
Patient Handling Update 2012 /2013 · Patient Handling Update ... session is to review and build...
17
Leicestershire Partnership NHS Trust The Academy April 2012 Patient Handling Update 2012 /2013
Transcript of Patient Handling Update 2012 /2013 · Patient Handling Update ... session is to review and build...
Leicestershire Partnership NHS Trust The Academy April 2012
Patient Handling Update
2012 /2013

Leicestershire Partnership NHS Trust The Academy April 2012

Leicestershire Partnership NHS Trust The Academy April 2012
Introduction
Welcome to your Patient Handling Update for 2012/2013. This session forms part of an
ongoing programme of training for all patient handling staff.
The aim of this programme is to provide staff with the knowledge that will assist them to reduce
their risk of back injury in the workplace.
Much of this information also applies outside the workplace; staff will be encouraged to consider
this during these situations.
You will be required to update your knowledge on a yearly basis.
Contents
Introduction – aims, objectives, and ground rules.
Summary of relevant legislation.
Back injury and the NHS.
Risk Assessment.
Summary of anatomy and physiology.
Principles of safe handling.
Unsafe / High risk moves.
Practical work: approved techniques and problem solving, including reference to:
Anatomy & Physiology: Risk Assessment, Principle of Safe Handling.
Training records and evaluation.
Leicestershire Partnership NHS Trust The Academy April 2012
Aims and Objectives
Aim
The aim of this session is to review and build upon the practical application of manual handling
in the workplace.
Objectives
At the end of the session you will be able to:
Explain the importance of risk assessment in relation to patient handling.
Demonstrate what measures you might consider when moving and handling patients that
would reduce the risk of injury.
Participate in a problem solving approach relevant to your area.
Ground Rules – PLEASE READ THIS SECTION CAREFULLY.
These rules are designed to make the training session safe for all participants. You are
expected to be fit enough to undertake this training.
You must inform the trainer, prior to the practical session, if – for any reason – you are unable to
participate fully in this part of the training, this could be for health, medical issues, pregnancy or
if you have given birth within the last 6 months.
This information will be treated in strict confidence. However, your training is not complete until
you have successfully taken part in the practical session, and the words “unable to take part in
the practical session –training incomplete” will be added to your training record. A copy of the
training record will be sent to your manager.
You are strongly advised to notify your manager of any illness or injury, which prevents you from
safely undertaking manual handling duties, in line with your legal and contractual
responsibilities.
You are required to wear your usual work clothing and appropriate footwear – flat heeled, non
slip shoes – for the practical session.
You must only perform manoeuvres under the supervision of a trainer.
Trainers can at any time, stop you taking part in an activity in the interests of safety.
Leicestershire Partnership NHS Trust The Academy April 2012
Summary of Relevant Legislation
Health and Safety at Work Act 1974
Employers have to:
Protect the health and safety of their employees
Protect the health and safety of others who might be affected by the way they go about
their work.
Employees have to:
Take care of own health and safety and that of others.
Co-operate with their employer
Management of Health and Safety at Work Regulations 1999
Employers have to:
Assess health and safety risk to employees and others, to identify the precautions
required by health and safety law.
Take particular account in their assessment of risks to new and expectant mothers and
their unborn and breast feeding children.
Provide employees with adequate training and instruction.
Employees have to:
Use equipment provide by their employers as instructed.

Leicestershire Partnership NHS Trust The Academy April 2012
Back Injury and the NHS
In the NHS, manual handling accidents account for 52% of all sickness absence.
Ref: MHOR 1993 amended 2002
The total annual cost to the NHS is 400 million pounds per year, enough to employ
16,000 nurses.
Ref: Back Care 2011 (Cited Nursing Times)
The highest compensation paid to date is £803,000.
According to the Royal College of Nursing:
1.5 million working days are lost every year because of back injuries to nurses
80% of nurses have time off with back problems each year; 3600 healthcare workers are
forced to retire early as a result of back injury
(Back Care (cited Nursing Times 2011))
It’s not only nursing staff that experience back pain:
As many as 1 in 6 physiotherapists may move speciality or leave the profession as a
result of injury.
Ref: Guidance in Manual Handling, Chartered Society of Physiotherapists, 2002
30% of catering, domestic and portering staff in the NHS experience back pain regularly.
Ref: Back in Work Sheet No 1, Department of Health, 2002
Leicestershire Partnership NHS Trust The Academy April 2012
Risk Assessment
A moving and handling risk assessment is a way of examining our work activities that relate to moving and handling with the purpose of helping us decide:
1. How to perform a job without endangering ourselves
AND
2. What safety precautions we need to use.
The Management of Health and Safety at Work Regulations (1999) impose a requirement
upon employers to undertake an assessment of any risk to the health and safety of their
employees. This piece of legislation is supported and extended by the Manual Handling
Operations Regulations (1992), which have established a hierarchy of measures in order to
reduce manual handling risks:
AVOID handling where ever possible. Many manual handling tasks are performed without an assessment that might indicate that equipment could be used, or that the patient could be encouraged to help themselves. In essence we should ask ourselves the question “does the task need to be done?”
ASSESS the risks of those tasks that cannot be avoided.
REDUCE the risk as far as reasonably practicable.
PROVIDE INFORMATION for example on the weight of the load to be handled
Knowing if there is a risk to injury is a matter of judgement in each case. However there are
things to look out for, such as bad postures, awkward or heavy loads, cramped working areas,
excessive fatigue or history of back problems. Staff can often highlight which activities are
unpopular or difficult.
Manual handling risk assessments offer many benefits and may potentially:
Protect the staff and patients Reduce injures Stop some injuries occurring Change the culture of an organisation Identify equipment needs
Training is very important but remember that, on its own, it cannot overcome a lack of mechanical
aids, unsuitable equipment and inappropriate systems of work. Risk assessments will be an asset in
partnership with training.
Leicestershire Partnership NHS Trust The Academy April 2012
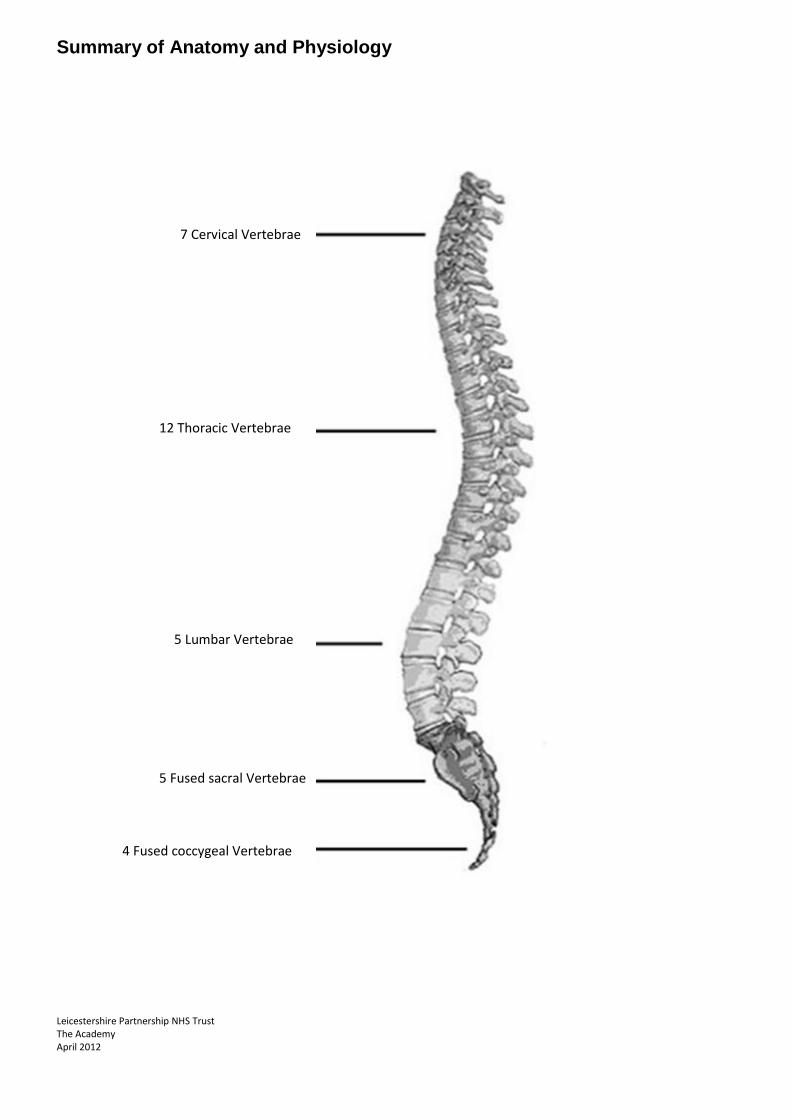
Summary of Anatomy and Physiology
7 Cervical Vertebrae
12 Thoracic Vertebrae
5 Lumbar Vertebrae
5 Fused sacral Vertebrae
4 Fused coccygeal Vertebrae

Leicestershire Partnership NHS Trust The Academy April 2012
Summary of Anatomy and Physiology
The spine is a column of 33 bones – called vertebrae separated from one another by ‘cushions’
of elastic tissue – the intervertebral discs.
The spine has 3 main functions:
- To support the upper body - To allow mobility - To provide a protective casing for the spinal cord
The spine of a newborn baby is ‘C’ shaped having two primary curves in the chest and sacral
regions. Once the infant lifts its head and, later begins to walk, the secondary curves of the
neck and the lower back regions develop, and the spine takes on its characteristic 3 curved ‘S’
shape.
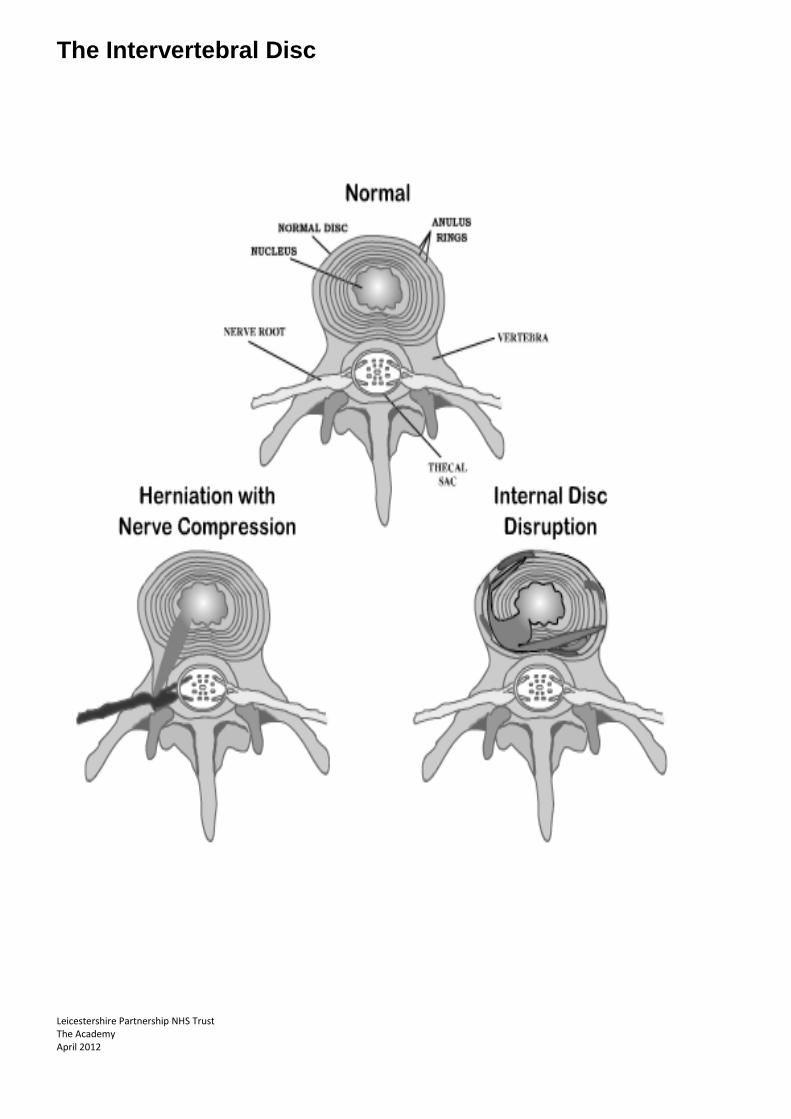
With the exception of the intervertebral disc, all the structures of the vertebral column have a
liberal nerve and blood supply.
Each intervertebral disc is comprised of a fibrous outer ring - the annulus fibrosus -, which holds
in place the inner jelly like nucleus pulposus. The discs act as hydraulic sacks that dampen the
shock of spinal actions and allow limited movement between vertebrae. It is the combined
actions of each disc all the way up the spine that provides the remarkable ability of the back to
stretch and move.
Leicestershire Partnership NHS Trust The Academy April 2012
The Intervertebral Disc

Leicestershire Partnership NHS Trust The Academy April 2012
Principles of Safe Handling
Apply these principles whenever manual handling is required:
Whenever moving or handling movable objects you need to remember your posture and
balance.
Wide stable base
Feet about hip-width apart, one foot slightly in front of the other, and with weight balanced
evenly between them. Once the load has been moved or lifted, the feet should move in the
direction of the load.
Keep natural curves of the back
Do not bend or twist – and remember, this includes your neck.
Elbows in
Keep your elbows tucked into the side of your body, to avoid increased stress on the neck. This
will also, automatically, bring the load in close to your body.
Bend knees
Use your powerful leg and buttock muscles
Bend your knees, but avoid squatting: it puts great strain on your knee joints
Head up/chin in
Look face on to the load to avoid twisting your neck. Hold your chin in slightly to avoid
extending your head back. Lead off the lift with your head – where the head goes the rest of the
body will follow.
Hold load close
The closer the load is held to the body, the less stress there is placed on the back.
Health and Safety Executive (2003)

Leicestershire Partnership NHS Trust The Academy April 2012
Unsafe / High Risk Techniques
There are a number of ‘traditional’ techniques which are now considered unsafe / high risk, and
which must no longer be used.
Legally it is the Manual Handling operations Regulations, 1992 - made under the Health and
Safety at Work Act 1974 – which govern all manual handling activities, and to which reference
should be made; the important publication here is Manual Handling operations Regulations1992
Guidance on regulations L23 (Health and Safety Executive, 1992).
All unsafe / high risk moves have either caused injuries to NHS and private sector patients,
handlers, or both and as a consequence, have featured in court cases. They are no longer
considered good practice AND MUST NOT BE USED.
A handler injured when using any of these techniques would find it difficult to obtain
compensation; a patient injured when being handled by any of these methods would find it easy
to do so.
IT IS TRUST POLICY THAT STAFF DO NOT USE NON-APPROVED MOVES.

Leicestershire Partnership NHS Trust The Academy April 2012
Unsafe / High Risk Moves The Drag Lift - This includes any way of handling the patient in which the handler places a hand or an arm under the patient’s axilla (armpit), whether the patient is being moved up the bed, sat up in the bed, being assisted from sitting to standing, or being assisted to change from one seated position to another – and regardless of whether the handler is facing or behind the patient, or whether there is more than one handler.
An example of a drag-lift

Leicestershire Partnership NHS Trust The Academy April 2012
An example of the worst kind of drag-lift

Leicestershire Partnership NHS Trust The Academy April 2012
The Orthodox Lift - a two-person lift, in which the handlers place one arm around the patient’s back and the other under the patient’s thighs. The handler’s may clasp each
other’s wrists, or they may hold the far side of the patient. Handling slings are sometimes used. In all
cases these lifts are dangerous.
The orthodox lift
Two-sling lift - (not shown) with slings placed under the patient’s lower back and thighs, the handlers stand either side of the patient with one knee on the bed; this is a
total body lift.
The shoulder lift - (shown below) Also known as the ‘Australian’ lift, regardless of whether the ‘Free arm’ is placed on the bed for ‘support’ or placed around the patient.

Leicestershire Partnership NHS Trust The Academy April 2012
Front transfer with one nurse - this includes the pivot transfer, the elbow lift and the ‘Bear Hug’, regardless of whether a belt or sling is used
An example of the ‘bear hug’ lift
You should not lift people because:
They weigh too much and are unpredictable
It is difficult or impossible for staff to get into a safe position to lift
Staff are at risk of injury in all manual handling techniques
Most lifts include a risk of injuring the patient
Manual lifts are not therapeutic; they do not improve the patient’s mobility.
For recommended patient handling techniques, refer to the Leicestershire Partnership NHS Trust
document ‘PROCEDURES FOR THE MOVING AND HANDLING OF PATIENTS’

Leicestershire Partnership NHS Trust The Academy April 2012
References
Backcare in collaboration with The Royal College of Nursing and The National Back Exchange. (cited
Nursing Times) 2011
The Guide to the Handling of People a systems approach 6th Edition 2011 BackCare.
Chartered Society of Physiotherapists (2000): Manual Handling for Chartered Physiotherapists.
Available from: http://admin.csp.org.uk/admin2/uploads/-38c9a362-ed71ce5fa5-
77d7/gimh4cp.PDF;LAST Reviewed Jan 2001.
Health and Safety Executive (2004) Manual Handling Operations Regulations (1992) (As amended),
Guidance on Regulations, 3rd Edition London:HMSO
Back in Work, Sheet No 1, Department of Health (2002)
Contacts
Moving and Handling Advisor, The Academy, Leicestershire Partnership NHS Trust , The Academy Reception 0116 225 5945 For details of training records contact the Academy Administration Services on 0116 225 3669 academy @leicspart.nhs.uk


















