PATHOLOGY AND MEDICAL MANAGEMENT OF THE CERVICAL SPINE
81
PTP 521, MUSCULOSKELETAL DISEASES AND DISORDERS PATHOLOGY AND MEDICAL MANAGEMENT OF THE CERVICAL SPINE
description
PATHOLOGY AND MEDICAL MANAGEMENT OF THE CERVICAL SPINE. PTP 521, Musculoskeletal Diseases and Disorders. Symbols. this is for your information only, it won’t be used for the exam important to know for exam. - PowerPoint PPT Presentation
Transcript of PATHOLOGY AND MEDICAL MANAGEMENT OF THE CERVICAL SPINE

PTP 521 , MUSCULOSKELETAL DISEASES AND DISORDERS
PATHOLOGY AND MEDICAL MANAGEMENT OF THE CERVICAL
SPINE

Symbols
this is for your information only, it won’t be used for the exam
important to know for exam
2

Cervical Spine Pathology
Trauma
Fractures Spinal StenosisRheumatoid Arthritis
Arthritic Conditions
DJD/Osteoarthritis
Other
DegenerativeDisk Disease
Disk Bulge, Herniation
C2-C7Radiculopathy
Joint
ImpingementSyndrome
Facet Syndrome
Bone Disk
Post ConcussionSyndrome
Whiplash
Soft Tissue
Headaches
Other
Hypomobility
3

Stiell IG, Clement C, et al. The Canadian C-Spine Rule versus the Nexus Low-Risk Criteria in Patients with Trauma.
JAMA 2003, 349;26
Sensitivity: 99.4%
Specificity: 45.1%
4
Canadian CervicalSpine Rule for RadiographicExamination

Canadian Cervical Spine Rule for Radiographic Examination
Stiell et al in 2003 examined patients to determine the characteristics of those who had positive cervical spine fractures versus those who were negative.
By following these rules, the number of unnecessary radiographs for the cervical spine was decreased dramatically
http://content.nejm.org/cgi/content/full/349/26/2510
(full text article)
5

Importance
By following the Canadian Cervical Spine Rules, A clinician can be reasonably certain that a patient needs a radiograph of the cervical spine.
Sensitivity is high, - SnNout- therefore, if following these rules and the tests are negative, and you send the patient for a radiograph, only 1% will have a fracture. 99% will not have a fracture.
Specificity is mid range - SpPin - therefore, if the tests are positive, you send the patient for a radiograph, only 45% will have a fracture.
6

Fractures of the Cervical Spine
Musculoskeletal Practice Pattern G
75% of all spine fractures occur in the cervical spine due to the instability of the atlanto-occipital joints
7

Jefferson’s Fracture:Burst Fracture of C1.
Head holder, so fragments everywhere, very unstable, neck brace or halo.
1. MOI: Axial Compression
2. Radiograph: odontoid view, greater than 7 mm difference between both lateral masses
of the atlas and those of the axis.
3. Unstable Fracture
8

Jefferson’s Fractures: Burst!
9

Hangman’s Fracture:
Fracture of the neural arch of the axis, fractures the pedicles of C2 with dislocation of C2 on C3
1. MOI: Hyperextension a blow on the forehead forcing the neck into extension is
a classic mechanism of injury producing fractures thru the pedicles
2. Radiograph: lateral view shows bilateral disruption through the pedicles of the axis
3. Unstable fracture
10

Hangman’s Fractures11

Hangman’s Fracture12

Dens Fractures
Type 1: (A ) avulsion of the tip of the dens as a result of apical or alar ligament stress
Type 2: (B) fracture of the junction of the dens with the body of the axis.
Type 3: (C) fracture deep within the body below the dens.
Type 4: see below
13

Dens Fractures
Left: Type 2 dens fracture at the junction of the dens with the vertebral body with posterior displacement
Right: fracture of the dens with posterior displacement of the atlas causing a small degree of spinal canal compression 14

CT scan of odontoid Fractures Type 3
Notice on this CT scan The foramen for the Vertebral artery
emedicine.medscape.com/article/94234-media
15

Dens Fracture
Type 4: sagittal or parasagittal fracture extending from a point lateral to the dens vertically or diagonally to the inferior surface of C2
16

Os Odontoideum:
Congenital Disorder
Failure of the dens to unite with the body of the vertebrae. 1. Radiograph: Odontoid view
-Tell it is not a dens fracture by the smoothness around parts
17

Wedge Fracture:
1. MOI: Hyperflexion and Compression
1. -Like a crunch, diving
2. Radiograph: lateral view, the anterior height of the vertebral body is shorter by 3mm than the posterior border
3. Stable fracture2. -If it has no neuro s(x),
then will not do anything, end with a little kyphosis curve
18

Wedge Fracture
This fracture is easy to see compared to some. In comparing anterior height to posterior height, you should see a difference.
19

Burst Fracture of the Vertebral Body
Lower cervical vertebrae
1. MOI: Axial Compression2. Radiograph: lateral
view, comminuted vertebral body is flattened centrally
3. Can be stable or unstable
3. -Described by presence of neuro s(x), impingement of the spinal canal.
20

Radiograph: lateral view, comminuted vertebral body is flattened centrally
emedicine.medscape.com/article/94234-media21

Clay-Shoveler’s Fracture
Avulsion fracture of the Spinous Process 1. MOI: a. Hyperflexion
-Where the pulley is over-used and detaches-Trapezius, Rhomboids, Para spinals
22

Hypomobility of the Cervical Spine
1. Pathology: tightness of the capsule of one of the synovial facet joints
2. Radiographic signs: generally none3. Clinical Symptoms: aching, dull, stiff
feeling in the neck *Headaches*4. Clinical Signs: loss of movement in a
capsular pattern for the facet joints Joint play is decreased at the segmental level Capsular end feel Pattern: Upper Cervical: limited lateral flexion
and rotation equally limited %-wise, then extension limited less.
-Lower cervical is opposite
23

Facet Syndrome
Pathology: joint capsules are stretched from joint subluxations or distension of the joint with fluid.-Looser the capsule gets, tight Para spinals.
Body will protect the area with posture and muscle spasms of the paravetebral muscles which leads to a decrease in spinal mobility and a secondary muscle fatigue.
Joint Dysfunction
24

Facet Syndrome
Occurs early in the degenerative process for the young or middle aged patient
Loading patterns change which lead to cartilage degeneration, facet hypertrophy and bony adaptation in the form of sclerosis or spurring (ostephyte formation).
Alters joint function which alters disc function
25

Radiographic Signs: Oblique view:
a. Hypertrophy of the facet joint
b. Osteophyte formation at the superior and inferior articulating processes
c. Decrease in joint space
26

Clinical Symptoms of Facet Syndrome
Presentation is variable, generally a steady ache with long periods of inactivity.
Pain present after activity, not during. Progression of pain gets more sever over time Pain will come and go with activity demands and
disease progression.Sharp pain with abrupt movements. Catching or locking sensation. Some radiation of pain may occur if nerve
root is involved
27

Clinical Signs of Facet Syndrome
Muscle spasms in the paraspinals Decrease lordosis Decrease ROM all directions particularly with
extension and rotation to one side Pain with extension Neurological exam is normal initially, may be
abnormal eventually with osteophyte formation.
28

29

Impingement Syndrome
1. Onset: sudden, often without a memorable trauma
2. Radiographic Signs: generally none
3. Clinical Symptoms: sharp, unilateral pain, stiff neck and c/o loss of movement
30

Signs of Impingement Syndrome
ROM limited in area’s that close or compress the facet joint on the painful side.
Extension and rotation to the side of dysfunction are limited
Lateral flexion may be painful, not as limited
Compression increases pain, distraction decreases pain.
Muscle guarding during passive and active movement.
31

Osteoarthritis, Degenerative Joint Disease
Pathology: progressive degeneration as a naturalconsequence of aging, loss offlexibility or movement occurs as the disease progresses
-Look for osteophyte formation, anteriorly first bridging between vertebrae.
Joint Dysfunction
32

Osteoarthritis: oblique view
Osteophyte formation is usually seen as bridging the vertebrae – carefully review the shape of the vertebrae in this view
Encroachment of the neural foramen is also noted emedicine.medscape.com/article/
305145-media
33

Cervical Spinal Stenosis:
Pathology: narrowing of the central spinal canal or the intervetebral foramina Increase in bone formation around the nueral
foramen.
Etiology: Developmental, congenital, or traumatic, age related Can be caused by intervetebral disc disease or
osteoarthritis
Joint Dysfunction
34

Symptoms and Signs of Spinal Stenosis
Symptoms: Radiating arm pain and numbness in nerve root
distribution Clumsiness if severe enough
Signs Myotomal weakness Hyperreflexia: will increase foramen space, so will
look down, and adjust entire posture to compensate. Clonus
-May think that it is a “Disk Herniation”, but way to differentiate is an MRI
35

Imaging Studies
MRI: imaging study of choice
CT myelogram can be used but will be invasive so may not be the one of choice
36

Disc Herniation Causing Impingement of Specific Spinal Nerve
37
Can occur with or without radiculopathy. Less common in the cervical spine than in the lumbar spine.
Individual nerve roots may be impinged or tethered within the foramin.

3. Herniation Sites38
a. C1-2: no discb. C2-3: rarec. C3-4: rared. C4-5:
1) clinical symptoms2) signs: Motor
Sensory Reflexes

Herniated Disc: MRI
Look at the spinal cord by C4-5 and C5-6. C4-5 is a larger herniation. This one is impinging on the spinal cord. Consider the clinical
symptoms this patient may have.
C5-6 slightly smaller and may only be a bulge.
39

Disc Herniation
MRI: encroachment by the disc on the spinal canal
Stenosis of the canal is also occurring giving the spinal cord a strangled appearance
www.mayfieldclinic.com/PE-HCDisc.htm
40

MRI
Best able to detect Disk height loss Annular fissures Osteophytosis End plate changes Herniation
APTA 2009 CRHazle
C5-6 disc herniation extending Posterior into the canal
41

Pathological Findings
Winking Owl Sign: Metastatic cancer to
the spine can show up initially as a missing pedicle
It gives the impression that the one of the “eyes” is closed.
= pedicle www.medscape.com/viewarticle/421516_6
42

Whiplash: Musculoskeletal Practice Pattern 4E
Definition: cervical strains or acceleration injuries “whiplash”
MOI: Sudden Acceleration-Deceleration movement of the head and neck
Causes: Falls, car accidents, sports injuriesHead inertia creates a high velocity force or accelerationResults in severe overstretch injuryAge of patient, general health, direction of forces and
magnitude of forces determines the extent of injury and the tissues that are involved
Soft tissue structures which can be potentially injured include: disc, spinal ligaments, capsule, muscles, nerves, spinal cord and vertebrae
43

Radiographic signs:
Changes in cervical curve on x-ray
Fanning of interspinous spaces (great space, curve in opposite direction)
Increased prevertebral space
Acute loss of disc height
Displaced prevertebral fat space
Vacuum cleft signParaspinals go into
sever spasms.
44

Force
Amount of force= weight of head plus speed that the head moves.
Direction of Force: Where was the car hit Symmetry of impact Double injury – hit from behind, pushed into another
vehicle Position of person in relation to impact
45

C. Onset: may not be for several hours after an accident
D. Symptoms: pain, stiffness, and muscle spasm in the cervical spine, headaches are usually posterior, may have some dysphagia
-Spasms are the Hallmark, extreme tenderness to palpation.
46

Post Concussion Syndrome
1. Pathology: blow to the head 2. Onset: develops after the concussion
within a 48 hour period after trauma May last several weeks or months after injury
3. Symptoms: persistent headaches, inability to concentrate, irritability and fatigue
SoftTissue
47

4. Medical Tests: CT scan usually negative for any brain injury
5. Specific Conditions related to return to play• Dependent upon severity of concussion – mild,
moderate, or severe• Number of concussions a player has had in a
season
48

Grade I: Mild Concussion
• Momentary confusion, no loss of consciousness, symptoms disappear within 15 minutes
• First concussion: return to play if asymptomatic for one week
• Second: return to play in 2 weeks if asymptomatic for 1-2 weeks
• Third: terminate season, may return to play next season if asymptomatic
49

Grade II: Moderate Concussion
Brief concussion, no loss of consciousness, symptoms last longer than 15 minutes First concussion: return to play if asymptomatic for
one week Second: minimum of 1 month off play and
asymptomatic for 1 week. If not asymptomatic, terminate season
Third: terminate season, may return next season
50

Grade III: Severe Concussion
Loss of consciousness – briefly or prolonged First concussion: return to play after a minimum of
one month off and asymptomatic for one week
Second: terminate season, may return to play next season if asymptomatic
51

Post Dural Puncture Headache
Spinal headacheRisk Factors:
Anyone who has an epidural or spinal tap procedure
SX: severe, dull, non-throbbing pain, usually in fronto-occipital region
Signs: aggravated by upright position, decreased in supine position
May have nausea, vomiting, visual disturbance and/or auditory disturbance
Self-limiting usuallyTell them to drink Mt. Dew (Caffine)
52

Other Dx
RA: particularly in the C spine can lead to spinal cord injuries, death if forced into hyper extension due to fragilely of the joints.
Other types of headaches covered in Neuro: Migraines Cluster Headaches Postural Headaches
53

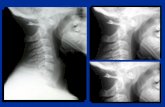
Cervical Spine: RadiologyTypical Views Special Views
Open Mouth ViewAP viewLateral ViewRight ObliqueLeft Oblique
Lateral FlexionLateral Extension
54

Evaluation using ABCDS
Odontoid or Open Mouth View Patient Position:
Supine, mouth open Beam: directed
downward into the open mouth
Film placed between posterior C-spine and table
-For Evaluating stability of upper cervical spine.
55

Alignment:
Demonstrate odontoid and lateral masses of C1.
Draw around the odontoid, and body of C2, draw the lateral masses of C1.
Look at the alignment between the lateral masses of C1 and the body of C2, these should match up
There shouldn’t be any overhanging edges laterally, if there is, this may suggest a burst fracture of C1
Look at the medial edges of the C1 lateral masses and the body of the dens, these should be symmetrical with the dens centered between them.
56

Bone Density and Dimension
Odontoid should have NO lucencies in superior portion, base, or vertebral body
Bones should have equal density, consistent with no unexpected lucencies
57

Cartilage and Soft Tissue:
Cartilage: No intervertebral disk, can evaluate facet joints. These should be parallel and equally spaced
Soft Tissue: not applicable in this view
58

AP View, Alignment
Patient Sitting or Supine
Assesses C3-C7
Alignment: Draw a vertical line superior to inferior along the
spinous processes to assess segmental rotation – SP are bifid
Identify Pedicles: look for rotation Vertebral Bodies: Size, C3-C7 Uncinate joints: for osteophyte formation
59

60

61

Bone Density and Dimension
Evaluate each pedicle and vertebral body for a change in density or dimensions. Compare with segments above and below to see if there are any asymmetries in size or position and measure horizontal and vertical dimensions
62

Cartilage and Soft Tissue
Cartilage: evaluated on lateral view, not assessed in AP view
Soft Tissue: identify bottle shaped trachea Should be mid line, if not mid line, it may indicate the
presence of a tumor, pneumothorax or hemothorax
63

Lateral View, Alignment
Patient Position Lateral standing Supine cross table view
Alignment: Line 1: anterior borders of vertebral bodies Line 2: posterior borders of vertebral bodies Line 3: spinolaminar line: junction of lamina at the
spinous processes These three lines help to assess for several types of
pathologies that can be found on this view such as spondylolisthesis or burst fractures
64

Alignment cont.
Check for the normal lordosis: Flat C spine: indicates muscle spasms from trauma Increased lordosis: Kyphosis: anterior segmental compression fracture
65

ADI: Atlantodens Interval: space MUST not exceed 3 mm. Any greater distance and this must be evaluated by a physician for C1 or C2 instabilities.
emedicine.medscape.com/article/93546-media
66

Alignment cont.
Look at the margins of each vertebrae for possible osteophyte formation
Evaluate the facet joints and look for possible osteophyte formation
67

68

Bone Density and Dimensions
Evaluate the density of each cervical vertebrae for changes in density
Measure the vertebral body height anteriorly and posteriorly
69

Cartilage and Soft Tissue
Cartilage: Assess disk height
Soft Tissue: Prevertebral tissue Fanning of cervical
vertebrae may demonstrate interspinous ligaments
Retropharyngeal space should measure 7mm or less
70

Retropharyngeal space: measure less than 7 mm
Space between C2 anterior vertebral body and the posterior pharyngeal wall
Retrotracheal space: should measure no more than 22 mm in adults and 14 mm in children
Space between C6 anterior vertebral body and the posterior tracheal wall
71

Oblique Radiographs
Patient Position: Posterioanterior or
Anterioposterior Standing, sitting, or
supine Patient rotated 45 dg
to one side and demonstrates opposite side neural foramina
Primarily used to evaluate the intervertebral foramina
72

Alignment
Evaluate both oblique views and compare side to side
Draw each foramen on the oblique radiograph, evaluate for narrowing of the foramen, osteophyte formation, and anterior movement of one vertebrae over the other
Can also look at the pedicles and laminae
73

Left Oblique74

Right Oblique75

Special Views
Lateral Flexion and Extension Stress Views: observe joint alignment with movement, largely replaced with fluoroscopy as you can watch the movement occur
Pillar View: view the lateral masses of the cervical vertebrae, patient is turned to one side about 45 dg and extended about 30 dg.
76

Special Views cont.
Swimmers view: Patient prone on table
with arm abducted to 180 dg
Cross table radiograph with central beam directed to the axis
Film on opposite side Visualizes C7, T1 and
T2 vertebrae
www.biomedcentral.com/.../2/figure/F1?highres=y
77

Cervical Spine: CT
Sagittal Slice:
Orientate by finding the dens, C1 is just anterior to the tip of the dens, C3-C6 bodies of the vertebrae can be seen on this view.
Spinous processes are posterior to the spinal canal
Small circle at the top of the Largest spinous process is the posterior arch of C1
Good view to see bone intruding into the spinal canal
Anterior arch ofC1
78

Trans axial CT: Intervertebral Space
Body of Vertebrae
Facet joints
Spinal canal
Lamina
Bifed Spinous process
emedicine.medscape.com/article/1264627-overview
79

MRI of the Cervical Spine
T2 weighted sagittal MRI of the cervical spine
Orientate by finding the dens, anterior arch of C1, posterior arch of C1, cervical vertebaral bodies of C3-C7, T1-T5
Spinous processes
Spinal Cord, canal – any buckling of the cord? Any encroachment by the vertebral bodies into the canal? Check out C5-6. What do you think?
Disk Space: evenly spaced? Disk height is similar?
Soft tissue
80

www.gehealthcare.com/.../products/cimages.html
Body of vertebrae is very dark in this MRI
Spinal Canal/Cord is lighter
As pictures progress, can see more of the spinal nerve appearing and its attachment to the cord
Muscle
Cervical Spine: MRI81