Pathogenesis and treatment of HIV- associated peripheral neuropathies Justin C. McArthur HIV...
39
Pathogenesis and treatment of HIV-associated peripheral neuropathies Justin C. McArthur HIV Neurosciences Program Johns Hopkins University February 7 th , 2006 No disclosures
-
Upload
tobias-harper -
Category
Documents
-
view
216 -
download
0
Transcript of Pathogenesis and treatment of HIV- associated peripheral neuropathies Justin C. McArthur HIV...

Pathogenesis and treatment of HIV-associated peripheral neuropathies
Justin C. McArthur
HIV Neurosciences ProgramJohns HopkinsUniversity
February 7th, 2006No disclosures

HIV sensory neuropathies
Objectives
• Clinical features of sensory neuropathies
• Changing epidemiology and risk factors
• Pathology and pathophysiology
• Animal and in vitro models
• Treatment strategies

Major Neuromuscular Syndromes in HIV Disease
Diagnosis and HIV stage
Sensory neuropathies (DSP, ATN): Variable
Mononeuropathy multiplex: Early (limited); Late (progressive), Hep C
Progressive polyradiculopathy: Late, CMV
Inflammatory demyelinating polyneuropathy: Early
Myopathy: Any (AZT); Early (polymyositis)
ALS-type disorder: Late, rare
HIV-associated neuromuscular weakness syndrome: D4T
Distal sensory polyneuropathy DSPAntiretroviral toxic neuropaty ATN
Modified from David Simpson

Clinical features of HIV sensory neuropathies
Common length-dependent symptoms:• Spontaneous pain in feet, paresthesias, • Evoked pain ~ touch, rubbing (not cold) • Numbness ~ unusual in fingers• Lancinating pains
Examination: sens. thresholds 85%• Absent/reduced AJ’s 96%• Distal weakness 33%• Atrophy or wasting 30%• Fasciculations 0%
Features of HIV distal sensory polyneuropathy and antiretroviral toxic neuropathy are identical. Neuropathic sx. are correlated with plasma HIV RNA
Cornblath, 1988; Tagliati M, 1999
…."springtime in nerveland”….

ACTG 5117 Neuropathy cohort: 83 HIV+ subjects ACTG 5117 Neuropathy cohort: 83 HIV+ subjects followed over 48 weeks: infrequent transitions followed over 48 weeks: infrequent transitions
Simpson DM, in pressSimpson DM, in press
Baseline
Week 48 Neuropathy free Only signs neuropathy
Symptomatic SN
Neuropathy free 18 (22.2%) 2 (2.5%) 6 (7.4%)
Only signs neuropathy
4 (4.9%) 6 (7.4%) 2 (2.5%)
Symptomatic SN 6 (7.4%) 0 37 (45.7%)
7-10% of subjects showed transition in either direction: predictors included
baseline severity, epidermal nerve fiber densities, and white race.

Epidemiology of HIV sensory neuropathies

Phase I/II trials: A reversible painful peripheral
neuropathy developed in 10 patients after 6-14 weeks' treatment with 2',3'-
dideoxycytidine.
Lancet. 1988 Jan 16;1(8577):76-81
ddC neuro-toxicity was noted early

Neurotoxic Nucleoside RT inhibitors
abbreviation : ddI preferred name : didanosine
trade name : Videx
2',3'-dideoxyinosine
abbreviation : d4T preferred name : stavudine
trade name : Zerit
2',3'-didehydro-2',3'-dideoxythymidine
abbreviation : ddC preferred name : zalcitabine
trade name : Hivid
2',3'-dideoxycytidine

Changing incidence of HIV-associated Neurological
ConditionsJohns Hopkins HIV Clinical Cohort
per 100 person years
0
2
4
6
8
10
12
1994
1996
1998
2000
2001
2002
2003
2004
HIV Dementia
HIV sensoryneuropathy
HAART
Richard Moore & Kelly Gebo

Rising prevalence of HIV-associated sensory neuropathies
Johns Hopkins HIV Clinical Cohort
0
5
10
15
20
25
30
35
40
45
1994 1996 1998 2000 2001 2002
per 100 persons
Identified risk factors:• age (2-3 fold) or DM
• nadir CD4 count• plasma HIV RNA• APOE4/mtDNA
haplogroup• d4T or ddI exposure
• ?? HCV
Richard Moore & Kelly Gebo

Neuropathy is frequent in advanced HIV/AIDS, and may be asymptomatic
• Of 187 patients, 99 (53%) had DSP. – Patients with neuropathy were older, and more
commonly male– Twenty-six of 99 patients with DSP were
asymptomatic. – Asymptomatic neuropathy was correlated with
opiate and sedative abuse and dependence– DSP was not correlated with plasma viral load,
decreased CD4 cell counts, or neurotoxic antiretroviral therapy
Morgello S. et al Arch Neurol. 2004 Apr;61(4):546-51

Risk Factors and Determinants for HIV-associated Sensory Neuropathies: Risk Factors and Determinants for HIV-associated Sensory Neuropathies: The role of dideoxynucleoside exposureThe role of dideoxynucleoside exposure
The Nerve Project (NS44807)The Nerve Project (NS44807)
Cherry C, et al Neurology, 2006

• The likelihood of having symptomatic neuropathy at baseline: strong association with use of ddI ever (OR=3.21, CI: 1.56, 6.60) strong association with use of d4T ever (OR=7.66, CI: 2.89, 20.33) • No association between months of exposure, time off a particular d-drug, hepatitis C, and presence of metabolic syndrome (Thomas D. AAN 2006)

Pathology of HIV sensory neuropathies

HIV-associated sensory neuropathy: Pathology
• HIV infection is confined to macrophages• Prominent macrophage activation both in
DRG and multifocally in proximal nerve• Ultra-structural: decrease in density of
dermal Remak bundles; abnormal and bizarrely shaped mitochondria in ATN.
Length-dependent loss of cutaneous and centrally-directed nerve fibers: both small and large fibers are affected

Distal sensory polyneuropathy: axonal degeneration
Control HIV-SN
Axonal degeneration is universal at autopsy. Griffin JW, 1994

Skin biopsy assesses unmyelinated nerve fibers
Thigh: normal density Distal leg: reduced density and nerve fiber
swellings
HIV sensory neuropathies
epidermisepidermis

Morphological abnormalities on skin biopsies
nerve fiber swellings
Segmented dermal fibers

A healthy Remak bundle at the papillary dermis containing 3 axons surrounded by collagen. (x25K)
Control
Remak bundle with dilated unmyelinated
axons showing watery axoplasm and granular
debris.
DSP neuropathy
Courtesy of Dr Gigi Ebenezer
Degenerating axons surrounded by
flattened Schwann cell processes. Large
abnormal mitochondria
ATN neuropathy

Nerve fiber repair is as impaired in HIV infection as in diabetes
0 25 50 75 100
Days
0
10
20
30
EN
FD
HIV neg controls HIV+ controls
HIV+ neuropathyDiabetics
Regenera
tion g
ap
Mike Polydefkis

Pathogenesis of distal sensory polyneuropathy
• associated with advanced HIV disease (Childs E., 1999)
• some response in thermal thresholds to HAART (Martin 2000)
• HIV proteins are toxic to cortical and DRG cultures (Nath 2001; Keswani, 2002)
• gp120 can bind to chemokine receptors in DRG neurons and induce calcium fluxes (Miller R, 2002)
• DRG macrophage activation prominent (Pardo C, 2001)

HIV infection is confined to macrophages within the DRG: p24 and GFAP do not colocalize
within in the perineuronal nest
Carlos Pardo
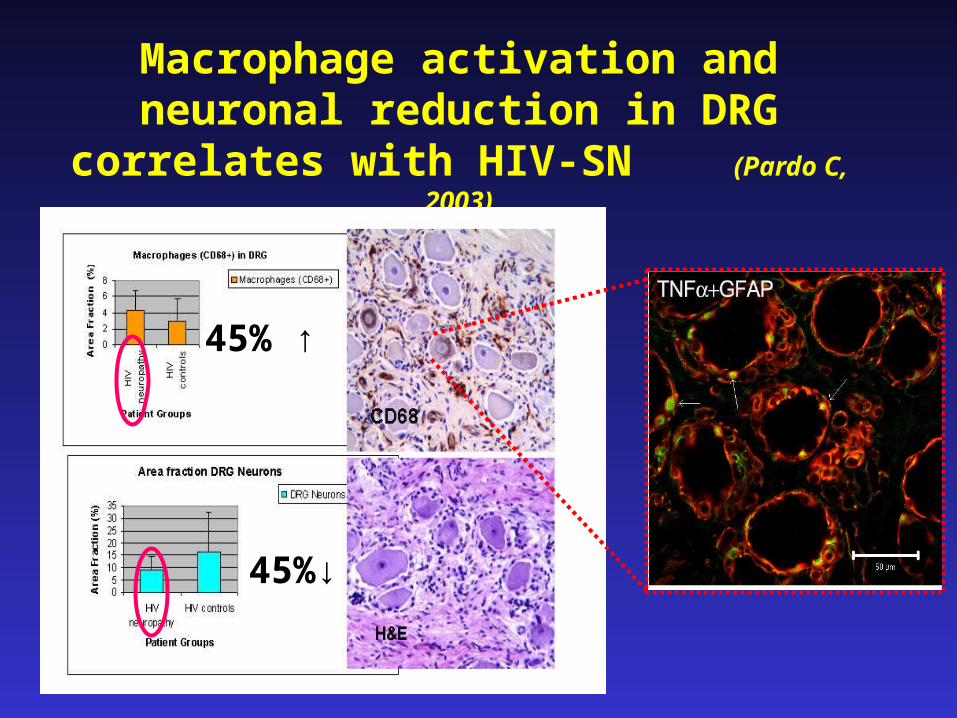
Macrophage activation and neuronal reduction in DRG correlates with HIV-SN
(Pardo C, 2003)
45% ↑
45%↓

Gp120 causes a dose-dependent axonal degeneration in sensory neurons in DRG cultures, mediated thru’ apoptosis
Gp120 [100pg/ml]Control Gp120 + DEVD
Keswani et al Ann of Neurol, 9/2003
Gp120 neuronal effect requires Schwann cells, but the axonal effect is mediated
thru’ chemokine receptorsHoke A and Melli G. 2005
Ahmet Hoke

SIV macaque model of HIV DSP (Mankowski J, Laast V, Zink MC, Clements J)
Epidermal nerve fiber density (% volume immunopositive for nerve fiber marker PGP 9.5) decreases
with severity of DRG ganglionitis.
CD68 immunostaining for activated/infiltrating macrophages in DRG of SIV-infected macaques
(squares) showing significant increase in macrophage staining in DRG

Pathophysiology of antiretroviral toxic neuropathy: a role for mitochondrial toxicity ?
• elevated serum lactate is a marker of ATN (Brew B., 2001)
• mitochondrial gamma DNA polymerase is inhibited by specific NRTI’s (Martin JL, 1994)
• acute ‘neuromyopathy’ with LAS (Marcus, 2001; Simpson 2004)
• mitochondrial DNA levels are reduced with prolonged exposure to d4T or ddI, and mtDNA haplogroups are risk factors (Cherry K, 2002; Hulgan T, 2005)

NRTI’s cause dose-dependent axonal degeneration in sensory neurons. Mediated thru’ necrosis
Keswani et al Ann of Neurol, 1/2003
Control ddC 1µM
ddC 10µM ddC 20µM
NRTI concentration
Tot
al N
euri
tic
Len
gth/
Neu
ron

Animal models have not been clarifying.
Absence of ddC effect on epidermal innervation in S-D rats: no denervation after 50-100mg/kg ddC daily IP for 8 months McArthur JC
unpubl.
Other animal studies:• axonal damage and ‘pain’ in chickens (Tatum A. unpubl.)
• ‘demyelinating’ neuropathy in NZW rabbits (Anderson TD, 1992)
• until now, few data in HIV transgenic animals• FIV model ~ epidermal denervation (Kennedy JM, 2004 )
• mixed pathology in primates
(Tsai, 1989; Kaul S, 1995 )

HIV-associated Sensory Neuropathies - a mouse model of antiretroviral toxicity
Hoke A et al
Transgenic mice expressing gp120 under GFAP promoter (developed by L. Mucke)
Gp120 protein is present in the brain, spinal cord and peripheral nerves
Animals are fed ddI (5 mg/ml) orally in their drinking water for 8 weeks

Intraepidermal nerve fiber density is reduced Number of Remak axons in distal foot nerves is reduced
Hoke A, Melli G

Treatment of HIV sensory neuropathies: what have we
learned ?

Sampling of controlled trials for HIV-sensory neuropathies
Agent Outcome CommentsAmitriptyline v. acupuncture
No effect • sham acupuncture used
Topical agents
• Lidocaine No • High % capsaicin YES
• advantage of intermittent topical therapies compared to oral agents
Amitriptyline v. mexilitene
No effect • underpowered
rh NGF Pain improved
• blinding compromised • no effects over 48 weeks on ENF
Lamotrigine Pain improved
• 2 separate trials• differential placebo effect in ATN

New (unlicensed) treatments for HIV sensory
neuropathies
Lamotrigine: Na channelGlucuronidation, rash
Topiramate: GlutamateRenal excretion, wt loss, kidney stones
Gabapentin/pregabalin: A2delta calciumRenal excretion, edema, sedation
Duloxetine: serotonin/norepinephrine RRINausea, hepatotoxicity
Combination therapies: eg NEJM study of gabapentin + morphine

Potential role for erythopoietin as a neuroprotective therapy for HIV-SN
EPO and its cognate receptor, EPOR are functionally expressed thru’ neuraxis
EPO may serve as an endogenous neuroprotective factor.
Schwann cells secrete EPO in response to injury to neighboring axons (NO is the signal), and may partially prevent axonal degeneration (Hoke & Keswani).
NARC-funded clinical trial planned to start Q2-2006 (Clifford & Thomas). Primary outcome ~ skin biopsy

• 9 structurally related alpha sub-units• Injury to peripheral nerves leads to
functional changes in channel subtypes: eg NaV1.8 is ‘essential’ for persistent pain states (Porreca F.)
• New agents are in development, eg GSK CDA54 which blocks the inactivated states of NaV1.7 and NaV1.8
• NaV changes are reversible by application of GDNF, with reductions in ectopic activity and pain behavior (Boucher, 2000)
• GDNF-based therapeutics are in development, gene therapy/stem cells/artemin (GFRa3-RET ligand)
Voltage-gated sodium channels are potential therapeutic target for HIV-SN

New trials for HIV-sensory neuropathies 2006-2008:
Agent Mechanism
Study design
High High concentratioconcentration capsaicinn capsaicin
Topical capsaicin 1%
• pain control required • registration trial planned
Pregabalin Pregabalin (Lyrica ®)(Lyrica ®)
A2-delta antagonist
• Early 2006 planned
NAALA-dase NAALA-dase inhibitorsinhibitors
L-acetyl L-acetyl carnitinecarnitine
ImmunophiliImmunophilinsns
Neuroprotective or regenerative agents with diverse mechanisms of action
• Will require both structural or functional outcome measures for neuropathy trials• LAC is in trial in ACTG 5157• Immunophilins in trial for PD and PPED

Summary: HIV-associated sensory neuropathies ~ 2006
• rising global prevalence with thecumulative use of neurotoxic ARTs
• pathology involves length-dependent axonal loss, macrophage activation, and impaired regeneration. Skin biopsy is useful to define the degree of distal axonal degeneration
• animal models are now available (transgenic mice, SIV macaques) and may be useful to test therapies
• current therapies are only symptomatic, and new neuroprotective strategies are needed, as well as improved outcome measures

Johns Hopkins University:HIV Neurosciences Program:
Patients, volunteers, other investigators ~ NARC, NEAD
Clinical research/imaging:K Carter, D Esposito, M Pomper, N Sacktor, A Venkataramana, R Skolasky, A King, R Benjamin, C Odol, M Fitchett, M Greene, J Creighton
Neuropathology/Cutaneous Nerve studies: C Pardo,M Polydefkis, D Thomas, P Hauer, JW Griffin, B Freeman, B Dearman, G Ebenezer
Neuroimmunology and Models:K Conant, S Gartner, N Haughey, A Hoke, A Nath
SIV macaque: J Clements, C Zink, J Mankowski, Laast V
JHU AIDS Service/CFAR:J Bartlett, R Moore, J Gallant
$$ ~ NINDS, NIAID, NIMH, NARC, ACTG

….if your feet hurt, your whole body hurts…”
Thank you