Patellofemoral Arthritis · 30 Bulletin of the NYU Hospital for Joint Diseases 2009;67(1):30-8...
9
Bulletin of the NYU Hospital for Joint Diseases 2009;67(1):30-8 30 Minkowitz RB, Bosco JA III. Patellofemoral arthritis. Bull NYU Hosp Jt Dis. 2009;67(1):30-8. Abstract Patellofemoral joint arthritis is a common condition which can be extremely debilitating. Although it is a common condi- tion, the treatment of isolated patellofemoral arthritis varies and remains controversial. The objective of this review is to provide an overview of the current understanding of patel- lofemoral arthritis and various different surgical options, indications, and their respective outcomes. D avies and colleagues 1 reported in a radiological study that isolated patellofemoral arthritis is found in 9.2% of 206 knees in 174 consecutive patients older than 40 years of age. The incidence was 13.6% in females older than 60 years and 15.4% in males older than 60 years. Another study by McAlindon and associates 2 found that as many as 24% of females and 11% of males older than 55 years with symptomatic knee arthritis had isolated degeneration of the patellofemoral articulation. In a review of 31,516 arthroscopies of the knee, 4% of knees had grade IV lesions; within this 4%, 21% had patella chondral wear and 15% had wear in the trochlear groove. 3 However, despite the frequency of patellofemoral arthritis and its various predisposing factors associated with ante- rior knee pain, this condition has historically proven to be relatively refractory to treatment. This is due, in part, to the complexity of the problem, and it reflects a possible previ- ous lack of recognition of the subtleties of the biomechanics at this articulation. More recently, the understanding of the disease and the biomechanics of the joint have improved, leading to a clear picture of the management of patello- femoral arthritis. Corresponding to the spectrum of disease associated with the degeneration of the patellofemoral joint, a range of management options are currently available. 4-7 Pathoanatomy The patellofemoral joint has a unique orchestration of static elements (ligamentous and osseous) and dynamic factors (neuromuscular) that contribute to its functional capacity, among them the osseous morphology and its dysplastic variants. The primary soft tissue static stabilizers of the patellofemoral joint are the medial and lateral patellofemo- ral and patellotibial complexes. 8 Patellofemoral stability is also dependent on limb alignment, which includes varus or valgus tibiofemoral alignment as well as rotational variances in femoral version. Furthermore, the relation of the knee to pelvic position and strength has been added as an important stabilizer of the knee and the patellar elements. This complex orchestration of factors offers challenges to understanding normal, and, thus, abnormal patellofemoral joint function. 4 Patellofemoral arthritis is defined as the loss of articu- lar cartilage on one or both surfaces of the patella and in the trochlear groove, or either. The greatest prevalence of chondral wear is on the lateral patellar facet. 4 The pres- ence of lateral facet arthritis is not necessarily caused by malalignment, but it does suggest that the lateral patellar facet becomes overloaded more commonly than the central or medial aspect of the patella. This suggests that there is some degree of tilt or malalignment of force in the etiology of lateral facet arthritis. In a series of patients with PF arthri- tis managed with patellofemoral arthroplasty, 61 out of 72 knees (85%) required some form of realignment procedure Patellofemoral Arthritis Reuven B. Minkowitz M.D., and Joseph A. Bosco III, M.D. Reuven B. Minkowitz M.D., was a Chief Resident in the Depart- ment of Orthopaedic Surgery, NYU Hospital for Joint Diseases, and is currently in Sports & Joint Reconstruction with Kaiser Permanente, Lancaster, California. Joseph A. Bosco III, M.D., is Assistant Professor, New York University School of Medicine, and Vice Chairman for Clinical Affairs, Department of Orthopaedic Surgery, NYU Hospital for Joint Diseases, NYU Langone Medical Center, New York, New York; [email protected]. Correspondence: Joseph Bosco, M.D., Department of Orthopaedic Surgery, Suite 1402, East 17th Street, New York, New York 10003; [email protected].
Transcript of Patellofemoral Arthritis · 30 Bulletin of the NYU Hospital for Joint Diseases 2009;67(1):30-8...

Bulletin of the NYU Hospital for Joint Diseases 2009;67(1):30-830
Minkowitz RB, Bosco JA III. Patellofemoral arthritis. Bull NYU Hosp Jt Dis. 2009;67(1):30-8.
Abstract
Patellofemoral joint arthritis is a common condition which can be extremely debilitating. Although it is a common condi-tion, the treatment of isolated patellofemoral arthritis varies and remains controversial. The objective of this review is to provide an overview of the current understanding of patel-lofemoral arthritis and various different surgical options, indications, and their respective outcomes.
Davies and colleagues1 reported in a radiological study that isolated patellofemoral arthritis is found in 9.2% of 206 knees in 174 consecutive patients
older than 40 years of age. The incidence was 13.6% in females older than 60 years and 15.4% in males older than 60 years. Another study by McAlindon and associates2 found that as many as 24% of females and 11% of males older than 55 years with symptomatic knee arthritis had isolated degeneration of the patellofemoral articulation. In a review of 31,516 arthroscopies of the knee, 4% of knees had grade IV lesions; within this 4%, 21% had patella chondral wear and 15% had wear in the trochlear groove.3
However, despite the frequency of patellofemoral arthritis and its various predisposing factors associated with ante-rior knee pain, this condition has historically proven to be relatively refractory to treatment. This is due, in part, to the
complexity of the problem, and it reflects a possible previ-ous lack of recognition of the subtleties of the biomechanics at this articulation. More recently, the understanding of the disease and the biomechanics of the joint have improved, leading to a clear picture of the management of patello-femoral arthritis. Corresponding to the spectrum of disease associated with the degeneration of the patellofemoral joint, a range of management options are currently available.4-7
PathoanatomyThe patellofemoral joint has a unique orchestration of static elements (ligamentous and osseous) and dynamic factors (neuromuscular) that contribute to its functional capacity, among them the osseous morphology and its dysplastic variants. The primary soft tissue static stabilizers of the patellofemoral joint are the medial and lateral patellofemo-ral and patellotibial complexes.8 Patellofemoral stability is also dependent on limb alignment, which includes varus or valgus tibiofemoral alignment as well as rotational variances in femoral version. Furthermore, the relation of the knee to pelvic position and strength has been added as an important stabilizer of the knee and the patellar elements. This complex orchestration of factors offers challenges to understanding normal, and, thus, abnormal patellofemoral joint function.4 Patellofemoral arthritis is defined as the loss of articu-lar cartilage on one or both surfaces of the patella and in the trochlear groove, or either. The greatest prevalence of chondral wear is on the lateral patellar facet.4 The pres-ence of lateral facet arthritis is not necessarily caused by malalignment, but it does suggest that the lateral patellar facet becomes overloaded more commonly than the central or medial aspect of the patella. This suggests that there is some degree of tilt or malalignment of force in the etiology of lateral facet arthritis. In a series of patients with PF arthri-tis managed with patellofemoral arthroplasty, 61 out of 72 knees (85%) required some form of realignment procedure
Patellofemoral Arthritis
Reuven B. Minkowitz M.D., and Joseph A. Bosco III, M.D.
Reuven B. Minkowitz M.D., was a Chief Resident in the Depart-ment of Orthopaedic Surgery, NYU Hospital for Joint Diseases, and is currently in Sports & Joint Reconstruction with Kaiser Permanente, Lancaster, California. Joseph A. Bosco III, M.D., is Assistant Professor, New York University School of Medicine, and Vice Chairman for Clinical Affairs, Department of Orthopaedic Surgery, NYU Hospital for Joint Diseases, NYU Langone Medical Center, New York, New York; [email protected]. Correspondence: Joseph Bosco, M.D., Department of Orthopaedic Surgery, Suite 1402, East 17th Street, New York, New York 10003; [email protected].

31Bulletin of the NYU Hospital for Joint Diseases 2009;67(1):30-8
at the time of arthroplasty.9 This suggests that patellofemoral malalignment can and often does lead to some presentations of patellofemoral arthritis. In summary, many factors have been thought to contribute to abnormal pathomechanics leading to pain in the patello-femoral joint. These include patella alta, trochlea dysplasia, an increased quadriceps or Q angle with secondary soft tissue problems, a weakened or hypoplastic vastus medialis oblique quadriceps muscle with a contracted lateral retinaculum, and an absent redundant medial patellofemoral ligament or the latter alone. These often lead to abnormal forces across the patella resulting in secondary degenerative changes to the articular surfaces of the patellofemoral joint. Other causes may include microtrauma and macrotrauma, weight and activity level, and genetic quality of the cartilage.10
Clinical PresentationIn general, patellofemoral pain is typically exacerbated by activities such as stair climbing and descent, ambulating on hills, rising from a seated position, sitting with the knee flexed, and squatting. Walking on level ground is typically less painful. Most patients will describe crepitus at the an-terior aspect of the knee.7
Physical examination is somewhat nonspecific; crepitus and effusions are common. Leslie and Bentley11 found that quadriceps wasting greater than 2 cm, effusions, and retropatellar crepitus were the best physical predictors of articular breakdown on the patella. By closely document-ing the degree of knee flexion at which maximal pain is elicited with compression of the articular surfaces of the patellofemoral joint, one can gain insight into the location of the articular lesion. More distal lesions are painful early in the flexion arc, and proximal lesions are not symptomatic until a position deep in flexion. The standard work-up for these patients includes a thor-ough review of the history and a careful physical examination of the axial alignment as well as the patellofemoral joint. A routine series of radiographs is made for all patients; these include standing anteroposterior, 45° posteroanterior flex-ion weightbearing,12 and lateral and skyline13 radiographs, as well as a 54 inch (1.37 m) axial alignment radiograph. When maltracking is suspected on clinical examination, a computed tomography (CT) scan can be performed to assess lateral patellar subluxation, the presence of dysplasia of the trochlea, and patellar height (Fig. 1). With this information, the underlying etiology of maltracking may be addressed.
Nonsurgical TreatmentMost patellofemoral joint pathology can initially be treated by nonoperative means.6,7,14 Conservative treatment is the mainstay of isolated patellofemoral arthritis; relatively few patients ultimately require surgical intervention. A directed therapy program emphasizing short arc quadriceps strength-ening, isometrics, stretching of the lateral retinacular struc-tures, and preservation of motion is frequently successful
in mitigating symptoms. There is some evidence to suggest that vastus medialis obliquus dysfunction may be associated with patellofemoral pain, which reinforces the importance of a directed strengthening program.6 Additionally, considering the excessive loads to which the anterior compartment of the knee is exposed, a supervised program of weight reduction can also be beneficial. Avoiding provocative maneuvers such as ascending and descending stairs, squatting, jumping, and biking can help minimize the loads of the patellofemoral joint and reduce the pain from arthritis. Additionally, anti-inflammatory medications or analgesics and intra-articular injections of corticosteroids or hyaluronans may be effective adjuvant therapeutic options. Furthermore, although data is lacking, patellar unloading sleeves, braces, or taping may play a role in the nonsurgical management of this condi-tion.6,15 In patients who fail to respond to a minimum of 3 to 6 months of conservative management, surgical management may be considered.16
Limited Surgical InterventionSome patients with patellofemoral arthritis have significant synovitis or a localized osteophyte such that a targeted resec-tion may bring considerable relief.17 Yercan and coworkers18 have shown that a lateral facetectomy can be palliative in many patellofemoral arthritis patients. Partial lateral fac-etectomy was performed on 11 knees in patients with an average age of 62 years and a mean follow-up of 8 years. An average Knee Society Score improved from a preoperative score of 150 to a score of 176. They conclude partial lateral facetectomy is relatively simple and an effective surgical
Figure 1 CT Axial view of the knee demonstrating PF arthritis with lateral subluxation.

Bulletin of the NYU Hospital for Joint Diseases 2009;67(1):30-832
treatment for middle-aged to elderly active patients with isolated lateral patellofemoral osteoarthritis who want to maintain activity level. Lateral release is a realignment procedure that historically has been widely used for the treatment of anterior knee pain. Studies have shown that an arthroscopic lateral retinacular release relieves anterior knee pain when there is radio-graphic documentation of pathologic lateral patellar tilt in the absence of patellar instability.19,20 The commonly held belief that a lateral retinacular release causes the patella to move medially is not borne out by biomechanical studies. The vector of the lateral retinaculum is a posterior lateral vector. One investigation revealed that cutting the lateral retinaculum resulted in a 10% decrease in the lateral re-straining force.21 This operation, therefore, whether open or arthroscopic, should be used only when there is a contracture of the lateral retinaculum that tethers the lateral border to the patella posterolaterally and when this is a source of pain or pressure-creating forces, or both, in the patellofemoral compartment. It should not be performed for instability. Aderinto and Cobb19 reviewed the results at an average of 31 months after arthroscopic lateral retinacular release in 53 patients with patellofemoral arthritis (with or without concomitant femorotibial arthritis). Four patients required a knee replacement within 18 months. Of the remaining 49 patients, 26 had isolated patellofemoral arthritis. Thirteen of those 26 patients were very satisfied or satisfied with the result of the lateral release, whereas the other 13 were dissat-isfied. Unfortunately, the investigators did not differentiate between patients with lateral arthritis and those with global (patellar and trochlear) involvement. Therefore, isolated lateral retinacular release in the treat-ment of patellofemoral arthritis may have some applicability when the following factors are present: 1. lateral patello-femoral arthritis on one or both sides of the patellofemoral joint, 2. radiographic evidence of tilt without subluxation, and 3. no clinical history of instability. Combining this re-lease with a partial lateral facetectomy when there is a large osteophyte may increase its clinical utility.4
Another alternative described is a concomitant application of arthroscopic debridement and lateral release. Satisfac-tory results are possible for patients with minimal arthritis of the lateral facet who have patellar tilt and minimal or no subluxation.19,20 In the face of clinically important arthritis, however, it should be understood that debridement and release have limited goals with typically incomplete and unpredictable pain relief and may often be precursors to the eventual need for more definitive interventions.
Autologous Chondrocyte ImplantationAutologous chondrocyte implantation is indicated in the management of focal chondral defects in the knee.4,5,10,22 The cartilage space must be documented as intact on standard radiographs to indicate that the overall joint space is patent, the margins are well shouldered, and the cartilage loss is not
diffuse, but contained. When a patient is considered a candidate for autologous chondrocyte implantation, arthroscopy is performed to as-sess the diameter and depth of the lesion and any maltrack-ing. A cartilage biopsy specimen is also obtained from the non-weightbearing portion of the superior intercondylar notch at this point for the cell culture process. Approximately 200 to 300 mg of articular cartilage is sent in a sterile trans-port medium to be commercially cultured and cryopreserved. The transplantation procedure is then performed. Technical issues that are specific to autologous chondrocyte implanta-tion in the patellofemoral joint include a suture technique that restores the articular surface shape of the patella and the trochlea, as well as a soft-tissue tensioning at the end of the procedure that allows the normal medial-to-lateral and proximal-to-distal patellar glide without overstuffing the patellofemoral joint. Typically, patients start to have pain relief by 4 to 6 months after surgery. Non-impact sports activities are commenced at 9 months postoperatively, and full-impact activities are begun by 18 months postoperatively. Maximal improvement may take as long as 3 years for patients who have large areas of chondrocyte implantation, as additional time is needed for graft maturation.
Results of ImplantationWhen autologous chondrocyte implantation (ACI) is being considered for the repair of a cartilage defect, it is critical that the etiology and the underlying cause or abnormal pathomechanics of the defect are accurately identified. The diagnosis and correction of these underlying abnormalities are crucial to a successful outcome with autologous chon-drocyte implantation. It is now clear that a failure to fully appreciate this point explains the disappointing early re-sults of resurfacing of the patella. In a study from Sweden published in 1994, autologous chondrocyte transplantation was successful (a good or excellent result) in only two of seven patients.23
However, in a larger series in which patellar tracking was also addressed at the time of transplantation, results are improved. Minas and Bryant10 followed 45 patients that had ACI subdivided into treatment groups: (I) isolated patella, n = 8; (II) isolated trochlea, n = 9; (III) patella plus trochlea, n = 4; (IV) weightbearing condyle plus patella, n = 2; (V) weightbearing condyle plus trochlea, n = 2; and (VI) weightbearing condyle plus patella plus trochlea n = 20. Osteotomy was performed (29 of 45 patients, 64%) in patients who had tibiofemoral malalignment, patellofemoral malalignment, or both. At 4-year follow-up (average), there were 11 patients (24%) whose procedures failed. Three of these were caused by failures of the weightbearing condyle ACI graft. The other eight failures (18%) were caused by a patella or a trochlea graft failure (which was evidenced by delamination or detachment of the graft from the adjacent cartilage and subchondral bone). One must take into consid-

33Bulletin of the NYU Hospital for Joint Diseases 2009;67(1):30-8
eration, that of the 11 patients with a Workers Compensation claim, five had a graft failure. Yet, in the patient survey, 71% of patients rated their outcomes as good or excellent, 22% rated outcome as fair, and 7% rated outcome as poor.
DiscussionAccording to Fulkerson,6 cartilage transplantation of the trochlea is an entirely different matter than resurfacing the patella. Loading of any unit area of the trochlea is transient, compared with loading of any area on the patella. Because the mechanics of patellofemoral contact allow for gliding of a unit surface area of the patella for substantially more time during the flexion arc than any corresponding part of the trochlea, the demands on patellar articular cartilage are much greater. Patellar articular cartilage, therefore, must be extremely durable. Furthermore, patellar subchondral bone is dense and the normal cartilage resurfacing techniques may not work as well on this less inviting surface. When there has been overload on the patella, such as the excessive lateral pressure syndrome, subchondral bone of the patella can become extremely dense. This can make autologous osteochondral implantation very difficult. The punches used to remove osteochondral grafts and to create recipient sites may not cut the subchondral patellar bone. The importance of correcting the underlying cause of the chondral injury cannot be underestimated. Pidoriano and colleagues22 demonstrated that with the anteromedial tibial tubercle osteotomy, a successful clinical outcome correlates with the location of the patellar articular lesion. Patients with type I (inferior pole) or type II (lateral facet) lesions were substantially more likely to have a good or excellent result than were those with type III (medial facet) or type IV (proxi-mal pole or diffuse) lesions. Central trochlear lesions were associated with medial patellar lesions, and these patients had a poorer result. Localization of the articular cartilage injury at the time of reconstruction is therefore important to determine whether osteotomy alone may predict a successful outcome. The data in the study by Minas and Bryant10 showed that when type III and IV chondral injuries to the patella as well as the central part of the trochlea were resurfaced, patients surprisingly had good clinical pain relief and improved function regardless of whether there had been preexisting patellofemoral maltracking requiring a Fulkerson osteotomy. The osteotomy effect alone would not account for the high success rate, according to the results described by Pidoriano and associates,22 because of the size and location of these chondral defects. Therefore, the additional role of autologous chondrocyte implantation benefit is seen. These results are similar to those found by Peterson and coworkers,5 who addressed patellar maltracking at the time of surgery or corrected it prior to the time of autologous chondrocyte implantation. The results in their patients re-mained durable for up to 10 years after implantation. These are excellent outcomes for patients with difficult problems.
Autologous chondrocyte implantation is indicated for the treatment of choice for disabling anterior knee pain resulting from large erosive chondral defects (4 to 6 cm2) when the radiographic joint space remains intact and the joint is well aligned. However, when collapse of the joint space can be seen on the Merchant or skyline radiograph, cartilage repair with autologous chondrocyte implantation is no longer pos-sible. The procedure relies on intact, full-thickness cartilage margins to maintain the joint space so that the growing cartilage repair tissue may fill the defect. With joint space collapse, a unicompartmental patellofemoral or total knee arthroplasty may be considered.4
Osteotomies of the Tibial Tubercle Tibial tubercle transfers are thought to help by alleviating pressure from the arthritic portion of the patellofemoral joint, allowing symptomatic relief. Maquet24 was the first to de-velop a procedure that moves the tibial tuberosity anteriorly. This osteotomy was reviewed by Schepsis and colleagues25 as an alternative to patellofemoral replacement. The theory behind this technique is to diminish load on a defective or arthritic patella. Results with straight anteriorization proce-dure were compromised by complications of skin necrosis and compartment syndrome. This procedure, therefore, has been used infrequently, mainly because of the deformity created by excessive anteriorization of the tibial tubercle and the concern about skin necrosis, nonunion, and compartment syndrome. The tendency with such surgery, which involves placing a bone block behind the elevated tibial tubercle, is to anteriorize too much, sometimes with disastrous results.6
To select the correct osteotomy, one must understand that moving the tibial tubercle anteriorly shifts contact on the patella such that more proximal patellar articular cartilage comes into contact earlier in the flexion arc. This is highly desirable when there is a distal patellar articular lesion that can be taken out of contact by anteriorization of the tibial tubercle. Most patients with malalignment-related patello-femoral breakdown have lateral and distal articular lesions. Anterior and medial transfer of the tibial tubercle, then, is well suited for the typical patient with malalignment-related patellofemoral breakdown.26
The key principles in successful tibial tubercle transfer for the treatment of patellofemoral arthritis are as follows:
1. Restore or maintain proper balance of the extensor mechanism.
2. Transfer load off a painful, degenerated area onto better cartilage. Transfer the tibial tuberosity medi-ally to unload the lateral aspect of the patella and anteriorly to unload the distal aspect of the patella.
3. Address retinacular sources of pain.4. Perform tibial tubercle transfer in a way that allows
early motion and prompt healing.26
Tibial tubercle transfer in the treatment of patellofemo-ral arthritis is particularly attractive for younger patients. When properly indicated, tibial tubercle transfer allows the
Bulletin of the NYU Hospital for Joint Diseases 2009;67(1):30-834
potential for a permanent solution to patellofemoral arthritis pain and dysfunction related to malalignment. The surgeon must first determine the part of the patellofemoral joint that needs to be unloaded by reviewing the findings of a detailed history, physical examination, radiographs with the knee in 45° of flexion combined with precise lateral views; magnetic resonance imaging scans, and arthroscopy. All of the findings of these studies should correlate. For example, if the patient sustained a dashboard injury or a crush injury of the patel-lofemoral joint with the knee in flexion, the patellar articular lesion is likely to be proximal since this area articulates with the femur when the knee is flexed. Once the location of a pain-producing lesion has been documented, the osteotomy design should be straightfor-ward. If there is a lateral articular lesion and lateral track-ing, the patella may be moved medially with use of a Trillat (straight medial) tibial tubercle transfer. If there is a purely
distal articular lesion with healthy proximal cartilage with normal alignment (relatively uncommon), a straight ante-riorization of the tibial tubercle is most appropriate. If the patella has been overloaded medially from previous surgery and there is medial articular cartilage breakdown, sometimes associated with medial patellar subluxation, anterolateral tibial tubercle transfer may be most appropriate.4,27
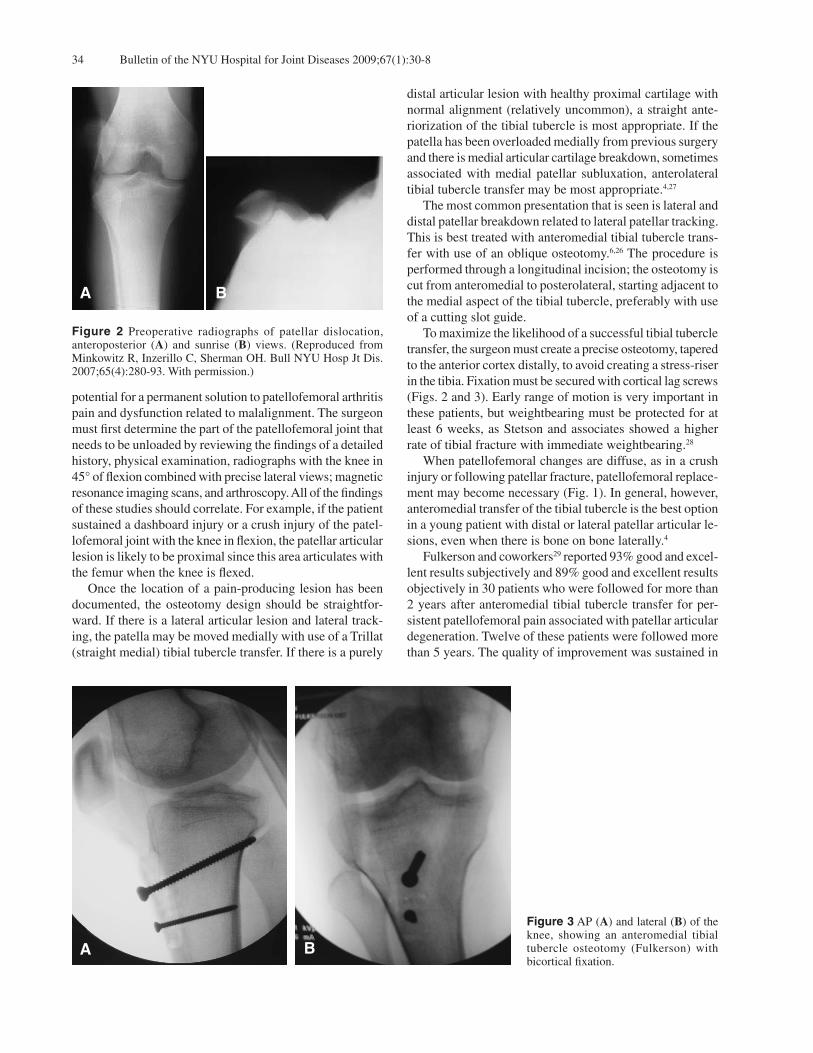
The most common presentation that is seen is lateral and distal patellar breakdown related to lateral patellar tracking. This is best treated with anteromedial tibial tubercle trans-fer with use of an oblique osteotomy.6,26 The procedure is performed through a longitudinal incision; the osteotomy is cut from anteromedial to posterolateral, starting adjacent to the medial aspect of the tibial tubercle, preferably with use of a cutting slot guide. To maximize the likelihood of a successful tibial tubercle transfer, the surgeon must create a precise osteotomy, tapered to the anterior cortex distally, to avoid creating a stress-riser in the tibia. Fixation must be secured with cortical lag screws (Figs. 2 and 3). Early range of motion is very important in these patients, but weightbearing must be protected for at least 6 weeks, as Stetson and associates showed a higher rate of tibial fracture with immediate weightbearing.28
When patellofemoral changes are diffuse, as in a crush injury or following patellar fracture, patellofemoral replace-ment may become necessary (Fig. 1). In general, however, anteromedial transfer of the tibial tubercle is the best option in a young patient with distal or lateral patellar articular le-sions, even when there is bone on bone laterally.4
Fulkerson and coworkers29 reported 93% good and excel-lent results subjectively and 89% good and excellent results objectively in 30 patients who were followed for more than 2 years after anteromedial tibial tubercle transfer for per-sistent patellofemoral pain associated with patellar articular degeneration. Twelve of these patients were followed more than 5 years. The quality of improvement was sustained in
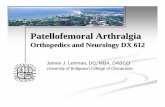
Figure 2 Preoperative radiographs of patellar dislocation, anteroposterior (A) and sunrise (B) views. (Reproduced from Minkowitz R, Inzerillo C, Sherman OH. Bull NYU Hosp Jt Dis. 2007;65(4):280-93. With permission.)
BA
Figure 3 AP (A) and lateral (B) of the knee, showing an anteromedial tibial tubercle osteotomy (Fulkerson) with bicortical fixation.
BA

35Bulletin of the NYU Hospital for Joint Diseases 2009;67(1):30-8
all 12 of the patients who were evaluated again after more than 5 years from surgery. When examined separately, 75% of those patients with advanced patellar arthrosis achieved a good result; none of these patients achieved an excellent result. In addition, postoperative continuous passive motion has markedly reduced the incidence of stiffness. Fulkerson concludes,6,26,27,29 that anteromedial transfer of the tibial tubercle is mechanically and clinically successful for alleviating intractable pain related to patellar malalign-ment and articular degeneration. This procedure enables the majority of appropriately selected patients with malalign-ment and patellar articular degeneration to resume increased levels of activity with substantially diminished pain.
PatellectomyRemoval of the patella (patellectomy) is a radical approach to relieving chronic patellofemoral pain related to severe patellar articular loss and chronic pain.30 Patients may benefit from patellectomy because the source of pain, the patella, is eradicated. The primary problem with patellectomy is chronic weakness and extensor lag. Patients frequently take an unduly long time to achieve functional strength for daily activities. Additionally, wear on the trochlea related to the tendon tracking on trochlear articular cartilage occurs with time. Nonetheless, complete patellectomy is a relatively simple and safe operation that can reliably decrease chronic patellofemoral pain related to the patella itself. The trade-off is a significant decrease in knee extension strength. It is extremely important to centralize the extensor mechanism and to avoid transecting the tendinous portion of the extensor mechanism when removing the patella. Therefore, removal through a longitudinal split and careful peeling out of the patella seems to be the best approach. Patellectomy, when viewed as a salvage procedure, is a reasonable alternative when the patella itself is severely degenerated and the trochlea is relatively intact. As with any patellofemoral salvage procedure, the extensor mechanism should be normally aligned at the time of patellectomy. It is unclear which patients should have patellectomy versus patellofemoral arthroplasty, but an important criterion is the maintenance of better strength after patellofemoral replace-ment.6
Patellofemoral Arthroplasty The patellofemoral replacement McKeever screw-on Vital-lium patellar shell was introduced in 1955.31 Blazina32 and Lubinus33 further developed McKeever’s concept in resurfac-ing both sides of the patellofemoral articulation. In 1979, Lubinus and Blazina introduced the first total patellofemoral arthroplasty.33,34
Patellofemoral arthroplasty has played a limited role in patella femoral arthritis. The original descriptions of the procedure did not include strict criteria, technical pitfalls were not yet appreciated, and little emphasis was placed on realignment of the extensor mechanism of the knee.
Consequently, reports pertaining to the earliest designs showed disappointing results. In Europe, this led to efforts to redesign the implant and improve the operative technique, and in the United States most surgeons simply abandoned the procedure.7
Patellofemoral arthroplasty, when compared to a total knee arthroplasty, has the potential advantages of retaining the menisci and cruciate ligaments and, thereby, the natural kinematics of the knee joint; however, the shortcoming of this procedure to date has been the durability of the arthro-plasty. For example, in a study of 76 knees, the Lubinus prosthesis had a failure rate of 50% at 8 years.35 The main reasons for failure have been persistent malalignment, wear, impingement, and disease progression. However, in the past 5 years newer device designs that more accurately reduplicated patellofemoral joint function have been introduced. In 2005, Ackroyd and Chir36 reported results of the Avon patellofemoral replacement, which is specifically designed to address the reasons for the failure described above. The design is based on the patellofemoral compartment of the Kinemax Plus total knee replacement (Howmedica, Rutherford, New Jersey). The femoral flange is shallow and broad, allowing unconstrained capture of the patella into a deeper trochlea with flexion. The patellar button is offset and chamfered on its medial side to create an odd facet and avoid impingement on the medial femoral condyle in deep flexion. The femoral component is lateral-ized slightly and externally rotated to aid patellar tracking (Fig. 4). An added advantage of the use of components based on a total knee design is that even if the patellofemoral replace-ment is not successful, this design facilitates later conver-sion to a total knee replacement. Lonner and colleagues, in 2006,37 reported good results on 12 patients converted to total knee arthroplasty from a patellofemoral arthroplasty, with a mean follow-up of 3.1 years. In this study they reported that Knee Society clinical and functional scores increased from 57 points preoperatively to 96 points and from 51 points preoperatively to 91 points, respectively. They conclude, “The results of total knee arthroplasty do not seem to be compromised after revision of the failed patellofemoral replacement.” Ackroyd and Chir36 performed 306 patellofemoral arthroplasties in 240 patients. Initial results show a high level of pain relief and improvement in function. There has been no deterioration in pain or function with follow-up at 5 years, and there were no late complications attributable to the arthroplasty. Disease progression in the tibiofemoral joint has occurred in 14 patients (16 knees, 5%) requiring revision in 10 of these patients (11 knees, 3.6%). Persistent anterior knee pain was recorded in 14 knees (4%). Sisto and Sarin, in 2006,38 reported results in 25 custom patellofemoral arthroplasties The customization was de-signed to recreate the patient’s own anatomy and address the inherent problems associated with off-the-shelf designs.

Bulletin of the NYU Hospital for Joint Diseases 2009;67(1):30-836
A software program utilizing a CT scan constructed a three-dimensional model of the patient’s femoral groove, which was converted into a cobalt chromium custom implant. At a mean follow-up of 73 months (6 years) all 25 implants were in place and functioning well. There were 18 excellent and seven good results. The mean Knee Society functional score was 89 points, and the mean Knee Society objective score was 91 points. No patient had required additional surgery or had component loosening. The early results of these new patellofemoral prostheses seem to be encouraging, with considerable improvement in pain, range of movement, and function. The procedure can produce consistently good quality functional results in appropriate patients and has the major advantage of preserv-ing the tibiofemoral joint, with normal menisci and cruciate ligaments. Patient selection for patellofemoral arthroplasty should be limited to patients with isolated patellofemoral osteo-arthrosis or posttraumatic arthrosis, after exhausting ap-propriate nonsurgical interventions. The procedure should not be done in patients with inflammatory arthritis or cal-cium pyrophosphate dihydrate crystal deposition disease (CPPD).39 It is most effective for treating patellofemoral dysplasia, but it should be used cautiously in patients with considerable maltracking or malalignment with an excessive Q angle. However, slight patellar tilt from lateral retinacular contracture and subluxation from trochlear dysplasia are not contraindications for this procedure. In such cases, a lateral retinacular release may be necessary at the time of arthroplasty, and a prosthesis accommodating of even subtle malalignment can address the dysplasia.39 The presence of tibiofemoral arthrosis is a contraindication for patello-femoral arthroplasty. Sisto and Sarin38 and Lonner39 have advocated patellofemoral arthroplasty rather than total knee arthroplasty or patellectomy for patients younger than 55 years with isolated anterior compartment arthrosis. Elderly patients may be better suited to total knee arthroplasty be-
cause of its remarkable track record and proven survivorship, and because some degree of tibiofemoral chondromalacia is ubiquitous in more elderly patients.4,39
Total Knee ArthroplastyThe use of total knee arthroplasty for the treatment of isolated patellofemoral arthritis has recently been reported as an effective method of managing this condition in older age-groups.40 This approach is not advocated for younger patients with isolated patellofemoral arthritis. Mont and as-sociates41 reported on 33 patients with an average follow-up of 81 months, who underwent total knee replacement for the treatment of severe patellofemoral arthritis in patients older than 55 years of age. There were 28 excellent, one good, and one poor result. The mean Knee Society objective score was 93 points (range, 67 to 100 points). They concluded that total knee arthroplasty is a viable treatment option in patients older than 55 with primarily severe patellofemoral disease and that realignment procedures and other osseous procedures such as patellectomy can be avoided. Careful adherence to correct techniques and compo-nent alignment are well recognized as being crucial to the success of any total knee arthroplasty. These issues are of even more critical importance in the treatment of isolated patellofemoral disease and its typical association with ab-normal mechanics and alignment. Particular attention must be directed toward the correction of extensor mechanism alignment, and, indeed, it has been found that the rate of lateral retinacular release in these patients is as high as 68%, which is as much as three times that of standard total knee arthroplasty.40
In another study, Laskin and van Steijn40 reported on 42 patients who were managed with total knee replacement for the treatment of primary patellofemoral arthritis. After a mean duration of follow-up of 4.2 years, these patients had superior knee scores (mean, 96 points) compared to a matched group of patients with tricompartmental arthritis
Figure 4 From left to right, AP, lateral, and sunrise views of a patellofemoral arthroplasty.
A B C

37Bulletin of the NYU Hospital for Joint Diseases 2009;67(1):30-8
(mean, 88 points). The investigators concluded that the re-sults of total knee replacement in the patellofemoral disease subgroup were as good as or superior to those in the group of patients with tricompartmental arthritis. The results of that study are in agreement with those of the study of Mont and coworkers, in which excellent or good clinical results were obtained in 29 (97%) of thirty knees.41
The debate regarding the use of this procedure currently centers on the fact that it may appear that a tricompartmental arthroplasty is an excessive response to a unicompartmental condition. Although more conservative approaches, in par-ticular patellofemoral arthroplasty (which has had increas-ingly encouraging results), would be theoretically more satisfactory, total knee arthroplasty currently remains the most proven and predictable single procedure in this specific population of older patients with patellofemoral disease.4,40,41 Total knee arthroplasty, therefore, remains a reasonable op-tion for these patients until its reliably excellent results can be equaled by other interventions.
ConclusionDespite the progress in the treatment of patellofemoral ar-thritis, it remains difficult to achieve absolute unanimity on the best course of treatment for a given patient. Therefore, although the standards for treatment of patellofemoral arthri-tis are not fully resolved, there are currently many exciting areas of progress. Most of these future spheres of progress are expected to be in the field of orthobiologics for carti-lage restoration and in improved designs of patellofemoral replacements. These advances offer considerable promise that this previously poorly managed spectrum of disease will ultimately prove amenable to a defined set of graduated interventions; thus, ensuring satisfactory symptomatic and functional outcomes for patients.
Disclosure StatementNone of the authors have a financial or proprietary interest in the subject matter or materials discussed, including, but not limited to, employment, consultancies, stock ownership, honoraria, and paid expert testimony.
References1. Davies AP, Vince AS, Shepstone L, et al. The radiologic
prevalence of patellofemoral osteoarthritis. Clin Orthop Relat Res. 2002;(402):206-12.
2. McAlindon TE, Snow S, Cooper C, Dieppe PA. Radiographic patterns of osteoarthritis of the knee joint in the community: the importance of the patellofemoral joint. Ann Rheum Dis. 1992;51(7):844-9.
3. Curl WW, Krome J, Gordon ES, et al. Cartilage injuries: a review of 31,516 knee arthroscopies. Arthroscopy. 1997;13(4):456-60.
4. Saleh KJ, Arendt EA, Eldridge J, et al. Symposium. Operative treatment of patellofemoral arthritis. J Bone Joint Surg Am. 2005;87(3):659-71.
5. Peterson L, Brittberg M, Kiviranta I, et al. Autologous
chondrocyte transplantation. Biomechanics and long-term durability. Am J Sports Med. 2002;30(1):2-12.
6. Fulkerson JP. Alternatives to patellofemoral arthroplasty. Clin Orthop Relat Res. 2005;(436):76-80.
7. Grelsamer RP. Patellofemoral arthritis. J. Bone Joint Surg Am. 2006;88:1849-60.
8. Arendt EA, Fithian DC, Cohen E. Current concepts of lateral patella dislocation. Clin Sports Med. 2002;21(3):499-519.
9. Cartier P, Sanouiller JL, Grelsamer R. Patellofemoral arthroplasty. 2-12-year follow-up study. J Arthroplasty. 1990;5(1):49-55.
10. Minas T, Bryant T. The role of autologous chondrocyte im-plantation in the patellofemoral joint. Clin Orthop Relat Res. 2005;(436):30-9.
11. Leslie IJ, G. Bentley. Arthroscopy in the diagnosis of chon-dromalacia patellae. Ann Rheum Dis. 1978;37(6):540-7.
12. TD Rosenberg, LE Paulos, RD Parker, et al. The forty-five-degree posteroanterior flexion weight-bearing radiograph of the knee. J Bone Joint Surg Am. 1988;70:1479-83.
13. Merchant AC, Mercer RL, Jacobsen RH, Cool CR. Roent-genographic analysis of patellofemoral congruence. J Bone Joint Surg Am. 1974;56:139-6.
14. Post WR, Fulkerson J. Knee pain diagrams: correlation with physical examination findings in patients with anterior knee pain. Arthroscopy. 1994;10(6):618-23.
15 McConnell J. Management of patellofemoral problems. Man Ther. 1996 Mar;1(2):60-6.
16. Barrack RL, Booth RE Jr, Lonner JH, et al. Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rose-mont, Illinois: American Academy of Orthopaedic Surgeons, 2006, pp. 71-77.
17. Kasim N, Fulkerson JP. Resection of clinically localized segments of painful retinaculum in the treatment of se-lected patients with anterior knee pain. Am J Sports Med. 2000;28(6):811-4.
18. Yercan HS, Ait Si Selmi T, Neyret P. The treatment of patel-lofemoral osteoarthritis with partial lateral facetectomy. Clin Orthop Relat Res. 2005;(436):14-9.
19. Aderinto J, Cobb AG. Lateral release for patellofemoral arthritis. Arthroscopy. 2002;18(4):399-403.
20. Shea KP, Fulkerson JP. Preoperative computed tomography scanning and arthroscopy in predicting outcome after lateral retinacular release. Arthroscopy. 1992;8(3):327-34.
21. Burks RT, Desio SM, Bachus KN. Biomechanical evalu-ation of lateral patellar dislocations. Am J Knee Surg. 1998;11(1):24-31.
22. Pidoriano AJ, Weinstein RN, Buuck DA, Fulkerson JP. Correlation of patellar articular lesions with results from anteromedial tibial tubercle transfer. Am J Sports Med. 1997;25(4):533-7.
23. Brittberg M, Lindahl A, Nilsson A, et al. Treatment of deep cartilage defects in the knee with autologous chondrocyte transplantation. N Engl J Med. 1994;331:889-95.
24. Maquet P. [Subcutaneous Rupture of the Tendon of Achilles]. Rev Med Liege. 1963;18:520-1. [French]
25. Schepsis AA, DeSimone AA, Leach RE. Anterior tibial tu-bercle transposition for patellofemoral arthrosis: a long-term study. Am J Knee Surg. Winter 1994;7:13-20.
26. Fulkerson JP. Patellofemoral pain disorders: evaluation and management. J Am Acad Orthop Surg. 1994;2(2):124-32.

Bulletin of the NYU Hospital for Joint Diseases 2009;67(1):30-838
27. Fulkerson JP. Diagnosis and treatment of patients with patel-lofemoral pain. Am J Sports Med. 2002;30(3):447-56.
28. Stetson WB, Friedman MJ, Fulkerson JP, et al. Fracture of the proximal tibia with immediate weightbearing after a Fulkerson osteotomy. Am J Sports Med. 1997;25(4):570-4.
29. Fulkerson JP, Becker GJ, Meaney JA, et al. Anteromedial tibial tubercle transfer without bone graft. Am J Sports Med. 1990;18(5):490-6; discussion 496-7.
30. Kelly MA, Brittis DA. Patellectomy. Orthop Clin North Am. 1992;23(4):657-63.
31. McKeever DC. Patellar prosthesis. J Bone Joint Surg Am. 1955;37(5):1074-84.
32. Blazina ME, Fox JM, Del Pizzo W, et al. Patellofemoral replacement. Clin Orthop Relat Res. 1979;(144):98-102.
33. Lubinus, H. Patella glide bearing total replacement. Ortho-pedics. 1979;2:119-27.
34. Blazina ME, Fox JM, Del Pizzo W, et al. Patellofemoral replacement. 1979. Clin Orthop Relat Res. 2005;(436):3-6.
35. Tauro B, Ackroyd CE, Newman JH, Shah NA. The Lubinus
patellofemoral arthroplasty. A five- to ten-year prospective study. J Bone Joint Surg Br. 2001;83(5):696-701.
36. Ackroyd CE, Chir B, Development and early results of a new patellofemoral arthroplasty. Clin Orthop Relat Res. 2005;(436):7-13.
37. Lonner JH, Jasko JG, Booth RE Jr. Revision of a failed patel-lofemoral arthroplasty to a total knee arthroplasty. J Bone Joint Surg Am. 2006;88(11):2337-42.
38. Sisto DJ, Sarin VK. Custom patellofemoral arthroplasty of the knee. J Bone Joint Surg Am. 2006;88(7):1475-80.
39. Lonner JH. Patellofemoral arthroplasty: pros, cons, and design considerations. Clin Orthop Relat Res. 2004;(428):158-65.
40. Laskin RS, van Steijn M. Total knee replacement for pa-tients with patellofemoral arthritis. Clin Orthop Relat Res. 1999;(367):89-95.
41. Mont MA, Haas S, Mullick T, Hungerford DS. Total knee arthroplasty for patellofemoral arthritis. J Bone Joint Surg Am. 2002;84(11):1977-81.