Part 3: Starting Treatment, treatment breaks and treatment trends
20
The following slides and audio are taken from a public HIV health and treatments update forum held in Sydney, Australia on 25 November 2008. The slides and audio have been edited for presentation on the web. The speaker is Dr Fraser Drummond, National Centre in HIV Epidemiology and Clinical Research. For more presentations from this event, visit the sponsor organisations’ websites:
-
Upload
napwa -
Category
Health & Medicine
-
view
906 -
download
2
description
A presentation from the 2008 HIV Health and Treatments Update forum held in Sydney on 25 Nov 2008. Part 3: a look at emerging research using biomarkers and their influence on decisions about starting streatment and taking treatment breaks, presented by Dr Fraser Drummond.
Transcript of Part 3: Starting Treatment, treatment breaks and treatment trends

The following slides and audio are taken from a public HIV health and treatments update forum held in Sydney,
Australia on 25 November 2008. The slides and audio have been edited for presentation on the web.
The speaker is Dr Fraser Drummond, National Centre in HIV Epidemiology and Clinical Research.
For more presentations from this event, visit the sponsor organisations’ websites:

HIV Treatment and Health UpdateHIV Treatment and Health Update25 November 2008
Part 3
Starting treatment, treatment breaks
and treatment trends

What is a Biomarker?
...a characteristic that is objectively measured and evaluated as an indicator of
normal biological processes
pathogenic processes
pharmacological responses to a therapeutic intervention

Proposed Hypothesis by which HIV affects inflammation/coagulation
HIV
Tissue Factor
Extrinsic Clotting Pathway
Thrombogenesis
Secondary Inflammation (IL6)
Coagulation Cascade
Increased D-dimer
Vascular endothelium of smooth muscle cells

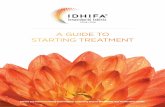
Change in D-dimer* (µg/mL) & IL-6 (log)* from Baseline to 1 Month
0
0.1
0.2
0.3
0.4
≤ 400 401-10,000 10,000-50,000 >50,000
Month 1 HIV RNA Level (copies/mL)
∆ D
-dim
er
(µg
/mL
)/ ∆
IL-6
(lo
g)
p=0.0005 for trend
* DC patients on ART at baseline with HIV RNA ≤ 400 copies/mL
p=0.0003 for trend

When to Start cART: 2008
CD4 count (cells/µL)
ARV recommendation
<350 cART recommended
>350 – <500*†‡ cART generally deferred; clinicians may treat if VL>100,000 copies/mL
>500*†‡ cART generally not recommended
symptomatic HIV disease: ARV recommended for all patients
asymptomatic HIV disease decision based on CD4+ T-cell count
DHHS, 2008; BHIVA, 2008; IAS, 2008
*BHIVA, consider ARV if HBV requiring Rx; HCV/HIV co-infection; low CD4%; established CVD or Framingham score >20% over 10 yrs; malignancy requiring chemotx; pregnancy†DHHS consider ARV if HBV requiring Rx; HIVAN; pregnancy‡“individualise” as above plus rapid decline of CD4+

Evolution of Focus of ConcernOpportunisticInfections &Malignancies
CMVPJPMAC
toxoplasmosiscryptococcosis
candidiasishistoplasmosis
Kaposi’s sarcomaothers?
Time

Evolution of Focus of ConcernOpportunisticInfections &Malignancies
CMVPJPMAC
toxoplasmosiscryptococcosis
candidiasishistoplasmosis
Kaposi’s sarcomaothers?
Complications of Therapy
CVDmetabolic
renal hepatic
neurologichaematologic
others?
Time

Evolution of Focus of ConcernOpportunisticInfections &Malignancies
CMVPJPMAC
toxoplasmosiscryptococcosis
candidiasishistoplasmosis
Kaposi’s sarcomaothers?
Complications of Therapy
CVDmetabolic
renal hepatic
neurologichaematologic
others?
SeriousNon-AIDS
Morbidities
MIstroke
renal Failurehepatic Failuremalignancies
others?
Time

Pros of Earlier Rx
Reduced viraemia
Improved QoL
Reduced risk of disease progression
Reduced infectiousness??

Cons of Earlier Rx
Adherence
Costs
Toxicity – do we have the best starting combinations yet?
Risk of resistance

Interrupting Therapy?
SMART results - not recommended
Certain situations:Acute toxicityIntercurrent illness limiting oral intakeSurgery
Planned interruptions should only be done in clinical trials

What to Start?
FEIN(t)RTI NNRTI IntI PI
AZT EFV SQV/r
NVP*
LPV/r
3TC ATV
ABV ATV/r
TFV fAPV/r
FTC DRV/r
*CD4+ restrictions apply

NRTI Backbone
Truvada – renal and bone issues, caution with NVP?
Kivexa – CVD and potency issues
Combivir – Lipoatrophy and Anaemia
Factors – need maximum potency, low side effects and ease of use, blood-brain barrier?

NRTI Backbone
Abacavir Concerns
Potency – is it strong enough?CVD risk
DAD and SMART?Channelling BiasNot naïve patientsMore data expected
Avoid if high CVD risk factorsMore data awaited – discuss with your doctor

Antiretroviral Drug Approval:1987 - 2008
0
5
10
15
20
25
30
1987 1989 1991 1993 1995 1997 1999 2001 2003 2005 2007
AZT ddIddC d4T
3TCSQV
RTVIDVNVP
NFVDLV
EFVABC
APVLPV/r
TDF
ENFATVFTCFPV TPV
DRV
ETRRAL MVC

New treatments
Integrase inhibitors work!
Raltegravir, Elvitegravir
CCR5 inhibitors – what role?
Maraviroc, Vicriviroc
New NNRTI(s)
Etravirine, Rilpivirine
Newish PIs
Darunavir, Tipranavir

Treatment Simplification
Improve QoL, adherence, avoid long term toxicities, reduce risk of viral failure
Resistance or not, within class or new class
Monitor closely after any switch

Will Treatment Be Forever?
Currently yes
Future??
Therapeutic Vaccination
Genetic ART selection
Novel monthly injections

For more presentations from this event, visit
www.napwa.org.au
or
www.acon.org.au