Patient Referral Form - Cardio Study
1
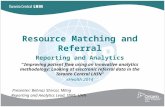
Patient Referral Form PATIENT INFORMATION / LABEL CARDIAC INVESTIGATIONS Last Name: First Name: Postal Code Work Date of Birth ( dd / mm / yyyy ) : Phone (home) Health Card # CLINICAL INFORMATION / INDICATIONS 2D ECHO AND COLOUR DOPPLER 12 LEAD ECG TREADMILL STRESS ECHO HOLTER MONITORING 48 HOURS 72 HOURS 14 DAYS 24 HOUR AMBULATORY BLOOD PRESSURE MONITORING (NOT COVERED BY OHIP) Sex: M F City Address VC / / 187 ST. CLAIR AVENUE WEST 2nd Floor TORONTO, ON M4V 1P7 Tel: 416-922-8535 Fax: 416-922-8787 ● ● Please complete form and fax to: 416-922-8787 LDS will contact the patient to schedule appointment. CARDIOLOGY CONSULT SouthWest block of Avenue Rd. and St Clair Ave. W. PHYSICIAN INFORMATION Referring Physician: Referring #: Phone: Fax: Signature: Date: Avenue Rd. St. Clair Ave. W Heath St. W Oriole Rd. Forest Hill Rd. Discontinuation of beta blockers and calcium blockers improves the diagnostic accuracy of exercise tests, but should only be done on the advice of the referring physician Patients should bring their LIST OF MEDICATIONS and HEALTH CARD with them 1st Available Dr. A. Crean MD, MRCP (UK) Dr. Z. Sasson MD, FRCP(C) Dr. S. Tandon MD, FRCP(C) Dr. T. Vakani MD, FRCP(C) INTERNAL MEDICINE CONSULT Dr. E. Bekier MD, FRCP(C) NOTES OR
Transcript of Patient Referral Form - Cardio Study

Patient Referral Form
PATIENT INFORMATION / LABEL
CARDIAC INVESTIGATIONS
LastName:
FirstName:
Postal Code
Work
Date of Birth ( dd / mm / yyyy ) :
Phone (home)
Health Card #
CLINICAL INFORMATION / INDICATIONS
2D ECHO AND COLOUR DOPPLER
12 LEAD ECG
TREADMILL STRESS ECHO
HOLTER MONITORING 48 HOURS 72 HOURS 14 DAYS
24 HOUR AMBULATORY BLOOD PRESSURE
MONITORING (NOT COVERED BY OHIP)
Sex: M F
City
Address
VC
/ /
187 ST. CLAIR AVENUE WEST2nd FloorTORONTO, ON M4V 1P7 Tel: 416-922-8535 Fax: 416-922-8787
●
●
Please complete form and fax to: 416-922-8787 LDS will contact the patient to schedule appointment.
CARDIOLOGY CONSULT
SouthWest block of Avenue Rd. and St Clair Ave. W.
PHYSICIAN INFORMATION
Referring Physician: Referring #:
Phone: Fax:
Signature: Date:
Avenue Rd.
St. Clair Ave. W
Heath St. W
Oriole Rd.
Forest Hill Rd.
Discontinuation of beta blockers and calcium blockers improves the diagnostic accuracy of exercise tests, but should only be done on
the advice of the referring physician
Patients should bring their LIST OF MEDICATIONS and HEALTH CARD with them
1st Available Dr. A. Crean MD, MRCP (UK)
Dr. Z. Sasson MD, FRCP(C)
Dr. S. Tandon MD, FRCP(C)
Dr. T. Vakani MD, FRCP(C)
INTERNAL MEDICINE CONSULTDr. E. Bekier MD, FRCP(C)
NOTES
OR