
Pathophysiology of Burn Injury
46
PATHOPHYSIOLOGY OF BURN INJURY IYAN ASIANA, dr KARMILE, dr AHMAD CIPTA, drg ANDI NUGRAHA S, dr
-
Upload
iyanasiana -
Category
Documents
-
view
240 -
download
6
description
Pathophysiology of Burn Injury
Transcript of Pathophysiology of Burn Injury
PATHOPHYSIOLOGY OF BURN INJURY
IYAN ASIANA, drKARMILE, drAHMAD CIPTA, drgANDI NUGRAHA S, dr

DEFINITION
A burn is an injury caused by an exogenous agent that produces a characteristic reaction to local tissues which may vary from mild erythema to full thickness destruction of the skin and deeper tissues.

INTRODUCTION
• BURN CAUSE COAGULATIVE NECROSIS OF EPIDEMIS AND UNDERLYING TISSUE
• THE DEPTH DEPENDING• TEMPERATURE• TIME EXPOSURE• SPECIFIC HEAT FROM CAUSATIVE AGENT
BURN CLASSIFICATION
• THERMAL : DRY HEAT, MOIST HEAT, FLASH• ELECTRICITY : CONDUCTION OF ELECTRIC
CURRENT• CHEMICALS : NOXIOUS CHEMICALS• SCALD : HOT LIQUID• CONTACT : HOT OR COLD SOLID
MATERIAL• RADIATION : RADIOACTIVE AGENT / SUN
BURN,

CAUSESTHERMAL
-DRY HEAT -MOIST HEAT -FLASH BURNS
CONTACT BURNS
FLAME BURNS

ELECTRIC -LOW VOLTAGE -HIGH VOLTAGE

CHEMICALS -ACIDS -ALKALI

RADIATIONS - IONIZING - NON-IONIZING

BURN CLASSIFICATION
• FIRST DEGREE : LOCALIZED TO THE EPIDERMIS
• SUPERFICIAL SECOND DEGREE : EPIDERMIS AND SUPERFICIAL DERMIS
• DEEP SECOND DEGREE : EPIDERMIS AND DEEP INTO THE DERMIS
• THIRD DEGREE : INTO SUBCUTANEOUS FAT
• FOURTH DEGREE : INTO UNDERLYING MUSCLE OR BONE
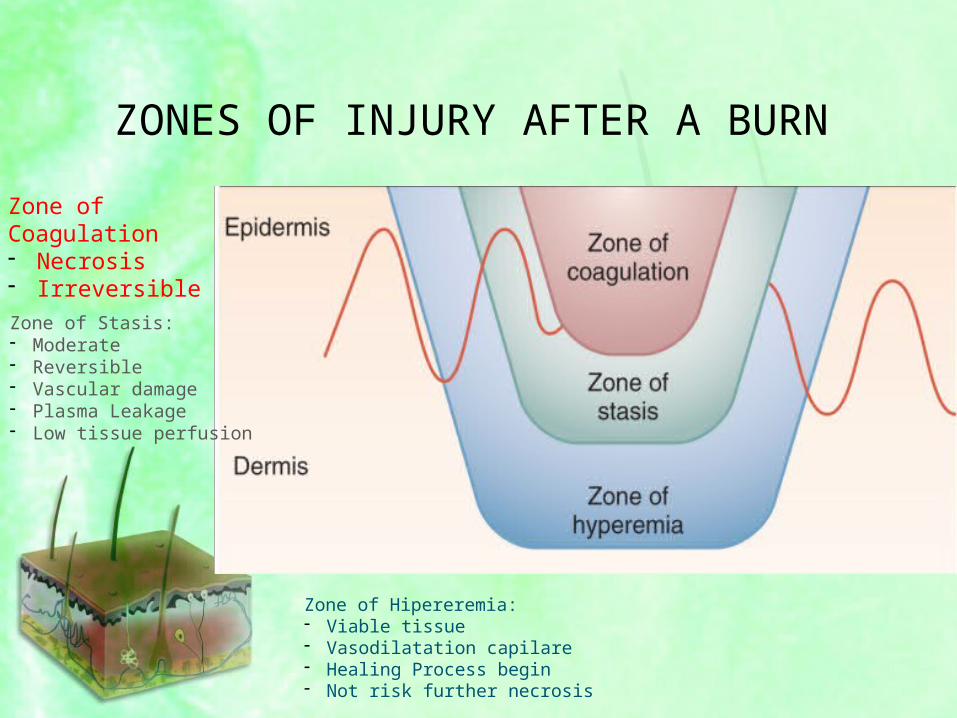
ZONES OF INJURY AFTER A BURN
Zone of Coagulation - Necrosis- Irreversible
Zone of Stasis:- Moderate- Reversible - Vascular damage- Plasma Leakage - Low tissue perfusion
Zone of Hipereremia:- Viable tissue- Vasodilatation capilare- Healing Process begin- Not risk further necrosis

CLASSIFICATIONNOMENCLATURE TRADITIONAL
NOMENCLATURE
SUPERFICIAL BURNS FIRST DEGREE
PARTIAL THICKNESS BURNS SECOND DEGREE
FULL THICKNESS BURNS THIRD DEGREE
FOR MORE DETAILS ICD 10’ T20-T32

ANATOMY OF SKIN

BURN DEPTH


SUPERFICIAL /FIRST DEGREE BURN
DEPTH• Epidermis involvement
CLINICAL FINDINGS• Erythema• Mild pain• Lack of blisters
OUTER LAYER OF THE SKIN IS DAMAGED ONLY

SUPERFICIAL / FIRST DEGREE
• INJURIES CONFINED TO EPIDERMIS
• PAINFUL AND ERYTHEMATOUS• BLANCH TO THE TOUCH• INTACT EPIDERMAL BARRIER• DO NOT RESULT IN SCARRING

PARTIAL THICKNESS/SECOND DEGREE BURN
DEPTH• Superficial (papillary) dermis• Deep (reticular) dermis
CLINICAL FINDINGS• Severe Pain• Blisters• Clear fluid
OUTER LAYER OF THE SKIN AND THE LAYER UNDERNEATH IT

SUPERFICIAL SECOND DEGREE
• INJURIES CONFINED TO SUPERFICIAL DERMIS
• PAINFUL AND ERYTHEMATOUS• BLANCH TO THE TOUCH• SPONTANEOUSLY RE-EPITHELIALIZE
FROM RETAINED EPIDERMAL STRUCTURES IN 7 TO 14 DAYS
• MAY RESULT IN SOME SLIGHT SKIN DISCOLORATION

DEEP SECOND DEGREE
• INTO THE RETICULAR DERMIS• DO NOT BLANCH TO TOUCH• PAINFUL TO PINPRICK• HEAL IN 14 TO 35 DAYS• OFTEN WITH SEVERE SCARRING AS A
RESULT OF THE LOSS DERMIS

FULL THICKNESS / THIRD DEGREE BURN
DEPTHDermis and underlying tissue and possibly fascia, bone or musle
DESTROYS THE DEEPEST LAYER OF THE SKIN AND TISSUES BENEATH IT
CLINICAL FINDINGS• No sensation• Hard• Leather like eschar• Purple fluid

THIRD DEGREE• FULL THICKNESS THROUGH
EPIDERMIS AND DERMIS• HARD, LEATHERY ESCHAR• NO EPIDERMAL AND DERMAL
APPENDAGES REMAIN• MUST HEAL BY RE-EPITHELIALIZATION
FROM THE WOUND EDGES

DETERMINATION OF SEVERITY OF INJURY


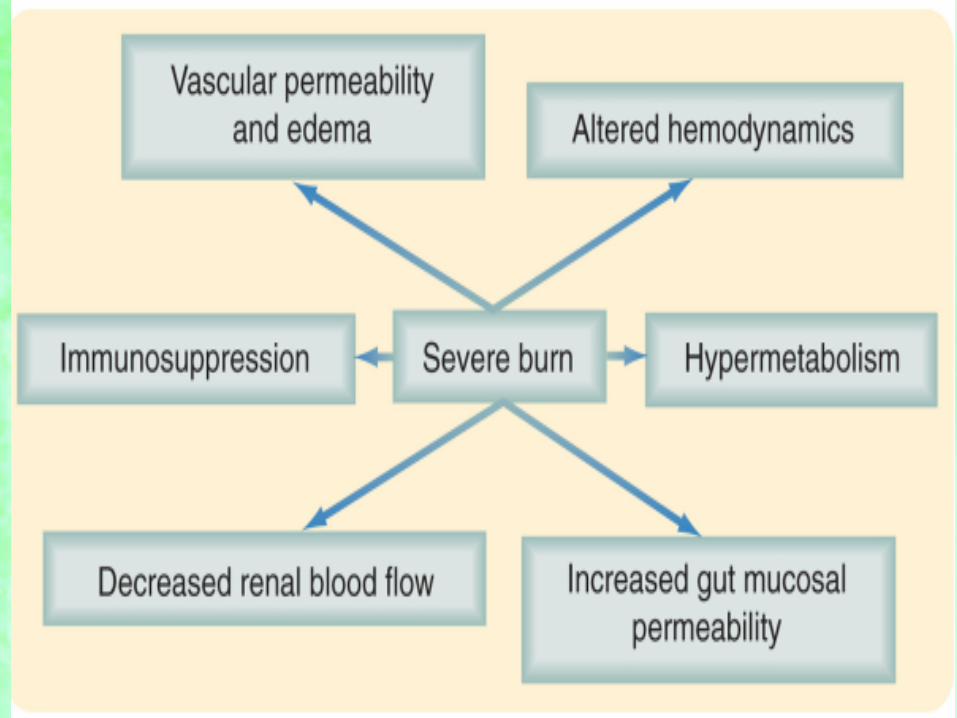
PATHOPHYSIOLOGY
BURNS
SKIN LOSS
AIRWAY & LUNG INJURIES
INFLAMMATORY & CIRCULATORY CHANGES
KIDNEYS
STOMACH
INTESTINE
OTHER CHANGES

SYSTEMIC CHANGES
• INTEGUMENTARY SYSTEM• RESPIRATORY SYSTEM• CARDIOVASCULAR SYSTEM• EFFECTS ON THE RENAL SYSTEM• EFFECTS ON THE GASTROINTESTINAL
SYSTEM• EFFECTS ON THE IMMUNE SYSTEM• MUSCULOSKELETAL SYSTEM• CENTRAL NERVOUS SYSTEM• INFLAMMATION & EDEMA• HYPERMETABOLISM

Integumentary System
• Thermal injury rapidly irreversible injury & cell death
• Epidermis – dermis – subcutaneous • Skeletal muscle
• Burn injury extended deeper + inflammatory response

Integumentary System
Burn injury
- Rapid loss of the intravascular fluid from the damaged capillaries
- Neutrophils adhering to endothelium & to each other
Obstruction of microvasculature
Poor perfusion
Deeper level of necrosis

Integumentary System
• The presence and extent of infection• Colonization proliferation extension (hair follicles) growth
(necrotic tissue)• Infection : bacterial, fungal
Coagulum on the surface
BURN ESCHAR
Necrotic epidermis&dermis

Respiratory System
• Direct thermal injury to the trachea and bronchi probably does NOT occur (except in the exposure to large quantities of steam)
• Problems related to airways related to :- Pneumothorax- Interstitial emphysema- Aspiration- Pulmonary embolism- Non specific pulmonary edema
Respiratory Infection
• Patient with respiratory failure sterile lung tissue
• Patient with sepsis extensive infection of the lung (+)
• Etiology : bacteria, fungi
• Angioinvasive infection to the lung :- antibiotic-resistant strains of
Pseudomonas - Aspergillus

Respiratory Infection
Bacteria & Fungi
Angioinvasive
Massive proliferation- The walls of pulmonary arteries
- Ischemic necrosis of segments of lung tissue

Diffuse Alveolar Damage
Damage/increased permeability of capillary and epithelial type I
Exudation of protein-rich fluid into alveolar space
Hyaline membrane (hours)
Collagenous fibrosis (days)
Obliterates alveoli Thickened the septa
Macrophages accumulate within alveoli
Multiplication of alveolar type II cell
SEVERE INTERSTITIAL FIBROSIS

Pathophysiology of Pulmonary Injury
Multiple mechanisms :- Activation of complement- Releasing of superoxide- Activation of Kinin System- The presence of high concentration of O2
Many patient do NOT develop clinically apparent respiratory difficulty delayed fluid resusctiation, limb ischemia, sepsis

Sistem Cardiovaskular
• Umum terjadi takikardia dan peningkatan cardiac output pada pasien luka bakar
• Dilatasi cardiac dan kontraktilitas myocardial yang jelek terjadi pasien luka bakar
• Hipertropi jantung reaksi dari takikardi dan stimulasi catecolamine
• Bacterial endocarditis pasien dengan luka bakar dengan sepsis

• Non bacterial thrombotic endocarditis (marantic endocarditis) peningkatan komplikasi embolik pada pasien dengan luka bakar luas dan sepsis karena spesies Acinetobacter

• Myocardial injury “contraction band necrosis”
• Perfusi jelek dan kebutuhan metabolic tinggi pada episode hipotensi
Sistem Urin
• Pasien luka bakar jika resusitasi pada jam pertama adequate fungsi ginjal normal
• Gagal ginjal bila resusitasi cairan tidak optimal dan sepsis
• Akut tubular nekrosis pada 80% kasus dan terdapat gagal ginjal• Ciri morfologis : edema pada seluruh
ginjal, peningkatan berat dan nekrosis sel tubular proximal dengan karyolisis, karyorrhexis dan peluruhan sel
• 48 jam regenerasi cell tubular yang selamat

Sistem digestiv, traktus hepatobiliar dan pankreas
• Ulcer duodenal terjadi pada luka bakar• Manifestasi awal, local mucosal nekrosis dan
hemorrhage• Defek pada mukosa mulitple, kecil dan bulat
berhubungan dengan pembuluh darah yang terbuka pada bagian dalam lesi
• Traktus intestinal rentan ischemic dan hypoxia• Sepsis berhubungan dengan peningkatan cedera
intestinal • Ischemic injury epitel intestinal memulai
translokasi flora intestinal ke sirkulasi mesenteric lymphatic dan ke sirkulasi vena portal
• Faktor lain perubahan ekologi bakteri usus

• Pembesaran hati terjadi 2-3 berat normal• Hepatomegali kompromi ventilasi • Lesi terlihat steatosis, deposition of large and small
lipid droplets in hepatocytic dan congestion , centrilobular necrosis

• Pankreatisis merupakan komplikasi yang sering• Focal necrosis of pancreatic tissue• Focal hemorrhage• Focal fat necrosis

LYMPHOID SYSTEM
• Depletion of Lymphocytes from lymphoid tissue
• Lymph nodes often lack germinal centre• Gastrointestinal lymphoid tissue of the
terminal ileum is generally atrophic • Appendix often shows a striking lack of
normal lymphoid tissue• These abnormalities of lymphoid tissue
correlate with the deficient immune responsiveness typical of patients with extensive burn injury

MUSCULOSKELETAL SYSTEM
• Lesions of skeletal muscle are uncommon in burn patients
• Occasionally, direct thermal injury extends into deep muscle and can be so severe
• Electrical injury often associated with with extensive necrosis of muscle
• Atrophy of skeletal muscle occurs as part of the catabolic state of burn patients, and represent s a challenge for those involved in rehabilitative efforts

CENTRAL NERVOUS SYSTEM
• Abnormalities can be found in the patients who die after burn injury
• The commonest lesion is degenerative lesion due to hypoxic and ischemic injury.
• Can be result of hypovolemia during resuscitation, shock or respiratory failure
• Extensive hypoxic brain injury caused by asphyxia during initial burn injury
• Severe hypoxic brain injury caused by CO poisoning


Selesai


















