PCMG Bulletin 2-12 for PCT10250236).pdf · 10/10/2013 · service providers to engage with contract...
16
The Bulletin Issue Number 17: Autumn 2012 Welcome to the PCMG newsletter no 17. If you were with us at PCMG Annual Conference in Portugal in June, here’s a chance to refresh your memories. If you weren’t there, read on to find out what you missed! The meeting was a great success as always, with many interesting presentations and great networking opportunities. Personally, I cannot even express my feelings of joy at getting “back to business” and seeing so many of the familiar faces I have not seen for some time. This Bulletin includes Andy Parrett’s critical dissection of strategic partnerships in our space, which has prompted a valuable debate in PCMG circles. Meanwhile a piece from Carl Emerson discusses the relationship between purchasing and outsourcing. Two words that can have the same meaning - or can they? We also have important information concerning Committee vacancies. Please read. There will be some big changes in the Committee next year, with Andy Parrett, David Davies, Rhona Saunders, Dave Webber and Tim Steven all deciding not to stand for re-election. I’m sure you will all join me in thanking them for their great contribution to PCMG! In other news, whilst the world still seems to be in financial crisis and the fate of the Euro continues to be hotly debated, we have responded to the limitations on member travel by organising our first webinar event. Held on the 12 th of September, the webinar featured findings of the recent PCMG supported PwC study in R&D outsourcing in hi-tech industries. Members responded with great interest, with 33 attendees. An impromptu survey of their thoughts on the event showed that 100% of respondents would attend future PCMG webinars. PCMG continues to support Informa’s Partnerships event held each November and perhaps you will be reading this copy inserted in your delegate bag! If so, I hope you have a very enjoyable and useful conference! Amy Anne Maria Ylisaari PCMG Committee Member [email protected].
Transcript of PCMG Bulletin 2-12 for PCT10250236).pdf · 10/10/2013 · service providers to engage with contract...

The Bulletin
Issue Number 17: Autumn 2012
Welcome to the PCMG newsletter no 17.
If you were with us at PCMG Annual Conference in Portugal in June, here’s a chance to refresh
your memories. If you weren’t there, read on to find out what you missed! The meeting was a great
success as always, with many interesting presentations and great networking opportunities.
Personally, I cannot even express my feelings of joy at getting “back to business” and seeing so
many of the familiar faces I have not seen for some time.
This Bulletin includes Andy Parrett’s critical dissection of strategic partnerships in our space, which
has prompted a valuable debate in PCMG circles. Meanwhile a piece from Carl Emerson discusses
the relationship between purchasing and outsourcing. Two words that can have the same meaning -
or can they?
We also have important information concerning Committee vacancies. Please read. There will be
some big changes in the Committee next year, with Andy Parrett, David Davies, Rhona Saunders,
Dave Webber and Tim Steven all deciding not to stand for re-election. I’m sure you will all join me
in thanking them for their great contribution to PCMG!
In other news, whilst the world still seems to be in financial crisis and the fate of the Euro continues
to be hotly debated, we have responded to the limitations on member travel by organising our first
webinar event. Held on the 12th of September, the webinar featured findings of the recent PCMG
supported PwC study in R&D outsourcing in hi-tech industries. Members responded with great
interest, with 33 attendees. An impromptu survey of their thoughts on the event showed that 100%
of respondents would attend future PCMG webinars.
PCMG continues to support Informa’s Partnerships event held each November and perhaps you will
be reading this copy inserted in your delegate bag! If so, I hope you have a very enjoyable and
useful conference!
Amy
Anne Maria Ylisaari
PCMG Committee Member

2
CONTENTS
PCMG Annual Conference Review ................................................................................................ 3
As Soon as One Conference Finishes.............................................................................................. 6
PCMG Committee Elections: Call for Nominations. ................................................................... 7
Musings on the Remits of Outsourcing Managers and Procurement ......................................... 8
Strategic Partnerships: The Emperor's New Clothes ................................................................... 9
December Workshop: An Inside Look at the Financial Side of Clinical Trials....................... 14
January Workshop: Working with Clinical Trial Technical Providers ....................... ........... 15
Event Schedule................................................................................................... ............................ 16
PCMG Membership
The Pharmaceutical Contract Management Group is a professionally-constituted body dedicated to
optimising the outsourcing performance of its members and their companies. It is open to anyone
employed by a pharmaceutical company who has a significant interest and involvement in
outsourcing.
PCMG Sponsorship
Our workshops and annual conference provide excellent opportunities for
service providers to engage with contract managers in the pharmaceutical
industry. Our popular workshop sponsorship includes a presentation slot for
your representative to discuss key industry issues with participants, whilst
conference packages provide a range of further opportunities.
Recruitment Advertising Opportunities
You can advertise job opportunities in Outsourcing, Contract Management or associated positions
directly to the PCMG membership via the PCMG website.
PCMG OFFICE CONTACT DETAILS
For all queries contact Sam Dignan: Tel: +44 (0) 1625 664 546.
Bulletin contributions are always welcome.
www.pcmg.org.uk

3
PCMG 8th Annual Conference 2012
Returning to the Algarve in Portugal this year, the 8th
PCMG Annual Conference tackled the
topic of “Innovation in a Changing Market”. Set in the impressive grounds of the Sheraton Pine
Cliffs Hotel, the location and agenda stimulated interesting discussions and worthwhile debate.
Committee member Lan Bandara reports.
Day One
Introduction
Opening the conference, PCMG Vice Chair
Rhona Saunders of Biogen Idec introduced
the agenda for the day. Rhona also covered
some key PCMG activities including an
update on the new PCMG website.
Strategic partnerships: As good
as they claim?
PCMG Chairman, Andy Parrett, started the
morning session with a thought-provoking
and controversial presentation. Andy critically
evaluated the proposed benefits of strategic
partnerships, stating that there was no
evidence supporting many of the claims made
regarding partnerships in the industry. He also
suggested that strategic partnerships may lead
to a lack of choice and so result in a
monopoly for the larger CROs.
The changing scene
Paul Richter of Jina Ventures followed Andy
with some interesting financial observations.
He noted that CRO growth is now outpacing
Pharma, due to Pharma downsizing and to
increased levels of outsourcing. CROs are
seen as very profitable businesses, and many
have been privatised in recent years through
venture capital investment.
Mike Sitton, Clear Cut Services, then
provided an entertaining personal perspective
of the changes in clinical research over the
last 25 years.
Rhona Saunders opening the conference
Following Mike, Professor Trott from the
University of Portsmouth reviewed some of
his research into outsourcing in this area.
Completing the morning session, Peter
Carberry of Astellas summarised some of the
key changes in the industry over the last 30
years. Both Pharma and CROs have evolved
their businesses to meet the challenges of the
economic environment. The next level of
innovation may be more use of co-
development/co-investment models.
Comparisons with other
industries
After lunch, Professor John Seddon of
Vanguard Consulting took everyone through
his observations of outsourcing and partnering
in different industries. He identified a
common pattern where segmenting
organisations into different compartments in
the wrong way has had a clear negative effect
on productivity and efficiency.

4
Fireside chat
The next session was a new take on an old
idea - the ‘Fireside Chat’ concept.
Conversation was fuelled by three
protagonists: Joe von Rickenbach, CEO of
Parexel and CRO pioneer, who gave the CRO
perspective; Mike Sitton, presenting the
sponsor viewpoint, and Prof John Seddon,
bringing a (potentially incendiary) external
perspective. The moderator was Richard
Scaife, Mitsubishi.
Debating whether CROs and strategic
alliances have really brought tangible benefits
to clinical trial management, each participant
had contrasting experiences. The conversation
suggested that CROs may be the main
beneficiaries of such relationships, but that
the reason for this lay partly at the door of
pharma: sponsors’ short-term outlooks can
prevent alliances from maturing and realizing
mutual benefits.
Heating up, the discussion moved on to
consider the evolution of ‘Mega-CROs’ and
the resulting polarization of the market. All
three protagonists shared concerns over the
potential diversion of business focus and
continuity during mergers and acquisitions.
Overall, the chat provided interesting insights
into the fact that innovation in our business
may not always be beneficial to all concerned.
“This house believes CROs are
the source of all innovation”
The first day ended with the popular Oxford
debate. This year, the motion tabled was
“This house believes CROs are the source of
all innovation.”
Supporting the motion were Jon Wood of
Syne Qua Non and Karen Redding of
Fireside chat with Richard Scaife, Josef Von
Rickenbach, John Seddon, and Mike Sitton.
Phlexglobal. In opposition were Craig
Coffman of Endo and Matthew Bardsley of
AstraZeneca.
Convincing lucid arguments were put forward
by both parties in this entertaining debate, and
it was left to the moderator, Steve Martindill
(Gilead Sciences), to choose the winner. In
the end, for the first time since the debates
began, he declared a draw!
The carnival comes to town
The gala dinner was another spectacular event
set outside in the grounds of the hotel. With
the sun setting in the background and a
refreshing breeze, everyone had the chance to
reflect on the first day’s presentations and
discuss thoughts and ideas arising from what
they had heard.
After an excellent meal, we were delighted to
hear how Stuart McGuire of Chiltern is on the
road to recovery.
A fantastic evening’s entertainment followed,
sponsored by Chiltern. Dazzling juggling and
fire eating acts were followed by carnival
dancing right off the streets of Rio.
We finished the night relaxed and refreshed,
ready to get back down to business on day
two.

5
Day Two
Innovation, complexity, and the
need to foster the right
environment
Faiz Kermani, SFL Regulatory Affairs &
Scientific Communication, kicked off the
second day with a summary of innovation in
the regulatory arena and highlighted a
surprising number of new initiatives in this
area. This was followed by John Bennett
(JABPharma) who discussed the complexity
of clinical trials.
Switching tracks, Roger Joby (1to1to1), a
long standing contributor to PCMG events,
highlighted the lack of innovation in clinical
contracts. He also noted, however, that there
was not much motivation in the industry to
make changes to this paradigm.
Matt Bolton completed the morning session
with a lively and refreshing review of
innovative companies. He pointed out that
innovation doesn’t always happen by chance.
Many companies make an investment in
fostering the right environment, and allocate
time specifically for work on innovation.
Operational innovation
The last session focused on operational
efforts. Dr Fraser Inglis from the Glasgow
Memory Clinic provided an investigator site
perspective, and Nicky Yarwood of Roche
Products took a closer look at monitoring.
The final presentation of the day was from
Steve Kent of Perceptive Informatics, who
reviewed many of the tools available in
clinical research.
Lively discussions on the terrace
Overall, the meeting provided a fantastic
overview of innovation in our industry. It’s
clear much progress has been achieved over
the last two decades – but perhaps things have
not progressed as quickly as in other
industries.
Over the next 20 years, we can certainly
expect to see more changes that impact the
way we work. There is still room for
improvement.
Lan Bandara
PCMG Committee
WANTED: Feedback,
News, Articles
We welcome your comments and views. We
promote and support an open exchange of
ideas and we welcome input from both our
Pharma members and from non-members
including service providers. If you have any
comments or suggestions concerning the
PCMG, the bulletin or any articles in it, or if
you would like to contribute to future
Bulletins, please get in touch with Sam
Dignan.

6
As Soon as One Conference Finishes...
It’s time to plan the next. Here, Richard Scaife, 2013 Conference Chairperson, reflects on how
we can make the annual conference as accessible and relevant as possible in today’s tough
climate, and introduces next year’s plans.
The hot question as soon as each Annual Conference closes is always "...where next year?" We
have listened to the broad range of feedback from members and sponsors and, while it's impossible
to meet everyone's preferences, we can have followed the key principles of making the conference
different, stimulating and feasible. The resort venue concept has worked well, but there was concern
that in the current business climate it was making it difficult for members submitting travel
requests. We also needed to improve accessibility for participants across Europe, and to consider
delegate room costs. After narrowing down a long list of potential venues, the PCMG committee
has now made the final selection..........Budapest!
The actual venue is now being finalised to make the meeting as special as ever, but still cost-
effective. However, we can confirm dates of Wednesday evening, 5th June 2013 finishing on
Friday 7th June, so block this space in your schedules now!
As for content, these are challenging times for sponsors and providers. Subsequently, the theme for
the 2013 conference is to go 'Back To Basics’, refining existing tools, developing new ones and
pooling our knowledge to develop baseline standards of practice. The Conference Steering
Committee and PCMG members are finalising an agenda that will challenge conventions, stimulate
interaction, and provide content of tangible value that delegates can take away and apply
immediately in the working environment.
As well as PCMG members’ attendance being crucial to the ongoing success of this meeting, please
start thinking now of how you can involve other project team members. Clinical PMs have a
vested interest in many of the agenda items such as study feasibility, pricing transparency, who is
best placed to be lead PM - sponsor or CRO?, communication best practice and more. While
budgets remain tight, there's no better time to remind your colleagues of the relatively low cost of
attending PCMG - a conference that is designed for content, not commercial gain.
That's my sermon for today. My thanks to everyone who has helped us in the intensive preparations
to date. Feedback, as always, is welcome!
2013 here we come....
Richard Scaife
PCMG 2013 Conference Chairperson

7
PCMG Elections
One of the great strengths of PCMG is that the organisation is run by members for the benefit of
members. The committee, the officers and the directors are active PCMG members who give time
when their day jobs permit to serve as a ‘management team’ and organise activities such as the
workshops, webinars, training events and the annual conference.
PCMG could not function without the support of these individuals. On behalf of the membership, I
would like to extend heartfelt thanks for the work they do week in and week out to further the goals
of PCMG.
The structure of the current PCMG management team is as follows:
Board Directors (3-4) Officers (4) Committee (Number not set)
Andy Parrett Chairman: Andy Parrett Alison Moor
Antje Hindahl Vice Chair: Rhona Saunders Anne Maria Ylisaari
Cliff Leat Treasurer: Cliff Leat David Webber
David Davies Secretary: David Davies Lan Bandara
Lesley Matthews
Richard Scaife
Stephanie Kamp
Steve Martindill
Tim Steven
The directors, officers and committee are appointed for a two-year period. After two years, the
individuals must either step down or offer themselves up for re-election. Andy Parrett, Dave
Webber, Rhona Saunders, Tim Steven and I have indicated that we will not stand for re-election for
the 2013-14 period. There will therefore be vacancies for one or two directors and three officers.
Meanwhile we expect a need to fill several vacancies on the wider committee.
Would you like to put your name forward to help drive PCMG forward in 2013-14, either as a
director, officer or a committee member?
Nominations are sought from the membership, to be received in writing on or before 14th December
2012. Please contact me or any of the current team if you would like to discuss any of the roles,
informally, in confidence.
Should we receive more candidates than vacancies for any given role, then an election will be held.
Elections must be concluded and ratified by the time of the AGM. This will be held on 23 January
2013, during the first workshop of the year.
This is your chance to make a real difference to PCMG in the future!
David Davies
PCMG Secretary
Tel: +44 (0) 7764682332

8
Musings on the Remits of Outsourcing/Contract Managers and Procurement Specialists
The topic of the balance between the roles and remits of outsourcing/contract managers and
those working in the procurement function is a perennial favourite. Carl Emerson has
experience in both clinical development and procurement. In this article, he shares observations
gained during more than twenty years of working in the field – and asks a few questions, too.
The early days
As pharmaceutical companies started out on their first outsourcing projects, they soon discovered
the adventure of outsourcing raises problems for the untrained and inexperienced. It quickly became
apparent that if the same difficulties were not to be repeated over and over again, it was going to be
essential to capture learning and build up a pattern of best practice. Further to this, it also became
clear that the skills required were too extensive to be simply bolted onto the job of a clinical
manager. This led to the emergence of a dedicated outsourcing management function, populated by
experts within clinical who were able to build up a toolbox of templates, establish workable
procedures, and guide the uninitiated and untaught through the muddy waters of first time RFPs and
contracts.
Procurement gets worried
As spend grew, and outsourcing became increasingly standard practice, the amount of money
changing hands inevitably caught the attention of senior management, and the procurement function
started to express concerns that best practice might not be being followed. This led, in many
companies, to an uneasy dialogue as both groups tried to communicate the importance of their
respective experience in this area of huge cost and critical delivery.
What’s the point of a clinical outsourcing manager?
So, the big question. Why is a clinical outsourcing manager necessary, when, for the rest of the
world’s industries, procurement can do it all? I’m now in a company where all outsourcing is done
through procurement. We do a fantastic job with source plans, category strategies, Porters' analysis,
market segmentation, savings targets and contract execution, all good procurement stuff. But the
customer groups want to see more of our managers, more operational support, more hands-on
running of meetings and training sessions.
These are all essential added-value activities, but not ones that contribute to our procurement
department objectives. This isn’t necessarily a problem, but it certainly raises a number of issues.
Is Pharma so different from other industries?
So, what makes these added-value extras so necessary in this industry? Anyone can say their
particular industry is different. Surely, it is just a question of project management?
The answer is that Pharma really is different. Yes, of course large Pharma companies need to apply
best procurement practice. As in every other industry, companies need watertight contracts,
transparency over spending, validated savings. But the projects outsourced are extremely complex,
requiring a high level of scientific understanding. Trial conditions can be very variable,
circumstances can change, and results can be unexpected.

9
Agreements have to take account of all these factors – and that’s why you can’t employ pure
procurement practices without clinical understanding.
To test the theory...
If you want to test the theory, just try calling an investigator a 'supplier' and treating him as such -
and see how far you get!
Carl Emerson
Strategic Partnerships: The Emperor's New Clothes
In this article, first published on 7th
August in Pharmaceutical Executive (www.pharmexec.com),
PCMG Chairman, Andy Parrett, argues that current strategic partnership models are neither
strategic nor partnerships. And they don’t add value to clinical trial outsourcing.
In Hans Christian Andersen’s ‘The Emperor’s New Clothes’, two tailors promise their leader a suit
that is invisible to anyone unfit for office. And everybody goes along with it: the Emperor not
wanting to seem incompetent; the people not daring to challenge him. In clinical trial outsourcing,
we are witnessing a similar phenomenon - except our Emperor is the pharmaceutical executive, our
tailors are the large CROs, and our invisible suit is strategic partnering. In the story, it takes the
foolhardy effrontery of a young boy to expose the truth. I’d like to cast myself in that role for this
article.
The popular view
Strategic partnership deals are the fashion in our space, with numerous public announcements in
recent years.1 And there have been a number of reviews and commentaries on the trend, most of
which conclude that strategic partnerships are beneficial to the sponsor companies implementing
them.1,2,5 A good summary of the popular view has been provided by industry observer Kenneth
Getz, who says:
“Partnerships hold promise in establishing long lasting relationships that benefit from strategic
insight into & engagement in future portfolio needs. Under these relationships, sponsors partner
with fewer CROs . They gain the assurance of dedicated global capacity and expertise under shared
governance, coordinated communication and issue resolution and integrated operating processes
and systems.”2
My italics there highlight the elements Getz associates with strategic partnerships and these recur
throughout the literature, along with others such as economies of scale, risk sharing and trust. But
what value is associated with each of these features? Are the benefits real? Where is the evidence?
The facts
The British mathematician and philosopher Bertrand Russell once said: “Never let yourself be
diverted either by what you wish to believe or by what you think would have beneficent social
effects if it were believed. But look only, and solely, at what are the facts.”3

10
This is a useful approach to take when examining strategic partnerships because, although the
vision of collaborative sponsor-CRO alliances — that is, we’re all in it together — might sound
appealingly noble, facts demonstrating real added value are hard to find and reasons to doubt are
many. Below, I list some common-sense objections to each strategic partnership feature – points
you will rarely hear these mentioned in the debate as, conveniently, facts are ignored in favour of
righteous platitudes.
Strategic Partnership
Feature Disadvantage
Long Lasting
Relationships
Reduced flexibility/agility. Reduced competition (which impacts on
cost, quality and innovation).
Fewer Providers See above.
Dedicated Global
Capacity
Dedicated resources negate the benefit of Just In Time resourcing.
And why pay the premium for global capacity every time if it might
be cheaper to match vendor capability to project requirements?
Shared Governance
Governance is expensive. Popular models are based on issue
escalation rather than Risk & Quality Management, and obscure
who the customer is so harming delivery.
Integration
Integration introduces prohibitive exit costs for the relationship,
therefore incurring the same disadvantage as Long Lasting
Relationships and Fewer Providers.
Economies of Scale What economies of scale? The big CROs who sell this benefit tend
to be the most expensive. Economies of flow are more important.4
Risk Sharing
Risk sharing in service contracting does not exist because if you try
to transfer risk, you pay a premium even if you never encounter the
risk.
Trust
Trust is a false concept where applied between organisations, but
one that appeals due to the mind’s tendency to personify groups. It
is used as an excuse for zero transparency, which should be the
real basis for prolonged engagement of a provider.
Just examine the literature. The main benefit said to arise from strategic partnerships is the promise
of savings. However, the only company that appears to have put their name to a figure on this is Eli
Lilly (20% on data management & monitoring)5 and in that case there is no detail given of how the
saving was achieved or measured. Meanwhile, there is evidence that savings are not materialising
in the partnership space, with last year’s RW Baird Survey suggesting CRO costs have increased,
particularly for large pharma where the majority of the strategic partnership deals have been
created.6

11
In a nutshell, there are two big problems with strategic partnerships in our industry. The first is that
they are not strategic. The second is that they are not partnerships.
What Does ‘Strategic’ Mean?
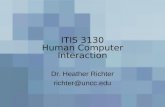
The concept of strategic purchasing can be traced back to a seminal paper by Peter Kraljic
published in Harvard Business Review in 1983.7 Kraljic explained how suppliers can be classified
in terms of cost and the risk they present of failing to supply (perhaps failing to recruit patients).
The implications of Kraljic are shown in Figure 1. When assessing suppliers, we calculate what the
supply failure risk is versus cost, which gives us a definition of value. Now, if awarding an entire
portfolio, it is reasonable to position small CROs at point A representing low cost but high risk,
while the larger, better-established CROs might occupy point B, representing high cost with lower
risk. The place any buyer would like to be is at point C, but that isn’t very realistic. Instead, the goal
might be to get to point D.
The message is that it may be better to do that by investing in mitigating the risk of a low cost
provider than by negotiating discounts with an established one.
Investment to support a provider is a real strategic
approach. Procurement professionals call it ‘supplier
development’, and it is clear to see how such a philosophy
might lend itself more readily to engaging cheaper, riskier,
smaller providers.
In our industry, however, we have made it a pre-requisite of strategic partnerships that the provider is large and global.
Figure 1
Kenneth Getz observes: “Small and mid-sized CROs have largely been left behind while major
CROs — the only organizations with sufficient scale and diverse talent — service a growing
number of integrated relationships.”2
This prevailing attitude reduces the science of procurement to mere shopping, and is reminiscent of
the old phrase “nobody ever got fired for hiring IBM.” Strategic purchasing should be about
mitigating supply failure risk, but in our space nobody ever talks about that in the same breath as
strategic partnering. The single biggest risk of supply failure — not recruiting patients — is never
mentioned. The focus instead is on discounts and, for me, it’s depressing that such tactical, point-of-
contract saving-mechanisms are constantly touted as strategic solutions when frankly they are not.
However, due to the $125 billion patent cliff our industry faces, pharmaceutical executives are
desperate to focus on savings – immediate savings – that can only be reported through tactical
means. So pharma talks strategic, but acts tactically, and nobody can blame the big CROs for
making some money out of the situation. It’s like the Emperor’s New Clothes. It wasn’t the fault of
the tailors. The Emperor brought his predicament entirely upon himself.

12
Partnerships and the Risk Dynamic
In the Journal of Clinical Research Best Practices, Ronald Waife writes: “[T]here is nothing to be
gained by characterizing service providers as partners… the criticism of a pay-for-service
relationship in favour of something somehow more lofty is misplaced and misleading.”8
True partners share interests, risks and profits. However, in Waife’s analysis, sponsor risks and
profits are high, while CRO risks and profits are more modest. But on this detail I tend to disagree
because my observation for the subset of CROs who have cornered the strategic partnership market
is that they generate profits (as a percentage of earnings) comparable to those of their clients.
Just consider the market. Private equity companies have been scrambling to get into the CRO
business over the last 8 years, with 14 formerly public CROs having moved into private ownership.9
Such investors don’t go hunting acquisitions in industries where profits are modest and, all the
while, strategic partnering is where they most want to be. The acquisition activity associated with
this has driven a consolidation of CROs, and economists tell us that as the number of suppliers
decreases, so prices rise in the pursuit of profit.10
This is especially true in the supplier base for strategic partnerships because, remember, we have
made it a pre-requisite of strategic partnerships that the provider is large and global. This has
limited our options, with one analyst claiming that the six largest CROs now account for 50% of
total clinical CRO revenues.11 This means a market that economists describe as ‘oligopoly’,
characterized by, among other features, high profits for the suppliers.10
It would be OK for the CRO side of the partnership to enjoy high profits if they shared the risk but,
as Waife points out, this is where the partnership concept really breaks down:
“The CRO’s risk in non-performance is mostly one of tarnished reputation… [but] responsibility for
failure is usually obscure… [and] sponsors are notoriously loathe to pursue penalties. If there is a
sanction it would most likely be loss of work. But … sponsors routinely continue to give work to
service providers who have failed them.”8
Put simply, risk sharing does not exist between customer and service provider, and you can’t have a
partnership without shared risk. Waife and I agree on the solution for this dilemma: accept that the
risk is always with the client, who should therefore take responsibility for managing the risk.
Taking responsibility for risk means being the boss, not a partner. Partnerships create governance
built on issue escalation and nannying project teams with CRO personnel in committees where they
are equal or senior to sponsor personnel, blurring the distinction between customer and service
provider and harming delivery. We should replace traditional governance with a lean system where
pharma focuses on risk and quality management and the CRO gets on with delivering its services.
Waife concludes: “[Why] not just pay your CRO for competent work without all the ‘partnership’
trappings? Look at any press release for a new sponsor-CRO partnership. Every single service or
advantage listed… can be purchased… from that CRO… without a partnership agreement.8

13
Waife might as well say that partnerships in our space are like lipstick on a pig. You can dress up
service delivery as something more beautiful, but it’s still service delivery. Any suggestion the
sponsor might benefit from subscribing to the partnership fantasy is groundless in fact and
potentially dangerous.
Conclusion
In summary, strategic purchasing is concerned with mitigating the risk of supply failure. This risk
cannot be shared, because service providers and sponsors have different interests. A partnership
relationship is one where risks are genuinely shared because interests are shared. The concept of a
strategic partnership is therefore an oxymoron. It cannot be fit for purpose, and is a classic example
of how an idea can become popular despite practically zero evidence of claimed benefits.
It has probably not escaped your notice that should (as would seem likely) the risk/cost profiles of
CROs described in Figure 1 vary significantly between trials (so that, for a given trial, a cheaper
CRO may also sometimes be less risky) then a policy of radically limiting one’s supplier base will
impact the possibility of achieving best value from one trial to another. Thorough study of this
dynamic — considering total cost of ownership in order to fully understand the pros and cons of
limiting one’s options — is therefore essential for any sponsor considering its sourcing strategy.
Taking such an evidence-based approach is well rehearsed in the procurement profession, where it
is called ‘value analysis’. However, to my knowledge, no such analysis has ever been undertaken
prior to implementing a preferred provider policy for clinical trial outsourcing.
Adoption of procurement best practice is what has been missing in clinical trial outsourcing as
pharmaceutical executives have preferred a wild goose chase for the utopian dream of partnering
with service providers. I would add that when sponsors accept that they alone own their risk — that
they cannot share it via misconceived partnerships — then they can justly demand full transparency
and slim profit margins from CROs who, ring-fenced from risk, will have no excuse not to comply.
Perhaps only then will sponsors secure the ultimate prize of reducing real costs rather than
recognizing imaginary savings…and subscribing to the myth of the Emperor’s New Clothes.
References 1. Graham Hughes, Contract Research Annual Review 2011, The Complete Picture of the Contract Research Market, Biopharm Knowledge Publications 2011.
2. Kenneth Getz, “Profound Shifts in Outsourcing Landscape”, 10–15, Inside Outsourcing, A Supplement to Applied Clinical Trials, November 2011.
3. Bertrand Russell, BBC Interview, 1959.
4. Prof. John Seddon, “Why do we believe in economy of scale?” White paper, July 2010.
5. Karyn Korieth, “Integrated CRO alliances growing but poorly executed,” 1, 12–16, CenterWatch Vol 18, issue 09, September 2011.
6. Nick Taylor, “CRO prices increasing, survey finds,” www.outsourcing-pharma.com, 29th September, 2011.
7. Peter Kraljic, “Purchasing must become supply management,” Harvard Business Review, September 1983.
8. Ronald S. Waife, “Partnership Heresy,” Journal of Clinical Research Best Practices, Vol. 8, No 1, January 2012.
9. Paul Richter, Jina Ventures, speaking at 8th Annual PCMG Conference, June 2012.
10. Hunt & Morgan, “The Comparative Advantage Theory of Competition,” Journal of Marketing, 1–15, Vol 59, April 1995.
11. Jim Miller, President PharmSource Information Services Inc, Feb 2011.
Andy Parrett
PCMG Chairperson

14
December Workshop
An Inside Look at the Financial Side of Clinical Trials
Nice, Thursday 6th December
This workshop explores the complex financial issues at the heart of every clinical trial contract.
Covering topics ranging from budgeting through to managing currency fluctuation, the workshop will
give participants insights and knowledge to help them manage their own spending more effectively.
Workshop Sessions
Financial Considerations in Clinical
Development
• Currency fluctuation.
• Inflation.
• Tax.
Led by: Daniel Nicholson, Outsourcing &
Contract Manager, Grünenthal GmbH.
How Much More are we Paying for
our Trials and is it Justified?
• A historical look at costs.
Led by: TBC, Medidata.
Case-Study: Streamlining Pass-
Through Costs
Led by: David Mantell, European Head,
Global Procurement - Pharma Development
Services, Bayer PLC.
Case Study: System-Supported
Budget Planning, Forecasting and
Management
• System requirements.
• Custom made versus off-the-shelf.
• System features.
• Lessons learned.
Led by: Birgit Viechtbauer, Planning &
Resource Manager, Grünenthal GmbH.
Financial Considerations Around
Outsourcing & Budgets in Other
Industries: What Can we Learn?
• Consulting as a business.
• An introduction to the construction
industry.
• Outsourcing: sub-contractors and
consultants, off-shore working, fully
outsourced model, pros and cons.
• Models and market drivers including
the Buro Happold position; current
position, planned position.
Led by: Andrew Comer, Director
Environment & Infrastructure / Buro Happold
Ltd.
Interactive Presentation: Financial
Assessment of Suppliers
• Why bother?
• Contingencies.
• Providers of credit-worthiness data.
Led by: Mike Sitton, Director, Clear Cut
Services Ltd.
.
Booking Information
Venue: Grand Hotel Aston, Nice.
To book: See www.pcmg.org.uk
PCMG workshops are open only to members
and guests from their company.

15
January Workshop and AGM
Working with Clinical Trial Technical Providers London,
Wednesday 23rd January
We start 2013 with a workshop that will be of value to all those who select and manage technical
providers. With topics ranging from initial assessment through to measuring and tracking, this
workshop will give you tools and techniques that will help you make better-informed decisions about
providers and get the best value from those you do decide to work with..
Workshop Sessions
The workshop will include a separate session
on each of five types of provider: Central
Laboratory Services, IVR, Cardiac Safety,
Imaging, and ePRO. Topics covered will
include:
• Assessment
• Value drivers
• Costs and cost models
• Interpreting proposals
• Measuring performance
There will also be a second session on
working with Central Laboratory providers.
This will focus on ways to track and improve
logistics budget management as study
specifications evolve from initial proposal
through to study delivery.
Central Laboratories
Presenters
Session one: Karolyn Jackson
Clinical Labs Performance Director
Alliance Management, AstraZeneca
Session two: Upinder Grewal
Director, Logistics, Icon Central Laboratory
IVR
Presenter: Wendy Allen-O’Grady
R&D Procurement Manager
Science & Technology Category, Global R&D
Procurement, AstraZeneca
Cardiac Safety
Presenter: Crister Malm
Vice President, Business Development
Europe, ERT & Pharma Guest Speaker TBD
Imaging
Presenter: Andrew McDonald
Imaging Outsourcing Specialist, Key Service
Area Manager, F. Hoffmann-La Roche Ltd.
ePRO
Presenters: Adam Wood, Account Director,
ERT & Pharma Guest Speaker TBD.
Booking Information
Venue: Hilton Kensington, London.
To book: See www.pcmg.org.uk
PCMG workshops are open only to members
and guests from their company.
PCMG AGM
The PCMG Annual General Meeting will be held from 11.40 – 12.15. It is open to all PCMG members, whether attending the workshop or not. Please join us if you can.

16
PCMG Event Schedule
Thurs 6th
December 2012 – Nice
Financial Management of Clinical Outsourcing Sponsored by Medidata
Committee Support – Stephanie Kamp & Alison Moor
Wed 23rd January 2013 – London
Clinical Trial Technical Providers Sponsored by ICON Labs and ERT
Committee Support – Cliff Leat & Andy Parrett
Wednesday 20th March 2013 – Germany (City TBC)
Advanced Negotiation Training Committee Support – Alison Moor
Wednesday 5
th- Friday 7
th June 2013 – Budapest
Annual Conference
Thursday 10th October 2013 –London
KPIs & Metrics Committee Support – Lan Bandara & Steve Martindill
January 2014 –London
Procurement Best Practice & Tools Committee Support – TBC
Non-PCMG Events