Congenital Heart Disease – What’s the Diagnosis? Heart Disease – What’s the Diagnosis?...
41
Congenital Heart Disease – What’s the Diagnosis? Angela M. Sharkey, M.D. FAAP Professor of Pediatrics
-
Upload
trinhthuan -
Category
Documents
-
view
213 -
download
0
Transcript of Congenital Heart Disease – What’s the Diagnosis? Heart Disease – What’s the Diagnosis?...

Congenital Heart Disease –What’s the Diagnosis?
Angela M. Sharkey, M.D. FAAPProfessor of Pediatrics

Disclosureso I have no relevant financial relationships with the
manufacturer(s) of any commercial product(s) and/or provider of commercial services discussed in this CME activity
o I do not intend to discuss an unapproved/investigative use of a commercial product/device in my presentation.

Practice ChangeUpon completion of this session, you should be able to: o Utilize clinical exam and hyperoxia testing to develop a
differential for congenital heart disease without an echocardiogram.
o Utilize tools to quickly review the potentially life-threatening forms of congenital heart disease.

Transitions Can Be Stressful:From Womb to Delivery Room
o Objectiveso Differentiate structural cardiac diseases in the neonate based
on physical exam o Describe the conditions in which prostaglandin therapy is
best usedo Identify cardiogenic shocko Summarize the utility of various diagnostic studies in the
evaluation of congenital heart disease and congestive heart failure

Baby Blue – The Historyo Full term, LGA, NSVDo Noted in nursery to be grunting and cyanotico Sat 80%o HR 150s, “normal” BPo Systolic murmur at left sternal bordero Lungs clear, slight retractionso Good pulses and perfusion
What is the differential??

Differential Diagnosiso Sepsiso Hypoglycemiao Lung Pathology
o Alveolar hypoventilationo Ventilation-perfusion mismatcho Impairment of diffusion
o Congenital Heart Disease

Diagnostic Helperso History
o Examo Signs of respiratory distress?
o Evidence of prematurity?
o Central versus peripheral cyanosis?
o Is there a murmur?
o Cardiac screen with pulse oximetry
o Hyperoxia Test
o 4 extremity BPs
o Chest x-ray

Cyanosis**o Peripheral
o Blueness of nail beds, hands and feeto related to circulation but not hypoxia
o Common finding in normal infanto Central
o Tongue, tip of noseo Difficult to detect unless Sat <85%
o Why?

Recognition of Cyanosis
o Detectable with 3-5gm/dl of reduced hemoglobino Factors that shift oxygen-hemoglobin to left delay appearance of
cyanosisPresence of Fetal HemoglobinHypothermia
o Skin pigmentation can alsoimpact ability to detect cyanosis

Diagnostic Helperso Examo Cardiac screen with pulse oximetryo Hyperoxia Test
o How is this test performed?
o Chest x-ray
o 4 extremity BPs
o Then Echo

Neonatal Pulse Ox Screening**
o Usual cut-off level of 94-96%o Repeat screening can limit false positives from transient
ductal shuntingo More reliable after 2 hours of ageo 1st day identifies other problems in addition to heart
disease, later screening is more specifico Greater sensitivity with post-ductal probe
AAP Scientific Guidelines, Pediatrics Vol. 124 No. 2 August 1, 2009

Hyperoxia Testo Room air arterial blood gaso Place patient in 100% oxyhood for 20 minutes. Again measure
arterial PAO2.o PAO2 greater than 250 = lung diseaseo PAO2 less than 150 = cardiac diseaseo Pulse oximetry is not sensitive
enough to detect change

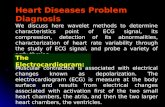
Cyanotic Lesionso The terrible T’s in frequency of appearance
o Tetralogy of Fallot **o Transposition**o Total anomalous pulmonary venous returno Tricuspid Atresiao Truncus
o Use your hand to remember them all!o Truncus, Transposition, Tri Atresia, Tetralogy, TAPVR

en.wikipedia.org

Tetralogy of Fallot
en.wikipedia.org

www.wikidoc.org

www.lookfordiagnosis.com

emedicine.medscape.com

www.stanfordchildrens.org

In the presence of cyanosis, is there a murmur?**
o TOF – pulmonary stenosis murmuro Critical pulmonary stenosis
o In these cases, augment pulmonary blood flow with prostaglandin
o Supplemental oxygen
o Truncus arteriosus with abnormal truncal valveo prostaglandin won’t help here

Cyanosis with no murmur
o Transposition**o Tricuspid Atresiao Pulmonary atresiao TAPVR

Cyanotic infant:Ductal Dependent PBF
o Desaturation is due to limited pulmonary blood flowo Tetralogy of Falloto Pulmonary atresia or critical pulnonary stenosiso Tricuspid atresia
o Due to high RV pressure, atrial level shunt from right to left occurs (i.e. blue blood mixes with red)
o May benefit from prostaglandin to maintain PDA flow from aorta to pulmonary artery**

Prognosis for Children with TOF**
36-year actuarial survival rate of 96% and normal life expectancy (J Am Coll Cardiol. 1997;30(5):1374-1383)
Repaired prior to onset of polycythemia No transannular patch
http://www.sts.org/patient-information/what-pediatric-heart-disease/

Baby Shocky – The Historyo This 11 day old female who was found to have a heart
murmur on routine newborn care on DOL #4. By report, the patient otherwise looked well. Referral to an outside cardiologist was made, and occurred on DOL 11. At this office visit, she was found to be severely ‘cyanotic’, grunting and cool to the touch.
o What’s the differential diagnosis?

Physical Examo HR 168, RR 80, Systolic BP 70, RA SaO2 90%o GEN: cyanotic infant in acute distresso HEENT: Anterior fontanelle softo CVS: RRR, + systolic murmur (not otherwise described),
no gallop,o Perfusion: poor with ~ 5 sec cap refillo ABD: soft, non tender, palpable livero EXT: cold and mottledo NEURO: awake, alert and responding to stimuli

Physical Findings of Shock**
o Tachycardia, tachypneao Respiratory distress, grunting, retractingo Pale or gray with poor perfusion, mottlingo Gallop rhythm o Hepatomegalyo Historical findings: Loss of appetite, vomiting, lethargy

SHOCK!**o Sepsiso Congenital Heart Disease – Left Heart Obstruction
o Coarctationo HLHSo Critical aortic stenosiso Interruption of the aortic arch
o Cardiomyopathyo Myocarditiso Anomalous left coronary arteryo Sustained tachyarrhythmia

DIMINISHED SYSTEMIC PERFUSION Sepsis-like picture, poor perfusion Not notably blue,
Do Pulse Ox screen Consider cardiac lesions:
Coarctation Interrupted aortic arch HLHS Critical AS
Treatment: Prostaglandin Avoid hyperventilation (CO2 rise = increase PVR)
www.stanfordchildrens.org

How to use PGE:Re-inventing the fetus!**
o It is not necessary or important to make the exact anatomic diagnosis prior to initiation of PGE therapy.
o It is necessary to make the diagnosis of highly probable CHD with either:o ductal dependent systemic (shock) or o ductal dependent pulmonary (cyanosis)
blood flow prior to initiation of PGE therapy.

Congenital Heart Disease in Patients with Abnormal Karyotype
o Turner syndrome**o Bicuspid aortic valveo Coarctationo “Care of Girls and Women with Turner Syndrome: A Guideline”, Pediatrics 2003
o Trisomy 21o 50% have cardiac disease,
o 40% of these are complete AV Canal o VSD, PDA, and Tetralogy of Fallot
o 75% of patients with AV Canal have Trisomy 21

Congestive Heart Failure
o Inadequate delivery of oxygen to tissueso Can result from
o structural abnormality (left to right shunt) or
o decreased cardiac function

o Clinical diagnosis:**o Tachycardia, Tachypnea o Pulmonary congestion
o Wheezingo Hepatomegaly & cardiomegalyo Dynamic precordium with gallop rhythmo Poor feeding and/or weight loss
Congestive Heart Failure

CHF in the Child/Adolescent
o Nausea/vomitingo Edemao Hepatomegalyo JVDo Gallop rhythmo +/- Cardiomegaly on CXR

Congestive Heart Failure**o Generally occurs AFTER first two weeks of life
o Early (weeks 1-2) Left sided obstructive lesionso Aortic Stenosis, Coarctation, Interruption of the Aortic Arch,
Hypoplastic Left Heart Syndromeo Late (weeks 2-8) Left to right shunts or pump failure
o L to R shunto Atrioventricular Canal, VSD, unobstructed TAPVR, PDA
o Pump failureo Anomalous Left Coronary Artery from the Pulmonary Artery
(ALCAPA), cardiomyopathy, myocarditis

Congestive Heart Failureo **Based on these potential diagnoses, evaluation of infants and
children presenting with congestive heart failure should include:o Chest radiographo ECGo Echocardiogramo And in addition, consideration for
o Troponino Lactateo BNP (B-type natriuretic peptide)o Viral panel o Genetic testing

Come to the case session to learn more!!!

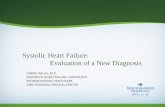
Anomalous Left Coronary Artery from the Pulmonary Artery
Normal Coronary Arteries ALCAPA

www.chop.edu

Conclusionso A “Cardiac Screen” should be performed on all
neonates with suspected CHD.o Vitals including 4 extremity blood pressureso Saturations by pulse oximetry, ideally repeated at
greater than 24 hours ageo Historical context and exam leads to further testing
o Infants appearing to have ductal dependent pulmonaryor systemic blood flow should be started on PGE1.

Practice ChangeUpon completion of this session, I encourage you to incorporate these changes into your practice: Utilize tools to quickly review the potentially life-threatening forms of congenital heart disease.
The hand rule for cyanotic congenital heart disease Cardiac screen with pulse oximetry Physical exam findings consistent with CHD

BibliographyScientific Statement from AHA and AAP: Role of pulse oximetry in examining newborns
for congenital heart disease. Circulation. 2009 Aug 4;120(5):447-58.
Care of Girls and Women with Turner Syndrome: A Guideline”, Pediatrics 2003Contemporary management of pediatric heart failure. Expert Reviews of Cardiovascular Therapy
2008 Feb;6(2):187-97.
Oxygen saturation as a screening test for critical congenital heart disease. Pediatric Cardiology 2002 Jul-Aug;23(4):403-9
2014 Appropriate Use Criteria for Initial Transthoracic Echocardiography in Outpatient Pediatric Cardiology. Pediatrics 2014;134:e1774
Cardiac Images: http://www.cdc.gov/ncbddd/heartdefects/index.html