Payment Model Reform: The Effects on Healthcare Information Technology
25
Page 1 of 25 Payment Model Reform: The Effects on Healthcare Information Technology Mark Lucido The University of Texas at Dallas HMGT 4321 Mehmet Ayvaci
-
Upload
mark-lucido -
Category
Documents
-
view
218 -
download
0
Transcript of Payment Model Reform: The Effects on Healthcare Information Technology

7/27/2019 Payment Model Reform: The Effects on Healthcare Information Technology
http://slidepdf.com/reader/full/payment-model-reform-the-effects-on-healthcare-information-technology 1/25
Page 1 of 25
Payment Model Reform: The Effects on Healthcare Information Technology
Mark LucidoThe University of Texas at Dallas
HMGT 4321Mehmet Ayvaci

7/27/2019 Payment Model Reform: The Effects on Healthcare Information Technology
http://slidepdf.com/reader/full/payment-model-reform-the-effects-on-healthcare-information-technology 2/25
Page 2 of 25

7/27/2019 Payment Model Reform: The Effects on Healthcare Information Technology
http://slidepdf.com/reader/full/payment-model-reform-the-effects-on-healthcare-information-technology 3/25
Page 3 of 25
Table of ContentsIntroduction .................................................................................................................................................. 5
Payment Model Overview ............................................................................................................................ 5
History of Payment Models .......................................................................................................................... 7
1900-1930 ................................................................................................................................................. 7
1931-1964 ................................................................................................................................................. 8
1965-1994 ................................................................................................................................................. 8
1995-2008 ................................................................................................................................................. 9
2009 – Present ........................................................................................................................................ 10
Healthcare Reform and Effects ................................................................................................................... 11
Risk Reduction Overview ............................................................................................................................ 12
Risk Reduction by Payer Type ................................................................................................................. 13
Commercial Payers ............................................................................................................................. 13
Government Payers ............................................................................................................................ 13
Affordable Care Act ..................................................................................................................................... 14
Coverage Options .................................................................................................................................... 14
Catastrophic ........................................................................................................................................ 14
Bronze (60%) ....................................................................................................................................... 14
Silver (70%) ......................................................................................................................................... 14
Gold (80%) ........................................................................................................................................... 15
Platinum (90%) .................................................................................................................................... 15
Payment Models ..................................................................................................................................... 15
Macroeconomic Effects .......................................................................................................................... 17
Providers ............................................................................................................................................. 18
Vendors ............................................................................................................................................... 19
Healthcare Revenue Cycle .......................................................................................................................... 19
Revenue Cycle Management ...................................................................................................................... 20
Patient Access ......................................................................................................................................... 21
Patient Encounter ................................................................................................................................... 22
Billing Cycle/Payment Management ....................................................................................................... 22
A/R Management .................................................................................................................................... 23

7/27/2019 Payment Model Reform: The Effects on Healthcare Information Technology
http://slidepdf.com/reader/full/payment-model-reform-the-effects-on-healthcare-information-technology 4/25
Page 4 of 25
Collections Management ........................................................................................................................ 23
Conclusion ................................................................................................................................................... 24
Works Cited ................................................................................................................................................. 25

7/27/2019 Payment Model Reform: The Effects on Healthcare Information Technology
http://slidepdf.com/reader/full/payment-model-reform-the-effects-on-healthcare-information-technology 5/25
Page 5 of 25
Introduction
Since the introduction of Medicare in the mid-Sixties, healthcare costs in the United States have risen
exponentially. In the decades that followed, each subsequent legislative action brings with it the
promise of lower costs beginning with the passage of the HMO Act in the Seventies. Costs have
continued to escalate; now upwards of $3 Trillion dollars, healthcare spending comprises nearly 18% of
GDP. Now with implementation of the Affordable Care Act in full swing, the introduction of new
payment models promises to change the incentives that drive healthcare costs and place the emphasis
on quality and outcomes. These payment models will come at a price to providers however both in
terms of risk and the technology outlay to manage day-to-day operations.
Payment Model Overview
There are a variety of payment models in use today in the United States. Most models fall under one of
two categories: Retrospective, or Prospective. Retrospective payment models reimburse a provider
after services have been rendered at the provider’s prevailing rates (Casto and Layman). Payment
models that fall under this category include:
Cost based – reimburses the provider based on provider’s cost
Fee For Service – reimburses the provider based on a fee schedule or discounted fee schedule
Prospective payment models on the other hand, compensate the provider based on pre-established
rates (Casto and Layman). Payment models in this category include:
Per Diem/Per Case – compensated on a per-day flat rate or on average resource levels for a
particular diagnosis with variations for levels of severity

7/27/2019 Payment Model Reform: The Effects on Healthcare Information Technology
http://slidepdf.com/reader/full/payment-model-reform-the-effects-on-healthcare-information-technology 6/25
Page 6 of 25
Value Based Purchasing (VBP)/Pay For Performance (P4P) – As the name implies, this payment
arrangement rewards providers through incentive payments based on certain predetermined
quality measures and patient outcomes. As opposed to some payment models that incent on
cost reductions, VBP/P4P incents providers to improve patient outcomes thus delivering value
for the healthcare dollar hence the name.
Episode of Care – also known as bundled payment. This compensation method remunerates a
group of providers for a single patient’s episode of care which spans the time horizon from
initial diagnosis to post-acute rehabilitation
A newer trend in healthcare reform known as Population Health is beginning to gather momentum.
Although this isn’t a payment model per se, we chose to categorize a few models that technically fall
under the Prospective Payment category, separately under Population Health for this research to
emphasize the shift away from the per-patient reimbursement methods of our past.
Under Population Health, the reimbursement rates are pre-negotiated based on a variety of variables
such as quality, cost, and average care utilization however the underlying basis for remuneration is a
group or population of insured members assigned to the provider.
Shared Savings – Bonus payments to ACO providers that incent coordination of care and cost
reduction across a population of patients and healthcare services by meeting predetermined
cost and quality measures
Capitation – a predetermined compensation amount paid to an individual provider or group of
providers based on a flat per member per month arrangement for the number of covered
members assigned to that provider

7/27/2019 Payment Model Reform: The Effects on Healthcare Information Technology
http://slidepdf.com/reader/full/payment-model-reform-the-effects-on-healthcare-information-technology 7/25
Page 7 of 25
History of Payment Models
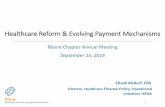
To better put these various payment models into perspective, a historical review of the issuing
legislature is important to understand. Exhibit 1 provides a graphical overview:
12/8/2003
Medicare Prescription Drug,
Improvement, and Modernization Act
3/23/2010
PPACA - Obamacare4/20/1983
S.S. Amendments of 1983
Prospective Payments1942
Stabilization Act of 1942
Employer Sponsored
Health Insurance
1965
Medicare1930
Blue Shield
1900 2050
1929
Baylor Health Plan
(Blue Cross)
Retrospective Prospective
Cost Reimbursement Fee For Service Per Diem/Per Case P4P Episode Capitation
Exhibit 1: Payment Model and Legislative Timeline
1900-1930
Prior to the 1920’s, the medical field had very low overhead based on a low technology curve and the
comparatively small amount of medical knowledge for the time. Because of these factors, a physician’s
only real cost was their time therefore payments to providers were for their cost. This changed starting
in 1929 however when Baylor Hospital in Dallas, Texas developed the first form of Hospital insurance for
Texas teachers which would become known as Blue Cross. The following year, Blue Shield plans began
to emerge and the Health Insurance market was established which would form the basis for our existing
system of misaligned incentives associated with third-party payers.

7/27/2019 Payment Model Reform: The Effects on Healthcare Information Technology
http://slidepdf.com/reader/full/payment-model-reform-the-effects-on-healthcare-information-technology 8/25
Page 8 of 25
1931-1964
The next significant development in Healthcare Reimbursement came during World War II when
America was forced to make important economic tradeoff in both raw materials and labor. Specifically,
on October 2, 1942, in an attempt to curve inflationary pressures, President Franklin D. Roosevelt
enacted the Stabilization Act of 1942 which established wage price controls or wage ceilings. As is
common with most attempts of Government to intervene, the unintended consequences became what
we know and love today as Employer Sponsored Health Insurance.
As our medical knowledge and technology grew, so did a provider’s cost curve. Provider’s fee schedules
were implemented to reflect these changes and insurance companies reimbursed based on these fee
schedules or variants of them discounted however for what was usual and customary within a region.
1965-1994
The 1960’s brought about many social changes in American culture which extended into our politics and
healthcare system. On July 30, 1965, President Lyndon Johnson signed into law the Medicare bill which
would dramatically change the landscape of the American Healthcare system forever. From this point
forward, healthcare spending in the United States would grow exponentially.
The introduction of Medicare Insurance is important to note in a review of reimbursement models
because since its introduction, Medicare not only serves as the gold standard in how commercial
insurance companies reimburse providers but also the Medicare reimbursement affects Commercial
payers through Hospital cost-shifting.
When Medicare was first implemented, the system reimbursed at the prevailing Fee for Service rates. In
the years and decades that followed there would be continued legislative attempts at controlling costs
by controlling reimbursement. The first of these came on December 29, 1973 with the enactment of the

7/27/2019 Payment Model Reform: The Effects on Healthcare Information Technology
http://slidepdf.com/reader/full/payment-model-reform-the-effects-on-healthcare-information-technology 9/25
Page 9 of 25
Health Maintenance Organization Act of 1973. Although this regulation didn’t directly affect the way
providers were remunerated, it is important to mention here because the HMO model of Managed Care
serves as the predecessor for our current ACO model which does have remuneration tied to it.
From a reimbursement perspective, the more important legislation to note is the Social Security
Amendments of 1983. This law became the milestone change in provider reimbursement through the
creation of the Prospective Payment system which effectively eliminated a direct Cost-Based or Fee for
Service reimbursement in exchange for one based on average costs across providers within a similar
grouping.
The other milestone event from this period that is important to mention in this research is the Health
Security Act of 1993. The proposals originally offered by the Clinton Administration never actually
passed to become law however, similar to the HMO Act of 1973, many of the elements from this reform
were used as the foundation for the Patient Protection and Affordable Care Act.
1995-2008
The 1990’s also saw another dramatic change in Healthcare with the passage of the Health Insurance
Portability and Accountability Act in 1996. As part of this act, a demonstration project was approved for
the Archer Medical Savings Account. This demonstration project however would not become
mainstream until December 8, 2003 with the enactment of The Medicare Prescription Drug,
Improvement, and Modernization Act which formalized the concept of Consumer Driven Health Care
through the creation of the Health Savings Account (HSA) (United States Congress).
As defined by the IRS, a Health Savings Account is a tax-exempt trust or custodial account that you set
up with a qualified HSA trustee to pay or reimburse certain medical expenses you incur (U.S.
Department of the Treasury, Internal Revenue Service). Funds can be directly contributed to an HSA

7/27/2019 Payment Model Reform: The Effects on Healthcare Information Technology
http://slidepdf.com/reader/full/payment-model-reform-the-effects-on-healthcare-information-technology 10/25
Page 10 of 25
either by you, on your behalf, or by your employer. Tax benefits apply provided they are used for
qualified medical expenses as outlined by the IRS. All contributions by you, on your behalf, or by your
employer are exempt from income taxes and excluded from Gross Income. Contributions are subject to
annual contribution limits to qualify for deductions. For 2013, the maximum allowable amount is $3,250
for single coverage and $6,450 for family coverage. Interest and earnings on the assets in the account
grow tax free. Funds remain in the account for future years. You own the account and account
holdings; therefore the account is portable or transferrable if you should change jobs or employers.
The importance of the HSA to Healthcare Reimbursement is that it was the first dramatic shift away
from a provider-driven consumption and a third-party-payer reimbursement system to one of patient
accountability. It places healthcare utilization in the hands of the consumer to determine their rate of
consumption through rational decision making. It also creates more risk for the provider to collect a
greater portion of their reimbursement directly from the consumer who is often stretched thin and is
not accustomed to planning ahead for catastrophic events. In addition to the Medicare Prescription
Drug, Improvement, and Modernization Act of 2003, the 2005 Deficit Reduction Act established Quality
Reporting standards that would later be built upon for Reimbursement Models adopted under the
PPACA in 2010.
2009 – Present
Fast forward our discussion now to March 23, 2010 and the passage of The Patient Protection and
Affordable Care Act (PPACA). With the exception of Medicare creation in 1965, all subsequent
legislature since has accomplished only small changes in healthcare primarily around reimbursement.
That is until The Affordable Care Act, which is a sweeping overhaul to address access, coverage and
quality of coverage and care. Additionally, there are both direct and indirect effects on provider
remuneration. Briefly postponing the indirect effects for a moment, the direct reimbursement changes

7/27/2019 Payment Model Reform: The Effects on Healthcare Information Technology
http://slidepdf.com/reader/full/payment-model-reform-the-effects-on-healthcare-information-technology 11/25
Page 11 of 25
outlined in the legislature include the creation of Accountable Care Organizations, CMS’ demonstration
project for the Shared Savings Program and the goals for Value Based Purchasing and Bundled
Payments.
Healthcare Reform and Effects
Just as we’ve seen with the establishment of price controls in 1942, Government regulations usually
involve some form of unintended consequences and considering the overarching goals of the PPACA,
there are bound to be many.
The three primary goals accomplished by The Affordable Care Act are:
Improve Quality and Affordability of Coverage
Increased Access and the role of Government programs
Improved Quality of Healthcare Services
In addition to the direct reimbursement changes previously outlined, there are indirect effects on
provider remuneration through the creation of inexpensive coverage options to expand covered lives.
Many of those lives will be covered under CDHP options in the exchanges which will result in significant
upside risk for providers to collect directly from patients.

7/27/2019 Payment Model Reform: The Effects on Healthcare Information Technology
http://slidepdf.com/reader/full/payment-model-reform-the-effects-on-healthcare-information-technology 12/25
Page 12 of 25
Risk Reduction Overview
Traditionally, the idea of insurance is to reduce the risk of an unexpected catastrophic event. By
collecting variable premiums from many individuals, an insurance company is able to spread that risk
across large groups of people. In our current system of reimbursement, provider remuneration comes
from one of two sources; Government Insurers or Commercial insurers who assume nearly all the risk
while the provider and patient or insured assumes very little risk. Over the years, with each change in
reimbursement, whether direct or indirect, the balance of risk is shifted away from the insurer and onto
both the provider and patient as illustrated in Exhibit 2 (Fleming, Forney W. MD, MBA).
Exhibit 2: Payment Models and Risk Transfer Over Time

7/27/2019 Payment Model Reform: The Effects on Healthcare Information Technology
http://slidepdf.com/reader/full/payment-model-reform-the-effects-on-healthcare-information-technology 13/25
Page 13 of 25
Risk Reduction by Payer Type
Commercial Payers
Traditionally, Commercial payers have been able to shift the risk onto their members by increasing some
combination of their premiums, copayments, deductibles or coverage limits. With the introduction of
the Health Savings Account, an even greater portion of risk has been shifted onto patients directly
through a combination of higher first-dollar deductibles, lower coverage limits and higher premiums. As
this risk is shifted to patients, an equal amount of risk is shifted to providers in that it requires greater
administrative processing and tools to collect directly from patients. Many of the provider’s Practice
Management and Patient Accounting systems do not incorporate the necessary tools to verify coverage,
verify propensity to pay and collect payment directly from patients therefore providers must rely on
third-party vendors to provide bolt-on solutions.
Government Payers
Risk reduction for Government payers is significantly different from that of Commercial payers.
Government payers are unable to simply raise prices on consumers as their overarching goal is a fair and
equitable entitlement for all citizens. This leaves only the provider community from which to choose
whom to shift the costs to. Traditionally, this has been managed by changing the payment models and
how providers are reimbursed and with each change brings with it more risk assumed by the provider.
This trend continues with the passage of The Affordable Care Act where three new payment models will
be adopted across the industry. The legislation doesn’t stop there however. With the introduction of
the Insurance Exchanges and the five coverage options, many of the lower cost plans offered will be
Consumer Driven, high-deductible plans. A large influx of previously uninsured patients will be entering
the system who is constrained by income limitations. There is a strong probability that a substantial
portion of the plans sold through the exchanges to the newly insured will fall under CDHPs creating a

7/27/2019 Payment Model Reform: The Effects on Healthcare Information Technology
http://slidepdf.com/reader/full/payment-model-reform-the-effects-on-healthcare-information-technology 14/25
Page 14 of 25
significant percentage of provider revenue that will need to be collected directly from patients who are
not accustomed to planning for catastrophic events. In addition, as has been discussed in the media
recently, many existing plans do not meet the minimum coverage requirements outlined in the PPACA
due to their low cost. Due to the popularity and low-cost nature of CDHPs, there is a high likelihood
those plans will be replaced with CDHPs further compounding the risk for providers.
Affordable Care Act
Coverage Options
There are 5 distinct health plan options offered through the Insurance Exchanges each ranging in
premium costs and coverage levels based on the actuarial value of the plan (United States Congress).
Catastrophic
Catastrophic plans are the least costly of all plans offered in the exchanges however these plans are
limited to only eligible individuals 29 and under or qualify for hardship exemptions. Plans in this level
provide coverage that is designed to provide benefits that are actuarially equivalent to less than 60
percent of the full actuarial value of the benefits provided under the plan.
Bronze (60%)
Bronze plans are the lowest premium cost of the standard plan options but the highest cost for total out
of pocket expense. Plans in this level provide coverage that is designed to provide benefits that are
actuarially equivalent to 60 percent of the full actuarial value of the benefits provided under the plan.
Silver (70%)
Silver plans are the next lowest premium cost of the standard plan options with the next highest cost for
total out of pocket expense. These plans provide coverage that is designed to provide benefits that are
actuarially equivalent to 70 percent of the full actuarial value of the benefits provided under the plan.

7/27/2019 Payment Model Reform: The Effects on Healthcare Information Technology
http://slidepdf.com/reader/full/payment-model-reform-the-effects-on-healthcare-information-technology 15/25
Page 15 of 25
Gold (80%)
Gold plans are the next most costly in premiums of the standard plan options with the next lowest cost
for total out of pocket expense of all plans. These plans provide coverage that is designed to provide
benefits that are actuarially equivalent to 80 percent of the full actuarial value of the benefits provided
under the plan.
Platinum (90%)
The most costly in premiums of all plan options, however offer the lowest total cost for out of pocket
expense. Platinum plans provide coverage that is designed to provide benefits that are actuarially
equivalent to 90 percent of the full actuarial value of the benefits provided under the plan.
Payment Models
As previously mentioned, there are three distinct payment models introduced in the Affordable Care Act
that should be considered: 1) Shared Savings Program, 2) Value-Based Purchasing and 3) Bundled
Payments. Following is a closer analysis of each:
Shared Savings Program - The CMS Shared Savings Program provides incentive bonus payments
to ACOs based on their provider’s combined ability to meet predetermined cost reductions and
quality performance standards (American College of Physicians) (RTI International). While this
model attempts to realign incentives within the industry to facilitate care coordination, in order
for providers to benefit from this model a clear and solid understanding of their colleague’s
performance is important when making care coordination decisions in order to maximize
revenue potential. To participate, providers must organize under an ACO which is a group of
providers and suppliers of services that work together to coordinate care for Medicare FFS
patients. ACOs must meet all eligibility and program requirements and must serve at least
5,000 Medicare FFS patients and agree to participate for three years and cannot participate in
any other shared savings program. Standard FFS payment arrangements continue however

7/27/2019 Payment Model Reform: The Effects on Healthcare Information Technology
http://slidepdf.com/reader/full/payment-model-reform-the-effects-on-healthcare-information-technology 16/25
Page 16 of 25
benchmarks are established that ACOs agree to perform against. There are 2 distinct
benchmark models: 1) One-sided in which sharing savings, but not losses for the entire term of
the first agreement and 2) two-sided model where both savings and losses for the entire term
are shared. Under both models, an ACO must meet quality standards, achieve savings and also
meet or exceed a Minimum Savings Rate. Savings are calculated based on the ACO quality
score. There are 33 quality measures across 4 domains: 1) Patient/caregiver experiences (7
measures), 2) Care coordination/patient safety (6 measures), 3) Preventive Health (8
measures), 4) At-risk populations (diabetes, hypertension, Ischemic Vascular Disease, Heart
failure, Coronary Artery Disease). Quality measures will be reported through a combination of
CMS claims and administrative data, the ACO GPRO web interface for clinical quality measure
reporting, and patient experience of care surveys.
Value-based Purchasing – Hospital providers who participate in the VBP incentive program will
receive bonus incentive payments for delivering quality of care to Medicare patients. For
participation in the program, providers must agree to an annual reduction in base operating
DRGs, as illustrated in Exhibit 3, in order to fund the incentive payments (Centers for Medicare
and Medicaid Services). To determine payment, hospitals will be measured on two domains, 1)
Clinical Process of Care and 2) Patient Experience of care starting with a benchmarking period
followed by subsequent performance periods. To measure hospital providers, CMS will use a
combination of claims data and thirteen Clinical Process of Care measures which were selected
from Hospital Inpatient Quality Reporting Program for Fiscal Year 2013.
FY 2013 FY 2014 FY 2015 FY 2016 FY 2017Subsequent
Years
DRG %
Reduction 1.00% 1.25% 1.50% 1.75% 2.00% 2.00%
Exhibit 3: Base Operating DRG Reduction Percentages

7/27/2019 Payment Model Reform: The Effects on Healthcare Information Technology
http://slidepdf.com/reader/full/payment-model-reform-the-effects-on-healthcare-information-technology 17/25
Page 17 of 25
Bundled Payments – According to the CMS website, there are four models being tested for
Bundled Payments (Centers for Medicare and Medicaid Services). They vary in nature from
retrospective based to prospective based. Model 1 emphasizes the Acute Inpatient setting
with a discounted prospective rate during the inpatient stay and separate payments to
individual physicians. Providers are permitted to share gains under certain circumstances
however. Model 2 has a retrospective basis that reconciles the hospital’s costs against a target
price for the particular episode of care. A single bundled payment is issued for the entire
episode of care based on up to 48 different clinical conditions selected by participants. Model
3 emphasizes the post-acute episode of care and is triggered by an acute care discharge. A
singled bundled payment is issued for the entire rehabilitation period based on up to 48
different clinical conditions selected by participants. Model 4 is a bundled payment that
applies to all services furnished during the entire episode for an inpatient stay only. All
physicians must submit zero dollar claims and will subsequently be paid by the hospital from
the bundled payment based on up to 48 different clinical conditions selected by the
participants.
Macroeconomic Effects
In order to understand what technology is affected by new payment models, one must first understand
the macroeconomic impacts. Patients will assume new risks of higher prices; however they will have
little influence over the technology other than the sheer increase in patient volumes coming from
increased access. Therefore in our research we only considered the impact to certain groups such as to
Providers and the impacts to software Vendors.

7/27/2019 Payment Model Reform: The Effects on Healthcare Information Technology
http://slidepdf.com/reader/full/payment-model-reform-the-effects-on-healthcare-information-technology 18/25
Page 18 of 25
Providers
Providers are the most impacted by payment model reform for many reasons. First, they are assuming
new risks of payment based on patient populations with little previous experience in actuarially
calculating that risk. There will soon be demand to develop solutions that assist with these actuarial
calculations. Secondly, providers are assuming more financial risk associated with a change in their
payer mix; a greater portion of their revenue is coming now from patients as opposed to third-party
payers. Stronger processes and solutions will be needed to reduce this risk through upfront eligibility
and verification checking in addition to propensity to pay, upfront patient collections and payment plan
solutions. Thirdly, when sharing revenue with multiple providers, a portion of that revenue is at risk
based on the performance of other providers whom you have no control over. Solutions in the clinical
setting will be needed to help identify and match high-performing providers/specialists in close
proximity to the patients they serve when referring patients. Next, there is the risk associated with the
technological constraints of these new models. Providers are increasingly becoming reliant on the
vendor community to offer solutions to the new models which will require a thorough understanding of
quality reporting and the types of data, mostly clinical in nature, needed to facilitate reimbursement
while much of that is unknown. Also there are currently Contract Management systems that are not
built to support these new contract types. Contract Management enables a provider to not only store
the providers contracts from the various commercial payers, but also model what if scenarios as they
approach contract renegotiations. These systems will have to be modified. Lastly, there has been a
significant trend over the last few years to acquire and consolidate among providers. Physician practices
have been consolidating while others have been acquired by hospitals to form larger ACOs. Each
acquisition or consolidation brings with it the technical challenge of integration and interoperability.
Solutions of all type will be needed to reduce this integration curve.

7/27/2019 Payment Model Reform: The Effects on Healthcare Information Technology
http://slidepdf.com/reader/full/payment-model-reform-the-effects-on-healthcare-information-technology 19/25
Page 19 of 25
Vendors
As a result of the shifts in payment models, vendors too have been affected indirectly for many of the
same reasons providers have. First, due to the bolt-on nature of the industry, many of the solutions are
fragmented, not only across the revenue cycle but also between physicians and hospitals. There are
many vendors who specialize serving the hospital market and others who specialize serving the
physician market. As provider acquisitions and consolidations continue, this is creating an environment
where some vendors are becoming disintermediated forcing them to make defensive moves into other
verticals (vertical integration) or acquire and consolidate amongst themselves forcing solution
integration. In both cases, this serves as a detractor from innovation and organic growth in solutions at
a time when innovation and integration are both at a premium.
Healthcare Revenue Cycle
Considering most healthcare IT investments emphasize the billing process, the industry has created
specific acronyms and terminology to describe this and communicate effectively. As illustrated in
Exhibit 4, the Healthcare Revenue Cycle describes the cyclical process surrounding reimbursement for a
patient encounter (Lucido, Mark). Since provider reimbursement and payment models are the core
focus of reform, it is appropriate to understand the Revenue Cycle and Revenue Cycle Management to
understand what systems are affected.
The process often begins prior to a patient’s arrival, also called Patient Access, proceeds with the patient
encounter and treatment, is followed by the billing cycle and concludes with payment and Accounts
Receivables management.

7/27/2019 Payment Model Reform: The Effects on Healthcare Information Technology
http://slidepdf.com/reader/full/payment-model-reform-the-effects-on-healthcare-information-technology 20/25
Page 20 of 25
Exhibit 4: The Healthcare Revenue Cycle
The Revenue Cycle is mostly similar between a physician’s practice and a hospital however there are
slight differences when comparing the two. For example, in the physician’s practice, these tasks are
consolidated across a select few individuals and handled within the four walls of the practice. In larger
multi-physician/multi-office practices and hospitals, these tasks are often departmentalized due to the
volume of patients and greater risk of revenue leakage.
Revenue Cycle Management
Administrative software in the healthcare environment is still predominantly a series of bolt-on
solutions to the core Practice Management or Health Information System. Bolt-on solutions solve for
specific niche problems and because of this, a more horizontal view of the Revenue Cycle, as illustrated

7/27/2019 Payment Model Reform: The Effects on Healthcare Information Technology
http://slidepdf.com/reader/full/payment-model-reform-the-effects-on-healthcare-information-technology 21/25
Page 21 of 25
in Exhibit 5, is necessary which allows Healthcare Administrators to consider each segment more
granularly which subsequently enables deeper workflow analysis (Lucido, Mark).
Exhibit 5: Hospital Revenue Cycle Management
Patient Access
Patient Access is the provider’s process of Patient Intake which also includes pre-intake activities.
Although these processes vary slightly between provider types, for the most part they are similar.
Scheduling and pre-registration/pre-arrival tasks emphasize scheduling, benefit verification and pre-
authorization while registration and check-in serve as a stop-gap for any missed activities in scheduling
and pre-registration. As a patient is admitted or checked-in to an office, there might be a few patient
collection activities or establishment of a payment plan. This vertical is a high area of impact for
payment reform.

7/27/2019 Payment Model Reform: The Effects on Healthcare Information Technology
http://slidepdf.com/reader/full/payment-model-reform-the-effects-on-healthcare-information-technology 22/25
Page 22 of 25
Patient Encounter
More recently because of healthcare reform, healthcare administrators are considering clinical tasks
within the provider’s revenue cycle primarily in order to share clinical information which is becoming a
required interdependency to making more sophisticated reimbursement decisions. This vertical is a
medium to high area of impact for payment reform for several reasons. First, new quality reporting
standards are required which is dependent on information generated during the patient encounter.
Secondly, there is a greater need to share this information across the revenue cycle creating a strong
demand for integration and new ways to use this information.
Billing Cycle/Payment Management
The most fragmented and sophisticated of the revenue cycle segments in terms of bolt-on solutions, the
billing cycle encompasses all tasks associated with coding, claims processing, claim validation and
payment tracking and can often include 7 or more different vendors servicing a single provider type.
The process begins with charge entry and validates correct coding with ancillary solutions that audit
coding practices to ensure revenue maximization. Once a patient encounter has been coded, a claim is
often dropped from the appropriate patient accounting system and scrubbed with HIPAA and payer
edits to ensure a high acceptance and first-pass payment by the payer. Once a claim has been
submitted, automated processes routinely check the payment status and retrieve payment information
to automatically post into the patient accounting system. More recently, comparative analytics is
becoming more important to understand a provider’s performance against their peers of equivalent
characteristics. Considering the solutions in this vertical are all developed to service a Fee For Service
payment model and the trend is to move away from Fee For Service, this vertical is highly impacted by
payment reform.

7/27/2019 Payment Model Reform: The Effects on Healthcare Information Technology
http://slidepdf.com/reader/full/payment-model-reform-the-effects-on-healthcare-information-technology 23/25
Page 23 of 25
A/R Management
The A/R Management segment of a provider’s revenue cycle is most prominent in large physician’s
offices and hospitals where greater revenue leakage is at risk and departmentalization is necessary to
reduce that risk. Most notably, provider types of this magnitude incorporate contract management
solutions into their revenue cycle so they can evaluate upcoming contract renegotiations and
underpayment against the contract. Denials Management is also an important component for this
segment to identify claims that require correction and resubmittal for reclamation of reimbursements
that are rightfully owed the provider. When these solutions are not integrated into a provider’s
revenue cycle, a greater portion of revenue is written off from receivables. Contract Management
solutions are highly impacted by payment reform and will need to be redesigned to service new
population health based payment models.
Collections Management
The last segment in the revenue cycle, Collections Management emphasizes the billing, collections and
write-off process after remuneration from all responsible insurance companies. Patient direct billing
usually involves frequent communications that are automated and timed throughout the revenue cycle.
This implies a tightly integrated set of solutions to coordinate letters and statements, especially when a
commitment to pay has been secured by the patient and a payment plan has been established. If a
provider does not maintain sufficient staffing for internal collections, outsourcing to a third-party
collections vendor is required which further demands integration externally with the vendor. Lastly, if a
payment commitment cannot be secured from a patient, an automated and thorough write-off and
charity process is necessary. This vertical is a medium to high area of impact for payment reform as
there will be greater demand for charity screening to avoid fraud, and providers will emphasize a more
efficient and stringent post-encounter patient communications and collection process.

7/27/2019 Payment Model Reform: The Effects on Healthcare Information Technology
http://slidepdf.com/reader/full/payment-model-reform-the-effects-on-healthcare-information-technology 24/25
Page 24 of 25
Conclusion
Over the last decade, the Healthcare IT field has seen a host of unlikely players entering the Revenue
Cycle segment. In 2007, MedAssets, a leader in Group Purchasing, began its expansion with the
acquisition of XactiMed for Claims Processing and later Accuro, a leader in Contract Management
solutions. In 2008, Experian, a leader in Consumer Credit Scoring, acquired SearchAmerica, a leader in
Healthcare Skip Tracing followed by its acquisition of Medical Present Value for Revenue Cycle
Management solutions in 2011 and most recently the acquisition of Passport Healthcare an even more
significant leader in Revenue Cycle Patient Access and Clearinghouse solutions. In 2011, Trizetto, a
leader in payer membership and claim adjudication systems, acquired Gateway EDI followed by its
acquisition of ClaimLogic in 2012 expanding its footprint into the Provider Revenue Cycle market. These
are just a few of the most substantial consolidations occurring in the industry to address not only
payment reform but more importantly innovative ways to consolidate a provider’s workflow processes
for gains in efficiency, economies of scale and cash flow.
While consolidation creates a strong competitive environment among vendors, the benefits to providers
are substantial. Our Healthcare system may be the most expensive in the world and is fraught with
waste, fraud and abuse resulting in low quality and outcomes. Payment reform addresses many of
these problems, but at the expense of the provider. Ultimately, Providers in the end maintain the
knowledge and skills required to treat, comfort and cure. If we remove all profit and marginalize the
provider, there remains no incentive to practice medicine.

7/27/2019 Payment Model Reform: The Effects on Healthcare Information Technology
http://slidepdf.com/reader/full/payment-model-reform-the-effects-on-healthcare-information-technology 25/25
Works CitedAmerican College of Physicians. "Accountable Care Organizations (ACOs)." n.d. PDF. 12 2013.
<http://www.acponline.org/advocacy/where_we_stand/assets/aco.pdf>.
Casto, Anne B. and Elizabeth Layman. Principals of Healthcare Reimbursement . Chicago: AmericanHealth Information Management Associations, 2006. Web.
Centers for Medicare and Medicaid Services. "Bundled Payments for Care Improvement (BPCI) Initiative:
General Information." Centers for Medicare and Medicaid Services, 2013. Web Page. 7 12 2013.
<http://innovation.cms.gov/initiatives/bundled-payments/>.
—. "Frequently Asked Questions: Hospital Value-Based Purchasing Program." 2012. PDF. 7 12 2013.
<http://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/hospital-
value-based-purchasing/Downloads/FY-2013-Program-Frequently-Asked-Questions-about-
Hospital-VBP-3-9-12.pdf>.
Fleming, Forney W. MD, MBA. "The American Healthcare System: Healthcare Payment Reform."
Richardson: University of Texas at Dallas, 2012.
Lucido, Mark. "Hospital Revenue Cycle Management." Richardson: Availity, LLC, 2012.
RTI International. "Accountable Care Organization 2013 ." Baltimore: Centers for Medicare and Medicaid
Services, 2012. PDF.
U.S. Department of the Treasury, Internal Revenue Service. "Health Savings Accounts and Other Tax-
Favored Health Plans." IRS Publication 969. Washington: GPO, 2011.
<http://www.irs.gov/pub/irs-pdf/p969.pdf >.
United States Congress. "Medicare Prescription Drug, Improvement, and Modernization Act of 2003."
United States Public Law . Washington: GPO, 2003. <http://www.gpo.gov/fdsys/pkg/PLAW-
108publ173/pdf/PLAW-108publ173.pdf>.
—. "Patient Protection and Affordable Care Act." United States Public Law . Washington: GPO, 2010.