PARTICIPANTS MANUAL 2017 - 2018 Improving ... · PARTICIPANTS MANUAL 2017 - 2018 Improving...
26
PARTICIPANTS MANUAL 2017 - 2018 Improving Immunocytochemistry for over 25 Years UK NEQAS ICC & ISH is part of the Cancer Institute at the University College London, Gower Street, London WC1E 6HX UK NEQAS ICC & ISH Finsbury Business Centre 40 Bowling Green Lane, Room 127, London, EC1R 0NE, UK Tel: (+44) (0) 20 7415 7065 Fax: (+44) (0) 20 7415 7048 [email protected] Director: Mr. Keith Miller Acting Manager: Suzanne Parry www.ukneqasiccish.org
Transcript of PARTICIPANTS MANUAL 2017 - 2018 Improving ... · PARTICIPANTS MANUAL 2017 - 2018 Improving...
PARTICIPANTS MANUAL 2017 - 2018
Improving Immunocytochemistry for over 25 Years
UK NEQAS ICC & ISH is part of the Cancer Institute at the University College London, Gower Street, London WC1E 6HX
UK NEQAS ICC & ISH Finsbury Business Centre 40 Bowling Green Lane, Room 127, London, EC1R 0NE, UK Tel: (+44) (0) 20 7415 7065 Fax: (+44) (0) 20 7415 7048 [email protected]
Director: Mr. Keith Miller Acting Manager: Suzanne Parry
www.ukneqasiccish.org

Participants Manual 2017-2018
NEQ MP7 2017-2018 © UK NEQAS ICC & ISH Page 1 of 26
TABLE OF CONTENTS
1.0 INTRODUCTION .................................................................................................................. 3
1.1 Modules and Accreditation (ISO 17043) ..................................................................................................... 3
1.2 Benefits of UK NEQAS ICC & ISH Membership ............................................................................................ 3
1.3 International EQA Service ........................................................................................................................... 4
1.4 Educational Remit of the Service ................................................................................................................ 4
1.5 Registration & Subscription ........................................................................................................................ 4
1.6 Subcontracted Services .............................................................................................................................. 4
2.0 GUIDELINES & PROCEDURES .......................................................................................... 5
2.1 Slide Distribution and Placement of NEQAS and In‐house Controls ............................................................ 5
2.2 Antibody Not Stocked ................................................................................................................................ 5
2.3 Web Based Data Entry System and Accessing Online Reports .................................................................... 5
2.4 Assessment Procedure ............................................................................................................................... 5
2.5 Assessment Scoring and Interpretation ...................................................................................................... 6
2.5.1 General assessment guide ......................................................................................................................... 6
2.5.2 Breast HER2 IHC assessment guide ........................................................................................................... 7
2.5.3 Gastric HER2 IHC assessment guide ........................................................................................................... 8
2.5.4 ALK NSCLC IHC assessment guide .............................................................................................................. 9
2.6 In‐house Tissue Recommendations ............................................................................................................ 9
2.6.1 All Modules .............................................................................................................................................. 10
2.6.2 Breast Hormonal Receptor Module ......................................................................................................... 10
2.6.3 Breast HER2 IHC Module ......................................................................................................................... 10
2.6.4 Gastric HER2 IHC Module ........................................................................................................................ 10
2.7 Participant Reports .................................................................................................................................. 10
2.7.1 Individual Participant Reports ................................................................................................................. 11
2.7.2 Graphical Data ......................................................................................................................................... 11
2.7.3 Technical Data ......................................................................................................................................... 11
2.7.4 Selected ‘Best Methods’ in Reports ......................................................................................................... 12
2.7.5 Photographic examples: Acceptable and unacceptable .......................................................................... 12
2.7.6 Immunocytochemistry E‐Journal ............................................................................................................. 13
2.8 Poor Performance Monitoring of (UK Clinical Laboratories Only) ............................................................. 13
2.8.1 Generic modules (all modules except Breast, Gastric IHC and ALK NSCLC IHC) ...................................... 14
2.8.2 Biomarker modules (Breast ER/PR IHC, Breast HER2 IHC, Gastric HER2 IHC, ALK NSCLC IHC and Breast HER2 ISH) ................................................................................................................................................................. 14
2.8.3 Breast HER2 ISH ....................................................................................................................................... 15
2.9 End of Year Performance Record / Certificate of Participation ................................................................. 16
2.10 Meetings & Practical Workshops .............................................................................................................. 16
3.0 IMMUNOCYTOCHEMISTRY MODULES .......................................................................... 16
3.1 MODULE 1: General Pathology ................................................................................................................. 16

Participants Manual 2017-2018
NEQ MP7 2017-2018 © UK NEQAS ICC & ISH Page 2 of 26
3.2 MODULE 2: Breast Pathology ‐ Hormonal Receptors ................................................................................ 17
3.3 MODULE 3: Breast Pathology ‐ HER2 Immunocytochemistry .................................................................... 17
3.4 MODULE 4: Lymphoid Pathology .............................................................................................................. 17
3.5 MODULE 5: Neuropathology .................................................................................................................... 17
3.6 MODULE 6: Cytopathology ....................................................................................................................... 17
3.7 MODULE 7: Alimentary Tract Pathology ................................................................................................... 18
3.7.1 Module 7A: Stromal tumours of the GI Tract (GIST) ................................................................................ 18
3.7.2 Module 7B: Lynch Syndrome/ Mismatch Repair Protein ........................................................................ 18
3.8 MODULE 8: Gastric HER2 IHC .................................................................................................................... 18
3.9 MODULE 9: Breast HER2 ISH ..................................................................................................................... 18
3.10 MODULE 10: NSCLC ALK IHC ..................................................................................................................... 18
4.0 IN-SITU HYBRIDISATION MODULES .............................................................................. 18
4.1 Breast HER2 ISH Interpretive Module 9A: ................................................................................................. 18
4.1.1 Interpretive Assessment procedure ........................................................................................................ 18
4.2 Breast HER2 ISH Technical Module 9B: ..................................................................................................... 19
4.2.1 Technical assessment .............................................................................................................................. 19
4.3 Troubleshooting Interpretive and Technical module Results .................................................................... 20
5.0 PERSONNEL & ASSESSORS .......................................................................................... 20
5.1 Key Personnel & Assistance ...................................................................................................................... 20
5.2 Assessor List ............................................................................................................................................. 21
6.0 APPEALS, COMPLAINTS & CONFIDENTIALITY ........................................................... 22
6.1 Appeals Procedure and Assistance ........................................................................................................... 22
6.2 Complaints Procedure .............................................................................................................................. 22
6.3 Confidentiality Policy ............................................................................................................................... 22
7.0 PROSPECTIVE NEW MODULES...................................................................................... 22
7.1 PD‐L1 in NSCLC ......................................................................................................................................... 22
8.0 ASSOCIATED SCHEMES AND MODULES ..................................................................... 22
8.1 Cellular Pathology Techniques .................................................................................................................. 22
8.2 Molecular Pathology EQA scheme ............................................................................................................ 22
9.0 TERMS & CONDITIONS .................................................................................................... 23
10.0 SELECTED REFERENCES ............................................................................................... 23
10.1 Publications .............................................................................................................................................. 23
10.2 Books ....................................................................................................................................................... 24
11.0 STEERING COMMITTEE FOR TECHNICAL SCHEMES IN CELLULAR PATHOLOGY 24

Participants Manual 2017-2018
NEQ MP7 2017-2018 © UK NEQAS ICC & ISH Page 3 of 26
1.0 INTRODUCTION The External Quality Assessment Scheme for Immunocytochemistry was founded in 1985 by Mr Gerry Reynolds at Mount Vernon Hospital, Middlesex. In 1988, the UK Department of Health recognised the scheme and from that time, it became known as the UK National External Quality Assessment Scheme for Immunocytochemistry (UK NEQAS-ICC) until ISH was added. 1.1 Modules and Accreditation (ISO 17043) Currently the UK NEQAS ICC & ISH scheme offers assessments in 10 different immunocytochemistry modules and 1 in situ-hybridisation module. These are carried out at approximately 3-monthly intervals throughout the fiscal year. Current modules include:
Details of each module can be found in the pages that follow. Participants are encouraged to participate in those modules that are compatible with the range of immunocytochemistry performed in their laboratory.
Accredited EQA Service The UK NEQAS ICC & ISH modules are currently accredited (see table above) by UKAS to the internationally recognised standard ISO 17043: Conformity assessment - General requirements for proficiency testing 1.2 Benefits of UK NEQAS ICC & ISH Membership
Comply with the requirements of ISO15189 regarding participation in EQA scheme for the provided modules
Four assessment runs are carried out per year Specific modules cater for the specialised areas of pathology Two antigens are assessed per assessment run for all Generic IHC modules (one antigen for the
Breast, Gastric & NSCLC ALK modules) Assessment is carried out on both the UK NEQAS distributed and participant in-house submitted
samples Web data entry and access to individual confidential reports Constructive assessor feedback Individual benchmarking graph to track performance over time Frequency charts illustrating the distribution of participant scores for each run Colour images showing optimal and sub-optimal demonstration of the antigens Tables of the main antibodies and immunocytochemical reagents used by participants Examples of submitted ‘Best Methods’. Interactive searchable web ‘Best Methods’ database An end of year certificate of participation (2 runs or more) along with an annual report Other articles and reviews from the scheme E-Journal after every run with module reviews and articles Participants ‘Help-line’ and details on obtaining advice Participant and scientific meetings and workshops
Module Area of Pathology ISO 17043 Accreditation Status
1 General Pathology Accredited 2 Breast Pathology (Hormonal Receptors) Accredited 3 Breast Pathology (HER2 IHC) Accredited 4 Lymphoid Pathology Accredited 5 Neuropathology Accredited 6 Cytopathology Accredited 7a GIST (Alimentary Tract) Accredited 7b Lynch Syndrome (HNPCC) (Alimentary Tract) Accredited 8 Gastric HER2 IHC Accredited 9 Breast HER2 ISH (Interpretive & Technical) Accredited
10 NSCLC ALK IHC Accredited

Participants Manual 2017-2018
NEQ MP7 2017-2018 © UK NEQAS ICC & ISH Page 4 of 26
1.3 International EQA Service The service currently attracts members from over 55 countries and welcomes participation from both UK and non-UK based laboratories.
All slides, irrespective of country of origin are assessed in exactly the same manner and during the same assessment period.
Assessments of slides are carried out anonymously and assessors are also blinded to their country of origin.
UK clinical laboratories are however monitored for poor performance (see section 2.8)
1.4 Educational Remit of the Service One of the main aims of the service is to provide useful information on methods and reagents that allow for improved quality of immunocytochemistry. To this end, the main technical steps employed by participants at assessment are collated onto a database and subsequently tabulated to show the proportion of participants using a particular reagent or automated system, which achieved acceptable staining at assessment. The results of these analyses appear as best methods and are presented in graph and table forms, along with some images, as part of the online results that participants receive (see section 2.7 below). 1.5 Registration & Subscription Laboratories wishing to participate in UK NEQAS ICC & ISH are recommended to read the detailed descriptions of each of the modules and elect to participate in those modules that cover the range of markers used routinely in their laboratory. UK NEQAS ICC & ISH receives no financial support for the running of the scheme, other than that generated from participants’ subscription fees. These are set to cover the costs of running the scheme on a strictly non-profit-making basis. The annual subscription fees will be provided to all currently subscribed members and will be sent out to those that wish to newly register.
Subscription fees are payable prior to the start of the EQA financial year, which runs from April to March. Subscription fees are non-refundable
Participants actively enrolled in the EQA service will automatically be sent new subscription forms.
Non-return of subscription forms will be taken to mean that a participant no longer wishes to continue with their subscription
Participants must inform UK NEQAS ICC & ISH if they wish to cease participating in the service. Participants must also inform UK NEQAS ICC & ISH of any changes in contact details. Participants are welcome to join anytime throughout the year, but only for the currently active
financial year. Subscription fees may be reduced according to the EQA period at which the participant wishes to subscribe.
Subscription forms, further information and guidance, can be obtained by contacting: [email protected]
1.6 Subcontracted Services UK NEQAS ICC & ISH uses several external suppliers including commercial and public sector organisations from both the UK and Overseas to:
Provide EQA material including formalin fixed paraffin embedded tissue and cell lines, Cell blocks and Cytospins
Provide cutting services for the above material Provide incrementally (every 25th or 50th section) stained samples
Only competent and appropriately accredited laboratories are used for these services. All EQA samples or material is dispatched to participants by UK NEQAS ICC & ISH and assumes the responsibility for all subcontracted work and services. Certain overseas participants will receive the EQA material through a distributor, who receives the material directly from UK NEQAS ICC & ISH. All stained material is validated by UK NEQAS ICC & ISH prior to dispatch.

Participants Manual 2017-2018
NEQ MP7 2017-2018 © UK NEQAS ICC & ISH Page 5 of 26
2.0 GUIDELINES & PROCEDURES 2.1 Slide Distribution and Placement of NEQAS and In-house Controls
Slides consist of two areas (see fig below) : a) Containing NEQAS EQA samples and b) Area for participants to cut their in-house samples/controls
Important:
For the Cytology module a separate in-house control slide/section is required For all modules (apart from the Cytology module) the ‘same slide’ method slides will be
distributed as ’unbaked’. Participants are requested to cut their in-house control material alongside the NEQAS samples and then bake the slide at either 37°C overnight OR 55-60°C for 1 hour. Once the slides have been dried participants should then carry out their usual staining procedure.
It is important that participants prepare control samples which are appropriate for the antibody and module requested and that they fit onto the slide area illustrated in the example above.
At each assessment laboratories are sent formalin-fixed paraffin processed tissue sections or cell lines (alcohol fixed cytospins or sections from a cell block for the cytology module). A run ‘cover letter’ is included with the slides and also e-mailed to participants to provide further information and instructions. Module specific instruction datasheets can also be found on the UK NEQAS webserver.
2.2 Antibody Not Stocked If a particular assessment antibody is not stocked by a participant, an alternative antibody will be suggested by UK NEQAS ICC & ISH.
UK NEQAS ICC & ISH may refer to the yearly antibody repertoire declaration to cross check that a participant has indicated on the survey that they do not currently stock a requested antibody
The data that UK NEQAS ICC & ISH collects yearly via the antibody survey helps to determine which antibodies will be chosen as the ‘Gold standard’: Only those antibodies stocked by at least 95% of labs are chosen as the gold standard. For this reason, most laboratories should stock the gold standard antibodies listed in the manual, and the UK NEQAS office staff may question when a laboratory does not stock a particular marker. However, UK NEQAS does appreciate that there are several specialist centres, which may only stock and use markers within their area of expertise.
If an alternative antibody is provided, slide(s) will be treated and marked in the same way as the original antibody, and will count towards a participants performance record. It is therefore important that you contact the UK NEQAS ICC & ISH office to ask for an alternative, and do not choose your own alternative.
2.3 Web Based Data Entry System and Accessing Online Reports All participants will be provided with access to the UK NEQAS web data entry and report system, which will allow access to instructions for each assessment, individual assessment reports, selected assessment images, graphical/ tabulated data and E-Journal. 2.4 Assessment Procedure
Typically, participants are asked to demonstrate 2 different antigens (one for the Breast modules, Gastric HER2 and NSCLC ALK IHC modules) on the slides provided and return the best one for assessment, along with their usual in-house control slide placed alongside the NEQAS samples (see section 2.1).
For most modules, one of the antigens requested is repeated from one assessment to the next, for a period of 12 months (4 times per year), and serves as a 'gold standard'. This allows participants to implement recommended changes if their quality of immunocytochemical staining is found to be suboptimal and to test improved technique at the next or subsequent assessments.
Participants are also requested to complete details of the antibody and method they have employed on the web based data collection forms.

Participants Manual 2017-2018
NEQ MP7 2017-2018 © UK NEQAS ICC & ISH Page 6 of 26
Returned slides are then marked by an expert panel of assessors (see section 5.2) consisting of senior biomedical / clinical scientists, and consultant histopathologists / cytopathologists; all assessors are vetted, approved and appropriately trained by the scheme prior to assessing participant’s EQA submissions.
2.5 Assessment Scoring and Interpretation Below is a general guide that assessors use when scoring each of the participant slides (see relevant sections for Breast/Gastric HER2 IHC, NSCLC ALK IHC and ISH modules) 2.5.1 General assessment guide
Each of the 4 assessors award a mark out of 5 (except the Breast HER2 ISH module) using the guidelines issued (Table below).
Marks are added together to give a final score out of 20. An acceptable level of staining is where a score is greater than 12/20. A borderline mark of 10-12/20 range indicates that whilst the staining may show some clinical
relevance, the staining is suboptimal and improvements are still required. A score of less than 10/20 is given for poor immunocytochemistry and where the participant has
failed to demonstrate clearly the required components or where there may be non-specific or false positive staining.
Individual assessor scoring guide:
Combined assessor score guide:
Score and Interpretation
Interpretation
16-20/20: Excellent
All 4 assessors agree that overall the staining is at the expected level for each of the UK NEQAS distributed samples
13-15/20: Acceptable
Some slight technical issues noted by some of the assessors, but overall the staining is suitable for interpretation
10-12/20: Borderline (Acceptable)
Overall, whilst the immunostaining is sufficiently good for clinical use, some technical improvements need to be made.
4-9/20: Unacceptable
The IHC staining of the samples is of unacceptable quality and not useful clinically. Signifiacnt technical improvements need to be made.
Score Score Interpretation and examples why marks may be deducted
0 No slide submitted for assessment
1/2 Overall not clinically readable Very weak/No demonstration of requested antigen; false positive/negative staining; non-specific or inappropriate staining; uninterpretable staining; excessive morphological damage ; excessive haematoxylin
3 Although clinically interpretable in that the immunostaining is considered appropriate for the target in question, the staining quality is not optimal and some improvement is advised. Some of these problems are outlined below: Weak demonstration of requested target antigen; background staining; diffuse staining; weak/excessive haematoxylin staining
4/5 Good/Excellent demonstration of the requested target antigen
Note: Marks may also be deducted for reasons which will be shown on individual participant reports such as: Excessive background staining, excessive antigen retrieval, poor quality of in-house tissue, inadequate choice of in-house control tissue, poor/inadequate fixation, damaged cell morphology

Participants Manual 2017-2018
NEQ MP7 2017-2018 © UK NEQAS ICC & ISH Page 7 of 26
2.5.2 Breast HER2 IHC assessment guide The assessors assess each of the NEQAS distributed samples (A-D), and provide their
interpretation on the membrane staining. Assessors will then also provide an overall score out of 5 with the four assessors’ marks added
together to give a possible score out of 20. Assessments are carried out by 4 assessors scoring independently using an adapted method
initially devised by the Clinical Trials Assay where percentage positivity and membrane intensity are taken into account.
Cell line samples are most often distributed for the Breast HER2 IHC module. Due to the nature of the cell lines, they can show an overall population viability range of between
30-90%, and therefore the overall percentage staining criteria cannot be accurately applied to each cell line. For this reason reference sections are prepared by staining, every 50th – 53rd cut section using currently available HER2 IHC standardised kits/assays (Dako HercepTest, Leica Oracle and Ventana Pathway 4B5). This provides a reference point to gauge the expected level of staining of participants’ submitted slides.
UK NEQAS ICC & ISH has devised an EQA specific algorithm for scoring the cell lines so as to provide participants additional technical feedback as shown in the table below: Cell line Expected
level of staining
Acceptable level/s of staining during assessments
Description of staining pattern used by the assessors
A: SK-BR-3 3+ 3+ only The 3+ cell line has a wide threshold of complete membrane staining showing strong staining. Only this level of membrane staining is deemed acceptable for this cell line
B: MDA-MB-453 2+ 2+ 2+/1+ or 1+/2+ 2+/3+ or 3+/2+
i) 2+/1+: 2+ membrane staining is present but also showing 1+ staining ii)1+/2+: Staining is weaker than expected with membrane staining showing more 1+ compared to 2+ iii) 2+/3+: 2+ membrane staining is present but also showing 3+ staining iv) 3+/2+: Staining is stronger than expected with membrane staining showing more 3+ compared to 2+
C: MDA-MB-175 1+ 1+ 1+/0 of 0/1+
i) 1+/0: Staining is more towards the weaker end of 1+ staining but still acceptable ii) 0/1+: Staining is weaker than expected with a low percentage of cells showing 1+ membrane staining, but still acceptable
D: MDA-MB-231 0 0 0/1+ or 1+/0
0/1+ or 1+/0: Cells are starting to show very weak membrane staining
‘U’/Uninterpretable Scores: Assessors may also give a score of ‘U’ which indicates that the
staining of the cell lines/tissue sections were ‘uninterpretable’ due to the reasons set out below. A score of U/x e.g. U/3+ or U/2+ or U/0, for the respective cell lines, is given to indicate that interpretation of the staining is difficult (borderline interpretation) and that some technical improvements are required.
Assessors look at each sample to see whether the cell membrane staining patterns are as expected. Assessors will mark down or fail a participant stain for the following reasons: Excessive cytoplasmic/background staining; excessive/insufficient haematoxylin staining; insufficient membrane staining; false positive/negative membrane staining; morphological damage; poor

Participants Manual 2017-2018
NEQ MP7 2017-2018 © UK NEQAS ICC & ISH Page 8 of 26
quality of in-house control tissue, poor/inadequate choice of control tissue, poor/inadequate fixation of in-house material.
Once the membrane staining has been interpreted for each of the NEQAS samples, assessors then provide an overall score of out 5, based on the interpretability of the membrane staining and technical quality. The four assessor’s scores are then combined to give a possible score out of 20 marks:
Score and Interpretation Interpretation
16-20/20: Excellent
All 4 assessors agree that, overall for the samples distributed, the staining is at the expected level for each of the distributed samples.
13-15/20: Acceptable
Some slight technical issues noted by some of the assessors, but overall the staining is suitable for interpretation
10-12/20: Borderline Acceptable
Overall the samples are borderline interpretable. Indicating, that while still being clinically relevant, technical improvements need to be made. Marks may have been deducted due to:
Weaker/stronger than expected membrane staining Some cytoplasmic staining Morphological damage
4-9/20: Unacceptable
Overall the samples are of unacceptable quality for clinical interpretation and technical improvements need to be made. Marks may have been deducted due to:
False positive/negative membrane staining Excessive cytoplasmic staining Excessive morphological damage Excessive staining of normal glands
2.5.3 Gastric HER2 IHC assessment guide
The Gastric HER2 scoring is based on the original guidelines set out by Hoffman and Ruschcoff for surgical resections.
Prior to sending out slides, and due to the heterogeneity of gastric tissue, reference sections are prepared and stained at approximately every 25th-28th serial section using the currently available commercial kits. Samples are further validated by ISH.
The NEQAS distributed Gastric HER2 slides include samples with a varying range of HER2 protein expression levels. The samples do not necessarily always include (and in the order of) a 3+, 2+, 1+ and 0 at each assessment run.
During the assessment, samples are assessed independently around a multi-header microscope, with each of the 4 assessors providing their interpretation on the membrane staining.
UK NEQAS ICC & ISH uses an EQA specific scoring criteria when scoring the tissue sections, so as to provide participants with additional technical feedback (see table below):
Expected staining Scoring criteria used by UK NEQAS ICC & ISH
3+ i) 3+: Staining is as expected ii) 2+/3+ or 3+/2+: Staining is weaker than expected with membrane staining showing more 2+ compared to 3+ (2+/3+) or 3+ membrane staining is present but also showing 2+ staining (3+/2+)
2+ i) 1+/2+ or 2+/1+: Staining is weaker than expected with membrane staining showing more 1+ compared to 2+ (1+/2+) or 2+ membrane staining is present but also showing 1+ staining (2+/1+) ii) 2+/3+ or 3+/2+: Staining is stronger than expected with membrane staining showing more 2+ compared to 3+ (2+/3+) or 3+ membrane staining is present but also showing 2+ staining (3+/2+)

Participants Manual 2017-2018
NEQ MP7 2017-2018 © UK NEQAS ICC & ISH Page 9 of 26
1+ i) 0/1+: Staining is weaker than expected with a low percentage of cells showing 1+ membrane staining, but still acceptable ii) 1+/0: Staining is more towards the weaker end of 1+ staining but still acceptable
0 0/1+ or 1+/0: Cells are starting to show very weak membrane staining
‘U’ = Uninterpretable: Assessors may also give a score of 'U' which indicates that the cell lines / tissue sections were 'uninterpretable’. U/x = Borderline interpretable: A score of U/x e.g. U/3+ or U/2+ or U/1+ or U/0 indicates that the staining is just about readable and further improvements are required. Any other membrane score other that assigned for each of the expected scores are deemed as unacceptable
Once the assessors have assessed the membrane interpretation for each of the 4 samples, an
individual score out of 5 is awarded, based on the interpretability of the membrane staining and the technical feedback. An overall pass mark is then awarded by combining the four assessor’s scores to give a score out of 20 as shown below:
Score and Interpretation
Interpretation
16-20/20: Excellent
All 4 assessors agree that, overall for the samples distributed, the staining is at the expected level for each of the distributed samples.
13-15/20: Acceptable
Some slight technical issues noted by some of the assessors, but overall the staining is suitable for interpretation
10-12/20: Borderline Acceptable
Overall the samples are borderline interpretable (still clinically relevant) indicating that technical improvements need to be made. Marks may have been deducted due to:
Weaker/stronger than expected staining Excessive non-specific staining Morphological damage
4-9/20: Unacceptable
Overall the samples are of unacceptable quality for clinical interpretation and technical improvements need to be made. Marks may have been deducted due to:
False positive/negative staining Excessive non-specific staining Excessive morphological damage
2.5.4 ALK NSCLC IHC assessment guide The NEQAS distributed material may contain up to 6 samples depending on the assessment Run, and will include a mixture of cell lines and tissue samples of known ALK IHC expression. Reference sections are prepared by staining every 25th-28th cut section using the currently available Ventana ALK for NSCLC assay. This provides a reference point to gauge the expected level of staining of participants submitted slides.
Assessments are carried out by 4 assessors scoring independently. Each assessor will assess the NEQAS distributed samples and provide their interpretation on the staining intensity (scoring as 3+, 2+, 1+ or 0).
‘U’/Uninterpretable Scores: Assessors may also give a score of 'U' which indicates that the cell lines / tissue sections are 'uninterpretable’.
Assessors will then also provide an overall score out of 5 with the four assessors’ marks added together to give a possible score out of 20 as shown in the table above (same as for the Gastric HER2 pass marks).
2.6 In-house Tissue Recommendations In-house samples should be placed onto NEQAS distributed slides as indicated in section 2.1. Appropriate controls must be used as outlined below (section 2.6.1).

Participants Manual 2017-2018
NEQ MP7 2017-2018 © UK NEQAS ICC & ISH Page 10 of 26
Quality of the submitted in-house tissue is important and must be well preserved with readable morphology. Poor fixation, antigen retrieval, counterstain etc. will also be taken into consideration when scoring.
Online data sheets MUST be filled in, indicating the tissue/tumour type, and where appropriate, which component (for example, in the breast module whether DCIS is to be assessed rather than IDC).
We DO NOT require unstained in-house control sections for any of the modules.
2.6.1 All Modules For all modules, in-house tissue must include appropriate controls for the antigen requested.
Marks may be deducted for inappropriate controls.
For example: o Alimentary tract GIST module: GIST + appendix or GIST with normal epithelium o Alimentary tract Lynch Syndrome module: Positive and negative tumour + appendix or
tumour with normal epithelium o Lymphoma module: Tumour + tonsil o NSCLC ALK IHC: ALK positive + negative NSCLC. Appendix is also recommended. o Breast hormonal receptors See section 2.6.2 o Breast and Gastric HER2 IHC See section 2.6.3 & 2.6.4
2.6.2 Breast Hormonal Receptor Module
Participants in-house control tissue MUST consist of composite breast tissue*, placed alongside the NEQAS distributed samples (see section 2.1) (i) >80% tumour positivity with high intensity (Allred/Quick score 7-8) (ii) 30-70% tumour positivity with low-moderate intensity (Allred/Quick score 3-6) (iii) Negative tumour, ideally with normal glands (Allred/Quick score 0) * Cell Lines are an acceptable alternative but those included with commercial kit/assays are not suitable and will not be assessed.
2.6.3 Breast HER2 IHC Module In-house control material must include samples from 3+, 2+ and 1+/0 HER2 expressing invasive
breast cancer cases. Cell Lines are an acceptable alternative but those included with commercial kit/assays are not suitable and will not be assessed.
DCIS breast tissue showing differing levels of membrane staining is an acceptable alternative. However, laboratories must indicate on their datasheet which component of the tumour they have scored, otherwise the invasive component, if present, will be assessed.
It is also acceptable to submit a heterogeneous in-house tumour control with areas of e.g. 3+ and 2+ membrane expression as long as the participant indicates the areas and expected levels of staining.
2.6.4 Gastric HER2 IHC Module In-house control material must include 3+, 2+ and 1+/0 HER2 expressing cases preferably of
gastric tumour, although breast tumour is also acceptable. Cell Lines are an acceptable alternative but those included with commercial kit/assays are not suitable and will not be assessed.
DCIS breast tissue showing differing levels of membrane staining is an acceptable alternative. Laboratories must indicate on their datasheet which component of the tumour they have scored, otherwise the invasive component, if present, will be assessed.
It is also acceptable to submit a heterogeneous in-house tumour control with areas of e.g. 3+ and 2+ membrane expression as long as the participant indicates the areas and expected levels of staining.
2.7 Participant Reports At the end of each assessment, participants are sent notification via email that reports are
available to view and download from the UK NEQAS ICC & ISH website. Participants also have access to graphs, technical tables showing antibodies used, automation
systems, retrieval methods etc. Furthermore, ‘Best Methods’ are also generated from anonymised participant technical data.

Participants Manual 2017-2018
NEQ MP7 2017-2018 © UK NEQAS ICC & ISH Page 11 of 26
2.7.1 Individual Participant Reports Individual reports consist of:
a. The individual assessors’ scores out of 5 and a total score out of 20 b. Assessor feedback if necessary c. Benchmarking graphs showing participants results of over 10 assessments compared to the
overall average for each assessment Report example from the breast hormonal receptor module
2.7.2 Graphical Data Graphs are provided showing the distribution of pass rates for a particular run on both the UK NEQAS ICC and in-house samples. This allows individual participants to gauge their performance against the rest of the participants.
Example of the graphical reports from the Alimentary Tract module
2.7.3 Technical Data Technical tables, showing choice of antibodies, automation systems, and retrieval methods are also provided. The data also shows the number of participants using a particular method (N) along with the percentage (%) that have passed (score>12/20 for most modules) using the selected parameters.
Participants Manual 2017-2018
NEQ MP7 2017-2018 © UK NEQAS ICC & ISH Page 12 of 26
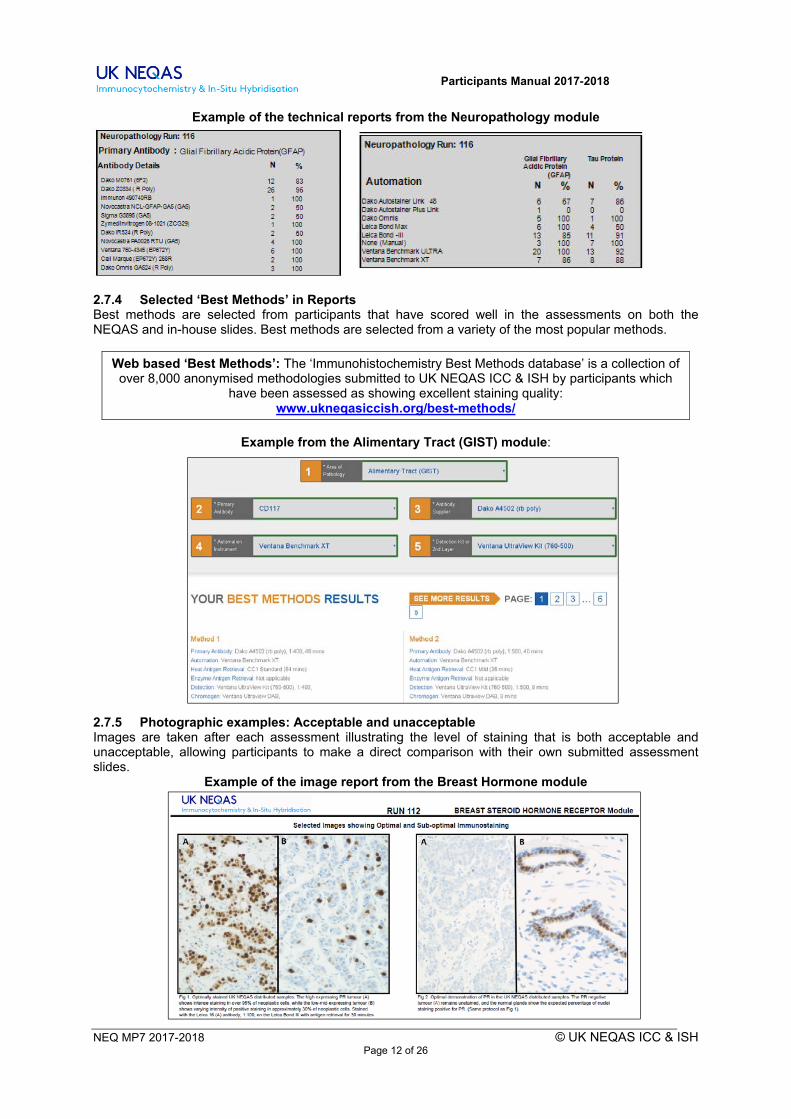
Example of the technical reports from the Neuropathology module
2.7.4 Selected ‘Best Methods’ in Reports Best methods are selected from participants that have scored well in the assessments on both the NEQAS and in-house slides. Best methods are selected from a variety of the most popular methods.
Web based ‘Best Methods’: The ‘Immunohistochemistry Best Methods database’ is a collection of over 8,000 anonymised methodologies submitted to UK NEQAS ICC & ISH by participants which
have been assessed as showing excellent staining quality: www.ukneqasiccish.org/best-methods/
Example from the Alimentary Tract (GIST) module:
2.7.5 Photographic examples: Acceptable and unacceptable Images are taken after each assessment illustrating the level of staining that is both acceptable and unacceptable, allowing participants to make a direct comparison with their own submitted assessment slides.
Example of the image report from the Breast Hormone module

Participants Manual 2017-2018
NEQ MP7 2017-2018 © UK NEQAS ICC & ISH Page 13 of 26
2.7.6 Immunocytochemistry E-Journal After each assessment all data is combined into a single E-Journal and is available to download after a few weeks of the assessment completion. All E-Journals are also freely available to download from: www.ukneqasiccish.org/journals/
2.8 Poor Performance Monitoring of (UK Clinical Laboratories Only) All UK EQA schemes are required by their accrediting body (UKAS ISO 17043/15189), to have in place a formal system whereby the performance of all of its UK based clinical laboratories are monitored. The service is required to notify the National Quality Assurance Advisory Panel (NQAAP) of any cases of persistent substandard performance in participating UK clinical laboratories. From September 2010, NQAAP made it mandatory for EQA schemes to use a ‘traffic light’ system for the grading of all its UK participants:
Green Rating: No issues with poor performance
Amber rating: Issues with poor performance, managed locally by the scheme
Red rating: Poor performance issues unresolved; persistent poor performer – referred to NQAAP
Although in-house sections are not part of the front line poor performance monitoring procedure, the importance of good in-house staining is to be emphasised and labs may be contacted if their in-house controls are suboptimal, or their choice of in-house control material is not appropriate. It will not be acceptable to perform well on UK NEQAS ICC & ISH material alone. Laboratories with persistent suboptimal staining of their in-house material will be contacted, and their EQA results discussed with a view to further action being taken if the situation continues.
The UK NEQAS ICC & ISH Poor Performance monitoring covers the 5 most recent runs following the upload of reports after each assessment.
For the generic modules, each module is treated as a separate entity; low scores from one module are not combined with low scores from another module to produce a poor performance.

Participants Manual 2017-2018
NEQ MP7 2017-2018 © UK NEQAS ICC & ISH Page 14 of 26
Therefore, a laboratory that is underperforming in one module may continue to submit returns for any of the other generic modules in which they are not underperforming.
Offer of Assistance letters When a laboratory has under-achieved in one (biomarker) or two (generic) assessments, the scheme will notify the laboratory to alert them of this situation. This will be an ‘Offer of Assistance’ letter. Although participants are not obliged to contact UK NEQAS ICC & ISH at this point, they may still wish to do so for advice and feedback to improve on future assessment results. Please note that for the generic modules it is possible to have one failed score, then two failed scores at a subsequent run and therefore receive an Amber letter (3 failed scores over 5 runs). Non-submission of slides: This will result in a score of zero (0), and will be included in poor performance monitoring, unless the lab has informed UK NEQAS ICC & ISH of a valid reason for the non-submission. NQAAP has stated that submission rates should be 100% for all UK Clinical laboratories. If a laboratory has not submitted for a run, then the EQA provider (UK NEQAS ICC & ISH) should be given/sent a valid explanation or reason why; e.g. antibody not stocked, not clinically testing or testing being outsourced. Retrospective explanations following the production of results, and subsequent poor performance reports, may not be acceptable. Important: The monitoring procedure shown above is liable to change depending on approval from NQAAP. UK participants will be notified of any changes in a separate communication. 2.8.1 Generic modules (all modules except Breast, Gastric IHC and ALK NSCLC IHC) This includes General Pathology, Cytology, Neuropathology, Lymphoma, and Alimentary tract (GIST and Lynch syndrome/HNPCC).
Status When Triggered Monitoring Procedure
GREEN
2 underperformances (scores <10/20) over 5 runs on NEQAS ICC Gold or second chosen antibody slides
No issues with poor performance. Participant will be offered assistance to improve.
AMBER
3 underperformances (scores <10/20) over 5 runs on NEQAS ICC Gold or second chosen antibody slides
Participant and Head of Department will be notified of continued underperformance and will be sent a ‘Warning letter’ indicating that they are close to being deemed a poor performer and to contact the scheme Director. The scheme Director will then provide advice and assistance on how the laboratory concerned might improve their results
RED
4 underperformances (scores <10/20) over 5 runs on NEQAS ICC Gold or second chosen antibody slides
Participant and Head of Department will be notified that they have been deemed a ‘poor performer’ and to contact the scheme Director to discuss the situation. The scheme is also obliged to refer the laboratory to NQAAP
Although in-house sections are not part of the poor performance monitoring system of this module, in-house material may also be used to gauge overall performance status. Laboratories should make every effort to submit appropriate control material for the antigen requested.
2.8.2 Biomarker modules (Breast ER/PR IHC, Breast HER2 IHC, Gastric HER2 IHC, ALK NSCLC IHC and Breast HER2 ISH) Because of the direct impact that the results of assays for biomarkers have on patient management, more stringent performance monitoring mechanisms are employed:

Participants Manual 2017-2018
NEQ MP7 2017-2018 © UK NEQAS ICC & ISH Page 15 of 26
Status When Triggered Monitoring Procedure
GREEN
1 underperformance (scores <10/20) over 5 runs on NEQAS ICC slides
No issues with poor performance. Participant will be offered assistance to improve
AMBER
2 underperformances (scores <10/20) over 5 runs on NEQAS ICC slides
Participant and Head of Department will be notified of continued underperformance and will be sent a ‘Warning letter’ indicating that they are close to being deemed a poor performer and to contact the scheme Director. The scheme Director will then provide advice and assistance on how the laboratory concerned might improve their results
RED
3 underperformances (scores <10/20) over 5 runs on NEQAS ICC slides
Participant and Head of Department will be notified that they have been deemed a ‘poor performer’ and to contact the scheme Director to discuss the situation. The scheme is also obliged to refer the laboratory to NQAAP
Although in-house sections are not part of the poor performance monitoring system of modules, in-house material may also be used to gauge overall performance status. Laboratories should make every effort to submit well-preserved composite tissue with the full range of tumours of varying expression levels (as outlined in sections 2.3.2 and 2.3.3). Participants not using the correct controls will be scored ≤12/20. In-house cell lines are an acceptable alternative and must also show the full range of expression. Kit control cell lines, i.e. HER2 ICC kits (Dako HercepTest, Leica Oracle, and Ventana Pathway) are not acceptable as in-house control.
N.B. Poor performance is carried out over the previous 5 runs. Participants may receive a letter to confirm their current status (e.g. Amber or Red) even if this may have been sent one previously. If a laboratory’s status changes following an appeal (reassessment), a revised letter will be sent to confirm the new status. 2.8.3 Breast HER2 ISH The value of ISH to determine HER2 gene amplification in breast cancer is evident. Published studies have also highlighted the importance of quality control to monitor this testing (1-5), and because of the direct impact that the results of assays for HER2 have on patient management, more stringent performance monitoring mechanisms are in place for NEQAS ICC and ISH to oversee the testing being carried out by laboratories. Status When Triggered Monitoring Procedure
GREEN
1 inappropriate score over 5 runs on NEQAS ISH slides
No issues with poor performance. Participant will be offered assistance to improve
AMBER
2 inappropriate scores over 5 runs on NEQAS ISH slides
Participant and Head of Department will be notified of continued underperformance and will be sent a ‘Warning letter’ indicating that they are close to being deemed a poor performer and to contact the scheme Director. The scheme Director will then provide advice and assistance on how the laboratory concerned might improve their results
RED
3 inappropriate scores over 5 runs on NEQAS ISH slides
Participant and Head of Department will be notified that they have been deemed a ‘poor performer’ and to contact the scheme Director to discuss the situation. The scheme is also obliged to refer the laboratory to NQAAP

Participants Manual 2017-2018
NEQ MP7 2017-2018 © UK NEQAS ICC & ISH Page 16 of 26
2.9 End of Year Performance Record / Certificate of Participation At the end of each fiscal/EQA year, the scheme provides all participants with a printed ‘certificate of participation’, listing all modules participated in. For each module, labs must have submitted at least twice during the EQA year. Participants also receive a summary of the results they achieved over the preceding year (annual report). 2.10 Meetings & Practical Workshops Participant and scientific meetings, and practical workshops are organised throughout the year, details of which are distributed to all UK NEQAS ICC & ISH subscribers. These meetings provide the opportunity for participants to discuss immunocytochemistry and EQA related topics with other participants, the scheme’s assessors, and UK NEQAS ICC & ISH personnel. 3.0 IMMUNOCYTOCHEMISTRY MODULES Laboratories are welcome to participate in any of the 10 different immunocytochemistry modules, depending on their service commitments and specialised areas of interest. All modules offer FOUR assessment runs per year. The generic modules (General Pathology, Cytology, Neuropathology, Lymphoma, and Alimentary tract (GIST and Lynch syndrome/HNPCC) assess TWO antibodies per module at each assessment:
One antibody is repeated at every assessment (the ‘gold standard’) On occasion we will use two alternating antibodies as Golds rather than a single antibody The second antibody will be different for every run, and will not be disclosed until the run is
issued. Every effort is made to ensure that only antibody markers used by the majority of participants are selected for assessment. The biomarker modules (Breast hormone, Breast HER2, Gastric HER2 and NSCLC ALK) assess ONE antibody at each run. All modules are assessed on both the UK NEQAS distributed slides and participant’s in-house control. 3.1 MODULE 1: General Pathology
‘Gold standard’ antigens for the year ahead will be: CD45 and TTF-1
A second antibody will be chosen from the list below. Every effort will be made to ensure that only markers used by the majority of participants are selected for assessment.
Epithelial Markers Broad Spectrum Cytokeratin (e.g. MNF116, AE1/AE3) Epithelial Membrane Antigen (EMA) Endothelial Markers CD31 CD34 Von Willebrand Factor (FVIII related antigen) Urological & Prostatic Markers Prostate Specific Antigen (PSA)/ Prostatic Acid Phosphatase (PAP) 34βE12 Cytokeratin 7 Cytokeratin 20 Cytokeratin 5 or Cytokeratin 5/6 LP34 P63
Neuroendocrine Markers Chromogranin Neuron Specific Enolase (NSE) Synaptophysin PGP 9.5 CD56 Mesothelial Markers AUA-1 Carcinoembryonic Antigen (CEA) Ber-EP4 Cytokeratin 5/6 Calretinin Thrombomodulin Melanoma Markers (excluding S-100) HMB45 Melan A Muscle Markers: Smooth Muscle Actin (SMA) Desmin
Miscellaneous Thyroglobulin Ki-67 or MIB-1 Human Chorionic Gonadotropin (HCG) Calcitonin CD56 TTF-1 WT1 CDX2 E-Cadherin S-100 Lymphoid Markers T-Cell markers e.g.CD3 B-Cell markers e.g. CD20, CD79a Leucocyte Common Antigen (CD45) CD68 Ig light chains (occasional)

Participants Manual 2017-2018
NEQ MP7 2017-2018 © UK NEQAS ICC & ISH Page 17 of 26
3.2 MODULE 2: Breast Pathology - Hormonal Receptors
Either Oestrogen receptor (ER) or Progesterone receptor (PR) will be chosen
3.3 MODULE 3: Breast Pathology - HER2 Immunocytochemistry Formalin fixed and paraffin processed cell lines showing the full range of HER2 IHC expression (3+, 2+, 1+ and 0) are generally used as the UK NEQAS assessment samples. Note: for HER2 ISH please see section 4.0 3.4 MODULE 4: Lymphoid Pathology
‘Gold standard’ antigen for the year ahead will be: BCL-6 A second antibody will be chosen from the list below. Every effort will be made to ensure that only markers used by the majority of participants are selected for assessment.
3.5 MODULE 5: Neuropathology
‘Gold standard’ antigen for the year ahead will be: Ki-67/MIB-1
A second antibody will be chosen from the list below. Every effort will be made to ensure that only markers used by the majority of participants are selected for assessment.
Neurological & Neuroendocrine Markers Markers for Metastatic Disease Neurofilament Protein (NFP) Broad Spectrum Cytokeratin Glial Fibrillary Acidic Protein (GFAP) Cytokeratin 7 and 20 Neuron-Specific Enolase (NSE) CD34 Chromogranin CD68 S-100 Protein Desmin Growth Hormone (GH) EMA Adrenocorticotrophic Hormone (ACTH) Leucocyte Common Antigen (LCA) Follicle Stimulating Hormone (FSH) Prostate-Specific Antigen (PSA) /Prostatic Luteinizing Hormone (LH) Acid Phosphatase (PAP) Thyroid Stimulating Hormone (TSH) Prolactin Beta-amyloid Ubiquitin
Tau-protein Ki-67 / MIB-1 IDH-1
3.6 MODULE 6: Cytopathology Cytospin preparations or cell block sections are distributed by the scheme for the UK NEQAS prepared slides. The participants’ in-house controls should preferably consist of complimentary preparations depending on your choice of sample.
‘Gold standard’ antigen for the year ahead will be: Ki-67/MIB-1
Alk-1 CD10 CD56 Mast Cell Tryptase Bcl-2 CD15 CD61 Ki-67/MIB-1 Bcl-6 CD1a
CD20 CD21
CD68 CD79a
PAX-5 Terminal deoxynucleotidyl Transferase (Tdt)
CD2 CD23 Cyclin D1 CD4 CD30 IgD CD5 CD35 IgM CD8 CD43 Ig Light chains

Participants Manual 2017-2018
NEQ MP7 2017-2018 © UK NEQAS ICC & ISH Page 18 of 26
A second antibody will be chosen from the list below. Every effort will be made to ensure that only markers used by the majority of participants are selected for assessment.
Lymphoid Markers
Mesothelioma Markers
Adenocarcinoma Others
CD3 HBME-1 EMA/HMFG-2 ER/PR CD20 Calretinin Cytokeratins Melanoma markers (S100, CD45 Thrombomodulin Ki-67/MIB-1 Melan A, HMB45) Cytokeratin 5/6 MOC-31
3.7 MODULE 7: Alimentary Tract Pathology 3.7.1 Module 7A: Stromal tumours of the GI Tract (GIST)
Gold standard for each assessment: CD117
A second antibody will be chosen from the list below.
DOG-1 SMA S100 CD34 Desmin
3.7.2 Module 7B: Lynch Syndrome/ Mismatch Repair Protein
MLH1 & PMS2 OR MSH2 & MSH6 will be requested alternately 3.8 MODULE 8: Gastric HER2 IHC NEQAS distributed samples will consist of gastric cancer samples showing varying levels of HER2 membrane protein expression. 3.9 MODULE 9: Breast HER2 ISH See section 4.0 3.10 MODULE 10: NSCLC ALK IHC NEQAS distributed samples will consist of Lung tumour and cell lines with varying levels of ALK expression. 4.0 IN-SITU HYBRIDISATION MODULES Currently the UK NEQAS ICC & ISH scheme runs a combined Breast HER2 ISH ‘interpretive’ and ‘technical’ module. The 2 parts of the module cannot be subscribed to separately, and assessments are carried out 4 times per fiscal year. Both parts of the module are fully accredited and as such UK laboratories will be monitored for poor performance. 4.1 Breast HER2 ISH Interpretive Module 9A: 4.1.1 Interpretive Assessment procedure
At each assessment, laboratories are sent formalin-fixed paraffin processed samples of known HER2 ISH status
Participants are requested to demonstrate HER2 gene amplification using either a dual probe assay (HER2/Cep17: ratio method) OR single probe assay (HER2 copy) (in accordance with the UK HER2 ISH guidelines).
Participants are required to complete and return scores for each sample using the online data entry system. In this module, a different panel of breast cancer specimens will be sent at each assessment to ensure coverage of the critical diagnostic ranges. They are also requested to input their methodology data to provide brief details of the probe and method they have employed.
Assessment of slides utilises a statistical method in order to provide concise information with regards to the inter-observer variability in enumerating HER2 copy, chromosome 17 and overall ratios. The table below describes the statistical approach used in the ISH interpretive scoring system

Participants Manual 2017-2018
NEQ MP7 2017-2018 © UK NEQAS ICC & ISH Page 19 of 26
Interpretive Assessment Score Guide
Dual Probe Single Probe (i) 36/36: Excellent level of performance (ii) 30-35/36: Acceptable level of
performance (iii) 24-29/36: Borderline level of
performance (iv) <24/36: Unacceptable level of
performance
(i) 12/12: Excellent level of performance (ii) 10-11/12: Acceptable level of performance (iii) 8-9/12: Borderline level of performance (iv) <8/12: Unacceptable level of performance
4.2 Breast HER2 ISH Technical Module 9B: As well as carrying out the ‘interpretive’ assessment (shown above) participants are also requested to return their slides for ‘technical’ evaluation 4.2.1 Technical assessment
Chromogenic ISH (CISH) slides are technically assessed around a multi-header microscope with each slide being assessed by 4 independent assessors. Each assessor provides a score out of 5, and then scores are added together to give a possible score out of 20, along with an overall comment on the score value.
Fluorescent ISH (FISH) slides are technically assessed by 4 assessors at the same time, achieved by incorporating a live-feed video from the fluorescence microscope with the image viewed on a large high definition monitor, allowing all 4 assessors to view and score the FISH slides at the same time.
Assessors examine the quality of the ISH staining BUT do not carry out probe enumeration. (This is assessed during the HER2 ISH interpretive assessment).
Technical evaluation procedure is shown below:
Individual Assessor Scores (CISH only) Scored out of 5
Overall Assessor Scores & Result (CISH & FISH) Scored out of 20
Score Interpretation
0 0 Slide not submitted for assessment
1 & 2
4-9/20 Unacceptable
The NEQAS distributed samples and/or in house samples are of unacceptable quality which are deemed to be uninterpretable: Examples of Reasons: Excessive / weak nuclear staining; Poor probe hybridisation ; Missing Her2 copy no. / CEP 17; Excessive background staining.

Participants Manual 2017-2018
NEQ MP7 2017-2018 © UK NEQAS ICC & ISH Page 20 of 26
3
10-12 Borderline
The NEQAS distributed samples and/or in house samples are of borderline quality indicating that interpretation may be possible but improvements must be made Example of Reasons: Weak nuclear staining; Weak Her2 copy no. / CEP 17 ; Background staining.
4 & 5 13-15/20 Acceptable 16-20/20 Excellent
The NEQAS distributed samples and/or in house samples show a good/very good standard of staining and are suitable for interpretation.
4.3 Troubleshooting Interpretive and Technical module Results Combining the results from the ‘Interpretive’ and ‘Technical’ HER2 ISH modules, allows laboratories to further troubleshoot their techniques as shown in the guide below:
5.0 PERSONNEL & ASSESSORS 5.1 Key Personnel & Assistance
Participants experiencing technical difficulties or requiring information about a particular antibody or reagent are encouraged to contact us using the email below and the relevant staff member will reply.
Replacement slides, following breakage, may be obtained by contacting the UK NEQAS ICC & ISH office. Ideally, all laboratories experiencing difficulties should contact the scheme for advice well before poor performance monitoring mechanisms come into effect. The scheme’s Director and Manager always welcome such calls. The scheme’s contact details are as follows:
For all enquiries email: [email protected] Telephone: +44 (0) 20 7415 7065
Interpretive & Technical Troubleshooting Guide
Technical Result
Interpretive Result
Acceptable Appropriate or Acceptable
Overall the NEQAS samples show a good standard of staining and have been interpreted correctly
Acceptable Unacceptable
Overall the NEQAS samples show a good standard of staining BUT there appears to be issues with interpretation i.e. HER2 copy number and/or CEP17 overestimated/underestimated. Recommend that scoring/counting criteria is reviewed
Unacceptable Appropriate or Acceptable
Overall the NEQAS samples are unacceptable for interpretation and caution should be taken when interpreting from these slides. Recommend that technical method (kit/assay) is optimised (or where relevant a standardised kit is used as per instructions) as interpretation, although appears correct, may lead to incorrect interpretation of clinical cases
Unacceptable Unacceptable
Overall the NEQAS samples are unacceptable for technical staining and interpretation. Reporting from such cases is very likely to lead to incorrect interpretation of clinical cases. If there is persistent underperformance:
- Seek assistance from kit/assay manufacturer - Seek assistance from UK NEQAS or colleagues - Re-validate protocol (retrospectively and prospectively) - Review scoring criteria - Consider sending out clinical cases to a reference centre
to confirm your results
Participants Manual 2017-2018
NEQ MP7 2017-2018 © UK NEQAS ICC & ISH Page 21 of 26
Director Mr Keith Miller
Deputy Director Mr Andrew Dodson
Acting Manager Ms Suzanne Parry
Quality Manager Ms Seema Dhanjal
Scientists Mrs Dawn Wilkinson Mr Neil Bilbe
Office Manager Mrs Ai Lin Rhodes
Clerical Assistant Mrs Clara Lynch
5.2 Assessor List UK NEQAS ICC & ISH assessments are a team effort and consist of experienced scientists and pathologists. The below table shows the current list of active UK NEQAS ICC & ISH assessors.
Australia Mrs J Brincat, Victoria Germany Dr Iris Nagelmeier, Kassel Hungary Dr T Krenacs, Szeged Ireland Prof E Kaye, Dublin Mr K McAllister, Dublin Dr T O’Grady, Dublin Netherland Prof E Erik Thunnissen, Amsterdam Portugal Dr J Cabecadas, Lisbon Mr A Ferro, Lisbon Mrs T Pereira, Lisbon Mr R Roque, Lisbon Mr J Matos, Lisbon Sonia Moliveira, Lisbon Mrs A Tavares, Lisbon Slovenia Dr M Flezar, Ljubljana Mrs S Gabric, Ljubljana Mrs I Kirbis, Ljubljana Mr D Vidovic, Maribor South Africa Mrs R Van Wijk, Cape town
Sweden Dr G Elmberger, Stockholm Switzerland Dr Pierre-Andre Diener, St Gallen Dr L Tornillo, Basel Saudia Arabia Dr T Khan, Saudia Arabia United Kingdom Mr C Abbott, Bristol Mr D Allen, London Dr M Arends, Edinburgh Dr M Ashton-Key, Southampton Mr N Bilbe, London Mr D Blythe, Leeds Mrs A Brown, London Dr C Cardozo, Lancashire Dr L Carson, Aberdeen Mrs A Clayton, Preston Mrs A Cramer, Manchester Mr I Downie, Glasgow Mr A Dodson, London Mrs G Donald, Maidstone Mr R Fincham, Cambridge Mr D Fish, Warwickshire Mrs S Forrest, Liverpool Mr S Forrest, Liverpool
United Kingdom Dr I Frayling, Cardiff Ms J Freeman, London Dr C Gillett, London Prof J Gosney, Liverpool Mrs L Govan, Lanarkshire Mr J Gregory, Birmingham Dr L Gudur, Preston Dr N Guppy, London Dr J Gupta, Maidstone Dr N Hand, Nottingham Ms L Happerfield, Cambridge Mrs C Hawker, Nottingham Mrs J Hogarth, Newcastle Dr R Hunt, Stockport Prof B Jasani, Cardiff Dr N Johnson, Cambridge Ms S Jordan, London Dr J Joseph, Preston Mrs L Kane, Glasgow Ms K Kennedy, Belfast Prof K Kerr, Aberdeen Dr G King, Aberdeen Mr J Linares, London Dr B Mahler-Araujo, Cambridge Mrs J MacMillan, Glasgow Mr C Marsh, Newcastle Dr P Maxwell, Belfast Mrs H McBride, Belfast Dr S McQuaid, Belfast Mr K Miller, London Dr J Moorhead, London
United Kingdom Ms A Newman, London Dr G Orchard, London Deepa Pandit, Lancashire Mrs G Valentine, London Ms S Parry, London Ms A Patterson, Belfast Prof S Pinder, London Dr M Pitt, Preston Dr E Provenzano, Cambridge Mrs F Rae, Edinburgh Dr A Riley, Stirling Mr G Rock, Birmingham Mr A Shore, London Dr J Starczynski, Birmingham Dr P Taniere, Birmingham Mrs C Thomas, Preston Mr P Thompson, Leeds Mr P Wells-Jordan, Nottingham Dr P Wencyk, Nottingham Mrs H White, Maidstone Mrs D, Wilkinson, London Mrs J Williams, Portsmouth

Participants Manual 2017-2018
NEQ MP7 2017-2018 © UK NEQAS ICC & ISH Page 22 of 26
6.0 APPEALS, COMPLAINTS & CONFIDENTIALITY 6.1 Appeals Procedure and Assistance
Participants who are not satisfied with their scores can appeal, and have their slides reassessed. Reassessments take place at the first assessors meeting after receipt of the request. If the
reassessment scores are different from the original ones, the score sheets and database are amended accordingly and the participant is sent amended scores and a letter of explanation.
An appeal can only be made from the most recent completed run. Only originally submitted slides will be reassessed. We are unable to reallocate or update marks
on newly stained slides. Participants are welcome to send in slides asking for feedback and advice at any time (see email
below) or include an enclosed letter with your slides. Do not use the UK NEQAS ICC & ISH reassessment forms for this service though.
UK NEQAS ICC & ISH is always ready to assist with advice and troubleshooting. A Reassessment form can be found on the UK NEQAS ICC & ISH general website:
http://www.ukneqasiccish.org/wp/wp-content/uploads/2016/12/NEQ-MF17-Request-for-Reassessment-of-Slides-v5.pdf
Contact: [email protected]
6.2 Complaints Procedure Formal complaints about the service (not an appeal against your score) offered by UK NEQAS ICC & ISH must be addressed to the scheme’s Director, Mr. Keith Miller; please use the official complaint form which also has the scheme Director’s contact details. Document is available at: http://www.ukneqasiccish.org/wp/wp-content/uploads/2016/12/NEQ-MF4-Participant-Complaint-Form_v6.pdf N.B. Do not use the above form if requesting a reassessment (see 6.1 above) 6.3 Confidentiality Policy UK NEQAS ICC & ISH maintains the confidentiality of a participants’ performance results at all times; except where the scheme is obliged to inform regulatory bodies (NQAAP) of UK clinical laboratories that are persistent poor performers; this is to ensure that patient safety is not endangered. During the actual assessments, and any subsequent use of data for educational purposes, the participants’ identity is never disclosed, beyond the use of the lab’s unique participation code that is known only to UK NEQAS ICC & ISH staff. Where a third party or an interested party enquires about the use of an individual participants’ data, this will only be disclosed if the participant waives its right to confidentiality. UK NEQAS ICC & ISH may provide anonymous data to third parties that have a direct involvement in UK NEQAS ICC & ISH. If UK NEQAS ICC & ISH is legally obliged to provide data, to a regulatory body or another organisation, the participants will be informed in all such instances. 7.0 PROSPECTIVE NEW MODULES 7.1 PD-L1 in NSCLC Pilot Module to be confirmed following the pre-pilot assessment 8.0 ASSOCIATED SCHEMES AND MODULES 8.1 Cellular Pathology Techniques Participants are assessed for the quality of their staining preparations in both Haematoxylin and Eosin stained sections and special staining methods. For further information please contact: [email protected]. Scheme Manager: Mrs Chantell Hodgson; [email protected] 8.2 Molecular Pathology EQA scheme The UK NEQAS for Molecular Pathology provides an EQA service for a variety of molecular tests on a range of diseases. Test are carried out on the patient tumour samples providing an EQA service for a variety of molecular tests, including, Non-small cell lung cancer, Colorectal cancer, Melanoma, and

Participants Manual 2017-2018
NEQ MP7 2017-2018 © UK NEQAS ICC & ISH Page 23 of 26
Gastrointestinal Stromal Cancer. For further information please contact: Dr Sandi Deans (Scheme Director); [email protected] 9.0 TERMS & CONDITIONS An active participant (laboratory, organization or individual) subscribed to our services, agrees and acknowledges the following:
Inform UK NEQAS ICC & ISH of any change of personnel or contact details Always quote your unique participants’ code whenever contacting UK NEQAS ICC & ISH Ensure slides are securely packaged to prevent breakages and possible non-assessment, and
returned in the correct labelled slide boxes to aid sorting Ensure slides are clearly labelled, and concealing your site’s identity where appropriate Adhere to submission deadlines – late submissions will be logged by the scheme Prompt payment of subscription fees, your account may be suspended if payment is not received Antibody repertoires, non-declaration of this may lead to a non-submission (0 score) and possible
poor performance issues Follow specific staining requirements for each of the subscribed modules Complete entry of methodology protocols Declares that the methodology submitted is the same method used in the routine setting of the
laboratory Producing local procedures for EQA, including the handling and interpretation of results Respect the anonymity and confidentiality aspect of EQA when corresponding with other
laboratories Suspected collusion and/or falsification of results, data or manipulation of EQA slides will result in
the participant/s being suspended from UK NEQAS ICC & ISH
UK NEQAS ICC & ISH requests as wide a range of markers for each module as possible, but cannot cover all antigens or tissue types. Participants should have their own alternative performance assessment activities to cover their repertoire
Provided assessment results, although confidential to each participant, may be used by the participant as they see fit (e.g. printed, placed on website etc). However under no circumstances should results be amended, concealed or used to give a false or misleading impression of their participation level or performance status
If individual reports are used in any form then the accompanying statement should be included: “Participation in UK NEQAS ICC & ISH is not an indication of the overall performance of the participant (laboratory, organisation or individual), and as such is not an endorsement of the overall quality of staining produced”
10.0 SELECTED REFERENCES 10.1 Publications
1. Merdol Ibrahim, Suzanne Parry, Dawn Wilkinson, Neil Bilbe, David Allen, Steven Forrest, Perry Maxwell, Anthony O’Grady, Jane Starczynski, Philippe Taniere, John Gosney, Keith Kerr, Keith Miller, Erik Thunnissen (2016) ALK Immunohistochemistry in Non-Small Cell Lung Carcinoma (NSCLC): Discordant Staining Can Impact Patient Treatment Regimen. J. thoracic Oncol
2. Matteo Brunelli, Alessia Nottegar, Giuseppe Bogina, Anna Caliò, Luca Cima, Albino Eccher,Caterina Vicentini, Lisa Marcolini, Aldo Scarpa, Serena Pedron, Eleonora Brunello, Sakari Knuutila, Anna Sapino, Caterina Marchiò, Emilio Bria, Annamaria Molino, Luisa Carbognin,Giampaolo Tortora, Bharat Jasani, Keith Miller, Ibrahim Merdol, Lucia Zanatta, Licia Laurino, Tiina Wirtanen, Giuseppe Zamboni, Marcella Marconi, Marco Chilosi, Erminia Manfrin, Guido Martignoni, Franco Bonetti Monosomy Of Chromosome 17 In Breast Cancer During Interpretation Of Her2 Gene Amplification. Am J Cancer Res 2015 15;5(7):2212-21. Epub 2015 Jun 15.
3. Bartlett JM, Starczynski J, Atkey N, Kay E, O'Grady A, Gandy M, Ibrahim M, Jasani B, Ellis IO, Pinder SE, Walker RA.HER2 testing in the UK: recommendations for breast and gastric in-situ hybridisation methods. J Clin Pathol. 2011 64 (8):649-653

Participants Manual 2017-2018
NEQ MP7 2017-2018 © UK NEQAS ICC & ISH Page 24 of 26
4. Barker C, Ibrahim M, Miller K, Reid V. (2009) Nondestructive quality control of HER2 control cell line sections: the use of interferometry for measuring section thickness and implications for HER2 interpretation on breast tissue. Appl Immunohistochem Mol Morphol. 17(6):536-542.
5. Bartlett JM, Ibrahim M, Jasani B et al., (2009) External quality assurance of HER2 FISH and ISH testing: three years of the UK national external quality assurance scheme. Am J Clin Pathol. 131(1):106-111.
6. Hoffman M, Stoss O, Shi D, et al. Assessment of a HER2 scoring system for gastric cancer: results from a validation study. Histopathology. 2008. 52 (7):797-805.
7. Ibrahim M, Dodson A, Barnett S, et al., (2008) Potential for false-positive staining with a rabbit monoclonal antibody to progesterone receptor (SP2): findings of the UK National External Quality Assessment Scheme for Immunocytochemistry and FISH highlight the need for correct validation of antibodies on introduction to the laboratory. Am J Clin Pathol. 129(3):398-409.
8. O'Grady A, Allen D, Happerfield L, Johnson N, Provenzano E, Pinder SE, Tee L, Gu M, Kay EW. An immunohistochemical and fluorescence in situ hybridization-based comparison between the Oracle HER2 Bond Immunohistochemical System, Dako HercepTest, and Vysis PathVysion HER2 FISH using both commercially validated and modified ASCO/CAP and United Kingdom HER2 IHC scoring guidelines. Appl Immunohistochem Mol Morphol. 2010 18(6):489-93.
9. Rakha EA, Pinder SE, Bartlett JM, Ibrahim M, Starczynski J, Carder PJ, Provenzano E, Hanby A, Hales S, Lee AH, Ellis IO; National Coordinating Committee for Breast Pathology.Updated UK Recommendations for HER2 assessment in breast cancer (2015). J Clin Pathol. 68(2):93-99
10. Ruschoff J, Dietel M, Baretton G et al. HER2 diagnostics in gastric cancer-guideline validation and development of standardized immunohistochemical testing. Virchows Arch. 2010 457(3):299-307.
11. Wolf RA, Hammond EH, Hicks, DG, et al. (2013). Recommendations for Human Epidermal Growth Factor Receptor 2 Testing in Breast Cancer: American Pathologists Clinical Practice Guideline Update. J Clin Pathol. 31(13):3997-4013.
10.2 Books
1. Antigen Retrieval Immunohistochemistry Based Research and Diagnostics (2010) (Wiley Series in Biomedical Engineering and Multi-Disciplinary Integrated Systems.) by Shan-Rong Shi and Clive R. Taylor
2. Advanced Techniques in Diagnostic Cellular Pathology (2009) by Mary Hannon-Fletcher and Perry Maxwell
3. Prognostic and Predictive Factors in Breast Cancer (2008) Second Edition by Rosemary A. Walker and Alistair M. Thompson
4. Merdol Ibrahim, John Bartlett, Keith Miller and Bharat Jasani (2011). Breast cancer biomarker: prognostic and predictive value and external quality assurance. In ’Breast Pathology’. Edited by Frances P. O’Malley, Sarah E. Pinder and Anna Marie Mulligan.
11.0 STEERING COMMITTEE FOR TECHNICAL SCHEMES IN CELLULAR PATHOLOGY Chairperson Mr Alex Javed. Service Manager - Laboratories and Radiology. NHS Highland, Inverness, Scotland Email: [email protected] Committee Members Mr. Paul Cross, Director of the UK NEQAS for Cellular Pathology Technique Email: [email protected]

Participants Manual 2017-2018
NEQ MP7 2017-2018 © UK NEQAS ICC & ISH Page 25 of 26
Ms. Chantell Hodgson, Manager of the UK NEQAS for Cellular Pathology Technique Email: [email protected] Mr. Keith Miller, Director of the UK NEQAS for Immunocytochemistry & ISH Email: [email protected] Mr. Andrew Dodson. Deputy Director of the UK NEQAS for Immunocytochemistry & ISH. Email: [email protected] Mrs Vivienne Beavers. Blackpool Victoria Hospital. IBMS rep (cytology). Email: [email protected] Dr. Sandi Deans, Director of the UK NEQAS for Molecular Pathology Email: [email protected]