
Tumor Cytogenetics - Welcome | Institute for Cancer … Cytogenetics Vundavalli Murty ... Short CR...
63
Tumor Cytogenetics Vundavalli Murty Department of Pathology & Cell Biology & Institute for Cancer Genetics Sept 21, 2015
Transcript of Tumor Cytogenetics - Welcome | Institute for Cancer … Cytogenetics Vundavalli Murty ... Short CR...

Tumor Cytogenetics Vundavalli Murty
Department of Pathology & Cell Biology
& Institute for Cancer Genetics
Sept 21, 2015

September 22, 2015 Page 2
Reference Material 1. Cancer Cytogenetics: Text Book: Heim S and Mitelman F, 2009 2. Recurrent Chromosome Aberrations in Cancer
Web site http://cgap.nci.nih.gov/Chromosomes/RecurrentAberrations
3. Atlas of Genetics and Cytogenetics in Oncology and Haematology
Web site: http://atlasgeneticsoncology.org//

September 22, 2015 Page 3
Overview - Chromosomes in human tumors are widely abnormal:
David von Hansemann 1890: nuclear and mitotic abnormalities in tumors
Boveri 1914: Chromosome abnormalities play a central role in transformaton
- Controversy: Early 1950s
Whether the chromosome changes are primary events or merely secondary phenomena?
- Changed view:
Recurring chromosome aberrations associated with leukemia, lymphoma, sarcoma, carcinoma
Proto-oncogenes identified at the breakpoints Experimental evidence for these genes in transformation Targeted drugs that inhibit gene product: e.g. STI571 for BCR-ABL

September 22, 2015 Page 4
Methods of Chromosome Preparations
• Availability of actively dividing cells to arrest at metaphase or prometaphase: use of mitotic stimulants
• Direct preparations or short-term cultures to represent in vivo conditions
• Hematologic Malignancies:
- Bone marrow, Lymph node, Peripheral blood, Other body fluids
- 12~96hr cultures with or with out mitogenic stimulation
Solid tumors: All types
Short-term cultures
September 22, 2015 Page 5
Chromosome preparation & Staining contd -Mitotic arrest (Colcemid: microtubule depolymerising drug)
-Hypotonic treatment -A variety of different types of methods: Giemsa-banding (best choice) -‐FISH (Fluorescence in situ hybridization) On methanol-acetic acid fixed cells, paraffin sections, touch imprints - To detect translocations, inversions, deletions, amplifications - Probes
-Other Molecular Cytogenetic methods: "
Chromosomal CGH, SKY, array CGH"

Methods Employed in Recognizing Chromosome Aberrations"
• Banding methods: Trypsin-Giemsa
• Chromosome painting:
• FISH:
• Comparative Genomic Hybridization CGH):
• Spectral Karyotyping (SKY):

September 22, 2015 Page 7

September 22, 2015 Page 8
Idiograms of G-band for normal Human Chromosomes Nomenclature "
p
q
Centromere
Region Band Number e.g., 1p34.1"

September 22, 2015 Page 9
Symbols and Abbreviated Terms: ISCN, 2009"
Important designations to describe cancer karyotype cen centromere del deletion der derivative chromosome dic dicentric chromosome dmin double minute chromosome dup duplication hsr homogeneously staining region i isochromosome ins insertion inv inversion mar marker chromosome minus (-) loss plus (+) gain p short arm parenthesis()surround structurally altered chromosoems and breakpoints ph Philadelphia chromosome q long arm r ring chromosome semicolon(;)separates altered chromosomes t translocation
A translocation between chromosomes "9 and 22 in CML at bands 9q34 "and 22q11.2"46,XX,t(9;22)(q34;q11.2)[20]"
A deletion of long arm of chromosome 5 at band 5q31 in a leukemia patient"
46,XY,del(5)(q31)[10]/46,XY[10]"
September 22, 2015 Page 10
Types & Consequences of Major chromosome changes
• Ploidy (e.g., haploid, triploid, tetraploid): Unclear"
• Aneuploidy (e.g.,tri-,tetra-, monosomy): Increased or decreased expression of set of genes"
• Reciprocal or non-reciprocal translocations (inversions): ""Overexpression/fusion gene"
• Deletions: Loss of expression"
• Duplications and Amplifications: Increased gene expression"
• Insertions: Loss or gain of function of genes"

September 22, 2015 Page 11
Chromosomal Translocations in Leukemia and Lymphoma
Consequences: Altered Expression and/or Fusion Proteins"
Gain of function; BCR/ABL
Over a 420 genes associated with translocations have been identified in human cancer.

- Tumor cells exhibit non-random chromosome abnormalities
- Recurrent in specific types of malignancies
- Have been used as diagnostic and prognostic markers
- Have lead to the understanding of biology of cancer
Cancer is a Genetic (Chromosomal) Disease

Will Focus on Specific Examples of Chromosome "
Aberrations that were Proven to be Highly Relevant "
In Cancer Diagnosis and Management"

September 22, 2015 Page 14
Chronic Myelogenous Leukemia (CML)
t(9;22)(q34;q11.2)
BCR/ABL fusion

05-1363
06-174
02-15
t(9;22) partial karyotype BCR/ABL FISH
t(9;22)(q34;q11.2)
t(9;22)(q34;q11.2)
t(9;22)(q22;q11.2)
CML: Karyotyping and FISH

Chromosome changes in CML progression
A: Karyotype: 47,XX,t(9;22)(q34;q11.2),+8,i(17)(q10) B: FISH--BCR/ABL C: FISH--CEP 8 (green) and D20S108 (red) D: FISH– TP53 (red) and ATM (green)

Chromosomal changes in Myelodysplatic Syndrome (MDS): Clinical significance
5q- syndrome Single defect; favorable with low risk of transformation (distinct morphologic entity; high prevalence in elderly females; RPS 14, CTNNA1 as target genes
del(5q)/- 5 Favorable as sole abnormality Additional abnormalities, therapy related--poor prognosis
del(7q)/-7 Unfavorable outcome
Trisomy 8 Intermediate
del(20q) Good prognosis (as sole change) Intermediate/unfavorable (with other abnormalities)
• Heterogenous group"• Primary and secondary MDS"• Cytogenetic changes have prognostic implications"The classification of MDS is based on clinical data (previous history, age) and biologic characteristics (morphology, cytochemistry, immunophenotype, cytogenetic and molecular alterations)

September 22, 2015 Page 18
Acute Myeloid Leukemia (AML)
>85% karyotypic abnormalities
Translocations, deletions, and inversions
Diagnostic and classification of risk groups
The classification of acute myeloid leukemia (AML) similar to myelodysplasic syndromes (MDS) is based on clinical data (previous history, age) and biologic characteristics (morphology, cytochemistry, immunophenotype, cytogenetic and molecular alterations)

September 22, 2015 Page 19
Recurring Chromosome Abnormalities in AML Morphologic Subset Chromosome change Genes Prognosis
M2 t(8;21)(q22;q22) ETO-AML1/RUNX1 (attenuates spindle checkpoint)
Favorable
(No adverse for additional changes)
M3 t(15;17)(q22;q12-q21) PML-RARA Variants: PLZF, NPM, NUMA
Favorable
M4Eo inv(16)(p13q22)"
t(16;16)(p13;q22)"
del(16)(q22)"
CBFß/MYH11 (core binding factor/myosin heavy chain)
Favorable
M1,M2, M4, M5a, therapy-related (Topoisomerase inhibitors)
11q23 abnormalities" MLL Poor, generally
Variable, translocation-based
Biphenotypic leukemia (BAL)
t(9;22)(q34;q11), 11q23 abnormalities"
BCR/ABL, MLL Worse
Many other categorized, Uncategorized, and Treatment-related

Inversion 16 in AML: Good prognostic AML"
9/22/15 Page 20

t(15;17) is a charcteristic chromosome change in APML

Therapy Related MDS and AML

Probabilities of 5-year survival according to cytogenetic stratifications in children with advanced primary or secondary MDS
Gohring G et al., Blood 116: 3766, 2010

An AML patient with complex karytoype and MLL amplification predicts poor prognosis
MLL gene amplified"
Diagnosis: "AML"
Age: " "74 years (Female) ""
Karyotype: 45,XX,-4,der(5)t(5;17)(q11.2-q21;q11.2),+6,+8, der(11)dup(11)(q13q23)ins(11;4)(q23;q22q28)hsr(11)(?23),-17,-18[cp35]
Amplification: MLL, ATM: Deletion: EGR1, TP53 "
Treatment: "Mylotarg, ATRA "
Survival: "5 days after diagnosis"

A patient of P. vera transformed to AML with complex karytoype
Diagnosis: "tAML"
Age: " "70 years (Male) ""
Karyotype: 61-63,<3N>,XY,-2,-3,-4,-5,-7,der(8)t(2;8)(?;p21),-9,+der(9)(?)x6,-10,-12,-13,-14,-15,-17,���-18,+der(18)t(11;18)(q13;p11.2),+21[25]
Treatment: "No data"
Survival: "No data"

Myeloid neoplasms with complex karyotypes predict poor prognosis"
No Diagnosis (age)
Treatment Karyotype Amplification
Increased copies
Deletion Survival
1 AML (74) Mylotarg, ATRA Complex MLL, ATM - EGR1, TP53 5 days
2 MDS/AML (65)
Doxorubicin, AraC HU " Complex MLL TP53 EGR1, AML1, TEL
8 months
3 MDS (74) NA Complex MLL ATM EGR1, TP53 NA
4 AML (87) No RX Complex MLL, ATM - EGR1, TP53 <5 days
5 MDS/AML (69)
Ida/Ara C refractory disease failed induction "
Complex MLL ATM EGR1, TEL 1 month
6 MDS/AML (69)
Topotecan/Ara C G-CSF persistent leukemia "
Complex MLL, ATM - EGR1, TEL 8 months
7 p.veraàAML NA Complex MLL ATM EGR1, TEL NA
8 AML (49) Ara C/Ida R " Complex - - EGR1, TP53 1 month
9 CML (69) HU, Ida/Ara " Complex MLL ATM EGR1, TP53 1 month
10 AML (65) No RX Complex MLL, ATM - EGR1, TEL 4 days
11 MDS/AML (75)
No RX Complex MLL - EGR1, TEL 1 month

September 22, 2015 Page 27
Acute Lymphoblastic Leukemia (ALL): Cytogenetics Diagnostic and prognostic significance"
Chromosome change Genes involved Subtype Diagnosis/Prognosis High hyperdiploidy
(>55 chromosomes)
Not known
(+4,+6,+8,+10,+14,+21)
Pre-B Good
(>90% cure in children)
Near haploidy (26-28) Not known Pre-B Poor (short complete remission)
Normal -- -- Poor
t(9;22)(q34;q11.2) BCR/ABL (p210 or p190)
B-cell (stem cell or progenitor)
Poor
t(4;11)(q21;q23) AF4/MLL B-cell (biphenotypc)
(also AML M5)
Short CR and prompt relapse
Generally Poor
t(11;19)(q23;p13.3) MLL/MLLT1 B-cell (biphenotypc)
Very Poor
t(12;21)(p12;q22) ETV6(TEL)/RUNX1(AML1) B-cell Excellent
t(8;14)(q24;q32) t(2;8)(p12;q24) t(8;22)(q24;q11)
MYC/IGH MYC/IGK MYC/IGL
B-cell ALL(L3) /NHL(BL)
Diagnostic and Adverse
t(1;19)(q23;p13) PBX/E2A ALL Adverse
Accumulation of malignant and immature lyphoid cells in marrow

September 22, 2015 Page 28
Chromosomal abnormalities in ALL: T-Cell ���Diagnostic and prognostic significance
Chromosome change Genes
involved
Subtype Diagnosis/
Prognosis
t(10;14)(q24;q11) HOX11/TCRA T-‐cell Favorable (Adult)
t(7;10)(q34;q24) TCRB/HOX11 T-‐cell Not known
t(11;14)(p13;q11) LMO2/TCRA T-‐cell Not known
t(8;14) (q24;q11) MYC/TCRA T-‐cell Poor
t(7;9)(q34;q34) TCRB/NOTCH1 T-‐cell Not known
inv(14)(q11q32.1)
t(14;14)(q11;q32.1)
TCRA-‐TCRD/TCL1 T-‐ PLL
AT
T-‐cell leukemia
/lymphoma
Aggressive course
NUP214/ABL1 amplificaWon ABL1 and NUP214(CAN)
T-‐cell SensiWve to Tyrosine Kinase inhibitor Gleevac

Cytogenetic Subsets in Pediatric ALL"
Mullighan CG. J. Clin Invest. 122; 3407, 2012
Favorable outcome
Poor outcome
Excellent prognosis
Poor prognosis
Poor outcome

Karyotype showing near haploid chromosomes in an ALL patient
Karyotype: 27<1N>,XY,+14,+18,+21

t(4;11)(q21;q23) in ALL
A: Karyotype--46,XY,t(2;19)(q23;q13.4),t(4;11)(q21;q23)
B: FISH: MLL break apart probe

September 22, 2015 Page 32
Prognostic Impact of Diagnostic Karyotypes in Pediatric ALL"
Karyotype
Event Free Survival (%)
2 yrs 5 yrs >50 chromosomes 90 80
47-50 chromosomes 70 60
Normal karyotype 70 60
t(1;19)(q23;p13) 50 40
t(9;22)(q34;q11.2) 40 30
t(8;14)(q24;q32) 40 30
11q23 abnormalities 30 20
Hypodiploid (<46) 30 20
t(4;11)(q21;q23) 20 20
Heim and Mitelman, 1995

Cytogenetics: Mature B- and T-Cell Lympoma

September 22, 2015 Page 34
Chromosome Translocations: Lymphocyte Development • Translocations are considered to arise as errors during intragenic physiologic rearrangements that assemble productive copies of IG and TCR genes during normal B- and T-cell development
• Translocations tend to be specific for breakpoints and show a high degree of association with histologic subsets
• Three Main Subsets of NHLs:
-- B-Cell
-- T-Cell/Natural Killer (NK) Cell
-- Hodgkin’s Lymphoma (HL)
• First description of karyotype in BL in 1963 (Jacobs et al., 1963)
• Identified as t(8;14)(q24;q32) in 1972 (Manolov and Manolova, 1972)
• t(8;14) was shown that MYC rearranges with IGH (Dalla-Favera et al., 1987)

September 22, 2015 Page 35
Burkitt’s Lymphoma"
Primary Chromosome change:
• --t(8;14)(q24;q32) MYC/IgH • Variant translocations:
• -- t(8;22)(q24;q11) (MYC/IgL)
• -- t(2;8)(p11;q24) (IgK/MYC)
• Duplication 1q: progression

September 22, 2015 Page 36
Follicular Lymphoma
Primary Chromosome Change: t(14;18)(q32;q21) (IgH/BCL2)(>75%)
variant translocations involving 18q21 break point (BCL2)
» 3q27 rearrangements (BCL6) » 6q21 deletions
t/der(1q), +7, del(6q), del(17p): Progression/transformation
t(14;18) negative tumors do exist, which exhibit complex and heterogeneous breakpoints (3q27; 8q24, ect)

September 22, 2015 Page 37
Diffuse Large B-Cell Lymphoma (DLBCL)
Generally complex, hyperdiploid
t(14;18)(q32;q21) (IgH/BCL2) followed by 3q27 rearrangements (BCL6)(many partners) t(8;14)(q24;q32) (MYC/IgH) Correlations with chromosome changes contradictory
-- der(1)(q21), +7, del(6q), del(17p) Associate with progression/transformation; predict adverse outcomes
--Chromosome amplifications frequent

September 22, 2015 Page 38
t(11;14)(q13;q32): The cytogenetic hallmark found in 70% of cases (CCND1/IgH)
• Monosomy 13/del(13q)
Mantle Cell Lymphoma (MCL)

del (17p13) (TP53) (v)"
del(11q22-q23) (ATM) (iv)"
Trisomy 12 (ii)"
Normal (iii)"
del(13q14.3)(sole) (i)"
"
Adverse
Progression "
Intermediate"
Intermediate"
Favorable"
30 "
80 "
115 "
110"
135
Chronic lymphocytic leukemia (CLL/SLL) A chronic lymphoproliferative disorder of mature B-lymphocytes
Tumor cells are inert with only a small proliferative compartment 50-60% abnormal by karyotype (>80% by FISH)
Chromosome change Prognosis OS (mo)
FISH panel targeting all the above changes
Absence of IGHV mutation: Aggressive course

Prognosis of deletions in CLL"
Dal Bo M et al. GENES, CHROMOSOMES & CANCER (2011)

September 22, 2015 Page 41
Multiple Myeloma (MM)
Cytogenetic change" Genes" Prognosis"
Hyperdiploidy (3, 5, 9, 11, 15, and 19)"
Not known" Good"
1p deletions" Not known" Poor"
14q32 rearrangements"
(at least 5 partners)"
IGH"
(partners: FGFR3, cMAF)"
Poor"
11q13, t(11;14)" IGH/CCND1" Favorable outcome"
6q deletions" MYB" --"
Del(13q)/-13" D13S319" Adverse outcome; shorter survival"
Karyotype detects only 30-50% cases with abnormalities
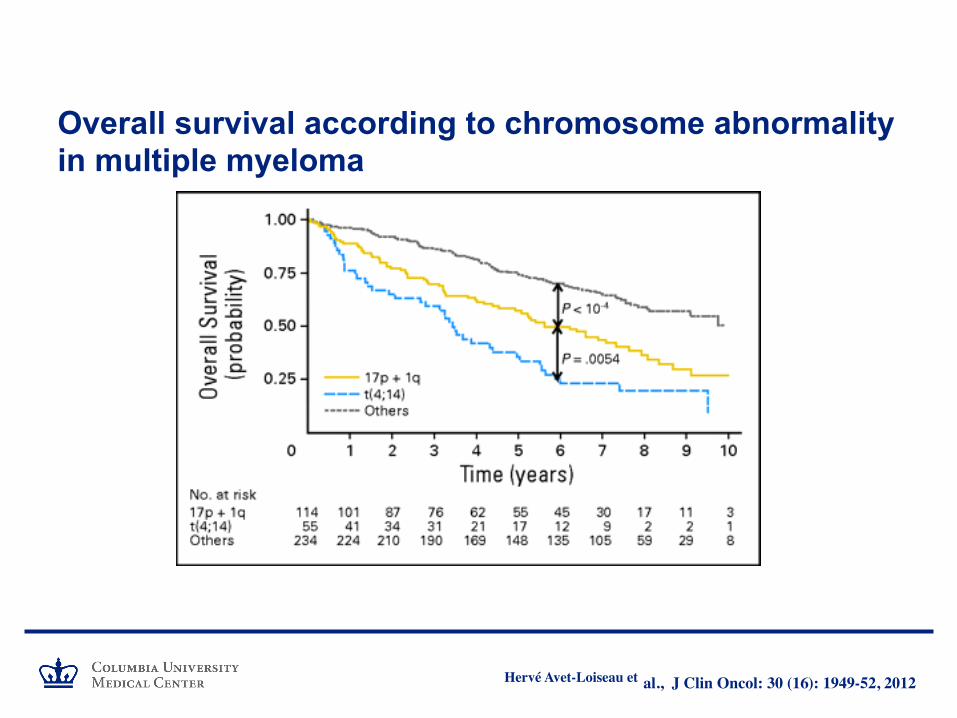
Overall survival according to chromosome abnormality in multiple myeloma
Hervé Avet-Loiseau et al., J Clin Oncol: 30 (16): 1949-52, 2012

Mature T-cell Neoplasms
Entity"
Chromosome change"
Anaplastic large cell lymphoma
t(2;5)(p23;q35) (NPM/ALK) Other partners exists; favorable prognosis
T-cell prolymphocytic leukemia (T-PLL)"
inv(14)(q11q32), t(14;14)(q11;q32)"(TCRa/d-TCL1)"7q34-36 translocation (TCRB)"
Angioimmunoblastic T-cell lymphoma"(EBV+ve in >75%)"
Trisomy 3 or i(3q), +5, +X, del(6q)"

Chromosome change in Anaplastic Large Cell Lymphoma (ALCL)

Genetic hallmark of T-PLL is inv(14)(q11.2q32) or t(14;14)(q11.2;q32) TCL1 gene at 14q32 juxtapose next to TCRA/D locus at 14q11.2 resulting in up regulation of the TCL1 expression. The TCR-associated translocations are regarded as the primary oncogenic events in T-PLL. T-PLL are generally very aggressive tumors among T-cell lymphomas and poorly responsive to chemotherapy.

September 22, 2015 Page 46
Karyotype Changes in NHL: ���diagnostic and prognostic significance
Type Diagnostic Change Progression/ Transformation
Poor outcome Good outcome
B-CLL/SLL - +12,del(11q23),t(14q32)
+12, del(11q) del(13q)
MM/LPL t(9;14)(p13;q32) - -13/del(13q) -
MALT t(11;18)(q21;q21) - - -
FL t(14;18)(q32;q21) +7,del(q),t(8;14) t(8;14) -
MCL t(11;14)(q13;q32) - del(17p) -
DLBCL - der(1q21),+7,del(6q),del(17p)
der(1q21),del(6q),del(17p
BL t(8;14)(q24;q32) dup(1q) - -
ALCL
(anaplastic)
t(2;5)(p23;q35) t(2;5)(p23;q35)
Chromosome abnormalities of 1, 6, and 17 are virtually seen in all lineage NHLs: Associated with poor clinical outcome

Solid Tumor Cytogenetics

September 22, 2015 Page 48
Ewing sarcoma/Primitive neuroectodermal tumor"• Heterogeneous group of distinct histologic types
• 90% cases with t(11;22)(q24;q12); in all histologic types
• Translocation results in the fusion of the EWS with FLI1, forming a chimeric protein
• variant translocations: t(21;22)(q12;q12)[EWS-ERG] and t(7;22)(p22;q12) [EWS-ETV1 in 5% cases
• EWSR1 is also rarely rearranged in other soft tissue tumors (Myxoid chondrosarcoma, Desmoplastic small round cell tumor, malignant melanoma of soft parts)

Page 49
Other soft tissue tumors- Karyotypic Changes
Tumor Chromosome translocation
Genes Comments
Myxoid liposarcoma" t(12;16)(q13;p11)"
Variant: t(12;22)"
DDIT3 (CHOP)-FUS (TLS)"
DDIT3/EWS"
Fusion protein; oncogenic"
Alveolar rhabdomyosarcoma (A-RMS)"
t(2;13)(q35;q14) (~80%)"
t(1;13)(p36;q14) (~15%)"
Variants"
PAX3 - FOXO1 (FKHR)"
PAX7-FKHR"
Poorer survival than ERMS"
ARMS and ERMS are two distinct genetic entities"
Synovial sarcoma" t(X;18)(p11.2;q11.2)"
Variants"
SSX1, SSX2, SSX4-SYT (SS18)"
Hybrid protein"
Poor prognosis"

Page 50
Neuroblastoma Sympathetic neuronal precursor: Embryonic origin
Common Extracranial pediatric tumor of infancy
Classified as low, intermediate, and high-risk groups
"
Two major types of Cytogenetic abnormalities:
Segmental chromsome aberrations 1p and 11q deletion (LOH)—High-risk
Amplification of NMYC is the most robust prognostic factor in NB

Landscape of genetic changes in neuroblastoma"
Page 51
Pugh TJ et al., Nat Genet 45: 279, 2013

September 22, 2015 Page 52
Gene Amplification: Double Minute Chromosomes

Tumors of Nervous System Gliomas
Oligodendrogliomas
Page 53
• 1p36 and 19q13 co-deletion occur in over 75% both grade II and III oligodendrogliomas • Correlate with response to chemotherapeutic drugs and radiation
1p36/1q25" 19q13/19p13" 1p36/1q25" 19q13/19p13"

Page 54
ALK break apart Probe for Lung Cancer
• In non-small cell lung cancer (NSCLC) development rearrangements of ALK gene are implicated"
• Rearrangement of ALK with echinoderm microtubule-associated protein-like 4 gene (EML4) results in in-frame fusions of EML4-ALK genes."
• ALK also forms fusions partners with TFE and KIF5B genes."
• Patients with ALK rearrangement positive NSCLC are eligible for treatment with crizotinib and achieves high-rate of tumor response in first 8 weeks.

Case History of a Patient with ALK+ve
• A 61 yr. old male, former smoker with stage IV lung cancer, with multiple rounds of chemo, metastatic to liver and bone.
• After 4 years of chemotherapy, no response was seen.
• The patient was about to enter hospice, but
• Patient sought 2nd opinion at CUMC and among other tests ALK was tested and found positive for rearrangement.
• The patient was treated with Xalkori (trade name for Crizotinib) and achieved complete remission in 10 weeks.
Apparently responded to targeted therapy
September 22, 2015 Page 56
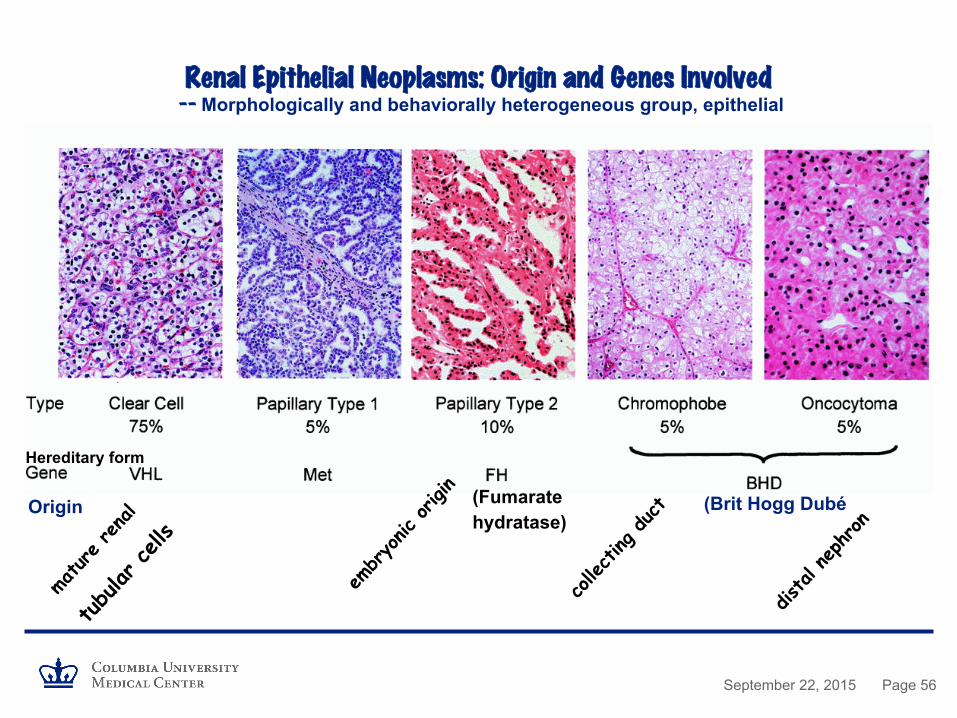
Renal Epithelial Neoplasms: Origin and Genes Involved��� -- Morphologically and behaviorally heterogeneous group, epithelial
Origin (Brit Hogg Dubé
Hereditary form (Fumarate hydratase)

September 22, 2015 Page 57
Clear Cell RCC
• Characteristic feature: Loss of 3p due to deletions or unbalanced translocations
• Number of common regions of deletions identified: 3p14, 3p21, and 3p25 (3q21 is essential)
• Trisomy 5q21-qter (partial trisomy): Predictive of good prognosis
• +12, +20
• Germ line mutation in VHL gene at 3p25 in familial cases
• No consensus on tumor suppressor on 3q21(Candidates: RASSF1A, FHIT, DUTT1, TTRC1, NRC1)

September 22, 2015 Page 58
Papillary RCC • Tri- or Tetrasomy of 17, 7, 16, 20, 12 • Loss of Y in men • Loss of Y, +7, +17 may correspond to papillary adenomas • Additional changes diagnostic papillary RCC • Inherited form of pRCC--Missense mutations in MET oncogene

September 22, 2015 Page 59
• Chromosome modal number 38-39"• Loss of chromosomes 1, 2, 6, 10, 13, 17, and 21"
• Difficulties in differential diagnosis from Oncocytoma"
• Karyotype (FISH) is useful in differential diagnosis
Chromophobe RCC

September 22, 2015 Page 60
CCND1 rearrangement of 11q13 in Oncocytoma

September 22, 2015 Page 61
Testicular Germ Cell Tumors
• Seminoma and Non-seminoma
• Over representation of 12p --85% with one or more copies of i(12p)
--tandem duplications of 12p (10%)
--Rarely, 12p amplification

September 22, 2015 Page 62
Her-2/neu (ERRB) Amplification in Breast Cancer
• ERBB2 gene is amplified and overexpressed in 20-25% of breast tumors
• Tumors showing ERBB2 amplification have predominantly lost estrogen receptor expression (ER-)
• Worsened course of the disease
• Target for therapeutically approaches using engineered anti-ERBB2 antibodies

September 22, 2015 Page 63
Utilities of Tumor Cytogenetics • To Establish Malignant Clone (normal karyotype doesn’t rule out)
• To Clarity/Establish Diagnosis
• To Indicate Prognosis (some changes associated with poor response)
• To Assist in Choice of Treatment Strategy
• To Monitor Response to Treatment
• To Establish Engraftment Status and Monitor
Number of targeted therapies already exists against specific genetic change that patient’s tumor uniquely possesses. "
"


















