Part 2B: Health Risk Assessment - RW CORKERY...ABN: 46 114 162 597 Part 2B: Health Risk Assessment...
70
ABN: 46 114 162 597 Part 2B: Health Risk Assessment Prepared for: R.W. Corkery & Co. Pty Limited 1st Floor, 12 Dangar Road PO Box 239 BROOKLYN NSW 2083 Tel: (02) 9985 8511 Email: [email protected] On behalf of: Gloucester Resources Limited Level 37, Riverside Centre 123 Eagle Street BRISBANE QLD 4000 Tel: (07) 3006 1830 Fax: (07) 3006 1840 Email: [email protected] Prepared by: Pacific Environment Limited Suite 1, Level 1 146 Arthur Street NORTH SYDNEY NSW 2060 Tel: (02) 9870 0900 Fax: (02) 9870 0999 Email: [email protected] Ref No: 7210 June 2016
Transcript of Part 2B: Health Risk Assessment - RW CORKERY...ABN: 46 114 162 597 Part 2B: Health Risk Assessment...

ABN: 46 114 162 597
Part 2B:
Health Risk Assessment
Prepared for: R.W. Corkery & Co. Pty Limited 1st Floor, 12 Dangar Road PO Box 239 BROOKLYN NSW 2083
Tel: (02) 9985 8511 Email: [email protected]
On behalf of: Gloucester Resources Limited Level 37, Riverside Centre
123 Eagle Street BRISBANE QLD 4000
Tel: (07) 3006 1830 Fax: (07) 3006 1840 Email: [email protected]
Prepared by: Pacific Environment Limited
Suite 1, Level 1 146 Arthur Street
NORTH SYDNEY NSW 2060
Tel: (02) 9870 0900 Fax: (02) 9870 0999 Email: [email protected] Ref No: 7210
June 2016

GLOUCESTER RESOURCES LIMITED SPECIALIST CONSULTANT STUDIES
Amended Rocky Hill Coal Project Part 2B: Health Risk Assessment
Report No. 806/14
2B-2
This Copyright is included for the protection of this document
COPYRIGHT
© Pacific Environment Limited, 2016 and
© Gloucester Resources Limited, 2016
All intellectual property and copyright reserved.
Apart from any fair dealing for the purpose of private study, research, criticism or review, as permitted under the Copyright Act, 1968, no part of this report may be reproduced, transmitted, stored in a retrieval system or adapted in any form or by any means (electronic, mechanical, photocopying, recording or otherwise) without written permission. Enquiries should be addressed to Pacific Environment Limited.

SPECIALIST CONSULTANT STUDIES GLOUCESTER RESOURCES LIMITED
Part 2B: Health Risk Assessment Amended Rocky Hill Coal Project
Report No. 806/14
CONTENTS Page
2B-3
GLOSSARY OF COMMONLY USED TERMS AND ACRONYMS ..................................................... 2B-5
DEFINITION OF TERMS...................................................................................................................... 2B-6
DEFINITION OF TERMS (CONT’D) .................................................................................................... 2B-7
EXECUTIVE SUMMARY...................................................................................................................... 2B-9
1. INTRODUCTION ...................................................................................................................... 2B-13
1.1 SCOPE OF WORK .......................................................................................................2B-13
1.2 BACKGROUND ............................................................................................................2B-13
1.3 OVERVIEW OF THE AMENDED PROJECT ...............................................................2B-15
2. METHODOLOGY ..................................................................................................................... 2B-20
2.1 WHAT IS A RISK ASSESSMENT? ..............................................................................2B-20
2.2 OVERALL APPROACH ................................................................................................2B-21
3. COMMUNITY PROFILE ........................................................................................................... 2B-22
3.1 SURROUNDING AREA AND POPULATION ..............................................................2B-22
3.2 POPULATION PROFILE ..............................................................................................2B-22
3.3 RESIDENCES AND SENSITIVE RECEIVERS ............................................................2B-24
3.4 COMMUNITY CONCERNS ..........................................................................................2B-24
4. OVERVIEW OF AIR QUALITY ASSESSMENT ...................................................................... 2B-25
4.1 EXISTING AIR QUALITY .............................................................................................2B-25
4.2 AIR QUALITY ASSESSMENT SCENARIOS ...............................................................2B-25
4.3 AIR QUALITY ASSESSMENT OUTCOMES ...............................................................2B-26
5. HEALTH RISK ASSESSMENT ............................................................................................... 2B-27
5.1 IDENTIFICATION OF EMISSIONS OF HAZARDOUS POLLUTANTS .......................2B-27
5.2 ASSESSMENT OF PARTICULATE MATTER .............................................................2B-28
5.2.1 Hazard Assessment ........................................................................................2B-28
5.2.2 Exposure Assessment .....................................................................................2B-40
5.2.3 Risk Characterisation ......................................................................................2B-41
5.2.4 Conclusion .......................................................................................................2B-46
5.3 ASSESSMENT OF NITROGEN DIOXIDE ...................................................................2B-46
5.3.1 Hazard Assesment ..........................................................................................2B-46
5.3.2 Exposure Assessment .....................................................................................2B-49
5.3.3 Risk Characterisation ......................................................................................2B-51
5.3.4 Conclusion .......................................................................................................2B-54
5.4 ASSESSMENT OF DIESEL .........................................................................................2B-54
6. LIMITATIONS .......................................................................................................................... 2B-56
7. CONCLUSIONS ....................................................................................................................... 2B-57
8. REFERENCES ......................................................................................................................... 2B-60

GLOUCESTER RESOURCES LIMITED SPECIALIST CONSULTANT STUDIES
Amended Rocky Hill Coal Project Part 2B: Health Risk Assessment
Report No. 806/14
CONTENTS Page
2B-4
APPENDICES
Appendix 1 Key Differences between the Health Risk Assessment for the 2013 Project and Amended Project ............................................................................................................ 2B-67
FIGURES
Figure 1.1 Locality Plan ................................................................................................................... 2B-14
Figure 1.2 Amended Site Layout ..................................................................................................... 2B-16
Figure 1.3 Amended Mine Area Layout ........................................................................................... 2B-17
Figure 1.4 Private Haul Road .......................................................................................................... 2B-19
Figure 3.1 Resource Company and Privately Owned Residences in the Vicinity of the Site ......... 2B-23
Figure 5.1 The Severity and Frequency of an Adverse Health Impact as a Result of Ambient Air Pollution Exposure (Source: WHO, 2001) ..................................................................... 2B-27
TABLES
Table 3.1 Population Age Profile Used in Analysis ........................................................................ 2B-22
Table 3.2 Community Concerns and Relevant Sections of the HRA ............................................. 2B-24
Table 5.1 NSW Impact Assessment Criteria for PM ...................................................................... 2B-29
Table 5.2 Concentration-Response Functions for PM2.5 based on Jalaludin and Cowie (2012) ... 2B-38
Table 5.3 Concentration-Response Functions for PM10 based on Jalaludin and Cowie (2012) .... 2B-39
Table 5.4 Maximum Predicted Project-only 24-hour Average Concentrations at the Most
Affected Receiver/residence (g/m3) ............................................................................. 2B-40
Table 5.5 Predicted Annual Average Concentrations at the Most Affected Receiver/Residence
(g/m3) ............................................................................................................................ 2B-41
Table 5.6 Baseline Health Incidence Rate per 100,000 used in Risk Calculations ....................... 2B-42
Table 5.7 Predicted Number of Attributable Cases Due to PM2.5 Exposure per 100,000: Gloucester State Suburb ................................................................................................ 2B-44
Table 5.8 Predicted Number of Attributable Cases Due to PM10 Exposure per 100,000: Gloucester State Suburb ................................................................................................ 2B-44
Table 5.9 Predicted Number of Attributable Cases Due to PM2.5 Exposure per 100,000: Faulkland State Suburb (Forbesdale Estate) ................................................................. 2B-45
Table 5.10 Predicted Number of Attributable Cases Due to PM10 Exposure per 100,000: Faulkland State Suburb (Forbesdale Estate) ................................................................. 2B-45
Table 5.11 Summary of National and International Criteria Established Relating to Short-term and Long-term Exposure to NO2 .................................................................................... 2B-49
Table 5.12 Cumulative maximum 1-hour and annual average NO2 concentrations (g/m3) ........... 2B-51
Table 5.13 Short-term and long-term HQs for Potential NO2 concentrations .................................. 2B-52
Table 5.14 Maximum Project-only 24-hour and Annual Average PM10 Concentrations at Private
Receivers/Residences (g/m3) ....................................................................................... 2B-53
Table 5.15 Short-term and long-term HQs for PM10 concentrations ................................................ 2B-53
Table 5.16 Short-term and long-term HIs for PM10 and NO2 concentrations ................................... 2B-54

SPECIALIST CONSULTANT STUDIES GLOUCESTER RESOURCES LIMITED
Part 2B: Health Risk Assessment Amended Rocky Hill Coal Project
Report No. 806/14
2B-5
GLOSSARY OF COMMONLY USED TERMS AND ACRONYMS
ABS Australian Bureau of Statistics
ACS American Cancer Society
CHPP Coal Handling and Preparation Plant
COPD Chronic Obstructive Pulmonary Disease
CRF Concentration Response Function
DA Development Application
DPE Department of Planning and Environment
EIS Environmental Impact Statement
EPHC Environment Protection and Heritage Council
FEV Forced Expiratory Volume
GLCs Ground Level Concentrations
GMR Greater Metropolitan Region
GP General Practitioner
HI Hazard Index
HQ Hazard Quotient
HRA Health Risk Assessment
LOAEL Lowest Observed Adverse Effect Levels
NEPM AAQM National Environment Protection (Ambient Air Quality) Measure
NO Nitric Oxide
NO2 Nitrogen Dioxide
NOAEL No Observed Adverse Effect Level
NOx Oxides of Nitrogen
NSW New South Wales
OEHHA Office of Environmental Health Hazard Assessment
PM Particulate Matter
PM10 Particulate Matter less than 10 micrometres in aerodynamic diameter
PM2.5 Particulate Matter less than 2.5 micrometres in aerodynamic diameter
PPB Part per Billion
PPM Parts per Million
SMC Stratford Mining Complex
UFPs Ultrafine Particles
US EPA United States Environmental Protection Agency
WHO World Health Organisation

GLOUCESTER RESOURCES LIMITED SPECIALIST CONSULTANT STUDIES
Amended Rocky Hill Coal Project Part 2B: Health Risk Assessment
Report No. 806/14
2B-6
DEFINITION OF TERMS
Term Definition
Air dispersion modelling Mathematical simulation of how air pollutants disperse in the ambient atmosphere.
Baseline health incidence
This is an estimate of the incidence rate (number of cases of the health effect per year, usually per 10,000 or 100,000 general population) in the assessment location corresponding to baseline pollutant levels in that location
Beta (β) coefficient The beta value is a measure of how strongly each predictor variable influences the criterion (dependent) variable. The beta is measured in units of standard deviation.
Ambient air quality The state of quality and chemical characteristics of air as it exists in the environment.
Concentration Response Function
A Concentration Response Function (CRF) (reported by epidemiological studies) is the empirically estimated relationship between the concentration of PM and the observed health endpoints of interest (for example, hospital admissions for asthma) in a population.
Carbon monoxide (CO) Carbon Monoxide (CO) is a toxic, colourless, odourless gas produced by burning any fuel.
Emissions Release of pollutants to air
Epidemiological studies These are studies that examine the patterns, causes, and effects of health and disease conditions in defined populations. Epidemiological information is used to plan and evaluate strategies to prevent illness
Exposure Assessment This identifies the groups of people who may be exposed to hazardous pollutants and provides an estimate as to the potential exposure concentrations.
Hazard Assessment Identifies hazards and health endpoints associated with exposure to hazardous pollutants and provides a review of the current understanding of the toxicity and risk relationship of the exposure of humans to the hazards.
Hazard Index A Hazard Index (HI) is the sum of the Hazard Quotients (HQs) for all pathways with similar toxic effects, assuming the health effects are additive
Hazard Quotient A Hazard Quotient (HQ) which is the ratio of predicted concentrations to the ambient air quality criterion
Health Risk Assessment (HRA)
A Health Risk Assessment (HRA) is an analysis that uses information about potentially hazardous pollutants to estimate a theoretical level of risk for people who might be exposed to defined levels of these pollutants. The information comes from scientific studies and measurement data of air emissions.
Lowest Observed Adverse Effect Level (LOAEL)
The lowest tested dose of a substance that has been reported to have no harmful (adverse) health effects on people or animals.
Nitrogen Dioxide (NO2) Nitrogen dioxide (NO2) is a reddish-brown gas. It is a lung irritant and is present in the highest concentrations among other oxides of nitrogen in ambient air. Nitric oxide (NO) and NO2 are collectively known as NOx.
No Observed Adverse Effect Level (NOAEL)
The highest tested dose of a substance that has been reported to have no harmful (adverse) health effects on people or animals.
NOx Oxides of nitrogen (NOx) is a generic term for mono-nitrogen oxides (NO and NO2). The oxides of nitrogen are predominantly (greater than 90%) nitric oxide (NO).
Particulate Matter (PM) Particulate Matter (PM) is a complex mixture of extremely small particles made up of a number of components, including acids (such as nitrates and sulphates), organic chemicals, metals, and soil or dust particles.

SPECIALIST CONSULTANT STUDIES GLOUCESTER RESOURCES LIMITED
Part 2B: Health Risk Assessment Amended Rocky Hill Coal Project
Report No. 806/14
2B-7
DEFINITION OF TERMS (CONT’D)
Term Definition
PM10 Particulate Matter less than 10 micrometres in aerodynamic diameter
PM2.5 Particulate Matter less than 2.5 micrometres in aerodynamic diameter
Risk Characterisation This provides the qualitative/quantitative evaluation of potential risks to human health. The characterisation of risk is based on the review of the dose-response relationship and the assessment of the magnitude of exposure.
Sensitive receiver/ residence locations
Locations where vulnerable members of the community gather e.g. hospitals, schools

GLOUCESTER RESOURCES LIMITED SPECIALIST CONSULTANT STUDIES
Amended Rocky Hill Coal Project Part 2B: Health Risk Assessment
Report No. 806/14
2B-8
This page has intentionally been left blank

SPECIALIST CONSULTANT STUDIES GLOUCESTER RESOURCES LIMITED
Part 2B: Health Risk Assessment Amended Rocky Hill Coal Project
Report No. 806/14
2B-9
EXECUTIVE SUMMARY
Gloucester Resources Limited (the Applicant) proposes to develop and operate an open cut
coal mine, approximately 3.5km to 7km southeast of the Gloucester urban area and
approximately 120km north of Newcastle, New South Wales (NSW) in the Gloucester Basin.
The Applicant contracted Pacific Environment Limited (then Toxikos Propriety Limited) to
update the Health Risk Assessment (HRA) undertaken for the 2013 Project using the air
quality modelling outcomes for the amended Project. The applied HRA methodology was
consistent with the protocols and guidelines recommended by the Australian enHealth Council
(enHealth, 2012a). This HRA addresses likely impacts on community health from exposure to
air emissions from the “amended Rocky Hill Coal Project” (“the amended Project”), considering
the direct health effects from acute (short-term) and chronic (long-term) exposures. Ground
Level Concentrations (GLCs) of key air quality metrics were predicted at discrete locations
around the Site using air dispersion modelling conducted by Pacific Environment (detailed
within the standalone Air Quality Impact Assessment – Part 2A of the Specialist Consultant
Studies Compendium). The emissions of concern addressed in the assessment were
Particulate Matter (PM), diesel exhaust (from activities associated with open cut coal mining)
and nitrogen dioxide (NO2) (resulting from blasting).
The exposure assessment used estimates of the total potential cumulative exposure
(i.e. background plus modelled PM2.5 and PM10 increment from the amended Project) on an
annual and daily basis at the most affected private receivers/residences (receiver 6 in
Gloucester and receiver 18 in Forbesdale) on the worst day of each modelled year. By using
the modelled predictions at the most affected private receivers/residences to represent
exposure across the populations of the respective state suburbs, the overall community
exposure is over estimated and the resulting HRA should be considered conservative. The air
quality impact assessment for the amended Project (Pacific Environment, 2016) presents the
dispersion modelling predictions for maximum 24-hour and annual average PM2.5 and PM10
GLCs at a total of 160 non-resource related assessment locations i.e. 157 privately-owned
receivers/residences in the vicinity of the Site and 3 sensitive receiver locations with the
Gloucester township. For both PM2.5 and PM10, the full dataset based on the 160 assessment
locations in conjunction with background were examined as part of the HRA.
The health endpoints assessed for PM2.5 and PM10 were short- and long-term mortality and
daily hospitalisations. The general approach used to calculate the risks to health has drawn
upon estimates determined to be relevant to the Australian context in order to determine the
impact of PM2.5 and PM10 on health in relation to the known health indicators for NSW. This
involved estimating the change in the incidence of a health outcome resulting from a given
change in PM2.5 and PM10 concentrations. Concentration-Response Functions (CRFs) for each
of the health endpoints were sourced from the review conducted by Jalaludin and Cowie 2012.
In examining the increased risk in the population as a consequence of the amended Project
(based on annual mortality rates, all causes) due to the increased long-term exposure to PM2.5
and PM10 concentrations as a result of cumulative and project-only exposure, it is noted that
the number of attributable health outcomes would be well below 1 in 100,000. The predicted
number of attributable cases are therefore considered to be “sufficiently small and to be of no
cause for concern” (NEPM AAQM). Shorter term exposures to PM2.5 and PM10 are also
considered not to pose an unacceptable risk as the predicted number of attributable cases due
to daily mortality (all cause all ages and cardiovascular disease all ages are less than 1 in
orders of magnitude lower than that due to long-term exposure.

GLOUCESTER RESOURCES LIMITED SPECIALIST CONSULTANT STUDIES
Amended Rocky Hill Coal Project Part 2B: Health Risk Assessment
Report No. 806/14
2B-10
The critical health outcomes from acute and chronic exposure to NO2 include respiratory
disease and associated symptoms, and associated changes in lung function. The NSW EPA
impact assessment criteria, which are protective of these health outcomes in sensitive
subpopulations, have been used to determine the potential for acute effects (246µg/m3) and
chronic effects (62µg/m3) in association with exposure to NO2 from the amended Project. As
NO2 emissions for the selected receivers/residences were less than the Australian air quality
criterion, it is considered unlikely that the blast emissions would cause direct acute and/or
chronic health effects.
The calculated HQs for blast NO2 emissions for the worst affected private receivers/residences
are all less than 1, therefore it is unlikely the cumulative NO2 emissions i.e. blasting, diesel
powered equipment and background monitoring data, would cause direct short-term and/or
long-term health effects. The calculated HIs for short-term cumulative blast and fuel
combustion associated NO2 and PM10 were slightly greater than unity (greater than 1) at three
of the four worst affected private receivers/residences. All the long-term HIs were less than
unity (less than 1). As such there is only a potential for short-term health effects due to
exposure from cumulative blast and fuel combustion associated NO2 and PM10. Given the
conservative approach to predicting NO2 emissions, it is considered appropriate that potential
short-term effects can be mitigated by the use of measures known to minimise fume
generation blast design, product selection and quality, blast crew education, on bench
practices and, and blasting under wind conditions that favour dispersion of pollutants. Each of
these measures would be identified in a Blast Fume Management Strategy appended to the
Blast Management Plan for the amended Project in order to prevent the modelled NO2
concentrations occurring that were utilised in this assessment.
Diesel exhaust particles are primarily PM2.5 (including a considerable component of ultrafine
particles, PM0.1) (WIMR-CAR, 2015). The organic fraction of diesel exhaust particulate matter
contains compounds such as aldehydes, alkanes and alkenes, aliphatic hydrocarbons,
polycyclic aromatic hydrocarbons and their derivatives. These substances are considered toxic
air contaminants and some of them are genotoxic and carcinogenic. Overall diesel exhaust
particles are considered to be carcinogenic (OEHHA, 2001). Therefore, it has been considered
appropriate to further assess the carcinogenic inhalation risk using the project-only PM2.5 –
diesel concentration i.e. the highest annual average PM2.5 – diesel concentration combined
with background monitoring data (receiver/residence 18 in Year 10).
This concentration was applied across the whole population i.e. Gloucester State Suburb and
Faulkland State Suburb (Forbesdale Estate) providing a conservative estimate of the potential
cancer risk. This PM2.5 – diesel concentration was then multiplied by the cancer unit risk factor
i.e. 0.000034 μg/m3, derived by the World Health Organisation (WHO) and an adjustment
factor (0.25). The resultant risk, 0.31 in 100,000 / 3.1 in 1,000,000, is within the acceptable
cancer risk range, i.e. 1 in 100,000 to 1 in 1,000,000 generally accepted by NSW, national and
international authorities, for airborne contaminants. In addition, it should be noted that real-time
monitoring of PM2.5 and PM10 particulates, reactive management of all particle emissions, and
regular maintenance of diesel vehicles and machinery on site, would reduce the exposure of
the community to diesel particles and further reduce potential risks to health.
There are inherent uncertainties in the methods used to estimate emissions and
concentrations and limitations on how accurately the impacts of the amended Project can be
estimated in future years. As such, in order to minimise the risk of under estimation throughout
the HRA, conservatism has been applied where possible. The modelling data used to inform

SPECIALIST CONSULTANT STUDIES GLOUCESTER RESOURCES LIMITED
Part 2B: Health Risk Assessment Amended Rocky Hill Coal Project
Report No. 806/14
2B-11
this HRA used worst case assumptions and therefore it is expected that actual ground level
concentrations would be lower during the normal operation of the amended Project. The
modelled predictions at the most affected private receivers/residences were used to represent
exposure across the populations of the respective state suburbs and consequently the overall
community exposure was over estimated. The PM2.5 and PM10 exposure assessment evaluates
the potential of the emissions to cause direct effects on individuals who may be exposed either
on a short-term, infrequent basis or long-term basis, i.e. assuming 24 hours per day for each
day of the year for 70 years. This exposure scenario is highly unlikely especially since the life
of the mine is estimated to be up to 21 years.
The applied exposure assessment method for PM2.5 and PM10 is typically reserved for
populations of greater than 25,000 because there are important challenges in translating
methods intended for large populations to those for addressing risk in smaller populations.
Nevertheless, when taken together with the modelling predictions, the uncertainties err on the
side of safety. The predicted NO2 emissions due to blasting considered a range of
meteorological conditions, including unrealistic scenarios of blasting during unfavourable
conditions and assuming a worst case Level 4 fume category, which over-estimated the peak
concentrations of NO2 at the selected private receivers/residences. The PM2.5 – diesel
exposure assessment used PM2.5 – diesel modelled predictions based on the highest diesel
consumption for any of the mining years, from a mine operation year (Year 7) predicted to
have the highest predicted PM2.5 concentration.
In consideration of the community concerns raised, it is important to note that health issues in
relation to exposure to PM - total, cumulative NO2 and PM2.5 – diesel from the amended Project
have been outlined and the associated potential for acute or chronic effects assessed. The
exposure assessments have used both standards adopted by all Australian jurisdictions and
exposure response functions relevant to the Australian population (where relevant) to estimate
likelihood of unacceptable risk. Susceptible/ vulnerable groups within adjacent communities
have been taken into consideration and a range of health end points assessed, i.e. short- and
long-term mortality and daily hospitalisations. Overall it is concluded that air emissions from
the amended Rocky Hill Coal Project present little likelihood of causing adverse health effects
to exposed individuals in the vicinity of the Site.

GLOUCESTER RESOURCES LIMITED SPECIALIST CONSULTANT STUDIES
Amended Rocky Hill Coal Project Part 2B: Health Risk Assessment
Report No. 806/14
2B-12
This page has intentionally been left blank

SPECIALIST CONSULTANT STUDIES GLOUCESTER RESOURCES LIMITED
Part 2B: Health Risk Assessment Amended Rocky Hill Coal Project
Report No. 806/14
2B-13
1. I N T RO D U C TI ON
1.1 SCOPE OF WORK
Gloucester Resources Limited (the Applicant) proposes to develop and operate an open cut
coal mine, approximately 3.5km to 7km southeast of the Gloucester urban area, approximately
120km north of Newcastle, New South Wales (NSW) in the Gloucester Basin (Figure 1.1).
The Applicant contracted Pacific Environment Limited (then Toxikos Propriety Limited) to
update the Health Risk Assessment (HRA) undertaken for the 2013 Project using the air
quality modelling outcomes for the “amended Rocky Hill Coal Project” (“the amended Project”).
The applied HRA methodology was consistent with the protocols and guidelines recommended
by the Australian enHealth Council (enHealth, 2012a). This HRA addresses likely impacts on
community health from exposure to air emissions from the amended Project, considering the
direct health effects from acute (short-term) and chronic (long-term) exposures. It evaluates
the potential of the emissions to cause direct effects on individuals who may be exposed either
on a short-term, infrequent basis or long-term basis, i.e. assuming 24 hours per day for each
day of the year for 70 years. Thus, from the aspect of long-term exposure assumptions, the
HRA is conservative (i.e. errs on the side of safety), as the life of the mine is estimated to be
up to 21 years.
Ground Level Concentrations (GLCs) of key air quality metrics were predicted at discrete
locations around the Site using air dispersion modelling conducted by Pacific Environment
(detailed within the standalone Air Quality Impact Assessment – Part 2A of the Specialist
Consultant Studies Compendium). The emissions of concern addressed in the HRA
assessment were Particulate Matter (PM), diesel exhaust (from activities associated with open
cut coal mining) and nitrogen dioxide (NO2) (resulting from blasting activities and fuel
combustion).
The HRA has been facilitated by provision of spreadsheet results from the dispersion
modelling undertaken by Pacific Environment Limited (presented within the Air Quality Impact
Assessment – Part 2A of the Specialist Consultant Studies Compendium). These modelled
outputs contain predicted Ground Level Concentrations (GLCs) of individual pollutants at a
total of 160 non-resource related assessment locations i.e. 157 privately-owned
receivers/residences in the vicinity of the Site and 3 sensitive receiver locations with the
Gloucester township.
1.2 BACKGROUND
In August 2013, Gloucester Resources Limited (“the Applicant”) submitted a Development
Application (No. SSD 5156) for the Rocky Hill Coal Project (the 2013 Project) which was
supported by an Environmental Impact Statement (EIS) prepared by R.W. Corkery & Co. Pty
Limited on behalf of the Applicant. The 2013 Project comprised the development of an open-
cut coal mine to produce up to 2.5 million tonnes per annum (Mtpa) of run-of-mine (ROM) coal,
a coal handling and preparation plant (CHPP), an overland conveyor and a rail load-out facility.
The 2013 Project also anticipated up to 1.75Mtpa of product coal would be transported by rail
to the Port of Newcastle for export. The Mine Area for the 2013 and amended Project is
situated 3.5km to 7.0km southeast of the Gloucester urban area within the former Gloucester
Local Government Area, in New South Wales (NSW).

GLOUCESTER RESOURCES LIMITED SPECIALIST CONSULTANT STUDIES
Amended Rocky Hill Coal Project Part 2B: Health Risk Assessment
Report No. 806/14
2B-14
Figure 1.1 Locality Plan

SPECIALIST CONSULTANT STUDIES GLOUCESTER RESOURCES LIMITED
Part 2B: Health Risk Assessment Amended Rocky Hill Coal Project
Report No. 806/14
2B-15
In June 2015, the Applicant submitted a request that the NSW Department of Planning and
Environment (DPE) to place the determination of its development application on hold as it was
in negotiations regarding a potential commercial arrangement with the owner of the Stratford
Mining Complex, Yancoal Australia Limited (Yancoal). In December 2015, the Applicant and
Yancoal formally advised DPE that a commercial agreement had been reached between the
two companies whereby sized ROM coal would be transported from the Rocky Hill Mine Area
to the Stratford Mining Complex via a private haul road and processed in the Stratford CHPP
before being loaded onto rail for transportation to the Port of Newcastle. Hence the amended
Project will no longer require its own CHPP, overland conveyor, rail loop or train loader.
1.3 OVERVIEW OF THE AMENDED PROJECT
The proposed amended Rocky Hill Coal Project comprises three principal components (see
Figure 1.2).
1. The “Mine Area” incorporating three contiguous open cut pits, a run-of-mine
(ROM) pad with a breaker station and sized coal bin, amenity barriers,
overburden emplacements and an administration area with site offices,
amenities, workshop, water treatment plant and ancillary facilities.
2. The “private haul road”, a 4.4km sealed road to be used for the transportation of
sized coal from the Rocky Hill Mine Area to the Stratford Mining Complex for
washing and despatch to the Port of Newcastle. The private haul road extends
from the southern boundary of the Rocky Hill Mine Area to the northern boundary
of the Stratford Mining Complex, owned by Stratford Coal Pty Limited.
3. Two “power line corridors” incorporating a re-located 132kV power line and a new
low voltage (11kV or as nominated by Essential Energy) power line external to
the Rocky Hill Mine Area.
Each of these components is located in an area referred to as “the Site”.
Figure 1.3 displays the conceptual layout of the Mine Area, including the following major
components.
The Mine Area entrance off McKinleys Lane, approximately 50m south of the
intersection with Waukivory Road.
An administration area, incorporating site offices, amenities, workshop, water
treatment plant and ancillary facilities. The administration area is located on land
off McKinleys Lane and would be accessed by a private road, referred to as the
Mine Area access road, which would be aligned generally parallel to and
immediately east of McKinleys Lane.
Three contiguous open cut pits (Avon, Bowen Road and Main) varying in depth
from approximately 80m to 220m. Though based on current planning, the open
cut pit depths nominated are approximate only given the steeply dipping nature of
the coal seams, the extent of geological knowledge, and the potential effects of
changes in controlling economic factors. The ultimate depths of development in
each open cut pit would reflect the optimisation of coal quality, the outcomes of
detailed planning as coal extraction progresses and market factors.

GLOUCESTER RESOURCES LIMITED SPECIALIST CONSULTANT STUDIES
Amended Rocky Hill Coal Project Part 2B: Health Risk Assessment
Report No. 806/14
2B-16
Figure 1.2 Amended Site Layout

SPECIALIST CONSULTANT STUDIES GLOUCESTER RESOURCES LIMITED
Part 2B: Health Risk Assessment Amended Rocky Hill Coal Project
Report No. 806/14
2B-17
Figure 1.3 Amended Mine Area Layout

GLOUCESTER RESOURCES LIMITED SPECIALIST CONSULTANT STUDIES
Amended Rocky Hill Coal Project Part 2B: Health Risk Assessment
Report No. 806/14
2B-18
A series of interim and long-term amenity barriers to visually screen areas of
activity and/or to provide for noise mitigation. The upper surfaces of the barriers
would either mimic the existing underlying landform or provide a variable
comparatively natural appearance. The barriers would either be stand-alone
structures (i.e. the western and northern amenity barrier) or comprise the western
faces of the permanent overburden emplacement as it is progressively
developed, i.e. interim amenity barriers.
A consolidated in-pit overburden emplacement and permanent out-of-pit
overburden emplacement extending to the west of the open cut pits. An interim
overburden emplacement which would be located to the north of the permanent
overburden emplacement but would be removed at the cessation of coal
extraction to provide some of the backfill for the final void in the Main Pit.
A ROM pad and associated breaker station comprising a feed conveyor, rotary
breaker, a sized coal conveyor and a nominal 500t capacity overhead sized coal
bin from which 60t nominal capacity road-registered trucks would be loaded. The
ROM pad would have a capacity to store approximately 80 000t of coal awaiting
processing through the breaker station, i.e. sufficient capacity for approximately
two weeks production at the maximum scheduled production rate.
A 5km section of re-located 132kV power line and a new 11kV power line
providing power for the on-site operations. The remaining sections of the re-
located 132kV power line and the 11kV power line lie external to the Mine Area
within the defined power line corridors.
Figure 1.4 displays the 4.4km private haul road comprising a minimum 7m seal on a 10m
formation extending between the sized coal bin and the boundary of ML1733, the northern
extent of the Stratford Mining Complex. The private haul road would link with a section of new
road to be constructed within ML1733 and then into the existing on-site haul road system
within the Stratford Mining Complex.
In light of this amendment, the Applicant has re-designed the open cut pits and mine
sequencing to focus on the production of metallurgical coal and is not proceeding with the
construction and operation of the on-site CHPP, overland conveyor, rail loop and rail load-out
facility.

SPECIALIST CONSULTANT STUDIES GLOUCESTER RESOURCES LIMITED
Part 2B: Health Risk Assessment Amended Rocky Hill Coal Project
Report No. 806/14
2B-19
Figure 1.4 Private Haul Road

GLOUCESTER RESOURCES LIMITED SPECIALIST CONSULTANT STUDIES
Amended Rocky Hill Coal Project Part 2B: Health Risk Assessment
Report No. 806/14
2B-20
2. M ET H O DO LO GY
2.1 WHAT IS A RISK ASSESSMENT?
Health is defined by the World Health Organization (WHO) as a state of complete physical,
mental and social well-being and not merely the absence of disease or infirmity (WHO, 1948).
Well-being is broadly described as an individual’s self-assessment of their state of happiness,
healthiness and prosperity. It relates to the quality of life and one’s ability to enjoy it. There are
many social and economic factors that impinge upon well-being.
The following are examples of determinants of health well-being (enHealth 2012a, NHC 2004):
Social and cultural factors (e.g. social support, participation, access to cultural
resources).
Economic factors (e.g. income levels, access to employment).
Environmental factors (e.g. land use, air quality).
Population-based services (e.g. health and disability services, leisure services).
Individual/behavioural factors (e.g. physical activity, smoking).
Biological factors (e.g. biological age).
According to enHealth (2012a), all developments have a potential impact on health. Some
would have positive health impacts by providing jobs, attracting health services to an area, and
improving overall economic well-being of a community, etc. Other developments may have
negative impacts such as increased risk of disease, social disruption, increased noise etc.
Many developments would have both positive and negative aspects. It should be understood
that the potential influence of the amended Project on local area economic factors, social
disruption and other such factors are not addressed in this document. These matters are
addressed as part of the Social Impact Assessment and Economic Impact Assessment (Parts
14 and 15 of the Specialist Consultant Studies Compendium). Air quality is one of the many
parameters influencing well-being. This HRA seeks to evaluate what the likelihood is for direct
health effects when exposures to air emissions from the amended Project occur.
A health risk assessment is an analysis that uses information about potentially hazardous
pollutants to estimate a theoretical level of risk for people who might be exposed to defined
levels of these pollutants.
Risk assessments are often conducted by considering possible or theoretical community
exposures based on the outcomes of air dispersion modelling. Conservative safety margins
are built into a risk assessment analysis to ensure protection of the public. Therefore, people
would not necessarily become unwell even if they are exposed to pollutants at higher
concentration levels than those estimated by the risk assessment. During a risk assessment
analysis, the most vulnerable people (e.g. children, the sick and elderly) are carefully
considered to make sure that all members of the public would be protected.

SPECIALIST CONSULTANT STUDIES GLOUCESTER RESOURCES LIMITED
Part 2B: Health Risk Assessment Amended Rocky Hill Coal Project
Report No. 806/14
2B-21
The risk assessment helps answer the following common questions for people who might be
exposed to hazardous pollutants in the environment, in this case components of the air
emissions from the amended Project.
Under what circumstances might I, my family and neighbours be exposed to
hazardous pollutants from the amended Project?
Is it possible we might be exposed to hazardous pollutants at levels higher than
those determined to be safe?
If the levels of hazardous pollutants are higher than regulatory standards, what
are the health effects that might occur?
The HRA is a useful tool for estimating the likelihood and severity of risks to human health,
safety and the environment and for informing decisions about how to manage those risks. It is
a document that assembles and synthesizes scientific information to determine whether a
potential hazard exists and/or the extent of possible risk to human health.
Although this report describes certain technical aspects of the risk assessment, it does not
address the processes of risk management and risk communication.
2.2 OVERALL APPROACH
The methodology adopted in the conduct of this HRA is consistent with the protocols and
guidelines recommended by the enHealth Council. These are detailed in the document
“Environmental Health Risk Assessment: Guidelines for assessing human health risks from
environmental hazards” (enHealth, 2012a).
The development of a formalised HRA has resulted in the process being categorised into
distinct stages. Some of the key factors and questions that are taken into consideration at each
of these stages include the following.
1. Hazard Assessment
Identifies hazards and health endpoints associated with exposure to hazardous
pollutants and provides a review of the current understanding of the toxicity and
risk relationship of the exposure of humans to the hazards.
2. Exposure Assessment
This task identifies the groups of people who may be exposed to hazardous
pollutants and provides an estimate as to the potential exposure concentrations.
3. Risk Characterisation
This task provides the qualitative/quantitative evaluation of potential risks to
human health. The characterisation of risk is based on the review of the dose-
response relationship and the assessment of the magnitude of exposure.

GLOUCESTER RESOURCES LIMITED SPECIALIST CONSULTANT STUDIES
Amended Rocky Hill Coal Project Part 2B: Health Risk Assessment
Report No. 806/14
2B-22
3. C OM M U NI TY PR O FI L E
This section discusses the community adjacent to the Site of the amended Project that may
potentially be affected by emissions over its lifetime. Figure 1.1 illustrates the location of the
amended Project and the potentially affected communities.
3.1 SURROUNDING AREA AND POPULATION
The Site is located approximately 120km north of Newcastle in the Gloucester Basin. The
amended Project is located in a rural area characterised by cattle (beef and dairy) grazing on
native and improved pastures, with intervening areas of remnant bushland. Other land uses in
the local area include rural residential, the existing Stratford Mining Complex (SMC) to the
south, residential development in Gloucester and other townships such as Stratford,
Barrington, Craven, estates such as Forbesdale and areas of National Park/Nature Reserve.
There are a number of privately-owned and resource company-owned residences in the
vicinity of the Site, as shown on Figure 3.1, with resource company-owned residences
comprising those owned by GRL, Yancoal, AGL or associated companies. Properties under a
purchase option to the Applicant subject to the receipt of development consent and/or a mining
lease are also identified as resource company-owned.
3.2 POPULATION PROFILE
The composition of the population in Gloucester, as defined by the State Suburb boundaries,
was reviewed. The State suburb of Gloucester includes the township of Gloucester as well as
the Avon River and Thunderbolt residential estates (Figure 1.1). There is no statistical
breakdown only covering the Forbesdale Estate area (Figure 1.1), therefore, given it is wholly
located within the Faulkland State Suburb, Faulkland State Suburb data has been used to
assess the health issues in the Forbesdale Estate. The population statistics considered for this
assessment are available from the Australian Bureau of Statistics (ABS) website for the
census year 2011 and are summarised in Table 3.1.
Table 3.1
Population Age Profile Used in Analysis
Age Group
Number of individuals
Gloucester State Suburb Faulkland State Suburb
(Forbesdale Estate)
All ages 2878 241
65+ years 799 57
30+ years 2017 176
15-64 years 1607 151
0-14 years 472 33
Source: ABS data 2011

SPECIALIST CONSULTANT STUDIES GLOUCESTER RESOURCES LIMITED
Part 2B: Health Risk Assessment Amended Rocky Hill Coal Project
Report No. 806/14
2B-23
Figure 3.1 Resource Company and Privately Owned Residences in the Vicinity of the Site

GLOUCESTER RESOURCES LIMITED SPECIALIST CONSULTANT STUDIES
Amended Rocky Hill Coal Project Part 2B: Health Risk Assessment
Report No. 806/14
2B-24
3.3 RESIDENCES AND SENSITIVE RECEIVERS
The HRA considers locations where maximum impacts of the amended Project may occur as
well as the adjacent locations where people live, i.e. Gloucester (including the Thunderbolt and
Avon River Estates) and Forbesdale. A total of 157 private receivers/residences, where people
reside and 3 sensitive receiver locations, where people gather were assessed. The
receivers/residences therefore captured the sensitive members in the communities, i.e. the
very young (0-14 years) and the elderly (65+years).
3.4 COMMUNITY CONCERNS
As part of the approval process, the Applicant initially lodged an Environmental Impact
Statement (EIS) for the 2013 Project to the (then) Department of Planning and Infrastructure
(DP&I). DP&I sought public comment on the EIS between 28 August 2013 and
28 October 2013. The concerns raised through this process were captured within the formal
response to submissions on the EIS for the 2013 Project, with the relevant sections of the HRA
for the amended Project addressing these as identified in Table 3.2.
Table 3.2
Community Concerns and Relevant Sections of the HRA
Concern Section
General health issues from air pollution 5.2 - 5.4
The potential for asthma impacts on children within 5km of the mine 5.2 - 5.4
Potential impacts of PM2.5 and PM10 to the susceptible/ vulnerable groups within adjacent communities
5.2
The range of health effects considered for the adjacent communities 5.2.1.4
Health effect due to diesel emissions 5.4
Use of appropriately stringent criteria in the assessment 5.2.1, 5.3.1 & 5.4

SPECIALIST CONSULTANT STUDIES GLOUCESTER RESOURCES LIMITED
Part 2B: Health Risk Assessment Amended Rocky Hill Coal Project
Report No. 806/14
2B-25
4. O VE RVI E W O F AI R Q U AL I T Y AS S E S SM E N T
A brief overview of the Air Quality Assessment is provided in the following subsections. Further
detail regarding the existing air quality environment, modelling methodology and modelling
outcome is provided within the Air Quality Assessment – Part 2A of the Specialist Consultant
Studies Compendium.
4.1 EXISTING AIR QUALITY
In July 2010, an air quality monitoring program was established to determine the baseline air
quality and meteorological conditions in the vicinity of the Mine Area. The monitoring network
consists of eight dust deposition gauges measuring dust deposition rates over the period of
one month, two Tapered Element Oscillating Microbalance (TEOMs) measuring continuous
PM10 and PM2.5 concentrations for 24-hour periods, two high volume air samplers (HVASs)
measuring PM10 concentrations for 24 hours periods on a one day in six run cycle and a
meteorological monitoring station. Prevailing winds at the Site are from the south and
northeast on an annual basis, and are similar but slightly different to winds measured at the
Stratford Mining Complex meteorological station, approximately 7km south of the Mine Area.
A review of the air quality monitoring data indicates that ambient air quality in the Stroud-
Gloucester Valley is generally good and well below the relevant ambient air quality criteria.
4.2 AIR QUALITY ASSESSMENT SCENARIOS
Mining operations would involve the sequential activities of vegetation clearing, soil stripping,
overburden/interburden removal, coal recovery, breaking of coal to <120mm, transportation of
sized coal via the private haul road, and progressive rehabilitation of the Mine Area. Four
operational scenarios were therefore chosen for quantitative air quality dispersion modelling.
These years, along with their rationale for selection, are provided below and were further
assessed in the Air Quality Assessment with the outcomes of the modelling used in this HRA.
1. Year 1: Representative of the development of the open cut pit and the western
and northern amenity barrier. Minimal ROM coal production and
operations restricted to day time only.
2. Year 4: Representative of operations at the commencement of day and evening
operations and ramping up of overburden and ROM coal production.
3. Year 7: Representative of operations at maximum overburden production, 80%
of maximum coal production and a wide geographic spread of activities
across the Mine Area.
4. Year 10: Representative of operations at maximum overburden production and
95% of maximum coal production but with mining activities occurring at
depth and overburden emplacement predominantly occurring in-pit.

GLOUCESTER RESOURCES LIMITED SPECIALIST CONSULTANT STUDIES
Amended Rocky Hill Coal Project Part 2B: Health Risk Assessment
Report No. 806/14
2B-26
4.3 AIR QUALITY ASSESSMENT OUTCOMES
The modelling indicates that no private receivers/residences are predicted to experience 24-
hour average PM10 or PM2.5 levels above the criterion of 50 μg/m3 and 25 μg/m3 respectively
across all mining years. There are no private receivers/residences that are predicted to
experience annual average PM10, PM2.5, TSP or dust deposition above the assessment criteria,
either from the amended Project alone or cumulatively.

SPECIALIST CONSULTANT STUDIES GLOUCESTER RESOURCES LIMITED
Part 2B: Health Risk Assessment Amended Rocky Hill Coal Project
Report No. 806/14
2B-27
5. H E ALT H R I S K AS S E S SM E N T
5.1 IDENTIFICATION OF EMISSIONS OF HAZARDOUS POLLUTANTS
Open cut mines, such as that proposed in the amended Project, mine coal using open cut
methods, predominately using haul trucks and hydraulic excavators. Emissions may occur
during the six distinct stages of the mining process i.e. land preparation, blasting, overburden
removal, coal recovery, coal processing and transport off site, and mined land rehabilitation. In
consideration of these activities, the main pollutants would be particulate matter (PM) and
oxides of nitrogen (NOx). Fugitive PM would be emitted at every stage of the mining process.
PM is typically characterised in terms of its size fractions, with common metrics for health
assessment being PM less than 10 micrometres in aerodynamic diameter (PM10) and PM less
than 2.5 micrometres in aerodynamic diameter (PM2.5). NOx would most likely be emitted
during the blasting phase of the mining process, and would comprise both nitric oxide (NO)
and nitrogen dioxide (NO2). From the point of view of impacts on human health and frequency
of exposure, it is PM which is of greatest concern.
The adverse health effects resulting from exposure to ambient pollutants, such as PM and
NO2, range from the relatively mild sub-clinical effects such as throat irritation, to clinical effects
of reduction in lung function or increased medication usage, through to seeking medical
attention from a General Practitioner (GP), emergency department attendances, hospital
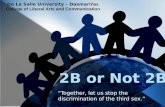
admission and premature mortality due to various diseases. Figure 5.1 illustrates the
relationship between the frequency of an adverse health outcome and its severity. Mortality
and hospital admissions are often studied in relation to ambient air pollutants, since they are
clearly defined health outcomes that have a measurable impact on the community. Further
discussion on the health endpoints of concern with respect to PM and NOX are provided in
Section 5.2.1 and Section 5.3.1.
Figure 5.1 The Severity and Frequency of an Adverse Health Impact as a Result of Ambient Air Pollution Exposure (Source: WHO, 2001)
Premature mortality
Hospital admissions
Emergency room visits
GP visits
Restricted activity/reduced performance Medication use
Symptoms
Impaired pulmonary functions
Subtle effects
Proportion of population affected
Severity of health impacts

GLOUCESTER RESOURCES LIMITED SPECIALIST CONSULTANT STUDIES
Amended Rocky Hill Coal Project Part 2B: Health Risk Assessment
Report No. 806/14
2B-28
5.2 ASSESSMENT OF PARTICULATE MATTER
5.2.1 Hazard Assessment
5.2.1.1 Types of Particulate Matter and Assessment Criteria
Particulate Matter (PM) is an air-suspended mixture of solid and liquid particles that vary in
number, size, shape, surface area, chemical composition, solubility and origin. PM is classified
by aerodynamic diameter, as size is a critical determinant of the likelihood and site of
deposition within the respiratory tract.
1. PM10 includes all inhalable particles less than 10 µm aerodynamic diameter.
These are sufficiently small to penetrate to the thoracic region. Coarse particles
consist of those between PM2.5 and PM10 (i.e. PM2.5-10) and sometimes may be
referred to as ‘thoracic’ particles.
2. PM2.5 (fine particles) includes those inhalable particles less than 2.5 µm
aerodynamic diameter. These have a high probability of deposition in the smaller
conducting airways and alveoli.
3. PM10 includes coarse, fine and ultrafine particles (< 0.1 μm).
4. PM2.5 includes fine and ultrafine particles (< 0.1 μm).
Both natural (e.g. crustal dust eroded from the earth’s surface) and anthropogenic processes
(e.g. mining, quarrying, wood fires) contribute to the atmospheric load of PM. The human
contribution to ambient PM in urban regions often exceeds the contribution from natural
sources and results in higher ambient PM concentrations compared to non-urban background
sites which receive lower contributions of PM generated by human activities. It has been
estimated that in 2008 in the Greater Metropolitan Region (GMR) of NSW (incorporating the
greater Sydney, Newcastle and Wollongong areas), the majority of PM emissions (>70%) were
of anthropogenic origin (Hime et al 2015). Coal mining in the GMR is estimated to contribute
~45% of the PM emissions i.e. 42.5% PM10 and 22.6% of PM2.5, via associated activities such
as coal extraction, transfer & loading of coal, removal of overburden and wheel generated dust
(NSW EPA 2012; WIMR-CAR 2015, Katestone 2011).
The generated dust can come from either disturbance of soil (e.g. land preparation and wheel
generated emissions from haul trucks), or coal dust (excavators digging soil and stockpiling the
coal). Coal dust is a fine powdered form of coal that is created during its mining, processing
and transportation. Most of the coal dust emissions are in the coarse particle fraction (PM2.5-10)
rather than PM2.5. However the amount of dust generated during mining and coal processing
depends on weather conditions, local geology, mining/processing activity, and methods of dust
suppression (Hime et al 2015).
All particles, irrespective of their origin, appear to cause adverse health impacts. In recent
years, a significant amount of research has focused on the health effects of particles and an
increasing body of literature reports associations between PM and adverse health effects. A
range of health effects have been found for both PM10 and PM2.5, with the majority of the
information coming from population-based epidemiological studies.

SPECIALIST CONSULTANT STUDIES GLOUCESTER RESOURCES LIMITED
Part 2B: Health Risk Assessment Amended Rocky Hill Coal Project
Report No. 806/14
2B-29
Table 5.1 presents a summary of the established NSW EPA impact assessment criteria (other
than PM2.5 which is drawn from NEPM 2016).
Table 5.1
NSW Impact Assessment Criteria for PM
Pollutant Averaging
period Criteria (µg/ m
3) Reference
PM2.5 24-hour 25 NEPM (2016)
Annual 8 NEPM (2016)
PM10 24-hour 50* NSW DEC (2005)
Annual 30 NSW DEC (2005)
*one exceptional exceedance
5.2.1.2 Coal Dust
Health consequences of significant coal dust exposure have been suspected ever since an
increase in the prevalence of pneumoconiosis became evident among coal workers in South
Wales in the 1930s (Heppleston 1992). There are many occupational exposure studies on coal
mine workers that have shown an association between coal dust exposure and
pneumoconiosis, chronic bronchitis, emphysema and loss of lung function (Heppleston 1992,
Wouters et al. 1994, Petsonk et al. 2013). Data indicate a dose-response relationship between
coal dust inhalation and the incidence and severity of pneumoconiosis as well as the
development of emphysema and chronic bronchitis (Finkelman et al. 2002, Cohen et al. 2009).
Though occupational exposure to coal dust can cause serious, sometimes fatal, respiratory
disease, the effects of occupational exposure cannot be directly extrapolated to the effects of
non-occupational exposures in the general community. Occupational exposure is often
substantially greater than community exposure due to the proximity of workers to the emission
source and the dispersion of coal dust in the atmosphere (Hime et al 2015).
No Australian studies have specifically examined the health effect of non-occupational
exposures to coal dust, however, there have been studies of the health of coal mining
communities. These studies report higher rates of respiratory disease, cardiovascular disease
and increased presentations to hospital emergency departments for asthma (NSW Health
2010a, NSW Health 2010b). None of these investigations included air pollution data in the
analyses, therefore, it is not clear whether any differences in health outcomes in areas
surrounding coal mining activity, compared to populations elsewhere, are the result of
exposure to locally emitted PM. Furthermore, the health data from these studies were not
adjusted for other possible causes of chronic disease such as rates of smoking and dietary
habits, making it problematic to assign any observed poor health outcomes to the
environmental health effects of coal mining. Given the limitations to the research to date, there
is insufficient evidence that reported adverse health outcomes in Australian communities
surrounding coal mining operations are related to exposure to coal dust. However,
observations of higher rates of respiratory and cardiovascular outcomes in some coal mining
areas warrant further investigation to determine associations between health outcomes
(adjusted for known causes of disease) and exposure to PM derived from coal mining activities
(NSW Health 2010a; NSW Health 2010b; WIMR-CAR 2015). Given the foregoing, the
following sections describe the hazardous effects of PM.

GLOUCESTER RESOURCES LIMITED SPECIALIST CONSULTANT STUDIES
Amended Rocky Hill Coal Project Part 2B: Health Risk Assessment
Report No. 806/14
2B-30
5.2.1.3 Health Effects of Particulate Matter
The health effects of particles linked to ambient exposures have been well studied and
reviewed by international agencies (NEPM, 2010; US EPA, 2004, 2009, 2012; WHO, 2006,
2013; OEHHA, 2000). In recent years, a large amount of research has focussed on the health
effects of particles and an increasing body of literature reports associations between particles
and adverse health effects. Effects have been found for both PM10 and PM2.5 and, to a lesser
extent, ultrafine particles (UFPs). Most information comes from population-based
epidemiological studies that find increases in daily mortality, as well as morbidity outcomes
such as increases in hospital admissions and emergency room attendances, and exacerbation
of asthma to be associated with daily changes in ambient particle levels. There has been an
increasing focus on the link between exposure to particles and cardiovascular outcomes. In
addition to studies on the various size metrics for particles, research has also investigated the
role of particle composition in the observed health effects (US EPA, 2009, 2012; WHO, 2013).
The evidence on the health effects of particles comes from several major lines of scientific
investigation: characterisation of inhaled particles; consideration of the deposition and
clearance of particles in the respiratory tract and the doses delivered to the upper and lower
airway and the alveoli; animal and cellular studies of toxicity; studies involving inhalation of
particles by human volunteers; and population-based epidemiological studies. The findings of
these different lines of investigation are complementary and each has well-identified strengths
and limitations. While the findings of epidemiological studies have been given the greatest
weight in setting standards for airborne particles, studies on human volunteers (clinical studies)
can provide information on exposure–response relationships for short-term, transient effects in
healthy and potentially susceptible individuals. Studies of this design, involving both healthy
persons and adults with chronic diseases, have been carried out using exposure to
concentrated ambient particles (US EPA, 2009).
There is substantial new evidence from time series studies of daily mortality, particularly from
multi-city studies that span Europe and North America (US EPA, 2012, 2009; WHO, 2013) and
also Australia (NEPM, 2010). Several studies conducted in Australia also show adverse effects
of both PM10 and PM2.5 on mortality and morbidity outcomes (Simpson et al., 2005a, b; Barnett
et al., 2005) similar to those observed in overseas studies. The effects observed in the
Australian studies appear to be higher than those observed in the US and Europe but
comparable to the results of Canadian studies. The epidemiological evidence is supported by
an increasingly strong foundation of toxicological research. Various mechanisms have been
proposed by which particles may cause and/or exacerbate short-term and chronic diseases.
Inflammation due to the production of reactive oxygen species is emerging as a central
mechanism.
PM2.5
The health effects of PM2.5 have been extensively studied and reviewed in recent years (WHO,
2013; US EPA, 2012, 2009; NEPM 2010). There is a large database that supports a causal
association between exposure to PM2.5 and a range of both short-term and long-term mortality
and morbidity outcomes. In 2013, a large European cohort study investigated the association
of exposure to PM2.5 with cause-specific mortality in adults included in the Rome Longitudinal
Study. The authors found that long-term exposure to PM2.5 is linked to increases in accidental
mortality associated with ischaemic heart diseases, cardiovascular diseases and lung cancer
(Cesaroni et al., 2013).

SPECIALIST CONSULTANT STUDIES GLOUCESTER RESOURCES LIMITED
Part 2B: Health Risk Assessment Amended Rocky Hill Coal Project
Report No. 806/14
2B-31
Short-term Health Effects of PM2.5
In recent years, there has been a substantive increase in studies showing associations
between particles and cardiovascular effects. Epidemiological studies that examined the
association between PM10, PM2.5 and mortality have provided strong evidence for particle-
related cardiovascular effects. Multi-city studies have found consistent, positive associations
between short-term exposure to PM2.5 and cardiovascular mortality ranging from 0.47 to 0.85%
in study locations with mean1 24-hour average PM2.5 concentrations above 12.8μg/m3. These
associations were reported at short lags (0-1 days). Although examinations of potential
confounders of the PM2.5-cardiovascular mortality relationship are limited, the observed
associations are supported by PM10-mortality studies, which found that particle risk estimates
remained robust to the inclusion of co-pollutants in models. Although the overall effect
estimates reported in the multi-city studies are consistently positive, it should be noted that a
large degree of variability exists between cities when examining city-specific effect estimates
potentially due to differences between cities and regional differences in PM2.5 composition.
An evaluation of the epidemiological literature indicates consistent positive associations
between short-term exposure to PM2.5 and all-cause, cardiovascular- and respiratory-related
mortality. The evaluation of multi-city studies found that risk estimates for all-cause (non-
accidental) mortality ranged from 0.29% to 1.21% per 10μg/m3 increase in 24-hour average
PM2.5 at lags of 1 and 0–1 days. These consistent effects were observed in study locations with
mean 24-hour average PM2.5 concentrations as low as 13μg/m3. Cardiovascular-related
mortality risk estimates were found to be similar to those for all-cause mortality whereas, the
risk estimates for respiratory-related mortality were consistently larger: 1.01–2.2% using the
same lag periods and averaging indices (US EPA, 2009).
Examinations of potential confounders of the PM2.5-respiratory mortality relationship are
limited, however, the observed associations are supported by PM10-mortality studies, which
found that particle risk estimates remained robust to the inclusion of co-pollutants in models
(Ostro et al. 2006, Franklin et al., 2008).
A large body of evidence from studies of the effect of PM2.5 on hospital admissions and
emergency department visits for cardiovascular diseases has shown that associations with
PM2.5 are consistently positive, with the majority of studies reporting increases in hospital
admissions or emergency department visits ranging from a 0.5% to 3.4% per 10μg/m3 increase
in PM2.5 (Bell et al., 2008, Dominici et al., 2006). The results of these studies provide support
for associations between short-term PM2.5 exposure and increased risk of cardiovascular
hospital admissions in areas with mean concentrations ranging from 7 to 18μg/m3.
A number of studies have found consistent associations between PM2.5 and hospital
admissions and emergency department visits for respiratory disease, with effect estimates in
the range of ~1% to 4% per 10μg/m3 increase in PM2.5. These associations have been
observed in areas with mean 24-hour PM2.5 concentrations between 6.1 and 22μg/m3. Further
studies have focused on increasingly specific disease endpoints such as asthma, Chronic
Obstructive Pulmonary Disease (COPD) and respiratory infection. The strongest evidence of
an association comes from large multicity studies of COPD, respiratory tract infection and all
respiratory diseases among Medicare recipients (65+ years old) (Dominici et al., 2006; Bell et
al., 2008). Studies of children have also found evidence of an effect of PM2.5 on hospital
admissions for all respiratory diseases, including asthma and respiratory infection (Peel et al.,
2005)
1 In this context, mean represents the arithmetic mean of 24-h average PM concentrations.

GLOUCESTER RESOURCES LIMITED SPECIALIST CONSULTANT STUDIES
Amended Rocky Hill Coal Project Part 2B: Health Risk Assessment
Report No. 806/14
2B-32
Controlled human exposure studies in adults demonstrating increased markers of pulmonary
inflammation following diesel exhaust and other traffic-related exposures, oxidative responses
to diesel exhaust and wood smoke, and exacerbations of allergic responses and allergic
sensitization following exposure to diesel exhaust particles add further support for these effects
(US EPA, 2009). Some controlled human exposure studies have reported small decrements in
various measures of pulmonary function following controlled exposures to PM2.5. Numerous
toxicological studies demonstrating a wide range of responses provide biological plausibility for
the associations between PM2.5 and respiratory morbidity observed in epidemiological studies.
Altered pulmonary function, mild pulmonary inflammation and injury, oxidative responses,
airway hyper responsiveness in allergic and non-allergic animals, exacerbations of allergic
responses and increased susceptibility to infections were observed in a large number of
studies involving exposure to concentrated ambient particles, diesel exhaust, other traffic-
related particles and wood smoke. The numerous and wide range of respiratory responses
observed in both the human clinical and toxicological studies provide biological plausibility for
an association between short-term exposure to PM2.5 and respiratory morbidity. The US EPA,
(2009) concluded that the consistent and coherent results found in the epidemiological, human
clinical, and toxicological literature provide sufficient evidence that a causal relationship is
likely to exist between short-term exposures to ambient concentrations of PM2.5 and respiratory
morbidity.
Epidemiological studies of asthmatic children have found increases in respiratory symptoms
and asthma medication use associated with higher PM2.5 or PM10 concentrations. Associations
with respiratory symptoms and medication use are less consistent among asthmatic adults,
and there is no evidence to suggest an association between respiratory symptoms with PM2.5
among healthy individuals (US EPA, 2009). In addition, respiratory symptoms have not been
reported following controlled exposures to PM2.5 among healthy or health-compromised adults.
Several new controlled human exposure studies report traffic or diesel-induced increases in
markers of inflammation in airway lavage fluid (fluid used to rinse the airways) from healthy
adults. There is also additional evidence in support of a pulmonary oxidative response to diesel
exhaust in humans. Preliminary findings indicate little to no pulmonary injury in humans
following controlled exposures to fine urban traffic particles or diesel exhaust, in contrast to a
number of toxicological studies demonstrating injury with concentrated ambient particles or
diesel exhaust.
Long-term Health Effects of PM2.5
The earlier studies on the long-term effects of PM2.5 on mortality – the Six Cities Study
(Dockery et al., 1993) and the American Cancer Society (ACS) study (Pope et al., 2002) –
have been pivotal in the development of air quality standards and guidelines worldwide. These
studies have been updated several times with systemic increases in the number of years of
analysis and deaths that were followed in these cohorts and in the statistical approaches used
in the analysis (Laden et al., 2006; Krewski et al., 2009). These reanalyses continue to find a
consistent, statistically significant association between long-term exposure to PM2.5 and the risk
of mortality. The magnitude of the effects estimate (the mortality effect per unit of exposure)
remains consistent with that of the original study (WHO, 2013). Using the 51 cities from the
ACS study, Pope et al., (2009) reported that reductions in PM2.5 across the metropolitan
regions between 1980 and 2000 were strongly associated with increases in life expectancy
after correcting for other risk factors.

SPECIALIST CONSULTANT STUDIES GLOUCESTER RESOURCES LIMITED
Part 2B: Health Risk Assessment Amended Rocky Hill Coal Project
Report No. 806/14
2B-33
A large number of new prospective cohort studies from Asia, Canada, Europe and the US
have been reported since 2005 (summarised in WHO, 2013). These studies provide additional
evidence of the effects of long-term exposure to PM2.5 on mortality. These effects have been
observed at lower concentrations than previously studied and there is still no evidence of a
threshold below which adverse effects do not occur. These studies have been undertaken in
areas that cover a variety of environmental settings, PM mixtures, baseline health conditions,
socioeconomic settings and personal characteristics. Given the consistency in the findings of
these studies, WHO (2013) and US EPA (2012; 2009) have determined that it is appropriate to
extrapolate the findings of these studies to other regions. The risk of ischemic heart disease
has particularly strong associations with PM2.5.
Hoek et al (2013) conducted a systematic review of the literature on the long-term effects of air
pollution on all cause, cardiovascular and respiratory mortality. Where more than 5 studies
were identified, a meta-analysis was conducted to obtain an overall effects estimate for each
outcome. The authors identified a number of cohort studies conducted in various parts of the
world that found associations between PM2.5 and PM10 and all cause, cardiovascular and
respiratory mortality. The effects estimates identified per 10μg/m3 increase in annual average
PM2.5 were 6% all cause, 11% cardiovascular and 3% respiratory mortality. For PM10, a 3.5%
increase in all-cause mortality per 10μg/m3 increase in annual average PM10 was found. There
was significant heterogeneity in the effects estimates from individual studies which was
thought to be due to differences in particle composition, indoor exposures as well as
population and baseline health status of the exposed populations.
Recent studies have also shown the effects of long-term exposure to PM2.5 on diseases other
than cardiovascular and respiratory diseases (WHO, 2013). Evidence suggests effects on
diabetes, neurological development in children and neurological disorders in adults (Ruckerl et
al., 2011). Epidemiological studies in Germany (Kramer et al., 2010) and Denmark (Anderson
et al., 2012; Raaschou-Nielsen et al., 2013) have all found strong associations between
exposure to PM2.5 and diabetes. These findings have been supported by mechanistic studies
(WHO, 2013).
The effects of PM2.5 on birth outcomes have been studied in a number of cohort studies
(Brauer et al., 2007; Gehring et al., 2010; MacIntyre et al., 2011; Morgenstern et al., 2007).
Evidence is accumulating for PM2.5 effects on low birth weight and infant mortality, especially
due to respiratory causes during the post-neonatal period. The mean PM2.5 concentrations
during the study periods ranged from 5.3 to 27.4μg/m3 with effects becoming more precise and
consistently positive in locations with mean PM2.5 concentrations of 15μg/m3 and above (US
EPA, 2009). Exposure to PM2.5 was usually associated with greater reductions in birth weight
than exposure to PM10. The evidence from a few studies that investigated PM10 effects on
foetal growth, which reported similar decrements in birthweight, provide consistency for the
PM2.5 associations observed and strengthen the interpretation that particle exposure may be
causally related to reductions in birth weight.
In summary, the potential health effects of PM2.5 are as follows:
Short-term:
1. Cardiovascular and respiratory mortality,
2. All cause cardiovascular effects e.g. Ischaemic heart diseases and respiratory
effects e.g. Asthma,
3. Hospital admissions and emergency department visits due to cardiovascular and
respiratory disease

GLOUCESTER RESOURCES LIMITED SPECIALIST CONSULTANT STUDIES
Amended Rocky Hill Coal Project Part 2B: Health Risk Assessment
Report No. 806/14
2B-34
Long-term
1. Accidental mortality associated with ischaemic heart diseases, cardiovascular
diseases and lung cancer
2. Other disease including diabetes, neurological development in children and
neurological disorders in adults
3. Birth outcomes including low birth weight and infant mortality
4. All cause, cardiovascular and respiratory mortality
PM10
Short-term Health Effects of PM10
Most of the evidence of an association between short-term exposure to particles and adverse
health outcomes comes from time-series epidemiological studies looking at daily increases in
mortality and hospital admissions and emergency room attendances linked to ambient particle
concentrations. In addition, the results of panel studies and controlled exposure studies add
further evidence for the association between short-term exposure to particles and adverse
health effects. The results of recent reviews and studies relevant to PM10 are summarised
below.
Mortality
The epidemiological literature indicates consistent positive associations between short-term
exposure to PM10 and all-cause mortality. The results of multicity studies report an approximate
0.12% to 0.81% increase in all-cause mortality per 10μg/m3 increase in PM10 with 24-hour
average PM10 concentrations ranging from 13 to 53.2μg/m3. Consistent positive associations
have also been found between PM10 and respiratory and cardiovascular-related mortality.
Studies conducted in Australia have found similar results with a 0.2% (-0.8% to 1.2%) increase
in all-cause mortality per 10μg/m3 increase in 24-hour average PM10 (Simpson et al., 2005a).
Morbidity
The majority of recent evidence for an association between short-term exposure to PM10 and
cardiovascular health effects is derived from epidemiological studies of hospital admissions
and emergency department visits. Although some regional heterogeneity is evident in the
single-city effect estimates, consistent increases in hospital admissions and emergency
department visits for cardiovascular diseases, have been observed across studies, with the
majority of estimates ranging from 0.5% to 1.0% per 10μg/m3 increase in PM10 (WHO, 2013). A
detailed examination of specific cardiovascular health outcomes has suggested that ischemic
heart disease and chronic heart failure are responsible for the majority of particle-related
cardiovascular disease hospital admissions, however, one large multicity study provides
evidence of an association between PM10 and ischemic stroke (US EPA, 2009). Overall, the
literature provides consistent evidence for associations between short-term exposure to PM10
and increased risk of cardiovascular hospital admissions and emergency department visits in
cities with mean 24-hour average concentrations ranging from 16.8 to 48μg/m3.
Epidemiological studies that examined the association between short-term exposure to PM10
and respiratory morbidity found consistent positive effects in asthmatic children and adults, but
no evidence of an association in healthy individuals in both Australian and overseas studies.
The majority of the studies that examined the association between PM10 and respiratory

SPECIALIST CONSULTANT STUDIES GLOUCESTER RESOURCES LIMITED
Part 2B: Health Risk Assessment Amended Rocky Hill Coal Project
Report No. 806/14
2B-35
symptoms and medication use found an increased risk ranging from ~1.0 to 1.75 for cough,
phlegm, difficulty breathing, and bronchodilator use in asthmatic children in cities with mean
24-hour average concentrations ranging from 16.8 to 64.5μg/m3. Positive, but less consistent
effects for respiratory symptoms and medication use were observed in asthmatic adults. An
evaluation of respiratory emergency department visits and hospital admission studies found
consistent positive associations at ambient PM10 concentrations ranging from 13.3 to
60.8μg/m3 among asthmatic children (~ 2% increase) and older adults with chronic obstructive
pulmonary disease (COPD) (~ 0 to 3% increase). Although no toxicological or human clinical
studies have examined the effect of short-term exposure to PM10 on respiratory morbidity, the
consistent epidemiological evidence alone was sufficient for the US EPA (2009) to conclude
that a causal relationship is likely to exist between short-term exposure to ambient
concentrations of PM10 and respiratory morbidity.
Long-term Health Effects of PM10
Most studies investigating the effects of long-term exposure to air pollution have focussed on
PM2.5. However there are some that have investigated the effects of PM10.
Mortality
Chen et al 2005 reported a positive association between PM2.5-10 and PM10 exposure and
coronary heart disease mortality which has been found to be more prevalent in females than
males. In addition, Gehring et al., 2006 has found that there is an association between
cardiopulmonary mortality and PM10 exposure.
Morbidity
Children may be at greater risk from long-term exposures to particles or other air pollutants
because the growth and development of the respiratory system may be permanently affected
by early environmental insults. Several studies have examined this and overall the evidence of
particle effects of morbidity in relation to long-term exposures is not as consistent as for
mortality. Overall, there is evidence of a particle-related effect on chronic morbidity, as
measured by chronic respiratory symptoms and lung function. However, it is not possible,
based on current evidence, to identify which size fractions or specific constituents are likely to
be most influential (US EPA, 2009; OEHHA, 2001).
In summary, the health effects of PM10 are as follows:
Short-term:
1. All-cause mortality,
2. Respiratory morbidity in asthmatics,
3. Hospital admissions and emergency department visits due to cardiovascular
health effects such as ischemic heart disease and chronic heart failure.
Long-term:
1. Respiratory morbidity, and
2. Coronary heart disease and cardiopulmonary mortality.

GLOUCESTER RESOURCES LIMITED SPECIALIST CONSULTANT STUDIES
Amended Rocky Hill Coal Project Part 2B: Health Risk Assessment
Report No. 806/14
2B-36
5.2.1.4 Health effects and Concentration-response Relationships
Studies have demonstrated that for a wide range of PM concentrations, including
concentrations below current assessment criteria, there are measurable associations between
incremental increases in particle concentration and adverse health effects. That is, no
threshold has been identified for particles and any increase in concentration may affect health.
As such, it can be deduced that ambient guidelines do not lead to complete protection against
adverse health effects of PM.
However, the results of epidemiological studies can be used to make quantitative estimates
concerning the health effects of air pollution on a population. A Concentration Response
Function (CRF) (reported by epidemiological studies) is the empirically estimated relationship
between the concentration of PM and the observed health endpoints of interest (for example,
hospital admissions for asthma) in a population. There is a dose-response relationship with PM
and many health outcomes where the health risk increases with exposure to both PM10 and
PM2.5.
Epidemiological studies estimating health outcomes in the population are often not available
for a particular location, or the available results from local studies may not be considered as
robust as the combined results of epidemiological studies from other locations/populations.
Because the uncertainty in the precision of the risk estimate from an epidemiological study
decreases with increasing sample size (for example, the population in the study), combining
results from several studies may yield more robust estimates of effect (e.g., meta-analysis). At
present, Australian studies, in particular studies involving mining and extractive industries, are
currently considered insufficient to reliably establish specific Australian concentration-response
relationships for relevant health outcomes and PM exposures. Therefore, overseas data has
been used to quantify health effects in this health risk assessment. Additionally, in line with
WHO advice, all particles should be treated as equally harmful irrespective of source and
chemical composition.
In order to generate sufficient data to adequately characterise the concentration-response
relationship for compounds present in air, meta-analytic point estimates rather than estimates
from one single study can enhance the value of the available information and deal with
potential heterogeneity between studies. As a result, cities with large populations provide the
best data upon which to study and characterise the concentration-response relationship for
compounds present in air. Similarly, multi-city studies can also produce even more reliable
effect estimates as the sample size is much larger than those in single city studies. While, the
results are based on compounds and exposures typical to an urban setting and not those of a
rural, mine-based setting, they nevertheless provide the best information upon which to
characterise the concentration-response.
Over the last few decades, there has been a substantial amount of research that has added to
the evidence that breathing PM is harmful to human health. Various lines of research have
helped connect some of the important gaps in our knowledge. Different studies using
alternative time series approaches and case crossover designs continue to observe
reasonably consistent associations between morbidity and mortality outcomes and daily
changes in PM. The associations are observed, not only in many single-city studies, but also in
various large multicity studies (Pope and Dockery, 2006). The evidence of long-term health
effects has been strengthened by various reanalyses and extended analyses of the Harvard
Six Cities study (Dockery et al. 1993), ACS cohorts (Pope et al. 1995) and by results from
several other independent studies of long-term PM exposure.

SPECIALIST CONSULTANT STUDIES GLOUCESTER RESOURCES LIMITED
Part 2B: Health Risk Assessment Amended Rocky Hill Coal Project
Report No. 806/14
2B-37
The PM-mortality effect estimates from the studies of long-term exposure are substantially
larger than those from the short-term time series or case-crossover studies that evaluate daily
changes in exposure. Overall, the results suggest that PM health effects are dependent on
both exposure concentrations and length of exposure and that the short-term studies only
capture a small amount of the overall health effects of PM exposure. Long-term repeated
exposures have larger, more persistent cumulative effects than short-term transient exposures.
It is important to note that the observed association between PM and health outcomes is
statistical. As such, particles are not the primary cause of the observed increase in mortality,
but are one of many environmental and other risk factors. The statistical associations have
been revised downwards based on a review of the statistical methods used, but the
association remains (HEI, 2003).
The specific health effects (or endpoints) evaluated in this assessment are outlined below:
1. Annual mortality all cause 30+ years
2. Cardiopulmonary mortality 30+ years
3. Ischaemic Heart Disease 30+ years
4. Lung Cancer mortality 30+ years
5. Daily mortality all causes all ages
6. Daily mortality cardiovascular disease all ages
7. Hospital admissions respiratory disease 65+
8. Hospital admissions cardiac disease 65+
9. Hospital admissions pneumonia and bronchitis 65+
10. Hospital admissions cardiovascular disease 65+ years
11. Hospital admissions respiratory disease 15-64 years
12. Emergency department visits (asthma) 1-14 years
The CRFs chosen for this risk assessment were taken from the review conducted by Jalaludin
and Cowie 2012, who recommended CRFs to be used for HRAs in the Australian context.
Jalaludin and Cowie 2012 presented functional forms of the CRFs as reported in
epidemiological studies (relative risks, odds ratios, percentage incidence/ prevalence). It was
therefore necessary to convert these into standardised estimates i.e. beta (β) coefficients, for
the purpose of risk characterisation using the following equation:
Table 5.2 and Table 5.3 present a summary of the health endpoints, concentration response
functions used and associated β coefficient relevant to the relative risk calculation.

GLOUCESTER RESOURCES LIMITED SPECIALIST CONSULTANT STUDIES
Amended Rocky Hill Coal Project Part 2B: Health Risk Assessment
Report No. 806/14
2B-38
Table 5.2
Concentration-Response Functions for PM2.5 based on Jalaludin and Cowie (2012)
Health Endpoint CRF Adopted β coefficient for
1µg/m3 increase in PM
Reference
Annual mortality all cause 30+ years 6% (4-8%) per 10 μg/m3 5.82e-3
(Krewski, Jerrett et al. 2009) (US EPA 2010)
Cardiopulmonary mortality 30+ years 14% (11-17%) per 10 μg/m3 1.31e-2
(Krewski, Jerrett et al. 2009) (US EPA 2010)
Ischaemic Heart Disease 30+ years 24% (19-28%) per 10 μg/m3 2.15e-2
(Krewski, Jerrett et al. 2009) (US EPA 2010)
Lung Cancer mortality 30+ years 14% (6-12.3%) per 10 μg/m3 1.31e-2
(Krewski, Jerrett et al. 2009) (US EPA 2010)
Daily mortality all causes all ages 0.9% (0.2-1.6%) per 3.78 μg/m3
2.37e-3 (EPHC 2005)
Daily mortality cardiovascular disease all ages 1.5% (0.7-2.3%) per 3.78 μg/m3 3.94e-3 (EPHC 2005)
Hospital admissions respiratory disease 65+ 1.6% (0.9-2.3%) increase per 3.78 μg/m3 4.20e-3 (EPHC 2005)
Hospital admissions cardiac disease 65+ 1.9% (1.0-2.7%) increase per 3.78 μg/m3 4.97e-3 (EPHC 2005)
Hospital admissions pneumonia and bronchitis 65+ 2.0% (0.8-3.2%) per 3.78 μg/m3 5.24e-3 (EPHC 2005)
Hospital admissions cardiovascular disease 65+ years 1.3% (0.6-2.0) increase per 3.78 μg/m3 3.42e-3 (EPHC 2005)
Hospital admissions respiratory disease 15-64 years 1.1% (0.0-2.1%) increase per 3.78 μg/m3 2.89e-3 (EPHC 2005)
Emergency department visits (asthma) 1-14 years 1.4% (0.9-1.8%) increase per 9.4 μg/m3 1.48e-3 (Jalaludin, Khalaj et al. 2008)

SPECIALIST CONSULTANT STUDIES GLOUCESTER RESOURCES LIMITED
Part 2B: Health Risk Assessment Amended Rocky Hill Coal Project
Report No. 806/14
2B-39
Table 5.3
Concentration-Response Functions for PM10 based on Jalaludin and Cowie (2012)
Health Endpoint CRF Adopted β coefficient for 1µg/m
3 increase in PM
Reference
Annual mortality all cause 30+ years 0.386% (0.295-0.477%) per 1 μg/m3 3.85e-3 (Pope, Thun et al. 1995)
Daily mortality cardiovascular disease all ages 1.3% (0.4-2.3%) per 10 μg/m3 1.29e-3 (Morgan, Sheppeard et al. 2010)
#
Hospital admissions respiratory disease 65+ 1.8% (0.6-3.0%) per 7.53 μg/m3 2.37e-3 (EPHC 2005)
Hospital admissions cardiac disease 65+ 1.04% (0.02- 2.07%) per 10 μg/m
3
(all ages = larger CRF) 1.035e-3 (Morgan, Sheppeard et al. 2010)
#
Hospital admissions pneumonia and bronchitis 65+ 1.4% (0.5-2.2%) per 7.53 μg/m3 1.85e-3 (EPHC 2005)
Hospital admissions respiratory disease 15-64 years 1.22% (0.41 to 2.03%) per 10 μg/m
3
(all ages = larger CRF) 1.21e-3 (Morgan, Sheppeard et al. 2010)
#
Emergency department visits (asthma) 1-14 years 1.04% (0.02- 2.07%) per 10 μg/m
3
(all ages = larger CRF) 1.035e-3 (Morgan, Sheppeard et al. 2010)
#
Annual mortality all cause 30+ years 0.386% (0.295-0.477%) per 1 μg/m3 3.85e-3 (Pope, Thun et al. 1995)
# In instances where there was no effect reported in Australian 4-cities meta-analysis (Environment Protection and Heritage Council 2005), the CRF recommendation for a sensitivity analysis was
used i.e. (Morgan, Sheppeard et al. 2010).

GLOUCESTER RESOURCES LIMITED SPECIALIST CONSULTANT STUDIES
Amended Rocky Hill Coal Project Part 2B: Health Risk Assessment
Report No. 806/14
2B-40
5.2.2 Exposure Assessment
The exposure assessment outlined below estimates the total cumulative exposure
(i.e. background plus modelled PM10 and PM2.5 increment from the amended Project) on an
annual and daily basis at the most affected private receivers/residences (receiver 6 in
Gloucester and receiver 18 in Forbesdale) on the worst day of each modelled year. By using
the modelled predictions at the most affected private receivers/residences to represent
exposure across the populations of the respective state suburbs, the overall community
exposure is over estimated and the resulting HRA would be considered conservative.
The air quality impact assessment for the amended Project (Pacific Environment, 2016)
presents the dispersion modelling predictions for maximum 24-hour and annual average PM2.5
and PM10 GLCs at a total of 160 non-resource related assessment locations. For both PM2.5
and PM10, the full dataset based on the 160 assessment locations in conjunction with
background were examined as part of the HRA.
An assessment of cumulative 24-hour average PM2.5 and PM10 impacts was conducted at the
five most impacted private receivers/residences i.e. receiver 6, 18, 19A and 23 and 36, via the
frequency distribution. For PM2.5, there were no predicted exceedances of 25µg/m3 as a result
of the amended Project-only however there was an increased probability at receiver 6, 18, 23
and 36 that cumulative 24-hour PM2.5 concentrations would result in two additional days of
average 24-hour PM2.5 concentrations over the Australian air quality criterion of 25µg/m3.
Similarly the PM10 assessment found no predicted exceedances of 50µg/m3 as a result of the
amended Project-only however there was an increased probability at receiver 6, 18 and 23 that
cumulative 24-hour PM10 concentrations would result in less than one additional day of
average 24-hour PM10 concentrations over the Australian air quality criterion of 50µg/m3.
Table 5.4 and Table 5.5 outline the modelled 24 hour project-only contributions of the
amended Project and annual average and cumulative concentrations (the background plus the
amended Project increment) respectively. These values were used in the risk calculations to
estimate the potential increase in base incidence due to attributable PM2.5 and PM10
concentrations.
Table 5.4
Maximum Predicted Project-only 24-hour Average Concentrations at the Most Affected
Receiver/residence (g/m3)
Gloucester State Suburb (Receiver 6)
Faulkland State Suburb (Forbesdale Estate) (Receiver 18)
PM2.5 PM10 PM2.5 PM10
Year 1 0.75 3.39 1.32 5.42
Year 4 3.58 19.70 2.75 16.60
Year 7 6.32 35.35 3.98 24.30
Year 10 3.48 21.03 4.60 24.91
Source: Pacific Environment (2016) – Tables 9.5 and 9.6.

SPECIALIST CONSULTANT STUDIES GLOUCESTER RESOURCES LIMITED
Part 2B: Health Risk Assessment Amended Rocky Hill Coal Project
Report No. 806/14
2B-41
Table 5.5
Predicted Annual Average Concentrations at the Most Affected Receiver/Residence (g/m3)
Gloucester State Suburb (Receiver 6)
Forbesdale State Suburb (Receiver 18)
PM2.5 PM10 PM2.5 PM10
Project-only
Year 1 0.05 0.26 0.17 0.79
Year 4 0.26 1.40 0.52 3.39
Year 7 0.42 2.29 0.75 4.94
Year 10 0.19 1.05 0.83 4.95
Cumulative
Year 1 4.70 9.44 4.95 10.6
Year 4 4.90 10.6 5.28 13.3
Year 7 5.06 11.5 5.51 14.8
Year 10 4.82 10.2 5.55 14.5
Source: Pacific Environment (2016) – Tables 9.2 and 9.3.
5.2.3 Risk Characterisation
The NEPM AAQM considers an additional risk of ‘1 per 100,000’ for adverse health outcomes
to be sufficiently small and to be of no cause for concern. The recent enHealth update on
environmental risk assessment has not prescribed a target risk level. Rather, it has noted that
any target risk level does not:
“… imply certainty that one person will get the disease if there are at least one
million people exposed. It is simply a way of expressing risk, as a numerical
expression of the likelihood of an event occurring under the defined conditions of
exposure, based on extrapolation of dose–response data.”
As such, it is important to note that the risk values provided based on the CRFs for PM
represent only probabilities, and not defined health outcomes.
5.2.3.1 Baseline Health Statistics
Baseline health incidence data was not available for the local areas i.e. Gloucester and
Faulkland State Suburbs, however, data was available for Tamworth, Newcastle and Sydney.
The data from Tamworth has been used in the calculations given that the local environment of
Tamworth is more similar to the local area under assessment, than Newcastle and Sydney.
Table 5.6 summarises the baseline health statistics used in the risk calculations.

GLOUCESTER RESOURCES LIMITED SPECIALIST CONSULTANT STUDIES
Amended Rocky Hill Coal Project Part 2B: Health Risk Assessment
Report No. 806/14
2B-42
Table 5.6
Baseline Health Incidence Rate per 100,000 used in Risk Calculations
Health Endpoint
Baseline Health Incidence Rate per 100,000
(Tamworth) - 2010
MORTALITY
All causes 30+ years 353
All cause (non-trauma) 30+ years 27
Cardiopulmonary disease 30+ years 164
Ischaemic Heart Disease 30+ years 66
Lung Cancer mortality 30+ years 16
All cause all ages -
All cause (non-trauma) all ages 350
Cardiovascular all ages 136
HOSPITAL ADMISSIONS
Respiratory disease 65+ years 297
Cardiac disease 65+ years 542
Pneumonia and bronchitis 65+ years 96
Cardiovascular disease 65+ years 747
Respiratory disease 15-64 years 299
Emergency department visits (asthma) 258
5.2.3.2 Risk Calculations
The general approach used to calculate the risks to health has drawn upon internationally
recognised estimates of the impact of PM on health in relation to the known health indicators
for NSW. It involves estimating the change in the incidence of a health outcome resulting from
a given change in PM concentrations. The CRFs provide an estimate of the relationship
between the health endpoint of interest and PM concentrations. The baseline health effect
incidence rate provides the number of cases of the health effect per year, usually per 100,000
of the general population.
The risk factors in Table 5.2 and Table 5.3 have been used to estimate the risks associated
with exposure to the particulate emissions both from the amended Project alone and
cumulatively. Baseline Health incidence statistics were obtained from the NSW Health website
(http://www.healthstats.nsw.gov.au).
The equation used to calculate the number of cases attributable to exposure to a contaminant
per 100,000 is as follows:

SPECIALIST CONSULTANT STUDIES GLOUCESTER RESOURCES LIMITED
Part 2B: Health Risk Assessment Amended Rocky Hill Coal Project
Report No. 806/14
2B-43
For example Year 7, PM2.5 cumulative modelled output for Gloucester
The number of attributable cases based on annual mortality rates for all causes (30+ years)
was calculated as follows:
= 0.210
Where:
Adopted β coefficient for 1µg/m3 increase in PM = 0.00582 (Table 5.2)
PM2.5 cumulative modelled output = 5.06 g/m3 (Table 5.5)
Baseline incidence rate per 100,000 = 353 (Table 5.6)
Population of Gloucester aged 30+ = 2017 (Table 3.1)
The resultant increase in base incidence for annual mortality all causes 30+ years was
calculated as follows:
= 0.05%
Where:
Number of attributable cases = 0.210 (Table 5.7)
Baseline incidence rate per 100,000 = 353 (Table 5.6)
Table 5.7 to Table 5.10 show the predicted number of attributable health effects for PM2.5 and
PM10 arising from the amended Project for each of these communities.
The average PM2.5 and PM10 concentrations that were used for both Gloucester and
Forbesdale in the calculations are shown in Table 5.4 and Table 5.5. These were the
maximum concentrations predicted within the state suburbs for each year assessed. These
were extrapolated across the whole community to take a conservative approach. For the
assessment of long-term mortality, the annual average concentrations were used in the
calculations. For the short-term effects, the predicted 24-hour average concentrations for the
same locations were used and extrapolated across the relevant populations. These values
were used to calculate the daily mortality health endpoints.

GLOUCESTER RESOURCES LIMITED SPECIALIST CONSULTANT STUDIES
Amended Rocky Hill Coal Project Part 2B: Health Risk Assessment
Report No. 806/14
2B-44
Table 5.7
Predicted Number of Attributable Cases Due to PM2.5 Exposure per 100,000: Gloucester State Suburb
Health Endpoint
Gloucester
Y1 Y4 Y7 Y10
Annual mortality all cause 30+ years 0.20 0.20 0.21 0.20
Cardiopulmonary mortality 30+ years 0.21 0.21 0.22 0.21
Ischaemic Heart Disease 30+ years 0.14 0.14 0.15 0.14
Lung Cancer mortality 30+ years 0.02 0.02 0.02 0.02
Daily mortality all causes all ages 0.00 0.00 0.00 0.00
Daily mortality cardiovascular disease all ages 0.00 0.00 0.00 0.00
Hospital admissions respiratory disease 65+ years 0.05 0.05 0.05 0.05
Hospital admissions cardiac disease 65+ years 0.10 0.11 0.11 0.11
Hospital admissions pneumonia and bronchitis 65+ years 0.02 0.02 0.02 0.02
Hospital admissions cardiovascular disease 65+ years 0.01 0.10 0.10 0.10
Hospital admissions respiratory disease 15-64 years 0.07 0.07 0.07 0.07
Emergency department visits (asthma) 1-14 years 0.01 0.01 0.01 0.01
Table 5.8
Predicted Number of Attributable Cases Due to PM10 Exposure per 100,000: Gloucester State Suburb
Health Endpoint
Gloucester
Y1 Y4 Y7 Y10
Annual mortality all cause 30+ years 0.26 0.29 0.31 0.29
Daily mortality all causes all ages 0.00 0.00 0.00 0.00
Daily mortality cardiovascular disease all ages 0.00 0.00 0.00 0.00
Hospital admissions respiratory disease 65+ years 0.02 0.03 0.03 0.03
Hospital admissions cardiac disease 65+ years 0.08 0.09 0.09 0.09
Hospital admissions pneumonia and bronchitis 65+ years 0.01 0.01 0.01 0.01
Hospital admissions respiratory disease 15-64 years 0.06 0.06 0.07 0.06
Emergency department visits (asthma) 1-14 years 0.01 0.01 0.01 0.01

SPECIALIST CONSULTANT STUDIES GLOUCESTER RESOURCES LIMITED
Part 2B: Health Risk Assessment Amended Rocky Hill Coal Project
Report No. 806/14
2B-45
Table 5.9
Predicted Number of Attributable Cases Due to PM2.5 Exposure per 100,000: Faulkland State Suburb (Forbesdale Estate)
Health Endpoint
Faulkland State Suburb (Forbesdale Estate)
Y1 Y4 Y7 Y10
Annual mortality all cause 30+ years 0.02 0.02 0.02 0.02
Cardiopulmonary mortality 30+ years 0.02 0.02 0.02 0.02
Ischaemic Heart Disease 30+ years 0.01 0.01 0.01 0.01
Lung Cancer mortality 30+ years 0.00 0.00 0.00 0.00
Daily mortality all causes all ages 0.00 0.00 0.00 0.00
Daily mortality cardiovascular disease all ages 0.00 0.00 0.00 0.00
Hospital admissions respiratory disease 65+ years 0.00 0.00 0.00 0.00
Hospital admissions cardiac disease 65+ years 0.01 0.01 0.01 0.01
Hospital admissions pneumonia and bronchitis 65+ years 0.00 0.00 0.00 0.00
Hospital admissions cardiovascular disease 65+ years 0.01 0.01 0.01 0.01
Hospital admissions respiratory disease 15-64 years 0.01 0.01 0.01 0.01
Emergency department visits (asthma) 1-14 years 0.00 0.00 0.00 0.00
Table 5.10
Predicted Number of Attributable Cases Due to PM10 Exposure per 100,000: Faulkland State Suburb (Forbesdale Estate)
Health Endpoint
Faulkland State Suburb (Forbesdale Estate)
Y1 Y4 Y7 Y10
Annual mortality all cause 30+ years 0.03 0.03 0.04 0.04
Daily mortality all causes all ages 0.00 0.00 0.00 0.023
Daily mortality cardiovascular disease all ages 0.00 0.00 0.00 0.00
Hospital admissions respiratory disease 65+ years 0.00 0.00 0.00 0.00
Hospital admissions cardiac disease 65+ years 0.01 0.01 0.01 0.01
Hospital admissions pneumonia and bronchitis 65+ years 0.00 0.00 0.00 0.00
Hospital admissions respiratory disease 15-64 years 0.01 0.01 0.01 0.01
Emergency department visits (asthma) 1-14 years 0.00 0.00 0.00 0.00
In examining the increased risk in the population (based on annual mortality rates, all causes)
due to the worst case annual average increased long-term exposure to PM2.5 and PM10 as a
result of the amended Project and cumulative exposure, it was noted that the resultant
increase in base incidence in Gloucester State Suburb and Faulkland State Suburb
(Forbesdale Estate) would be less than 1 in 100,000 therefore considered to be “sufficiently
small and to be of no cause for concern” (NEPM AAQM).
Shorter term exposures to PM2.5 and PM10 are also considered not to pose an unacceptable
risk as the predicted number of attributable cases due to daily mortality (all cause all ages and
cardiovascular disease all ages are less than 1 in orders of magnitude lower than that due to
long-term exposure.

GLOUCESTER RESOURCES LIMITED SPECIALIST CONSULTANT STUDIES
Amended Rocky Hill Coal Project Part 2B: Health Risk Assessment
Report No. 806/14
2B-46
5.2.4 Conclusion
The analysis provides estimates of the increase in annual and daily mortality due to cumulative
and project-only emissions from the amended Project at the private receivers/residences 6 and
18, i.e. the most affected private receivers/residences in each of the Gloucester and Faulkland
State Suburbs in each modelled year. In addition, estimates are provided on the increase in
daily hospital admissions that could be expected from the most exposed individual due to
maximum predicted impacts from the amended Project. In examining the increased risk in the
population (based on annual mortality rates, all causes) due to the increased long-term
exposure to PM2.5 and PM10 concentrations as a result of cumulative and project-only
exposure, it is noted that the number of attributable health outcomes would be well below 1 in
100,000 therefore considered to be “sufficiently small and to be of no cause for concern”
(NEPM AAQM).
In examining the four most impacted private receivers/residences via the frequency
distribution, it was noted that, based on the air modelling, the cumulative maximum 24 hour
average PM2.5 concentrations showed less than two additional days over the 25µg/m3 criterion
than would occur anyway due to background in the absence of the amended Project.
Cumulative 24 hour PM10 concentrations showed that there was an increased probability that
Residences 6 and 18 would experience less than one additional day of average 24 hour PM10
concentrations of the 50µg/m3 criterion than would occur anyway in the absence of the
amended Project.
Considering the context of these risk assessment results, it should be noted that the dispersion
modelling results are estimates only and the predicted annual average concentration for PM2.5
and PM10 represent a very low concentration and are subject to significant conservatism. It is
also important to note that PM2.5 and PM10 exposure alone does not result in mortality, but is
one of many factors that can combine to contribute to a premature mortality in susceptible
populations (e.g., elderly, persons with breathing problems – COPD, etc.).
Shorter term exposures to PM2.5 and PM10 are also considered not to pose an unacceptable
risk as the predicted number of attributable cases due to daily mortality (all cause all ages and
cardiovascular disease all ages are less than 1 in orders of magnitude lower than that due to
long-term exposure.
Based on the above discussion, it is considered unlikely that an unacceptable risk due to PM
exposure would result from the amended Project.
5.3 ASSESSMENT OF NITROGEN DIOXIDE
5.3.1 Hazard Assesment
Blasting activities and fuel combustion (i.e. motor vehicles and industry) within the Site have
the potential to result in emissions of oxides of nitrogen (NOX). NOX comprises both nitric oxide
(NO) and nitrogen dioxide (NO2).
In recent years, the health effects of NO2 linked to ambient exposures have been well studied
and reviewed by international agencies (US EPA, 2008; WHO, 2006; OEHHA 1999). The main
short-term health outcomes identified in epidemiology studies are increased respiratory

SPECIALIST CONSULTANT STUDIES GLOUCESTER RESOURCES LIMITED
Part 2B: Health Risk Assessment Amended Rocky Hill Coal Project
Report No. 806/14
2B-47
disease and symptoms. The evidence for the long-term effects of long-term exposure to NO2 is
limited. As with short-term exposure, the critical health outcomes with long-term exposure
include respiratory disease and associated symptoms, and associated changes in lung
function. Individuals with asthma and other chronic lung disease and cardiovascular diseases
are recognised as being particularly vulnerable. Other susceptible populations include infants,
children and the elderly (>65 years of age) (NEPM 2010).
Only very high concentrations of NO2 (approximately 2,000μg/m3 (~1,050 ppb)) affect
breathing in healthy people. However, small changes in lung function (< 5%) and changes in
airway responsiveness have been reported in several studies of sensitive asthmatics or the
elderly exposed to concentrations as low as 375-575μg/m3 (~200-300 ppb) over a period of 20
minutes to 4 hours (Bauer et al., 1986; Bylin et al., 1988; Roger et al., 1985; Morrow et al.,
1992; Strand et al., 1996, 1997, Streeton 1997). These levels represent a clear lowest-
observed-effect level (LOEL) for NO2 based on increased responsiveness in mild asthmatics to
bronchoconstrictors or in subjects with chronic obstructive pulmonary disease (COPD). It is
noted that the study by Bauer et al., (1986) did not find a significant change in pulmonary
function when asthmatics were exposed to 560μg/m3 NO2 when resting, with decreases
recorded only after the subjects exercised. Similarly, testing asthmatics the day after exposure
to 490μg/m3 NO2 did not decrease lung function before allergen challenge (Strand et al.,
1997), noting that the effects of NO2 exposure are transient in nature.
The identification of an obvious No Observed Adverse Effect Level (NOAEL) is less clear, but it
is suggested to be around 200μg/m3 (approximately 100 ppb). Studies have shown that effects
can be detected in mild asthmatics after short-term exposure (20 minutes to 4 hours in
duration) to 488-500μg/m3 (260-240 ppb) NO2 who are subsequently exposed to an inhalation
challenge (Strand et al., 1996, 1997; Kraft et al., 2005). However, in a study where mild
asthmatic subjects were exposed for 1hour to 200μg/m3 (~100 ppb) NO2 and then immediately
exposed to a house dust mite challenge, the late asthmatic response (as tested using Forced
Expiratory Volume in one second; FEV1) was found to be greater than when compared to air
(NO2 -7.76% vs. Air -2.85%), but the results were not found to be significant (Tunnicliffe et al.,
1994). The current air guideline for short-term exposure to NO2 in the NEPM is 246µg/m3 (0.12
ppm) measured as a 1hour average.
According to Streeton (1997), there is an increasing body of evidence to suggest that longer
term (years) ambient exposure to significantly lower concentrations of NO2, of the order of 40
to 80 ppb (approx. 75-150μg/m3) during early and middle childhood years can lead to the
development of recurrent upper and lower respiratory tract symptoms, such as recurrent
‘colds’, a productive cough, and an increased incidence of respiratory infection with resultant
absenteeism from school.
Similarly, more recent studies of self-reported asthmatic individuals living in homes with flue-
less gas heaters have shown significant effects of NO2 exposures to those aged ≤ 14 years,
with chest tightness, breathlessness on exertion and asthma attacks experienced either the
same day or with one-day lag (Smith et al., 2000). The range of median indoor levels of NO2
measured by positional passive samplers in homes during this study were indicated to be
between 0 to 147 ppb (0 to 277μg/m3) with time weighted average levels measured by
personal passive sampler of 0 to 1 760 ppb (0 to 3 300μg/m3). Subsequent investigations with
flue-less space heaters in primary schools indicated that over the 12 week winter heating
period, asthma symptoms were significantly higher in children exposed to gas combustion
products, with mean NO2 levels of 47.0 ppb (88μg/m3) versus children in schools where a
replacement intervention programme had removed or replaced the flue-less gas heaters,
leading to a mean NO2 level of 15.5 ppb (29.3μg/m3) (Pilotto et al., 2004).

GLOUCESTER RESOURCES LIMITED SPECIALIST CONSULTANT STUDIES
Amended Rocky Hill Coal Project Part 2B: Health Risk Assessment
Report No. 806/14
2B-48
Streeton 1997 also found that NO2 was demonstrated to potentiate the effects of exposure to
other known irritants such as ozone, sulfur dioxide and respirable particles (DoH 1993). NO2
interaction with respirable particles is relevant to this HRA, however, the understanding of this
interaction is limited.
Based upon a review of the literature, Streeton (1997) considered short-term ambient
exposures to 200 to 300 ppb (375 to 565μg/m3) NO2 and long-term exposures between 40 to
80 ppb (75 to 150μg/m3) capable of causing recurrent upper and lower respiratory tract
symptoms, an increased incidence of respiratory infection and onset of symptoms in mild
asthmatics. Streeton (1997) considered these effects as the Lowest Observed Adverse Effect
Levels (LOAEL), and has suggested that a safety factor of 50% of the LOAEL need apply to
account for susceptible people within the population, therefore establishing a short-term
exposure guideline in the range 100 to 150 ppb (188 to 282μg/m3) as a 1hour average and a
long-term exposure guideline between 20 to 40 ppb (37.6 to 75.2μg/m3) for longer term
exposures as an annual average.
The WHO (1997, 2000a) took a different approach to reach a similar conclusion. Similar to
Streeton (1997), the WHO noted the epidemiological studies suggesting human health effects
associated with long-term NO2 exposures. However, the WHO (1997) have stated that this is
supported by animal toxicological findings showing increased susceptibility to respiratory
infections and impairment of host defences as a result of sub chronic or chronic exposures to
NO2 concentrations near ambient concentrations (i.e. 20 to 60μg/m3; 11 to 32 ppb). On the
basis of a background level of 15μg/m3 (8 ppb) as determined in Finland during the 1980s
(Jaakkola et al., 1991) and the fact that significant adverse health effects occur with an
additional concentration of 28.2μg/m3 (15 ppb) or more, which is an estimate of an increased
risk of about 20% for respiratory symptoms and disease (Hasselblad et al., 1992; WHO, 1997),
an annual guideline value of 40μg/m3 (22 ppb) was derived by the WHO (1997). The WHO
considers the guideline value would be protective of most serious effects. The fact that a no-
effect level for sub chronic or chronic NO2 exposure concentrations has not yet been
determined was emphasised.
Since their publication, both the NEPM AAQM and the WHO air quality guidelines for particles,
ozone, nitrogen dioxide and sulfur dioxide have been subject to review (NEPM, 2010; WHO,
2006). In both instances, review of the guidelines considered newly available information from
various locations around the world, including Australia. The WHO concluded that the scientific
literature has not accumulated sufficient evidence to justify revising the existing NO2
guidelines. According to NEPM AAQM (2010), available epidemiological information indicates
increased hospital admissions and emergency department attendance for respiratory
symptoms, particularly in asthmatics and children, following short-term exposure to ambient
concentrations. However, the available information remains under consideration by the NEPM
AAQM and no changes to the standards have been made at this point in time (NEPM 2010).
In summary:
Concentrations of NO2 of around 2,000μg/m3 (~1,000 ppb) are needed to affect
respiration of healthy people based on short-term exposure (less than 24 hours).
The low effect level of NO2 for increased bronchial reactivity in sensitive
asthmatics is 375 to 575μg/m3 (~200 to 300 ppb) for exposures from 20 minutes
up to 4 hours.

SPECIALIST CONSULTANT STUDIES GLOUCESTER RESOURCES LIMITED
Part 2B: Health Risk Assessment Amended Rocky Hill Coal Project
Report No. 806/14
2B-49
The no effect level for increased bronchial reactivity based on short-term
exposure is ~376μg/m3.
The increased bronchial reactivity may remain for up to 10 hours after cessation
of NO2 exposure.
Table 5.11 presents a summary of guideline values established relating to short-term exposure
to NO2. For the estimation of risks, the NEPM (1998) AAQ has been used.
Table 5.11
Summary of National and International Criteria Established Relating to Short-term and Long-term Exposure to NO2
Guideline Averaging period
Derivation Reference µg / m
3 ppb
246 120 1 hour
The Australian National Environmental Protection Council ambient air quality standard. It is based on a LOAEL of 0.2 to 0.3 ppm derived from statistical reviews of epidemiological data suggesting an increased incidence of lower respiratory tract symptoms in children and aggravation of asthma. A safety factor of 0.5 to protect susceptible people (i.e. asthmatic children) was applied to the LOAEL.
NEPM (1998), Streeton (1997)
62 30 Annual
The Australian National Environmental Protection Council ambient air quality standard. It is based on a LOAEL of 0.04 to 0.08 ppm derived from statistical reviews of epidemiological data suggesting development of recurrent upper and lower respiratory tract symptoms and an increased incidence of respiratory infection with resultant absenteeism from school in children. A safety factor of 0.5 to protect susceptible people (i.e. asthmatic children) was applied to the LOAEL.
NEPM (1998), Streeton (1997)
The Australian NEPM AAQ criteria, which are protective of health outcomes in sensitive
subpopulations, are used to determine the potential for short-term effects (246µg/m3) and long-
term effects (62µg/m3) in association with exposure to NO2 from the amended Project.
5.3.2 Exposure Assessment
The cumulative air dispersion modelling conducted by Pacific Environment (2016) provided
probability estimates for the predicted concentrations of NO2 resulting from blasting, diesel
combustion and existing background levels at four selected private receivers/residences.
Concentrations of NO2 in the air from blasting and, to a lesser extent, diesel combustion, are
not constant: the concentrations are anticipated to vary according to the direction and strength
of the wind, time of day, and how far away a receiver/residence is from the blast and operating
equipment. Other factors known to contribute to blast fume generation include geology and
influence of controls in terms of explosive selection, quality, blast design and on bench
practices.

GLOUCESTER RESOURCES LIMITED SPECIALIST CONSULTANT STUDIES
Amended Rocky Hill Coal Project Part 2B: Health Risk Assessment
Report No. 806/14
2B-50
The mine plans for Year 4 and Year 7 were chosen for modelling of blasting as these years
represent the periods when blasting impacts are expected to be greatest (i.e. when pits are
largest and therefore closest to private receivers/residences). The modelling assumed a
possible 2190 hours per year when blasting could occur (6 hours a day, 365 days a year). In
reality, blasting would only occur to a maximum of four events per week and a maximum of
120 per year, when meteorological conditions are favourable. As outlined in Section 11 of the
Air Quality Assessment, the initial NO2 concentration in the blast plumes were based on the
Rating 4 Fume Category which would typically appear as an orange / red plume. However, an
ACARP monitoring study that assessed emissions from blasting from open cut coal mines over
18 months and 500 blasts determined that 73% of blasts had a Rating 0 Fume Category, i.e.
little to no NO2 was produced (Day et.al, 2013). Given that a visible orange / red plume from a
blast is considered to be a reportable incident and based on the ACARP monitoring study, the
likelihood of a Rating 4 Fume Category is very low. Furthermore, measures to minimise or
avoid imperfect blasts and blasting in unfavourable conditions would be implemented and
addressed in a Blast Management Plan.
The modelling for diesel combustion was based on the highest diesel consumption for any of
the mining years (Year 10) but has been applied to mine operation year (Year 7) which is
predicted to have the highest PM concentrations. Private receivers/residences 6, 18, 19A and
23 were chosen for the assessment as they represented the highest potential impacts and
provided spatial variety around the Site. In addition these private receivers/residences were
consistent with those chosen for Monte Carlo analysis. In capturing a range of meteorological
conditions, including unrealistic scenarios of blasting during unfavourable conditions and
assuming a worst case Rating 4 Fume Category, this also over-estimates the peak
concentrations of NO2 at the selected private receivers/residences resulting in a conservative
assessment of potential exposure.
To factor a person’s behaviour (i.e. average daily movements) into a risk assessment is quite
challenging, and is rarely done. Instead, an assumption is made that, throughout their entire
life, a person is in a situation where they could be exposed to the highest concentrations
predicted to occur by the dispersion modelling. This assumption adds conservatism
(i.e. safety) into the risk assessment. Based on this assumption, whether or not a person is
affected by a pollutant compound in air requires them to be present at the location at the same
time the high concentration occurs. However, people do not spend all their time in one spot, for
example an average adult only spends approximately 1.5 hours outdoors per day. Given that
people also move around during the time they spend outdoors, the chance of being present in
the unlikely event that NO2 concentrations are elevated may also be quite low.
Table 5.12 provides the cumulative predicted concentrations for 1 hour average NO2 at the
four private receivers/residences based on the above conservative assumptions. The
cumulative predicted concentrations consisted of NO2 from blasting, diesel powered equipment
and background monitoring data from the closest EPA monitoring station Wallsend EPA
monitoring station2.
Annual NO2 concentrations were determined by averaging the 1 hour time series NO2
concentrations at the private receivers/residences for the assessment years (Pacific
Environment 2016).
2 Source: Pacific Environment (2016) – Section 11.5

SPECIALIST CONSULTANT STUDIES GLOUCESTER RESOURCES LIMITED
Part 2B: Health Risk Assessment Amended Rocky Hill Coal Project
Report No. 806/14
2B-51
Table 5.12
Cumulative maximum 1-hour and annual average NO2 concentrations (g/m3)
Receiver 6 Receiver 18 Receiver 19A Receiver 23
1-hour maximum concentration
Year 4 138 186 160 138
Year 7 143 187 160 139
Annual maximum concentration
Year 4 24 25 23 23
Year 7 25 26 24 24
Source: Pacific Environment (2016) – Tables 13.1 and 13.2.
5.3.3 Risk Characterisation
Streeton (1997) provides the most scientifically defensible information with respect to the
potential for both short-term and long-term effects in association with exposure to NO2. As a
result, the NSW EPA impact assessment criteria which are protective of health outcomes in
sensitive subpopulations are used to determine the potential for short-term effects (246µg/m3)
and long-term effects (62µg/m3) in association with exposure to NO2 from the amended
Project. For assessing the potential short-term and long-term health impacts of NO2, the
predicted cumulative concentrations are presented in Table 5.12 are compared to individual
health-based ambient air quality criteria generated to protect public health. This comparison is
performed by calculating a Hazard Quotient (HQ) which is the ratio of predicted concentrations
to the ambient air quality criterion. A Hazard Index (HI) is the sum of the HQs for all pathways
with similar toxic effects, assuming the health effects are additive”, and is evaluated as follows:
1. HIs of less than or equal to one means that all the maximum predicted
concentrations are below the health based air guideline value and there are no
additive health impacts of concern.
2. HIs of greater than one means that there is the potential for adverse health
effects
The HQ is calculated using the simple equation below.
HQ = Predicted concentration/Health based air guideline value
An example of the calculation is shown below:
For example short-term HQ at receiver 6 in year 4
HQ = 0.49
Where:
Predicted Concentration = 120 g/m3 (Table 5.12)
Health based air guideline value = 246 g/m3 (Table 5.11)

GLOUCESTER RESOURCES LIMITED SPECIALIST CONSULTANT STUDIES
Amended Rocky Hill Coal Project Part 2B: Health Risk Assessment
Report No. 806/14
2B-52
An ‘unacceptable’ risk, as defined by regulatory standards and requirements, is often
determined as the exposure being larger than the air quality criterion used to calculate the
HQs/HIs, i.e. the HQs/HIs >1. This definition of unacceptable risk does not equate with
imminent adverse health effects or even high risk of adverse health effects. It simply means
that the health guideline level has been exceeded.
Notwithstanding their use in this risk assessment, HQs/HIs are relatively blunt tools used to
assist in characterising and prioritising risks. Care must be taken as to the level of importance
that is placed on the numerical value of the HQs/HIs. HQs/HIs should not be used in isolation
of other pertinent data such as mechanistic information on the toxic mode of action and
knowledge of the conservatism incorporated into the exposure assessment and the toxicity
values.
The general rule of thumb for interpreting HQs/HIs is that, values less than 1 present no cause
for concern and values greater than 1 but less than 10 generally also do not represent cause
for concern because of the inherent conservatism embedded in the exposure portions of a risk
assessment. However, it is usual to examine, and perhaps refine, the level of conservatism
that has been assumed in the exposure assumptions. HQs/HIs that are around 10 or greater
present some concern regarding possible health risks, and in these circumstances it is usual to
evaluate the extent to which the “safety margins” in the health guideline value used to compare
estimated exposures may have been eroded in order to gauge whether concern is warranted.
It is common that the risk assessment needs to be refined using site-specific exposure
information or additional analytical data when HQs/HIs are greater than unity (greater than 1).
5.3.3.1 Risk Calculations
Table 5.13 shows the short-term and long-term HQs for the representative of predicted
concentrations of cumulative NO2 at the four modelled private receivers/residences. All the
HQs are less than unity (less than 1) indicating short-term health effects are very unlikely.
Table 5.13
Short-term and long-term HQs for Potential NO2 concentrations
Receiver 6 Receiver 18 Receiver 19A Receiver 23
1 hour maximum concentration
Year 4 0.56 0.76 0.65 0.56
Year 7 0.58 0.76 0.65 0.57
Annual Maximum concentration
Year 4 0.39 0.40 0.37 0.37
Year 7 0.40 0.42 0.39 0.39
It is noted that NO2 and PM10 potentially have additive effects (Streeton, 1997). As such, a
summary of the PM10 emissions (all operations) is presented in Table 5.14 and an assessment
was conducted for the HQ of PM10 and the HI for PM10 and NO2 as presented in Table 5.15
and Table 5.16.

SPECIALIST CONSULTANT STUDIES GLOUCESTER RESOURCES LIMITED
Part 2B: Health Risk Assessment Amended Rocky Hill Coal Project
Report No. 806/14
2B-53
Table 5.14
Maximum Project-only 24-hour and Annual Average PM10 Concentrations at Private
Receivers/Residences (g/m3)
Receiver 6 Receiver 18 Receiver 19A Receiver 23
24 hour maximum concentration
Year 4 18.81 16.60 10.36 19.70
Year 7 35.35 24.30 15.12 32.45
Annual maximum concentration
Year 4 1.40 3.39 2.09 1.16
Year 7 2.28 4.94 3.03 1.76
Source: Pacific Environment (2016) – Tables 9.2 and 9.5.
An example of the HQ calculation is shown below:
For example short-term HQ at receiver 6 in Year 4
HQ = 0.38
Where:
Predicted Concentration = 18.8 g/m3 (Table 5.14)
Health based air guideline value = 50 g/m3 (Table 5.1)
Table 5.15
Short-term and long-term HQs for PM10 concentrations
Receiver 6 Receiver 18 Receiver 19A Receiver 23
Short-term
Year 4 0.38 0.33 0.21 0.39
Year 7 0.71 0.49 0.30 0.65
Long-term
Year 4 0.05 0.11 0.07 0.04
Year 7 0.08 0.16 0.10 0.06
Table 5.16 shows the short-term and long-term HIs for the representative of predicted
concentrations of NO2 and PM10 from the four modelled private receivers/residences
associated with blast and fuel combustion emissions.

GLOUCESTER RESOURCES LIMITED SPECIALIST CONSULTANT STUDIES
Amended Rocky Hill Coal Project Part 2B: Health Risk Assessment
Report No. 806/14
2B-54
Table 5.16
Short-term and long-term HIs for PM10 and NO2 concentrations
Receiver 6 Receiver 18 Receiver 19A Receiver 23
Short-term
Year 4 0.94 1.09 0.86 0.95
Year 7 1.29 1.25 0.95 1.22
Long-term
Year 4 0.44 0.51 0.44 0.41
Year 7 0.48 0.58 0.49 0.45
Four of the short-term HIs were slightly above unity however it should be noted that these
values were based on conservative predictions (See Section 5.3.2). It is therefore considered
appropriate that potential short-term effects can be mitigated by the use of measures known to
minimise fume generation blast design, product selection and quality, blast crew education, on
bench practices, and blasting under wind conditions that favour dispersion of pollutants. Each
of these measures would be identified in a Blast Fume Management Strategy appended to the
Blast Management Plan for the amended Project in order to prevent the modelled NO2
concentrations (orange / red plumes) occurring that were utilised in this assessment.
All of the long-term HIs were found to be less than unity (less than 1). Therefore the cumulative
PM10 and NO2 emissions do not present a long-term health concern.
5.3.4 Conclusion
Because all of HQs for cumulative NO2 emissions for the worst affected private
receivers/residences are all less than or approximately 1, it is very unlikely the emissions
would cause direct short-term and/or long-term health effects. The calculated HIs for
cumulative blast and fuel combustion associated NO2 and PM10 were slightly greater than unity
(greater than 1) at three of the four worst affected private receivers/residences. All the long-
term HIs were less than unity (less than 1). As such there is only a potential for short-term
health effects due to exposure from cumulative blast and fuel combustion associated NO2 and
PM10. Given the conservative approach to predicting NO2 emissions, it is considered
appropriate that potential short-term effects can be mitigated by the use of measures known to
minimise fume generation blast design, product selection and quality, blast crew education, on
bench practices and, and blasting under wind conditions that favour dispersion of pollutants.
Each of these measures would be identified in a Blast Fume Management Strategy appended
to the Blast Management Plan for the amended Project in order to prevent the modelled NO2
concentrations occurring that were utilised in this assessment.
5.4 ASSESSMENT OF DIESEL
Diesel exhaust particles are primarily PM2.5 (including a considerable component of ultrafine
particles, PM0.1) (WIMR-CAR, 2015). These particulates consist mainly of aggregates of
spherical carbon particles coated with organic and inorganic substances, with the composition
of the particles being predominantly organic and inorganic carbon. The organic fraction of
diesel exhaust particulate matter contains compounds such as aldehydes, alkanes and

SPECIALIST CONSULTANT STUDIES GLOUCESTER RESOURCES LIMITED
Part 2B: Health Risk Assessment Amended Rocky Hill Coal Project
Report No. 806/14
2B-55
alkenes, aliphatic hydrocarbons, polycyclic aromatic hydrocarbons and their derivatives. These
substances are considered toxic air contaminants and some of them are genotoxic and
carcinogenic. Overall diesel exhaust particles are considered to be carcinogenic (OEHHA,
2001).
Therefore, calculation of the carcinogenic inhalation risk due to PM2.5 – diesel has been
completed to enable an assessment of the cancer risk in the local community attributable to
the use of diesel within the Site. There is a precedent by NSW authorities i.e. NSW Health and
Office of Environment and Heritage (OEH) that the acceptable cancer risk range for airborne
contaminants is 1 in 100,000 to 1 in 1,000,000. The carcinogenic inhalation risk was therefore
calculated using project-only PM2.5 – diesel concentration i.e. the highest annual average PM2.5
– diesel concentration combined with background monitoring data from the closest EPA
monitoring station Wallsend EPA monitoring station3. This concentration was applied across
the whole population i.e. Gloucester State Suburb and Faulkland State Suburb (Forbesdale
Estate) providing a conservative estimate of the potential cancer risk. This PM2.5 – diesel
concentration was then multiplied by the cancer unit risk factor i.e. 0.000034 μg/m3, derived by
the World Health Organisation (WHO) and an adjustment factor (0.25). The adjustment factor
assumes that residents in the adjacent communities would be at home for 20 hours per day for
365 days of the year for the life of the mine i.e. 21 years. The adjustment factor was therefore
calculated as follows: (20/24 hours x 21/70 years) = 0.25.
The results of the PM2.5 – diesel emissions for the project-only at the 157 privately-owned
receivers/residences and 3 sensitive receiver locations show that the highest annual average
PM2.5 concentration was 0.37 μg/m3 at receiver/residence 18 in Year 104.
The carcinogenic inhalation risk calculation is shown below:
= 0.000003145 i.e. ~0.31 in 100,000/ 3.1 in 1,000,000
The resultant risk of 0.31 in 100,000 is within the acceptable cancer risk range, i.e. 1 in
100,000 to 1 in 1,000,000, generally accepted by NSW, national and international authorities
for airborne contaminants. In addition, it should be noted that real-time monitoring of PM2.5 and
PM10 particulates, reactive management of all particle emissions, and regular maintenance of
diesel vehicles and machinery on site, would reduce the exposure of the community to diesel
particles and further reduce potential risks to health.
3 Source: Pacific Environment (2016) – Section 11.5
4 Source: Pacific Environment (2016) – Table 12.4

GLOUCESTER RESOURCES LIMITED SPECIALIST CONSULTANT STUDIES
Amended Rocky Hill Coal Project Part 2B: Health Risk Assessment
Report No. 806/14
2B-56
6. L I M I TAT I O N S
There are inherent uncertainties in the methods used to estimate emissions concentrations
and limitations on how accurately the impacts of the amended Project can be estimated in
future years. Conservatism has been applied where possible to minimise the risk of any
potential impacts being underestimated in the HRA. These are listed below:
1. Some of the applied concentration response functions (CRFs) were prescribed
for sensitive analysis in situations where a prescribed concentration response
function was not available. This is not unusual because the CRF is a value that is
usually derived from epidemiological studies of an exposed population and relies
on the population being large enough for the health effect to be discernible.
Furthermore multiple CRFs can exist depending on the potency of the
contaminant and the health effect under study. To overcome this, the best CRFs
were chosen with respect to the studied location and population.
2. The population statistics used for mortality were not normalised to account for
demographic differences between different cities and towns. In addition hospital
admissions data did not have any small count suppression for NSW data (public
and private data). Finally emergency department data was only available for
public hospitals. This is not unusual simply because it is not possible to measure
individuals attending private medical practices.

SPECIALIST CONSULTANT STUDIES GLOUCESTER RESOURCES LIMITED
Part 2B: Health Risk Assessment Amended Rocky Hill Coal Project
Report No. 806/14
2B-57
7. C O N C L U SI O NS
This health risk assessment has estimated the risks of an increased incidence of selected
health outcomes due to increased exposures of PM - total, cumulative NO2 and PM2.5- diesel
as a consequence of the amended Project.
The exposure assessment used estimates of the total potential cumulative exposure
(i.e. background plus modelled PM2.5 and PM10 increment from the amended Project) on an
annual and daily basis at the most affected private receivers/residences (receiver 6 in the
Gloucester State Suburb and receiver 18 in the Faulkland State Suburb - Forbesdale) on the
worst day of each modelled year. By using the modelled predictions at the most affected
private receivers/residences to represent exposure across the populations of the respective
state suburbs, the overall community exposure is over estimated and the resulting HRA should
be considered conservative. The air quality impact assessment for the amended Project
(Pacific Environment, 2016) presents the dispersion modelling predictions for maximum 24-
hour and annual average PM2.5 and PM10 GLCs at a total of 160 non-resource related
assessment locations. For both PM2.5 and PM10, the full dataset based on the160 non-resource
related assessment locations in conjunction with background were examined as part of the
HRA.
The health endpoints assessed for PM2.5 and PM10 were short- and long-term mortality and
daily hospitalisations. The general approach used to calculate the risks to health has drawn
upon estimates determined to be relevant to the Australian context, to determine the impact of
PM2.5 and PM10 on health in relation to the known health indicators for NSW. This involved
estimating the change in the incidence of a health outcome resulting from a given change in
PM2.5 and PM10 concentrations. Concentration-response functions (CRFs) for each of the
health endpoints were sourced from the review conducted by Jalaludin and Cowie 2012. In
examining the increased risk in the population (based on annual mortality rates, all causes)
due to the increased long-term exposure to PM2.5 and PM10 concentrations as a result of
cumulative and project-only exposure, it is noted that the number of attributable health
outcomes would be well below 1 in 100,000. The predicted number of attributable cases are
therefore considered to be “sufficiently small and to be of no cause for concern” (NEPM
AAQM). Shorter term exposures to PM2.5 and PM10 are also considered not to pose an
unacceptable risk as the predicted number of attributable cases due to daily mortality (all
cause all ages and cardiovascular disease all ages are less than 1 in orders of magnitude
lower than that due to long-term exposure.
The critical health outcomes with acute and chronic exposure to NO2 include respiratory
disease and associated symptoms, and associated changes in lung function. The NSW EPA
impact assessment criteria, which are protective of these health outcomes in sensitive
subpopulations, have been used to determine the potential for acute effects (246µg/m3) and
chronic effects (62µg/m3) in association with exposure to NO2 from the amended Project. As
NO2 emissions for the selected receivers/residences were less than the Australian air quality
criterion, it is considered unlikely that the blast emissions would cause direct acute and/or
chronic health effects.
The calculated HQs for blast NO2 emissions for the worst affected private receivers/residences
are all less than 1, therefore it is unlikely the cumulative NO2 emissions i.e. blasting, diesel
powered equipment and background monitoring data, would cause direct short-term and/or
long-term health effects. The calculated HIs for cumulative blast and fuel combustion

GLOUCESTER RESOURCES LIMITED SPECIALIST CONSULTANT STUDIES
Amended Rocky Hill Coal Project Part 2B: Health Risk Assessment
Report No. 806/14
2B-58
associated NO2 and PM10 were slightly greater than unity (greater than 1) at three of the four
worst affected private receivers/residences. All the long-term HIs were less than unity (less
than 1). As such there is only a potential for short-term health effects due to exposure from
cumulative blast and fuel combustion associated NO2 and PM10. Given the conservative
approach to predicting NO2 emissions, it is considered appropriate that potential short-term
effects can be mitigated by the use of measures known to minimise fume generation blast
design, product selection and quality, blast crew education, on bench practices and, and
blasting under wind conditions that favour dispersion of pollutants. Each of these measures
would be identified in a Blast Fume Management Strategy appended to the Blast Management
Plan for the amended Project in order to prevent the modelled NO2 concentrations occurring
that were utilised in this assessment.
Diesel exhaust particles are primarily PM2.5 (including a considerable component of ultrafine
particles, PM0.1) (WIMR-CAR, 2015). Calculation of the carcinogenic inhalation risk due to
PM2.5 – diesel enabled an assessment of the cancer risk in the local community attributable to
the use of diesel within the Site. The carcinogenic inhalation risk was therefore calculated
using project-only PM2.5 – diesel concentration i.e. the highest annual average PM2.5 – diesel
concentration combined with background monitoring data (receiver/residence 18 in Year 10).
This concentration was applied across the whole population i.e. Gloucester State Suburb and
Faulkland State Suburb (Forbesdale Estate) providing a conservative estimate of the potential
cancer risk. This PM2.5 – diesel concentration was then multiplied by the cancer unit risk factor
i.e. 0.000034 μg/m3, derived by the World Health Organisation (WHO) and an adjustment
factor (0.25). The resultant risk, 0.31 in 100,000, is within the acceptable cancer risk range, i.e.
1 in 100,000 to 1 in 1,000,000 generally accepted by NSW, national and international
authorities, for airborne contaminants. In addition, it should be noted that real-time monitoring
of PM2.5 and PM10 particulates, reactive management of all particle emissions, and regular
maintenance of diesel vehicles and machinery on site, would reduce the exposure of the
community to diesel particles and further reduce potential risks to health.
There are inherent uncertainties in the methods used to estimate emissions and
concentrations and limitations on how accurately the impacts of the amended Project can be
estimated in future years. Consequently, in order to minimise the risk of under estimation
throughout the HRA, conservatism has been applied where possible. The modelling data used
to inform this HRA used worst case assumptions and therefore it is expected that actual
ground level concentrations would be lower during the normal operation of the amended
Project. The modelled predictions at the most affected private receivers/residences were used
to represent exposure across the populations of the respective state suburbs with the result
that the overall community exposure was over estimated. This is further discussed in the
amended air quality assessment (Pacific Environment, 2016). The PM2.5 and PM10 exposure
assessment evaluates the potential of the emissions to cause direct effects on individuals who
may be exposed either on a short-term, infrequent basis or long-term basis, i.e. assuming 24
hours per day for each day of the year for 70 years. This exposure scenario is highly unlikely
especially since the life of the mine is estimated to be up to 21 years. The applied exposure
assessment method for PM2.5 and PM10 is typically reserved for populations of greater than
25,000 because there are important challenges in translating methods intended for large
populations to those for addressing risk in smaller populations. Nevertheless, when taken
together with the modelling predictions, the uncertainties err on the side of safety. The
predicted NO2 emissions due to blasting considered a range of meteorological conditions,
including unrealistic scenarios of blasting during unfavourable conditions as well as assuming
a worst case Level 4 fume category, which over-estimated the peak concentrations of NO2 at

SPECIALIST CONSULTANT STUDIES GLOUCESTER RESOURCES LIMITED
Part 2B: Health Risk Assessment Amended Rocky Hill Coal Project
Report No. 806/14
2B-59
the selected private receivers/residences. This is further discussed in the amended air quality
assessment (Pacific Environment, 2016). The PM2.5 – diesel exposure assessment used PM2.5
– diesel modelled predictions based on the highest diesel consumption for any of the mining
years, from a mine operation year (Year 7) predicted to have the highest predicted PM2.5
concentration.
In consideration of the community concerns raised, it is important to note that health issues in
relation to exposure to PM - total, NO2 and PM2.5 – diesel from the amended Project have been
outlined and the associated potential for acute or chronic effects assessed. The exposure
assessments have used both standards adopted by all Australian jurisdictions and exposure
response functions relevant to the Australian population (where relevant) to estimate likelihood
of unacceptable risk. Susceptible/ vulnerable groups within adjacent communities have been
taken into consideration and a range of health end points assessed i.e. short- and long-term
mortality and daily hospitalisations. Overall it is concluded that air emissions from the amended
Rocky Hill Coal Project present little likelihood of causing adverse health effects to exposed
individuals in the vicinity of the Site.

GLOUCESTER RESOURCES LIMITED SPECIALIST CONSULTANT STUDIES
Amended Rocky Hill Coal Project Part 2B: Health Risk Assessment
Report No. 806/14
2B-60
8. R E F E RE N C ES
Anderson GB, Krall JR, Peng RD, Bell ML (2012). Is the relation between ozone and mortality
confounded by chemical components of particulate matter? Analysis of 7 components
in 57 US communities. Am J Epidemiol. Oct 15;176(8):726-32
Barnett, A. G., Williams, G. M., Schwartz, J., Neller, A. H., Best, T. L., Petroeschevsky, A. L. &
Simpson, R. W. (2005). Air pollution and child respiratory health: a case-crossover
study in Australia and New Zealand” American Journal of Respiratory & Critical Care
Medicine, 171, 1272-8.
Bauer, M.A., Utell, M.J., Morrow, P.E., Speers, D.M. and Gibb, F.R. (1986). “Inhalation of 0.30
ppm nitrogen dioxide potentiates exercise-induced bronchospasm in asthmatics” Am.
Rev. Respir. Dis. 134(6): 1203 - 1208. (As cited in IEH, 1996).
Bell ML; Levy JK; Lin Z (2008). “The effect of sandstorms and air pollution on cause-specific
hospital admissions in Taipei, Taiwan”. Occup Environ Med, 65: 104-111.
Brauer M, Hoek G, Smit HA, de Jongste JC, Gerritsen J, Postma DS, Kerkhof M, Brunekreef
B. (2007). “Air pollution and development of asthma, allergy and infections in a birth
cohort” Eur Respir J. May;29(5):879-88. Epub 2007 Jan 24.
Bylin, G., Hedenstierna, G., Lindvall, T. and Sundin, B. (1988). Ambient nitrogen dioxide
concentrations increase bronchial responsiveness in subjects with mild asthma Eur.
Respir. J. 1(7): 606 - 612.
Cesaroni G, Badaloni C, Gariazzo C, Stafoggia M, Sozzi R, Davoli M, Forastiere F. (2013)
“Long-term exposure to urban air pollution and mortality in a cohort of more than a
million adults in Rome” Environ Health Perspect. Mar;121(3):324-31.
Chen LC; Hwang JS (2005).Effects of subchronic exposures to concentrated ambient particles
(CAPs) in mice IV Characterization of acute and chronic effects of ambient air fine
particulate matter exposures on heart-rate variability Inhal Toxicol, 17: 209-216.
Cohen R., Patel A. and Green F. (2009). Lung disease caused by exposure to coal mine and
silica dust. Seminars in Respiratory and Critical Care Medicine 29(06): 651-661.
Department of Health (DoH) 1993. ‘Oxides of Nitrogen’. Third Report, Advisory Group on the
Medical Aspects of Air Pollution Episodes; HMSO, London.
Department of Health (DoH) 1995. ‘Health Effects of Exposures to Mixtures of Air Pollutants’.
Fourth Report, Advisory Group on the Medical Aspects of Air
Pollution Episodes; HMSO, London.
Dockery D W, Pope C A, Xiping Xu, Spengler J D, Ware J H, Fay M E, Ferris B G and Speizer
F E (1993) “An association between air pollution and mortality in six US cities” The New
England Journal of Medicine, Volume 329, Number 24,1753-1759

SPECIALIST CONSULTANT STUDIES GLOUCESTER RESOURCES LIMITED
Part 2B: Health Risk Assessment Amended Rocky Hill Coal Project
Report No. 806/14
2B-61
Dominici F; Peng RD; Bell ML; Pham L; McDermott A; Zeger SL; Samet JL (2006). Fine
particulate air pollution and hospital admission for cardiovascular and respiratory
diseases. JAMA, 295: 1127-1134.
enHealth (2012a). Environmental health risk assessment. Guidelines for assessing health risks
from environmental hazards. Department of Health and Aging and enHealth Council,
Commonwealth of Australia.
enHealth (2012b). Australian Exposure Factor Guidance. Guidelines for assessing health risks
from environmental hazards. Department of Health and Aging and enHealth Council,
Commonwealth of Australia.
Environment Protection and Heritage Council (2005). Expansion of the multi-city mortality and
morbidity study. Final report. Volume 3. Tabulated results, Environment Protection and
Heritage Council.
Finkelman R.B., Orem W., Castranova V., Tatu C.A., Belkin H.E., Zheng B. et al. (2002).
Health impacts of coal and coal use: Possible solutions. International Journal of Coal
Geology 50: 425-443
Franklin M; Koutrakis P; Schwartz J (2008). The role of particle composition on the association
between PM2.5 and mortality. Epidemiology, 19: 680-689.
Gehring U, Wijga AH, Brauer M, Fischer P, de Jongste JC, Kerkhof M, Oldenwening M, Smit
HA, Brunekreef B. (2010). Traffic-related air pollution and the development of asthma
and allergies during the first 8 years of life. Am J Respir Crit Care Med. Mar
15;181(6):596-603.
Gehring U; Heinrich J; Kramer U; Grote V; Hochadel M; Sugiri D; Kraft M; Rauchfuss K;
Eberwein HG; Wichmann H-E (2006). Long-term exposure to ambient air pollution and
cardiopulmonary mortality in women. Epidemiology, 17: 545-551
Hasselblad, V., Eddy, D.M. and Kotchmar, D.J. (1992). Synthesis of environmental evidence:
nitrogen dioxide epidemiology studies. J. Air Waste Manage. Assoc. 42: 662 - 671.
HEI, Health Effects Institute, (2003) Revised Analyses of Time-Series Studies of Air Pollution
and Health, Special Report
Heppleston A.G. (1992). Coal workers' pneumoconiosis: a historical perspective on its
pathogenesis. American Journal of Industrial Medicine 22: 905-923.
Hime N., Cowie C., Marks G. (2015). “Review of the health impacts of emission sources, types
and levels of particulate matter air pollution in ambient air in NSW”
Hoek, G, Ranjini M Krishnan , Rob Beelen , Annette Peters , Bart Ostro , Bert Brunekreef and
Joel D Kaufman (2013). Long-term air pollution exposure and cardio- respiratory
mortality: a review Environmental Health 2013,
Jaakkola, J.J.K., Paunio, M., Virtanen, M. and Heinonen, O.P. (1991). Low-level air pollution
and upper respiratory infections in children. Am. J. Public Health 81: 1060 - 1063. (As
cited in WHO, 1997).

GLOUCESTER RESOURCES LIMITED SPECIALIST CONSULTANT STUDIES
Amended Rocky Hill Coal Project Part 2B: Health Risk Assessment
Report No. 806/14
2B-62
Jalaludin, B and Cowie, C (2012), Health Risk Assessment – Preliminary Work to Identify
Concentration Response Functions for Selected Ambient Air Pollutants, report
prepared for EPA Victoria, Respiratory and Environmental Epidemiology, Woolcock
Institute of Medical Research, Glebe, NSW, 30 June 2012.
Jalaludin, B., B. Khalaj, et al. (2008). "Air pollution and ED visits for asthma in Australian
children: a case-crossover analysis." International Archives of Occupational and
Environmental Health 81(8): 967-974.
Jalaludin, B, and Cowie, C (2012), “Health Risk Assessment – Preliminary Work to Identify
Concentration Response Functions for Selected Ambient Air Pollutants”, Respiratory
and Environmental Epidemiology, Woolcock Institute of Medical Research, Glebe, 30
June 2012
Katestone Environmental Pty Ltd (2011). “NSW Coal Mining Benchmarking Study:
International Best Practice Measures to Prevent and/or Minimise Emissions of
Particulate Matter from Coal Mining”
Kraft, M., Eikmann, T., Kappos, A., Künzli, N., Rapp, R., Schneider, K., Seitz, H., Voss, J-U.
and Wichmann, E-H. (2005). The German view: Effects of nitrogen dioxide on human
health – derivation of health-related short-term and long-term values. Int. J. Hyg.
Environ. Health 208: 305 – 318.
Krewski D, Jerrett M, Burnett R T, Ma R, Hughes E, et al. (2009). Extended follow- up and
spatial analysis of the American Cancer Society study linking particulate air pollution
and mortality. HEI Research Report, 140, Health Effects Institute, Boston, MA.
Laden F; Schwartz J; Speizer FE; Dockery DW (2006). Reduction in fine particulate air
pollution and mortality: extended follow-up of the Harvard Six Cities study. Am J Respir
Crit Care Med, 173: 667-672
MacIntyre EA1, Karr CJ, Koehoorn M, Demers PA, Tamburic L, Lencar C, Brauer M (2011).
Residential air pollution and otitis media during the first two years of life. Epidemiology.
Jan;22(1):81-9.
Morgan, G., V. Sheppeard, et al. (2010). "Effects of bushfire smoke on daily mortality and
hospital admissions in Sydney, Australia." Epidemiology 21(1): 47-55.
Morgenstern V, Zutavern A, Cyrys J, Brockow I, Gehring U, Koletzko S, Bauer CP, Reinhardt
D, Wichmann HE, Heinrich J. (2007). Respiratory health and individual estimated
exposure to traffic-related air pollutants in a cohort of young children. Occup Environ
Med. Jan;64(1):8-16. Epub 2006 Aug 15.
Morrow, P.E., Utell, M.J., Bauer, M.A., Smeglin, A.M., Frampton, M.W., Cox, C., Speers, D.M.
and Gibb, F.R. (1992). Pulmonary performance of elderly normal subjects and subjects
with chronic obstructive pulmonary disease exposed to 0.3 ppm nitrogen dioxide. Am.
Rev. Respir. Dis. 145(2 Pt 1): 291 - 300.
NEPM, National Environment Protection Measure (1998). Ambient Air Quality National
Environmental Protection Measure (NEPM). National Environmental Protection Council
(NEPC).

SPECIALIST CONSULTANT STUDIES GLOUCESTER RESOURCES LIMITED
Part 2B: Health Risk Assessment Amended Rocky Hill Coal Project
Report No. 806/14
2B-63
NEPM, National Environment Protection Measure (2010). Review of the National Environment
Protection (Ambient Air Quality) Measure: Discussion Paper Air Quality Standards.
National Environmental Protection Council (NEPC).
NHC, National Health Council (2004). A Guide to health impact assessment: A policy tool for
New Zealand. Public Health Advisory Committee, National Health Council of New
Zealand. March 2004. Available at
http://www.nhc.govt.nz/PHAC/publications/GuideToHIA.pdf
NSW EPA, New South Wales Environment Protection Authority (2012). Air Emissions
Inventory for the Greater Metropolitan Region in New South Wales: Technical Report
No. 1 Consolidated Natural and Human-Made Emissions. Sydney, NSW Environment
Protection Authority.
NSW Health, New South Wales Environment Health (2010a). Analysis of Beach General
Practitioner Encounter Data to Examine the Potential Health Effects of the Mining
Industry and Other Exposures in Singleton, Muswellbrook and Denman. Sydney, NSW,
NSW Health.
NSW Health, New South Wales Environment Health (2010b). Respiratory and Cardiovascular
Diseases and Cancer Among Residents in the Hunter New England Area Health
Service. Sydney, NSW, NSW Health.
OEHHA, Office of Environmental Health Hazard Assessment (1999). Nitrogen Dioxide Acute
Toxicity Summary; Determination of Acute Reference Exposure Levels for Airborne
Toxicants. Office of Environmental Health Hazard Assessment Californian
Environmental Protection Agency.
http://www.oehha.ca.gov/air/acute_rels/pdf/10102440A.pdf
OEHHA, Office of Environmental Health Hazard Assessment 2001, Particulate Matter Health
Effects and Standard Recommendations Office of Environmental Health Hazard
Assessment Californian Environmental Protection Agency.
http://oehha.ca.gov/air/criteria-pollutant/2001-particulate-matter-health-effects-and-
standard-recommendations
Ostro B; Broadwin R; Green S; Feng W-Y; Lipsett M (2006). Fine particulate air pollution and
mortality in nine California counties: results from CALFINE. Environ Health Perspect,
114: 29-33.
Peel JL; Tolbert PE; Klein M; Metzger KB; Flanders WD; Knox T; Mulholland JA; Ryan PB;
Frumkin H (2005). Ambient air pollution and respiratory emergency department visits.
Epidemiology, 16: 164-174.
Pacific Environment Limited (2016). Rocky Hill Coal Project Updated Air Quality and
Greenhouse Gas Assessment. Prepared for Gloucester Resources Limited.
Petsonk E.L., Rose C. and Cohen R. (2013). Coal mine dust lung disease. New lessons from
old exposure. Am J Respir Crit Care Med 187(11): 1178-1185.

GLOUCESTER RESOURCES LIMITED SPECIALIST CONSULTANT STUDIES
Amended Rocky Hill Coal Project Part 2B: Health Risk Assessment
Report No. 806/14
2B-64
Pilotto, L.S., Nitschke, M., Smith, B.J., Pisaniello, D., Ruffin, R.E., McElroy, H.J., Martin, J.,
Hiller, J.E. (2004). Randomized controlled trial of unflued gas heater replacement on
respiratory health of asthmatic schoolchildren. Int. J. Epidemiol. 33(1): 208 - 214.
Pope CA 3rd, Ezzati M, Dockery DW (2009). Fine-particulate air pollution and life expectancy
in the United States. New England Journal of Medicine, 360(4):376–386.
Pope, C. A., III, M. J. Thun, et al. (1995). "Particulate air pollution as a predictor of mortality in
a prospective study of US adults." American Journal of Respiratory and Critical Care
Medicine 151(3): 669-674.
Pope, C. A., III. and D. W. Dockery (2006). “Health effects of fine particulate air pollution: Lines
that connect”. Journal of the Air & Waste Management Association 56(6): 709-742.
Pope, C.A.; III; Burnett, R.T.; Thun, M.J.; Calle, E.E.; Krewski, D.; Ito, K.; Thurston, G.D.
(2002). “Lung Cancer, Cardiopulmonary Mortality, and Long-Term Exposure to Fine
Particulate Air Pollution; J. Am. Med. Assoc. 287, 1132-1141.
Pope, CA, Dockery, DW, & Schwartz, J (1995). ‘Review of epidemiological evidence of health
effects of particulate air pollution’, Inhalation Toxicology, 7: 1-18.
Raaschou-Nielsen O, Andersen ZJ, Beelen R, Samoli E, Stafoggia M, Weinmayr G, Hoffmann
B, Fischer P, Nieuwenhuijsen MJ, Brunekreef B, Xun WW, Katsouyanni K,
Dimakopoulou K, Sommar J, Forsberg B, Modig L, Oudin A, Oftedal B, Schwarze PE,
Nafstad P, De Faire U, Pedersen NL, Ostenson CG, Fratiglioni L, Penell J, Korek M,
Pershagen G, Eriksen KT, Sørensen M, Tjønneland A, Ellermann T, Eeftens M,
Peeters PH, Meliefste K, Wang M, Bueno-de-Mesquita B, Key TJ, de Hoogh K, Concin
H, Nagel G, Vilier A, Grioni S, Krogh V, Tsai MY, Ricceri F, Sacerdote C, Galassi C,
Migliore E, Ranzi A, Cesaroni G, Badaloni C,
Forastiere F, Tamayo I, Amiano P, Dorronsoro M, Trichopoulou A, Bamia C, Vineis P, Hoek G.
(2013). Air pollution and lung cancer incidence in 17 European cohorts: prospective
analyses from the European Study of Cohorts for Air Pollution Effects (ESCAPE).
Lancet Oncol. Aug;14(9):813-22.
Roger, L.J., Horstman, D.H., McDonnell, W.F., Kehrl, H., Seal, E., Chapman, R.S. and
Massaro, E.J. (1985). Pulmonary effects in asthmatics exposed to 0.3 ppm NO2 during
repeated exercise. Toxicologist 5: 70. (As cited in IEH, 1996).
Rückerl R, Schneider A, Breitner S, Cyrys J, Peters A (2011). Health effects of particulate air
pollution: A review of epidemiological evidence.. Inhal Toxicol. Aug;23(10):555-92
Simpson R, Williams G, Petroeschevsky A, Best T, Morgan G, Denison L, Hinwood A, Neville
G, Neller A (2005a).The short-term effects of air pollution on daily mortality in four
Australian cities. Aust N Z J Public Health 2005; 29: 205-12
Simpson R, Williams G, Petroeschevsky A, Best T, Morgan G, Denison L, Hinwood A, Neville
G (2005b). The short-term effects of air pollution on hospital admissions in four
Australian cities. Aust N Z J Public Health 2005; 29:213-21

SPECIALIST CONSULTANT STUDIES GLOUCESTER RESOURCES LIMITED
Part 2B: Health Risk Assessment Amended Rocky Hill Coal Project
Report No. 806/14
2B-65
Smith, B.J., Nitschke, M., Pilotto, L.S., Ruffin, R.E., Pisaniello, D.L. and Willson, K.J. (2000).
Health effects of daily indoor nitrogen dioxide exposure in people with asthma. Eur.
Respir. J. 16(5): 879 - 885.
Strand, V., Rak, S., Svartengren, M. and Bylin, G. (1997). Nitrogen dioxide exposure enhances
asthmatic reaction to inhaled allergen in subjects with asthma. Am. J. Respir. Crit. Care
Med. 155(3): 881 - 887.
Strand, V., Salomonsson, P., Lundahl, J. and Bylin, G. (1996). Immediate and delayed effects
of nitrogen dioxide exposure at an ambient level on bronchial responsiveness to
histamine in subjects with asthma. Eur. Respir. J. 9(4): 733 - 740.
Streeton, J. A. (1997). A review of existing health data on six air pollutants. Prepared for the
National Environment Protection Council. May. NEPC Service Corporation.
http://www.ephc.gov.au/pdf/Air_Quality_NEPM/6_pollutants_report_em_Streeton.pdf
Tunnicliffe, W.S., Burge, P.S. and Ayres, J.G. (1994). Effect of domestic concentrations of
nitrogen dioxide on airway responses to inhaled allergen in asthmatic patients. Lancet
344(8939-8940): 1733 - 1736.
US EPA, United States Environmental Protection Agency (2001). Acute Exposure Guideline
Levels for Selected Airborne Chemicals: Volume 11. National Academy of Sciences.
US EPA, United States Environmental Protection Agency (2004). ‘Air Quality Criteria for
Particulate Matter Vol 1’, USA, EPA/600/P-99/002aF, Available at
http://oaspub.epa.gov/eims/eimscomm.getfile?p_download_id=435945.
US EPA, United States Environmental Protection Agency (2008). Draft scope and methods
plan for risk/exposure assessment: secondary NAAQS review for oxides of nitrogen
and oxides of sulfur.
US EPA, United States Environmental Protection Agency (2010). Quantitative Health Risk
Assessment for Particulate Matter, Health and Environmental Impacts Division, US
Environmental Protection Agency, NC, USA: 596.
US EPA, United States Environmental Protection Agency (2012). Provisional Assessment of
Recent Studies on Health Effects of Particulate Matter Exposure, National Centre for
Environmental Assessment RTP Division Office of Research and Development U.S.
Environmental Protection Agency Research Triangle Park, NC 27711, December 2012,
EPA/600/R-12/056F
US EPA, United States Environmental Protection Agency (2009). Final Report: Integrated
Science Assessment for Particulate Matter. U.S. Environmental Protection Agency,
Washington, DC, EPA/600/R-08/139F
WHO, World Health Organisation (1948). Preamble to the Constitution of the World Health
Organization as adopted by the International Health Conference, New York, 19-22
June, 1946 ; signed on 22 July 1946 by the representatives of 61 States (Official
Records of the World Health Organization, no. 2, p. 100) and entered into force on 7
April 1948.

GLOUCESTER RESOURCES LIMITED SPECIALIST CONSULTANT STUDIES
Amended Rocky Hill Coal Project Part 2B: Health Risk Assessment
Report No. 806/14
2B-66
WHO, World Health Organisation (1997). Environmental Health Criteria 188, Nitrogen Oxides.
Second Edition. World Health Organisation. Geneva.
http://www.inchem.org/documents/ehc/ehc/ehc188.htm
WHO, World Health Organisation (2000a). Guidelines for Air Quality. World Health
Organisation, Geneva.
WHO, World Health Organisation (2000b). Air Quality Guidelines for Europe 2nd Edition.
World Health Organisation Regional Office for Europe (WHO Regional Publications,
European Series Number 91). http://www.euro.who.int/document/e71922.pdf
WHO, World Health Organisation (2001). Quantification of the health effects of exposure to air
pollution. Report of a WHO Working Group. European Centre for Environmental Health.
http://www.euro.who.int/__data/assets/pdf_file/0011/112160/E74256.pdf.
WHO, World Health Organisation (2006). Air quality guidelines. Global update. 2005.
Particulate matter, ozone, nitrogen dioxide and sulfur dioxide Copenhagen, WHO
Regional Office for Europe.
WHO, World Health Organisation (2013). Health effects of particulate matter. Policy
implications for countries in eastern Europe, Caucasus and central Asia, WHO
Regional Office for Europe.
WIMR-CAR, Woolcock Institute of Medical Research, Centre for Air Quality and Health
Research and Evaluation (2015). “Review of the health impacts of emission sources,
types and levels of particulate matter air pollution in ambient air in NSW”
http://www.car-
cre.org.au/images/content/Health%20impacts%20of%20PM%20report_final%20for%20
web.pdf
Wouters E.F.M., Jorna T.H.J.M. and Westenend M. (1994). Respiratory effects of coal dust
exposure: clinical effects and diagnosis. Experimental Lung Research 20: 385-394.

SPECIALIST CONSULTANT STUDIES GLOUCESTER RESOURCES LIMITED
Part 2B: Health Risk Assessment Amended Rocky Hill Coal Project
Report No. 806/14
2B-67
APPENDIX 1
Key Differences between the Health Risk Assessment for the 2013 Project and
Amended Project
(Total number of pages including blank pages = 4)

GLOUCESTER RESOURCES LIMITED SPECIALIST CONSULTANT STUDIES
Amended Rocky Hill Coal Project Part 2B: Health Risk Assessment
Report No. 806/14
2B-68
This page has intentionally been left blank

SPECIALIST CONSULTANT STUDIES GLOUCESTER RESOURCES LIMITED
Part 2B: Health Risk Assessment Amended Rocky Hill Coal Project
Report No. 806/14
2B-69
Key Differences between the Health Risk Assessment for the 2013 Project and Amended Project
Project Component 2013 Project Amended Project
Assessment Locations
The considered assessment locations included 150 privately-owned residences in the vicinity of the Site and 3 sensitive receiver locations within Gloucester township.
The considered assessment locations included 157 privately-owned residences in the vicinity of the Site and 3 sensitive receiver locations within Gloucester township.
Concentration Reference Factors
The source of the Concentration Reference Factors (CRFs) used in the exposure assessment was Anderson et al (2004).
The source of the CRFs used in the exposure assessment was changed to Jalaludin and Cowie (2012) because the latter study outlined recommended CRFs to be used for health risk assessments in the Australian context.
Baseline Health Statistics
The baseline health statistics used were based upon the Hunter New England Local Health District for 2009-2010 and daily hospital admissions for all of NSW in 2006-2007.
A total of four health endpoints were evaluated (i.e. long-term deaths, short-term deaths, hospitalisations due to cardiovascular and hospitalisations due to all respiratory disease).
The baseline health statistics used was for Tamworth given the local environment was more similar to the assessed communities i.e. State suburb of Gloucester and Faulkland State Suburb (Forbesdale Estate area).
The specific health endpoint evaluated in the exposure assessment was expanded to twelve health effects.
Blasting & Diesel Combustion
Blast fume assessed, however, no consideration of diesel combustion sources generating PM2.5 and NO2. No characterisation of risk for PM10.
Assessment of both blast fume and diesel combustion. The assessment of -diesel was conducted based upon the worst affected private residence during the year with the highest diesel consumption.
The potential additive effects of cumulative NO2 and PM10 were also considered as part of the Hazard Index calculation
Data Presentation The particulate matter and NO2
concentrations used in the exposure assessment were presented as percentiles.
The particulate matter and NO2
concentrations used in the exposure assessment are presented as maximum concentrations.
Health Risk Outcomes
From a health-risk perspective, the 2013 project assessed project-only particulate levels which resulted in an increase in base incidence in Gloucester State Suburb and Faulkland State Suburb (Forbesdale Estate) of less than 1 in 100,000, which is considered to be “sufficiently small and to be of no cause for concern” (NEPM AAQM).
From a health-risk perspective, the amended Project assessed cumulative particulate levels which resulted in an increase in base incidence in Gloucester State Suburb and Faulkland State Suburb (Forbesdale Estate) of less than 1 in 100,000, which is considered to be “sufficiently small and to be of no cause for concern” (NEPM AAQM). Whilst the changes in health risk are not directly comparable between the assessments, given the reductions in project-only particulate emissions, the overall health risk is likely to have similarly reduced.

GLOUCESTER RESOURCES LIMITED SPECIALIST CONSULTANT STUDIES
Amended Rocky Hill Coal Project Part 2B: Health Risk Assessment
Report No. 806/14
2B-70
This page has intentionally been left blank