Parenteral Nutrition Competency Education · and diarrhea Central PN Peripheral PN Short term...
59
Parenteral Nutrition Competency Education Version 1.6 Last Updated: 05/03/2019 Developed by the Nutrition and Metabolic Support Team
Transcript of Parenteral Nutrition Competency Education · and diarrhea Central PN Peripheral PN Short term...

Parenteral NutritionCompetency Education
Version 1.6
Last Updated: 05/03/2019
Developed by the Nutrition and Metabolic Support
Team

Goals
• Provide education support and learning resources for Parenteral
Nutrition (PN) to prescribers, dietitians, nurses and pharmacists.
• Provide a framework for developing and maintaining competency
for the safe prescription of Nutrition and Metabolic Support (NMS)
by attending physicians.
• Draft and modify policies and procedures to ensure safe practices
for the prescribing, administration, and monitoring of PN.
• Reduce patient care costs.
• Facilitate and accelerate the achievement of nutritional goals.
• Reduce harm and improve patient safety.
2

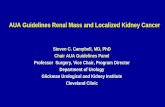
Nutrition Assessment
Functional GI tract
Yes No
EN PN
Intolerance to EN or
moderate-to-severe
malnutrition in whom oral
intake or EN is not possible or
sufficient
Hospice/Terminally Ill/Poor Prognosis
Do not recommend PNPN Indications:
• Peritonitis• Obstruction• Ileus• GI ischemia• Intractable vomiting
and diarrhea
Central PNPeripheral
PN
Short term Long-term or fluid restriction
GI function returns
GI function
Normal Compromised
Standard formula
Peptide or elemental formula
Timeframe for Initiating PN in Adults
Initiation ofPN
Considerations
7 days Well-nourished, stable adult patients unable to receive ≥50% of estimated oral or enteral nutrients
3-5 days Nutritionally-at-risk and unlikely to achieve desired oral intake or EN
ASAP Baseline moderate or severe malnutrition in whom oral intake or EN is not possible or sufficient
Delay Patients with severe metabolic instability until condition has improved
NMS Support Decision Tree
Ayers P. (2014). ASPEN PN Handbook, 2nd edition
Worthington et al. JPEN 2017;41;324-377.
3

NMS Support Decision Tree
Purpose:
A guideline to assist clinical dietitians and physicians in evaluating the
appropriateness of PN.
Goal:
1. To minimize inappropriate PN orders.
2. To reduce unnecessary risk and complications, such as infections, resulting
from prescribing PN that is not indicated.
4

Clinical Conditions Warranting Cautious Initiation of PN in Adults
Conditions Suggested Criteria
Hyperglycemia Glucose greater than 180 mg/dL
Azotemia Blood urea nitrogen greater than 100 mg/dL
Hypertriglyceridemia Serum TG greater than 200 mg/dL
Hyponatremia Serum sodium less than 130 mEq/L
Hypernatremia Serum sodium greater than 150 mEq/L
Hypokalemia Serum potassium less than 3 mEq/L
Hypomagnesemia Serum magnesium less than 1.3 mEq/L
Hypocalcemia Ionized calcium less than 4.5 mg/dL
Hypophosphatemia Serum phosphorous less than 2 mg/dL
Worthington et al. JPEN 2017;41;324-377.
5

Clinical setting where PN is NOT Indicated
1. Aggressive nutritional support is not desired by the patient or
legal guardian.
2. Prognosis does not warrant aggressive nutritional support.
3. PN therapy is anticipated to be less than 5 days.
4. Patients has a functional GI tract capable of adequate
absorption of nutrients.
5. Risks of PN are judged to exceed the potential benefits.
6

Initiation of PN
• Nutrition Assessment:
• Should be performed prior to the initiation of PN.
• Electrolytes:
• Standard electrolytes solutions are used preferentially over customized formulations.
• In addition to the standard electrolytes solution, additional amounts of individual electrolytes can be added to the PN.
• Individual electrolytes cannot be removed from the standard solution.
• Lab value monitoring:
• All patients receiving PN should have baseline and follow-up laboratory values ordered and monitored.
• A standard PN laboratory order set is available and should be considered at the time PN is ordered.
• Additives:
• Multivitamins (MVI) and trace elements (MTE) are added automatically.
• Additional additives should be tailored to the patient based upon any deficiency, excess, or disease process that affects requirements.
• Only drugs that are compatible with PN are to be added to the PN formulation. Contact the pharmacist (ext. 55492) for assistance.
• PN admixtures contain lipids unless there is a contraindication (e.g. soybean and/or egg allergies).
7

Cycling PN
• Infusion of full volume of PN for < 24hr/day (e.g. 12 hours overnight)
• Associated with better quality of life.
• Has shown some advantage to reverse fatty liver resulted from continuous
PN infusion.
• Requires a higher infusion rate which may not be tolerated by all patients.
• Cycling should only be considered after the patient has been stable on
continuous 24 hour infusion for several days.
• Rate calculation (calculated by pharmacist):
• Half rate for first and last hours to avoid hyper- and hypoglycemia.
• Full rate for 10 hours.
• e.g., 2200 ml PN over 12 hours will be infused at:
• 100 ml/hr for the first hour
• 200 ml/hr for the next 10 hours
• 100 ml/hr for the final hour
8

Abrupt Discontinuation of PN
• If PN must be intentionally held or discontinued once administration has
begun, reduce infusion rate by 50% for 2 hours and the stop the infusion
completely.
• If PN is abruptly discontinued for any reason and the patient is not being fed
orally or enterally*:
• D10W will be infused via a peripheral or central line at the same rate
as the PN solution,
• The prescriber will be contacted for further orders,
• The nurse will obtain venous blood sugar results after 30 minutes, and
• D50W will be readily available.
*POLICY STAT ID #5426057
9

Routes of PN infusion: Central Line PN
• Usual osmolarity = >1200 mOsmol/L
• Advantages:
• Can provide full nutritional support since there are no limits to the concentration of dextrose and amino acids.
• No risk of thrombophlebitis.
• No infusion-related pain.
• Disadvantages:
• Requires a surgical procedure for line placement.
• Higher risk of sepsis compared to peripheral PN administration.
• High risk of mechanical complications.
10

Routes of PN infusion: Peripheral Line PN
• Maximum osmolarity = 900 mOsmol/L
• Indications:• Only for short-term use (no more than 10-14 day).• As supplemental PN or bridge therapy during transition periods.• Where oral intake or enteral nutrition (EN) is suboptimal.• Where clinical circumstances do not justify central line placement.
• Advantages:• Does not require a surgical procedure for line placement.• Less risk of sepsis compared to Central Line PN.• No risk of mechanical complications.
• Disadvantages:• High risk of thrombophlebitis.• Infusion-related adverse events, especially pain.
• Excessively high volumes are required to maintain osmolarity below 900 mOsmol/L which may preclude full nutrition support.
11

Parenteral Nutrition Solutions: The Basics
• Contain admixtures of carbohydrate, amino acids, fats,
electrolytes, vitamins, minerals and trace elements.
• Provide all of the necessary nutrients to meet requirements for
growth, anabolism, weight gain and wound healing.
• Individualized, with consideration given to each patient’s clinical
status, diagnosis, fluid status, electrolyte balance, and goal of
therapy.
12

Fluid Requirements
• Amount of fluid required is dependent on the patient’s age (neonate, pediatric, or adult.)
• Most adults require 30-35 ml/kg per 24 hours.
• Additional volume may be need to account for fluid losses due to vomiting, nasogastric tube output, diarrhea, large open wound, fever, hyperventilation, fistula drainage.
• Caution must be used in patients with history of CHF or evidence of volume overload
13

Energy Requirements:
• If the patient is NOT mechanically ventilated, the Mifflin St Jeor Equation can be
used to calculate resting metabolic rate (RMR).
Men: RMR = (9.99 X weight) + (6.25 X height) – (4.92 X age) + 5
Women: RMR = (9.99 X weight) + (6.25 X height) – (4.92 X age) – 161
(NB: weight in kg, height in cm)
Nutrition Care Manual Calculators. Available at:
Nutritioncaremanual.org. Accessed April 12, 2018.
14

Appropriate PN Dosing for Adult Patients:
15

Carbohydrate: DEXTROSE
• General information:• Ordered in “grams/day”
• Peripheral: Maximum concentration = 10% (10 g per 100 ml of PN solution)
• Provides 3.4 kcal/g
• Initiation of PN:• General population: 150-200 g/day
• Critically ill, DM, hyperglycemia: 100-150 g/day• See insulin dosing guidelines on Slide 34: Glycemia Related Complications
• Daily requirements:• General population: 4.3-7 g/kg/day
• Critically ill, DM, hyperglycemia: 2.9-5.8 g/kg/day
• Maximum recommended dose: ≤ 7 g/kg/day in stable patients.
Derenski et al. NCP. 2016;31:578-595.
16

Fat: INTRAVENOUS LIPID EMULSION (Intralipids®)
• General information:
• Ordered in “grams/day”
• Provides 10 kcal/g
• 20% lipid emulsion provides 2 kcal/ml
• Contains soybean oil and phospholipids from powdered egg yolk
• Contraindicated in patients with soy or egg allergy
• Necessary for the prevention of essential fatty acid deficiency.
• Dosing information:
• Stable patient: 1 g/kg/day
• Critically ill patient: ≤ 1 g/kg/day
Ayers P. (2014). ASPEN PN Handbook, 2nd edition.
17

Protein: AMINO ACIDS (Plenamine®, Aminosyn®, etc.)
• General information:
• Ordered in “grams/day”
• Provides 4 kcal/g
• 1 g of nitrogen is equivalent to 6.3 g of protein
• Dosing information:
18

Electrolyte Requirements
Electrolyte Maintenance Range Intake Maximums
Sodium 1-2 mEq/kg/d 150 mEq/L
Potassium 1-2 mEq/kg/d 240 mEq/d
Calcium 10-15 mEq/d 25 mEq/d
Magnesium 8-20 mEq/d 48 mEq/d
Phosphate 20-40 mmol/d 60 mmol/d
Chloride/acetate Change to maintain acid base balance
Derenski et al. NCP. 2016;31:578-595.
19

Electrolyte Requirements (cont’d)
• Electrolyte requirements for each patient depend on the current lab values,
current renal function, and the patient’s fluid status.
• Monitor electrolytes closely for patient on diuretics or with large GI fluid losses.
• Phosphate should be ordered in mMol (not mEq):
• Sodium Phosphate: 3 mMol phosphates per 4 mEq sodium
• Potassium Phosphate: 3 mMol phosphates per 4.4 mEq potassium
• The solubility of calcium and phosphate in PN solutions is dependent on the
final concentration of both calcium and phosphate, temperature, pH, and the
final concentration of both the amino acid and dextrose in the PN.
• The calcium and phosphorus product should not exceed 300 mEq in the PN
solution (>68 mg/dL serum) or tissue precipitation of calcium may occur.
20

Multivitamins (MVI)
• General information:
• Daily vitamin needs are provided by the standard addition of MVI.
• Certain disease states may require alterations in the daily minimum
requirements. For example,
• Chronic EtOH abuse
• Renal failure
• Short bowel syndrome
• Dosing information:
• 10 ml (1 amp) adult MVI is added automatically to each PN.
21

MVI contentsVitamin Daily Dose (10mL)
Thiamine (B1) 6 mg
Riboflavin (B2) 3.6 mg
Niacinamide (B3) 40 mg
Folic Acid 600 mcg
Dexpanthenol 15 mg
Pyridoxine (B6) 6 mg
Cyanocobalamin (B12) 5 mcg
Biotin 60 mcg
Ascorbic Acid (C) 200 mg
Retinol (A) 1 mg (3300 USP units)
Ergocalciferol (D3) 5 mcg (200 USP units)
dl-α Tocopherol acetate (E) 10 mg (10 USP units)
Phylloquinone (K1) 150 mcg
22

Trace Elements (TE, MTE, MTE-5®)
Trace Element 3 mL dose of MTE-5 Recommended daily dose
Chromium 12 mcg 10-15 mcg
Copper 1.2 mg* 0.3-0.5 mg*
Manganese 0.3 mg 0.6-0.10 mcg
Selenium 60 mcg 20-60 mcg
Zinc 3 mg 2.5-5 mg
Ayers P. (2014). ASPEN PN Handbook, 2nd edition.
* MTE-5® and generic versions are fixed-combination products providing the doses indicated in the above table. The American Society for
Parenteral and Enteral Nutrition (A.S.P.E.N.) has conducted an intensive review of commercially available trace element products and has
made recommendations on adjusting the amounts of TE in these products. Per A.S.P.E.N., “(e)fforts are currently under way to engage the
U.S. Food and Drug Administration (FDA) and the parenteral nutrient industry so A.S.P.E.N.'s recommendations can become a commercial
reality.” Nutr Clin Pract. 2015 Aug;30(4):559-69. doi: 10.1177/0884533615589992. Epub 2015 Jun 25.
23

Trace Elements (cont’d)
• General information:• MTE-5® (zinc, copper, chromium, manganese, and selenium) is routinely
added to PN solutions.
• Caution should be used in patients with liver impairment.
o Copper and manganese are hepatically cleared and should be excluded from PN until liver dysfunction resolves.
• Pharmacy will assist with adjusted dosing or alternatives when MTE are unavailable from manufacturers.
• Dosing information:• Recommended dose: 3 ml of MTE-5
• Selenium: Recommended daily dose of 60 mcg is provided in MTE-5.
o If there is a primary deficiency or increased need (e.g., CRRT), additional selenium should be ordered, up to 100 μg/day.
Worthington et al. JPEN 2017;41;324-377.
24

Trace Elements (cont’d)
Trace Element Clinical Considerations
Chromium Commercially unavailable at this time with no likelihood of availability for the foreseeable future; Likely not needed as a “stand-alone” PN additive since other PN additives feature chromium as a contaminant.
Copper Excreted in bile. Reduce or eliminate in severe hepatic dysfunction or cholestasis. Needs may increase with burns or CRRT.
Manganese Toxicity reported with current multiple-trace element product doses. Reduce or eliminate in severe hepatic dysfunction or cholestasis.
Selenium Add to PN if multiple-trace element products do not include selenium. Requirements may increase with CRRT.
Zinc Requirements may increase with skin (burns) and gastrointestinal (diarrhea, fistula, drains) losses.
Mundi et al. JPEN 2017;41;535-549.
25

Monitoring PN
Safe and effective PN therapy requires, at a minimum:
• Clinical monitoring of patient’s status.
• Weighing the patient prior to initiation of PN and daily
thereafter.
• Monitoring vitals signs: Temperature, pulse, RR, BP.
• Blood sugar checks every 4 hours for duration of PN with
appropriate insulin sliding scale coverage.
• Intake and output during each nursing shift.
26

Suggested Monitoring for PN PatientsParameter Baseline Initiation Critically Ill Stable Inpatient
Serum chemistries (Na, K, Cl,
CO2, serum urea nitrogen,
creatinine, ionized calcium,
magnesium, phosphorous,
serum glucose)
ALT, AST, ALP, total bilirubin
Yes Daily x 3 days Daily 1-2 x per week
Serum TG Yes Day 1 Weekly Weekly
CBC with differential Yes Weekly Weekly
INR, PT Yes Day 1 Weekly As needed
Capillary glucose No As needed Every 1-6 hours As needed
Weight Yes Daily Daily 2-3 x per week
Intake and output Yes Daily Daily Daily unless fluid
status assessed via
physical
examination
Derenski et al. NCP. 2016;31:578-595.
27

PN Adult Lab Order Set
TEST FREQUENCY
CMP DAILY X 30 DAYS
Mg DAILY X 5 DAYS, then WEEKLY X 30 DAYS
Phos DAILY X 5 DAYS, then WEEKLY X 30 DAYS
INR At initiation of PN, then WEEKLY x 30 DAYS
TG DAILY X 2 DAYS then WEEKLY X 30 DAYS
ACCUCHECKS Q4H for duration of PN therapy with correctional
insulin scale; contact MD for orders
28

Soarian CPOE:
BOTH FIELDS MUST BE CHECKED
29

Complications of PN
• Catheter related
• Biochemical
• Glycemia related
• Lipid disorders
• Refeeding syndrome
• Organ-specific complications
30

Catheter related Complications
• Mechanical:
o Occlusion
o Thromboses
o Pneumothorax
• Infection
o Central venous catheter infections
31

Biochemical complications
• Hypo- or Hypernatremia
• Hypo- or Hyperkalemia
• Hypo- or Hyperchloremia
• Hypo- or Hypercalcemia
• Phosphate abnormalities
• Vitamin abnormalities
32

Prevention of Biochemical Complications
• Measure the electrolyte levels daily beginning with initiation of PN and
monitor at set intervals.
• Recognize that the likelihood of certain biochemical alterations can be
increased by pre-existing diseases including:
• Chronic renal failure
• Cirrhosis
• DM
• Acidosis
• Severe nutritional deficiency
• Recognize the need for supplementation of specific vitamins and
minerals.
33

Glycemia Related Complications
• Blood sugar goal = <180 mg/dL
• Hyperglycemia is a frequent consequence of PN, most often due to an underlying
inability to handle a glucose load.
o May result in unwanted renal effects such as polyuria and hyperfiltration.
o May also be a contributing factor in the development of fatty liver.
• Gastric dysrhythmias may also occur making PN weaning difficult.
• Insulin is often infused in the PN solution in the following recommended* initial doses:
o 1 unit / 11 gm of dextrose in patients with DM.
o 1 unit / 20 gm of dextrose in non-DM patient.
• Hypoglycemia will usually occur only in one of two situations: during PN cycling or at PN
discontinuation.
o In order to avoid this, patients should be monitored every fifteen minutes for one hour after the discontinuation of PN.
o PN should be discontinued using the tapering methods described above in slides #8 & #9.
*Gosmanov, et al Management of Hyperglycemia During Enteral and Parenteral Nutrition Therapy Curr Diab Rep. 2013 Feb; 13(1): 155–162.
34

Lipid Disorders
• The most common lipid abnormality seen with the use of PN is a combination
of decreased HDL, elevated LDL and increased triglyceride levels.
o Possible causes:
Secondary to the lipid solution overwhelming the ability to metabolize the infusion.
Possible alteration in lipoprotein lipase activity.
• Use caution in initiating PN for patients with triglycerides ≥400.
• Consider reducing or discontinuing lipids if triglycerides >300.
• Elevated lipid levels are believed to be directly responsible for the development
of fatty liver.
• Cycling of PN allows the patient time to metabolize and redistribute the infused
lipids and ultimately avoid lipid alterations and associated sequela.
35

Refeeding Syndrome
• Refeeding syndrome can be defined as the potentially fatal shifts in fluids and
electrolytes that may occur in malnourished patients receiving artificial refeeding
(whether enterally or parenterally). These shifts result from hormonal and
metabolic changes and may cause serious clinical complications.*
• Commonly seen in patients with severe malnutrition or prolonged NPO status
• Feeding with carbohydrates results in endogenous insulin release, leading to
enhanced intracellular uptake of glucose, phosphorous, potassium and
magnesium. Low serum concentrations of these electrolytes occur secondary to
total body depletion. Fluctuation of water soluble vitamins, especially thiamine
may also occur.
• Feeding with carbohydrates also results in a reduction of sodium and water
excretion which can lead to a rapid expansion of extracellular fluid volume and
may predispose the patient to fluid overload.
• May need to consider giving additional thiamine 100 mg per day in PN solution
*BMJ. 2008 Jun 28; 336(7659): 1495–1498.
36

Refeeding Syndrome
• Clinical symptoms of refeeding may occur in the first 24-48 hours after
initiation of nutritional support and may include:
• CHF
• Confusion
• Weakness
• Glucose intolerance
• Respiratory depression
• Nutritional repletion should be carefully initiated at less than full caloric and
fluid requirements, and gradually advanced to avoid cardiac overload and
rapid electrolyte shifts.
• Electrolytes should be closely monitored during the first week of refeeding
and adjusted as necessary.
37

Organ-specific Effects: RENAL
• For patients with chronic renal disease, hydration is a critical issue:
o UNDERHYDRATION: may result in a worsening of the renal function
while overhydration.
o OVERHYDRATION: may lead to fluid overload and edema.
• Electrolytes should be carefully monitored and managed.
o Special attention should be paid to magnesium and phosphate
levels as they may accumulate in these patients.
38

Organ-specific Effects: HEPATIC• 90% of patients receiving PN will have alterations in liver enzymes in the first
2 weeks of therapy.
• After 6 weeks of PN therapy:
o 100% of PN patients will have biliary sludge
o 42% will eventually develop stones
o 4% will get acalculous cholecystitis
o 19% will develop calculous cholecystitis
• Monitor liver enzymes. Most abnormal enzymes will resolve spontaneously. If
elevations in the enzymes persist, it may be necessary to discontinue PN
therapy.
• Recent data has suggested that many hepatic complications of PN can be
avoided by cycling PN.
• Excessive calories should be avoided as this may result in a predisposition to
fatty liver.
39

GI Effects
• Although studies performed in normal volunteers show that
there is no change in gastrointestinal permeability to nutrients
when given PN, there is clearly a mucosal atrophy that is
measurable when the GI tract is not bathed in nutrients
during normal digestion.
• A small amount of enteral nutrition can be provided during
PN which may curtail the changes in the integrity of the GI
tract making tolerance for the restarting of feeding easier.
• After initiation of PN, the GI tract should be reassessed for
opportunity to initiate enteral nutrition.
40

Reassessing GI Tract
• Due to documented benefits of enteral nutrition (EN), repeated efforts should
be made to transition the patient to EN.
• Considerations in transitioning to EN:
o Bowel sounds and evidence of bowel function (i.e., passing flatus or stool) are not required for initiation of EN.
o Upon initiation of EN, PN calories should be reduced;
PN should be discontinued when patient meets >60% of energy needs from oral or enteral nutrition.
McClave et al. JPEN. 2016;40:159-211.
41

Restarting Enteral Nutrition
• Consult dietitian for specific recommendation
• Polymeric formula
• Contains intact nutrients (whole proteins)
• Use for normal or near normal functioning bowel
• Hydrolyzed formula
• Contains partially or completely hydrolyzed nutrients (peptides, amino acids, or combination of both) and altered fats
• Use for extensive impairment of GI function (significant malabsorptive disorders such as persistent diarrhea, pancreatic disease or significant GI resection)
Kozenicki et al. NCP. 2015;30:634-651.
42

Requirements for PN Ordering
1. Order must be submitted via CPOE before 1 PM.
2. Patient must have active IV line.
3. Patient must have nutrition consult.
4. Both “Day 1 Adult Parenteral Nutrition with Consults” and “Parenteral Nutrition – Adult
Lab Orders” boxes must be checked when entering PN via CPOE. (See Slide #7.)
5. In the event that a renewal order has not been received by Pharmacy for a patient
currently receiving PN therapy, a NUTRITION and METABOLIC SUPPORT (NMS)
CONSULT will be initiated.
43

For Questions and Help
• Pharmacy Department: 55492
• Clinical Nutrition Department: 53136
44

Questions
45

TRUE or FALSE:
Complications of PN include:
• Line-related complications
• Biochemical complications
• Glycemia-related complications
• Lipid disorders
• Refeeding syndrome
46

True
47

TRUE or FALSE:
Biochemical complications include:
• Hypo- or Hypernatremia
• Hypo- or Hyperkalemia
• Hypo- or Hyperchloremia
• Hypo- or Hypercalcemia
• Phosphate abnormalities
• Vitamin abnormalities
48

True
49

TRUE or FALSE:
To prevent biochemical complications:
• Measure the electrolyte levels daily beginning with the
initiation of PN.
• Continue to monitor electrolyte levels at set intervals.
50

True
51

Choose the best answer:
What appropriate measures must be taken if PN is abruptly
discontinued?
A. Hang D5W at the same rate as the PN was running.
B. Hang D10W at the same rate as the PN was running.
C. Hang D10W at the same rate as the PN was running AND
obtain blood glucose levels after 30 minutes.
D. Change to PO diet.
52

C.
53

PN solutions with an osmolarity > 900 mOsmol/L may be
infused peripherally if the patient has adequate peripheral
access.
TRUE or FALSE:
54

FALSE
55

TRUE or FALSE:
It is appropriate to provide PN to patients with a functioning
GI tract.
56

FALSE
57

TRUE or FALSE:
Because safe and timely processing of PN orders requires multiple steps, including:
• Consultation and recommendations from the RD,
• CPOE by the prescriber,
• Evaluation by the pharmacist for clinical appropriateness,
• Clarification of orders, if necessary,
• Transmission to the outsource provider for compounding by their cutoff time of 3:30pm,
• Delivery by courier from Philadelphia to the pharmacy by 730pm daily,
• Additional checking by the evening pharmacist,
• Delivery to the patient prior to 9pm,
• Final checking by the RN and administration to the patient.
PN orders must be submitted via CPOE before 1 PM.
58

TRUE
59