
Pancreas Transplantation - Avera Health 1 Pancreas Transplantation Ahmad Bashar Abdulkarim, MD, PhD,...
30
3/24/2015 1 Pancreas Transplantation Ahmad Bashar Abdulkarim, MD, PhD, FACS Transplant Surgery Avera Health Center Sioux Falls, SD Pancreas Transplantation Facts: • Diabetes patients with chronic kidney disease (CKD) experience excessive morbidity and mortality • Simultaneous pancreas and kidney (SPK) Simultaneous pancreas and kidney (SPK) transplantation has been shown to significantly improve quality of life, and increase life expectancy of uremic diabetes patients
Transcript of Pancreas Transplantation - Avera Health 1 Pancreas Transplantation Ahmad Bashar Abdulkarim, MD, PhD,...

3/24/2015
1
Pancreas Transplantation
Ahmad Bashar Abdulkarim, MD, PhD, FACS
Transplant Surgery
Avera Health Center
Sioux Falls, SD
Pancreas Transplantation
Facts:
• Diabetes patients with chronic kidney disease (CKD) experience excessive morbidity and mortality
• Simultaneous pancreas and kidney (SPK)Simultaneous pancreas and kidney (SPK) transplantation has been shown to significantly improve quality of life, and increase life expectancy of uremic diabetes patients

3/24/2015
2
Pancreas Transplantation
Facts:
• One-year and 5-year pancreas graft survival rates are now comparable with those of kidney, liver, and heart transplants
• Half life of an SPK is about 14 years
Pancreas Transplantation
• IndicationsA- Simultaneous kidney and pancreas transplant (SPK): ESRD secondary to diabetic nephropathy.
B- Pancreas Transplant alone (PTA):
* Brittle diabetics Brittle diabetics
* Frequent episodes of DKA
* Hypoglycemic unawareness

3/24/2015
3
Pancreas Transplantation
• ContraindicationsA- Malignancy:A- Malignancy:
* Screening* Free of recurrence for 2 years before the transplant; this will eliminate about 2/3 of recurrences
-Malignant melanomas, breast Ca, and Colon Ca with higher tumor stages; nodalColon Ca with higher tumor stages; nodal involvement (5 years)- Carcinoma in situ; skin, small incidental renal cell carcinoma (no waiting time)
Pancreas Transplantation
• Contraindications
B- Infections
Viruses:
HIV: [HAART] Small series show comparable outcomes.
Grossi, PA et al, Transplantation, 2012; 12(4): 1039-1045

3/24/2015
4
Pancreas Transplantation
B- Infections
Viruses:
HBsAg+:
KTx; Similar pt and graft survival but higher risk of dying of hepatic failure
PTx; Few reports with encouraging results when using Lamivudine for the first year post transplantation.
Reddy et al, Clin Am J Soc Neph 2011 6(6): 1481-7
Akalin E, Clin Transplant 2005, 19(3): 364-6
Pancreas Transplantation
B- Infections
Viruses:
HepC: No significant effect on graft or patient survival, small reports.
Miguel M et al, Transplantation 2010; 90(1):61-67

3/24/2015
5
Results of SPK Transplantation in The USA
Pancreas Transplantation
T1DM vs T2DMT1DM vs.T2DM
-Obesity, and later age of onset, for example, often blur the diagnosis between T1DM vs. T2DM.
-C-peptide (renal failure/gastroparesis.. False elevation)

3/24/2015
6
Pancreas Transplantation
T2DMT2DMThe pathophysiology of T2DM includes genetic causes of
chronic inflammation and insulin resistance leading to hyperinsulinemia, which ultimately results in beta-cell exhaustion.
T1DMPatients classically suffer autoimmune-mediated damage to beta cells leading to decreased (or absent) insulin secretion.
Pancreas Transplantation
Given the increasing prevalence of T2DM in most westernGiven the increasing prevalence of T2DM in most western countries, and
Given that T2DM is among the leading causes of kidney disease,
Therefore, pancreas transplantation may
be underutilized in this population. Currently,
• 8% of SPKs in the USA are performed for T2DM, and 5% and 1% for PAK and PTA, respectively

3/24/2015
7
Pancreas Transplantation
Indications for SPK in T2DMIndications for SPK in T2DM-BMI <28
-Insulin dependence (<1 unit/kg/day)
-C peptide >2ng/ml
Pancreas Transplantation
• Types:
A- Simultaneous pancreas and kidney transplant (SPK).
B- Pancreas after kidney (PAK)
C- Pancreas transplant alone (PTA)
D- Islet Transplantation

3/24/2015
8
Pancreas Transplantation
D O tiDonor Operation

3/24/2015
9

3/24/2015
10

3/24/2015
11
Pancreas Transplantation
Recipient Operation

3/24/2015
12
Pancreas Transplantation
• Types of Pancreas Functions
A- Exocrine:
-Amylase
-Lipase
-Bicarbonate…..
B- Endocrine:
-Insulin
-Glucagon
-Somatostatin….
3/24/2015
13
Pancreas Transplantation
• Types of Pancreas Functions
A- Exocrine:
-Amylase
-Lipase
-Bicarbonate….
B- Endocrine:
-Insulin Pancreas Islet Transplant
-Glucagon…..
Pancreas Transplantation
Islet Transplantation
IndicationThis therapy is only suitable in its current form for patients with
unstable glycemic control that cannot be corrected by standard conventional and intensive insulin therapies
Shapiro, N Engl J Med, 2000, 343 (4):230

3/24/2015
14
Pancreas Transplantation
Islet Transplantation
Not currently considered for islet transplantation
1- Patients with good glycemic control
2- Children are not currently considered for islet transplantation
Shapiro, N Engl J Med, 2000, 343 (4):230
Pancreas Transplantation
Islet Transplantation vs. Insulin Pump
Hgb A1c Corrected Varies
Diabetic Nephropathy Progression No effect
Shapiro, Curr opin organ transplant, 2011, 16(6): 627
Thompson, Transplantation 2011, 91(3): 373

3/24/2015
15
Pancreas Transplantation
• Types: (Based on drainage of donor duodenum)
A- Bladder-drained
B- Enteric-drained
(Based on venous drainage)(Based on venous drainage)
A- Systemic
B- Portal

3/24/2015
16
Pancreas Transplantation
Bladder-drained Pancreas
3/24/2015
17
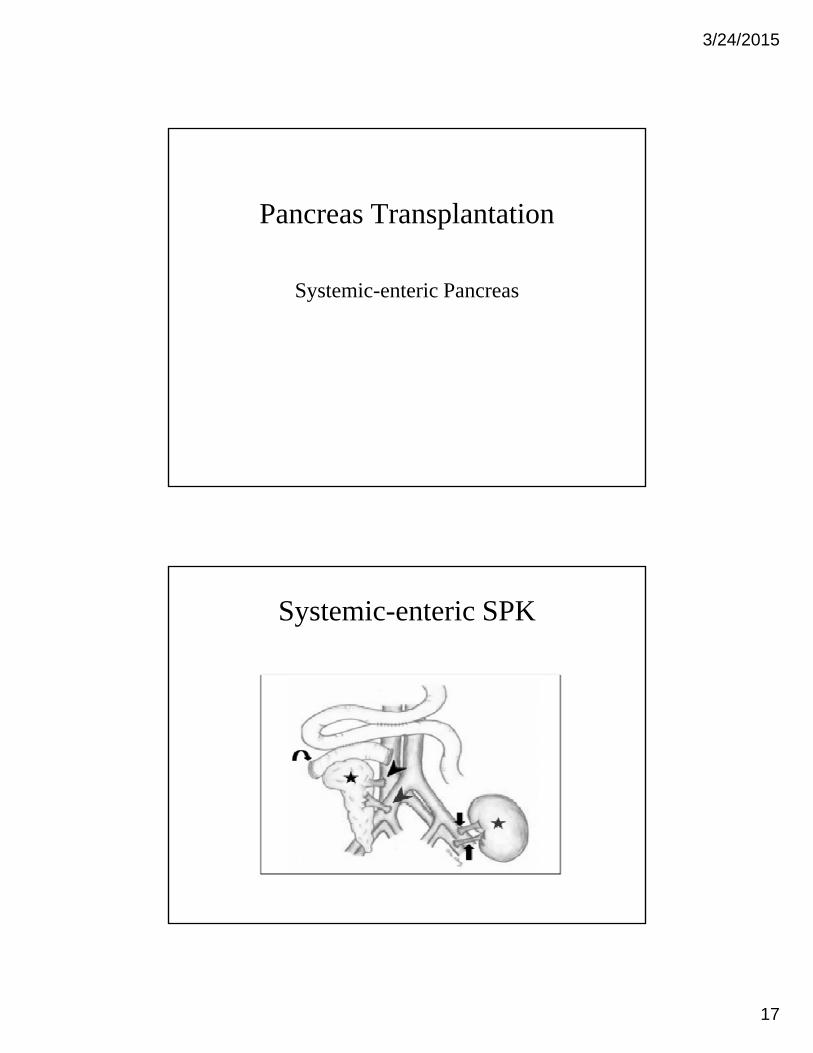
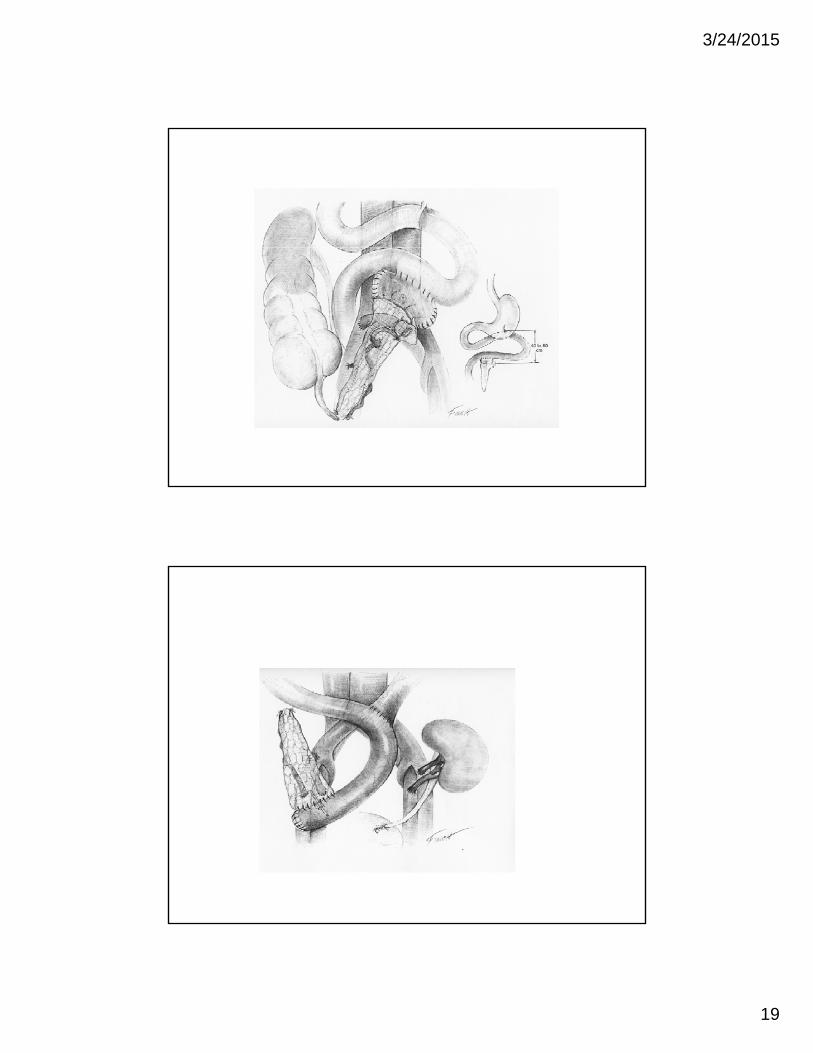
Pancreas Transplantation
Systemic-enteric Pancreas
Systemic-enteric SPK

3/24/2015
18
3/24/2015
19

3/24/2015
20
Portal vs. Systemic Drainage Pancreas Tx
Systemic vs. Portal Drainage
• Bypassing the liver causes peripheral hyperinsulinemia and portal hypoinsulinemiahyperinsulinemia and portal hypoinsulinemia
(50% of insulin is degraded during the first pass)
– Hyperinsulinemia has been associated with:• The development of atherosclerosis, both directly
(stimulation of arterial smooth muscle growth) and indirectly (development of dyslipidemia and y ( p y phypertension).
• It has also been linked to increased conc. plasminogen activator inhibitor (PAI-1), which predisposes vessels to formation of lipid-laden rather than cell-rich plaques.

3/24/2015
21
Systemic vs. Portal Drainage
Hyperinsulinemia has been associated with:I li i t lt f i d h ti• Insulin resistance as a result of increased hepatic glucose production, reduced postprandial peripheral glucose disposal, reduced insulin-stimulated glucose storage …..
• Downregulates insulin receptors and postreceptor pathways in the muscle and adipose tissues, thus causing insulin resistancecausing insulin resistance
• Hypertension, CVD, weight gain, and, in women, polycystic ovary syndrome
Systemic vs. Portal Drainage
Portal hypoinsulinemia leads to lipoprotein abnormalities that lead to development andabnormalities that lead to development and progression of atherosclerosis.

3/24/2015
22
Systemic vs. Portal Drainage
• A beneficial effect on pancreas graft tacceptance
(Hypothesis: antigen delivery via the portal vein favorably alters antigen presentation with subsequent induction of immunologic hyporeactivity and even tolerance)
More studies are needed to prove the immunologic advantage in favor of portal vein drainage
ObservationsObservations

3/24/2015
23
Pancreas Tx Volume
• Rates of pancreas transplantation have declined, despite improved pancreatic graft outcomes.
Pancreas Transplant Volume
Kandaswamy R et al; AJT 2013(13) [Suppl 1}:47-72
3/24/2015
24
Pancreas Tx Volume
• Fewer patients are placed on the waiting list
• Changes in the rate of diabetic nephropathy development
• Delayed progression of late-stage CKD
• Greater availability of better insulin-delivery tsystem
Pancreas Tx Volume (contin.)
• Better diabetes education
• Regional waiting list rules
• More stringent donor selection
• Greater scrutiny of center outcomes

3/24/2015
25
Acute RejectionAcute Rejection
Pancreas Transplantation
Acute Rejection
• The incidence of rejection within 1-year post-transplantation in a cohort of 162 patients of all pancreas transplant types, including many re-transplants undergoing for-cause biopsies, was 21%, with antibody mediated rejection (AMR) acutewith antibody-mediated rejection (AMR), acute cellular rejection (ACR), and mixed rejection
occurring in nearly equal frequency
Neiderhaus, AJT 2013

3/24/2015
26
Pancreas Transplantation
Acute Rejection
• In their study, the majority of pancreas rejection episodes were successfully reversed and graft function was maintained. However, 20% of grafts were lost within a year of diagnosis
Thi hi hli h h d f l di i d• This highlights the need for early diagnosis and efficient surveillance
Acute Rejection
• Rejection of the pancreas may be discordant with the kidney after SPK and there is a greater appreciationkidney after SPK and there is a greater appreciation of antibody-mediated rejection of the pancreas allograft
• De-novo donor-specific antibody without graft dysfunction remains an active area of study, and the treatment for this condition is uncleartreatment for this condition is unclear

3/24/2015
27
Acute Rejection
A ll f bi ll h• A pancreas allograft biopsy allows the surgeon to accurately identify and define rejection, and should be incorporated into the portfolio of pancreas transplant monitoring
Acute Rejection
O h li i l f j i• Other clinical parameters for rejection:
-hyperglycemia
-serum amylase/lipase
-C-peptide level
-hemoglobin A1C, or g ,
-(if bladder drained) urinary amylase
are insufficient because they are either too late or nonspecific

3/24/2015
28
Acute Rejection
Th ili d ff i f ill• The utility and cost–effectiveness of surveillance biopsies have not yet been studied
• Contrary to prior assumptions, concordance in pathology between kidney graft and pancreas graft biopsies after SPK transplantation is not 100% and grafts can exhibit differing types and degrees ofgrafts can exhibit differing types and degrees of rejection. Therefore, kidney biopsies alone for SPK patients are insufficient to determine the pathologic status of the pancreatic graft
Acute Rejection
Di d l b d d l ff bi• Discordant results between a duodenal cuff biopsy and pancreas parenchymal biopsy also occur

3/24/2015
29
Trends in Immunosuppression
Conclusion
• Pancreas Transplantation improves quality of life and life expectancy in uremic diabetic patientslife expectancy in uremic diabetic patients
• Improvement in surgical technique and rejection screening have made long-term outcome comparable to other organ transplants; kidney, liver, and heart
• Islet transplantation still holds promise for treatment of brittle diabetics

3/24/2015
30
Thank You


















