
Kristi Kuper, PharmD, BCPS Clinical Director, Infectious Diseases ...

Patricia Louzon, PharmD, BCPS
Clinical Manager, Critical Care and ED Services
Florida Hospital Orlando
Clinical Assistant Professor, University of Florida College of Pharmacy

Discuss evidence based practice for the pharmacologic management of pain, agitation and delirium

78 y/o F admitted from a skilled nursing facility with shortness of breath, cough and fever
PMH: COPD, HTN, CAD, pneumonia
Admitted for suspected pneumonia
Intubated due to worsening respiratory status
Initial pain/agitation/delirium regimen
◦ Midazolam 2mg/hr, titrate to RASS -1 to -2
◦ Morphine 1mg IV q8h PRN pain

Questions:
◦ Is this an appropriate initial regimen for the patient?
Why?
Is there enough information to decide?
What other factors should we look for?
What are some alternatives?
◦ How should her pain and sedation level be assessed?
◦ How should her sedation be titrated?
◦ What other strategies should be employed?

2013 Clinical Practice Guidelines for Adult Patients in the ICU
◦ Pain and Analgesia
◦ Agitation and Sedation
◦ Delirium
Components interrelated
Crit Care Med. 2013 Jan;41(1):263-306.
Delirium

Incidence
◦ ICU patients routinely experience pain
At rest
With routine ICU care
Increased in certain populations (ex post surgical)
Assessment
◦ Behavioral Pain Scale (BPS)
◦ Critical-Care Pain Observation Tool (CPOT)
◦ Vital signs should not be used alone for pain assessment
Crit Care Med. 2013 Jan;41(1):263-306.

Payen et al. Crit Care Med 2001;29(12):2258-63.

Gélinas et al. Am J Crit Care. 2006 Jul;15(4):420-7.

Opiates Onset(IV)
T 1/2 Metabolism Active Metabolites
Inter-mittentDosing
IV Infusion
Rates
Side Effects and Other Information
Fentanyl 1-2 min
2-4 hr Hepatic (CYP3A4/5)
None 25-100mcg IV
q0.5-1 hr
50-700mcg/hr
Less hypotension, accumulation with
hepatic impairment, chest wall rigidity
Hydro-morphone
5-15 min
2-3 hr Hepatic None 0.2-0.6mg IV
q1-2 hr
0.5-3 mg/hr
Accumulation with hepatic/renal
impairment, more potent thanmorphine
Morphine 5-10 min
3-4 hr Hepatic 6- and 3-glucuronide
2-4mg IV
q1-2 hr
2-30mg/hr
Accumulation with hepatic/renal impairment,
Histamine release
Crit Care Med. 2013 Jan;41(1):263-306.

Factors to consider
◦ Age
◦ Renal/hepatic function
◦ Pain level
◦ Is patient opioid tolerant or naïve?
Home pain medications
◦ Interval to schedule
◦ Sources of pain

All available IV opioids, when titrated to similar pain intensity endpoints, are equally effective
Optimal choice of opioid and dosing regimen for individual patient depends on many factors, including the drug’s pharmacokinetic and pharmacodynamic properties
Nonopioid analgesics may be used to decrease the amount of opioids administered
Crit Care Med. 2013 Jan;41(1):263-306.

Delirium

Incidence
◦ Agitation and anxiety occur frequently in critically ill patients
◦ Associated with adverse clinical outcomes
Assessment
◦ Richmond Agitation-Sedation Scale (RASS)
◦ Sedation-Agitation Scale (SAS)
Crit Care Med. 2013 Jan;41(1):263-306.

Sedation is a risk factor
◦ Cognitive impairment
◦ Delirium
◦ Post-ICU post traumatic stress disorder
Midazolam equivalent ≥ 100 mg/day (~4mg/hr)
Mean morphine equivalent ≥ 100mg/day (~4mg/hr)
% of ICU days on opiates is a protective factor!
Bienvenu O.J. Psychological Medicine 2013 (not yet published)

+4 Combative Overtly violent, immediate danger to self and/or staff.
+3 Very Agitated Pulls or removes tube(s) or catheters; aggressive
+2 Agitated Frequent non-purposeful movement, fights ventilator
+1 Restless Anxious, apprehensive, but not aggressive
0 Alert and calm
-1 Drowsy Awakens to voice with eye opening, eye contact (> 10 seconds).
-2 Light sedation Briefly awakens with eye contact to voice (< 10 seconds).
-3 Moderate sedation Movement or eye opening to voice (no eye contact).
-4 Deep sedation No response to voice, but movement or eye opening to physical stimulation
-5 Unarousable No response to voice or physical stimulation.
Ely et al. JAMA. 2003 Jun 11;289(22):2983-91.

Riket et al. Crit Care Med. 1999 Jul;27(7):1325-9.

Propofol(Diprivan®)
Dexmedetomidine(Precedex®)
Midazolam(Versed®)
Lorazepam(Ativan®)
Onset 10-50 sec immediate 1-3 min 5-20 min
Duration 3-10 min 6 min 1-3 hrs, longerwith drips
4-8 hrs, longer with drips
Dosing 5-50 mcg/kg/min 0.1-1 mcg/kg/hr 1-10 mg/hr 1-10 mg/hr
Side effects -Bradycardia-Hypotension-↑ triglycerides-Propofol infusion syndrome (PRIS)-metabolic acidosis, renal failure
-Hypotension-Bradycardia
-Respiratory depression-Delirium
-Respiratory depression-Delirium-Propylene glycol toxicity (vehicle)
Notes - Avoid in heart failure-1.1 calorie/mL due to lipid formula-Avoid long-term use
-Useful for sedative weaning-Can be used in non-intubated-Renewal q5days
- Accumulates in liver failure, duration of action longer
-High risk for delirium-Avoid high-dose, prolonged infusions due to propylene glycol

1) Maintain light sedation levels
2) Daily sedation interruption
3) Light sedation levels PLUS daily interruption
WHICH TO USE???

Lots of evidence!
Ligher sedation arms◦ Shorter duration of mechanical ventilation◦ No increase in clinicically significant physiologic stress (e.g.
myocardial ischemia) ◦ Less (or no change) in PTSD
Crit Care Med 1999; 27: 2609Lancet 2008: 371:126N Engl J Med 2000; 342:1471CHEST 1098; 114:834-6.
Crit Care Med 2007; 35: 365Anesth Analhg 1997; 85:971.Anesthesiology 1997; 86: 785-96Crit Care Med 2003; 830Nurse Crit Care 2007; 12:93.
Intensive Care Med 2006; 32: 93 Crit Care Med 2009; 37: 2527. Am J Respir CCM 2003; 168:1457Nurse Crit Care 2007; 12:93.

◦ Randomized, controlled trial, N=128
◦ Midazolam or propofol and morphine infusions
◦ Interrupted daily until patient responded or became agitated
◦ Restarted at HALF the previous rate if needed
◦ Intervention group had
Shorter duration of mechanical ventilation (4.9 vs 7.3, p=0.004)
Shorter length of stay in ICU (6.4 vs 9.9 days, p=0.02)
No difference in overall length of hospitalization
No difference in complications (self extubation)
Kress et al. N Engl J Med. 2000;342:1471-7.

Randomized, controlled trial, N=430
Protocolized sedation titrated to light sedation vs protocolizedwith daily interruption
If indicated, resumed at HALF the previous rate
◦ No differences
Duration of mechanical ventilation (both 7 days)
Length of stay in ICU (both 10 days)
Overall length of hospitalization (both 20 days)
◦ Interpretation: Addition of daily interruption did not change outcomes
Mehta et al. JAMA. 2012;308 (19):E1-E8.

Maintain light levels of sedation (RASS -1 to -2) unless there is a contraindication
Use EITHER light level of sedation or daily interruption
Nonbenzodiazepine sedatives (propofol or dexmedetomidine) preferred in mechanically ventilated patients
◦ Intermittent pushes alternative strategy to continuous sedation
Choice should be driven by:
1. Specific indications and sedation goals for each patient
2. The clinical pharmacology of the drug
3. Overall costs
Crit Care Med. 2013 Jan;41(1):263-306.

Some patients need deeper sedation!◦ Facilitate mechanical ventilation
Poor oxygenation
Aggressive ventilator settings
Oscillator
◦ Neuromuscular blockers
◦ High risk of self extubation or self harm
◦ History of drug and ethanol abuse

Delirium

Cardinal features◦ A disturbed level of consciousness (i.e., a reduced clarity of
awareness of the environment), with a reduced ability to focus, sustain, or shift attention
◦ Either a change in cognition (i.e., memory deficit, disorientation, language disturbance), or the development of a perceptual disturbance (i.e., hallucinations, delusions)
Subtypes◦ Hyperactive (agitated)◦ Hypoactive (calm or lethargic)
Assessment◦ CAM-ICU or ICDSC
American College of Critical Care Medicine. Crit Care Med. 2013 Jan;41(1):263-306.
Four baseline risk factors positively and significantly associated with the development of delirium in the ICU:
1. Preexisting dementia
2. History of hypertension
3. Alcoholism
4. High severity of illness at admission
Independent risk factors:
◦ Coma
◦ Benzodiazepine use
American College of Critical Care Medicine. Crit Care Med. 2013 Jan;41(1):263-306.

Varying study findings
Increased development of delirium 1-2
◦ Lorazepam shown to be an independent risk factor 2
Associated with longer delirium duration3
~20% less delirium in a population treated with dexmedetomidine than benzodiazepines in 2 studies 4,5
Other studies showed no relationship 6-8
1. Pandharipande P, et al. J Trauma 2008; 65:34–41 .2. Pandharipande P, et al. Anesthesiology 2006; 104:21–26. 3. Pisani et al. Crit Care Med 2209;37:1-7.4. Riker R et al. JAMA 2009; 301:489–499.5. Pandharipande P, et al. Crit Care 2010; 14:R38.6. Ouimet S. Intensive Care Med 2007; 33:66–73 .7. Lin S et al. J Crit Care 2008; 23: 372–379 .8. Van Rompeay. Crit Care 2009; 13:R77.

Use of different benzodiazepines◦ Midazolam vs. lorazepam
Studies not powered as primary analysis
Different patient populations
General consensus:◦ Potential association

Do any meds need to be
stopped or lowered?
• Especially consider sedatives
• Is patient on minimal amount necessary? – Daily sedation cessation– Targeted sedation plan
• Do sedatives need to be changed?
Toxic Situations• CHF, shock, dehydration• Deliriogenic meds (tight titration)• New organ failure (liver/kidney)
Hypoxemia
Infection/sepsis (nosocomial)
Immobilization
Nonpharm interventions• Hearing aids, glasses, reorient,
sleep protocols, music, noise control, ambulation
K+ or electrolyte problems
Devlin, J.

Haloperidol
(Haldol®)
Quetiapine
(Seroquel®)
Risperidone
(Risperdal®)
Olanzapine
(Zyprexa®)
Ziprasidone
(Geodon®)
Peak Plasma
Time
2-6 hr (PO)
10-20 mins
(IM)
1.5 hr (IR)
6 hr (XR)
1 hr 6 hr (PO)
15-45 mins (short-
acting IM)
7 days (ER- IM)
6-8 hr (PO)
≤ 60 mins (IM)
Half Life 18 hr
3 weeks
(decanoate)
6 hr (IR)
7 hr (XR)
20 hr (PO)
3-6 days (IM)
21-54 hr (IR)
30 days (ER Injection)
7 hr (PO)
2-5 hr (IM)
Dosing 1-5 mg q4-6h 50 mg PO BID 1 mg PO BID 2.5 - 5 mg PO Qday 10 mg IM q2h or 20
mg q4h
Side effects:
QT
prolongation
IV/high doses-
high
PO-Low
Low-to-
Moderate
Low Low Moderate
Anti-
cholinergic
low Low
Dry mouth
rare low rare
Sedation low moderate low moderate low
EPS highest rare moderate low low
Weight gain low moderate moderate highest rare
Notes - Can dose
based on 25%
of bolus doses
required
-Metabolic
changes
-Dyslipidemia
Hyperglycemia
-Can contribute to
delirium
-Renal/hepatic
dose adjustments
-Parkinsonism
-Metabolic changes
- Dyslipidemia
- Hyperglycemia
-IM x 3 days only
-Use with caution in
renal/hepatic
- Max dose
40mg/day

Prevention◦ Perform early mobilization◦ For patients at risk, infusions of dexmedetomidine rather
than benzodiazepines may be associated with lower prevalence No recommendations for use
◦ No recommendation for using a pharmacologic delirium prevention protocol
Treatment◦ No published evidence that treatment with haloperidol
reduces duration of delirium in ICU patients◦ Atypical antipsychotics may reduce the duration of delirium
American College of Critical Care Medicine. Crit Care Med. 2013 Jan;41(1):263-306.

Delirium

Early mobilization
Promoting sleep by optimizing patients’ environments
Provider education
Use of protocols and order forms
Quality ICU rounds checklists to facilitate the use of pain, agitation, and delirium guidelines or protocols◦ Aim for a light target level of sedation in mechanically
ventilated patients
◦ Analgesia-first sedation use
American College of Critical Care Medicine. Crit Care Med. 2013 Jan;41(1):263-306.

Implement CAM-ICU screening twice daily
Change to CPOT pain assessment
Pharmacy and interdisciplinary involvement
ABCDE Bundle Rounds
PAD order set trial

Education to RN’s and pharmacy by MD and pharmacist
◦ Daily energizers
◦ Staff meetings
◦ One on one with each included patient
◦ One on one to day and night shift
◦ During interdisciplinary rounds
Daily screening (weekday) of 40 MICU/CCU patients by MD and pharmacist for order set use
Paper orders scanned to pharmacy
Edits to order set periodically based on nursing and physician feedback
Louzon et al. Critical Care Medicine 2013;41(12)suppl.

Retrospective case control study
Primary outcome endpoints:◦ Time on continuous sedation (hours)
Secondary outcome endpoints:◦ Total sedation usage (measured as number of sedative drips
removed from automated dispensing cabinet for patient)
◦ ICU length of stay
◦ Ventilator length of stay (hours)
◦ Re-intubation rates (yes/no)
Louzon et al. Critical Care Medicine 2013;41(12)suppl.

Inclusion◦ Order set utilized (study group) between October 1, 2012 and
March 15, 2013 OR
◦ Continuous infusion midazolam and fentanyl for > 24 hours in 5800 unit
Louzon et al. Critical Care Medicine 2013;41(12)suppl.

Exclusion Criteria◦ Age <18
◦ Prisoners
◦ Palliative Care/ terminal condition (cancer, end stage heart disease)
◦ Receiving neuromuscular blockers at time sedation
◦ Chronic respiratory failure prior to admission
◦ Continuous sedation used for < 24 hours
Louzon et al. Critical Care Medicine 2013;41(12)suppl.

• Similar baseline characteristics
Age
(mean)
History
Etoh/drug
use/psych/
dementia
n (%)
FiO2
(mean)
PEEP
(mean)
On one
pressor
PRN
sedation
used prior
to starting
pilot
Control
n=3556.5 6 (17) 45 6.2 16 (46) 22 (63)
Intervention
n=3568.4 7 (20) 40 5.6 12 (34) 14 (40)
p value 0.002 0.758 0.063 0.120 0.329 0.056
Louzon et al. Critical Care Medicine 2013;41(12)suppl.
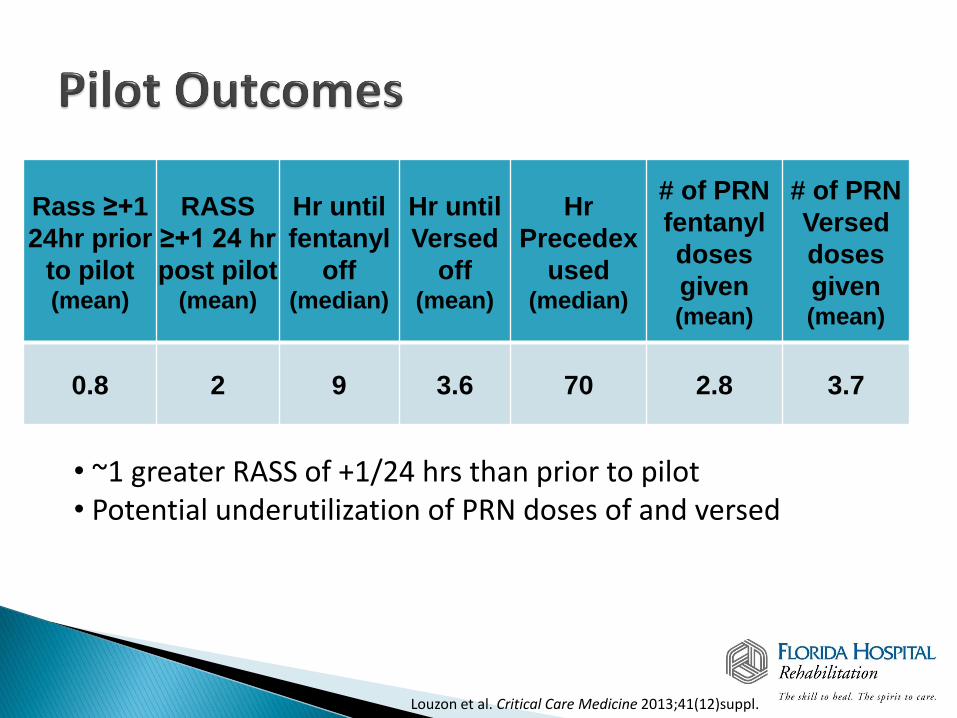
Rass ≥+1
24hr prior
to pilot(mean)
RASS
≥+1 24 hr
post pilot(mean)
Hr until
fentanyl
off (median)
Hr until
Versed
off (mean)
Hr
Precedex
used (median)
# of PRN
fentanyl
doses
given(mean)
# of PRN
Versed
doses
given(mean)
0.8 2 9 3.6 70 2.8 3.7
• ~1 greater RASS of +1/24 hrs than prior to pilot• Potential underutilization of PRN doses of and versed
Louzon et al. Critical Care Medicine 2013;41(12)suppl.

• 100 Less hours on sedation• 15 Less total sedation drips dispensed• 4.6 Less benzodiazepine drips dispensed• All p values significant
Hrs on
sedation(mean)
Total # drips
dispensed(mean)
# Benzo drips
dispensed(mean)
Control
n=35252.2 27.6 7.3
Intervention
n=35150.3 12.6 2.7
p value 0.0025 <0.001 0.0029
Louzon et al. Critical Care Medicine 2013;41(12)suppl.

ICU LOS (mean days)
Vent LOS (median days)
Reintubatedn (%)
Mortalityn (%)
Controln=35
16.5 8.56 5 (14) 9 (26)
Interventionn=35
11.5 7.38 3 (9) 8 (23)
p value 0.011 0.07 0.452 0.78
•ICU LOS- 5 days shorter•Vent LOS- 1.18 days shorter•Similar reintubation rates and mortality
Louzon et al. Critical Care Medicine 2013;41(12)suppl.

Sedation use decreased
Time on continuous sedation decreased
Decrease in ICU LOS
Louzon et al. Critical Care Medicine 2013;41(12)suppl.

Single way to order sedation regimens
Components:◦ Target RASS -1 to -2◦ Sedation vacation◦ Pain first!◦ Sedation duration expected <72 hours
Non-benzodiazepine strategies◦ Sedation duration expected >72 hours
Consider non-benzodiazepines
Benzodiazepine intermittent dosing preferred
Midazolam preferred to lorazepam
Continuous infusions for select patients only

Integrated Approach to
PADMD Champion
RN Champion
RT Champion
PharmacyChampion
PhysicalTherapy
Champion
HospitalAdministrators
Family
Patient
Courtesy J Barr, MD

Keys to Success
4 E’s◦ Engage
◦ Educate
◦ Execute
◦ Evaluate
Johns Hopkins Critical Care Rehab conference, 2013

Engage/ stimulate interest!
◦ Nurse educator
◦ Physician champions
◦ Grand rounds and faculty meetings
Educate
◦ New sedation protocol, RASS, CAM-ICU
◦ Nursing- lectures, one-on-one, case studies, quiz
◦ Physicians- pocket card

Execute
◦ New sedation protocol
◦ Nurse report Cam-ICU, RASS goal, and RASS scores at rounds
◦ Move to CPOT pain assessment
Evaluate
◦ Monthly barrier review by team
◦ MICU pharmacist feedback at rounds (protocol adherence, delirium management)
◦ Audit RASS and CAM-ICU documentation

78 y/o F admitted from a skilled nursing facility with shortness of breath, cough and fever
PMH: COPD, HTN, CAD, pneumonia
Admitted for suspected pneumonia
Intubated due to worsening respiratory status
Initial pain/agitation/delirium regimen◦ Midazolam 2mg/hr, titrate to RASS -1 to -2
◦ Morphine 1mg IV q8h PRN pain

Questions:
◦ Is this an appropriate initial regimen for the patient?
Why?
What are some alternatives?
◦ How should her pain and sedation level be assessed?
◦ How should her sedation be titrated?
◦ What other strategies should be employed?

Patricia Louzon, PharmD, BCPS
Clinical Manager, Critical Care and ED Services
Florida Hospital Orlando
Clinical Assistant Professor, University of Florida College of Pharmacy




![Teresa M. [Breslin] DeLellis, PharmD, BCPS, BCGPatomalliance.org/.../2019/01/DeLellis_CV_11_2018.pdf · DeLellis 1 Teresa M. [Breslin] DeLellis, PharmD, BCPS, BCGP 1021 Woodland Pass](https://static.fdocuments.us/doc/165x107/5fba322bc915c30e9e04ab57/teresa-m-breslin-delellis-pharmd-bcps-delellis-1-teresa-m-breslin-delellis.jpg)













