
Partnerships To Meet Primary Care and ACO Challenges … · Care & ACO Challenges in Behavioral...
43
Partnerships To Meet Primary Care & ACO Challenges in Behavioral Health Northwest Regional Telehealth Resource Center Annual Conference – March 24, 2014 Portland, Oregon Maureen Ideker RN, BSN, MBA Essentia Health Duluth, MN
Transcript of Partnerships To Meet Primary Care and ACO Challenges … · Care & ACO Challenges in Behavioral...

Partnerships To Meet Primary Care & ACO Challenges in
Behavioral Health
Northwest Regional Telehealth Resource Center Annual Conference – March 24, 2014
Portland, Oregon
Maureen Ideker RN, BSN, MBA Essentia Health Duluth, MN

Disclosure • Practice Gap: Lack of awareness on how to provide specialty care
services to under-served populations in the region. • Desired Outcome: • Providers will be able to apply knowledge acquired from the
conference to better provide care using telemedicine to patients across the region.
• Providers will be able to solve problems within their practice using telemedicine.
• Providers will be able to identify the services available for their patients via telemedicine within their region.
• Providers will be able to recognize the changes in telemedicine and how best to continue improving their practices during change.
• Disclosure of relevant financial relationships in the past 12 months: I have no relevant financial relationships with commercial interests that may have a direct bearing on the subject matter of this CME activity.

Essentia Health Telehealth Network – 2 Years Old
Telehealth Programs: Hospital Services:
• Behavioral Health • Emergency Department • Hospitalist • Stroke Care • Toxicology
Clinic Services:
• Allergy • Behavioral Health • Cardiology – Congestive Heart Failure • Cardiology – Electrophysiology • Chronic Pain Management • Dermatology
Essentia Health Telehealth Network
• Dietician Services • Infectious Disease • Medical Weight Loss • Medication Therapy Management • Nephrology • Rehab Therapy • Urology • Wound Care • 109 Telehealth Providers • 23 sites

Accountable Care Organization
• Moving from Fee for Service to
Population Health • Using Health Care Homes Across
Essentia Clinics – (top 10% of sickest patients)
• How does behavioral health fit into this?

A Story of…..
• A mental health patient in crisis seeking help in the Fosston, MN CAH ER
• No access to mental health professionals for assessment or assistance
• Long ER wait • Carrie, SW calls for help from Telehealth • NWMHC, Crookston, MN identified as a willing
partner

Life Expectancy Differences
• “The gap in life expectancy in patients with
a mental illness and the general population has widened since 1985 and efforts to reduce this gap should focus on improving physical health.”
Lawrence D., 2013

http://www.integration.samhsa. gov/research
• Center for Integrated Health Solutions
(CIHS) • This is the “national home” for promoting
the integration of behavioral health and primary care

“Target interventions that improve quality of life outcomes” • Ohio (1998-2002) study of 608 patient deaths
from pts. admitted to a public mental health hospital, cause of death:
• Heart Disease 126 • Suicide 108 • Obesity 144 • Hypertension 136
Miller B.J., 2006

ACO Typical Strategies Providing Care • Increase Units • Decrease Direct Costs
(personnel, supplies, etc.) • Maximize Prices • Cost Based Pricing • Chase Your Tail
(Revenues Exceed Costs)
Managing Health • Increase Population Served • Manage Opportunities to
Decrease Utilization, Improve Quality
– Transition of Care – Care Coordination – Clinical Pathways – Reduce Unnecessary Care
• Improve Health of Members • Decrease Direct Costs • Price Based Costing • Manage to a Target (TCOC)

Accountable Care What’s New?
From To Volume (FFS) Value
Reactive Care Proactive Care
Physician Centered Patient Centered
Fragmented Information Electronic Health Record
Electronic Health Record Data Mining, Population Analytics
Individual Care Individual & Population Health

Essentia’s Strategy for Becoming an ACO
• Create New Models of Care • Establish Tools and New Competencies to
Manage the Health of a Defined Population
• Common Electronic Medical Record Across Essentia
• Common Electronic Business Platform

A Few Cost the Most
% of Population
% of Total Healthcare Expense
Mean Annual Cost per Person
1%
9%
20%
70%
Source: Thomson Reuters Markets can Database
29%
39%
21%
11%
$101,000
$15,000
$3,700
$580
National Sample of 21 Million Insured Americans, 2003-2007

The Role of Clinical Care in Outcomes
University of Wisconsin (UW)
Population Health Institute Annual County Health
Rankings
Mortality (length of life) 50%
Morbidity (quality of life) 50%Health Outcome
Tobacco Use
Diet & Exercise
Alcohol Use
Unsafe Sex
Health Behaviors(30%)
Access to Care
Quality of Care
Clinical Care(20%)
Education
Employment
Income
Family & Social Support
Community Safety
Social & Economic Factors(40%)
Environmental Quality
Built Environment
Physical Environment
(10%)Programs
and Policies
Health Factors
County Health Rankings model © 2010 UWPHI

We are Called to Make a Healthy Difference in Peoples Lives
How are 97,000 patients eligible for colonoscopy doing?
Across The U.S. • Behavioral Health patients with other complex
illnesses have worse health outcomes • All MN & ND counties are in Mental Health
Professional Service Areas • MN has a joint effort going to improve outcomes by
forming primary care collaboration with behavioral health providers……INTEGRATION
24/7 Tele-Behavioral Health Services
• Established between Fosston, MN CAH Emergency Room &Clinic
• With the Northwest MN Mental Health Center at Crookston, MN (25 miles away.)
• Crisis Center and 1 hour response time

Goals: • Decrease behavioral health crisis occurrences thru
improved access
• Assist with ER disposition decisions for behavioral health patients in crisis
• Decrease crisis bottlenecks in ER
• Reduce unnecessary transfers to inpatient unit
• Improve rural ER & primary care services
Global initiatives • Similar goals in University Hospital of North Norway
• 2012 research being conducted regarding their on-call system for psychiatric emergencies. Their goals included … (strengthening collaboration & coordination.) Trondsen M.V., et al, 2012
• A United Kingdom 2007 nursing study of mental health emergency assessments of 375 people showed 12.8% or 45 were admitted. Zip code analysis showed a difference in a socio-economic factors between affluent @ 5% and deprived @ 19% that influenced admission referrals. Brooker C., et al, 2007

How:
• Use both secure broadband networks for videoconference telehealth connections during week days 9 – 5 p.m.
• Use mobile devices I-Pads (not IPhones) and
home laptops with hot spots after hours and on week-ends.

Improved access using telehealth and through increased awareness
and use of NWMHC overall.
• Daily referrals to NWMHC • Use of crisis center via telehealth • Emergency Room referral to crisis team
after hours via telehealth – 1 hr. response time.

Equipment • Mobile video cart – wireless in ER @ Fosston
(shared with Clinic)
• Desktop PC with Video software & camera @ NWMHC
• Mobile devices with hot spots – for 22 mental health providers
• Broadband – 5 up, 10 down both sites
• Problems @ NWMHC – disrupted office to hospital/clinic functioning and postponed Go-Live.
Process Excellence Tools used
• Charter • Workflow Process Maps (NWMHC &
Fosston ER, Clinic • Implementation Checklist • Education Plan including Pilot • Timeline of Key Events • E-Learning Module (DVD)

Charter
Our Mission: We are called to make a healthy difference in people’s lives
Project Title: EH-Fosston-Behavioral Health-Design SPE Name: Nancy Tario (Maureen Ideker Bus. Lead)
An opportunity exists to provide additional access to health care and behavioral health services for the Fosston service area patients receiving telehealth. This can be achieved by services from Northwest Mental Health Center, Crookston, MN, a community mental health agency offering crisis services 24/7. Same day, timely services will be provided for the emergency department and the clinic via interactive videoconferencing and/or on-site appointments either at Crookston or Fosston.
Baseline (FY13): Behavioral health crisis ED & Clinic patients: ER = 12/year Clinic = 566/year Total = 578 NWMHC Zip code analysis of Fosston 56542 area = 417 clients Health Care Home patients with behavior health co-morbidity with mental health provider active = out of 73 enrolled, 2 have Mental Health with Co-Morbidities and 2 have a mental health provider.
OPPORTUNITY/PROBLEM STATEMENT Each behavioral health patient in crisis in the ED or clinic has increased access to professional in behavioral health. Fosston pts in the service area of both NWMHC and EH-Fosston will grow by 10%. Decreased by 25% of EH-Fosston ED disposition problems for behavioral crisis pts/provider team. Financial Impact: Prevention of unnecessary admissions/transfers (avoided costs) for behavioral health patients; revenue through clinic facility fees for telehealth visits; Expected Benefit: Reduce ER patients from 12 to 9 (25%) Avoided costs @ 3 pts./year @ $2000 day x 3 days = $18,000. Facility fees @ 12 pts/month x $24 each = $288.00 (Net ACO benefit = $24,144 per year).
TARGETED PROJECT GOAL(S)/FINANCIAL IMPACT
IN: Essentia Health Fosston NWMHC
OUT: Any other facility, except SMSH
CONSTRAINTS: Available time for Telehealth visits by professionals at NWMHC.
PROJECT SCOPE
Team: Maureen Ideker, Director Telemedicine; Shauna Reitmeier, NWMHC; Lynae Finseth, Fosston; Carrie Nephew, SW Fosston; Brian Kittelson, IS Duluth; Nancy Tario, Process Excellence; Mike Anderson, MSW NWMHC; Brenda Dale, Supervisor Front Desk NWMHC; Jason Stewart, IS Fargo; Abe Deusterman, IS Fosston; Lela Hier, NWMHC IS; Devra Carlson, Director of Hospital Patient Care Fosston; Holly Wagner, Scheduling Manager Fosston; Naomi Hagen, Clinic Nurse Manager Fosston; Kathy Anderson, Financial Director NWMHC
Business Owners: Maureen Ideker, Teri Gunnarson MD & Lynae Finseth, Fosston; Shauna Reitmeier, CEO NWMHC
Resource: Martin Sinclair, Atty.; Kevin Gish, Administrator Graceville & Fosston; Kim Bodensteiner, CFO Fosston SPE/Coach: Nancy Tario_ Sponsor: John Smylie, COO EH SLT: John Smylie COO EH Finance Contact: Wayne Anderson – Financial Analyst Duluth
START DATE January 2013
DEFINE January 2013
MEASURE June 23, 2013
ANALYZE September 1, 2013
DESIGN November 1, 2013 VERIFY April 30, 2014
PHASE COMPLETION TARGETS
P1 We will provide convenient, timely, coordinated care & support. P4 We will excel in efficient & effective operations. P5 We will transform to thrive in a new healthcare environment.
STRATEGY MAP ALIGNMENT
TBD
BSC MEASUREMENT
• Provide stable & consistent coverage by behavioral health • Improve quality pt. handoffs from CA hospital (pt. safety &
community) • Provide admission decision support to avoid unnecessary
transfers • Improved provider productivity • Improved access for patients
PATIENT AND MISSION IMPACT
PROJECT RESOURCES
Rev 8-28-2013 NT
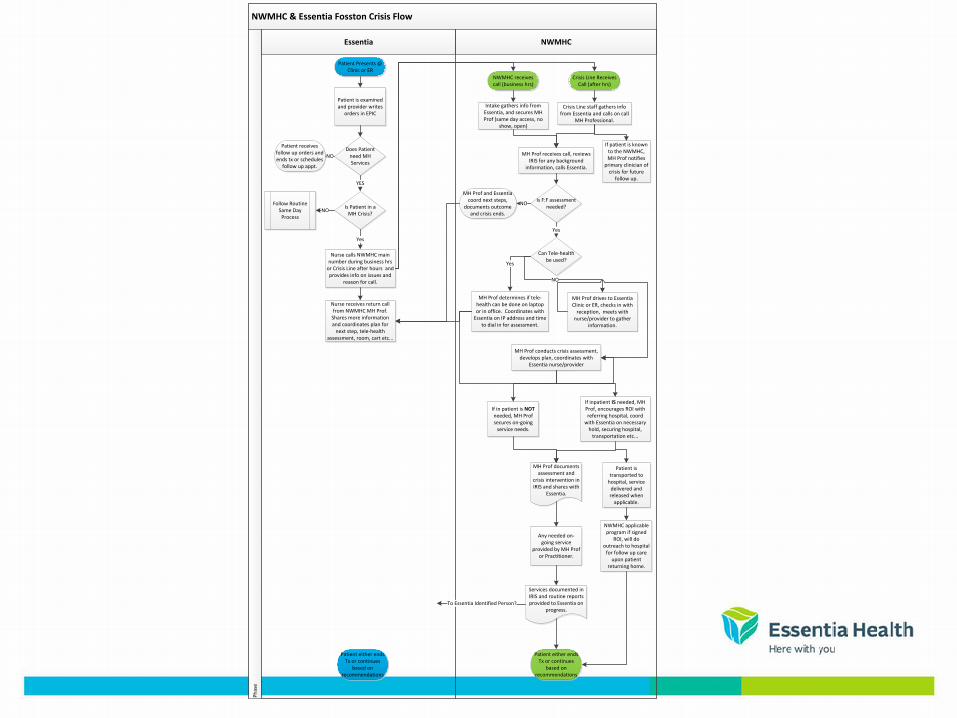
NWMHC & Essentia Fosston Crisis Flow
Essentia NWMHC
Phas
e
Patient Presents @ Clinic or ER
Patient is examined and provider writes
orders in EPIC
Does Patient need MH Services
Is Patient in a MH Crisis?
Patient receives follow up orders and ends tx or schedules
follow up appt.
Nurse calls NWMHC main number during business hrs
or Crisis Line after hours and provides info on issues and
reason for call.
Intake gathers info from Essentia, and secures MH Prof (same day access, no
show, open)
Patient either ends Tx or continues
based on recommendations
Patient either ends Tx or continues
based on recommendations
NWMHC receives call (business hrs)
YES
NO
Follow Routine Same Day
ProcessNO
Crisis Line Receives Call (after hrs)
Crisis Line staff gathers info from Essentia and calls on call
MH Professional.
MH Prof receives call, reviews IRIS for any background
information, calls Essentia.
Is F:F assessment needed?
If patient is known to the NWMHC, MH Prof notifies
primary clinician of crisis for future
follow up.
Can Tele-health be used?
MH Prof determines if tele-health can be done on laptop or in office. Coordinates with
Essentia on IP address and time to dial in for assessment.
MH Prof drives to Essentia Clinic or ER, checks in with
reception, meets with nurse/provider to gather
information.
MH Prof conducts crisis assessment, develops plan, coordinates with
Essentia nurse/provider
If inpatient IS needed, MH Prof, encourages ROI with referring hospital, coord
with Essentia on necessary hold, securing hospital,
transportation etc...
MH Prof documents assessment and
crisis intervention in IRIS and shares with
Essentia.
If in patient is NOT needed, MH Prof secures on-going
service needs.
Patient is transported to
hospital, service delivered and released when
applicable.
NWMHC applicable program if signed
ROI, will do outreach to hospital
for follow up care upon patient
returning home.
Any needed on-going service
provided by MH Prof or Practitioner.
Services documented in IRIS and routine reports provided to Essentia on
progress.
Yes
Nurse receives return call from NWMHC MH Prof.
Shares more information and coordinates plan for
next step, tele-health assessment, room, cart etc...
Yes
Yes
NO
MH Prof and Essentia coord next steps,
documents outcome and crisis ends.
NO
To Essentia Identified Person?


Privileging & Credentialing • Privileged and credentialed 22 Behavioral
Health Professionals: • Psychiatric Nurse Practitioner • Licensed Independent Clinical Social Worker • Licensed Marriage and Family Therapist • Master’s prepared Social Worker • All reimbursable providers in MN

Go-Live: November 1, 2013 Revised 8/14/2013 NTDELIVERABLES ACTION REQUIRED STATUS RESPONSIBLE DUE DATE
Develop charter and type draft Complete (need baseline data) Maureen/Nancy 6/15/2013Site Visit: Develop Agenda and Conduct Gap Analysis Draft Implementation Plan Maureen/Nancy 7/31/2013Establish Telehealh Implementation Team (suggested members below): Maureen/Hub/Admin/Spokes 7/31/2013
Clinic & administrative leadership (clinic adminstrator, dept. manager or designee) from both hub and spoke sites. 7/31/2013Telehealth team (Maureen Ideker, RN Director; Adam Meier & Brian Kittelson, IT; Kimberly Shropshire, Admin Assistant; Nancy Tario, SPE 7/31/2013Provider(s) from Hub 7/31/2013Compliance/Legal from Hub 7/31/2013Privileging, Credentialing and Payer Enrollment from Hub 3rd Thursday September 7/31/2013Direct user NPMH: Champion - Chris Green, Julene Brown, Fosston: Kim Bodensteiner NW: Shauna, Kathy, Lynae, Kevin Gish, Holly Wagner 7/31/2013Reimbursement Analysists for coverage guidelines, coding, and billing from hub and spokes 7/31/2013Marketing Department member Added Vanessa Hughes 7/31/2013
Conduct in-person meetings with administration and medical staff
One with NWMHC visit. EH & NWMHC meet monthly to do case mgmt. Create a cheat sheet w/NWMHC.
Maureen/Dr. Gunnarson/Clinic & Hospital Adminstration 5/31/2013
Presentation by Specialist provider to rural Medical Staff
Initial Complete. Do again after the flow process at med staff meeting 2nd Friday. Rural Clinic Admin/Provider 10/11/2013
Patient Brochure CompletedMedical Staffs at Hub & Spoke CompletedStaff newsletter (external for NWMHC) Will e-mail NWMH: Colleen McCray
Implementation Plan: TeleBehavioral Health Fosston/NWMHC Project
Preparation
Team
Communications

Gray = Completed Updated 9/26/2013 NAT
COMPLETE BY: ACTIVITIES RESPONSIBLE
7/31/2013 Rapid Cycle Event - Gap Analysis Maureen/Nancy
8/26/2013 Super User Training (Mary Dirdhl, Brittany Djernes) Maureen/Brian/Abe
8/14/2013Implementation Team meets every 2 weeks via conference calls, 2nd & 4th Thursday 10:30 AM Kimberly put on calendar
8/15/2013 Send intake pkts from NWMHC to EH - Fosston Brenda & Holly
8/26/2013 IS Testing Brian, Abe, Andy & NWMHC
9/1/2013 FY13 Query / Clarity Maureen/Dr. Gunnarson
9/1/2013 Equipment Checks Leela, Naomi, Devra
9/1/2013 Marketing - Contact Vanessa Hughes (Fargo) & Patty Flaa (Fosston) Maureen
Sept-OctInternal Communication - all staff meeting (Hospital, Clinic, LT Care, Home Health) Lynae & Carrie
9/1/2013Registration (done) & Scheduling & Practice NWMHC/EH - mock patient - both sides? Leela, Brenda & Holly
9/10/2013Documentation: (1) define turn-around time (2) e-mail In-Basket, Fax'd - Ward Clerk, group (Fosston Registration?) Naomi & NWMHC
10/1/2013 Clinic Skills Fair Naomi
9/15/2013 Resource Manual Lynae & Nancy
9/15/2013 Contract - draft form. Talked to Martin Sinclair - few pieces missing. Shauna & Kevin
9/17/2013 NWMHC Crisis Meeting (Kick Off Inservice) Naomi & Lela (NWMHC)
9/17-10/17/2013 Piloting/Demo/Testing (NWMHC & EH)Leela, Devra, Naomi, Abe &
Andy
9/18/2013 Credentialing Shauna & Kevin
9/20/2013 ER Nurses/Hospital Skills and Demo Devra
10/11/2013 Medical Staff Demo - EH Naomi, Devra, Abe & Andy
10/14/2013 Begin Daily Checks NWMHC/Leela
11/1/2013 Go Live
3/31/2014 Verification completed
Timeline of Key EventsFosston - NWMHC TeleBehavioral Health Project
Clinical Concerns from Hospital/Clinic
• Response times to ER for crisis
• Getting documentation quickly
• Failed experience previously
• Technical/equipment malfunctions

Overcoming a previously failed Tele-Behavioral Health experience
• Pilot Program prior to go live • Twice daily live connection checks 8 am, 5pm (built
familiarity with equipment for daily use & built relationships between sites and providers)
• 22 licensed providers practiced live connections 4 times
each (From office, home, in-town, to ER and to Clinic) • Mobile device connectivity validated for each provider,
hot-spots used • I-Phones didn’t work
Successes • Increased use of NWMHC services for both crisis
and preventative services, underutilized before
• 22 licensed Behavioral providers privileged & credentialed at hospital and clinic, relationship development
• Highly skilled IT teams worked together
• Strengthened relationships all around
• Started week night & Week-end coverage first
Patient Outcomes
• As the relationships between Fosston and NWMHC grew, during 2013:
• 6- mental health hospitalizations were prevented • (4 –used the Stabilization Unit) • (2-used Crisis Center at Crookston) • During 2014: • (1 –used Crisis Center) • (1-assessed as not needing mph.
hospitalization)

Improved access thru telehealth helps reduce “No-Shows”.
• Idaho example in 2011 showed 10% improvement, from 33% to 20% in one year (1)

Barriers • Lack of Broadband Capacity at NWMHC
hindered QOS, postponed a successful Go-Live
• Restricted IT resources at NWMHC for investment in infrastructure
• Contracted IT assistance at NWMHC added months of “stalling the Go-Live”
• Time-lapse between training and Go-Live
Broadband Changes caused Internal NWMHC problems
• Program started with providing after hours and weekend crisis Telehealth outreach.

Corporate Concerns • Contract negotiations – “Ownership” of the
patient
• Access to the medical record
• Getting the documentation into the secure electronic medical record
• Billing directly vs. contracting with the hospital (A potential deal-breaker!)

ACO Metrics • Reduced overall use and costs of medical resources
• Decreased ER visits
• Avoided inpatient behavioral health admits
• Decreased medical admissions
• Improved “Community Measures” in clinic-physical health and prevention
• Non-ACO: maintained employment

Documentation/Communication
• “Direct e-mail”
• Scanned to EMR
• Communicate with ER RN after visit
• Call or video with ER or referring provider immediately after visit

Reference Sources:
• Brooker C., et al, 2007, Journal of Clinical Nursing 16, 1313-1322
• County Health Model C 2010 UWPHI • Grantham, D. Behavioral Healthcare: Oct
20122; 31, 7; Pro Quest Medical Library • http://www.integration.samhsa.gov/research • Lawrence D.,Telethon Institute for Child Health
Research, the University of Western Australia (Press Office) 2013

References • Miller, BJ et al. Psychiatric Services, 2006 Oct,
57 (10): 1482-7 • Reitmeier S, Northwestern Mental Health
Center, Crookston MN Feb.2014 (Ph: 218- 281-3940)
• Smylie J, Essentia Health Senior Leadership Retreat, Duluth, MN, Sept. 2013
• Thomson Rueters Markets can Database • Trondsen M.V., et al, BMC (Bio Med Central)
Health Services Research 2012, 12 – 470
Maureen Ideker, MBA, BSN, RN [email protected]








![The Richard Merkin Initiative on Payment Reform and ... · PART 2: INNOVATIONS IN CARE . RGV ACO Diabetes Care Plan . The mission of the RGV ACO is to “[improve] the quality of](https://static.fdocuments.us/doc/165x107/5ed15a04fc37b04d07005cb8/the-richard-merkin-initiative-on-payment-reform-and-part-2-innovations-in-care.jpg)









