Shashank V. Joshi, MD, FAAP Jeremy Wilkinson, MD Lucile Packard Children’s Hospital at Stanford

Raul V. Destura MDInternal Medicine-Infectious Diseases
Director, Institute of Molecular Biology and Biotechnology,
National Institutes of Health
Convenor, Study Group on Enteric Diseases in the Philippines

The Interaction of Malnutrition and Infection Micronutrients and Infectious Disease Resistance
Broadening Focus on Human Pathogens and Resistance Focus on HIV
Immunonutrition and Sepsis
Newer Paradigms on the Research Horizon

Critical Care Nutrition (Canada)
NCBI Resource: Pub Med


Protein-energy malnutrition is usually measured in
terms of body size
Indicators in children Stunting: low height-for-age Underweight: low weight-for-age Wasting or acute malnutrition: low weight-for-height
Indicators in adults Low body mass index (BMI)

in its mild and moderate forms is not always recognized
often referred to as “hidden hunger”
Most commonly reported micronutrient deficiencies in both adults and children are
• iron
• vitamin A
• iodine deficiency
Micronutrient malnutrition

Deficiencies in other vitamins and minerals that
are vital for the body’s normal functions and for the
work of the immune system are not commonly
measured, but they occur frequently in populations
with high infectious disease burden
monotonous, poor quality diets
diets characterized by limited consumption of animal products and seasonal or periodic food insecurity

Infections affect nutritional status by reducing dietary intake and nutrient absorption, and by increasing the utilization and excretion of protein and micronutrients as the body responds to invading pathogens.
Anorexia, fever, and catabolism of muscle tissue frequently accompany
the acute phase response
Even mild infectious diseases influence nutritional status
Almost any nutrient deficiency, if sufficiently severe, will impair resistance to disease.

Infections also result in the release of pro-oxidant cytokines and other reactive oxygen species.
The relationship between HIV and nutrition is complicated by the fact that the virus directly attacks and destroys the cells of the immune system.
The vicious cycle of micronutrient deficiencies and HIV pathogenesis: Nutritional deficiencies affect immune functions that
may influence viral expression and replication, further affecting HIV disease
HIV affects the production of hormones which are involved in the metabolism of carbohydrates, proteins and fats

As adjuvant to the mitigation of Infections Vitamin A Supplementation
Extensive research and meta-analysis largely confirms:
Survival Advantage and reduction in morbidity for complicated Measles
(Hussey GD & Klein M, 1990; Coutsoudis A., et. al., 1991; HuimingY, et. al., 2005)
Zinc Supplementation + ORS Reduces the duration and severity of episodes and has been
officially recommended by WHO (WHO 2004)

In the prevention of Infections
Vitamin A Supplementation Prevents infectious disease complications among small premature
infantsDarlow BA., et al. Cochrane Review. 2002
Zinc Supplementation Reduces risks of infection and re-infection of Enteric Pathogens
Roy Sk., et al., 1999; Baqui AH, et al., 2002
Vitamin D Increasing promise for prophylactic application in epidemic viral
diseases such as Influenza and diverse microbial infections Tremyzaygues L., et al., 2006; Canell JJ., et al., 2006

Parasitic Infections
HIV

Malnutrition, protozoa and multicellular parasites
Classic scenario – depleting nutritional stores caused by intestinal hookworms
Vitamin A deficiency – filarial nematodes which have evolved elaborated retinoid receptor systems to access the vitamin A of their hosts
Sani BP & Comley JC., 1985

Human Immunodeficiency Syndrome Discovered in 1981
We are seeing a rising epidemic in the Philippines particularly among young urban professionals working in unique environments like the call centers

South African political cartoon, April 2005

The Vicious Cycle of Malnutrition and HIV is well recognized
Insufficient dietary intake
Malabsorption, diarrhea
Altered metabolism and
nutrient storage
Increased HIV
replication
Hastened disease
progression
Increased morbidity
Increased oxidative
stress
Immune suppression
Nutritional
deficiencies
Source: Semba and Tang, 1999
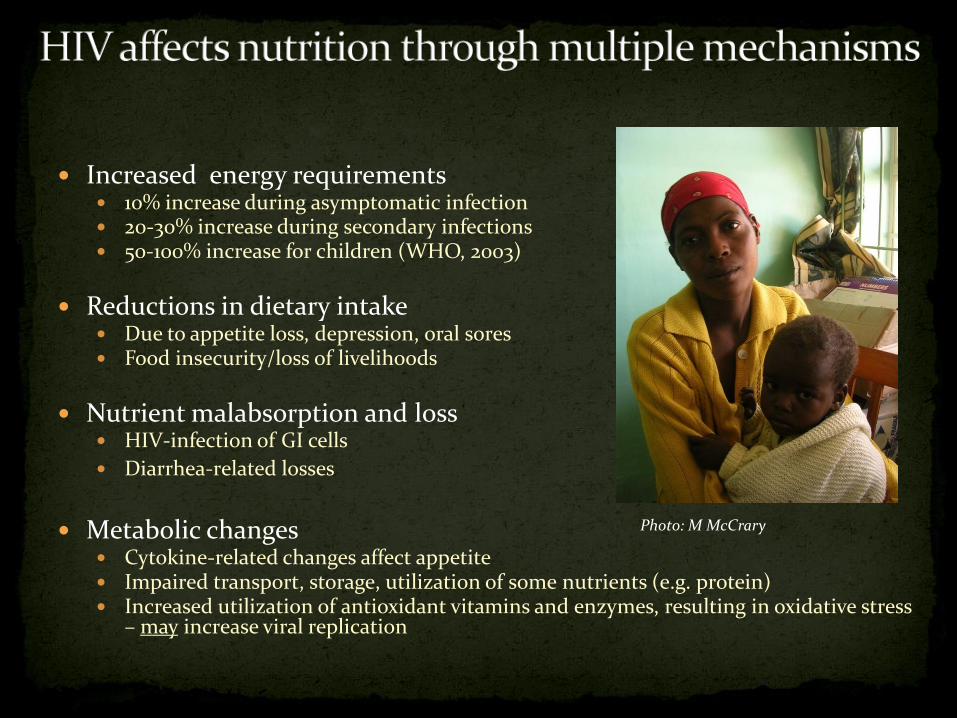
Increased energy requirements 10% increase during asymptomatic infection 20-30% increase during secondary infections 50-100% increase for children (WHO, 2003)
Reductions in dietary intake Due to appetite loss, depression, oral sores Food insecurity/loss of livelihoods
Nutrient malabsorption and loss HIV-infection of GI cells
Diarrhea-related losses
Metabolic changes Cytokine-related changes affect appetite Impaired transport, storage, utilization of some nutrients (e.g. protein) Increased utilization of antioxidant vitamins and enzymes, resulting in oxidative stress
– may increase viral replication
Photo: M McCrary

Micronutrients and host defence and resistance to infections in humans
Antioxidant capacity Immune system Resistance to infections
A ↑ ↑↑↑ ↑↑↑ / ↓
B ↑ ↑
C ↑↑↑ ↑
E ↑↑↑ ↑↑
Iron ↓ ↑ ↑/↓
Zinc ↑↑↑ ↑↑↑ ↑↑↑
Selenium ↑↑↑ ↑ ↑
↑: increase, ↓: decrease, number of arrows indicate relative importance, arrows in both directions indicate conflicting findings

Vitamin A Iron Zinc Multiple MN supplements


Perinatal and Child Outcomes- Mother-to-child transmission (MTCT)- Other birth outcomes (BW, SGA, prematurity)- Child morbidity, growth, and mortality- Child immunologic status
Adult Outcomes- Immunological and virological progression
- Clinical disease progression and mortality
Studies on micronutrients and HIV have measured a range of outcomes

Lack of adequate biomarkers of MN status, especially in presence of acute phase response
Underlying nutritional status, diet intake infrequently measured yet may affect relationships
• Sometimes causes conflicting results• Makes it difficult to compare across studies
Potential confounding (SES/poverty) & HIV-related reporting bias for dietary intakes when measured


Early observational studies showed an inverse dose-response relationship between maternal serum retinol and HIV viral load (Kenya) and MTCT of HIV-1 (Malawi)
Semba, Lancet 1994;343:1593
Serum retinol mmol/L
MALAWI
Nduati, J Infect Dis 1995;172:1461
KENYA

As a result, several RCT were designed to look at the impact of Vitamin A supplementation on MTCT and related outcomes
Country Recruitme
nt
N Study intervention (placebo controlled) Co-interventions (to all)
Micronutrien
t
Daily Postpartum Iron/folate
(mother)
Vitamin A
South
Africa
28-32 wk 728 Vitamin A 5.000 IU + 30 mg -carotene 200.000 IU 60/5 mg/day
Malawi 18-28 wk 697 Vitamin A 10.000 IU 30/0.4 mg/day 100.000 IU at 6 weeks
(mother)
Tanzania
Zimbabwe
14-27 wk
1-4 d
1075
4495
Vitamin A
Multivitamins
Vitamin A
5.000 IU + 30 mg -carotene
Vitamins B, C and E
200.000 IU
Continued
400,000 IU
(Mother)
50,000 IU
(Baby)
120/5 mg/day 100.000 IU at 6, 12, 18
months (infant)
Coutsoudis et al – South Africa - Study intervention and iron/folate given from recruitment until delivery.
Kumwenda et al. – Malawi . Study intervention and iron/folate given from recruitment until delivery.
Fawzi et al. – Tanzania - Two-by-two factorial design, i.e. two placebo-controlled interventions. Study intervention and iron/folate given from recruitment and
throughout and several years after lactation. Multivitamins included 20 mg thiamin, 20 mg riboflavin, 25 mg vitamin B6, 50 mg vitamin B12, 100 mg niacin, 0.8
mg folate, 500 mg vitamin C, and 30 mg vitamin E.
Humphrey et al – Zimbabwe – Two by two factorial design that included > 9500 HIV negative mothers also. Mothers, babies randomized to single dose VA
or placebo
Adapted from Table by Friis, 2005

South Africa (Coutsoudis et al, 1999; Kennedy-Oji et al, 2002)
Lower risk of pre-term deliveries
No overall effect on MTCT Improved maternal PP weight
retention
Malawi (Kumwenda et al, 2002)
Higher BW & weight & length at 6 w,
Lower PNT 6 w-24 mo (2.8% vs. 7.7%; p=0.04)
Lower anemia at 6 w
Tanzania (Fawzi et al, 2000; 2002; Baylin et al, 2005)
Improved infant serum retinol, reduced VAD
No effect on birth outcomes No effect on PNT, mortality Total MTCT significantly higher
by 24 months (34.2% v 25.4%;p=0.009)
Zimbabwe (Humphrey et al, 2006)
If IP infected infants, VAS reduced mortality (by 28%; p = 0.01)
No effect on PNT 2-fold increased risk of death
in infants alive, PCR negative at 6 w

Positive impact of VAS on morbidity and growth of hospitalized children (HIV+/HIV-) – Tanzania Villamor et al. Pediatrics 2002
Positive impact of VAS on morbidity of HIV+ children – South Africa – Coutsoudis et al, 1995
No effect of VAS on vaginal shedding of HIV, plasma HIV levels, immune status in women – Kenya – Baeten et al, 2002
Suggestive effect of maternal VAS on risk of maternal HIV acquisition – Zimbabwe

Variable Adj. HR 95% CI p
Maternal VAS (vs. placebo)
1.09 (0.85, 1.38) 0.51
Age (y) 0.94 (0.92, 0.97) 0.001
Parity > 1 1.44 (1.07 – 1.93) 0.02
Serum retinol
< 70 mmol/L
10.43 (3.00-36.28) 0.001
Hb <70 g/L 2.68 (1.18-6.07) 0.02
Models adjusted for marital status*sexual activity & occupation
Incidence of new infections: 3.4% per year (95% CI: 3.0-3.8%)
VAS tended to be protective against incidence in women with low Se Retinol
Adj. HR = 0.29 (95% CI 0.03 - 2.60; P=0.26)


Anemia of chronic disease (ACD) Hb, Reticulocytes, Serum Fe, Transferrin, % Fe saturation,
normal or serum ferritin, low serum EPO, normal or Fe stores in bone marrow
Nutrient deficiencies (Fe, folate, B12)
Hookworm, malaria
Malignancies
Opportunistic infections of bone marrow
ART use (ZDV), other OI drugs suppress RBC production

51.9
68.964.7
78.481.778.9
0
25
50
75
100
Mali Cote d'Ivoire Burkina Faso
% l
ow
hem
og
lob
in
HIV+
HIV-
Sources: Mali (Diallo et al, 2003); CI (Ramon et al, 1999); BF (Meda et al, 1999)
… and is associated with higher maternal mortality, LBW, pre-maturity, MTCT (next slides)

Taha et al Bull WHO, 2006- Malawi – predictors of death by 24 months post-delivery
Adj HR 95% CI
BF status (yes/no) 0.35 0.12-1.03
Age (< 25 y) 0.71 0.35-1.46
Viral load(Log 10)
3.84 2.06-7.16
Hb (g/L) 0.80 0.68-0.93
BMI 0.82 0.75-1.00

Maternal Hb at delivery(g/L)
Adj. OR – IP (n=3375)
Adj. HR – PN(n=2870)
<70
70<90
90<110
>=110
2.40 (1.16-4.97; p=0.02)
1.53 (0.99-2.37; p=0.05)
1.25 (0.93-1.69; p=0.15)
1.00
2.66 (1.06-6.68; p=0.04)
1.02 (0.54-1.96; p=0.94)
1.03 (0.67-1.59; p=0.88)
1.00
Both models adjusted for maternal B/L plasma viral load, CD4 cell count
IP model: gestational age, duration of membrane rupture, infant birth weight
PN model: maternal age, MUAC, early feeding pattern, death during F/U
Neither VAS nor infant sex were significant predictors of IP, PN transmission

A few studies suggest that supplemental iron given to HIV+ may cause increased iron stores in bone marrow and other tissues, oxidative stress, faster HIV disease progression, and subsequent increased mortality (Friis et al., 2003; Boelart et al., 1996).
Associated with haptoglobin 2-2, a specific type of this heme-binding protein (Friis et al., 2003; Gordeuk et al., 2001; Delanghe et
al., 1998).

P=0.31 for test of difference in decline of VL between groups; no effect of Fe supplementation after controlling for baseline VL, hookworm infection


Early observational studies showed increased mortality (shorter survival) in HIV+ adults with higher zinc intakes
Additional concerns that Zn supplementation may induce HIV replication
HIV-Tat protein and HIV nucleocapsid protein NCp7, which play a role in viral replication, are strongly zinc dependent

96 HIV+ infants randomized to daily Zn sulfate (10 mg/d) vs. placebo in Durban, SA
Block randomization stratified by age (6-23 m, 24-41, 42-60 mo) Hypothesis: Zn will decrease plasma viral log (VL) by 0.5 log
HIV RNA, CD4, CD4 %, measured at baseline, 3 wks, 3 mo, 6 mo post-intervention (NO EFFECT)
Morbidity, growth, survival measured (BENEFIT-morbidity) - next slide
Author’s conclusion: “Zinc supplementation is safe and beneficial and 10 mg/day should be part of the nutritional package for HIV+ children”

Zinc Placebo
P*Routine All Routine All
# of visits 360 407 370 447
% watery diarrhea 6.7 7.4 10.5 14.5 0.001
% pneumonia 10.8 14.0 12.7 18.6 0.07
% URI 39.2 40.3 44.6 45.2 0.1
% ear infection 10.8 11.3 14.1 14.5 0.2
% tuberculosis 8.3 14.9 7.3 6.5 0.1
*Chi-square test comparing proportion of all visits with diagnosis

400 HIV+ women randomized to daily Zn (30 mg Zn sulfate) or placebo from 12-27 wks gestation to 6 wks post partum (fizzy tablet)
All received MV supplement (BCE), ferrous sulfate (400 mg=120 mg ferrous Fe), folate (5 mg) daily, prophylactic chloroquine, sd NVP
No effect of Zn on pregnancy duration (p=0.99), BW (p=0.96), BL (p=0.87), change in CD4 (p=0.97), CD4:CD8 (p=0.23)
Zn associated with non-significant increase in fetal, peri-natal & neonatal mortality & MTCT - next 2 slides
Zn associated with lower PP HB recovery (p=0.03), change in RBC count (p<0.01), packed cell volume (p=0.01), also associated with increased risk of wasting in HIV+ women (Villamor et al, 2006)

Non-significant adverse effect of maternal Zinc supplements on fetal and early postpartum infant survival
Outcome No. at
Risk
Zinc
n (%)
Placebo
n (%)
Relative risk (95%
CI)6
p-value
Abortion 397 5 (2.5) 3 (1.5) 1.68 (0.17, 40.3) 0.50
Stillbirth 397 13 (6.6) 10 (5.0) 1.31 (0.44, 4.55) 0.53
Fetal death1 397 18 (9.1) 13 (6.5) 1.39 (0.58, 3.86) 0.36
Perinatal death 397 28 (14.1) 20 (10.1) 1.41 (0.73, 2.96) 0.22
Neonatal death 397 10 (5.5) 7 (3.8) 1.44 (0.38, 7.04) 0.47
1 Includes stillbirths and abortions
Slide by W Fawzi; From Fawzi et al, 2004

Maternal Zinc supplements (25 mg/d) given in addition to vitamins BCE from 12-27 wks gestation through 6 wks post-delivery are associated with non-significant increases in MTCT in HIV+
Tanzanian mothers -2
Villamor et al, EJCN, 2006


Vit A
Beta
carotene Vit D
Vit E
Vit C
Vit B1
Vit B2Niacin
Vit B6
Vit B12Vit KFolic
Acid
Folacin Pantothenic
Acid
Iron Zinc
CopperSelenium
Iodine
Magnesium
Manganese Chromium
Cystine
Which combination/dose of micronutrients is the most effective and safe?
A Tomkins slide

Vit A
Beta
carotene Vit D
Vit E
Vit C
Vit B1
Vit B2Niacin
Vit B6
Vit B12Vit KFolic
Acid
Folacin Pantothenic
Acid
Iron Zinc
CopperSelenium
Iodine
Magnesium
Manganese Chromium
Cystine
Micronutrient formulation in Thai study (yellow)
A Tomkins slide

0.53
0.37
0.26
0
0.3
0.6
Overall CD4 <200 CD4 < 100
Adju
sted M
orta
lity
Ris
k(P=0.10)
(P=0.05)
(P=0.03)
There was no effect on HIV viral load, genital shedding

Vit A
Beta
carotene Vit D
Vit E
Vit C
Vit B1
Vit B2Niacin
Vit B6
Vit B12Vit KFolic
Acid
Folacin Pantothenic
Acid
Iron Zinc
CopperSelenium
Iodine
Magnesium
Manganese Chromium
Cystine
Micronutrient Formulation in Tanzania Trial

Relative Risk 95% CI P-value
AIDS related death
0.73 0.51-0.04 0.09
Progression to stage 4
0.50 0.28-0.90 0.02
Progression to stage 3
0.72 0.58-0.90 0.003
>= 2 stage increases
0.66 0.52-0.84 <0.001
Fawzi et al, NEJM, 2004
Mean diff in viral load = -0.18 log – or est. 30% increase in survival time

Relative Risk 95% CI P-value
Thrush 0.47 0.30-0.73 <0.001
Oral ulcers 0.44 0.28-0.68 <0.001
Dysentery 0.66 0.45-0.95 0.03
ARI 0.79 0.66-0.96 0.02
Fawzi et al, NEJM, 2004
Other protective effects – gingival erythema, angular chelitis, nausea and vomiting, difficulty swallowing, painful mouth, fatigue, rash

28 30 32 34 36 38 40
59
60
61
62
63
MV
NO MV
Weight (kg)
Week of Gestation
238 g/wk
185 g/wk

Fetal Death
Low Birthweight (<2500g)
Preterm Birth (<37 weeks)
Small for Gestational Age
Severe Preterm Birth (<34 weeks)
0 0.5 1.0 1.5 2.0
Slide from W Fawzi Relative Risk

….and prevented MTCT by most vulnerable mothersFawzi et al, AIDS, 2002
0.99
0.37
1.01
0.48
1.03
0.51
1.07
0.27
0.0
0.2
0.4
0.6
0.8
1.0
1.2
1.4
1.6
1.8
Relative Risk
P=0.03P=0.06 P=0.06
P=0.04

Reduced morbidity and hospitalizations in adults ( B, C, E - Fawzi et al, 2004; Se -Burbano et al, 2003)
Increased survival in adults (Fawzi et al, 2004; Jiamton et al, 2003)
Improved immune recovery in adults on HAART (Kaiser et al, 2006; Odunukwe, 2006)
Increased weight gain in HIV+ pregnant women (Villamor et al, 2002)
Reduced morbidity and improved growth in HIV+ children (Vitamin A – Coutsoudis et al, 1995; BCE – Villamor et al, 2002; 2005; Zinc – Bobat et al, 2005)
Improved birth outcomes and infant immune status (Fawzi et al, 1998; 2003; Friis et al, 2004)
Reduced MTCT in nutritionally and immunologically vulnerable (Fawzi et al, 2002)

“There is no conclusive evidence at present to show that MN supplementation effectively reduces morbidity and mortality among HIV-infected adults. It is reasonable to support the current WHO recommendations to promote and support adequate dietary intake of MN at RDA levels wherever possible. There is evidence of benefit of VA supplementation in children. The long-term clinical benefits, adverse effects, and optimal formulation of MN supplements require further investigation.” (Irlam et al, The Cochrane
Collaboration, 2005)

> 1 RDA may be needed to correct nutritional deficiencies
But there is concern that high doses of some nutrients may cause adverse outcomes.
Current MN requirements are similar for PLWHA until more data available (WHO 2003)
“Adequate intake is best met through an adequate diet. “ However, in settings where these intakes and status cannot be achieved, multiple micronutrient supplements may be needed in pregnancy and lactation. Pending additional information, micronutrient intakes at the RDA level are recommended for HIV-infected women during pregnancy and lactation.”

Vitamin A supplementation Clear evidence of benefit for HIV+ children No evidence of benefit for HIV+ mothers, with possible exception of
those who are severely deficient, and harm not ruled out
Zinc supplementation Evidence of benefit for HIV+ children No evidence of benefit for HIV+ adults (possible harm if not
deficient; same re: Se)
Iron supplementation Limited data Same recommendations as for HIV-negative pregnant women and
treatment of anemia


Insult
• infection• trauma• I/R• hypoxemic/hypotensive
Activation ofPMN’s
= oxidative stress
Death
organ = failure
Pathophysiology of Critical Illness (1)
mitochondrial dysfunction
Role ofGIT
Key nutrient deficiencies(e.g. glutamine, selenium)
activation of coagulation
generation of OFR (ROS + RNOS)
endothelial dysfunction
elaboration of cytokines, NO, and other mediators
cellular = energeticfailure
Microcirculatory Dysfunction


Metabolic Effects of Arginine
enteral / parenteralsupply
L-Arginine L-CitrullineL-Ornithine
Polyamine Synthesis
• Putrescine• Spermidine• Spermine
Hormone release
• GH• IGF• Insulin• Glucagon• Prolactin• catecholamines
Urea
Nitrogenous compounds
• Nitric oxide• Nitrite• Nitrate
Suchner Brit J Nutrition 2001

Mitaka Shock 2003;19: 305
Underlying PathophysiologyRole of Nitric Oxide

cNOS
cNOS + iNOS
Har
mfu
l
Arginine / NO
availability
Optimal NO-Balance
- Hemodynamic instability
- Immune Suppression
- Cytotoxicity
- Organe dysfunction
- Microcirculation
- Immune augmentation
Suchner Brit J Nutrition 2001

Randomized, double
blind, placebo-controlled
Beagles
Parenteral L-arginine (+
NAC) vs placebo
Canine model of E. coli peritonitis
Kalil Crit Care Med 2006;34:2719

Arginine administration
associated with:Plasma arginine
NO products
And worse shock,
worse organ injury
Increased mortality!
Kalil Crit Care Med 2006;34:2719
No effect of NAC

3 RCTs
3 different products
All describing excess
mortality in patients with infection
0
2
4
6
8
10
12
14
16
mortality
Arginine
Control
1) Bower Crit Care Med 1995;23:436
2) Dent, Crit Care Med 2003;30:A17
3) Bertolini Intesive Care Med 2003;29:834


Copyright ©2007 The American Society for Nutrition
Mechanisms by which fatty acids can affect immune cell function
Wanten, G. J. et al. Am J Clin Nutr 2007;85:1171-1184

NFκB Binding
CytokinesIL-8
TNF-α
PGE1
mRNA

CytokinesIL-8
TNF-α
PGE1
mRNA
NFκB Binding

T.T. Pluess1, D. Hayoz2, M.M. Berger1, L. Tappy3, J.P. Revelly1, B. Michaeli1, Y.A. Carpentier4 and R.L. Chioléro1

21 patients with sepsis requiring TPN
Randomized to recieve PN with an n-3 or n-6 lipid emulsion for 5 days
Dose: 350 ml og s 10% n-3 lipid emulsion (Omegevan)
Am J Respir Crit Care Med 2003; 167: 1321

TPN with N-3 vs n-6 FAs in severe sepsis. Monocyte membrane FA composition: arachidonic, EPA, DHA
Mayer K, Am J Respir Crit Care med 2003; 167: 1321
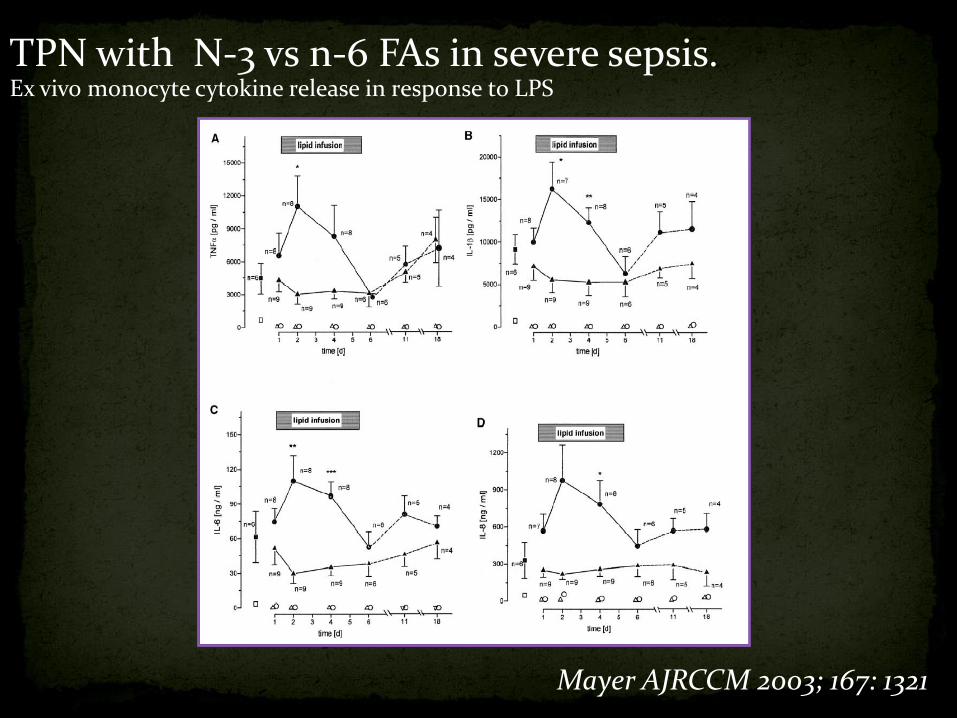
TPN with N-3 vs n-6 FAs in severe sepsis. Ex vivo monocyte cytokine release in response to LPS
Mayer AJRCCM 2003; 167: 1321

47 Patients with severe acute pancreatitis
Randomized, double blind study of PN
N-3 lipid emulsion (omegaven 10%) vs. Soybean emulsion with TPNx 5days
Dose of fish oils: 0.15-0.20 g/kg/d
Patients comparable at baseline
Control group mortality 10%; no deaths in FO group
Wang JPEN 2008;32:236

Put figure 2 and 3
Wang JPEN 2008;32:236

RCT of 146 critically ill
patients with ALI and BAL+
for WBCs
Double-blinded; ITT
Experimental: Oxepa®
Control: high fat diet
Groups well matched at
baseline
Gadek Crit Care Med 1999;27:1409
After 3-4 days
• Reduction in AA and increase in EPA in lung and alveolar macrophage
• Decrease in neutrophils recovered in BAL fluid
• Improved oxygenation

RCT of 146 critically ill
patients with ALI and BAL+
for WBCs
Double-blinded; ITT
Experimental: Oxepa®
Control: high fat diet
Groups well matched at
baseline
0
5
10
15
20
25
Vent
Days
ICU
Days
ICU
Deaths
Oxepa
control
Gadek Crit Care Med 1999;27:1409
P=0.03 P=0.17P=0.02

www.criticalcarenutrition.com


Potential Beneficial Effects of Glutamine
Fuel for
Enterocytes
Fuel for
Lymphocytes
Nuclotide
Synthesis
Maintenance of
Intestinal
Mucosal Barrier
Maintenance of
Lymphocyte
Function
Preservation
of TCA Function
Decreased FreeRadical availability (Anti-inflammatory action)
Glutathione
Synthesis
GLN
pool
GlutamineTherapy
Enhanced Heat
Shock Protein
Anti-cataboliceffect
Preservation of Muscle mass
Reduced
Translocation
Enteric Bacteria
or Endotoxins
Reduction of
Infectious
complications
Inflammatory Cytokine
Attenuation
NF- B
?
Preserved CellularEnergetics-ATP content
GLN
Pool
Critical Illness
Enhancedinsulinsensitivity

Effect of Glutamine:A Systematic Review of the Literature
www.criticalcarenutrition.com
Infectious Complications

Effect of Glutamine:A Systematic Review of the Literature
www.criticalcarenutrition.com
Mortality

Pharmaconutrients Impact Outcomes!
www.criticalcarenutrition.com
1 10 1000.1.01
Glutamine
Antioxidants
Fish/Borage OilsPlus AOX
Effect on Mortality
Arginine

Death
Metabolic
Shutdown
Survivors
•↓mt DNA
•↓ ATP, ADP,
NADPH
•↓ Resp chain
activity
•Ultra structural
changes
↓ mitochondrial
activityProlonged
inflammationNO
Endocrine
effects
cytokine
effect
Genetic down
regulation
Tissue
hypoxia
• preserved ATP
•Recovery of mt DNA
•Regeneration of mito
proteins

Hypoxia Accelerates Nitric Oxide Inhibition of Complex 1 Activity
Nitration of Complex 1 in Macrophages activated with LPS and IFN
21% O2 1% O2
Frost Am J Physio Regul Interg Comp Physio 2005;288:394
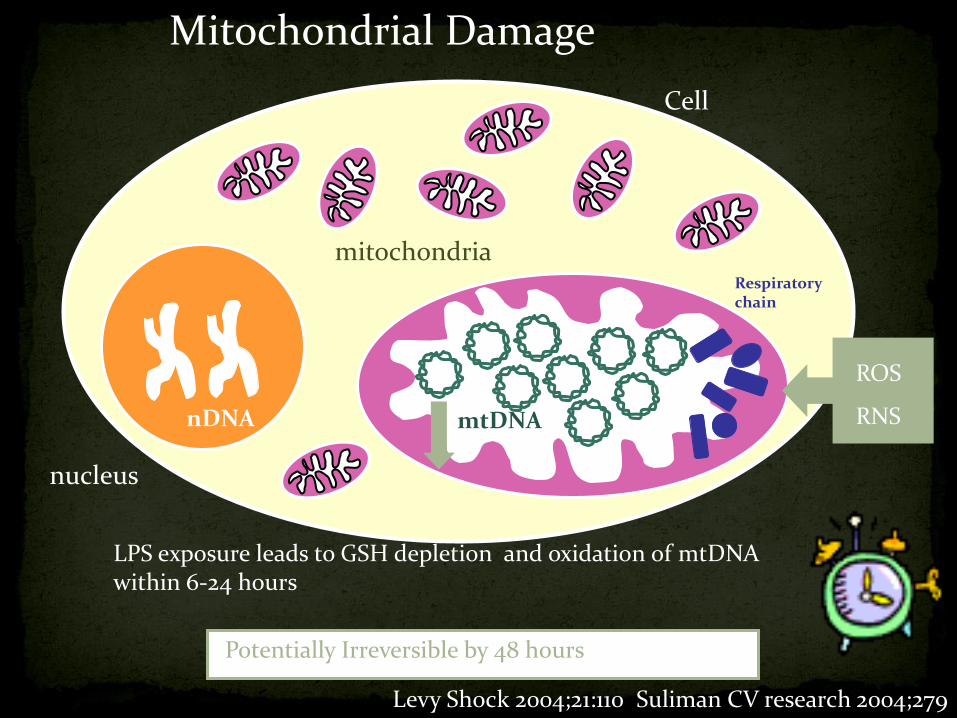
mitochondria
Cell
Respiratorychain
nucleus
nDNA mtDNA
Mitochondrial Damage
ROS
RNS
LPS exposure leads to GSH depletion and oxidation of mtDNA within 6-24 hours
Levy Shock 2004;21:110 Suliman CV research 2004;279
Potentially Irreversible by 48 hours

mtDna/nDNA Ratio by Day 28 Survival
0 5 10 15 20 250.0
0.5
1.0
1.5
2.0
Alive Individuals
Expired Individuals
Alive Reg line
Expired Reg Line
P=0.04
Day
mtD
na
/nD
NA
Ra
tio
Heyland JPEN 2007;31:109

Effect of Antioxidants on Mitochondrial Function
Heyland JPEN 2007;31:109

Single center RCT double-blinded
ITT analysis
40 patients with severe sepsis Mean APACHE II 18
Primary endpoint: need for RRT
standard nutrition plus 474 ug x 3 days, 316 ug x 3 days; 31.6 ug thereafter vs 31.6 ug/day in control
Mishra Clinical Nutrition 2007;26:41-50

Increased selenium levels
Increased GSH-Px activity
No difference in
• RRT (5 vs 7 patients)
• mortality (44% vs 50%)
• Other clinical outcomes
Mishra Clinical Nutrition 2007;26:41-50
*p=<0.006
* *
Effect on SOFA scores
•

0
50
100
150
200
250
0 1 2 3 4 5
Cardiac
Trauma
SAH
CRP levels daily in the Control groups
Significant reduction with AOX in Cardiac and Trauma but not SAH
Berger Crit Care 2008
RCT
200 patients
IV supplements for 5 days after admission (Se 270 mcg, Zn 30 mg, Vit C 1.1 g, Vit B1 100 mg) with a double loading dose on days 1 and 2 (AOX group), or placebo.
No affect on clinical outcomes

Nathens Ann Surg 2002;236:814
Surgical ICU patients, mostly trauma
770 randomized; 595 analysed
alpha-tocopherol 1,000 IU (20 mL) q8h per naso- or orogastric tube and 1,000 mg ascorbic acid IV q8h or placebo
Tendency to less pulmonary morbidity and shorter duration of vent days

Multicenter RCT in Germany double-blinded
non-ITT analysis
249 patients with severe sepsis
standard nutrition plus 1000 ug bolus followed by 1000 ug/day or placebo x14 days
0
10
20
30
40
50
60
70
80
90
100
28 day Mortality
Selenium
Placebo
Greater treatment effect observed in those
patients with:
•supra normal levels vs normal levels of selenium
•Higher APACHE III
•More than 3 organ failures Crit Care Med 2007;135:1
p=0.11

Effect of Combined Antioxidant Strategies in the Critically Ill
Effect on Mortality
www.criticalcarenutrition.com

Inflammation/oxidative stress
Mitochondrial dysfunction
Organ dysfunction
Antioxidants
Antioxidants
Antioxidants

INTESTINAL EPITHELIUM
SIRS
Bacteria
DISTAL ORGAN
INJURY
(Lung, Kidneys)
via thoracic duct
Underlying Pathophysiologyof Critical Illness (3)

Characteristics : Time dependentCorrelation to disease severity
Consequences: Risk of infectionRisk of MOFS

• Maintenance of gut barrier function
• Increased secretion of mucus, bile, IgA
• Maintenance of peristalsis and blood flow
•Attenuates the stress response
Alverdy (CCM 2003;31:598)

www.criticalcarenutrition.com

www.criticalcarenutrition.com


The Keshan’s disease story
Progressive fatal pulmonary disease
Associated with low selenium levels
Murine model of pulmonary infections using benign mouse coxackie virus Same virus turned virulent when selenium deficient mice were
inoculated
THIS OBSERVATION POINST TOWARDS A NEW DEPARTURE IN NUTRITION:INFECTION INTERACTIONS – WHERE THE MICRONUTRIENT STATUS OF THE HOST COULD DETERMINE THE VIRULENCE OF PATHOGENS ACROSS A WHOLE SOCIETY


















