
Pco, PCO2 -...
8
UNILATERAL HYPOVENTILATION IN MAN DURING TEMPO- RARY OCCLUSION OF ONE PULMONARY ARTERY* BY E. W. SWENSONt T. N. FINLEY,t AND S. V. GUZMAN § (From the Cardiovascular Research Institute, University of California Medical Center, San Francisco, Calif.) (Submitted for publication November 16, 1960; accepted January 19, 1961) Occlusion of the right or left pulmonary artery forces the opposite lung to perform the total gas exchange. The alveolar ventilation of the one functioning lung must increase if it is to maintain normal arterial blood oxygen and carbon dioxide tensions (1). One would predict that total ven- tilation would increase about 80 to 90 per cent to achieve the necessary increase in alveolar ventila- tion. S6derholm, however, found only a 30 per cent increase in total ventilation when one pulmo- nary artery was occluded even though arterial blood oxygen saturation, carbon dioxide tension and pH did not change (2). Other investigators (3, 4) have noted even smaller changes in total ventilation during temporary unilateral pulmonary arterial occlusion (TUPAO). If tidal volume, fre- quency of breathing and oxygen consumption re- main the same, these findings could be explained only if some or all of the ventilation of the non- perfused lung were shifted to the functioning lung. Moore, Humphreys and Cochran (5) have shown that such a shift of ventilation did occur in most dogs when one pulmonary artery was oc- cluded by tightening a ligature brought out through the chest wall. They attributed this shift to a loss of erectile support of the vascular bed in the lung. Venrath, Rotthoff, Valentin and Bolt (6) also reported a redistribution of ventilation in dogs when one pulmonary artery was occluded by a balloon. They believed that the shift was caused by the low CO, on the nonperfused side, which is consistent with Nisell's observation (7) that bronchoconstriction occurred in excised cat lungs * This investigation was supported in part by a re- search grant (H-4029) from the National Heart Institute. f Senior Research Fellow of the San Francisco Heart Association. t Research Fellow of the National Tuberculosis As- sociation. § Research Fellow of the American Heart Association. Present address: Dept. of Physiology, Medical School, Univ. of the Philippines, Herran, Manila. when alveolar CO, was reduced. On the other hand, Folkow and Pappenheimer (8), Julian, Travis, Robin and Crump (9), and Carlens, Han- son and Nordenstr6m (10) found no significant shift of ventilation during TUPAO. We decided to reinvestigate the effect of uni- lateral cessation of pulmonary blood flow on the distribution of ventilation in dogs and man. In dogs (11) we have confirmed the findings of Nisell and of Venrath and co-workers that the low alveolar Pco, in the lung with no pulmonary ar- terial blood flow produces bronchoconstriction which results in redistribution of ventilation favor- ing the opposite lung. Our present studies indi- cate that such redistribution also occurs in man during TUPAO and is initiated by the same mechanism-i.e., the decrease in alveolar PCO2 in the nonperfused lung. METHODS AND MATERIALS The plan of the investigation involved a) studies dur- ing and after temporary unilateral pulmonary arterial occlusion in patients before bronchospirometry and b) repetition of the studies in the same patients during bronchospirometry. Table I gives the physical, clinical, and pulmonary function data for the patients; all of the patients had some pulmonary disease. Control and TUPAO studies were performed 9 times in 8 patients without bronchospirometry, and once in each of the 9 patients during bronchospirometry. Studies before bronchospirometry. With the patient supine on a fluoroscopy table, we placed a triple lumen cardiac catheter in the pulmonary artery of choice, via an antecubital vein. We then inflated a balloon near the tip of the catheter to obstruct the flow of mixed ve- nous blood to that lung (3). The first measurements were made during the period of vascular occlusion; this allowed the control studies to follow after deflation of the balloon and eliminated any intervening period of fluoroscopy and manipulation of the catheter. We col- lected expired gas in a Tissot spirometer which recorded tidal volume and frequency of breathing. After three preliminary collections, we made the final collection for a 3 minute period; we drew systemic and pulmonary arterial blood samples during the second minute. We 828
Transcript of Pco, PCO2 -...

UNILATERAL HYPOVENTILATION IN MANDURINGTEMPO-RARYOCCLUSIONOF ONEPULMONARYARTERY*
BY E. W. SWENSONtT. N. FINLEY,t AND S. V. GUZMAN§
(From the Cardiovascular Research Institute, University of California Medical Center,San Francisco, Calif.)
(Submitted for publication November 16, 1960; accepted January 19, 1961)
Occlusion of the right or left pulmonary arteryforces the opposite lung to perform the total gasexchange. The alveolar ventilation of the onefunctioning lung must increase if it is to maintainnormal arterial blood oxygen and carbon dioxidetensions (1). One would predict that total ven-tilation would increase about 80 to 90 per cent toachieve the necessary increase in alveolar ventila-tion. S6derholm, however, found only a 30 percent increase in total ventilation when one pulmo-nary artery was occluded even though arterialblood oxygen saturation, carbon dioxide tensionand pH did not change (2). Other investigators(3, 4) have noted even smaller changes in totalventilation during temporary unilateral pulmonaryarterial occlusion (TUPAO). If tidal volume, fre-quency of breathing and oxygen consumption re-main the same, these findings could be explainedonly if some or all of the ventilation of the non-perfused lung were shifted to the functioning lung.
Moore, Humphreys and Cochran (5) haveshown that such a shift of ventilation did occur inmost dogs when one pulmonary artery was oc-cluded by tightening a ligature brought out throughthe chest wall. They attributed this shift to a lossof erectile support of the vascular bed in the lung.Venrath, Rotthoff, Valentin and Bolt (6) alsoreported a redistribution of ventilation in dogswhen one pulmonary artery was occluded by aballoon. They believed that the shift was causedby the low CO, on the nonperfused side, which isconsistent with Nisell's observation (7) thatbronchoconstriction occurred in excised cat lungs
* This investigation was supported in part by a re-search grant (H-4029) from the National Heart Institute.
f Senior Research Fellow of the San Francisco HeartAssociation.
t Research Fellow of the National Tuberculosis As-sociation.
§ Research Fellow of the American Heart Association.Present address: Dept. of Physiology, Medical School,Univ. of the Philippines, Herran, Manila.
when alveolar CO, was reduced. On the otherhand, Folkow and Pappenheimer (8), Julian,Travis, Robin and Crump (9), and Carlens, Han-son and Nordenstr6m (10) found no significantshift of ventilation during TUPAO.
We decided to reinvestigate the effect of uni-lateral cessation of pulmonary blood flow on thedistribution of ventilation in dogs and man. Indogs (11) we have confirmed the findings ofNisell and of Venrath and co-workers that the lowalveolar Pco, in the lung with no pulmonary ar-terial blood flow produces bronchoconstrictionwhich results in redistribution of ventilation favor-ing the opposite lung. Our present studies indi-cate that such redistribution also occurs in manduring TUPAO and is initiated by the samemechanism-i.e., the decrease in alveolar PCO2 inthe nonperfused lung.
METHODSAND MATERIALS
The plan of the investigation involved a) studies dur-ing and after temporary unilateral pulmonary arterialocclusion in patients before bronchospirometry and b)repetition of the studies in the same patients duringbronchospirometry. Table I gives the physical, clinical,and pulmonary function data for the patients; all of thepatients had some pulmonary disease. Control andTUPAO studies were performed 9 times in 8 patientswithout bronchospirometry, and once in each of the 9patients during bronchospirometry.
Studies before bronchospirometry. With the patientsupine on a fluoroscopy table, we placed a triple lumencardiac catheter in the pulmonary artery of choice, viaan antecubital vein. We then inflated a balloon nearthe tip of the catheter to obstruct the flow of mixed ve-nous blood to that lung (3). The first measurementswere made during the period of vascular occlusion; thisallowed the control studies to follow after deflation ofthe balloon and eliminated any intervening period offluoroscopy and manipulation of the catheter. We col-lected expired gas in a Tissot spirometer which recordedtidal volume and frequency of breathing. After threepreliminary collections, we made the final collection fora 3 minute period; we drew systemic and pulmonaryarterial blood samples during the second minute. We
828

829UNILATERAL HYPOVENTILATION DURING PULMONARYARTERYOCCLUSION
TABLE I
Clinical and routine pulmonary function data of ten patients studied *
Maximal flow ratesBefore/After iso-proterenol aerosol Sao2 Pao2
Age, Sex RV,' Breath- Breath-Patient BSA Diagnosis VC MBC TLC SB 02 MEFR MIFR ing air ing 02 DCo
4 predicted N% 2 L,'iLi, inin' m Hg %pr-edict.
Bilat. nodularscars, esp RtUL
Ca in LLLold tbc RUL
Bilat. midlungtbc infilt.
Emp)hysenma;bilat. bronchiect.
Ca in RUL;inactive bilat.apical tbc
Oat cell Ca in RLL
LLL bullae
Ca in RLL:inactive bilat.apical tbcCa+abscess inSS, LLL
RUL tumor
152 33 3.5 333, 300,' 96 595 68
117 119 33 4.0 273/375 186'214 91
131 120 13 3.5 500,
64
375,' 96 650 Ill
79 35 41 11.0 75, 83 2557280 97 76
82 64 48 6.5 83,88 1 1 5,7 115 88 525 34
139 23 4.0 250.' 214,' 93
104 134 34 3.5 430,'
96 50
172
803757 ' 96
5.0 123,150 123,7136 85 659
105 81 46 5.0 57,'1 1 7 96, 1 0 89
101 54 5.0 2147200 209!200 95 510
* Abbreviations: VC =vital capacity; MBC=maximal breathing capacity; RV,'TLC =residual volume per total lung capacity; SB 02 =riseN2 concentration between 750 and 1,250 ml expired after a single breath of pure O2 (1); MEFRand MIFR =maximal expiratory and inspiratoryflow rates (I); Sao2 =% arterial oxygen saturation; Pao2 =arterial oxygen tension; Dco =breath-holtling diffusing capacity for carbon monoxideat rest; RUL=right upper lobe; SS, LLL =superior segment of left lower lobe; Ca =carcinoma.
measured the 02 and CO2 concentrations of expired gas
(using the Scholander apparatus) and of blood (usingthe Van Slyke apparatus). We determined systemic ar-
terial 02 and CO2 tensions with special electrodes (12).We calculated 02 uptake, CO. elimination, respiratoryquotient, cardiac output, physiological dead space andalveolar ventilation.
We calculated anatomic dead space during and afterTUPAO from continuous recordings of expired CO2concentration and flow (13) ; CO2 concentration was ob-tained with the Beckman Spinco apparatus and flow witha Fleisch pneumotachygraph. The lag of the CO2 meterwas measured at the time each patient was studied; itaveraged 0.1 second.
In order to determine whether venous to arterialshunts were present during the vascular occlusion, we
gave two patients (O.B. and A.G.) pure oxygen tobreathe for 20 minutes before we deflated the balloon;they continued to breathe oxygen during and after bal-loon deflation. We measured the oxygen tension ofarterial blood (12) just before deflation and 1 minuteafterwards. Finally, to determine whether shunts were
due to easily reversible atelectasis, we asked the patientsto take several deep breaths and repeated the measure-
ment of arterial blood P02.Studies during brontchospironmetry. At the completion
of the previous studies, we injected intravenously 0.75 to1.0 mg of atropine sulfate and 75 to 100 mg of pento-barbital sodium as premedication for bronchospirometry.
The patient then sat up and we anesthetized his airwaywith 1 per cent tetracaine, and passed a Carlens catheter(French 41) by indirect laryngoscopy. With the pa-
tient again supine and breathing air, we collected ex-
pired gas from each lung simultaneously in meteorologicballoons. We noted the time of collection and the re-
spiratory rate so that we could calculate mean tidalvolume. We determined the oxygen uptake, carbon di-oxide output, minute and tidal volumes of each lung.Under fluoroscopic control we then reoccluded the pul-monary artery to one lung and repeated the above studies.
Wethen measured the anatomic dead space in each lungin sequence, starting with the perfused lung. Duringeach determination, a sample of systemic arterial bloodwas drawn for measurement of CO. tension. Low tidalvolumes, especially on the side of the pulmonary arterialocclusion, made measurements of the anatomic dead space
difficult, but they were nevertheless reproducible withina limit of 5 ml.' While monitoring CO2 and air flow ofthe lung with a blocked pulmonary artery, we then de-flated the occluding balloon. Figure 1 shows an exampleof the increase in alveolar (end tidal) CO2 and floW.2
l Calculated anatomic dead space volumes were cor-
rected for 15 ml of apparatus dead space (catheter lu-men and tubing) so that they represent volumes "belowthe carina."
2 Low end tidal CO2 values were useful as a criterion ofthe unilateral blockade of perfusion. However, oxygen
A.D. 59 M1.82
F.Er. 67 M1.68
J.j. 33 M1.86
D. K. 23 M1.71
L.M. 63 M1.48
L.P. 50 M1.91
N.P. 60 M1.73
F.T. 52 M1.74
E. D. 62 M1.70
A.G. 71 M1.98

SWENSON,FINLEY AND GUZMAN
40 - 10 SEC.
mmHg
FLOW _
BEG/N coMP6ErDEFLATION OF BALLOON OCCLUDING R.P.A.
FIG. 1. INSPIRED AND EXPIRED Pco, AND FLOW TRAC-INGS IN PATIENT L.P. MONITOREDAT THE EXTERNALORI-
FICE OF THE RIGHT LUMEN OF THE BRONCHOSPIROMETRIC
CATHETER BEFORE, DURING AND AFTER DEFLATION OF THE
BALLOON BLOCKING THE RIGHT PULMONARYARTERY.
We again measured anatomic dead space on each side.The time between the dead space measurements of theright and left lung during either the control period ofunilateral pulmonary arterial occlusion was less than 5minutes.
In the last two patients (E.T. and E.P.) we tested theeffect of administering 6 per cent CO2 (in air or oxygen)
uptake data showed that the occlusion was not alwayscomplete, even when an allowance was made for anenlarged bronchial collateral flow of blood and the mildhypoxemia associated with the patient's disease and thenature of the procedure (see Discussion).'
to the unperfused lung to determine the effect of changingconcentrations of CO2 on the distribution of tidal volumebetween the two lungs.
RESULTS
Table II shows the results of nine studies ineight patients with the airway undivided. Associ-ated with the occlusion, there was no significantincrease in total ventilation. The unchangedarterial CO2 tension suggests that alveolar ventila-tion remained normal even though there was no in-crease in total ventilation. Mean values for alveo-lar ventilation (total minus physiologic dead space
ventilation) were 4.21 L per minute after, and 4.10during the occlusion, a decrease of 3 per cent (notstatistically significant). The mean oxygen up-
take and carbon dioxide output each decreased 8per cent (the differences again were not statisti-cally significant) and the respiratory quotientstayed approximately the same. The physiologicdead space increased slightly while the mean ana-
tomic dead space decreased slightly. The mean
values for both the arteriovenous oxygen differ-ence and the cardiac index decreased slightly butnot to a statistically significant degree.
TABLE II
Studies "at the mouthpiece" (undivided airway) after and during temporaryunilateral pulmonary arterial occlusion *
PA occluded Physiol. Anat.Patient side VE f VT PacO2 VD VA VD V02 VCO2 RQ AVD CI
min L/min per ml mmHg ml L/min ml ml/min ml/min ml/L L/min/min m2
A.D. 0 7.10 16 444 39 210 3.74 216 176 0.814 40 2.98R 15 6.84 11 622 41 313 3.40 205 168 0.818 43 2.63
F.Fr. 0 9.23 22 419 46 272 3.25 148 208 171 0.821 46 2.69L 15 9.92 22 451 45 301 3.30 130 227 175 0.770 42 3.21
J.J. 0 8.86 12 738 39 286 5.43 170 297 236 0.796 58 2.76R 20 10.48 14 749 40 376 5.22 140 300 236 0.787 45 3.60
D.K. 0 9.75 20 487 36 226 5.23 273 215 0.788 40 4.00R 20 11.61 21 552 34 256 6.23 282 240 0.851 42 3.930 10.35 22 470 36 247 4.92 256 207 0.808 52 2.92R 15 11.30 20 565 34 307 5.16 264 198 0.750 38 3.95
L.M. 0 9.53 22 433 39 264 3.72 90 209 167 0.799 41 3.44R 75 10.05 24 418 37 264 3.71 100 174 158 0.910 42 2.81
L.P. 0 9.20 14 657 40 338 4.47 90 276 208 0.754 38 3.66R 15 6.06 14 433 42 239 2.71 80 178 134 0.798 33 2.54
N.P. 0 7.44 13 572 40 105L 86 7.78 12 648 41 100
E.T. 0 10.89 26 419 33 252 242 205 0.848 35 3.97R 20 9.60 24 400 35 250 3.60 206 167 0.815 39 3.03
Mean control 9.15 19 516 39 262 4.21 121 265 212 0.861 44 3.31TUPAO 31 9.30 18 536 39 288 4.10 110 246 197 0.870 41 3.21
*Abbreviations: VE =total ventilation; f =respirations per minute; VT =tidal volume; PacO2 =arterial C02 tension; Physiol. VD=physio-logic dead space uncorrected for 100 ml apparatus dead space; VA=alveolar ventilation; Anat. VD=anatomic dead space; V02 =oxygen uptake;VCO2=carbon dioxide output; RQ=respiratory quotient; AVD=arteriovenous 02 content difference; CI =cardiac index.
830
UNILATERAL HYPOVENTILATION DURING PULMONARYARTERYOCCLUSION
Cl Cl) Cl) Cl
O CO -t 00
00 0_ (.CI CN i
00 --0
0 \0CLn - 00
N _.n) U)
(s .- 00 COCl)'0 0%1
_"0\m
C)) C' - CI
_ \0 \0 C\
Ul) 0
CN 00 00\0 (0%\
00 C-.r- 0
00 es0C -ml'0 a,
CO
C 000010 to) CO4 00
enL)Cl0 0t--' 0'0t
cooto)CO C(. q_O
CS4en
m V)
_)Cl0%
00
UcOt 8
Cl)t
Id 00
00 (40% -.") o Co
tn tn 0%0
U~Uto oo0(-4 "
Cl CO4 C) ~-
Cl C4 t- 0%
CO3 CO
't -
Cl)
rm mO
Cl Ct- CLO LO 00enC)'0 00
'0 CO4 -0 COC.) l) cO4
'0 CO-s00 Cqo00l't--0In)1t MC0-00 0\
00 0%C.) C.)
Cl) C) Cl
to) O"0 Clen 0% " ClCO4 -4 C -
0%t Clt
Co\ "t Cs£
CO4 Ml CO
\0 "00 CO0'0tCloe' C-r \0
0% to)000a, --(D 0% 0% 0 C-rCO. en) - CO4 m
q eq in 00 0 l t in 0 0% \'0 - '0 '0cN CSOt1 - C_ C_t.- _ CON CO
, - 0% 0% 0 00 1C - C) - Cl % CO msC 0% C0% U) C' - in) 0 0% 00
i; 06 t _; ci C4 C; 0 if;; ; (0 -._ O ~
¢¢¢¢¢¢ ¢¢ ¢¢ ¢¢ ¢¢g6
0 m
0 c o
ClS) Clfn M
'0 ool)
00
0000\C- CO 0
Cl 0%o U
Cl) '0_ UU'0000cli i
00 CS _ U) 00 CO"tren\ l-)
o 'n 0
Ul Cr) 00 '0 00O; (Ii e
a; a~ ~ ~ ;
831
Cl1) Cl) Cl) Cl)
Ce4 00 I-
m0 )'.4 m0
'0
Cl) Cl)
0_
'0
N.00 80
\ 0
'0rC'I%
C'- CLO 00 in
N q-
Cr) Cr) +
00
41
00e 00
0) u
00 C)C
t t
ON C- or4
C 5tCr, 0%.
S 0
tl)"
00CN _,t \0 to W)
ce0 >
0u
Ca0cd
0 )0
._
0 d0
ew 0
oz
(: Cd
S0d
te,.-
H
a am
0) C
r. bo
o0
O4
._
a:~
_ 0CN -
'0)- _Co
00d ~ 00
SCl Cs
'o
CO CO
COCC) os
0 0
40 N0
cr 0
Cl 06
*
0.)
0
0
0
0
*0)
0o
-0
?
0)
0)
0
0)
x: -
02).)
3 d
3 oA
0 0
0-0
>: 0
0 od
0
r.
Cd
-Cd>
0C
UC's0CZ.
C0
a1cd
00 oo
-o r.
:>W
, Q.w
0C- 0090
00
.O Y
>2o0 =
At>
C00.9 cd
0
Do0
-CZ
CO°
000
tC 0
U b;
-: CO'0. 0
U.
C0
*00t
* 0).u,-.03
50 u0
0 01
'0~o
0
0u
CZ
0¢4H-

SWENSON,FINLEY AND GUZMAN
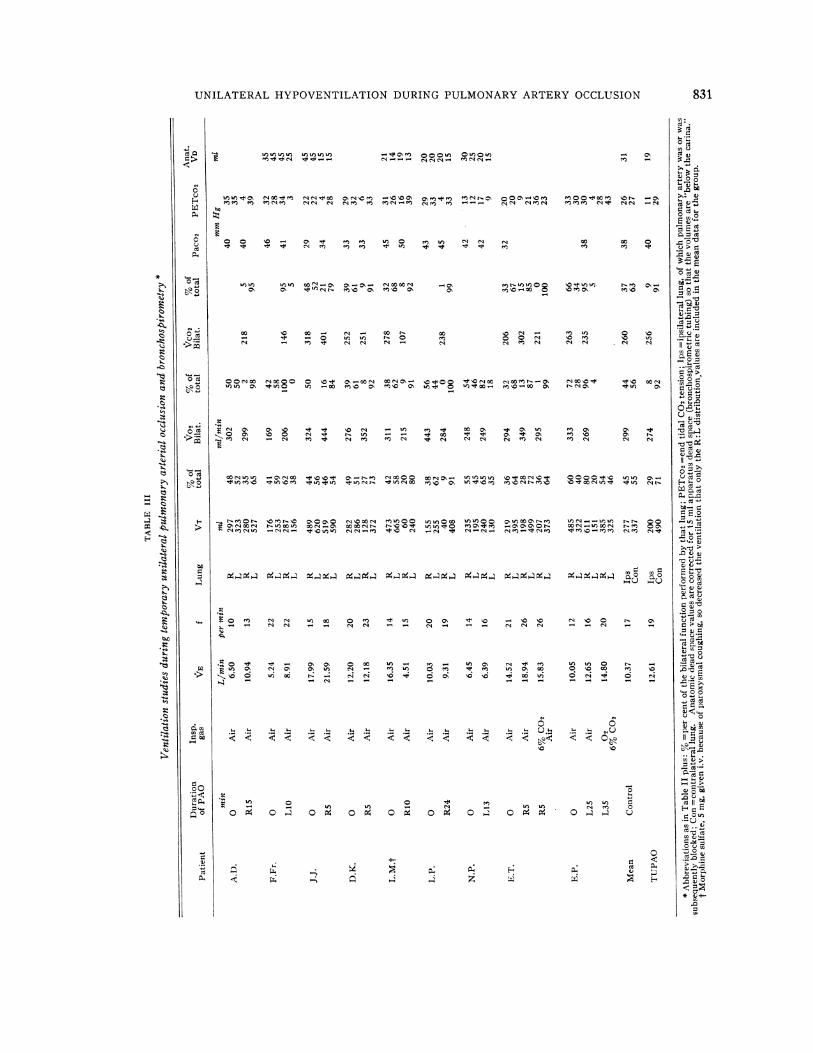
Table III shows the results of TUPAOduringbronchospirometry in nine patients. The totalventilation (mean) increased 22 per cent; how-ever, the ventilation of the lung with the occludedpulmonary artery was only 29 per cent of the totalas compared with a control value of 44 per cent.The anatomic dead space of that lung also de-creased. When 6 per cent CO2 in air or oxygenwas breathed by the unperfused lung (PatientsE.T. and E.P.), the fraction of the total ventila-tion of that lung returned to control values.
DISCUSSION
Unilateral pulmonary arterial obstruction in anormal individual must create a considerable in-crease in physiologic dead space, if ventilation ofalveoli on this side continues. Under these con-ditions, total ventilation should increase about 80per cent to maintain normal 02 and CO2 tensionsin systemic arterial blood. Nevertheless, previousinvestigators (2-4) have not found an increasein total ventilation of the magnitude predicted,and our study confirms this.
There are several possible ways of explaininghow arterial blood O., and CO2 tensions can re-main normal during TUPAOwith little or no in-crease in over-all ventilation.
1. The pulmonary circulation may have beenoccluded by disease before the balloon occlusion.This was not true in our patients; bronchospiro-metric studies showed that the 02 consumptionof the experimental lung averaged 44 per cent ofthe total for the two lungs in the control period,and in only one patient (E.P.) was it less than 30per cent of the total.
2. TUPAOmay be accompanied by a decreasein body metabolism which occurs either coinci-dentally (change in environment) or by some re-flex action. A decrease in O. consumption maybe responsible in part in Patients L.P. (Table II)and L.M. (Table III), but the mean values of°2 consumption were only 8 per cent lower thanduring the control period, which could not explainthe data observed.
3. Breathing may change to a slower and deeperpattern so that alveolar ventilation may increase,although over-all minute ventilation does not.This mechanism may afford a partial explanationin Patient A.D. (Table II), but in the other pa-
tients there was either little change in respiratoryfrequency or there was an increase.
4. Anatomic dead space may decrease. Themean value decreased from 121 to 110 ml duringTUPAO. This change is too small to explainthe data observed.
5. Redistribution of inspired air may occur sothat a large fraction of it enters perfused alveoliand little enters the nonperfused lung.
We believe that the major factor in the main-tenance of normal arterial blood 02 and CO2 ten-sions during TUPAO is a redistribution of in-spired air. The data obtained during broncho-spirometry show unequivocally that the percentageof inspired air directed to the nonperfused lungdecreases (mean decrease from 45 to 29 per cent)and that to the other lung increases (mean in-crease from 55 to 71 per cent). There is a sug-gestion that the shift is more effective when theairway is not divided, since the change in totalventilation was less than that noted during bron-chospirometry. Atropine, used as premedicationfor bronchospirometry. may act to prevent bron-choconstriction, since it is known to increase theanatomic dead space (14). However, in our ani-mal studies, atropine did not alter the ventilatoryshift associated with the unilateral occlusion ( 11 ).Topical anesthesia may also play a role. It is alsopossible that the procedure of bronchospirometryleads to an increase in sympathetic nervous sys-tem activity and that this tends to decrease theresponse. Wehave been able to block the responsecompletely by administering isoproterenol as anaerosol to the side with the arterial occlusion orby infusing epinephrine into the main pulmonaryartery in animals ( 11 ). A mechanism such as thismay have been responsible for the negative resultsin some previous studies in dogs (9) and patients(10). Patient J.J. failed to show any decrease inhis ipsilateral tidal volume during TUPAO; hismean systemic arterial pressure rose graduallyfrom a normal level to 150 mmHg during bron-chospirometry and TUPAO.
The mechanism responsible for the redistribu-tion of inspired air in man appears to be the sameas in the dog: TUPAOleads to decreased elimina-tion of CO2 ipsilaterally and to a decrease in al-veolar CO2 tension; this in turn leads to broncho-constriction. Addition of CO2 to the gas inspired
832
UNILATERAL HYPOVENTILATION DURING PULMONARYARTERYOCCLUSION
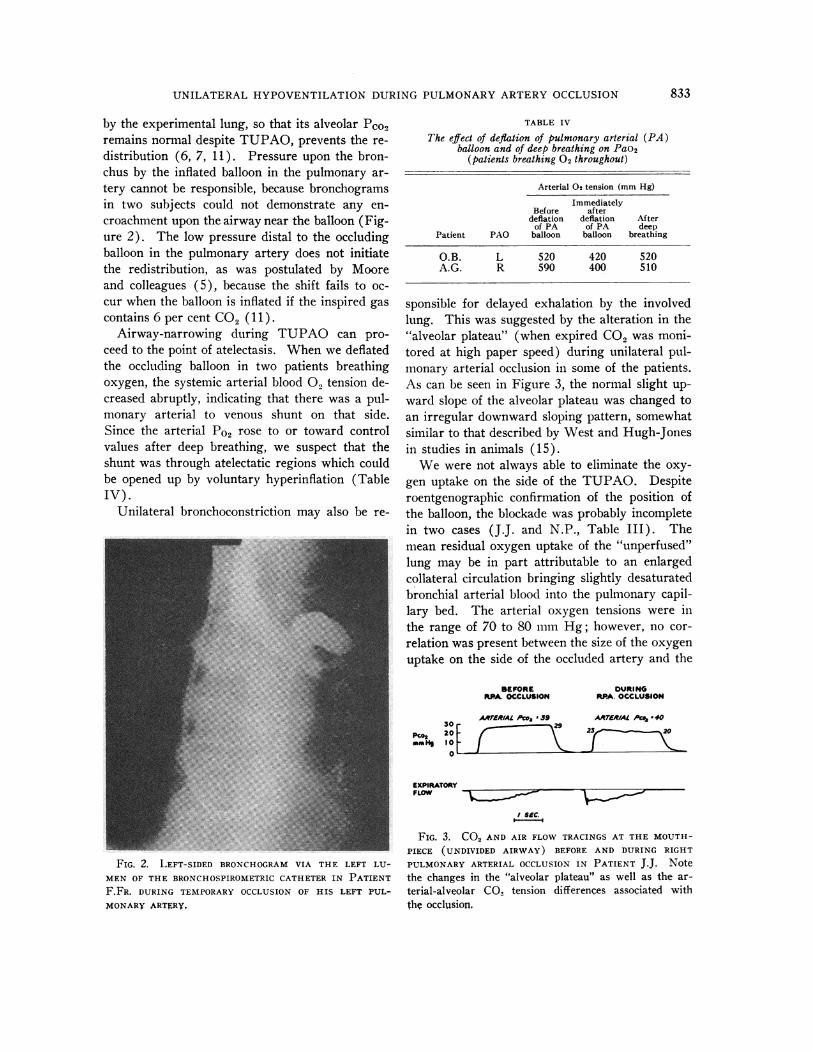
by the experimental lung, so that its alveolar Pco,remains normal despite TUPAO, prevents the re-distribution (6, 7, 11). Pressure upon the bron-chus by the inflated balloon in the pulmonary ar-tery cannot be responsible, because bronchogramsin two subjects could not demonstrate any en-croachment upon the airway near the balloon (Fig-ure 2). The low pressure distal to the occludingballoon in the pulmonary artery does not initiatethe redistribution, as was postulated by Mooreand colleagues (5), because the shift fails to oc-cur when the balloon is inflated if the inspired gascontains 6 per cent CO2 (11).
Airway-narrowing during TUPAO can pro-ceed to the point of atelectasis. Whenwe deflatedthe occluding balloon in two patients breathingoxygen, the systemic arterial blood 02 tension de-creased abruptly, indicating that there was a pul-monary arterial to venous shunt on that side.Since the arterial Po2 rose to or toward controlvalues after deep breathing, we suspect that theshunt was through atelectatic regions which couldbe opened up by voluntary hyperinflation (TableIV).
Unilateral bronchoconstriction may also be re-
TABLE IV
The effect of deflation of pulmonary arterial (PA)balloon and of deep breathing on Pao2
(patients breathing 02 throughout)
Arterial 02 tension (mm Hg)
ImmediatelyBefore after
deflation deflation Afterof PA of PA deep
Patient PAO balloon balloon breathing
O.B. L 520 420 520A.G. R 590 400 510
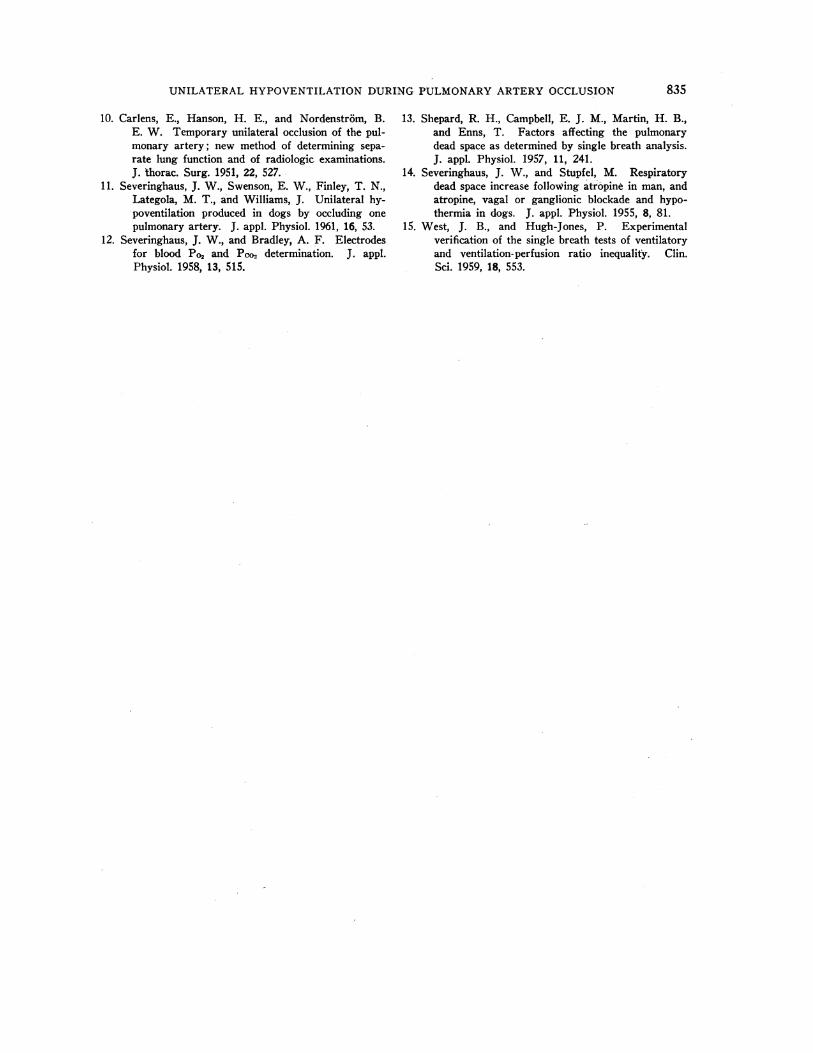
sponsible for delayed exhalation by the involvedlung. This was suggested by the alteration in the"alveolar plateau" (when expired CO2 was moni-tored at high paper speed) during unilateral pul-monary arterial occlusion in some of the patients.As can be seen in Figure 3, the normal slight up-ward slope of the alveolar plateau was changed toan irregular downward sloping pattern, somewhatsimilar to that described by West and Hugh-Jonesin studies in animals (15).
Wewere not always able to eliminate the oxy-gen uptake on the side of the TUPAO. Despiteroentgenographic confirmation of the position ofthe balloon, the blockade was probably incompletein two cases (J.J. and N.P., Table III). Themean residual oxygen uptake of the "unperfused"lung may be in part attributable to an enlargedcollateral circulation bringing slightly desaturatedbronchial arterial blood into the pulmonary capil-lary bed. The arterial oxygen tensions were inthe range of 70 to 80 mmHg; however, no cor-relation was present between the size of the oxygenuptake on the side of the occluded artery and the
BEFORERPA. OCCLUSION
AAFER/AL Aco, * 39
;~~~~2
DURINGRPA. OCCLUSION
ARTERIAL Pc.8 .4023, 20
FIG. 2. LEFT-SIDED BRONCHOGRAMVIA THE LEFT LU-MENOF THE BRONCHOSPIROMETRICCATHETERIN PATIENTF.FR. DURING TEMPORARYOCCLUSION OF HIS LEFT PUL-MONARYARTERY.
EXPIRATORYFLOW
I SEC.
FIG. 3. CO2 AND AIR FLOW TRACINGS AT THE MOUTH-PIECE (UNDIVIDED AIRWAY) BEFORE AND DURING RIGHT
PULMONARYARTERIAL OCCLUSION IN PATIENT J.J. Notethe changes in the "alveolar plateau" as well as the ar-terial-alveolar CO2 tension differences associated withthe occlusion,
30
Pco2 201-amH, 10 _
0% _
833

SWENSON,FINLEY AND GUZMAN
arterial oxygen tension or saturation before vas-cular occlusion when the airway was undivided.The CO2 output of the "unperfused" lung wasconsistently greater (mean of 9 per cent of thebilateral CO2 output) than the contribution of thatlung to the total oxygen uptake. The high re-spiratory quotient resulting is explainable on thebasis of the high CO2 gradient and ready diffusi-bility of this gas from the bronchial collateral(systemic arterial) blood to the alveoli of the lungwhose supply of mixed venous blood is blocked.
SUMMARY
1. In eight patients with chronic lung disease,studied during and after temporary unilateral pul-monary arterial occlusion (TUPAO) in order todetermine the ventilatory response to one-sidedobstruction of the flow of mixed venous blood:a) On the average, the total ventilation was un-changed. b) At the same time, the mean arterialPco2 did not rise, indicating that alveolar hypo-ventilation had not occurred. c) The physiologicdead space increased less than might have been ex-pected considering that 45 per cent of the totalventilation and oxygen uptake was originallyperformed by the lung whose pulmonary arterywas later blocked. d) In several cases the "alveo-lar plateau" of CO2became irregular during the oc-clusion and sloped downward; this was interpretedas delayed emptying of the lung whose CO2 out-put was curtailed from lack of perfusion.
2. In nine patients, studied by bronchospirom-etry and unilateral pulmonary arterial occlusion:a) After obstructing the flow of blood to one lungthe tidal volume of that lung decreased so that itscontribution to the total ventilation diminishedfrom a mean of 45 to 29 per cent during the oc-clusion. b) During unilateral pulmonary arterialocclusion the anatomic dead space in that lung(below the carina) decreased from a mean of 31ml before, to 19 ml during occlusion. c) Althoughthe total ventilation increased by a mean of 22per cent, under these circumstances the shift inthe distribution of ventilation allowed the con-tralateral lung to increase its ventilation by a meanvalue of 63 per cent (5.73 L per minute before,9.32 during occlusion); the normal arterial PCO2figures (mean of 38 before, 40 mmHg during)attest to the magnitude of this shift. d) Allowing
the "unperfused" lung to breathe 6 per cent CO2in two cases resulted in a return to the preocclu-sion values for distribution of inspired gas to theright and left lungs.
3. Wesuggest that the immediate reduction ofventilation in one lung following the occlusion ofits pulmonary artery is due to bronchoconstrictionwhich occurs in response to local airway hypo-capnia and leads to regional atelectasis.
ACKNOWLEDGMENTS
The authors wish to express their thanks to Drs.Julius H. Comroe, Jr. and John W. Severinghaus fortheir encouragement, advice and assistance in the prepara-tion of the manuscript. Mrs. Louise Brandorff and Mrs.Tillie Leake contributed with their technical assistanceduring cardiac catheterization and bronchospirometry.
REFERENCES
1. Comroe, J. H., Jr., Forster, R. E., Dubois, A. B.,Briscoe, W. A., and Carlsen, E. The Lung.Clinical Physiology and Pulmonary Function Tests.Chicago, Year Book Publ., 1955, p. 182.
2. S6derholm, B. The hemodynamics of the lesser cir-culation in pulmonary tuberculosis. Effect of exer-cise, temporary unilateral pulmonary artery oc-clusion, and operation. Scand. J. Clin. lab. Invest.1957, 9, suppl. 26.
3. Brofman, B. L., Charms, B. L., Kohn, P. M., Elder,J., Newman, R., and Rizika, M. Unilateral pul-monary artery occluslon in man. Control studies.J. thorac. Surg. 1957, 34, 206.
4. Denolin, H., De Coster, A., and Dumont, A. Reper-cussions circulatoires et respiratoires de l'occlusiond'une artere pulmonaire chez l'homme. J. Physiol.(Lond.) 1960, 52, 71.
5. Moore, R. L., Humphreys, G. H., and Cochran,H. W. The effect of sudden occlusion of eitherprimary branch of the pulmonary artery on cardiacoutput and pulmonary expansion. J. thorac. Surg.1934, 3, 573.
6. Venrath, H., Rotthoff, R., Valentin, H., and Bolt,W. Bronchospirographische Untersuchungen beiDurchblutungsstdrungen im kleinen Kreislauf.Beitr. Klin. Tuberk. 1952, 107, 291.
7. Nisell, 0. I. Some aspects of the pulmonary circu-lation and ventilation. Int. Arch. Allergy 1952,3, 142.
8. Folkow, B., and Pappenheimer, J. R. Components ofthe respiratory dead space and their variation withpressure breathing and with bronchoactive drugs.J. appl. Physiol. 1955, 8, 102.
9. Julian, D. G., Travis, D. M., Robin, E. D., andCrump, C. H. Effect of pulmonary artery oc-clusion upon end-tidal CO, tension. J. appl. Phys-iol. 1960, 15, 87.
834
UNILATERAL HYPOVENTILATION DURINGPULMONARYARTERYOCCLUSION
10. Carlens, E., Hanson, H. E., and Nordenstr6m, B.E. W. Temporary unilateral occlusion of the pul-monary artery; new method of determining sepa-
rate lung function and of radiologic examinations.J. thorac. Surg. 1951, 22, 527.-
11. Severinghaus, J. W., Swenson, E. W., Finley, T. N.,Lategola, M. T., and Williams, J. Unilateral hy-poventilation produced in dogs by occluding one
pulmonary artery. J. appl. Physiol. 1961, 16, 53.12. Severinghaus, J. W., and Bradley, A. F. Electrodes
for blood Po% and Pco2 determination. J. appl.Physiol. 1958, 13, 515.
13. Shepard, R. H., Campbell, E. J. M., Martin, H. B.,and Enns, T. Factors affecting the pulmonarydead space as determined by single breath analysis.J. appl. Physiol. 1957, 11, 241.
14. Severinghaus, J. W., and Stupfel, M. Respiratorydead space increase following atropine in man, andatropine, vagal or ganglionic blockade and hypo-thermia in dogs. J. appl. Physiol. 1955, 8, 81.
15. West, J. B., and Hugh-Jones, P. Experimentalverification of the single breath tests of ventilatoryand ventilation-perfusion ratio inequality. Clin.Sci. 1959, 18, 553.
835


















