
PDAs and Practice Extenders: Integration of 5-A Tobacco Use Intervention Myra A. Crawford, PhD T....
42
PDAs and Practice PDAs and Practice Extenders: Integration Extenders: Integration of 5-A Tobacco Use of 5-A Tobacco Use Intervention Intervention Myra A. Crawford, PhD Myra A. Crawford, PhD T. Michael Harrington, MD T. Michael Harrington, MD Toya V. Russell, PhD Toya V. Russell, PhD Brenda K. Baumann, MD Brenda K. Baumann, MD The University of Alabama at Birmingham The University of Alabama at Birmingham Alabama Practice Based Research Network Alabama Practice Based Research Network (APBRN) (APBRN)
-
Upload
lorena-simon -
Category
Documents
-
view
213 -
download
0
Transcript of PDAs and Practice Extenders: Integration of 5-A Tobacco Use Intervention Myra A. Crawford, PhD T....

PDAs and Practice PDAs and Practice Extenders: Integration Extenders: Integration of 5-A Tobacco Use of 5-A Tobacco Use
InterventionIntervention
Myra A. Crawford, PhDMyra A. Crawford, PhD
T. Michael Harrington, MD T. Michael Harrington, MD Toya V. Russell, PhD Toya V. Russell, PhD Brenda K. Baumann, MD Brenda K. Baumann, MD
The University of Alabama at BirminghamThe University of Alabama at Birmingham
Alabama Practice Based Research Network Alabama Practice Based Research Network (APBRN)(APBRN)

ProblemProblemNational clinical practice guidelines for the National clinical practice guidelines for the treatment of tobacco use and dependence treatment of tobacco use and dependence have existed for over a decade, but have have existed for over a decade, but have not been widely integrated into routine not been widely integrated into routine
practice.practice.
Public awareness of the dangers of tobacco use has Public awareness of the dangers of tobacco use has increased dramatically since the first US Surgeon increased dramatically since the first US Surgeon
General’s report was released 40 years ago, yet the General’s report was released 40 years ago, yet the national adult smoking prevalence rate remains at national adult smoking prevalence rate remains at
23%. 23%.

Physicians & Physicians & Tobacco UseTobacco Use
Over half of all medical office visits in the US are to primary Over half of all medical office visits in the US are to primary care physicians. care physicians.
Most visits for common chronic illnesses – including those Most visits for common chronic illnesses – including those attributable to smoking - take place in primary care attributable to smoking - take place in primary care practices.practices.
Primary care physicians cite tobacco use among their top Primary care physicians cite tobacco use among their top patient care concerns.patient care concerns.
Just 3 minutes of counseling can increase quit rates by 30% Just 3 minutes of counseling can increase quit rates by 30% and evidence shows that even 1 minute may be effective.and evidence shows that even 1 minute may be effective.

Patients & Tobacco Patients & Tobacco UseUse Over 70% of people who smoke want to quit.Over 70% of people who smoke want to quit. Seven out of ten smokers visit a physician each year. Seven out of ten smokers visit a physician each year. Most report that they value their physicians’ advice Most report that they value their physicians’ advice
regarding tobacco use. regarding tobacco use. Physician advice has been cited as the single most Physician advice has been cited as the single most
important motivator in encouraging cessation.important motivator in encouraging cessation. Behavioral therapies can increase and sustain Behavioral therapies can increase and sustain
cessation. When combined with pharmacotherapy, cessation. When combined with pharmacotherapy, the likelihood of success more than doubles.the likelihood of success more than doubles.
Yet, only 50% of patients Yet, only 50% of patients who use tobacco report ever who use tobacco report ever being advised to being advised to
quit by a physician.quit by a physician.**
** Integration of health behavior counseling in Integration of health behavior counseling in routine medical careroutine medical care. . Washington, DC: Center for the Advancement of Health, Washington, DC: Center for the Advancement of Health, 2001. 2001.

Why ?Why ? Primary care physicians often address multiple, Primary care physicians often address multiple,
complex or chronic problems within extremely complex or chronic problems within extremely short office visitsshort office visits
Patients rarely present with tobacco use as their Patients rarely present with tobacco use as their chief complaintchief complaint
Scheduling constraints / lack of timeScheduling constraints / lack of time
Lack of reimbursement for preventive servicesLack of reimbursement for preventive services
Doubts about effectiveness of intervening Doubts about effectiveness of intervening
Lack of training in appropriate counseling methodsLack of training in appropriate counseling methods
SolutionSolutionUsing the guidelines’ 5-A model, develop a Using the guidelines’ 5-A model, develop a
PDA-based tobacco use assessment and PDA-based tobacco use assessment and counseling tool for use in routine counseling tool for use in routine
care.care.
Field test and evaluate the tool among members of the Field test and evaluate the tool among members of the Alabama Practice Based Research network (APBRN) – Alabama Practice Based Research network (APBRN) – a voluntary consortium of primary care physicians a voluntary consortium of primary care physicians
conducting practice-based research in Alabamaconducting practice-based research in Alabama

AHRQ Smoking Study 16 MDs, 13 Practices, 11 Counties Baldwin Chambers Coosa
DeKalb Etowah Jefferson Lawrence Madison Shelby Talladega Tallapoosa
APBRN Membership (As of 4/1/04) 40 MDs, 30 Practices, 21 Counties Baldwin Calhoun Chambers
Coosa Covington Conecuh DeKalb Etowah Hale Jefferson Lawrence Lowndes Madison Marion/Winston Marshall Mobile Montgomery Shelby Talladega Tallapoosa Tuscaloosa
APBRN Study APBRN Study Sites Sites
& Membership & Membership
P4H Smoking Study 8 MDs, 5 Practices, 2 Counties Jefferson Shelby
PurposePurpose
PDAsPDAs to guide physicians through an evidence- to guide physicians through an evidence-based based 5-A5-A tobacco use intervention at the point of tobacco use intervention at the point of carecare ((AHRQAHRQ))
andand
Practice ExtendersPractice Extenders (PEs) to augment the (PEs) to augment the assistassist and and arrangearrange steps by providing: steps by providing:
To explore the feasibility of using . . . To explore the feasibility of using . . .
motivation / support motivation / support
resourcesresources feedback to physicians feedback to physicians
((PP44HH))

Research Research QuestionsQuestions Can the guideline be translated into a simple, but Can the guideline be translated into a simple, but
effective, PDA program for clinical use?effective, PDA program for clinical use? ( ( AHRQ AHRQ ))
Can PDA-based interventions be easily integrated into Can PDA-based interventions be easily integrated into routine care?routine care? ( ( AHRQ AHRQ ))
Can research data collection occur simultaneously?Can research data collection occur simultaneously? ( ( AHRQ AHRQ ))
Is a system of electronic data collection and transfer Is a system of electronic data collection and transfer from multiple remote sites possible and practical?from multiple remote sites possible and practical? ( ( AHRQ AHRQ ))
Can Practice Extenders (PEs) effectively augment the Can Practice Extenders (PEs) effectively augment the Assist and Arrange steps?Assist and Arrange steps? ( ( PP44HH ))

The 5-AsThe 5-As
AAsksk Identify and document tobacco use status for Identify and document tobacco use status for every patient at every visit.every patient at every visit.
AAdvise dvise In a clear, strong, personalized manner urge In a clear, strong, personalized manner urge every tobacco user to quit.every tobacco user to quit.
AAssessssess Is tobacco user willing to make a quit attempt?Is tobacco user willing to make a quit attempt?
AAssistssist If willing, use counseling & pharmacotherapy.If willing, use counseling & pharmacotherapy.If If ununwilling, address resistance (5-Rs)willing, address resistance (5-Rs)
AArrangerrange Schedule follow-up contact within 1 week after Schedule follow-up contact within 1 week after quit date.quit date.
Clinical Practice Guideline, p. 26

The 5-RsThe 5-Rs
Clinical Practice Guideline, p. 32-33
RRelevanceelevance Indicate how / why quitting is personally relevant. Indicate how / why quitting is personally relevant. Motivational info has greatest impact if relevant to Motivational info has greatest impact if relevant to disease status / risk, family or social situation, or disease status / risk, family or social situation, or other personal characteristics.other personal characteristics.
RRisksisks Identify Identify consequencesconsequences of tobacco use. of tobacco use. Suggest / highlight those most relevant. Suggest / highlight those most relevant.
RRewardsewards Identify Identify benefitsbenefits of stopping tobacco use. of stopping tobacco use. Suggest / highlight those most relevant. Suggest / highlight those most relevant.
RRoadblockoadblockss
Identify Identify barriersbarriers to quitting. Note treatment elements to quitting. Note treatment elements (problem solving, pharmacotherapy) to address. (problem solving, pharmacotherapy) to address.
RRepetitionepetition Repeat motivational intervention Repeat motivational intervention at each clinic visitat each clinic visit. . Encourage continued efforts to quit. Encourage continued efforts to quit.

Phase I:Phase I: Building the Alabama Practice Based Research Building the Alabama Practice Based Research NetworkNetwork
US Agency for Healthcare Research and QualityUS Agency for Healthcare Research and Quality ((AHRQAHRQ) )
# 1 R21 HS13529 # 1 R21 HS13529 9/30/02 9/30/02 –– 9/29/04 9/29/04
Phase II:Phase II: Testing PDA-based Interventions for Testing PDA-based Interventions for Smoking and Smoking and Unhealthy Diet Unhealthy Diet / / “Prescription for Health”“Prescription for Health” ( (PP44HH) )
The Robert Wood Johnson Foundation (with AHRQ)The Robert Wood Johnson Foundation (with AHRQ)
# 637046 # 637046 7/1/03 7/1/03 – – 10/31/0410/31/04
Funding Funding SupportSupport

ObjectivObjectivesesPhase I Phase I -- AHRQAHRQ
1)1) CreateCreate PDA program to guide MDs through brief PDA program to guide MDs through brief interventionintervention
2)2) IncreaseIncrease number of patients receiving “best practice” care number of patients receiving “best practice” care
3)3) TestTest feasibility of PDA program to guide intervention as a feasibility of PDA program to guide intervention as a means ofmeans of Integrating guidelines into routine care Integrating guidelines into routine care andand
Translating research into practiceTranslating research into practice
Phase II Phase II -- PP44HH
1) Evaluate1) Evaluate the revised PDA intervention protocol the revised PDA intervention protocol
2)2) Establish Establish a system of MD referral to Practice Extenders via a system of MD referral to Practice Extenders via PDA PDA
3)3) TestTest feasibility / effectiveness of PEs to augment Assist & feasibility / effectiveness of PEs to augment Assist & ArrangeArrange

Methods - Methods - PDAsPDAs MDs provided with PDAs MDs provided with PDAs ( ( Palm OS Palm OS ))
5-A intervention simplified 5-A intervention simplified
PDA program created using Pendragon softwarePDA program created using Pendragon software
Web-based server links / permissions establishedWeb-based server links / permissions established
Provider representative visited participating sites Provider representative visited participating sites • Installed softwareInstalled software• Established server connectivityEstablished server connectivity• Trained MDs in study protocolTrained MDs in study protocol
MDs delivered PDA-based interventions to patientsMDs delivered PDA-based interventions to patients

Methods - Methods - MDsMDs PDA protocol guided MDs through 5-A intervention at point PDA protocol guided MDs through 5-A intervention at point
of care of care
Patients indicating readiness to quit at Patients indicating readiness to quit at AssessAssess informed of informed of availability of PE services availability of PE services
Consent to PE contact obtained by MD and entered on PDA Consent to PE contact obtained by MD and entered on PDA
Data collected during interventions automatically Data collected during interventions automatically transferred to secure off-site server when MD transferred to secure off-site server when MD synchronized PDA at desktop PCsynchronized PDA at desktop PC
Data retrieved at APBRN Coordinating Center; Data retrieved at APBRN Coordinating Center; communicated to PEs (PDA as referral mechanism)communicated to PEs (PDA as referral mechanism)
MDs had option of referring patients by faxMDs had option of referring patients by fax

MethodsMethods - PEs - PEs PEs - research assistants - one assigned to each practicePEs - research assistants - one assigned to each practice
Received specialized training in:Received specialized training in: tobacco use, including addiction and cessationtobacco use, including addiction and cessation health intervention and counseling methods health intervention and counseling methods study protocolstudy protocol
On initial telephone contact, confirmed consent and helped patients On initial telephone contact, confirmed consent and helped patients develop quit plans develop quit plans
Mailed personalized packets containing printout of plan, self-help Mailed personalized packets containing printout of plan, self-help materials, and info on free or low-cost resources to aid quit attemptmaterials, and info on free or low-cost resources to aid quit attempt
Followed up by phone 1 week and 1 month post quit date; available Followed up by phone 1 week and 1 month post quit date; available for phone support between scheduled contacts for phone support between scheduled contacts
After one month follow up, provided progress reports to physiciansAfter one month follow up, provided progress reports to physicians
PDA ProtocolPDA ProtocolPhase IPhase I
AHRQAHRQ April 2003April 2003 (( Pendragon iForms v. 3.2 Pendragon iForms v. 3.2 ))

Phase IPhase I - Methods - Methods 5-A intervention simplified 5-A intervention simplified
PDA program created using Pendragon softwarePDA program created using Pendragon software
Web-based server links / permissions establishedWeb-based server links / permissions established
MDs provided with PDAs MDs provided with PDAs ( ( Palm OS Palm OS ))
Provider representative visited participating sites Provider representative visited participating sites • Installed softwareInstalled software• Established server connectivityEstablished server connectivity• Trained MDs in study protocolTrained MDs in study protocol
MDs delivered PDA-based interventions to patientsMDs delivered PDA-based interventions to patients

AskAskFields 3-5:
Demographics
(Age, Gender, Ethnicity)

Advise & Advise & AssessAssess
Fields 10, 11: Not Ready
(Identify Barriers)
END
CONTINUE

AssistAssist
CONTINUE

ArrangeArrange
END

Phase IPhase I ResultsResults
MDs MDs
Time:Time:
Tech Tech Issues:Issues:
#1 Barrier:#1 Barrier:#1 #1
Facilitator: Facilitator:
21 enrolled; 16 completed (76%)
9 rural, 7 urban / suburban
Orientation to protocol 15 min Intervention delivery 3.5 min
Slow internet, firewall, PDA crash, individual
PCs / computer systems
MDs forgetting to sync PDA
Provider Representative (on site training /
assistance)
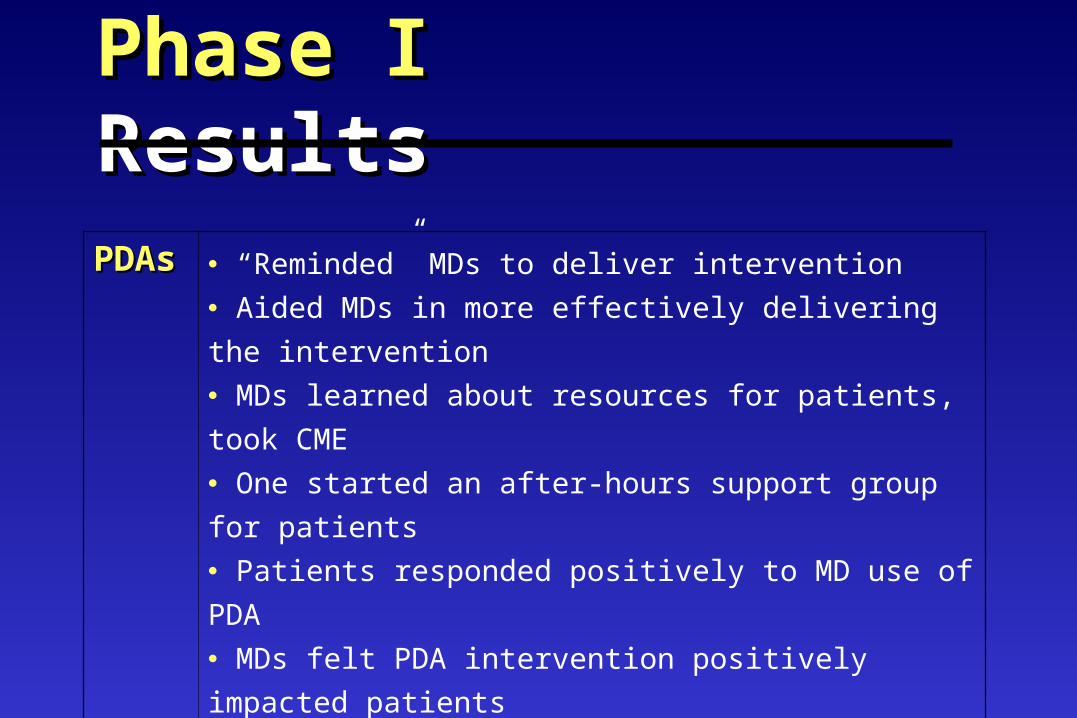
Phase IPhase I ResultsResultsPDAPDAss
“Reminded” MDs to deliver intervention
Aided MDs in more effectively delivering the
intervention
MDs learned about resources for patients, took
CME
One started an after-hours support group for
patients
Patients responded positively to MD use of PDA
MDs felt PDA intervention positively impacted
patients

Phase IPhase I ResultsResultsPatientPatientss
639 received intervention
431 (67%) willing to discuss quit attempt
180 (42%) of those willing to set quit date
(28% of all patients receiving intervention)
NeedNeed More detailed infoMore detailed info
Prompts for personalizing interventionPrompts for personalizing intervention
Means of implementing and following up Means of implementing and following up on on Assist & Arrange stepsAssist & Arrange steps
PDA ProtocolPDA ProtocolPhase IIPhase II
PP44HH** March 2004March 2004
(( Pendragon Forms v. 4.0 Pendragon Forms v. 4.0 ))
** Prescription for HealthPrescription for Health ( RWJF / ( RWJF / AHRQ )AHRQ )

Phase II Phase II = = PP44H H ** PDA Protocols revised in response to MD feedbackPDA Protocols revised in response to MD feedback
Added features allowed for greater personalization: Added features allowed for greater personalization: Info on risks and resistance to change (5 Rs) Info on risks and resistance to change (5 Rs)
Fagerstrom score calculator and pharmacotherapy info Fagerstrom score calculator and pharmacotherapy info
Info on physical, behavioral and social aspects of tobacco useInfo on physical, behavioral and social aspects of tobacco use added, as well as practical suggestions / tips for patientsadded, as well as practical suggestions / tips for patients
Practice Extender (PE) component added to augment Practice Extender (PE) component added to augment AssistAssist and and ArrangeArrange stepssteps
PDAs served triple function:PDAs served triple function:1)1) guide 5-A intervention guide 5-A intervention 2)2) data collection tool data collection tool3)3) referral mechanism referral mechanism
** Prescription for Prescription for HealthHealth (AHRQ / RWJF)(AHRQ / RWJF)
PDA protocols revised in response to MD feedbackPDA protocols revised in response to MD feedback
Added features allowed for greater personalization:Added features allowed for greater personalization: Info on risks and resistance to change (5 Rs) Info on risks and resistance to change (5 Rs)
Fagerstrom score calculator and pharmacotherapy info Fagerstrom score calculator and pharmacotherapy info
Info on physical, behavioral and social aspects of tobacco Info on physical, behavioral and social aspects of tobacco use added, as well as practical suggestions / tips for use added, as well as practical suggestions / tips for patientspatients
Practice Extender (PE) component added to Practice Extender (PE) component added to augment Assist and Arrangeaugment Assist and Arrange stepssteps
Phase II Phase II - Methods- Methods

Outcome MeasuresOutcome Measures Physician adherence to study protocolPhysician adherence to study protocol Patient consent to PE contactPatient consent to PE contact Delivery of PE assistanceDelivery of PE assistance Patients’ self-reported behavior changePatients’ self-reported behavior change End-of-study qualitative review with MDs and End-of-study qualitative review with MDs and
PEs also provided insights on PEs also provided insights on feasibility, utility, sustainability andfeasibility, utility, sustainability and
potential to affect patient outcomespotential to affect patient outcomes

AskAsk
optional

AdviseAdviseFagerstrom Fagerstrom
ScoreScoreGuides Guides
CounselingCounseling
optional
continue

AssessAssessoptiona
l
optional
continue
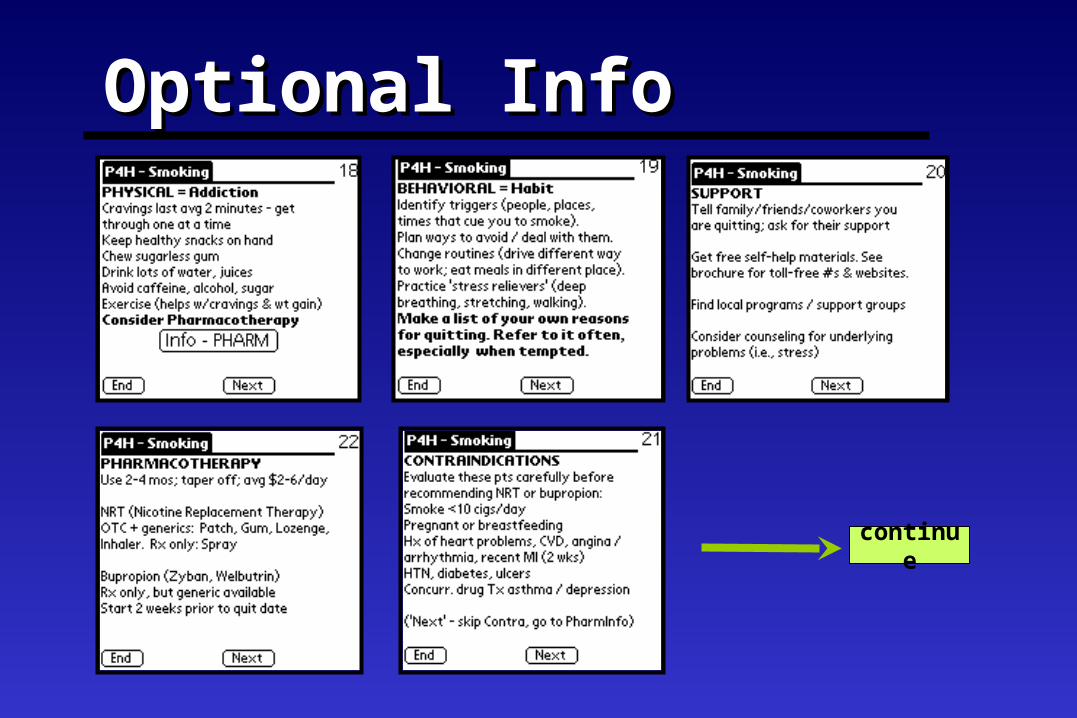
Optional InfoOptional Info
continue

Assist & Assist & ArrangeArrange
optional
Augmented by Augmented by Practice Practice
ExtendersExtenders

Phase IIPhase II ResultsResultsMDsMDs 8 MDs in 5 urban-suburban practices
Competing practice demands / incentives took
priority
Purpose of study misunderstood / forgotten over
time ( integrate intervention; PDAs for referral; role of PEs )
Forgetting to sync / charge PDA
Once 5-As memorized, PDA not used/data not
entered

Phase IIPhase II ResultsResultsPDAsPDAs Navigability of program (no back button)
No record retention
Added info accessed infrequently:
Risks: 41 times 5Rs: 14 times
Physical: 65 times Behavioral: 20 times
Social: 26 times Pharmacotherapy: 26
times

Phase IIPhase II ResultsResultsPatienPatientsts
110 received intervention
81% were willing to quit
79% of those willing to quit elected PE contact /
services Inaccurate representation of stage of change / readiness to quit (desire to please MD?)
Inaccurate contact info provided
PEsPEs Both MDs and patients felt PEs were effectiveBoth MDs and patients felt PEs were effective
Reported benefits / appreciation for PE efforts Reported benefits / appreciation for PE efforts
Having “someone who cared” especially Having “someone who cared” especially meaningfulmeaningful

Protocol Protocol FlowFlow
1 MDPDA
Patient
2MD syncs
PDA
SecureOffsiteServer
3CC
retrieves data
4PE
Patient
5PEMD
11 MD delivers PDA-based intervention. MD delivers PDA-based intervention. 22 MD syncs PDA. Data sent to server. MD syncs PDA. Data sent to server.33 Coordinating Center ( Coordinating Center (CCCC) retrieves data.) retrieves data.
P4H Referral info to PEAHRQ from MD
PP44H H 44 PE contacts patient. Sends PE contacts patient. Sends
personalized personalized materials. Follows up by phone 1 wk & materials. Follows up by phone 1 wk & 1 mo post change date + available for1 mo post change date + available for support between scheduled contacts.support between scheduled contacts. 55 PE faxes PE faxes feedbackfeedback to MD on status of to MD on status of patient’s behavior change. patient’s behavior change. Informs future MD-Patient interaction.Informs future MD-Patient interaction.
AHRQAHRQ CC solicits CC solicits feedbackfeedback from from
MDsMDs Answers research questionsAnswers research questions related to utility / feasibilityrelated to utility / feasibility Informs future researchInforms future research
informs future research
informs future interaction
PP44HH At At AssessAssess patients told of PE patients told of PE services. services. Consent & contact info entered on Consent & contact info entered on PDA.PDA.

ConclusionsConclusions PDA protocols may be cost-effective, easy PDA protocols may be cost-effective, easy
to use tools for promoting healthy to use tools for promoting healthy behaviors that can be easily integrated behaviors that can be easily integrated into routine care.into routine care.
In communities where cessation programs In communities where cessation programs are not readily available, Practice are not readily available, Practice Extenders may fill the void. Extenders may fill the void.

ConclusionsConclusionsMaking it easy for busy physicians to Making it easy for busy physicians to
integrate evidence-based interventions into integrate evidence-based interventions into clinical practice is an important first step clinical practice is an important first step
toward improving health care and outcomes toward improving health care and outcomes for patients who use tobacco. for patients who use tobacco.
Assisting them in doing so – by using PDAs or Assisting them in doing so – by using PDAs or PEs – is an important second step. PEs – is an important second step.

T. Michael Harrington, MD T. Michael Harrington, MD Director DirectorMyra A. Crawford, PhD Myra A. Crawford, PhD Co-Director Co-Director
APBRN Coordinating CenterAPBRN Coordinating CenterUAB Family & Community MedicineUAB Family & Community Medicine
Division of ResearchDivision of Research930 South 20930 South 20thth Street, Room 307 Street, Room 307
Birmingham, AL 35205Birmingham, AL 35205
Phone: Phone: (205) 934-9376 (205) 934-9376 Email: Email: [email protected]@fms.uab.edu
A consortium of primary A consortium of primary care physicians care physicians
conducting practice-conducting practice-based research in based research in
Alabama Alabama
www.apbrn.netwww.apbrn.net













![Copy of AKGÜN SON REFERANSLAR.xlsx [Read-Only] · İnŞaat-beyaz İnŞaat ortakliĞi lamİnat parke lamİnat parke 62.555 m2 toya moda toya grup lamİnat parke lamİnat parke 30.000](https://static.fdocuments.us/doc/165x107/60177654d3cc1602192743a7/copy-of-akgoen-son-read-only-naat-beyaz-naat-ortaklii-lamnat-parke.jpg)


