informed decisions
is higher where
resources are
limited

Outline
• Introduction
• Medical applications (diagnostics to therapy)
• Public health considerations
• Discussion

Diagnostic
radiologyNuclear Medicine
(diagnostic and
therapeutic
applications)
Interventional
radiology
(diagnostic and
therapeutic
applications)
Radiotherapy
Diagnostics Therapy
About 4 billion/y X-ray
exams (> 10% in
children)
About 40 million/y NM
proceduresAbout 8 million/y radiation
oncology treatments
Role of radiation in health care

Diagnostic Radiology
Digital radiography is replacing film-based radiography, with
images instantly available, lower costs and facilitated access.
• Chest radiograph represents 40% of all imaging procedures (about
10% in children e.g. pneumonia diagnosis). It accounts for 13% of
the population collective dose.
Computed tomography (CT) allows for a fast assessment of
illness and injury, often replacing less accurate or more invasive
diagnostic procedures.
• It represents 6% of all medical imaging procedures and accounts
for 43% of the population collective dose.
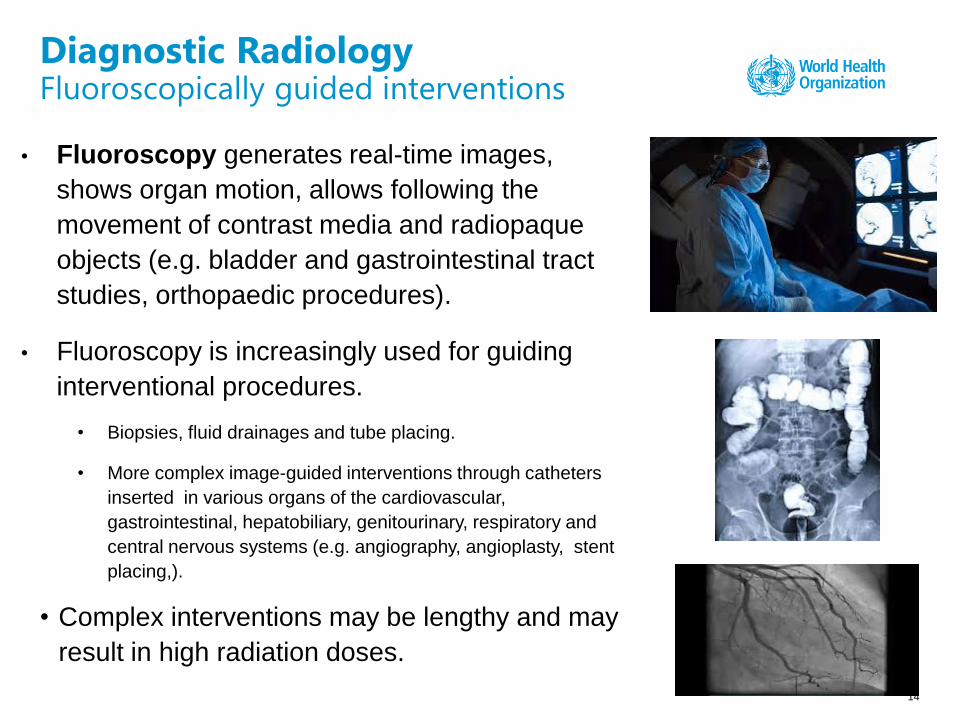
• Fluoroscopy generates real-time images,
shows organ motion, allows following the
movement of contrast media and radiopaque
objects (e.g. bladder and gastrointestinal tract
studies, orthopaedic procedures).
• Fluoroscopy is increasingly used for guiding
interventional procedures.
• Biopsies, fluid drainages and tube placing.
• More complex image-guided interventions through catheters
inserted in various organs of the cardiovascular,
gastrointestinal, hepatobiliary, genitourinary, respiratory and
central nervous systems (e.g. angiography, angioplasty, stent
placing,).
• Complex interventions may be lengthy and may
result in high radiation doses.
14
Diagnostic RadiologyFluoroscopically guided interventions

Nuclear medicine diagnosis
Diagnostic nuclear medicine uses radioactive tracers
(e.g. radioisotopes or radiolabeled pharmaceutical
products) to visualize organs (heart, brain, tumours, ..)
and provide information on diseases (cardiovascular
diseases, dementia, cancer,..)
Gamma emitters are administered through injection,
inhalation or ingestion, and the emitted radiation is
detected by a g camera which converts into a digital
format.
NM imaging can be performed by using planar gamma
cameras, single photon emission computed
tomography (SPECT) and positron emission
tomography (PET), and now hybrid imaging e.g.
PET/CT, SPECT/CT, PET/MRI).
Bone scintigraphy
(Technesium-99m)
SPECT
(Thallium-201)
myocardial
perfusion
PET-CT scan with Fluorine-18
deoxyglucose (18F-FDG)
(18F has a half-life of 109.8 min and
therefore must be produced in a cyclotron
placed very close to the PET scanner)

Radionuclide therapy
Radionuclide therapy uses beta- and alpha- emitters
that accumulate in a tissue and can selectively destroy
specific targets (e.g. cancer cells).
✓ benign thyroid disease or thyroid cancer using iodine-
131
✓ bone metastasis with labelled bone-seeking agents (e.g.
radium-223, strontium-89 and samarium-153)
✓ non-Hodgkin lymphoma using radiolabeled antibodies
(i.e. radioimmunotherapy) for (e.g. yttrium-90 and
lutetium-177)
✓ neuroblastomas in children and young adults using
iodine-131 mIBG
✓ liver cancer with radiolabeled resin and glass
microspheres (e.g. yttrium-90)
• Theranostics combines the diagnostic properties of
gamma-emitters with the use of beta- and alpha-
emitters for therapy. 16

External Beam Radiotherapy (EBRT)
EBRT plays an essential role in cancer treatment. It most often uses
photon beams (e.g. X-rays from linear accelerators/ LINACs, Co-60
gamma rays from telecobalt therapy units. EBRT is usually delivered as
fractionated treatments repeated once per weekday for several weeks,
depending on the clinical protocol.
Advanced technology allows today delivering EBRT in a more precise way,
(e.g. 3-D conformal RT, intensity-modulated RT /IMRT, image-guided RT
(IGRT). Stereotactic radiosurgery can be used to treat small tumors with
well-defined edges (e.g GammaKnife for brain tumours), usually in one
single session.
Use of heavy-particles, in particular protons shows clinical advantages,
specially for pediatric tumours. New proton therapy centers are being
installed in high- and even middle-income countries, but are very costly.
17

Internal radionuclide therapy (Brachytherapy)
Brachytherapy (BT) uses sealed radioactive sources in
close proximity to the tissues, in different configurations,
e.g.:
• surface plaques or molds (e.g. eye and skin cancer);
• sources inside body cavities (i.e. gynecological cancers);
• intraluminal sources (e.g. esophagus cancer);
• interstitial sources as needles, wires or seeds (e.g. soft tissue
cancers, breast cancer, prostate cancer);
• It is becoming a main means of treatment as they give less
overall radiation to the body, are more localized and cost-
effective

Outline
• Introduction
• Medical applications (diagnostics to therapy)
• Public health considerations
• Discussion

The public health perspectiveGlobal causes of premature deaths
http://vizhub.healthdata.org/gbd-compare/

Causes of premature deaths(Sub-Saharan Africa)
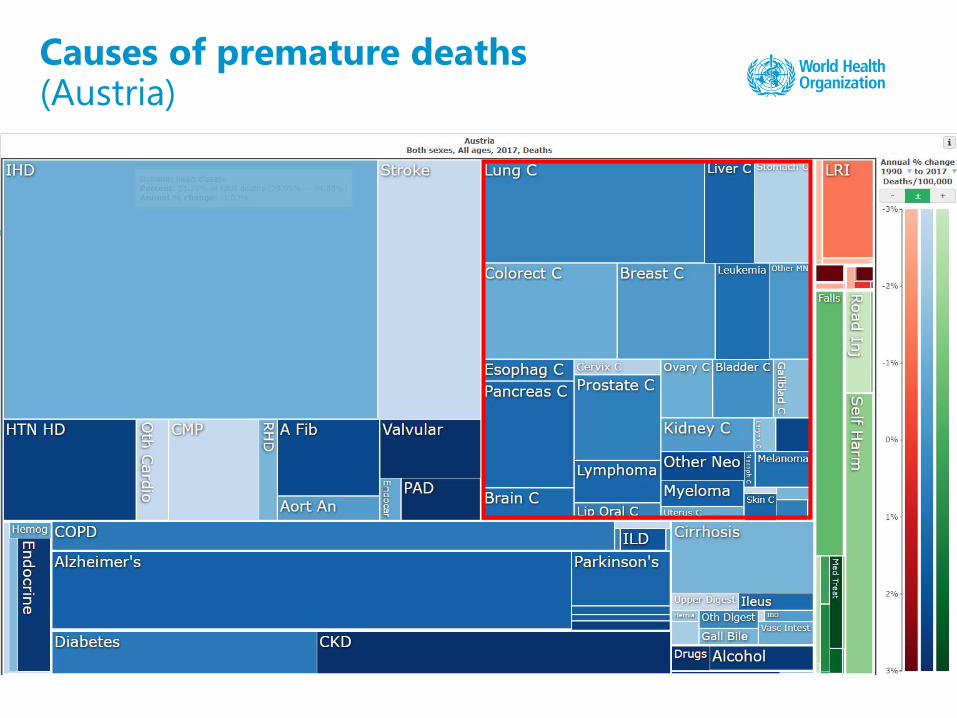
Causes of premature deaths(Austria)
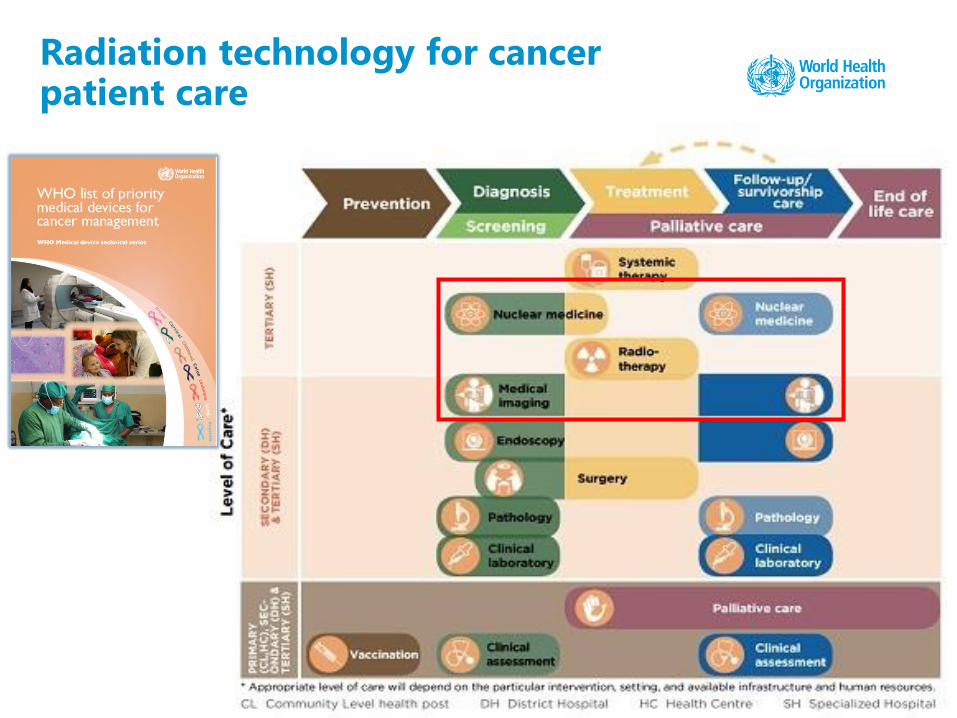
Radiation technology for cancer patient care

Outline
• Introduction
• Medical applications (diagnostics to therapy)
• Public health considerations
• Discussion

Medical use of radiation
• The clinical value of the use of radiation
in radiology is unquestionable: it saves
lives
• Exciting times with many novel
technologies
• Complex medical interventions that need
o Sophisticated infrastructures
o Equipment with adequate QC
(maintenance, calibration, waste
management, …)
o Educated and highly-skilled staff
Skilled workforce for NM
• Nuclear medicine physicians
• Nuclear medicine
technologists
• Radiologists (hybrid imaging)
• Radiographers (hybrid
imaging)
• Medical physics experts
• Biomedical engineers
• Radiopharmacists,
radiochemists
• Nurses, assistants
• IT support, AI engineers, …

Medical use of radiation
Inappropriate or unskilled use may result in unnecessary
exposures, increasing risk without adding any benefit.
A major challenge: to minimize health risks while maximizing
the benefits.
Benefits outweigh the risks when the procedures are
appropriately prescribed and properly performed.

Medical use of radiation
System of radiation protection (justification, optimization, …)
• Justification of procedures:
• While most LMICs cannot provide access to the necessary radiological
medical procedures, high-income countries are facing the challenge of
overuse. It was reported that about 30% of the radiological imaging
procedures are not justified (i.e. do not provide a net benefit)
• Optimization of protection: Optimization of protection in medical exposures
requires the management of the radiation dose to the patient to be
commensurate with the medical purpose

Adverse effects in interventional radiology
• Fluoroscopy-guided interventional procedures are now routinely used and doses to patients and staff may be significant.
• Adverse effects are being increasingly reported in patients (e.g. skin injuries). Need to monitor patient dose in real time and implement clinical follow-up of high-dose patients.
• A higher prevalence of cataract has been reported in staff working in catheterization laboratories, associated to exposure of the lens of the eye. Need to ensure dose monitoring, suitable shielding and personal protective equipment (e.g. lead glasses).
WHO’s norms and guidance on radiopharmaceuticals
1. The International Pharmacopoeia
▪ Source material for reference or adaptation by Member States wishing to establish pharmaceutical requirements.
▪ The pharmacopoeia, or any part of it, shall have legal status, whenever a national or regional authority expressly introduces it into appropriate legislation.
▪ It is free for use by WHO Member States http://apps.who.int/phint/en/p/about/
2. Good Manufacturing Practices (GMPs)
▪ WHO-IAEA guidelines for radiopharmaceutical products, providing a general overview of GMP requirements.
▪ Linked to main principles of GMP, i.e. pharmaceutical products and sterile pharmaceutical products
▪ Unless otherwise specified, GMP requirements for radiopharmaceuticals take precedence over GMP requirements for pharmaceutical products
International Radiation Basic Safety Standards (BSS)
• Global benchmark for radiation safety, cosponsored by 8
international organizations.
• Safety requirements on medical exposures are
substantially expanded in the latest BSS
• Safety guide to support the implementation of BSS safety
requirements in medicine (co-sponsored by IAEA, PAHO,
WHO and ILO).
• WHO cooperates with the IAEA to support the
implementation of the BSS in medical facilities.

Bonn Call for Action10 actions to improve radiation protection in medicine

Conclusions
• Medical applications of nuclear energy for diagnosis and treatment
provide very successful procedures
• It is important to ensure reliable supply of radioisotopes
• Quality and safety of the procedures are key, which requires a trained
workforce
• Some relevant Sustainable Development Goals
• SDG target 3.4 to reduce by one-third by 2030 premature deaths from
NCDs, primarily cardiovascular disease, cancers, diabetes and chronic
respiratory diseases
• SDG target 3.8 to achieve universal health coverage.
Thanks to • Maria Perez, Radiation Programme, Public Health, Environmental
and Social Determinants of Health• Elena Fidarova, Management of Noncommunicable Diseases• Sabine Kopp, Technologies Standards and Norms• Adriana Velazquez, Innovation, Access and Use
World Health OrganizationGeneva Switzerland