![[2021]EWHC (QB) CaseNo: G90MA404 …](https://static.fdocuments.us/doc/165x107/618bcc54dc416d05cc58d0a6/2021ewhc-qb-caseno-g90ma404-.jpg)
Patient Name: Jones, Melvin Accession / CaseNo: Discovery ... › sites › default › files ›...
9
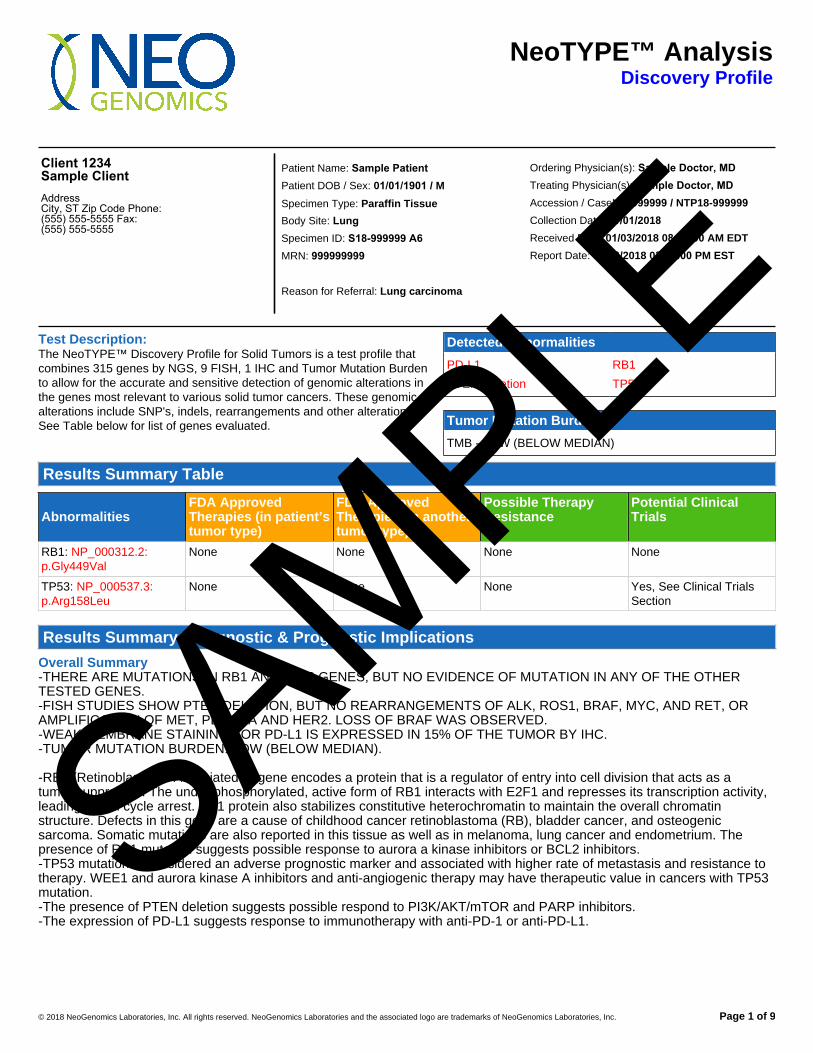
© 2018 NeoGenomics Laboratories, Inc. All rights reserved. NeoGenomics Laboratories and the associated logo are trademarks of NeoGenomics Laboratories, Inc. Page 1 of 9 NeoTYPE™ Analysis Discovery Profile Client 1234 Sample Client Address City, ST Zip Code Phone: (555) 555-5555 Fax: (555) 555-5555 Ordering Physician(s): Sample Doctor, MD Treating Physician(s): Sample Doctor, MD Accession / CaseNo: 999999 / NTP18-999999 Collection Date: 01/01/2018 Received Date: 01/03/2018 08:00:00 AM EDT Report Date: 01/13/2018 03:00:00 PM EST Patient Name: Sample Patient Patient DOB / Sex: 01/01/1901 / M Specimen Type: Paraffin Tissue Body Site: Lung Specimen ID: S18-999999 A6 MRN: 999999999 Reason for Referral: Lung carcinoma Test Description: The NeoTYPE™ Discovery Profile for Solid Tumors is a test profile that combines 315 genes by NGS, 9 FISH, 1 IHC and Tumor Mutation Burden to allow for the accurate and sensitive detection of genomic alterations in the genes most relevant to various solid tumor cancers. These genomic alterations include SNP's, indels, rearrangements and other alterations. See Table below for list of genes evaluated. Detected Abnormalities PD-L1 PTEN Deletion RB1 TP53 Tumor Mutation Burden TMB - LOW (BELOW MEDIAN) Results Summary Table Abnormalities FDA Approved Therapies (in patient’s tumor type) FDA Approved Therapies (in another tumor type) Possible Therapy Resistance Potential Clinical Trials RB1: NP_000312.2: p.Gly449Val None None None None TP53: NP_000537.3: p.Arg158Leu None None None Yes, See Clinical Trials Section Results Summary / Diagnostic & Prognostic Implications Overall Summary -THERE ARE MUTATIONS IN RB1 AND TP53 GENES, BUT NO EVIDENCE OF MUTATION IN ANY OF THE OTHER TESTED GENES. -FISH STUDIES SHOW PTEN DELETION, BUT NO REARRANGEMENTS OF ALK, ROS1, BRAF, MYC, AND RET, OR AMPLIFICATION OF MET, PDGFRA AND HER2. LOSS OF BRAF WAS OBSERVED. -WEAK MEMBRANE STAINING FOR PD-L1 IS EXPRESSED IN 15% OF THE TUMOR BY IHC. -TUMOR MUTATION BURDEN: LOW (BELOW MEDIAN). -RB1 (Retinoblastoma-Associated 1) gene encodes a protein that is a regulator of entry into cell division that acts as a tumor suppressor. The under phosphorylated, active form of RB1 interacts with E2F1 and represses its transcription activity, leading to cell cycle arrest. RB1 protein also stabilizes constitutive heterochromatin to maintain the overall chromatin structure. Defects in this gene are a cause of childhood cancer retinoblastoma (RB), bladder cancer, and osteogenic sarcoma. Somatic mutations are also reported in this tissue as well as in melanoma, lung cancer and endometrium. The presence of RB1 mutation suggests possible response to aurora a kinase inhibitors or BCL2 inhibitors. -TP53 mutation is considered an adverse prognostic marker and associated with higher rate of metastasis and resistance to therapy. WEE1 and aurora kinase A inhibitors and anti-angiogenic therapy may have therapeutic value in cancers with TP53 mutation. -The presence of PTEN deletion suggests possible respond to PI3K/AKT/mTOR and PARP inhibitors. -The expression of PD-L1 suggests response to immunotherapy with anti-PD-1 or anti-PD-L1. SAMPLE
Transcript of Patient Name: Jones, Melvin Accession / CaseNo: Discovery ... › sites › default › files ›...
Patient Name: Jones, Melvin
Patient DOB / Sex: 09/17/1954 / M
Accession / CaseNo: 1633870 / NTP18-008868
© 2018 NeoGenomics Laboratories, Inc. All rights reserved. NeoGenomics Laboratories and the associated logo are trademarks of NeoGenomics Laboratories, Inc. Page 1 of 9
NeoTYPE™ AnalysisDiscovery Profile
Client 1234Sample ClientAddressCity, ST Zip Code Phone: (555) 555-5555 Fax: (555) 555-5555
Ordering Physician(s): Sample Doctor, MD Treating Physician(s): Sample Doctor, MD Accession / CaseNo: 999999 / NTP18-999999 Collection Date: 01/01/2018Received Date: 01/03/2018 08:00:00 AM EDT Report Date: 01/13/2018 03:00:00 PM EST
Patient Name: Sample Patient Patient DOB / Sex: 01/01/1901 / M Specimen Type: Paraffin Tissue Body Site: LungSpecimen ID: S18-999999 A6MRN: 999999999
Reason for Referral: Lung carcinoma
Test Description:The NeoTYPE™ Discovery Profile for Solid Tumors is a test profile thatcombines 315 genes by NGS, 9 FISH, 1 IHC and Tumor Mutation Burdento allow for the accurate and sensitive detection of genomic alterations inthe genes most relevant to various solid tumor cancers. These genomicalterations include SNP's, indels, rearrangements and other alterations.See Table below for list of genes evaluated.
Detected Abnormalities
PD-L1
PTEN Deletion
RB1
TP53
Tumor Mutation Burden
TMB - LOW (BELOW MEDIAN)
Results Summary Table
AbnormalitiesFDA ApprovedTherapies (in patient’stumor type)
FDA ApprovedTherapies (in anothertumor type)
Possible TherapyResistance
Potential ClinicalTrials
RB1: NP_000312.2:p.Gly449Val
None None None None
TP53: NP_000537.3:p.Arg158Leu
None None None Yes, See Clinical TrialsSection
Results Summary / Diagnostic & Prognostic Implications
Overall Summary-THERE ARE MUTATIONS IN RB1 AND TP53 GENES, BUT NO EVIDENCE OF MUTATION IN ANY OF THE OTHERTESTED GENES.-FISH STUDIES SHOW PTEN DELETION, BUT NO REARRANGEMENTS OF ALK, ROS1, BRAF, MYC, AND RET, ORAMPLIFICATION OF MET, PDGFRA AND HER2. LOSS OF BRAF WAS OBSERVED.-WEAK MEMBRANE STAINING FOR PD-L1 IS EXPRESSED IN 15% OF THE TUMOR BY IHC.-TUMOR MUTATION BURDEN: LOW (BELOW MEDIAN).
-RB1 (Retinoblastoma-Associated 1) gene encodes a protein that is a regulator of entry into cell division that acts as atumor suppressor. The under phosphorylated, active form of RB1 interacts with E2F1 and represses its transcription activity,leading to cell cycle arrest. RB1 protein also stabilizes constitutive heterochromatin to maintain the overall chromatinstructure. Defects in this gene are a cause of childhood cancer retinoblastoma (RB), bladder cancer, and osteogenicsarcoma. Somatic mutations are also reported in this tissue as well as in melanoma, lung cancer and endometrium. Thepresence of RB1 mutation suggests possible response to aurora a kinase inhibitors or BCL2 inhibitors.-TP53 mutation is considered an adverse prognostic marker and associated with higher rate of metastasis and resistance totherapy. WEE1 and aurora kinase A inhibitors and anti-angiogenic therapy may have therapeutic value in cancers with TP53mutation.-The presence of PTEN deletion suggests possible respond to PI3K/AKT/mTOR and PARP inhibitors.-The expression of PD-L1 suggests response to immunotherapy with anti-PD-1 or anti-PD-L1.
SAMPLE

Patient Name: Sample PatientPatient DOB / Sex: 01/01/1901 MAccession / CaseNo: 9999999 / NTP18-999999
© 2018 NeoGenomics Laboratories, Inc. All rights reserved. NeoGenomics Laboratories and the associated logo are trademarks of NeoGenomics Laboratories, Inc. Page 2 of 9
Clinical SignificanceThe NeoTYPE™ Discovery Profile for Solid Tumors is a test profile that combines 315 genes by NGS, 9 FISH, 1 IHC andTumor Mutation Burden to allow for the accurate and sensitive detection of genomic alterations in the genes most relevant tovarious solid tumor cancers. These genomic alterations include SNP's, indels, rearrangements and other alterations. Testingcan aid in the diagnosis of various diseases and provide information to develop strategies for the treatment and managementof the underlying disease. In addition, the results obtained from the NeoTYPE™ Discovery Profile for Solid Tumors can alsobe used in current or future clinical research projects.Studies in lung cancer, melanoma and bladder cancers showed that objective response to checkpoint immunotherapy waspredicted by the presence of high Tumor Mutation Burden (TMB). It is currently believed that other types of tumors may alsoshow the same trend. In lung cancer patients, high nonsynonymous burden (defined as above the median in lung cancer)experienced higher rate of durable clinical benefits, objective response, and progression free survival. High TMB is definedas higher than median or upper third. However, cut-off might vary dependent on the type of tumor.In lung cancer, there is no correlation between PD-L1 expression and TMB. Patients with MSI usually show high TMB.
Therapeutic Implications
Drug SensitivityTP53 NP_000537.3:p.Arg158Leu: At present, there are no approved therapies targeting TP53 alterations, despite their highprevalence in cancer. Therapeutic approaches under investigation include gene therapy for TP53 and (dendritic cell-based)TP53 vaccines.Inhibition of components of the DNA damage checkpoint, including Checkpoint Kinase 1 (Chk1) and Wee1, has beenreported to enhance the activity of DNA-damaging agents in preclinical cancer models with deficiency of p53 function.Clinical trials of the Wee1 inhibitor MK-1775 are currently underway for patients with solid tumors and hematologicmalignancies.Studies have reported Aurora kinase A to be activated in cells harboring TP53 mutation, and Aurora kinase A and B inhibitorshave been reported to activate wild-type p53 in cellular assays; thus, tumors retaining a wild-type TP53 allele may benefitfrom Aurora kinase inhibitors.
Possible Therapy ResistanceTP53 NP_000537.3:p.Arg158Leu: Mutations in TP53 may increase resistance to ionizing radiation therapy.
Clinical Trials Information
NOTE: Although we make every attempt to ensure that the information provided is as accurate as possible, please notethat the information provided in this report has been obtained through public domains that are updated constantly andshould be researched by the physician or research professionals. NOT ALL TRIALS ARE INCLUDED. Please go towww.clinicaltrials.gov to perform a detailed search of available clinical trials as the trials provided in this report is not meant tobe a complete list.
Gene Trial ID Title Targets Phase Additional Information
RB1: None None None None None
TP53: NCT02576444 OLAParib COmbinations AKT, ATR,MTOR,mTORC1,mTORC2,PARP,RPS6KB1,WEE1
Phase 2 http://clinicaltrials.gov/show/NCT02576444
TP53: NCT02448589 An Investigation of TAS-119Monotherapy and in CombinationWith Docetaxel
Aurora kinase A Phase 1 http://clinicaltrials.gov/show/NCT02448589
TP53: NCT02134067 Dose-escalating, Safety,Tolerability and PK Study ofTAS-119 in Combination WithPaclitaxel in Patients WithAdvanced Solid Tumors
Aurora kinase A Phase 1 http://clinicaltrials.gov/show/NCT02134067SAMPLE
Patient Name: Sample PatientPatient DOB / Sex: 01/01/1901 MAccession / CaseNo: 9999999 / NTP18-999999
© 2018 NeoGenomics Laboratories, Inc. All rights reserved. NeoGenomics Laboratories and the associated logo are trademarks of NeoGenomics Laboratories, Inc. Page 3 of 9
Gene Trial ID Title Targets Phase Additional Information
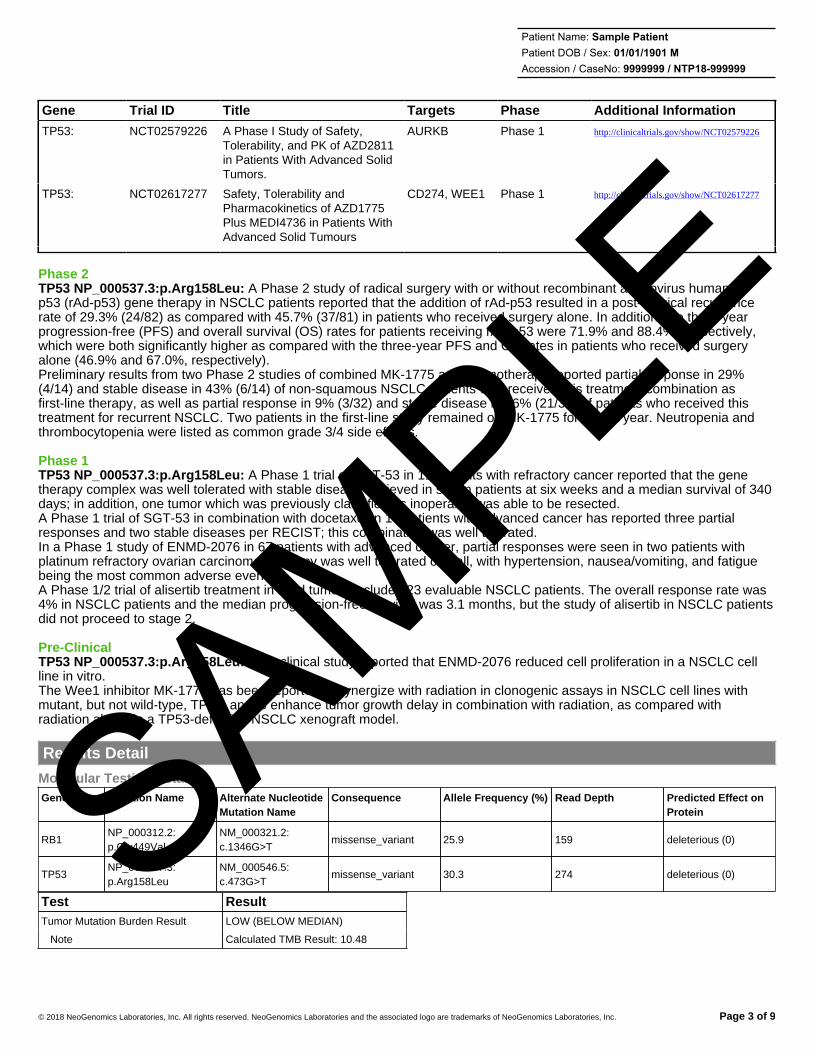
TP53: NCT02579226 A Phase I Study of Safety,Tolerability, and PK of AZD2811in Patients With Advanced SolidTumors.
AURKB Phase 1 http://clinicaltrials.gov/show/NCT02579226
TP53: NCT02617277 Safety, Tolerability andPharmacokinetics of AZD1775Plus MEDI4736 in Patients WithAdvanced Solid Tumours
CD274, WEE1 Phase 1 http://clinicaltrials.gov/show/NCT02617277
Phase 2TP53 NP_000537.3:p.Arg158Leu: A Phase 2 study of radical surgery with or without recombinant adenovirus humanp53 (rAd-p53) gene therapy in NSCLC patients reported that the addition of rAd-p53 resulted in a post-surgical recurrencerate of 29.3% (24/82) as compared with 45.7% (37/81) in patients who received surgery alone. In addition, the three-yearprogression-free (PFS) and overall survival (OS) rates for patients receiving rAd-p53 were 71.9% and 88.4%, respectively,which were both significantly higher as compared with the three-year PFS and OS rates in patients who received surgeryalone (46.9% and 67.0%, respectively).Preliminary results from two Phase 2 studies of combined MK-1775 and chemotherapy reported partial response in 29%(4/14) and stable disease in 43% (6/14) of non-squamous NSCLC patients who received this treatment combination asfirst-line therapy, as well as partial response in 9% (3/32) and stable disease in 66% (21/32) of patients who received thistreatment for recurrent NSCLC. Two patients in the first-line study remained on MK-1775 for over a year. Neutropenia andthrombocytopenia were listed as common grade 3/4 side effects.
Phase 1TP53 NP_000537.3:p.Arg158Leu: A Phase 1 trial of SGT-53 in 11 patients with refractory cancer reported that the genetherapy complex was well tolerated with stable disease achieved in seven patients at six weeks and a median survival of 340days; in addition, one tumor which was previously classified as inoperable was able to be resected.A Phase 1 trial of SGT-53 in combination with docetaxel in 14 patients with advanced cancer has reported three partialresponses and two stable diseases per RECIST; this combination was well tolerated.In a Phase 1 study of ENMD-2076 in 67 patients with advanced cancer, partial responses were seen in two patients withplatinum refractory ovarian carcinoma. Therapy was well tolerated overall, with hypertension, nausea/vomiting, and fatiguebeing the most common adverse events.A Phase 1/2 trial of alisertib treatment in solid tumors included 23 evaluable NSCLC patients. The overall response rate was4% in NSCLC patients and the median progression-free survival was 3.1 months, but the study of alisertib in NSCLC patientsdid not proceed to stage 2.
Pre-ClinicalTP53 NP_000537.3:p.Arg158Leu: A preclinical study reported that ENMD-2076 reduced cell proliferation in a NSCLC cellline in vitro.The Wee1 inhibitor MK-1775 has been reported to synergize with radiation in clonogenic assays in NSCLC cell lines withmutant, but not wild-type, TP53, and to enhance tumor growth delay in combination with radiation, as compared withradiation alone, in a TP53-defective NSCLC xenograft model.
Results Detail
Molecular Testing Detail:Gene name Mutation Name Alternate Nucleotide
Mutation NameConsequence Allele Frequency (%) Read Depth Predicted Effect on
Protein
RB1NP_000312.2:p.Gly449Val
NM_000321.2:c.1346G>T
missense_variant 25.9 159 deleterious (0)
TP53NP_000537.3:p.Arg158Leu
NM_000546.5:c.473G>T
missense_variant 30.3 274 deleterious (0)
Test ResultTumor Mutation Burden Result LOW (BELOW MEDIAN)
Note Calculated TMB Result: 10.48
SAMPLE
Patient Name: Sample PatientPatient DOB / Sex: 01/01/1901 MAccession / CaseNo: 9999999 / NTP18-999999
© 2018 NeoGenomics Laboratories, Inc. All rights reserved. NeoGenomics Laboratories and the associated logo are trademarks of NeoGenomics Laboratories, Inc. Page 4 of 9
FISH Testing Detail:Test Results ISCN Data
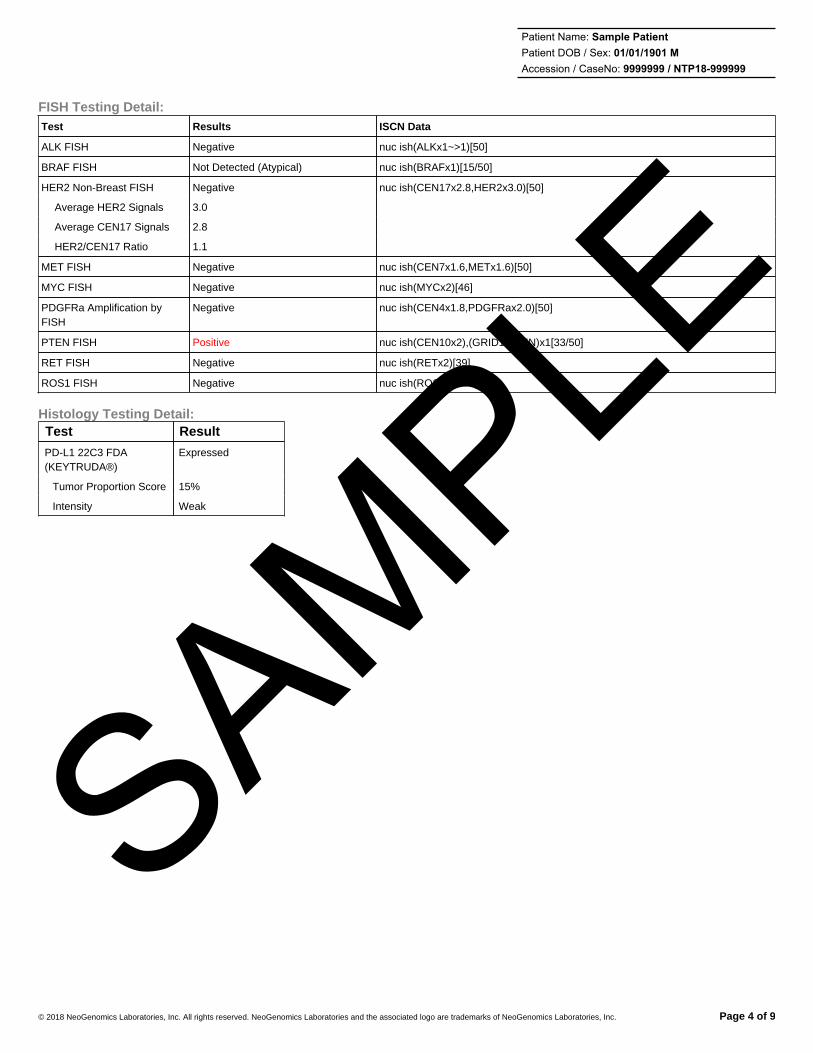
ALK FISH Negative nuc ish(ALKx1~>1)[50]
BRAF FISH Not Detected (Atypical) nuc ish(BRAFx1)[15/50]
HER2 Non-Breast FISH Negative nuc ish(CEN17x2.8,HER2x3.0)[50]
Average HER2 Signals 3.0
Average CEN17 Signals 2.8
HER2/CEN17 Ratio 1.1
MET FISH Negative nuc ish(CEN7x1.6,METx1.6)[50]
MYC FISH Negative nuc ish(MYCx2)[46]
PDGFRa Amplification byFISH
Negative nuc ish(CEN4x1.8,PDGFRax2.0)[50]
PTEN FISH Positive nuc ish(CEN10x2),(GRID1,PTEN)x1[33/50]
RET FISH Negative nuc ish(RETx2)[39]
ROS1 FISH Negative nuc ish(ROS1x1~>1)[50]
Histology Testing Detail:Test Result
PD-L1 22C3 FDA(KEYTRUDA®)
Expressed
Tumor Proportion Score 15%
Intensity Weak
SAMPLE

Patient Name: Sample PatientPatient DOB / Sex: 01/01/1901 MAccession / CaseNo: 9999999 / NTP18-999999
© 2018 NeoGenomics Laboratories, Inc. All rights reserved. NeoGenomics Laboratories and the associated logo are trademarks of NeoGenomics Laboratories, Inc. Page 5 of 9
Genes Evaluated (by molecular analysis unless otherwise noted)
ABL1 ABL2 ACVR1B AKT1 AKT2 AKT3 ALK ALK FISHAMER1(FAM123B)
APC AR
ARAF ARFRP1 ARID1A ARID1B ARID2 ASXL1 ATM ATR ATRX AURKA AURKB
AXIN1 AXL BAP1 BARD1 BCL2 BCL2L1 BCL2L2 BCL6 BCOR BCORL1 BLM
BRAF BRAF FISH BRCA1 BRCA2 BRD4 BRIP1 BTG1 BTKC11orf30(EMSY)
CARD11 CBFB
CBL CCND1 CCND2 CCND3 CCNE1 CD274 CD79A CD79B CDC73 CDH1 CDK12
CDK4 CDK6 CDK8 CDKN1A CDKN1B CDKN2A CDKN2B CDKN2C CEBPA CHD2 CHD4
CHEK1 CHEK2 CIC CREBBP CRKL CRLF2 CSF1R CTCF CTNNA1 CTNNB1 CUL3
CYLD DAXX DDR2 DICER1 DNMT3A DOT1L EGFR EP300 EPHA3 EPHA5 EPHA7
EPHB1 ERBB2 ERBB3 ERBB4 ERG ERRF11 ESR1 EZH2 FAM46C FANCA FANCC
FANCD2 FANCE FANCF FANCG FANCL FAS FAT1 FBXW7 FGF10 FGF14 FGF19
FGF23 FGF3 FGF4 FGF6 FGFR1 FGFR2 FGFR3 FGFR4 FH FLCN FLT1
FLT3 FLT4 FOXL2 FOXP1 FRS2 FUBP1 GABRA6 GATA1 GATA2 GATA3 GATA4
GATA6GID4(C17orf39)
GLI1 GNA11 GNA13 GNAQ GNAS GPR124 GRIN2A GRM3 GSK3B
H3F3AHER2 NBFISH
HGF HNF1A HRAS HSD3B1 HSP90AA1 IDH1 IDH2 IGF1R IGF2
IKBKE IKZF1 IL7R INHBA INPP4B IRF2 IRF4 IRS2 JAK1 JAK2 JAK3
JUNKAT6A(MYST3)
KDM5A KDM5C KDM6A KDR KEAP1 KEL KIT KLHL6 KMT2A (MLL)
KMT2C(MLL3)
KMT2D(MLL2)
KRAS LMO1 LRP1B LYN LZTR1 MAGI2 MAP2K1 MAP2K2 MAP2K4
MAP3K1 MCL1 MDM2 MDM4 MED12 MEF2B MEN1 MET MET FISH MITF MLH1
MPL MRE11A MSH2 MSH6 MTOR MUTYH MYC MYC FISHMYCL(MYCL1)
MYCN MYD88
NF1 NF2 NFE2L2 NFKBIA NKX2-1 NOTCH1 NOTCH2 NOTCH3 NPM1 NRAS NSD1
NTRK1 NTRK2 NTRK3 NUP93 PAK3 PALB2 PARK2 PAX5 PBRM1 PDCD1LG2 PDGFRA
PDGFRa amp PDGFRa amp PDGFRB PDK1PD-L122C3 FDA(KEYTRUDA®)
PIK3C2B PIK3CA PIK3CB PIK3CG PIK3R1 PIK3R2
PLCG2 PMS2 POLD1 POLE PPP2R1A PRDM1 PREX2 PRKAR1A PRKCI PRKDC PRSS8
PTCH1 PTEN PTEN FISH PTPN11 QKI RAC1 RAD50 RAD51 RAF1 RANBP2 RARA
RB1 RBM10 RET RET FISH RICTOR RNF43 ROS1 ROS1 FISH RPTOR RUNX1 RUNX1T1
SDHA SDHB SDHC SDHD SETD2 SF3B1 SLIT2 SMAD2 SMAD3 SMAD4 SMARCA4
SMARCB1 SMO SNCAIP SOCS1 SOX10 SOX2 SOX9 SPEN SPOP SPTA1 SRC
STAG2 STAT3 STAT4 STK11 SUFU SYK TAF1 TBX3 TERCTERT(promoteronly)
TET2
TGFBR2 TNFAIP3 TNFRSF14 TOP1 TOP2A TP53 TSC1 TSC2 TSHRTumorMutationBurden
U2AF1
VEGFA VHL WISP3 WT1 XPO1 ZBTB2 ZNF217 ZNF703
MethodologyThe NeoTYPE™ Discovery Profile for Solid Tumors combines 315 genes by NGS, 9 FISH, 1 IHC and Tumor MutationBurden to allow for the accurate and sensitive detection of genomic alterations in the genes most relevant to various solidtumor cancers. These genomic alterations include SNP's, indels, rearrangements and other alterations. Testing can aid inthe diagnosis of various diseases and provide information to develop strategies for the treatment and management of theunderlying disease. In addition, the results obtained from the NeoTYPE™ Discovery Profile for Solid Tumors can also beused in current or future clinical research projects.Studies in lung cancer, melanoma and bladder cancers showed that objective response to checkpoint immunotherapy waspredicted by the presence of high Tumor Mutation Burden (TMB). It is currently believed that other types of tumors may alsoshow the same trend. In lung cancer patients, high nonsynonymous burden (defined as above the median in lung cancer)experienced higher rate of durable clinical benefits, objective response, and progression free survival. High TMB is definedas higher than median or upper third. However, cut-off might vary dependent on the type of tumor.In lung cancer, there is no correlation between PD-L1 expression and TMB. Patients with MSI usually show high TMB.SAMPLE

Patient Name: Sample PatientPatient DOB / Sex: 01/01/1901 MAccession / CaseNo: 9999999 / NTP18-999999
© 2018 NeoGenomics Laboratories, Inc. All rights reserved. NeoGenomics Laboratories and the associated logo are trademarks of NeoGenomics Laboratories, Inc. Page 6 of 9
Abnormal Biomarker Information
RB1 NP_000312.2:p.Gly449Val: The functional consequences of RB1-G449V are unknown.RB1 encodes the retinoblastoma protein (Rb), a tumor suppressor and negative regulator of the cell cycle. Loss of Rbfunction, which has been identified in many cancer types due to various mechanisms, results in the upregulation oftranscription and cell proliferation.Loss of RB1 has been associated with lack of response to Cdk4/6 inhibitors.At this time, there are no therapeutic options to target the inactivation of Rb. Preclinical studies are actively investigatingpossible therapies to address Rb inactivation, exploring avenues such as Aurora kinase inhibitors, Bcl-2 family inhibitors, andNotch pathway activation.As the alteration reported here has not been functionally characterized, the relevance of any available therapeuticapproaches is unknown.
TP53 NP_000537.3:p.Arg158Leu: TP53-R158L is an inactivating mutation.TP53 is a tumor suppressor that encodes the p53 protein; alterations in TP53 may result in a loss of p53 function, yet anincrease in the expression and stability of the mutant p53 protein in the nucleus, sometimes leading to oncogenic effects,including genomic instability and excessive cell proliferation.At present, there are no approved therapies targeting TP53 alterations, despite their high prevalence in cancer. Therapeuticapproaches under investigation include gene therapy for TP53 and (dendritic cell-based) TP53 vaccines.Tumors with TP53 mutations may be sensitive to the Wee1 inhibitor MK-1775, and clinical trials are currently underway forpatients with solid tumors and hematologic malignancies.Aurora kinase A inhibitors are another therapeutic approach under investigation for TP53-mutated cancers.
Molecular FunctionRB1 NP_000312.2:p.Gly449Val: RB1 G449V is a missense alteration within the A pocket domain of the Rb protein(UniProt).The Rb pocket domain, which consists of domain A and domain B, has been reported to be involved in the interaction of Rbwith several proteins, including adenovirus E1A, SV40 large T antigen, HPV E7, and E2F transcription factors.However, this alteration has not been reported (COSMIC, Nov 2017) or functionally characterized (PubMed, Nov 2017);therefore, its effect on protein function is unknown.
TP53 NP_000537.3:p.Arg158Leu: TP53 R158 in NM_000546 corresponds to R119 in another transcript (IntegrativeGenomics Viewer, v.2.3).TP53 R158L is a missense alteration located within the DNA-binding domain (DBD) of the p53 protein.DBD mutations are thought to result in loss of function via the loss of transactivation of p53-dependent genes.TP53 R158L has been reported to be an inactivating mutation that results in complete loss of p53 protein function.
IncidenceRB1 NP_000312.2:p.Gly449Val: RB1 mutations have been reported in 2.5% (36/1462) of Lung adenocarcinoma samplesanalyzed in COSMIC (Jun 2018).RB1 mutations have been reported in 0.0-6.2% of Lung adenocarcinoma samples (cBioPortal for Cancer Genomics, Jun2018).RB1 mutation has been reported in 6.5% (2/31) of NSCLC cases in one study, and a separate study detected RB1 mutationin 3.7% (7/188) of lung adenocarcinoma cases.
TP53 NP_000537.3:p.Arg158Leu: TP53 mutations have been reported in 32% (980/3040) of Lung adenocarcinomasamples analyzed in COSMIC (Jun 2018).TP53 mutations have been reported in 40-53% of Lung adenocarcinoma samples (cBioPortal for Cancer Genomics, Jun2018).TP53 is one of the most commonly mutated genes in lung cancer; scientific studies have reported TP53 mutations in 29-42%of non-small cell lung carcinoma (NSCLC) cases, with a higher incidence cited in tumors of the squamous cell carcinomasubtype as compared with the adenocarcinoma subtype.SAMPLE

Patient Name: Sample PatientPatient DOB / Sex: 01/01/1901 MAccession / CaseNo: 9999999 / NTP18-999999
© 2018 NeoGenomics Laboratories, Inc. All rights reserved. NeoGenomics Laboratories and the associated logo are trademarks of NeoGenomics Laboratories, Inc. Page 7 of 9
Role in DiseaseTP53 NP_000537.3:p.Arg158Leu: Loss of tumor suppressor p53, which is encoded by the TP53 gene, is common inaggressive advanced cancers.Carriers of a germline mutation in TP53 have Li-Fraumeni Syndrome, an inherited cancer syndrome resulting in multipletumors in early adulthood, including breast cancer, brain tumors, and leukemias.Expression of p53 in normal cells is low; however, TP53 alterations, including those that result in loss of p53 tumorsuppressor function, may lead to stabilization and increased expression of p53, particularly in the nucleus, and severalstudies have shown that it may have oncogenic gain-of-function effects.TP53 alterations are believed to be early events in NSCLC, preceding lymph node metastasis.TP53 mutation and expression of p53 have been correlated with the lung squamous cell carcinoma subtype, and p53expression in lung squamous cell carcinoma has also been associated with disease stage and higher grade tumors.
SAMPLE

Patient Name: Sample PatientPatient DOB / Sex: 01/01/1901 MAccession / CaseNo: 9999999 / NTP18-999999
© 2018 NeoGenomics Laboratories, Inc. All rights reserved. NeoGenomics Laboratories and the associated logo are trademarks of NeoGenomics Laboratories, Inc. Page 8 of 9
ReferencesAllaman-Pillet N, Oberson A, Munier F, Schorderet D The Bcl-2/Bcl-XL inhibitor ABT-737 promotes death of retinoblastoma cancer cells.
Bircan A, Bircan S, Kapucuoglu N, Songur N, Ozturk O, Akkaya A Maspin, VEGF and p53 expression in small biopsies of primary advanced lung cancer and relationship with clinicopathologic parameters.
Bridges K, Hirai H, Buser C, Brooks C, Liu H, Buchholz T, Molkentine J, Mason K, Meyn R MK-1775, a novel Wee1 kinase inhibitor, radiosensitizes p53-defective human tumor cells.
Brown C, Lain S, Verma C, Fersht A, Lane D Awakening guardian angels: drugging the p53 pathway.
Burkhart D, Sage J Cellular mechanisms of tumour suppression by the retinoblastoma gene.
Chang Y, Wu C, Shih J, Lee Y Comparison of p53 and epidermal growth factor receptor gene status between primary tumors and lymph node metastases in non-small cell lung cancers.
Dearth L, Qian H, Wang T, Baroni T, Zeng J, Chen S, Yi S, Brachmann R Inactive full-length p53 mutants lacking dominant wild-type p53 inhibition highlight loss of heterozygosity as an important aspect of p53status in human cancers.
Deng B, Sun T, Tang B, Tao S, Kang P, Qian K, Jiang B, Li K, Li K, Zhou J, Wang R, Tan Q Surgery combined with adenoviral p53 gene therapy for treatment of non-small cell lung cancer: a phase II study.
Diamond J, Bastos B, Hansen R, Gustafson D, Eckhardt S, Kwak E, Pandya S, Fletcher G, Pitts T, Kulikowski G, Morrow M, Arnott J, Bray M, Sidor C, Messersmith W, Shapiro G Phase I safety,pharmacokinetic, and pharmacodynamic study of ENMD-2076, a novel angiogenic and Aurora kinase inhibitor, in patients with advanced solid tumors.
Ding L, Getz G, Wheeler D, Mardis E, McLellan M, Cibulskis K, Sougnez C, Greulich H, Muzny D, Morgan M, Fulton L, Fulton R, Zhang Q, Wendl M, Lawrence M, Larson D, Chen K, Dooling D, Sabo A, HawesA, Shen H, Jhangiani S, Lewis L, Hall O, Zhu Y, Mathew T, Ren Y, Yao J, Scherer S, Clerc K, Metcalf G, Ng B, Milosavljevic A, Gonzalez-Garay M, Osborne J, Meyer R, Shi X, Tang Y, Koboldt D, Lin L, AbbottR, Miner T, Pohl C, Fewell G, Haipek C, Schmidt H, Dunford-Shore B, Kraja A, Crosby S, Sawyer C, Vickery T, Sander S, Robinson J, Winckler W, Baldwin J, Chirieac L, Dutt A, Fennell T, Hanna M, JohnsonB, Onofrio R, Thomas R, Tonon G, Weir B, Zhao X, Ziaugra L, Zody M, Giordano T, Orringer M, Roth J, Spitz M, Wistuba I, Ozenberger B, Good P, Chang A, Beer D, Watson M, Ladanyi M, Broderick S,Yoshizawa A, Travis W, Pao W, Province M, Weinstock G, Varmus H, Gabriel S, Lander E, Gibbs R, Meyerson M, Wilson R Somatic mutations affect key pathways in lung adenocarcinoma.
El-Deiry W The role of p53 in chemosensitivity and radiosensitivity.
Fletcher G, Brokx R, Denny T, Hembrough T, Plum S, Fogler W, Sidor C, Bray M ENMD-2076 is an orally active kinase inhibitor with antiangiogenic and antiproliferative mechanisms of action.
Fry D, Harvey P, Keller P, Elliott W, Meade M, Trachet E, Albassam M, Zheng X, Leopold W, Pryer N, Toogood P Specific inhibition of cyclin-dependent kinase 4/6 by PD 0332991 and associated antitumoractivity in human tumor xenografts.
Gorgoulis V, Zacharatos P, Kotsinas A, Liloglou T, Kyroudi A, Veslemes M, Rassidakis A, Halazonetis T, Field J, Kittas C Alterations of the p16-pRb pathway and the chromosome locus 9p21-22 in non-small-cell lung carcinomas: relationship with p53 and MDM2 protein expression.
Gully C, Velazquez-Torres G, Shin J, Fuentes-Mattei E, Wang E, Carlock C, Chen J, Rothenberg D, Adams H, Choi H, Guma S, Phan L, Chou P, Su C, Zhang F, Chen J, Yang T, Yeung S, Lee M Aurora Bkinase phosphorylates and instigates degradation of p53.
Herrera-Abreu M, Palafox M, Asghar U, Rivas M, Cutts R, Garcia-Murillas I, Pearson A, Guzman M, Rodriguez O, Grueso J, Bellet M, Cortés J, Elliott R, Pancholi S, Baselga J, Dowsett M, Martin L, Turner N,Serra V Early Adaptation and Acquired Resistance to CDK4/6 Inhibition in Estrogen Receptor-Positive Breast Cancer.
Hirai H, Arai T, Okada M, Nishibata T, Kobayashi M, Sakai N, Imagaki K, Ohtani J, Sakai T, Yoshizumi T, Mizuarai S, Iwasawa Y, Kotani H MK-1775, a small molecule Wee1 inhibitor, enhances anti-tumorefficacy of various DNA-damaging agents, including 5-fluorouracil.
Hook K, Garza S, Lira M, Ching K, Lee N, Cao J, Yuan J, Ye J, Ozeck M, Shi S, Zheng X, Rejto P, Kan J, Christensen J, Pavlicek A An integrated genomic approach to identify predictive biomarkers ofresponse to the aurora kinase inhibitor PF-03814735.
Houben R, Hesbacher S, Schmid C, Kauczok C, Flohr U, Haferkamp S, Müller C, Schrama D, Wischhusen J, Becker J High-level expression of wild-type p53 in melanoma cells is frequently associated withinactivity in p53 reporter gene assays.
Hu Q, Dyson N, Harlow E The regions of the retinoblastoma protein needed for binding to adenovirus E1A or SV40 large T antigen are common sites for mutations.
Joerger A, Fersht A Structural biology of the tumor suppressor p53.
Kalous O, Conklin D, Desai A, Dering J, Goldstein J, Ginther C, Anderson L, Lu M, Kolarova T, Eckardt M, Langerød A, Børresen-Dale A, Slamon D, Finn R AMG 900, pan-Aurora kinase inhibitor,preferentially inhibits the proliferation of breast cancer cell lines with dysfunctional p53.
Katayama H, Sen S Functional significance of Aurora kinase A regulatory interactions with p53-ERα complex in human breast cancer cells.
Kato S, Han S, Liu W, Otsuka K, Shibata H, Kanamaru R, Ishioka C Understanding the function-structure and function-mutation relationships of p53 tumor suppressor protein by high-resolution missensemutation analysis.
Kim Y, Hammerman P, Kim J, Yoon J, Lee Y, Sun J, Wilkerson M, Pedamallu C, Cibulskis K, Yoo Y, Lawrence M, Stojanov P, Carter S, McKenna A, Stewart C, Sivachenko A, Oh I, Kim H, Choi Y, Kim K,Shim Y, Kim K, Song S, Na K, Choi Y, Hayes D, Kim J, Cho S, Kim Y, Ahn J, Ahn M, Getz G, Meyerson M, Park K Integrative and comparative genomic analysis of lung squamous cell carcinomas in EastAsian patients.
Knudsen E, Knudsen K Tailoring to RB: tumour suppressor status and therapeutic response.
Knudsen E, Wang J Targeting the RB-pathway in cancer therapy.
Koga T, Hashimoto S, Sugio K, Yoshino I, Nakagawa K, Yonemitsu Y, Sugimachi K, Sueishi K Heterogeneous distribution of P53 immunoreactivity in human lung adenocarcinoma correlates with MDM2protein expression, rather than with P53 gene mutation.
Kratzke R, Greatens T, Rubins J, Maddaus M, Niewoehner D, Niehans G, Geradts J Rb and p16INK4a expression in resected non-small cell lung tumors.
Lee J, Russo A, Pavletich N Structure of the retinoblastoma tumour-suppressor pocket domain bound to a peptide from HPV E7.
Levine A p53, the cellular gatekeeper for growth and division.
Li Z, Sun Y, Chen X, Squires J, Nowroozizadeh B, Liang C, Huang J p53 Mutation Directs AURKA Overexpression via miR-25 and FBXW7 in Prostatic Small Cell Neuroendocrine Carcinoma.
Liu P, Morrison C, Wang L, Xiong D, Vedell P, Cui P, Hua X, Ding F, Lu Y, James M, Ebben J, Xu H, Adjei A, Head K, Andrae J, Tschannen M, Jacob H, Pan J, Zhang Q, Van den Bergh F, Xiao H, Lo K, PatelJ, Richmond T, Watt M, Albert T, Selzer R, Anderson M, Wang J, Wang Y, Starnes S, Yang P, You M Identification of somatic mutations in non-small cell lung carcinomas using whole-exome sequencing.
Ludovini V, Gregorc V, Pistola L, Mihaylova Z, Floriani I, Darwish S, Stracci F, Tofanetti F, Ferraldeschi M, Di Carlo L, Ragusa M, Daddi G, Tonato M Vascular endothelial growth factor, p53, Rb, Bcl-2expression and response to chemotherapy in advanced non-small cell lung cancer.
Ma C, Janetka J, Piwnica-Worms H Death by releasing the breaks: CHK1 inhibitors as cancer therapeutics.
Ma X, Rousseau V, Sun H, Lantuejoul S, Filipits M, Pirker R, Popper H, Mendiboure J, Vataire A, Le Chevalier T, Soria J, Brambilla E, Dunant A, Hainaut P Significance of TP53 mutations as predictivemarkers of adjuvant cisplatin-based chemotherapy in completely resected non-small-cell lung cancer.
Maeng C, Lee H, Kim Y, Choi M, Hong J, Jung H, Lee K, Kim H, Kwon O, Sun J, Ahn J, Park K, Um S, Ahn M High-throughput molecular genotyping for small biopsy samples in advanced non-small cell lungcancer patients.
Malkin D, Li F, Strong L, Fraumeni J, Nelson C, Kim D, Kassel J, Gryka M, Bischoff F, Tainsky M Germ line p53 mutations in a familial syndrome of breast cancer, sarcomas, and other neoplasms.
Marxer M, Ma H, Man W, Poon R p53 deficiency enhances mitotic arrest and slippage induced by pharmacological inhibition of Aurora kinases.
Mattioni M, Soddu S, Prodosmo A, Visca P, Conti S, Alessandrini G, Facciolo F, Strigari L Prognostic role of serum p53 antibodies in lung cancer.
Melichar B, Adenis A, Havel L, et al. Phase (Ph) I/II study of investigational Aurora A kinase (AAK) inhibitor MLN8237 (alisertib): Updated ph II results in patients (pts) with small cell lung cancer (SCLC), non-SCLC (NSCLC), breast cancer (BrC), head and neck squamous cell carcinoma (HNSCC), and gastroesophageal cancer (GE).
Melichar B, Adenis A, Lockhart A, Bennouna J, Dees E, Kayaleh O, Obermannova R, DeMichele A, Zatloukal P, Zhang B, Ullmann C, Schusterbauer C Safety and activity of alisertib, an investigational aurorakinase A inhibitor, in patients with breast cancer, small-cell lung cancer, non-small-cell lung cancer, head and neck squamous-cell carcinoma, and gastro-oesophageal adenocarcinoma: a five-arm phase 2study.
SAMPLE

Patient Name: Sample PatientPatient DOB / Sex: 01/01/1901 MAccession / CaseNo: 9999999 / NTP18-999999
© 2018 NeoGenomics Laboratories, Inc. All rights reserved. NeoGenomics Laboratories and the associated logo are trademarks of NeoGenomics Laboratories, Inc. Page 9 of 9
Michaud K, Solomon D, Oermann E, Kim J, Zhong W, Prados M, Ozawa T, James C, Waldman T Pharmacologic inhibition of cyclin-dependent kinases 4 and 6 arrests the growth of glioblastoma multiforme intracranial xenografts.
Miyasaka A, Oda K, Ikeda Y, Sone K, Fukuda T, Inaba K, Makii C, Enomoto A, Hosoya N, Tanikawa M, Uehara Y, Arimoto T, Kuramoto H, Wada-Hiraike O, Miyagawa K, Yano T, Kawana K, Osuga Y, Fujii T PI3K/mTOR pathway inhibition overcomes radioresistance via suppression of the HIF1-α/VEGF pathway in endometrial cancer.
Mogi A, Kuwano H TP53 mutations in nonsmall cell lung cancer.
Molina-Vila M, Bertran-Alamillo J, Gascó A, Mayo-de-las-Casas C, Sánchez-Ronco M, Pujantell-Pastor L, Bonanno L, Favaretto A, Cardona A, Vergnenègre A, Majem M, Massuti B, Morán T, Carcereny E, Viteri S, Rosell R Nondisruptive p53 mutations are associated with shorter survival in patients with advanced non-small cell lung cancer.
O'Leary B, Finn R, Turner N Treating cancer with selective CDK4/6 inhibitors.
Olivier M, Petitjean A, Marcel V, Pétré A, Mounawar M, Plymoth A, de Fromentel C, Hainaut P Recent advances in p53 research: an interdisciplinary perspective.
Pirollo K, Nemunaitis J, Leung P, Nunan R, Adams J, Chang E Safety and Efficacy in Advanced Solid Tumors of a Targeted Nanocomplex Carrying the p53 Gene Used in Combination with Docetaxel: A Phase 1b Study.
Saito H, Ando S, Morishita N, Lee K, Dator D, Dy D, Shigemura K, Adhim Z, Nibu K, Fujisawa M, Shirakawa T A combined lymphokine-activated killer (LAK) cell immunotherapy and adenovirus-p53 gene therapy for head and neck squamous cell carcinoma.
Santibáñez-Koref M, Birch J, Hartley A, Jones P, Craft A, Eden T, Crowther D, Kelsey A, Harris M p53 germline mutations in Li-Fraumeni syndrome.
Schuler P, Harasymczuk M, Visus C, Deleo A, Trivedi S, Lei Y, Argiris A, Gooding W, Butterfield L, Whiteside T, Ferris R Phase I dendritic cell p53 peptide vaccine for head and neck cancer.
Senzer N, Nemunaitis J, Nemunaitis D, Bedell C, Edelman G, Barve M, Nunan R, Pirollo K, Rait A, Chang E Phase I study of a systemically delivered p53 nanoparticle in advanced solid tumors.
Spigel DR, Dakhil S, Beck JT Phase II studies of AZD1775, a WEE1 kinase inhibitor, and chemotherapy in non-small-cell lung cancer (NSCLC): Lead-in cohort results
Srivastava S, Zou Z, Pirollo K, Blattner W, Chang E Germ-line transmission of a mutated p53 gene in a cancer-prone family with Li-Fraumeni syndrome.
Taylor-Harding B, Aspuria P, Agadjanian H, Cheon D, Mizuno T, Greenberg D, Allen J, Spurka L, Funari V, Spiteri E, Wang Q, Orsulic S, Walsh C, Karlan B, Wiedemeyer W Cyclin E1 and RTK/RAS signaling drive CDK inhibitor resistance via activation of E2F and ETS.
Tekpli X, Landvik N, Skaug V, Gulsvik A, Haugen A, Zienolddiny S Functional effect of polymorphisms in 15q25 locus on CHRNA5 mRNA, bulky DNA adducts and TP53 mutations.
Tentler J, Ionkina A, Tan A, Newton T, Pitts T, Glogowska M, Kabos P, Sartorius C, Sullivan K, Espinosa J, Eckhardt S, Diamond J p53 Family Members Regulate Phenotypic Response to Aurora Kinase A Inhibition in Triple-Negative Breast Cancer.
Vermeij R, Leffers N, van der Burg S, Melief C, Daemen T, Nijman H Immunological and clinical effects of vaccines targeting p53-overexpressing malignancies.
Viatour P, Ehmer U, Saddic L, Dorrell C, Andersen J, Lin C, Zmoos A, Mazur P, Schaffer B, Ostermeier A, Vogel H, Sylvester K, Thorgeirsson S, Grompe M, Sage J Notch signaling inhibits hepatocellular carcinoma following inactivation of the RB pathway.
Vignot S, Frampton G, Soria J, Yelensky R, Commo F, Brambilla C, Palmer G, Moro-Sibilot D, Ross J, Cronin M, André F, Stephens P, Lazar V, Miller V, Brambilla E Next-generation sequencing reveals high concordance of recurrent somatic alterations between primary tumor and metastases from patients with non-small-cell lung cancer.
Vilgelm A, Pawlikowski J, Liu Y, Hawkins O, Davis T, Smith J, Weller K, Horton L, McClain C, Ayers G, Turner D, Essaka D, Stewart C, Sosman J, Kelley M, Ecsedy J, Johnston J, Richmond A Mdm2 and aurora kinase a inhibitors synergize to block melanoma growth by driving apoptosis and immune clearance of tumor cells.
Wang Y, Lin R, Tan Y, Chen J, Chen C, Wang Y Wild-type p53 overexpression and its correlation with MDM2 and p14ARF alterations: an alternative pathway to non-small-cell lung cancer.
Wiedemeyer W, Dunn I, Quayle S, Zhang J, Chheda M, Dunn G, Zhuang L, Rosenbluh J, Chen S, Xiao Y, Shapiro G, Hahn W, Chin L Pattern of retinoblastoma pathway inactivation dictates response to CDK4/6 inhibition in GBM.
Xiao B, Spencer J, Clements A, Ali-Khan N, Mittnacht S, Broceño C, Burghammer M, Perrakis A, Marmorstein R, Gamblin S Crystal structure of the retinoblastoma tumor suppressor protein bound to E2F and the molecular basis of its regulation.
Young R, Waldeck K, Martin C, Foo J, Cameron D, Kirby L, Do H, Mitchell C, Cullinane C, Liu W, Fox S, Dutton-Regester K, Hayward N, Jene N, Dobrovic A, Pearson R, Christensen J, Randolph S, McArthur G, Sheppard K Loss of CDKN2A expression is a frequent event in primary invasive melanoma and correlates with sensitivity to the CDK4/6 inhibitor PD0332991 in melanoma cell lines.
Zagorski W, Knudsen E, Reed M Retinoblastoma deficiency increases chemosensitivity in lung cancer.
Zöchbauer-Müller S, Fong K, Virmani A, Geradts J, Gazdar A, Minna J Aberrant promoter methylation of multiple genes in non-small cell lung cancers.
NCCN NCCN Guidelines® are referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Acute Myeloid Leukemia V.1.2016, Breast Cancer V.1.2016, Central Nervous System Cancers V.1.2015, Gastric Cancer V.3.2015, Non-Small Cell Lung Cancer V.4.2016, Colon Cancer V.2.2016, Rectal Cancer V.1.2016, Melanoma V.2.2016, Neuroendocrine Tumors V.1.2015, Ovarian Cancer V.2.2015, Pancreatic Adenocarcinoma V.1.2016, Prostate Cancer V.2.2016, and Uterine Neoplasms V.2.2016. © 2016 National Comprehensive Cancer Network, Inc. All rightsreserved. The NCCN Guidelines® and illustrations herein may not be reproduced in any form for any purpose without the express written permission of the NCCN. To view the most recent and complete version of the NCCN Guidelines, go online to NCCN.org
Electronic SignatureSample Doctor, M.D., Pathologist - NeoGenomics LaboratoriesThe Technical Component Processing, Analysis and Professional Component of this test was completed at NeoGenomics California, 31 Columbia, Aliso Viejo, CA / 92656 / 866-776-5907 / CLIA#05D1021650 / Medical Director(s): Lawrence Weiss, M.D. .The performance characteristics of this test have been determined by NeoGenomics Laboratories. This test has not been approved by the FDA. The FDA has determined such clearance or approval is not necessary. This laboratory is CLIA certified to perform high complexity clinical testing.Images that may be included within this report are representative of the patient but not all testing in its entirety and should not be used to render a result.SAMPLE