PATHOGENESIS
27
PATHOGENESIS
-
Upload
hedwig-phillips -
Category
Documents
-
view
34 -
download
0
description
PATHOGENESIS. Shigella cause bacillary dysentery There are two types of dysentery They are : a) Amoebic dysentery b) Bacillary dysentery. AMOEBIC DYSENTERY. BACILLARY DYSENTERY. Incubation period is long Insidious onset Local abdominal tenderness Moderate tenesmus - PowerPoint PPT Presentation
Transcript of PATHOGENESIS

PATHOGENESIS
Shigella cause bacillary dysentery
There are two types of dysentery
They are : a) Amoebic dysentery
b) Bacillary dysentery
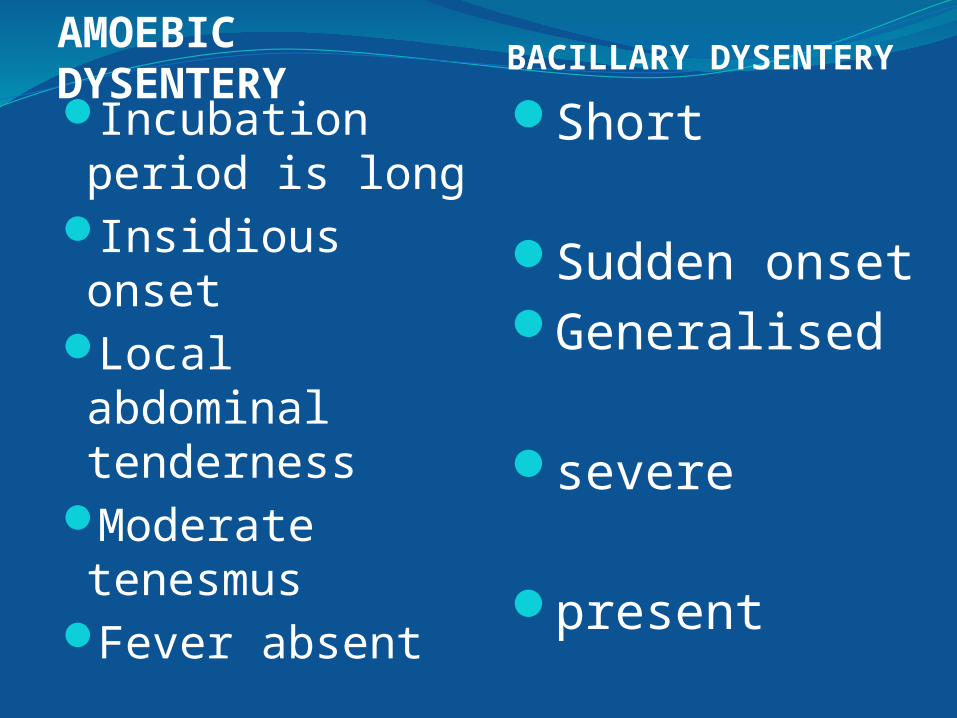
AMOEBIC DYSENTERY
BACILLARY DYSENTERY
Incubation period is long
Insidious onset
Local abdominal tenderness
Moderate tenesmus
Fever absent
Short
Sudden onsetGeneralised
severe
present
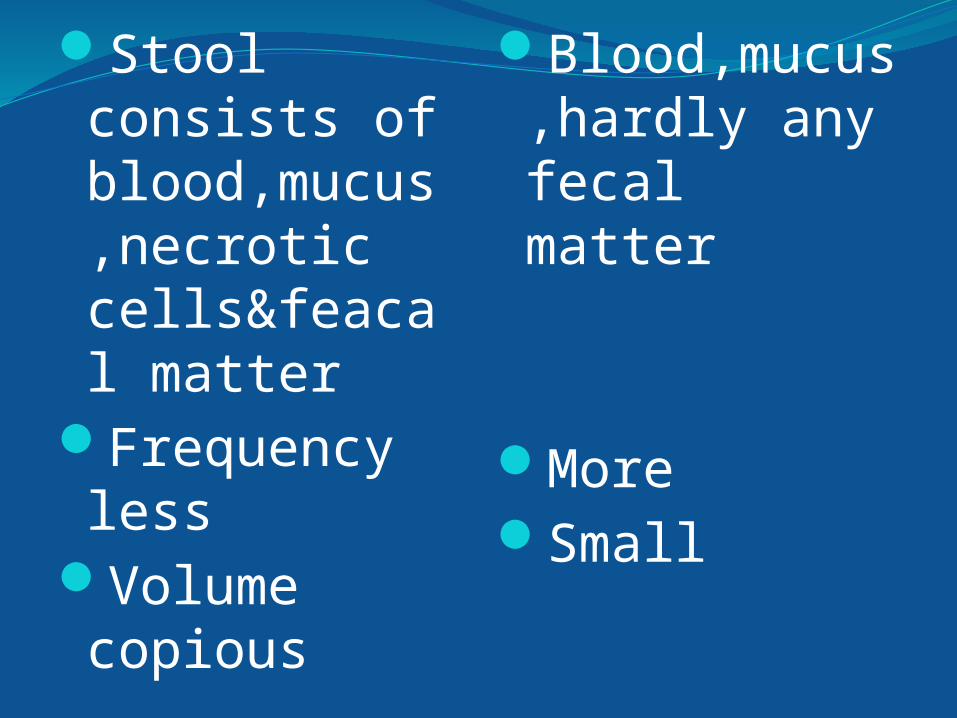
Stool consists of blood,mucus,necrotic cells&feacal matter
Frequency less
Volume copious
Blood,mucus,hardly any fecal matter
MoreSmall
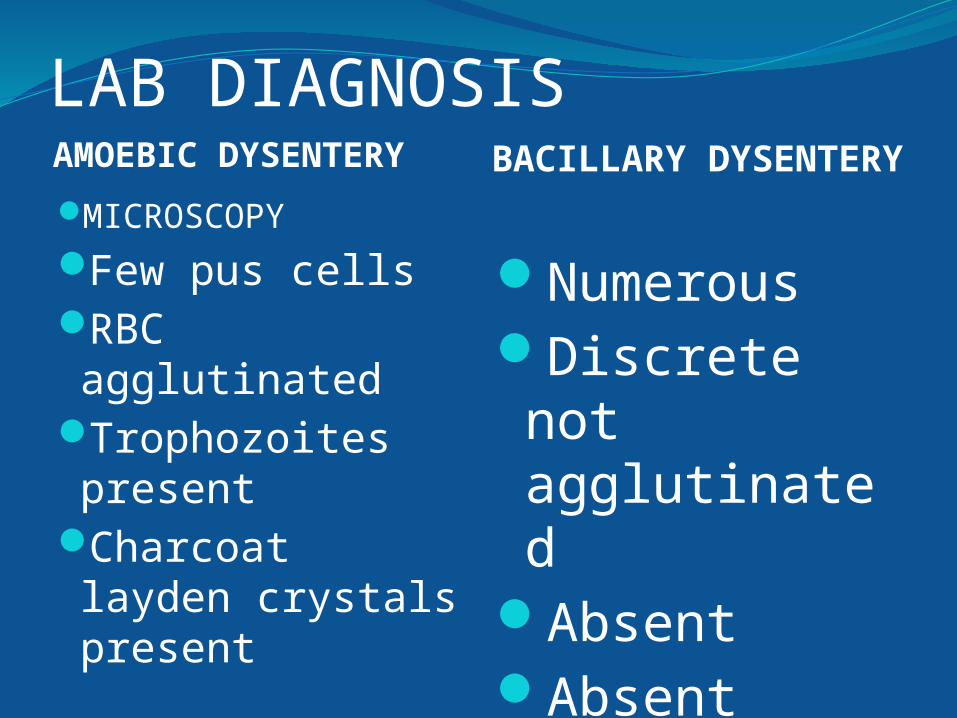
LAB DIAGNOSISAMOEBIC DYSENTERY BACILLARY
DYSENTERYMICROSCOPY
Few pus cellsRBC agglutinated
Trophozoites present
Charcoat layden crystals present
NumerousDiscrete not agglutinated
AbsentAbsent

Bacilli not demonstrated in stool culture
Mild leucocytosis in blood smear
Serum agglutination negative
Can be demonstrated
Marked leukocytosis
positive

Source-infected human beingsMode of transmission
DirectFomitesWaterContaminated foodFliesIn young male homosexuals
Minimum infective dose is low
Pathogenecity resemble that of EIEC

MECHANISM OF ACTION. Bacilli infect the epithelial cells of villi in LI multiplication Inflammatory reaction with capillary thrombosis Necrosis of epithelial cells

Sh.dysenteriae type 1 forms an exotoxin.
CONGO RED BINDING TEST.
VIRULENCE MARKERS ANTIGENS
Virulence test.

CLINICAL MANIFESTATIONS
Incubation period-1 to 7 days.
SYMPTOMSFrequent passage of loose scanty stools containing blood & mucus
Abdominal crampsTenesmusFever & vomiting
In severe cases- bacteremiaCOMPLICATIONS.
ArthritisToxic neuritis ConjunctivitisParotitisHUS

Severity ranges from mild diarrhoea to acute fulminating dysentery
The whole spectrum of infection is termed as SHIGELLOSIS.
Of 10,000 people ingested with Sh.flexneri
25% asymptomatic25% transient fever25%fever with watery diarrhoea25% typical dysentery

EPIDEMIOLOGY

Epidemics always accompanies wars,poverty,lack of sanitation.
Source-humansCasesLess often carriers

ASYLUM DYSENTERY.In USA
North-Sh.sonneiSouth-Sh.flexneri.

In INDIA ,all age groupsFlexneri 50-85%Dysentriae 8-25%Sonnei 2-24% Boydii 0-8%

In recent years,suddenly Sh. Dysentriae became virulent epidemic form.

LAB DIAGNOSIS.

Diagnosis depends on isolating bacilli from feaces.. 1.SPECIMENS.
-fresh stool -rectal swab -ideal specimen -direct swab of an ulcer.
2.TRANSPORT. Sach’s buffered glycerol saline.
3.DIRECT MICROSCOPY.Saline & Iodine preparations.4.CULTURE.MacConkey’s agarDCA
5.COLONY MORPHOLOGY&STAINING
NLFGram negativeMotility6.BIOCHEMICAL REACTIONS.Urease,citrate,H2S,KCN-negative.
7.SLIDE AGGLUTINATION

TREATMENT
Uncomplicated shigellosis-self limiting.
Dehydration has to be corrected in infants and children
Antibacterial treatment not indicatedIn severe cases-nalidixic acid,norfloxacin,other flouroquinolones.
PREVENTIONGeneral prophylaxis.Chemoprophylaxis. Immunoprophylaxis.

Thank you